")
Back to Journals » Journal of Pain Research » Volume 15
Pain Empathy and Its Association with the Clinical Pain in Knee Osteoarthritis Patients
Authors Zhao R, Ji Y, Li J, Li X, Wu T, Wu H, Liu C
Received 20 June 2022
Accepted for publication 5 November 2022
Published 19 December 2022 Volume 2022:15 Pages 4017—4027
DOI https://doi.org/10.2147/JPR.S379305
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Ruipeng Zhao,1 Yupei Ji,2 Jiahui Li,1 Xinhua Li,1 Ting Wu,1 Hongru Wu,3 Cuizhen Liu2
1Department of Orthopaedics, The Second Hospital of Shanxi Medical University, Shanxi Key Laboratory of Bone and Soft Tissue Injury Repair, Taiyuan, People’s Republic of China; 2School of Psychology, Shaanxi Normal University, Xi’an, People’s Republic of China; 3Shanxi Institute of Sports Science, Taiyuan, People’s Republic of China
Correspondence: Cuizhen Liu, 199 South Chang’an Road, Xi’an, 710062, People’s Republic of China, Tel +86-15129060061, Email [email protected]
Objective: Knee osteoarthritis (KOA) is a painful chronic disorder. Evidence has shown that a history of chronic pain plays an important role in shaping empathy. Empathy, a valuable indicator of social functioning that refers to an individual’s ability to share the experiences of others, however, has been overlooked in KOA patients. This study aimed to investigate empathy and its association with clinical pain in KOA patients.
Methods: KOA patients (n=47) and healthy controls (HCs, n=44) completed two empathy-for-pain tasks: a pain judgment task in which participants judged whether a person in an image felt pain or not, and a pain rating task in which they estimated pain intensity for themselves and others. The Interpersonal Reactivity Index was used to measure participants’ trait empathy, and clinical severity and psychological factors were assessed using relevant instruments.
Results: Compared to HCs, KOA patients showed higher accuracy when judging pain and non-pain images and reported overall higher pain intensity when rating for themselves and others. KOA patients also showed greater personal distress than HCs in terms of their self-reported empathy. Moreover, pain catastrophizing particularly mediated the relationship between pain severity and pain ratings for others, and depression, anxiety, and pain catastrophizing all mediated the association between pain severity and empathy-induced personal distress.
Conclusion: These findings suggest that patients with KOA have increased empathy, demonstrated by elevated sensitivity to pain-related scenes and intense emotional responses.
Keywords: empathy, pain, knee osteoarthritis, pain catastrophizing, emotion
Introduction
Knee osteoarthritis (KOA) is a degenerative type of arthritis characterized by chronic pain and widespread disability. Patients with KOA often demonstrate pain sensitization and hypervigilance to pain, showing reduced pain threshold and increased sensitivity to experimental pain and pain-related cues.1,2 It has been proposed that a history of chronic pain could play an important role in shaping people’s empathy for pain in pain-related disorders such as fibromyalgia,3 somatoform pain disorder,4 and musculoskeletal disorder.5 Empathy, referring to the ability of individuals to share the experiences of others, is of high importance for the maintenance of interpersonal relationships.6 Thus, empathy may play a protective role in the psychological and social aspects of chronic pain.7,8 Investigating empathy in patients with KOA has the potential to enhance our understanding of the social functioning associated with the condition and shed light on psychological approaches to the management of KOA pain.
Empathy consists of two dissociable components: affective empathy, which highlights the ability to resonate with others’ mental and physical states (eg, vicariously experiencing their emotions and affectively reacting to the observed feelings), and cognitive empathy, which refers to the ability to adopt another’s perspective and comprehend their experiences.9,10 In painful situations, observing others in pain elicits automatic affective responses to empathize with others’ physical and emotional experiences.7 Explicitly assessing others’ pain intensity via perspective-taking reflects an individual’s cognitive empathy in responding to painful stimuli.11,12 Notably, previous research regarding the affective and cognitive aspects of responding to a painful stimulus has primarily focused on state empathy via laboratory-based experiments.13 However, empathy has also been studied as a trait, referred to as a relatively stable characteristic that reflects people’s general sensitivity to the states and emotions of others.9 Evidence has shown that state and trait empathy seem to be related, possibly interacting with each other to shape behaviors.14,15 Therefore, investigating empathy from both state and trait perspectives can broaden clinicians’ understanding of patients’ empathy, contributing to both research and clinical decision-making.
In KOA, long-term suffering from pain and the diminished ability to carry out daily activities is often accompanied by mental health problems such as depression and anxiety,16,17 and KOA patients with higher pain intensity have a higher risk of developing these problems.18,19 KOA can also be accompanied by impaired cognitive function, particularly, pain catastrophizing, which has been found to explain a significant proportion of pain in KOA patients.20 Considering that chronic pain causes cognitive-emotional disturbances and cognitive and emotional factors shape empathy, it is reasonable to assume that the relationship between pain severity in KOA and empathy is likely to be mediated by these psychological processes.
Briefly, despite the prevalence of emotional problems associated with KOA, the highly related psychological process of empathy, particularly empathy for pain, is often overlooked in patients with KOA.21 Therefore, the present study aimed to investigate empathy and its association with clinical pain in KOA from a multidimensional perspective. Specifically, we instructed participants on two classical empathy-for-pain paradigms—the pain judgment task and the pain rating task—to measure state empathy. Moreover, Interpersonal Reactivity Index (IRI), developed by Davis22 was applied to measure both affective and cognitive components of participants’ trait empathy. Furthermore, the putative modulatory roles of psychosocial factors including depression and anxiety, as well as pain catastrophizing, were explored to elucidate the relationship between pain severity and empathy in KOA. We hypothesized that KOA patients would reveal increased empathy, and that the relationship between pain severity and empathy is likely to be mediated by illness-related emotions and cognition such as depression, anxiety, and pain catastrophizing.
Methods
Participants
Forty-seven inpatients with chronic KOA pain (13 males and 34 females; Mage = 66.26 years, SD = 6.52) and 44 healthy controls (HCs; 18 males and 26 females; Mage = 64.75, SD = 8.41 years) participated in the study. The demographic characteristics of all subjects were collected. This study was approved by the Ethics Committee of the Second Hospital of Shanxi Medical University. All participants voluntarily signed informed consent forms before participation.
