Back to Journals » Patient Preference and Adherence » Volume 20
Exploring Information Needs and Perspectives on a Patient Decision Aid for Biologic Therapy: A Qualitative Interview Study Among Individuals with Rheumatoid Arthritis
Authors Rai SK, McCormick N ![]() , Yokose C, De Vera MA
, Yokose C, De Vera MA ![]() , Li LC
, Li LC ![]() , Choi HK
, Choi HK
Received 4 October 2025
Accepted for publication 16 December 2025
Published 23 June 2026 Volume 2026:20 565490
DOI https://doi.org/10.2147/PPA.S565490
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Sharan K Rai,1– 3 Natalie McCormick,1– 4 Chio Yokose,1– 3 Mary A De Vera,4,5 Linda C Li,4,6 Hyon K Choi1– 4
1Division of Rheumatology, Allergy, and Immunology, Massachusetts General Hospital, Boston, MA,USA; 2Department of Medicine, Harvard Medical School, Boston, MA, USA; 3The Mongan Institute, Department of Medicine, Massachusetts General Hospital, Boston, MA, USA; 4Arthritis Research Canada, Vancouver, BC, Canada; 5Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC, Canada; 6Department of Physical Therapy, University of British Columbia, Vancouver, BC, Canada
Correspondence: Sharan K Rai, Division of Rheumatology, Allergy, and Immunology, Massachusetts General Hospital and Harvard Medical School, 55 Fruit Street, Bulfinch 165, Boston, MA, 02114, USA, Email [email protected] Hyon K Choi, Harvard Medical School, Division of Rheumatology, Allergy, and Immunology, Massachusetts General Hospital and Harvard Medical School, 55 Fruit Street, Bulfinch 165, Boston, MA, 02114, USA, Email [email protected]
Purpose: Significant advances in therapeutic and management options have been made for rheumatoid arthritis (RA), including the development of biologics. However, some patients have expressed hesitancy with respect to their use. We aimed to (1) investigate RA patient perspectives on a biologic patient decision aid; and (2) explore how this decision aid addressed their broader information needs in a US healthcare context.
Patients and Methods: We conducted in-depth telephone interviews with RA patients who were considering either initiating a biologic for the first time or switching to another biologic. Participants were recruited from across the US by a research coordinator based at Massachusetts General Hospital. Participants were first invited to access an existing decision aid developed to support individuals with RA who are considering a biologic. We conducted an iterative content analysis guided by the grounded theory approach.
Results: We interviewed 14 patients with RA, among whom five were biologic-naive. We identified four major themes: 1) treatment-related information seeking behavior (including connecting with others with a chronic disease); 2) helpful aspects of the decision aid (including access to patient stories); 3) decision aid limitations and potential solutions (including content preferences and accessibility); and 4) impacts on the decision to initiate a biologic (including empowerment to engage in shared decision-making).
Conclusion: These four themes highlight key factors to consider for the design/refinement and implementation of patient decision aids in the US (including key information needs and the utility of patient stories) to appropriately meet the needs of patients who are considering a biologic.
Keywords: rheumatoid arthritis, DMARDs, biologic therapy, qualitative research, patient education, decision aid
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory rheumatic disease that is characterized by progressive articular damage and extra-articular manifestations.1 RA is associated with an increased comorbidity burden, high rate of health resource utilization, and corresponding high cost of illness spanning both direct medical costs and indirect costs from lost productivity.2–4 There have been significant advances in therapeutic and management options for RA, including the development of several classes of biologic medications.1 Despite these advances, treatment adherence varies widely, with a meta-analysis estimating a 66% adherence rate across all disease-modifying anti-rheumatic drugs (DMARDs),5 although biologic treatment adherence may be slightly higher compared with that for conventional DMARDs.6,7 Nevertheless, despite the demonstrated clinical benefit of biologic use among those with RA who are indicated for treatment, some patients continue to report feelings of hesitancy with respect to initiating or continuing these medications.8–10 This may be driven by multiple factors, including fear of needles, cost, confusion about treatment options, perception of illness, and, in marginalized communities, awareness of historical injustices in healthcare and health research.8–10 To that end, a shared decision-making approach using a patient decision aid may improve disease management by supporting RA patients through the process of making informed treatment decisions. Patients who have used decision aids are more knowledgeable about their treatment, have more realistic expectations, and feel less conflicted with their decisions compared to those in usual care,11 which may in turn lead to improved medication adherence and outcomes. These findings suggest that a patient decision aid may serve as a useful tool for individuals with RA and their clinicians who are considering the use of a biologic. To assess this further, we recruited patients with RA living in the US who were considering initiating or switching biologics to access an existing web-based decision aid and provide their perspectives on its use as well as discuss their broader information needs through in-depth telephone interviews.
