Back to Journals » Orthopedic Research and Reviews » Volume 18
Exploring the Role of Cissus quadrangularis in Osteoporosis Management
Authors Manocchio N ![]() , Sorbino A, Devito A, Gallelli L
, Sorbino A, Devito A, Gallelli L ![]() , Romanello D, Rotunno S, Foti C
, Romanello D, Rotunno S, Foti C ![]() , Migliore A
, Migliore A ![]()
Received 15 March 2026
Accepted for publication 2 May 2026
Published 18 May 2026 Volume 2026:18 609378
DOI https://doi.org/10.2147/ORR.S609378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qian Chen
Nicola Manocchio,1 Andrea Sorbino,1 Antonio Devito,2 Luca Gallelli,3 Daniele Romanello,2 Sara Rotunno,2 Calogero Foti,1 Alberto Migliore4
1Physical and Rehabilitation Medicine, Clinical Sciences and Translational Medicine Department, Tor Vergata University, Rome, Italy; 2Internal Medicine Unit, S. Pietro Fatebenefratelli Hospital, Rome, 00189, Italy; 3Department of Health Science, University Magna Graecia of Catanzaro, Catanzaro, 88100, Italy; 4Rheumatology Unit, S. Pietro Fatebenefratelli Hospital, Rome, 00189, Italy
Correspondence: Nicola Manocchio, Email [email protected]
Abstract: Cissus quadrangularis (CQ) is a Vitaceae-derived medicinal plant rich in flavonoids, phytosterols, triterpenoids, vitamins, and bone-relevant minerals, conferring combined antioxidant, anti-inflammatory, phytoestrogenic, and osteoanabolic properties that modulate key pathways involved in bone remodeling. This narrative review aims to synthesize preclinical and clinical evidence on CQ as a potential adjunct in osteoporosis management. Preclinical studies demonstrate that CQ enhances osteoblast differentiation, collagen and matrix deposition, and mineralization, while inhibiting osteoclastogenesis and inflammatory osteoclastogenic cytokines, leading to improved bone microarchitecture, bone mineral density, and callus formation in fracture and estrogen-deficiency models. CQ phytobioactives have also been successfully integrated into advanced biomaterials, exosome-like vesicles, and self‑emulsifying drug delivery systems, improving bioavailability, osseointegration, and regenerative performance in critical-sized defects and implant models. Clinical data, although limited and heterogeneous, consistently indicate that CQ accelerates fracture healing, reduces bone pain, and increases functional recovery in maxillofacial and mandibular fractures, with favorable effects on serum calcium, alkaline phosphatase, and osteopontin expression and without major safety concerns based on available short-term data. In postmenopausal osteopenia, randomized trials show that 24‑week oral CQ stabilizes bone turnover markers and delays bone loss, albeit without short‑term gains in bone mineral density. CQ thus emerges as a multi-target, generally well-tolerated candidate for integrative osteoporosis care, particularly for early bone loss (i.e., osteopenia), fracture healing, and osteoprotection during antiresorptive drug holidays (i.e., temporary suspension of bisphosphonate therapy, particularly in the context of dental procedures). However, the absence of standardized formulations, small sample sizes, short follow-ups, and lack of head‑to‑head comparisons with standard anti‑osteoporotic therapies currently available underscore the need for long-term, multicenter randomized controlled studies using bioavailable, well-characterized CQ preparations.
Keywords: bisphosphonates, bone mineral density, Cissus, osteoporosis, review
Introduction
Osteoporosis (OP) is a significant global health concern affecting over 200 million individuals, particularly postmenopausal women and the elderly. It is characterized by reduced bone mineral density (BMD) and deterioration of bone tissue microarchitecture, leading to an increased risk of fractures that can cause substantial morbidity and diminished quality of life (QoL).1 The condition results in physical limitations in activities of daily living (ADLs) and consequent increased healthcare costs, making effective treatment strategies imperative.2 A multitude of pharmacological therapies are now available for OP management, including bisphosphonates, selective estrogen receptor modulators (SERMs), denosumab, teriparatide, and romosozumab.3 These medications serve distinct roles; for example, bisphosphonates and SERMs primarily act as antiresorptive agents, while teriparatide and romosozumab function as anabolic therapies.4 Despite the efficacy of these treatments in enhancing BMD and reducing fracture risk, adherence and compliance remain significant challenges due to associated side effects and financial burdens. Studies have indicated that while drugs such as romosozumab demonstrate superior fracture risk reduction compared to traditional bisphosphonates, concerns about adverse events like cardiovascular complications and the cost of these newer therapies influence patient acceptance.5 It is noteworthy that cost-effectiveness analyses indicate that while agents like romosozumab and denosumab yield better clinical outcomes, they also represent a considerable expense, complicating decisions related to long-term management of OP.6 Furthermore, transitioning patients between therapies poses additional challenges. For instance, pharmaceutical strategies such as suspending bisphosphonates in conjunction with dental procedures can complicate treatment regimens and necessitate therapeutic windows to minimize adverse effects during a transition period.7 This is particularly critical for patients with a history of osteoporotic fractures, who comprise a substantial demographic that may face heightened risk factors during treatment adjustments.8 The clinical implications of these suspensions and the need for careful management highlight the intricate balance required in optimizing therapeutic outcomes while ensuring patient safety and adherence.
In this context, the necessity for potential alternative treatments becomes paramount.
This need is further amplified by documented patient preferences: epidemiological surveys have consistently reported that many patients under treatment for OP use some form of complementary and alternative medicine, with herbal preparations, vitamin supplements, and relaxation techniques being the most frequently reported modalities.9 Poor long-term adherence to conventional anti-osteoporotic pharmacotherapy, driven by gastrointestinal intolerance, fear of rare but serious adverse events such as osteonecrosis of the jaw or atypical femoral fracture, and the financial burden of long-term treatment, further motivates patients to seek plant-derived adjuncts perceived as safer and more aligned with a holistic approach to skeletal health.10 Throughout history, medicinal plants have served as remedies for diverse pathological conditions.11 Cissus quadrangularis (CQ - a.k.a. Veldt grape, Winged Treebine, or Adamant Creeper - Figure 1), predominantly found in regions such as America, Australia, India, Sri Lanka, Java, Southeast Asia, and Africa, is a well-known medicinal plant belonging to the Vitaceae family.
 |
Figure 1 Cissus quadrangularis plant. |
CQ exhibits a unique bone-joining ability, earning it the Sanskrit name Asthisandhan and the Hindi name Hadjod, both of which literally translate to “bone setter”.12 Although not very widespread in the Western world, CQ is widely utilized in Eastern medicine, primarily for the treatment of bone fractures and as an analgesic. CQ extracts have been reported to contain a wide variety of bioactive compounds, including alkaloids, phytoestrogenic steroids, calcium, resveratrol, piceatannol, Parthenocissus, ascorbic acid, carotene, flavonoids, vitamins, enzymes, nicotinic acid, tyrosine, triterpenoids (including β-sitosterol, δ-amyrin, and ketosteroid).13 Amongst the various medicinal properties (e.g., anti-inflammatory, antioxidant, antimicrobial, antiobesity, antinociceptive, anticonvulsant, and antidiabetic effects), anti-osteoporotic ones are the most studied and demonstrated for CQ.14,15 Notably, unlike currently approved pharmacological agents, which are classified as either predominantly antiresorptive (e.g., bisphosphonates, denosumab) or predominantly osteoanabolic (e.g., teriparatide, romosozumab), CQ appears to confer both antiresorptive and osteoanabolic effects simultaneously within a single phytocomplex.
From a regulatory perspective, CQ is available in several jurisdictions as an over-the-counter dietary supplement or traditional herbal preparation, with regulatory classification varying by country and no harmonized EU-level authorization currently in place.
This narrative review aims to report a qualitative synthesis of the current literature on CQ in OP management, focusing on its mechanisms, efficacy, safety, and research gaps, with the goal of exploring the possibility and the opportunity to integrate CQ in some clinical scenarios of OP management.