For patients, the criteria for inclusion were as follows: (i) inpatients clinically diagnosed with KOA, (ii) aged above 50 years, (iii) course of disease ≥ 1 year with overall pain intensity ≥ 3/10 on the Numerical Rating Scale (NRS), (iv) have no other types of chronic pain, (v) have no other major physical or mental disorders, and (vi) have no cognitive impairments that prevent them from completing the study assessment procedures. The inclusion criteria for controls were the same as those for the patients, excluded criteria i and iii.
Pain Severity Assessments
Bilateral weight-bearing fixed-flexion posteroanterior radiographs of the knee were obtained by the patients’ physicians. The radiographic K-L classification was used to reflect the severity of knee illness.23 The participants also reported the duration of their illness course. Five patients could not recall the date of illness onset; thus, they left this item blank when checking the details of the illness.
Knee-specific pain was assessed using the Western Ontario and McMaster Universities Arthritis (WOMAC) Index.24 The WOMAC is a multidimensional and responsive questionnaire that provides information on osteoarthritis symptoms, including pain (five items), stiffness (two items), and functional disability (17 items).
Questionnaires
As the participants in this study were older adults, depression and anxiety were assessed using the Geriatric Depression Scale - shortened form (GDS-S)25 and Geriatric Anxiety Inventory (GAI),26 respectively. The GDS-S is a 15-item scale that measures the presence of depression in older adults via responses in a “yes/no” format. The GAI consists of 20 “agree/disagree” items designed to assess general anxiety symptoms. The Pain Catastrophizing Scale (PCS) is a 13-item scale developed to help quantify catastrophic thinking related to pain.27 Of note, these questionnaires are all short and easy to use, making them ideal for older adults who are easily fatigued or limited in their ability to concentrate for a long time.
Self-report trait empathy was assessed using the Interpersonal Reactivity Index (IRI), a 28-item questionnaire consisting of four discrete seven-item subscales.22 The fantasy subscale assesses one’s tendency to imaginatively transpose oneself into fictitious situations and characters, such as in books and movies. The perspective-taking subscale gauges one’s ability or proclivity to adopt another’s perspectives when interacting with other people in real-life scenarios, reflecting cognitive empathy. The final two subscales reflect emotional empathy, with the empathic concern subscale assessing the degree to which one experiences the feelings of others, and the personal distress subscale measuring one’s own feelings when witnessing the negative experiences of others. These psychological questionnaires were administered to both the patient and HC groups.
Empathy Tasks: Pain Judgment and Pain Rating Task
After completing the above questionnaires, the participants were instructed to perform a pain judgment and body laterality judgment task. The pain judgment task is used extensively to assess empathy for pain, reflected by judgment accuracy. As illustrated in Figure 1, each trial began with a fixation cross presented on the screen for 2–4s. Then, the image was presented and participants were required to judge whether the person in the image felt pain or not within 5s. Their responses were highlighted in a white rectangle for 1s. In the laterality judgment task, following the same timeline, participants were asked to judge whether the image depicted the left or right side of the body part (eg, hand/foot). The laterality judgment task measures individuals’ implicit aspect of empathy, as research has demonstrated that empathetic responses can be elicited automatically without explicit demand to evaluate pain in this task.28 Notably, the pain judgment task and laterality judgment task enlist equivalent cognitive load and match in task difficulty.28
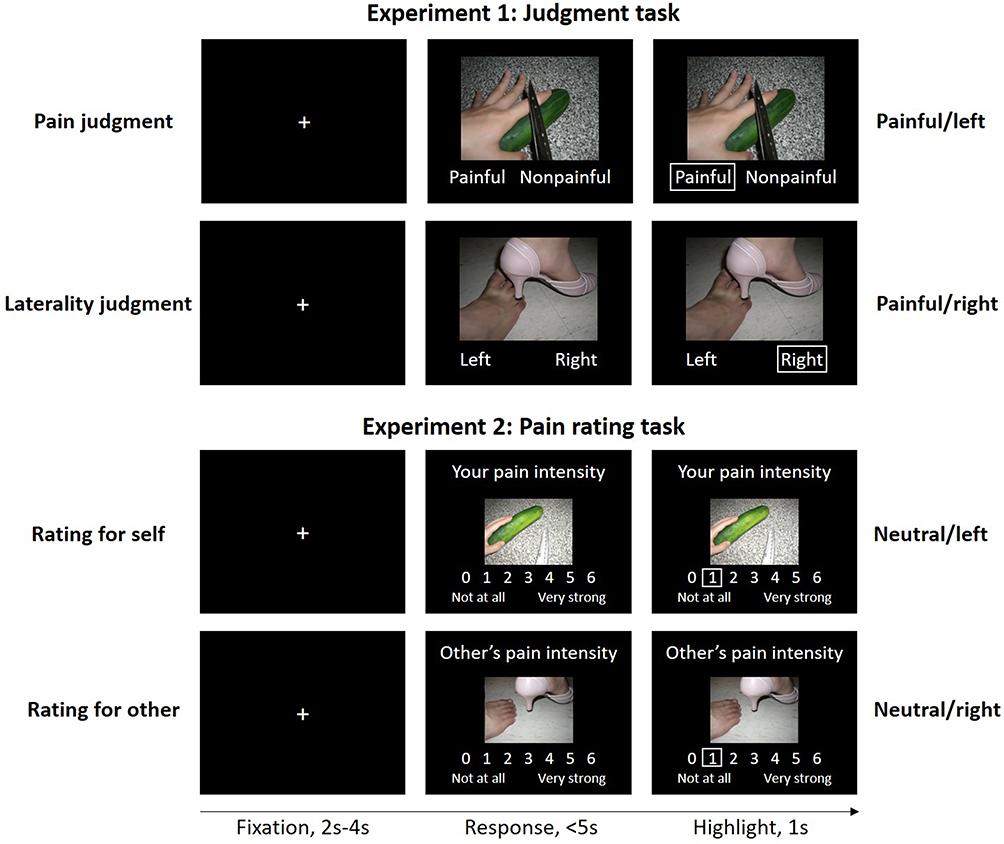 |
Figure 1 Sample stimuli, task designs, and procedures. Stimuli used in the current study are digital photographs showing another person’s left or right body part (eg, hand/foot) in painful or neutral situations. Four representative examples of stimuli (painful/left, painful/right, neutral/left, neutral/right) are displayed in four task sample trials. In Experiment 1, participants indicated whether the person in the image was suffering pain or not in the pain judgment session and whether the image depicted the left or right side of the body part in the laterality judgment session. In Experiment 2, participants reported the pain intensity of the depicted painful image for themselves and others respectively. |
Following the pain and body side judgment tasks, participants completed a pain rating task in which they reported pain intensity for themselves and others, respectively (Figure 1). In the self condition, participants were asked to imagine how painful it would be if they experienced the scenario depicted in the picture. In the other condition, participants rated the pain intensity that would be experienced by a familiar person (eg, their spouse). Ratings were made from 0 to 6, with 0 representing no pain at all, and 6 representing very strong pain.