Materials and Methods
Participant Recruitment and Eligibility
Eligible participants were those who met all the following criteria: 1) who received a diagnosis of RA from a rheumatologist; 2) whose rheumatologists have recommended that they consider either starting a biologic or switching to another biologic; 3) who resided in the US; 4) who had Internet (and email) access; and 5) who were comfortable speaking and accessing online content in English. Primary recruitment took place at Massachusetts General Hospital (MGH) and was led by a research coordinator. To supplement our clinic-based recruitment, we employed several web-based strategies. We advertised our study on Research Match, a nonprofit program that is funded by the National Institutes of Health. Web advertisements were deployed in the Arthritis Foundation’s RA-focused newsletter, on Craigslist, and through institutional Twitter accounts. Finally, through word of mouth, additional participants were recruited from internet RA-focused support groups. For individuals recruited outside of MGH clinic settings, the research coordinator conducted a phone screen to confirm they met eligibility criteria. We collected baseline demographic data as well as information on participants’ present self-rated health status and perceived change in health status compared with one year ago. These data were collected and managed using the Research Electronic Data Capture (REDCap) web-based platform.12,13 Participant recruitment continued until thematic saturation was reached.
Online Decision Aid
Enrolled participants were asked to access an independently developed online decision aid that was designed specifically for individuals considering initiating or switching to a new biologic. Originally developed for the Canadian context, this decision aid has been described in detail previously14 and excerpts are provided in Supplementary Figure 1. Prior to study commencement, this existing decision aid was minimally adapted to suit a US healthcare context (namely removing references to Canadian provinces and updating insurance language to reference the combination of public and private payers rather than a single-payer system). The decision aid included information from current systematic reviews and clinical practice guidelines, and spanned all tumor necrosis factor (TNF) inhibitors, an interleukin-6 antagonist, an anti-CD28 drug, an anti-B cell drug, and a JAK inhibitor.14 Participants were asked to access the decision aid at home (estimated completion time ~30 minutes) following a visit with their rheumatologist where they had been recommended to either initiate or switch to a new biologic. Qualitative interviews took place approximately one month after participants accessed the decision aid. Participants in the current study received a $75 honorarium for their efforts.
Qualitative Interviews
Eligible individuals participated in a telephone interview with a facilitator trained in qualitative research to describe their experience with using the decision aid. We developed an interview topic guide, which included open-ended questions about the participants’ feelings about receiving medication information on this digital platform compared with other sources and whether the tool was helpful in making decisions surrounding biologics (Box 1). All interviews were digitally recorded and transcribed verbatim. Transcripts were checked against the recording for accuracy. All participants were assigned a pseudonym.