Phytochemical Composition and Mechanisms of Action
CQ extracts are rich in various phytochemicals and minerals relevant to bone health. The bone protective potential of CQ is highlighted by various phytochemicals that support two complementary ways to improve bone homeostasis: anabolic stimulation of osteoblast differentiation and mineralization, and antiresorptive suppression of osteoclastogenesis.
CQ contains flavonoids such as quercetin, kaempferol, daidzein, and quercitrin, as well as polyphenols like resveratrol and piceatannol.16 These compounds possess significant antioxidant and anti-inflammatory activities, which contribute to their beneficial effects on bone metabolism.17 Flavonoids including quercetin, kaempferol, and daidzein have been demonstrated to enhance osteoblast differentiation, inhibit osteoclastogenesis, and regulate signaling pathways involved in bone remodeling, such as the mitogen-activated protein kinase (MAPK), receptor activator of nuclear factor-κB and its ligand (RANK/RANKL), osteoprotegerin (OPG), and estrogen receptor pathways.18 Quercetin and kaempferol, in particular, promote osteogenic activity, while daidzein acts as a phytoestrogen with anti-resorptive effects.19 Phytosterols, particularly β-sitosterol, have high concentration in CQ extracts. CQ also features ketosteroids (anabolic or phytoestrogenic steroidal substances). These compounds may participate in modulating lipid metabolism and exhibit estrogenic action relevant for bone metabolism.20 CQ “triterpenoid” fraction, which includes δ-amyrin and δ-amyrone, among other alkaloids, appears to contribute to the plant’s antioxidant and anti-inflammatory properties and may further support bone regenerative effects.21 Vitamins are also well represented. CQ is a natural source of vitamin C (i.e., ascorbic acid), vitamin A (i.e., carotene), and provides a significant content of minerals such as calcium, phosphorus, zinc, iron, magnesium, and strontium. These are all relevant nutrients for bone formation and mineralization.22
CQ offers a dual approach to managing OP by both enhancing bone formation (i.e., osteogenesis) and inhibiting excessive bone resorption. The management of oxidative stress is vital, given that excessive free radical generation and compromised antioxidant defenses contribute to the onset of age-related diseases, including metabolic bone disorders and bone mass reduction.23 Flavonoids are integral to this action by providing antioxidant and anti-inflammatory capacity, effectively alleviating cellular oxidative stress which otherwise impairs bone remodeling and precipitates bone mass decline.24 Specifically, flavonoids suppress pro-inflammatory osteoclastogenic cytokines, including interleukin 1β (IL-1β), IL-6, and Tumor Necrosis Factor α (TNF-α), while elevating anti-osteoclastogenic signals.15,25 Quercetin and isorhamnetin can modulate inflammatory cell activity and the transcription of pro-inflammatory genes, notably by suppressing the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway.26 CQ extract has shown potential in protecting osteogenic cells, such as MC3T3-E1 cells, from hydrogen peroxide-induced oxidative damage, supporting its role in cellular defense and bone maintenance.27 Concurrently, the triterpenes and alkaloids in CQ promote the synthesis and deposition of collagen and mucopolysaccharides, essential elements for matrix mineralization and repair.28,29 Additionally, CQ inhibits gene expression of key cytokines and matrix metalloproteinases, thus alleviating inflammatory responses at the cellular level.28 Phytosterols and steroidal compounds exhibit phytoestrogenic activity, modulating the bone remodeling process by stimulating osteoblasts via estrogen receptors and contributing to anti-resorptive potential.30 Lastly, the high natural content of calcium and phosphorus in CQ provides the foundational mineral elements, accelerating matrix biomineralization and contributing to the observed enhancement of BMD and mechanical strength through the upregulation of MAPK-dependent alkaline phosphatase activity in osteoblasts.31 This multifaceted phytochemical profile ultimately supports improved osteoblast differentiation and mineralization, while inhibiting RANKL-induced osteoclastogenesis and reducing bone loss. Table 1 summarizes main CQ’s components and mechanisms of action.
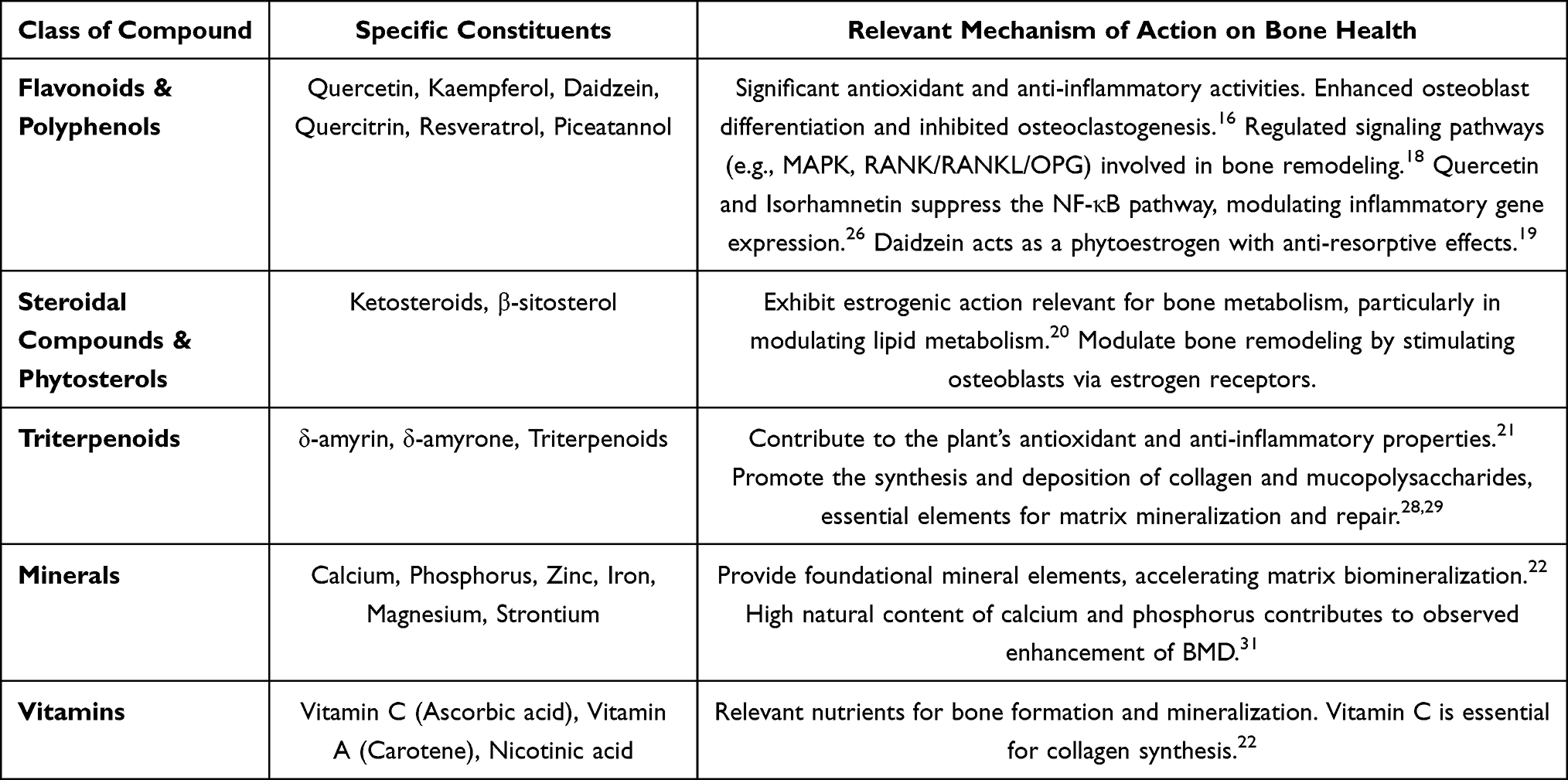 |
Table 1 Main Cissus Quadrangularis Components and Mechanisms of Action |
Preclinical Evidence
The robust anti-osteoporotic potential of CQ has been comprehensively validated across diverse preclinical platforms, revealing critical mechanisms underpinning its dual-action capacity.32 Beyond stimulating the upregulation of osteogenic markers like Runx2 and Alkaline Phosphatase (ALP) demonstrated in in vitro studies,33 the pro-osteogenic activity of CQ extends to innovative regenerative applications. For instance, exosome-like nanovesicles isolated from CQ callus tissue actively induce osteogenic lineage commitment in human mesenchymal stem cells (hMSCs) and myoblast (C2C12) cells.34 These CQ exosomes significantly enhance ALP activity and mineralization (assessed through Alizarin Red staining) in hMSCs, surpassing levels achieved by positive control media after 14 and 21 days, respectively. Furthermore, extracts obtained using ethyl acetate (0.3 mg/mL) demonstrated superior efficacy in promoting the maturation of bone marrow mesenchymal stem cells (BM-MSCs) by increasing ALP gene expression three times compared to positive controls.35 In complex tissue engineering, CQ phytobioactives integrated into nano-hydroxyapatite ceramic nano-cement enhanced neo-bone formation in a critical-sized tibial defect model in vivo, yielding significantly higher volumes of mineralized tissue and volumetric bone formation compared to non-functionalized cement.27 This optimized bioactive fraction, rich in polyphenols and flavonoids, concomitantly provided protection against cellular oxidative stress while promoting cellular proliferation and migration in vitro. The translational relevance