Participants practiced each task to familiarize themselves with the procedure. The images used in the practice sessions were different from those in the formal test session. The pain judgment task consisted of 48 trials. The pain rating task consisted of 24 trials, as only images depicting painful scenarios used in the pain judgment task were included in this task. The entire procedure could be completed in approximately 20 min.
Statistical Analyses
Statistical analyses were performed using SPSS version 25.0 (https://www.ibm.com/products/spss-statistics) and R version 4.1.1 (https://www.r-project.org/). Demographic characteristics and psychological questionnaire scores were compared between KOA patients and HCs using an independent-samples t-test or a Pearson’s chi-square test, as appropriate. Descriptive statistics were provided for clinical variables. The relationships between pain sensitivity, pain catastrophizing, self-report empathy, and task-measured empathy were estimated using Spearman correlation analyses.
To assess between-group differences in the judgment task, we conducted a 2 (task: pain judgment vs body judgment) × 2 (group: KOA vs HC) repeated-measures analysis of variance (ANOVA) on task accuracy. Post hoc simple t-tests were applied following significant interactions. Moreover, considering that education may affect task performance, we treated it as a covariate in the ANOVA analysis to control its potential influence.
To assess between group differences in the pain rating task, a mixed-effects ordinal logistic regression was conducted in R, considering the ordinal attribute of pain ratings and repeated measures. The group (KOA vs HC) and condition (rating for the self and others) were treated as the fixed effects and the subject as the random effect. Spearman correlations were further used to examine whether there was consistency in performance between the judgment and rating tasks, given that both reflect empathy.
To investigate the potential mediating effects of disease-related emotion/cognition (depression, anxiety, and pain catastrophizing) on the relationship between pain severity and empathy (both scale-measured and task-measured indexes), mediation analyses using PROCESS v3.0 were conducted,29 with significant correlations among these variables as preconditions. The significance of the mediation effects was calculated using a bootstrapping procedure, with 5000 bootstrap resamples to generate bias-corrected 95% confidence intervals (CIs). CIs that did not include the zero value indicated a significant mediation effect.
Results
Demographical and Clinical Characteristics
Detailed demographic information and questionnaire scores for the participants are presented in Table 1. KOA patients had defects in either one or both knees. Radiographs of both knees were assessed according to the K-L grading criteria for the patient, and the final grade assigned to a subject’s knee score was the highest grade for the more severely affected knee.30 Accordingly, among 47 KOA patients, 23 (49%) had severe changes (K-L grade = 4), 23 (49%) had moderate changes (K-L grade = 3), and one (2%) had minimal change (K-L grade = 2). The average duration of illness was 9.95 ± 7.17 years for the representative affected knee.
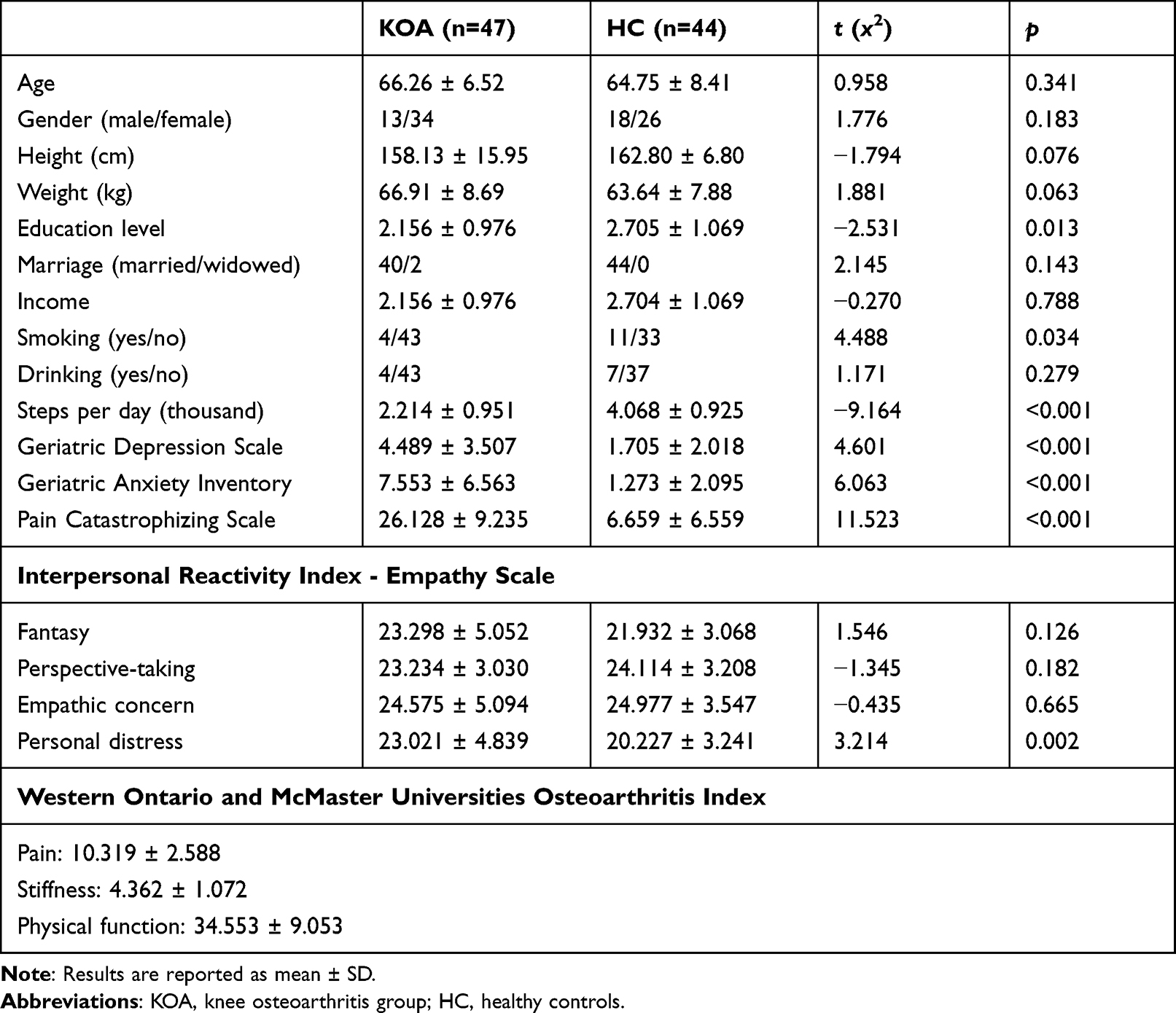 |
Table 1 Demographic and Psychological Characteristics of Knee Osteoarthritis Patients and Healthy Controls |
Notably, two KOA patients and two HCs did not complete the computer-based empathy procedures, as they were not willing to continue. One KOA patient quit the study after completing the empathy judgment task because of an unexpected disruption, leaving 42 patients for analysis.