is further supported by evidence from a rabbit model, where a novel CQ Chitosan Hydrogel coating on titanium implants significantly improved osseointegration, showing higher new bone formation and increased Implant Stability Quotient and Removal Torque Quotient values at 12 weeks.36 Crucially, the anti-resorptive capacity of CQ is robustly demonstrated in models simulating postmenopausal osteoporosis.15 In ovariectomized mice, oral CQ attenuated inflammatory bone loss, resulting in a significant reduction in bone resorption markers, such as Howship’s lacunae in femoral cortical areas. Micro-computed tomography confirmed that CQ dramatically enhanced bone microarchitecture, significantly improving parameters like volumetric bone formation, trabecular thickness, and connectivity density in the fifth lumbar vertebra region and femur, while reducing destructive indices. This protection seems to be partially mediated through an osteoimmunological effect: CQ regulates the host immune system by significantly increasing anti-osteoclastogenic immune cells [e.g. lymphocytes T helper1 (Th1), Th2, Regulatory T cells (Tregs), and Regulatory B cells (Bregs)] and concurrently lowering osteoclastogenic Th17 cells in lymphoid organs.15 This results in a favorable shift in the serum cytokine balance, characterized by increased anti-osteoclastogenic cytokines [e.g. Interferon-gamma (IFN-γ), IL-4, and IL-10] and decreased pro-inflammatory osteoclastogenic cytokines (e.g., TNF-α, IL-6, and IL-17). The preclinical evaluation of CQ extends beyond generalized OP models into specialized regenerative medicine, tissue engineering, and pharmaceutical formulation optimization. For guided bone regeneration applications, a composite biomaterial incorporating CQ extract within a gelatin/pectin polymeric matrix reinforced by β-tricalcium phosphate (β-TCP) demonstrated substantial in vitro osteogenic expression, achieving 168.0% and 188.0% upregulation for Runt-related transcription factor 2 (RUNx2) and Osteocalcin (OCN) respectively, positioning it as a potent biomaterial for bone tissue repair.30 Furthermore, CQ’s efficacy in complex tissue restoration is highlighted in models of periodontal regeneration, where scaffolds composed of hyaluronic acid (HA) doped with ovine tendon extracellular matrix (ECM) and CQ extract showed maximum proliferation and tenogenic activity of mesenchymal stem cells in vitro, confirming its utility beyond purely osseous tissue.37 This regenerative capacity was mirrored in a zebrafish caudal fin amputation model, employed to mimic periodontal bone regeneration criteria, where composite scaffolds containing CQ, carrageenan, tendon ECM, and silver tricalcium phosphate (Ag-TCP) exhibited superior regeneration characterized by organized tissue regrowth, enhanced collagen deposition, and reduced inflammatory responses compared to control groups.38 In published fracture healing models, the use of alcoholic CQ extracts (alone or combined with Cryptolepis buchanani and Sardinella longiceps) in Wistar rats effectively restored bone strength and reduced the repair period by supplying rich phytochemicals that elevate serum calcium levels.16 Lastly, in inflammatory models such as monosodium iodoacetate (MIA)-induced osteoarthritis (OA) in rats, CQ extract mitigates knee joint damage, reduces subchondral bone erosion, and preserves cartilage integrity by suppressing the mRNA expression of key inflammatory mediators (i.e., inducible nitric oxide synthase, Cyclooxygenase-2, 5-Lipoxygenase) and Matrix Metalloproteinases, thereby preventing extracellular matrix degradation.32 Collectively, these preclinical findings strongly support CQ’s versatility as an effective dual-action agent that promotes osteogenesis and facilitates complex tissue repair, justifying its integration into next-generation regenerative materials and improved delivery platforms. Table 2 summarizes main findings from preclinical studies assessing CQ potential.
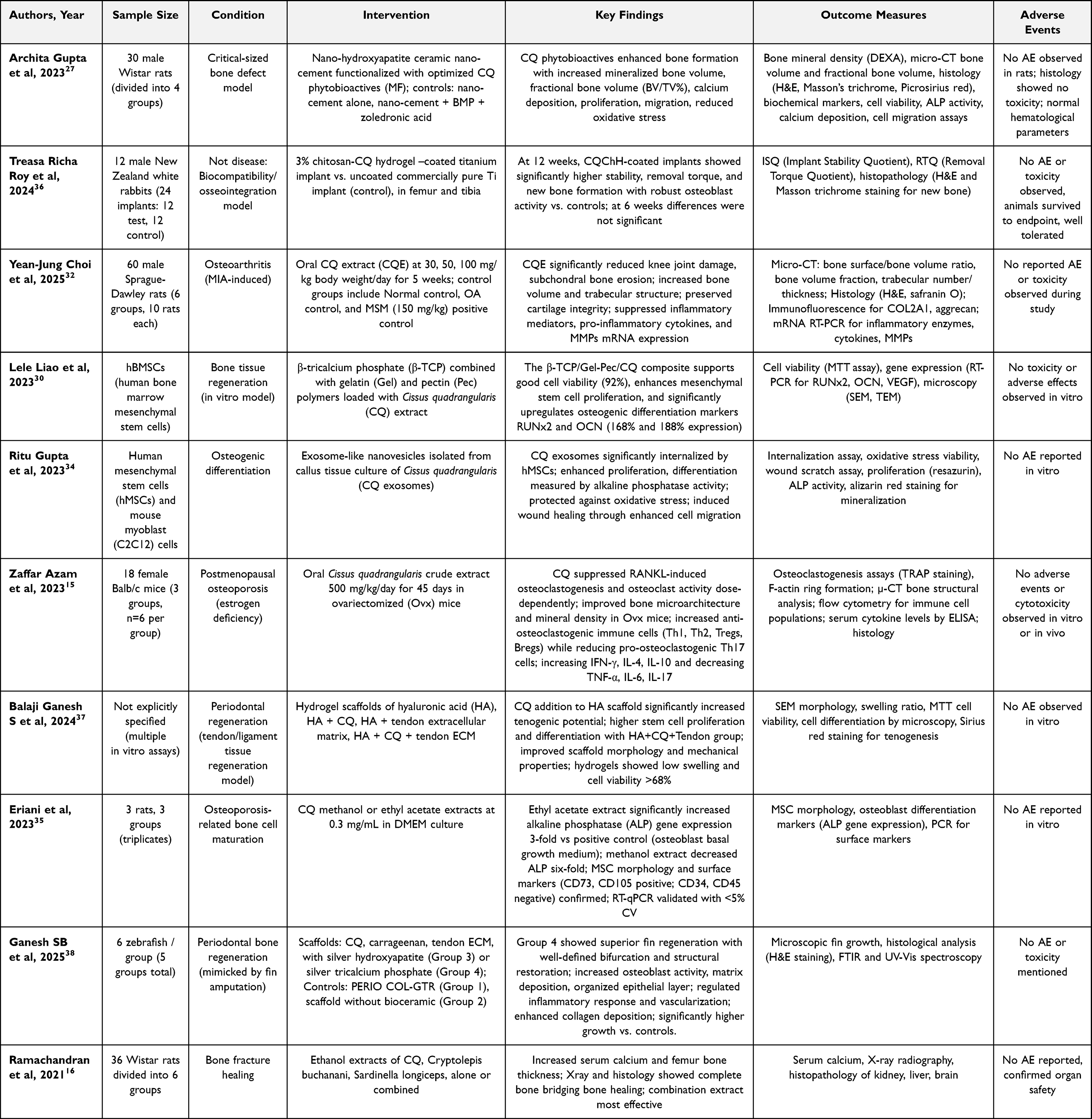 |
Table 2 Main Findings from Preclinical Studies Assessing Cissus Quadrangularis Potential |
Advanced and Innovative Delivery Systems
The therapeutic potential of CQ in managing bone loss is fundamentally constrained by low aqueous solubility of several phytoconstituents, which limits dissolution in gastrointestinal fluids and reduces the fraction available for absorption. In addition, first‑pass intestinal and hepatic metabolism can further reduce systemic exposure, leading to inconsistent plasma levels and therapeutic responses.39,40 The administration begins with ingestion, where CQ preparations are exposed to gastric pH, enzymes and mechanical mixing. Many plant secondary metabolites are unstable or undergo degradation or transformation in gastric juice, and co‑ingested food can modify gastric emptying and complex with phytochemicals, thereby influencing subsequent bioavailability.41 Absorption becomes critical once CQ constituents reach the small intestine, which is the main site for uptake of most orally administered drugs and phytochemicals. The intestinal epithelium constitutes a selective barrier; limited passive diffusion, active efflux and variable permeability for different CQ components can substantially restrict the amount entering the portal circulation.42 After crossing the intestinal barrier and entering the systemic circulation, CQ constituents undergo distribution to tissues, which represents the distribution phase. Plasma protein binding, tissue affinity for bone, and competition with concomitant drugs or nutrients for transporters and binding sites can all modulate effective concentrations at skeletal targets and thereby the anti‑osteoporotic potential of CQ.43