There were no significant differences between the KOA and HC groups in age (p = 0.341), sex (p = 0.183), marriage (p = 0.143, 5 missing), income (p = 0.788), and drinking status (p = 0.279). The education level of HCs was higher than that of KOA patients (p = 0.013), and there were more smokers in the HC group than in KOA patients (p = 0.034). The HC group members on average had significantly more steps per day than KOA patients (p < 0.001).
Regarding psychological questionnaires, the KOA group had significantly higher scores for depression (p < 0.001), anxiety (p < 0.001), and pain catastrophizing (p < 0.001) than the HC group. With regard to self-reported empathy, KOA patients showed greater personal distress than HCs (p = 0.002), suggesting increased emotional empathy in KOA patients (ie, feeling more anxiety and discomfort when observing others’ negative experiences). There were no significant differences in scores for the fantasy (p = 0.126), perspective-taking (p = 0.182), or empathic concern (p = 0.665) subscales between the groups.
Heightened Empathy for Pain in Judgment and Rating Tasks in KOA Patients
In Experiment 1, a repeated-measures ANOVA on judgment accuracy revealed a main effect of the task [F(1, 85) = 67.01, p < 0.001,  = 0.44], with a higher accuracy rate for the body side judgment (M = 0.92, SE= 0.01) than for the pain judgment (M= 0.80, SE = 0.01) (Figure 2A). The main effect of group (KOA vs HC) was not significant [F(1, 85) = 1.15, p = 0.286,
= 0.44], with a higher accuracy rate for the body side judgment (M = 0.92, SE= 0.01) than for the pain judgment (M= 0.80, SE = 0.01) (Figure 2A). The main effect of group (KOA vs HC) was not significant [F(1, 85) = 1.15, p = 0.286,  = 0.01]. Importantly, there was a significant interaction between group and task [F(1, 85) = 31.24, p < 0.001,
= 0.01]. Importantly, there was a significant interaction between group and task [F(1, 85) = 31.24, p < 0.001,  = 0.27]. Specifically, in the pain judgment task, KOA patients showed higher accuracy (M = 0.87, SE = 0.01) than HCs (M = 0.83, SE = 0.02; p < 0.001). In the body laterality judgment task, however, KOA patients showed lower accuracy (M = 0.77, SE = 0.02) than HCs (M = 0.96, SE = 0.01; p = 0.006). Furthermore, considering the significant differences in education levels between KOA patients and HCs and its potential influence on task performance, we included education as a covariate for the analysis of judgment accuracy, and found the pattern of results was consistent without its inclusion. These findings suggest that KOA patients have heightened empathy for pain, given the increased accuracy of pain judgment. Notably, the pain judgment task captured the explicit affective component of empathy.
= 0.27]. Specifically, in the pain judgment task, KOA patients showed higher accuracy (M = 0.87, SE = 0.01) than HCs (M = 0.83, SE = 0.02; p < 0.001). In the body laterality judgment task, however, KOA patients showed lower accuracy (M = 0.77, SE = 0.02) than HCs (M = 0.96, SE = 0.01; p = 0.006). Furthermore, considering the significant differences in education levels between KOA patients and HCs and its potential influence on task performance, we included education as a covariate for the analysis of judgment accuracy, and found the pattern of results was consistent without its inclusion. These findings suggest that KOA patients have heightened empathy for pain, given the increased accuracy of pain judgment. Notably, the pain judgment task captured the explicit affective component of empathy.
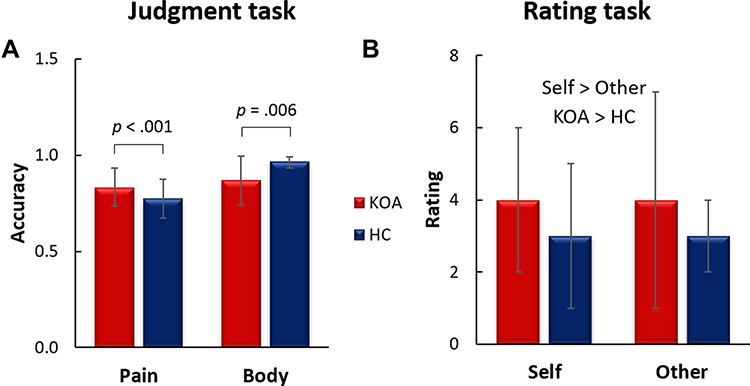 |
Figure 2 (A) Judgment accuracy for conditions of pain (painful or not) and body laterality (left or right) judgments between KOA and HC groups in the judgment task. p values indicate simple t-test results following the significant interaction. Error bars represent standard deviations. (B) Medians of pain rating for conditions of rating for self and others between KOA and HC groups in the rating task. KOA > HC indicates the main effect of the group. Self > Other indicates the main effect of the condition. Error bars represent interquartile ranges. Abbreviations: KOA, knee osteoarthritis; HC, healthy control. |
In Experiment 2 of the rating task, the logistic regression on pain rating showed a main effect of the condition (z = 2.52, p = 0.01), reporting higher pain intensity when rating for oneself than for others (Figure 2B). The main effect of group was also significant (z = 4.67, p < 0.001). KOA patients reported overall higher pain intensity than HCs, suggesting increased pain empathy for others in KOA patients. There was no interaction between self/other conditions and group (z = 0.11, p = 0.91). Increased pain ratings in the KOA patients indicated that patients were sensitive to others’ pain, showing a heightened cognitive empathy in evaluating others.