Achieving enhanced bioavailability of CQ’s active constituents is thus essential to guarantee adequate outcomes. Addressing this pharmacological challenge, advanced delivery approaches, such as the Self-Emulsifying Drug Delivery System (CQ-SEDDS), have been successfully developed to facilitate absorption by forming nano-emulsions upon dispersion in the gastrointestinal tract.44 Preclinical testing of this system in an osteoporotic rat model demonstrated that CQ-SEDDS resulted in approximately 76% enhancement in the bioavailability of active CQ markers, effectively reducing variability. This improved kinetic profile directly translated to enhanced therapeutic efficacy in ovariectomized rats, yielding greater BMD gains compared to crude extracts. Moreover, innovative localized delivery systems, such as CQ-loaded polyhedral oligomeric silsesquioxane-reinforced chitosan-based bilayer sponges, are being designed for tissue engineering applications.22 These bilayer systems, designed to mimic skin tissue structure, successfully encapsulated CQ extract and provided a controlled release profile of up to 78%−80% cumulative release over 4 days, demonstrating antibacterial activity and inducing cell proliferation and collagen deposition in vitro. Therefore, modifying the delivery system from traditional crude forms, which carry associated risks of high dosage and limited efficacy, to novel carriers, whether for systemic absorption or sustained local delivery, is critical for unlocking CQ’s full multi-target synergistic osteoprotective potential for clinical application.
Available Clinical Evidence
Clinical evidence supporting the use of CQ in managing bone loss pathologies is still in development. Available data primarily validates CQ traditional application in acute trauma, while emerging data investigates its potential in chronic conditions. Systematic reviews of randomized controlled trials (RCTs) focusing on bone fractures have demonstrated that CQ provides a measurable benefit, specifically by significantly reducing bone pain scores compared to placebo.45 An open-label RCT evaluating a combination product including CQ in patients with maxillofacial fractures reported a promising osteoanabolic effect characterized by early pain relief, supporting the acceleration of healing and restoration of functional outcomes.46 This capacity to accelerate repair is further supported by observations that CQ treatment improves new bone formation in patients undergoing dental implant placement in atrophic ridges.47 The pilot RCT by Brahmkshatriya et al evaluated the osteogenic efficacy of CQ in patients with maxillofacial fractures, comprising 9 subjects (8 male, 1 female, aged 20–63) who underwent open reduction and internal fixation.48 Over 45 days, those receiving CQ capsules (500 mg thrice a day for 6 weeks) showed greater reductions in pain, swelling, and fragment mobility, with accelerated bone healing as evidenced by earlier periosteal reaction and callus formation on CT scans at day 21 and complete bone deposition by day 45, compared to controls receiving standard care alone. Additionally, CQ recipients had significantly increased serum calcium and phosphorus levels, and the supplement was well tolerated with no reported side effects. Mohammad et al too examined the comparative effectiveness of Ocimum sanctum, CQ, and placebo for mandibular fracture healing in 29 patients.49 Patients treated with CQ (3.5 g of 80% alcoholic extract powder thrice a day) demonstrated significantly improved fracture healing evidenced by shortened immobilization time, increased serum calcium, and enhanced alkaline phosphatase levels, reflecting active bone formation. Additionally, the CQ group showed the greatest increase in bite force, good radiographic healing, and favorable hematinic and hypoglycemic effects, all without reported adverse events. Singh et al evaluated the osteogenic activity of CQ in 60 patients with mandibular fractures (age 20–35), allocated to receive either CQ capsules or placebo.50 Patients in the CQ group (300 mg per capsule, 2 capsules BID) demonstrated superior clinical and radiological fracture healing, with marked reductions in pain, swelling, and mobility at fracture sites and greater increases in bite force relative to controls. Biochemical analyses revealed significantly elevated serum calcium and alkaline phosphatase levels in the CQ group, alongside sustained and significant osteopontin expression, particularly within CD4+ T cell populations, at all sampled time points (0, 4, 6 weeks), correlating with early callus formation, neovascularization, and enhanced bone remodeling. No adverse effects were reported, supporting both efficacy and safety of CQ as an adjunct in osteogenic therapy for fractures.
Beyond acute repair, clinical investigations have explored CQ in chronic degenerative conditions such as bone loss in postmenopausal women. A study administering oral CQ for 24 weeks to postmenopausal women with osteopenia revealed a significant delaying effect on bone loss, indicated by a measurable reduction in bone turnover markers, suggesting a slower overall bone remodeling rate. Crucially, however, this short-term intervention did not result in a significant change in BMD at any measured site compared to the placebo group.51 A similar, pivotal, RCT involving 108 postmenopausal women with osteopenia assessed CQ at oral doses of 1.2 and 1.6 g/day for 24 weeks, focusing on BMD and bone turnover markers as primary endpoints.52 Although BMD changes at the lumbar spine, femoral neck, and total hip sites did not significantly differ from placebo over the 24-week period, CQ supplementation notably stabilized the bone remodeling process, as shown by stable serum C-telopeptide of type 1 collagen and a significant reduction in procollagen type 1 amino-terminal propeptide compared to the continuous increase seen with placebo. These effects, while moderate, were achieved without an increased incidence of adverse events, indicating a favorable safety profile in the studied population.
Despite these positive indications in acute fracture repair and encouraging early results in bone loss and related musculoskeletal diseases, there is still a critical need for comprehensive, high-quality, long-term RCTs to conclusively validate CQ’s efficacy and establish optimal dosing for the chronic management of OP. Table 3 summarizes main findings from clinical studies assessing CQ potential.
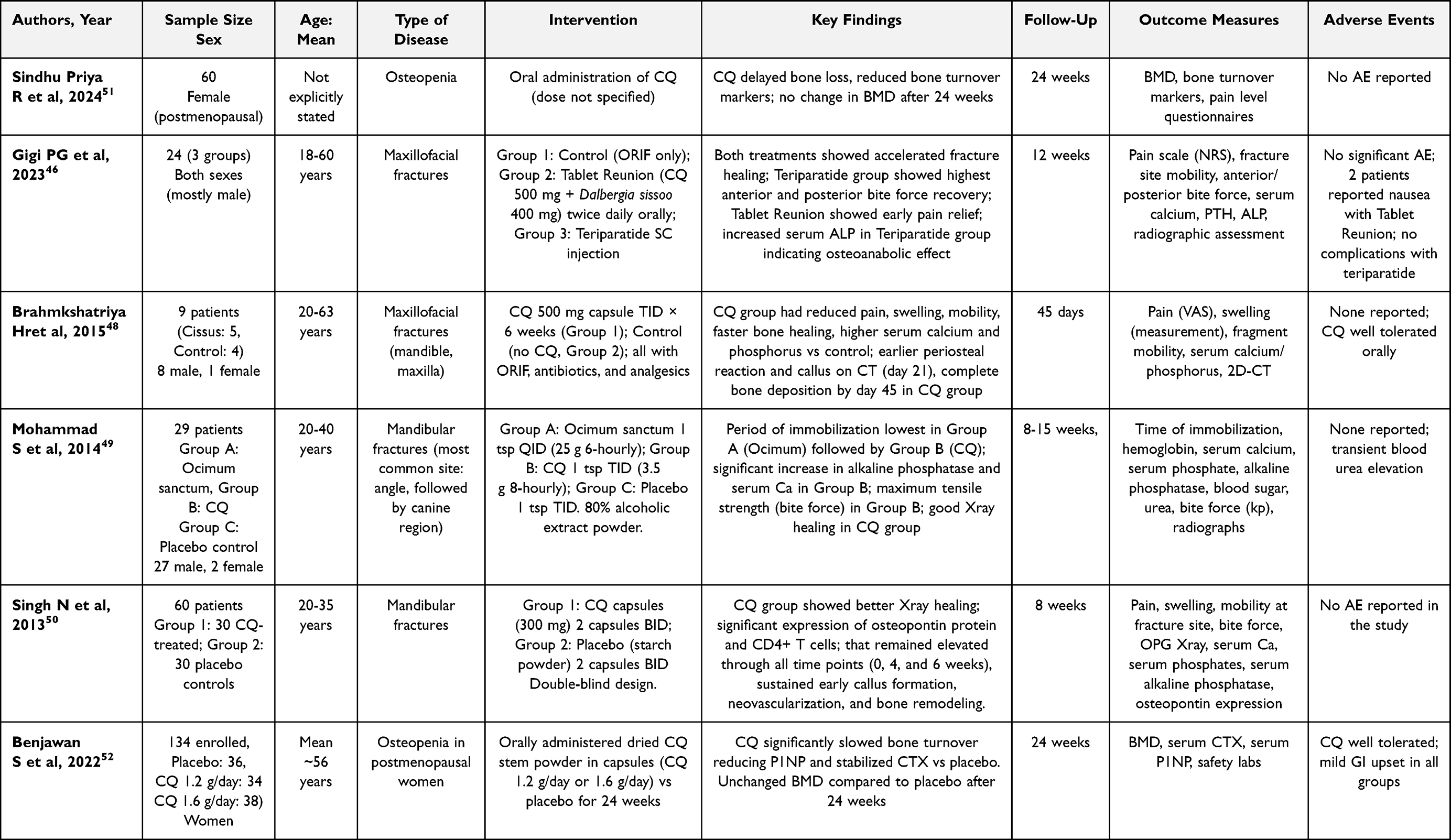 |
Table 3 Main Findings from Clinical Studies Assessing Cissus Quadrangularis Potential |
Clinical Implications and Limitations
The clinical implication of CQ as an anti-osteoporotic agent is rapidly transitioning from traditional medicine to evidence-based acceptance, driven by its unique pharmacological profile. The core therapeutic advantage of CQ lies in its dual mechanism of action, distinguishing it from many conventional monopathway pharmaceutical interventions, as it effectively acts both by stimulating osteoblasts (enhancing osteogenesis) and inhibiting osteoclasts (reducing resorption).13,33,36 The potential for CQ to be included in integrative OP management, especially as a potential alternative in selected conditions or in low-resource settings, is affirmed by emerging clinical data, such as the discussed recent RCTs demonstrating a delaying effect on bone loss in postmenopausal women, evidenced by a reduction in bone turnover markers.51,52 This application is highly favorable given that CQ is consistently demonstrated to be safe and devoid of major toxicity in preclinical models, presenting fewer associated risks compared to synthetic agents.53 Crucially, the historical challenge of poor oral bioavailability of CQ’s active constituents is now showing potential to be mitigated by modern pharmaceutical technology.22,44 Advanced delivery modalities like the SEDDS may help in overcoming this bioavailability barrier, showing a substantial 76% enhancement in the bioavailability of active markers in preclinical studies, a pharmacokinetic leap that promises superior clinical efficacy by ensuring adequate systemic exposure. However, the existing clinical evidence presents limitations, notably small clinical sample sizes and short follow-up durations (typically ≤6 months), coupled with a pervasive lack of standardized extraction protocols that hinders replicability.45,51 Furthermore, there remains a critical absence of head-to-head trials comparing CQ against established standard OP drugs.
Consequently, defining the exact colocation of CQ in the OP general picture across multiple clinical scenarios necessitates future research, specifically demanding large-scale, multi-center RCTs using standardized, bioavailable CQ formulations, alongside long-term safety and efficacy studies and specialized combination therapy studies with conventional anti-osteoporotic agents. However, some hypotheses related to the current CQ picture can be made. Considering CQ capacity to accelerate bone injury repair by directly affecting callus formation and contributing to accelerated mineralization due to its calcium content and given its dual action (i.e., stimulating osteogenesis and inhibiting osteoclastogenesis) and its safety profile, CQ appears as an option for patients unwilling or unable to take bisphosphonates or other therapies, which often carry side effects such as osteonecrosis of the jaw or hypercalcemia.54,55 Furthermore, CQ is a potential therapeutic agent for patients with osteopenia or for individuals (such as men under 50 or premenopausal women) with risk factors that do not meet the indications for bisphosphonates.56 CQ can also be used in more complex settings: for patients who, despite being treated with antiresorptives (such as bisphosphonates), show worsening densitometry without fractures, CQ could be used as an adjunct. These indications also make it an attractive alternative for patients who must suspend antiresorptive therapy for dental treatments (a period known as a “drug holiday”), providing osteoprotective support without the risks associated with conventional medications.57
Table 4 summarizes CQ potential clinical indications.