Correlations Between Empathy Tasks in Two Groups
Task performance in the two empathy experiments was correlated for the HCs. Specifically, there was a positive correlation between pain judgment accuracy and self-pain rating in HCs (r = 0.503, p =0.001) (Figure 3A). Pain judgment accuracy was also correlated with pain ratings for others (r =0.399, p =0.009) (Figure 3B). However, no such correlation was observed in KOA patients. Specifically, the correlation between pain judgment accuracy and pain rating for self was not significant (r = –0.108, p =0.486), and the correlation between pain judgment accuracy and pain rating for others was not significant as well (r = –0.114, p = 0.462) in patients (Figure 3C and D). Together, these findings suggest consistency in participants’ responses to the pain perception and evaluation tasks in the HCs, while KOA patients were less consistent in their pain-related empathy responses.
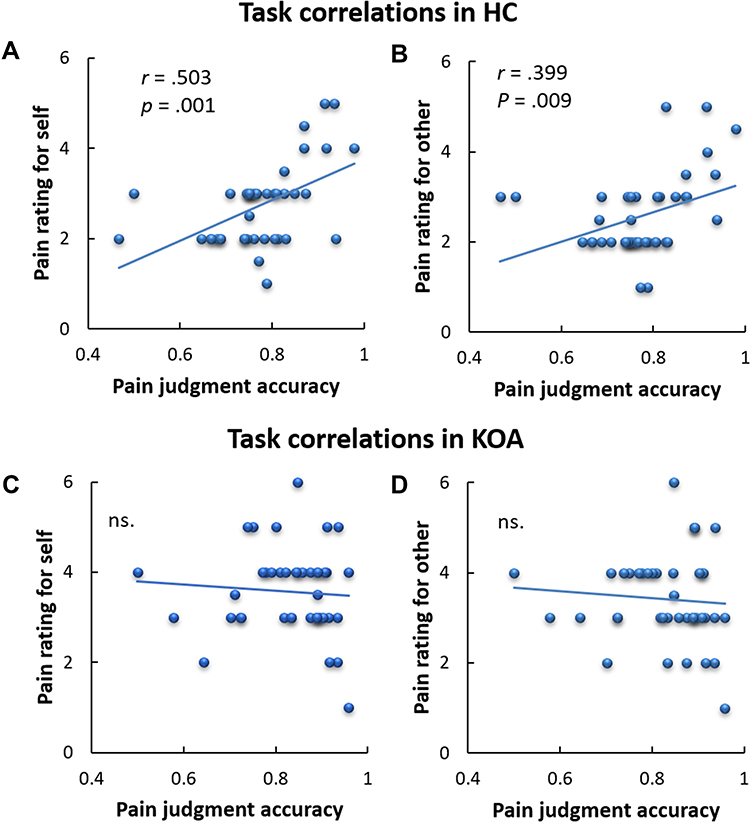 |
Figure 3 Positive correlations between pain judgment accuracy and pain ratings in healthy controls (A and B). No correlations in knee osteoarthritis patients (C and D). Abbreviations: KOA, knee osteoarthritis; HC, healthy control; ns., not significant. |
Depression, Anxiety, and Pain Catastrophizing Mediate the Relationship Between Pain Severity and Empathy in KOA Patients
Correlations between pain severity (WOMAC score), depression (GDS-S score), anxiety (GAI score), pain catastrophizing (PCS score), and empathy in patients are summarized in Table 2. Of note, in the exploratory analysis, the WOMAC score was only correlated with the IRI personal distress and pain ratings for others, but not with other empathy indices. Thus, we examined the mediation effect of these two empathy indices.
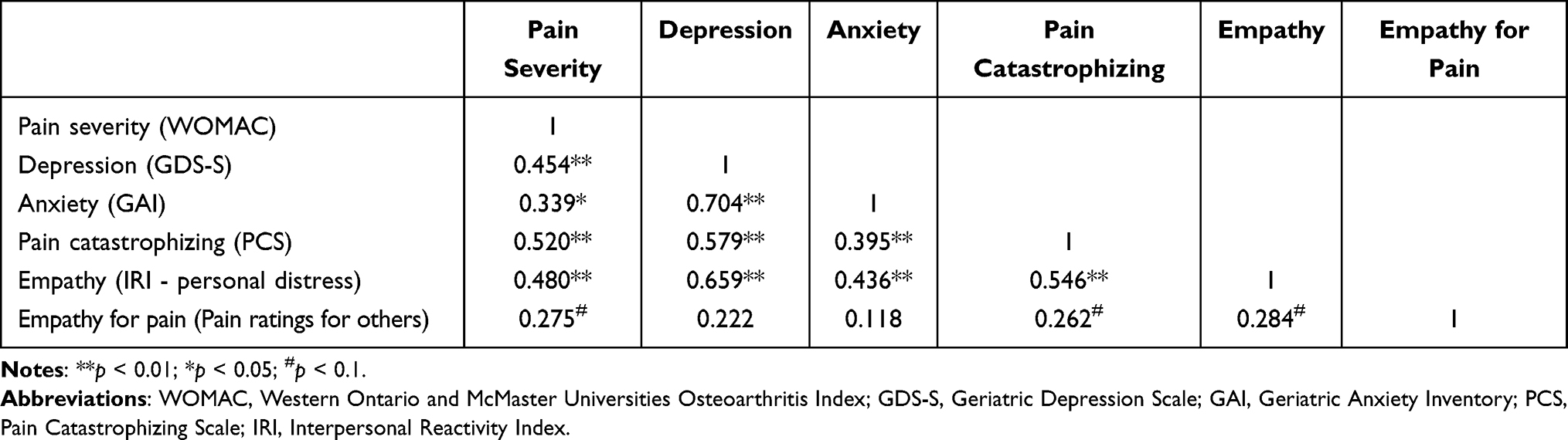 |
Table 2 Correlations Between Pain Severity, Psychological Variables, and Empathy in Knee Osteoarthritis Patients |
Pain rating for others (assessed in the rating task) was only correlated with pain catastrophizing, but not with depression and anxiety. Therefore, we examined the mediating role of pain catastrophizing. The results showed that pain catastrophizing mediated the relationship between pain severity and pain ratings (Figure 4A). This finding suggests that severe symptoms of illness lead to abnormal pain catastrophizing cognition, which further results in heightened empathy for pain in others.
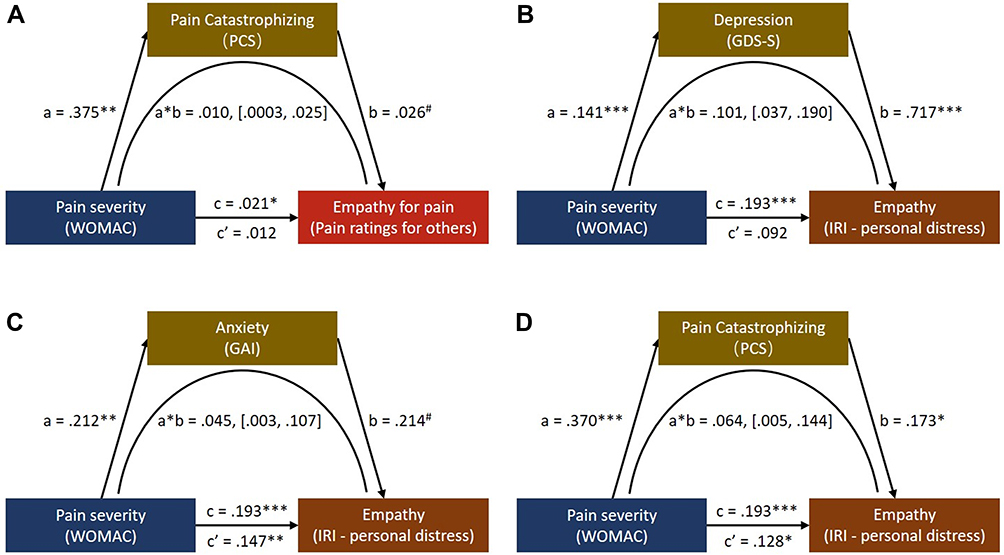 |
Figure 4 (A) The mediating role of pain catastrophizing on the effect of pain severity (WOMAC) on empathy for pain (pain ratings for others). (B–D) The mediating roles of depression, anxiety, and pain catastrophizing on the effect of pain severity (WOMAC) on empathy (IRI - personal distress). ***p < 0.001; **p < 0.01; *p < 0.05; #p = 0.06, which indicates a marginal significance. Values in [] represent bootstrapping results with 95% confidence intervals for the lower and upper limits. Abbreviations: WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; GDS-S, Geriatric Depression Scale - shortened form; GAI, Geriatric Anxiety Inventory; PCS, Pain Catastrophizing Scale; IRI, Interpersonal Reactivity Index. |
Mediation models of empathy-personal distress showed that depression (Figure 4B), anxiety (Figure 4C), and pain catastrophizing (Figure 4D) mediated the influence of pain severity on personal distress. These findings indicate that severe illness causes negative emotions (eg, depression and anxiety) as well as pain catastrophizing, and these negative feelings and cognitions affect the empathy components of individuals’ personal distress.
Discussion
This study obtained several key findings. First, in the pain judgment task, in comparison to HCs, KOA patients showed higher accuracy when judging pain and non-pain images. In the pain rating task KOA patients reported an overall higher pain intensity in rating for themselves and others than did the HCs. KOA patients also showed greater personal distress than HCs in terms of their self-reported empathy. Overall, these findings suggest that KOA patients have increased empathy, that is, heightened sensitivity to pain-related scenes and intense emotional responses. However, in the pain empathy paradigms, pain judgment accuracy was positively correlated with the pain rating for oneself and others across HCs, but no such significant correlations were observed in KOA patients. This inconsistency in patients’ pain-related empathy responses suggests that patients with KOA might display an abnormal, heightened response pattern in pain perception and evaluation. Furthermore, depression, anxiety, and pain catastrophizing mediated the association between pain severity and empathy-induced personal distress. In particular, pain catastrophizing mediated the relationship between pain severity and pain ratings for others. Together, these findings indicate that increased empathy in patients may result from intense affective reactions and abnormal pain catastrophic cognition, which are caused by severe disease symptoms.
The elevated empathy for pain in KOA patients suggests that past experiences may increase empathy. Consistent with this finding, Fallon et al found that patients with fibromyalgia, a disorder characterized by widespread chronic pain, not only have elevated sensitivity to first-hand experimental pain, but also exhibit increased empathic ratings and augmented event-related potential (ERP) responses to others’ pain.3 Moreover, among healthy individuals, research also implies that people with higher sensitivity to first-hand pain reveal greater sensitivity in discriminating others’ pain, estimate greater pain intensity in others, and have greater ERP responses.31 Taken with the results of the current study, we can conclude that chronic pain experiences shape individuals’ pain-related empathy processing at the behavioral and brain levels.
It is worth noting that although empathy is fundamental for social interaction, hyperarousal of empathic response is not beneficial for healthy social functioning. Previous studies have reported that acute distress and insufficient inhibitory control, implying a poorer capacity to control arousal and reactivity, are associated with people who are overly sensitive to others’ pain.32,33 In this context, our findings suggest that KOA patients may be hypersensitive to others’ pain, suggesting an abnormal pattern in pain perception and emotional response. Indeed, this view is further supported by our findings on the correlations between empathy and pain tasks. In general, as demonstrated in the HCs, there should be consistency between pain judgment performance and pain intensity rating, given that both capture one’s pain empathy capacity. However, no correlation was observed in the KOA group. In other words, although KOA patients showed relatively heightened sensitivity to the pain of others, their ability to process this information appeared to be impaired, revealing an inconsistency in empathic responses. Thus, a more nuanced interpretation of empathic disturbances in KOA patients is required.