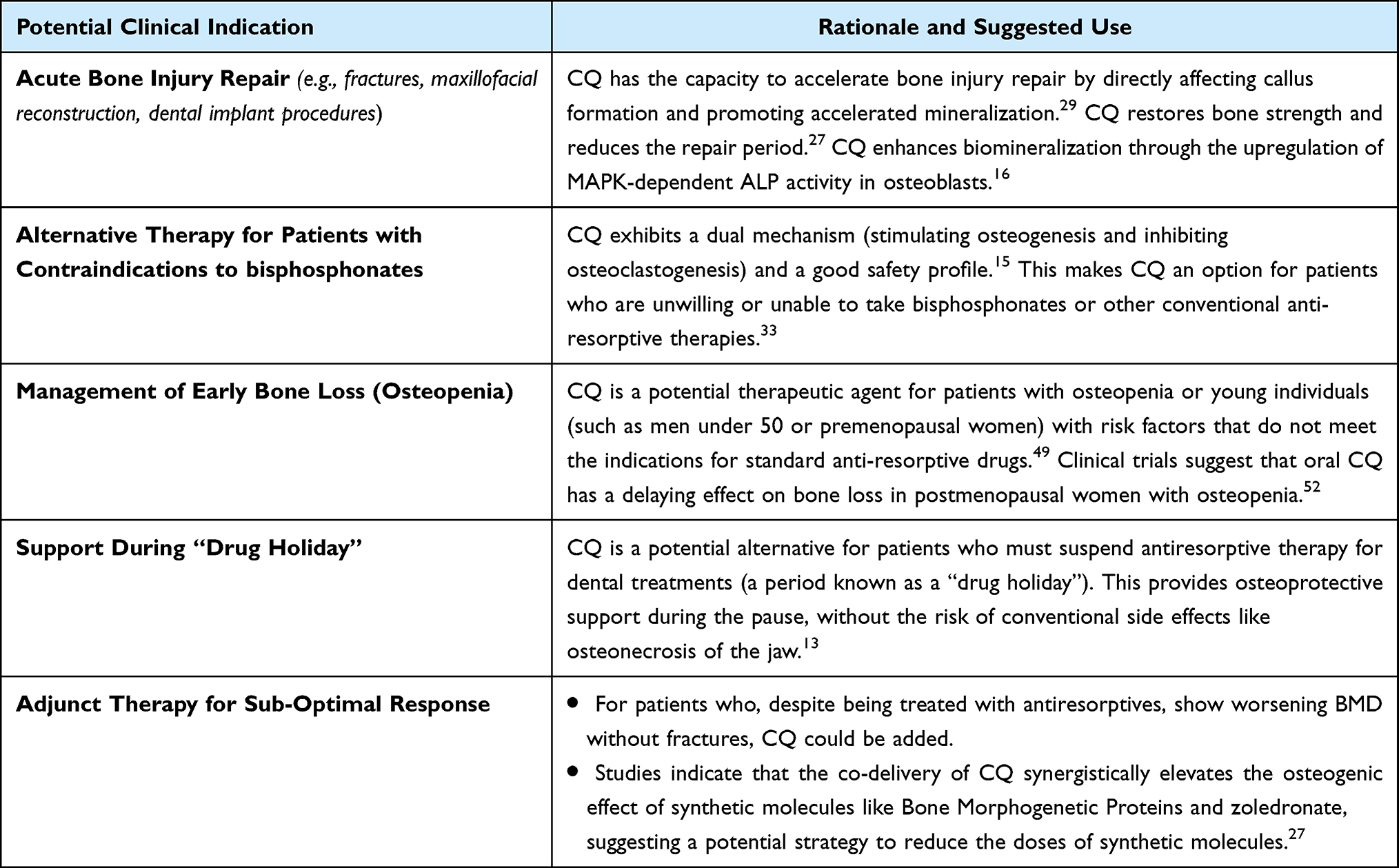 |
Table 4 Cissus Quadrangularis Potential Clinical Indications |
However, a clinical dosing or timing guideline has not yet been standardized, and therapy should be personalized according to the single patient condition. Based on current clinical evidence, clinical administration has varied significantly, depending on the study’s focus and the formulation utilized.45 For the purpose of accelerating bone fracture healing, CQ has been clinically administered at a high range, with systematic reviews noting clinical use ranging from 1.2 to 10 g/day for 4–12 weeks.45,58 Specific pilot studies administered one capsule of CQ (500 mg) thrice a day for 6 weeks (total 1500 mg/day).48 For chronic bone loss conditions, such as osteopenia in postmenopausal women, CQ was administered orally for 24 weeks, a period which, at the time of publication, represented the longest continuous oral CQ administration reported to date.52 Doses evaluated in this trial were 1.2 g/day and 1.6 g/day, with the 1.6 g/day dose showing a promising effect in delaying bone loss by significantly reducing bone turnover markers. This lack of standardization in both dosage and administration time represents an actual limitation. Moreover, studies frequently employ different dosage forms and extraction procedures, which makes direct comparison of clinical effects challenging. Lastly, the majority of current clinical trials are of short duration, often lasting six months or less, and limited data exist on the long-term safety required for the chronic management of osteoporosis. Therefore, future research must focus on conducting large-scale, long-term randomized controlled trials (RCTs) to conclusively validate the efficacy, establish the optimal dose, and define the appropriate duration of therapy for CQ.
An additional topic that deserves discussion is CQ economic accessibility. Conventional pharmacological agents approved for OP management carry substantial direct costs, with annual per-patient expenditures ranging from approximately US$458-$1,874 for oral bisphosphonates to US$1,838 for denosumab and up to US$22,156 for teriparatide, placing a considerable financial burden on both patients and healthcare systems. In contrast, CQ is currently marketed in most jurisdictions as a dietary supplement or herbal/nutraceutical product rather than a licensed pharmaceutical drug, and is therefore available without prescription at substantially lower cost, with commercially available standardized extracts retailing at approximately US$13–$40 per month for clinically evaluated dose ranges.59,60 However, CQ is typically not reimbursed by public or private insurance systems, and the wide variability in extraction protocols and phytochemical standardization across commercial preparations introduces significant uncertainty regarding therapeutic equivalence with formulations used in clinical trials. Until high-bioavailability, standardized CQ formulations receive formal regulatory approval and undergo health technology assessment, any cost-effectiveness conclusion remains premature.
Conclusion
The comprehensive data accumulated across centuries of traditional use and modern investigation strongly establishes the promising osteoprotective potential of CQ. Its distinction from conventional pharmaceuticals lies in its dual mechanism of action (i.e., simultaneously promoting osteogenesis by stimulating osteoblasts and inhibiting bone resorption by suppressing osteoclasts). Robust preclinical studies consistently confirm this activity, demonstrating enhanced callus formation, improvements in bone microarchitecture and BMD, and the suppression of inflammatory bone loss in estrogen-deficient models. Emerging human evidence supports its clinical relevance, particularly its measurable benefit in reducing bone pain scores associated with fractures and its role in delaying bone loss among postmenopausal women with osteopenia.
This therapeutic relevance is significantly amplified by continuous advancements in delivery technology, with pharmacokinetic improvements that translate to enhanced efficacy.
Given its safety profile and multi-target action, CQ is positioned not as a replacement for established pharmacotherapy but as a valuable adjunct in comprehensive OP management. This role is particularly relevant for managing early bone loss (osteopenia) or serving as osteoprotective support during patient-specific scenarios, such as when antiresorptive therapies must be suspended for dental treatments (“drug holiday”). However, the current evidence is insufficient to recommend CQ as monotherapy for established OP due to many limitations, including small sample sizes and short follow-up durations (≤6 months), coupled with a persistent lack of standardized extraction protocols. Therefore, a definitive clinical conclusion requires larger-scale, multi-center RCTs utilizing standardized, high-bioavailability CQ formulations, along with long-term safety assessments and studies exploring its synergistic potential in combination therapy with established anti-osteoporotic agents.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ibrahim MO, Kolleri A, Ginawi A. The use of bone density scan in monitoring treatment response in patients diagnosed with osteoporosis: a retrospective cohort study. Int J Rheumatol. 2023;2023:1–14. doi:10.1155/2023/2160346
2. Luo C, Qin S-X, Wang Q-Y, et al. Cost-effectiveness analysis of five drugs for treating postmenopausal women in the united states with osteoporosis and a very high fracture risk. J Endocrinol Invest. 2022;46:367–379. doi:10.1007/s40618-022-01910-7
3. Khan AA, AbuAlrob H, Al-alwani H, et al. Post hip fracture orthogeriatric care—a canadian position paper addressing challenges in care and strategies to meet quality indicators. Osteoporos Int. 2023;34:1011–1035. doi:10.1007/s00198-022-06640-3
4. Wang H, Luo Y, Wang H, Li F, Yu F, Ye L. Mechanistic advances in osteoporosis and anti-osteoporosis therapies. MedComm. 2023;4:e244. doi:10.1002/mco2.244
5. Tobias JH. Sclerostin and cardiovascular disease. Curr Osteoporos Rep. 2023;21:519–526. doi:10.1007/s11914-023-00810-w
6. Wu D, Li L, Wen Z, Wang G. Romosozumab in osteoporosis: yesterday, today and tomorrow. J Transl Med. 2023;21:668. doi:10.1186/s12967-023-04563-z
7. Lane J, Langdahl B, Stone M, et al. Romosozumab in patients who experienced an on-study fracture: post hoc analyses of the FRAME and ARCH Phase 3 Trials. Osteoporos Int. 2024;35:1195–1204. doi:10.1007/s00198-024-07049-w
8. McCloskey EV, Johansson H, Harvey NC, Lorentzon M, Shi Y, Kanis JA. Romosozumab efficacy on fracture outcomes is greater in patients at high baseline fracture risk: a post hoc analysis of the first year of the frame study. Osteoporos Int. 2021;32:1601–1608. doi:10.1007/s00198-020-05815-0
9. Yoo Y-S, Kim M-G, Park H-J, et al. Additional effects of herbal medicine combined with bisphosphonates for primary osteoporosis: a systematic review and meta-analysis. Front Pharmacol. 2024;15:1413515. doi:10.3389/fphar.2024.1413515
10. Mak JCS, Faux S. Complementary and alternative medicine use by osteoporotic patients in Australia (CAMEO-A): a Prospective Study. J Altern Complement Med. 2010;16:579–584. doi:10.1089/acm.2009.0425
11. Aware CB, Patil DN, Suryawanshi SS, et al. Natural bioactive products as promising therapeutics: a review of natural product-based drug development. South Afr J Bot. 2022;151:512–528. doi:10.1016/j.sajb.2022.05.028
12. Mathangi R, Devarajan N, Lakshmi UD. An overview of the osteogenic potential of indian herb Cissus quadrangularis (veldt grape). South East Eur J Public Health. 2024;2210–2214. doi:10.70135/seejph.vi.2354
13. Nath R, Kar BK, Dhadiwal RK, Daftary GV, Khemnar BM, Patil NN. Role of Cissus quadrangularis in bone loss pathologies. Int J Orthop Sci. 2024;10:196–201. doi:10.22271/ortho.2024.v10.i1c.3521
14. Ruangsuriya J, Charumanee S, Jiranusornkul S, et al. Depletion of β-sitosterol and enrichment of quercetin and rutin in Cissus quadrangularis linn fraction enhanced osteogenic but reduced osteoclastogenic marker expression. BMC Complement Med Ther. 2020;20:105. doi:10.1186/s12906-020-02892-w
15. Azam Z, Sapra L, Baghel K, et al. Cissus quadrangularis (hadjod) inhibits rankl-induced osteoclastogenesis and augments bone health in an estrogen-deficient preclinical model of osteoporosis via modulating the host osteoimmune system. Cells. 2023;12(2):216. doi:10.3390/cells12020216
16. Ramachandran S, Fadhil L, Gopi C, Amala M, Dhanaraju MD. Evaluation of bone healing activity of Cissus quadrangularis (linn), cryptolepis buchanani, and sardinella longiceps in wistar rats. Beni-Suef Univ J Basic Appl Sci. 2021;10:30. doi:10.1186/s43088-021-00120-z
17. Zhang B, Zhao L, Sun Y. Machine learning and molecular dynamics reveal anti-osteoporosis potential of dietary flavonoids. Medicine. 2025;104:e44958. doi:10.1097/MD.0000000000044958
18. Ramesh P, Jagadeesan R, Sekaran S, Dhanasekaran A, Vimalraj S. Flavonoids: classification, function, and molecular mechanisms involved in bone remodelling. Front Endocrinol. 2021;12:779638. doi:10.3389/fendo.2021.779638
19. Sharma AR, Lee Y-H, Bat-Ulzii A, et al. Molecular mechanism, and targeted delivery of flavonoids for bone loss. Nutrients. 2023;15:919. doi:10.3390/nu15040919
20. Na Takuathung M, Aisara J, Sawong S, Koonrungsesomboon N. The effects of Cissus quadrangularis on bone-related biomarkers in humans: a systematic review and meta-analysis. BMC Complement Med Ther. 2025;25:286. doi:10.1186/s12906-025-04995-8
21. Potphode VR, Deshmukh AS, Mahajan VR. Self-micro emulsifying drug delivery system: an approach for enhancement of bioavailability of poorly water soluble drugs. Asian J Pharm Technol. 2016;6:159. doi:10.5958/2231-5713.2016.00023.4
22. Aker SD, Tamburaci S, Tihminlioglu F. Development of Cissus quadrangularis -loaded poss-reinforced chitosan-based bilayer sponges for wound healing applications: drug release and in vitro bioactivity. ACS Omega. 2023;8:19674–19691. doi:10.1021/acsomega.3c00999
23. Płóciniczak A, Bukowska-Olech E, Wysocka E. The complexity of oxidative stress in human age-related diseases-a review. Metabolites. 2025;15:479. doi:10.3390/metabo15070479
24. Sundaran J, Begum R, Vasanthi M, Kamalapathy M, Bupesh G, Sahoo U. A short review on pharmacological activity of Cissus quadrangularis. Bioinformation. 2020;16:579–585. doi:10.6026/97320630016579
25. Messeha SS, Fidudusola FF, Gendy S, Latinwo LM, Odewumi CO, Soliman KFA. Nrf2 activation as a therapeutic target for flavonoids in aging-related osteoporosis. Nutrients. 2025;17:267. doi:10.3390/nu17020267
26. Boesch-Saadatmandi C, Loboda A, Wagner AE, et al. Effect of quercetin and its metabolites isorhamnetin and quercetin-3-glucuronide on inflammatory gene expression: role of miR-155. J Nutr Biochem. 2011;22:293–299. doi:10.1016/j.jnutbio.2010.02.008
27. Gupta A, Kumar Mehta S, Qayoom I, Gupta S, Singh S, Kumar A. Biofunctionalization with Cissus quadrangularis phytobioactives accentuates nano-hydroxyapatite based ceramic nano-cement for neo-bone formation in critical sized bone defect. Int J Pharm. 2023;642:123110. doi:10.1016/j.ijpharm.2023.123110
28. Farjana HN, Valiathan GM, Mohanasatheesh S. In-silico study on biomolecules derived from Cissus quadrangularis towards anti-inflammation. J Genet Eng Biotechnol. 2025;23:100571. doi:10.1016/j.jgeb.2025.100571
29. Vinoth K, Kumar SR. Morphological, molecular, and pharmacological review of veldt grape (Cissus quadrangularis l.): an underutilized medicinal plant. Front Plant Sci. 2025;16:1586624. doi:10.3389/fpls.2025.1586624
30. Liao L, Zhu W, Tao C, Li D, Mao M. Cissus quadrangularis l extract-loaded tricalcium phosphate reinforced natural polymer composite for guided bone regeneration. J Mater Sci Mater Med. 2023;34:33. doi:10.1007/s10856-023-06739-x
31. Szwed-Georgiou A, Płociński P, Kupikowska-Stobba B, et al. Bioactive materials for bone regeneration: biomolecules and delivery systems. ACS Biomater Sci Eng. 2023;9:5222–5254. doi:10.1021/acsbiomaterials.3c00609
32. Choi Y-J, Jung JI, Bae J, Lee JK, Kim EJ. Evaluation of the anti-osteoarthritic effects and mechanisms of Cissus quadrangularis extract containing quercetin and isorhamnetin in a rat model of monosodium iodoacetate-induced osteoarthritis. Food Nutr Res. 2025;69. doi:10.29219/fnr.v69.12173.