Notably, our findings revealed the mediating role of pain catastrophizing in pain intensity and empathy for pain in KOA patients. Specifically, severe and chronic pain in KOA patients causes pain catastrophizing, and such negative feelings and cognitions affect patients’ empathy when evaluating others’ pain in the pain rating task. As pointed out previously, KOA is a typical chronic pain disorder and is often accompanied by negative affective and cognitive responses. Notably, these heightened negative emotions may trigger more catastrophic thoughts about pain, leading to catastrophic elevation of pain.34 Moreover, evidence has demonstrated that pain catastrophizing could predict individuals’ pain sensation for both themselves and others,35 causing those in current pain (eg, KOA patients) to have higher levels of pain empathy.36 Considering that pain catastrophizing is an important risk factor in shaping empathy in KOA patients, it should be treated via cognitive-emotional therapeutic approaches that target patients’ exaggerated attitudes toward pain and reduce pain symptoms in patients.37
Among the IRI subscales, KOA patients displayed higher personal distress scores than HCs, indicating that KOA patients experienced an amplified degree of self-oriented distress and heightened levels of anxiety and discomfort in the face of other people in need. Moreover, KOA patients with severe pain reported even greater personal distress. These findings confirm that KOA patients have increased empathy for pain and suggest that patients can transpose themselves imaginatively into others’ emotions more easily and become more distressed after experiencing chronic pain first-hand.38 Furthermore, we found that the relationship between pain severity and empathy-related personal distress in KOA patients was mediated by psychological factors including depression, anxiety, and pain catastrophizing. As a degenerative disease characterized by chronic pain and diminished physical function, KOA has the potential to change the mental state of those who experience it, and patients are more prone to suffer depression, anxiety, and pain-related cognitive impairment.39 Indeed, these illness-related emotions and cognitions (depression, anxiety, and pain catastrophizing) are intercorrelated themselves,40 and they work jointly to mediate the association between pain severity and empathy-related personal distress in KOA patients. Together, the current study illustrates the functions of these psychological factors in modulating emotional empathy in patients with KOA, highlighting the necessity to intervene in these psychological processes.
To our knowledge, this is the first study to examine the relationship between empathy and clinical pain in KOA patients. We used a multidimensional measurement approach, combining empathy-for-pain experiments with a questionnaire to assess state and trait empathy systematically. Notably, the participants had a high degree of homogeneity and were all KOA patients or HCs over 50 years old. Thus, our findings provide a targeted reference value for future treatments in this group. Several limitations of this study should be considered when interpreting the findings. First, the present study only assessed outcomes for individuals experiencing KOA; hence, the internal associations found in the current study and to what extent these findings generalize to chronic pain conditions other than KOA are worth further exploration. It would be helpful to compare KOA patients with other chronic pain disorders via clinical trials on empathic capacity. Second, it is worth noting that the correlations between clinical pain severity and psychological measures were weak, which limited the application of the findings into clinical practice. In addition, further studies of the pathophysiology and associated neurocognitive functions of KOA are needed to identify the potential mechanisms underlying the increased empathic capacity in KOA patients.
In conclusion, our study elucidated the detailed relationship between pain and empathy in KOA patients. These patients have increased empathy, demonstrating heightened sensitivity to pain-related scenes and intense emotional responses. Moreover, the relationship between pain severity and empathy in patients is regulated by pain-related mood and cognition (eg, depression, anxiety, and pain catastrophizing). Overall, these findings provide new insights into the psychological mechanisms of empathy for pain, as well as chronic pain prevention and management strategies for KOA patients.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the Second Hospital of Shanxi Medical University.
Acknowledgments
The abstract of this paper was presented at the IASP Conference as a poster presentation with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ at the 2022 World Congress on Pain: [https://iaspworldcongress2022.org/presentations/presentation/pain-empathy-in-knee-osteoarthritis-patients-ptu26/].
Funding
This work was supported by grants from the National Natural Science Foundation of China (Grant No. U21A20353), the Shanxi Province Colleges and Universities Science and Technology Innovation Project (Grant No. 2021L179), the Basic Research Program of Shanxi Province (Grant No. 202103021223443), and the Start-up Funding of Shaanxi Normal University (Grant No. 1110011242).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Fingleton C, Smart K, Moloney N, et al. Pain sensitization in people with knee osteoarthritis: a systematic review and meta-analysis. Osteoarthr Cartil. 2015;23(7):1043–1056. doi:10.1016/j.joca.2015.02.163
2. Pujol J, Martínez-Vilavella G, Llorente-Onaindia J, et al. Brain imaging of pain sensitization in patients with knee osteoarthritis. Pain. 2017;158(9):1831–1838. doi:10.1097/j.pain.0000000000000985
3. Fallon N, Li X, Chiu Y, et al. Altered cortical processing of observed pain in patients with fibromyalgia syndrome. J Pain. 2015;16(8):717–726. doi:10.1016/j.jpain.2015.04.008
4. Peng W, Meng J, Lou Y, et al. Reduced empathic pain processing in patients with somatoform pain disorder: evidence from behavioral and neurophysiological measures. Int J Psychophysiol. 2019;139:40–47. doi:10.1016/j.ijpsycho.2019.03.004
5. Zhang H-B, Ou H, Meng D-H, et al. Impaired cognitive empathy in outpatients with chronic musculoskeletal pain: a cross-sectional study. Neural Plast. 2021;2021:1–10. doi:10.1155/2021/4430594
6. Coutinho JF, Silva PO, Decety J. Neurosciences, empathy, and healthy interpersonal relationships: recent findings and implications for counseling psychology. J Couns Psychol. 2014;61(4):541. doi:10.1037/cou0000021
7. Goubert L, Craig KD, Vervoort T, et al. Facing others in pain: the effects of empathy. Pain. 2005;118(3):285–288. doi:10.1016/j.pain.2005.10.025
8. Lim J-A, Choi S-H, Lee WJ, et al. Cognitive-behavioral therapy for patients with chronic pain: implications of gender differences in empathy. Medicine. 2018;97(23):e10867. doi:10.1097/MD.0000000000010867
9. Cuff BMP, Brown SJ, Taylor L, et al. Empathy: a review of the concept. Emot Rev. 2016;8(2):144–153. doi:10.1177/1754073914558466
10. Walter H. Social cognitive neuroscience of empathy: concepts, circuits, and genes. Emot Rev. 2012;4(1):9–17. doi:10.1177/1754073911421379
11. Jackson PL, Brunet E, Meltzoff AN, et al. Empathy examined through the neural mechanisms involved in imagining how I feel versus how you feel pain. Neuropsychologia. 2006;44(5):752–761. doi:10.1016/j.neuropsychologia.2005.07.015
12. Fan Y, Duncan NW, de Greck M, et al. Is there a core neural network in empathy? An fMRI based quantitative meta-analysis. Neurosci Biobehav Rev. 2011;35(3):903–911. doi:10.1016/j.neubiorev.2010.10.009
13. Nezlek JB, Schutz A, Lopes P, Smith CV. Naturally occurring variability in state empathy. In: Empathy in Mental Illness. Cambridge University Press; 2007:187–200.
14. Olsson A, McMahon K, Papenberg G, et al. Vicarious fear learning depends on empathic appraisals and trait empathy. Psychol Sci. 2016;27(1):25–33. doi:10.1177/0956797615604124
15. Van der Graaff J, Meeus W, de Wied M, et al. Motor, affective and cognitive empathy in adolescence: interrelations between facial electromyography and self-reported trait and state measures. Cogn Emot. 2016;30(4):745–761. doi:10.1080/02699931.2015.1027665
16. Edwards RR, Cahalan C, Mensing G, et al. Pain, catastrophizing, and depression in the rheumatic diseases. Nat Rev Rheumatol. 2011;7(4):216–224. doi:10.1038/nrrheum.2011.2
17. Iijima H, Aoyama T, Fukutani N, et al. Psychological health is associated with knee pain and physical function in patients with knee osteoarthritis: an exploratory cross-sectional study. BMC Psychol. 2018;6(1):1–10. doi:10.1186/s40359-018-0234-3
18. Sharma A, Kudesia P, Shi Q, et al. Anxiety and depression in patients with osteoarthritis: impact and management challenges. Open Access Rheumatol. 2016;8:103. doi:10.2147/OARRR.S93516
19. Rosemann T, Laux G, Szecsenyi J, et al. Pain and osteoarthritis in primary care: factors associated with pain perception in a sample of 1021 patients. Pain Med. 2008;9(7):903–910. doi:10.1111/j.1526-4637.2008.00498.x
20. Somers TJ, Keefe FJ, Pells JJ, et al. Pain catastrophizing and pain-related fear in osteoarthritis patients: relationships to pain and disability. J Pain Symptom Manage. 2009;37(5):863–872. doi:10.1016/j.jpainsymman.2008.05.009
21. Lyness E, Vennik JL, Bishop FL, et al. Exploring patient views of empathic optimistic communication for osteoarthritis in primary care: a qualitative interview study using vignettes. BJGP Open. 2021;5(3):
22. Davis MH. Measuring individual differences in empathy: evidence for a multidimensional approach. J Pers Soc Psychol. 1983;44(1):113. doi:10.1037/0022-3514.44.1.113
23. Kellgren JH, Lawrence J. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494. doi:10.1136/ard.16.4.494
24. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15(12):1833–1840.
25. Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5(1–2):165–173.
26. Pachana NA, Byrne GJ, Siddle H, Koloski N, Harley E, Arnold E. Development and validation of the geriatric anxiety inventory. Int Psychogeriatr. 2007;19(1):103–114. doi:10.1017/S1041610206003504
27. Sullivan MJ, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524. doi:10.1037/1040-3590.7.4.524
28. Gu X, Liu X, Guise KG, et al. Functional dissociation of the frontoinsular and anterior cingulate cortices in empathy for pain. J Neurosci. 2010;30(10):3739. doi:10.1523/JNEUROSCI.4844-09.2010
29. Hayes AF. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling. University of Kansas; 2012.
30. Lethbridge‐çejku M, Scott WW, Reichle R, et al. Association of radiographic features of osteoarthritis of the knee with knee pain: data from the Baltimore longitudinal study of aging. Arthritis Care Res. 1995;8(3):182–188. doi:10.1002/art.1790080311
31. Li X, Liu Y, Ye Q, et al. The linkage between first-hand pain sensitivity and empathy for others’ pain: attention matters. Hum Brain Mapp. 2020;41(17):4815–4828. doi:10.1002/hbm.25160
32. Young KA, Gandevia SC, Giummarra MJ. Vicarious pain responders and emotion: evidence for distress rather than mimicry. Psychophysiology. 2017;54(7):1081–1095. doi:10.1111/psyp.12865
33. Decety J, Lamm C. Human empathy through the lens of social neuroscience. Sci World J. 2006;6:1146–1163. doi:10.1100/tsw.2006.221
34. Wong WS, Lam HMJ, Chen PP, et al. The fear-avoidance model of chronic pain: assessing the role of neuroticism and negative affect in pain catastrophizing using structural equation modeling. Int J Behav Med. 2015;22(1):118–131. doi:10.1007/s12529-014-9413-7
35. Sullivan M, Martel MO, Tripp DA, et al. Catastrophic thinking and heightened perception of pain in others. Pain. 2006;123(1):37–44. doi:10.1016/j.pain.2006.02.007
36. Serbic D, Ferguson L, Nichols G, et al. The role of observer’s fear of pain and health anxiety in empathy for pain: an experimental study. Br J Pain. 2020;14(2):74–81. doi:10.1177/2049463719842595
37. Martinez-Calderon J, Flores-Cortes M, Clavero-Cano S, et al. The role of positive psychological factors in the association between pain intensity and pain interference in individuals with chronic musculoskeletal pain: a cross-sectional study. J Clin Med. 2020;9(10):3252. doi:10.3390/jcm9103252
38. Moriarty O, McGuire BE, Finn DP. The effect of pain on cognitive function: a review of clinical and preclinical research. Prog Neurobiol. 2011;93(3):385–404. doi:10.1016/j.pneurobio.2011.01.002
39. Bäckryd E, Persson EB, Larsson AI, et al. Chronic pain patients can be classified into four groups: clustering-based discriminant analysis of psychometric data from 4665 patients referred to a multidisciplinary pain centre (a SQRP study). PLoS One. 2018;13(2):e0192623. doi:10.1371/journal.pone.0192623
40. Galvez-Sánchez CM, Montoro CI, Duschek S, et al. Depression and trait-anxiety mediate the influence of clinical pain on health-related quality of life in fibromyalgia. J Affect Disord. 2020;265:486–495. doi:10.1016/j.jad.2020.01.129
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.