33. Kaur J, Sharma G, Mahajan A, Katare OP, Bhadada SK, Ghoshal G. Role of Cissus quadrangularis in the management of osteoporosis: an overview. Crit Rev Ther Drug Carr Syst. 2021;38:27–51. doi:10.1615/CritRevTherDrugCarrierSyst.2021033808
34. Gupta R, Gupta S, Gupta P, Nüssler AK, Kumar A. Establishing the callus-based isolation of extracellular vesicles from Cissus quadrangularis and elucidating their role in osteogenic differentiation. J Funct Biomater. 2023;14:540. doi:10.3390/jfb14110540
35. Eriani K, Desriani D, Putri VC, et al. The effect of Cissus quadrangularis salisb. extract on maturation of rat mesenchymal stem cells. Braz J Biol. 2023;83:e270335. doi:10.1590/1519-6984.270335
36. Roy TR, Nelogi S, Chowdhary R, Naik VV, Peter M, Santhosh VN. Influence of chitosan and cissus quandrangularis coating on osseointegration in titanium implants in rabbits: a preclinical in vivo study. J Stomatol Oral Maxillofac Surg. 2024;125:101727. doi:10.1016/j.jormas.2023.101727
37. Ganesh S, Sabu B, Kaarthikeyan A, Eswaramoorthy G. Development of a Cissus quadrangularis-doped extracellular matrix and a hyaluronic acid-incorporated scaffold for periodontal regeneration: an in vitro study. Cureus. 2024. doi:10.7759/cureus.56507
38. Balaji Ganesh S, Anees FF, Kaarthikeyan G, Martin TM, Kumar MSK, Sheefaa MI. Zebrafish caudal fin model to investigate the role of Cissus quadrangularis, bioceramics, and tendon extracellular matrix scaffolds in bone regeneration. J oral Biol craniofacial Res. 2025;15:809–815. doi:10.1016/j.jobcr.2025.05.009
39. Koppula S, Shaik B, Maddi S. Phytosomes as a new frontier and emerging nanotechnology platform for phytopharmaceuticals: therapeutic and clinical applications. Phytother Res. 2025;39:2217–2249. doi:10.1002/ptr.8465
40. Alagga AA, Pellegrini MV, Gupta V. Drug Absorption. Treasure Island (FL): StatPearls Publishing; 2025.
41. Sun S, Wang Y, Wu A, Ding Z, Liu X. Influence factors of the pharmacokinetics of herbal resourced compounds in clinical practice. Evid-Based Compl Altern Med ECAM. 2019;2019:1983780. doi:10.1155/2019/1983780
42. Azman M, Sabri AH, Anjani QK, Mustaffa MF, Hamid KA. Intestinal absorption study: challenges and absorption enhancement strategies in improving oral drug delivery. Pharm Basel Switz. 2022;15:975. doi:10.3390/ph15080975
43. Sai Parinam PS, Hedaoo RP, Patil M, Mohile A, Khatwani N, Aainapure A. Therapeutic potential of Cissus quadrangularis linn. (veld grape) in osteoporosis and arthritis: a scoping review of preclinical evidence. J Appl Pharm Sci. 2025. doi:10.7324/JAPS.2025.247119
44. Garg J, Ghoshal G, Sharma G, Katare OP, Bhadada S. Self emulsifying delivery system of Cissus quadrangularis: evidence of enhanced efficacy and promising pharmacokinetic profile in the management of osteoporosis. AAPS Pharm Sci Tech. 2024;25(5):107. doi:10.1208/s12249-024-02821-x
45. Sawangjit R, Puttarak P, Saokaew S, Chaiyakunapruk N. Efficacy and safety of Cissus quadrangularis l. in clinical use: a systematic review and meta-analysis of randomized controlled trials: efficacy and safety of cissus in clinical use. Phytother Res. 2017;31:555–567. doi:10.1002/ptr.5783
46. Pg G, Chugh A, Chaudhry K, et al. Comparison of teriparatide and combination of Cissus quadrangularis and Dalbergia sissoo on bone healing against the control group in maxillofacial fractures: a randomized open-label control trial. Craniomaxillofacial Trauma Reconstr. 2023;16:23–33. doi:10.1177/19433875211067007
47. Altaweel AA, Baiomy AABA, Shoshan HS, et al. Evaluation of osteogenic potential of Cissus quadrangularis on mandibular alveolar ridge distraction. BMC Oral Health. 2021;21:491. doi:10.1186/s12903-021-01847-y
48. Brahmkshatriya H, Shah K, Ananthkumar G, Brahmkshatriya M. Clinical evaluation of Cissus quadrangularis as osteogenic agent in maxillofacial fracture: a pilot study. AYU Int Q J Res Ayurveda. 2015;36:169. doi:10.4103/0974-8520.175542
49. Mohammad S, Pal U, Pradhan R, Singh N. Herbal remedies for mandibular fracture healing. Natl J Maxillofac Surg. 2014;5:35. doi:10.4103/0975-5950.140167
50. Singh N, Singh V, Singh R, et al. Osteogenic potential of cissus qudrangularis assessed with osteopontin expression. Natl J Maxillofac Surg. 2013;4(52). doi:10.4103/0975-5950.117884
51. Priya RS, Swathi R, Selvi ST, et al. The study to assess the effectiveness of Cissus quadrangularis among postmenopausal women with osteopenia. J Pharm Bioallied Sci. 2024;16:S2889–S2891. doi:10.4103/jpbs.jpbs_574_24
52. Benjawan S, Nimitphong H, Tragulpiankit P, Musigavong O, Prathanturarug S, Pathomwichaiwat T. The effect of Cissus quadrangularis l. on delaying bone loss in postmenopausal women with osteopenia: a randomized placebo-controlled trial. Phytomedicine. 2022;101:154115. doi:10.1016/j.phymed.2022.154115
53. Bafna PS, Patil PH, Maru SK, Mutha RE. Cissus quadrangularis l: a comprehensive multidisciplinary review. J Ethnopharmacol. 2021;279:114355. doi:10.1016/j.jep.2021.114355
54. Gupta M, Gupta N. Bisphosphonate-Related Jaw Osteonecrosis. Treasure Island (FL): StatPearls Publishing; 2025.
55. Van Den Wyngaert T, Huizing MT, Vermorken JB. Bisphosphonates and osteonecrosis of the jaw: cause and effect or a post hoc fallacy? Ann Oncol. 2006;17:1197–1204. doi:10.1093/annonc/mdl294
56. LeBoff MS, Greenspan SL, Insogna KL, et al. The clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int. 2022;33:2049–2102. doi:10.1007/s00198-021-05900-y
57. Adami G, Saag KG. Expert perspective: how, when, and why to potentially stop antiresorptive drugs in osteoporosis. Arthritis Rheumatol. 2025;77:1294–1304. doi:10.1002/art.43179
58. Stohs SJ, Ray SD. A review and evaluation of the efficacy and safety of Cissus quadrangularis extracts. Phytother Res. 2013;27:1107–1114. doi:10.1002/ptr.4846
59. Li N, Cornelissen D, Silverman S, et al. An updated systematic review of cost-effectiveness analyses of drugs for osteoporosis. PharmacoEconomics. 2021;39:181–209. doi:10.1007/s40273-020-00965-9
60. Leung P-C, Siu W-S. Herbal treatment for osteoporosis: a current review. J Tradit Complement Med. 2013;3:82–87. doi:10.4103/2225-4110.110407
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Hemoglobin Levels and Osteoporosis in Chinese Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Ye T, Lu L, Guo L, Liang M
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2803-2811
Published Date: 14 September 2022
Associations of Obesity Indices with Bone Mineral Densities and Risk of Osteoporosis Stratified Across Diabetic Vascular Disease in T2DM Patients
Zheng S, Zhou J, Wang K, Wang X, Li Z, Chen N
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3459-3468
Published Date: 3 November 2022
Clinical Utility of Romosozumab in the Management of Osteoporosis: Focus on Patient Selection and Perspectives
Lim SY, Bolster MB
International Journal of Women's Health 2022, 14:1733-1747
Published Date: 15 December 2022
The Effects of Switching from Dipeptidyl Peptidase-4 Inhibitors to Glucagon-Like Peptide-1 Receptor Agonists on Bone Mineral Density in Diabetic Patients
Huang CF, Mao TY, Hwang SJ
Diabetes, Metabolic Syndrome and Obesity 2023, 16:31-36
Published Date: 11 January 2023
The Relationship Between Serum 25-Hydroxyvitamin D Levels and Osteoporosis in Postmenopausal Women
Wang D, Yang Y
Clinical Interventions in Aging 2023, 18:619-627
Published Date: 18 April 2023