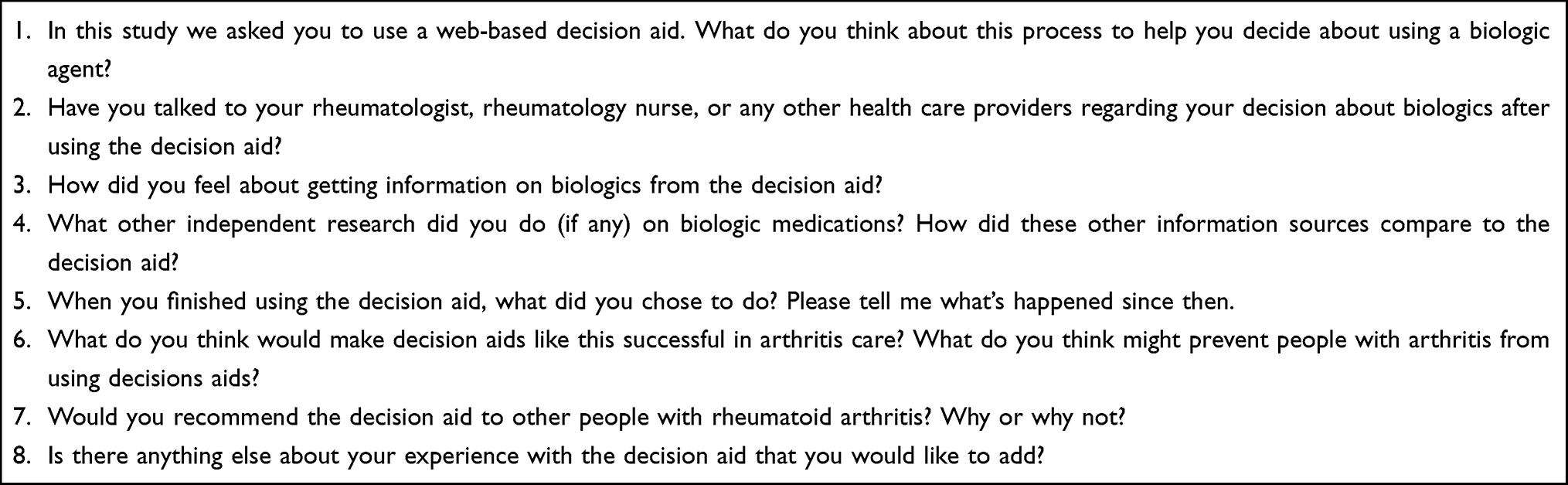 |
Box 1 Topic Guide for Qualitative Interview Facilitation |
Qualitative Data Analysis
We imported all transcripts (verbatim) into QDA Miner Lite® for data analysis. We conducted an iterative content analysis that was guided by the grounded theory approach, wherein theories are “grounded” in the data (ie, they emerge from the data collected as the data guides the research [contrasted with the use of a guiding framework for data exploration]).15 Two authors (SKR and NM) independently read all transcripts and assigned (and revised) categories and subcategories belonging to overarching themes in an iterative coding process. The same two authors subsequently discussed their coding scheme for consensus. In instances where a third opinion was required, a third author (CY) provided input, and discussion continued among all three authors until consensus was achieved.
Engagement of Patient Research Partners
This project was originally refined through discussions with six patient partners living with RA, including representatives from patient groups (ie, the Arthritis Patient Advisory Board and Arthritis Consumer Experts). Patient collaborators participated in discussions with the research team through e-mails, telephone calls, and/or face-to-face meetings, and have offered unique and constructive advice for developing this project. Throughout our work, we employed the “FIRST” model (Facilitate, Identify, Respect, Support, and Train) as a guiding framework for consumer-researcher collaborations.16
Ethics Approval
The current study was approved by the Institutional Review Board of Mass General Brigham (protocol identification number 2015P002116) and was conducted in accordance with the guidelines outlined in the Declaration of Helsinki. All participants provided written informed consent to participate as well as have their anonymized responses included in published scientific reporting prior to study participation.
Results
Participant Characteristics
A total of 14 individuals with RA participated in qualitative interviews; their characteristics are provided in Table 1. Nearly all participants were women (85.7%). Five participants were newly considering a first biologic, while the other nine participants were considering switching to a new biologic. Ten participants had completed a bachelor’s degree or higher. Over half of participants rated their current health status as “fair” with another five rating it “good”. Half of the participants rated their current health status as either “somewhat worse” or “much worse” compared with one year ago.
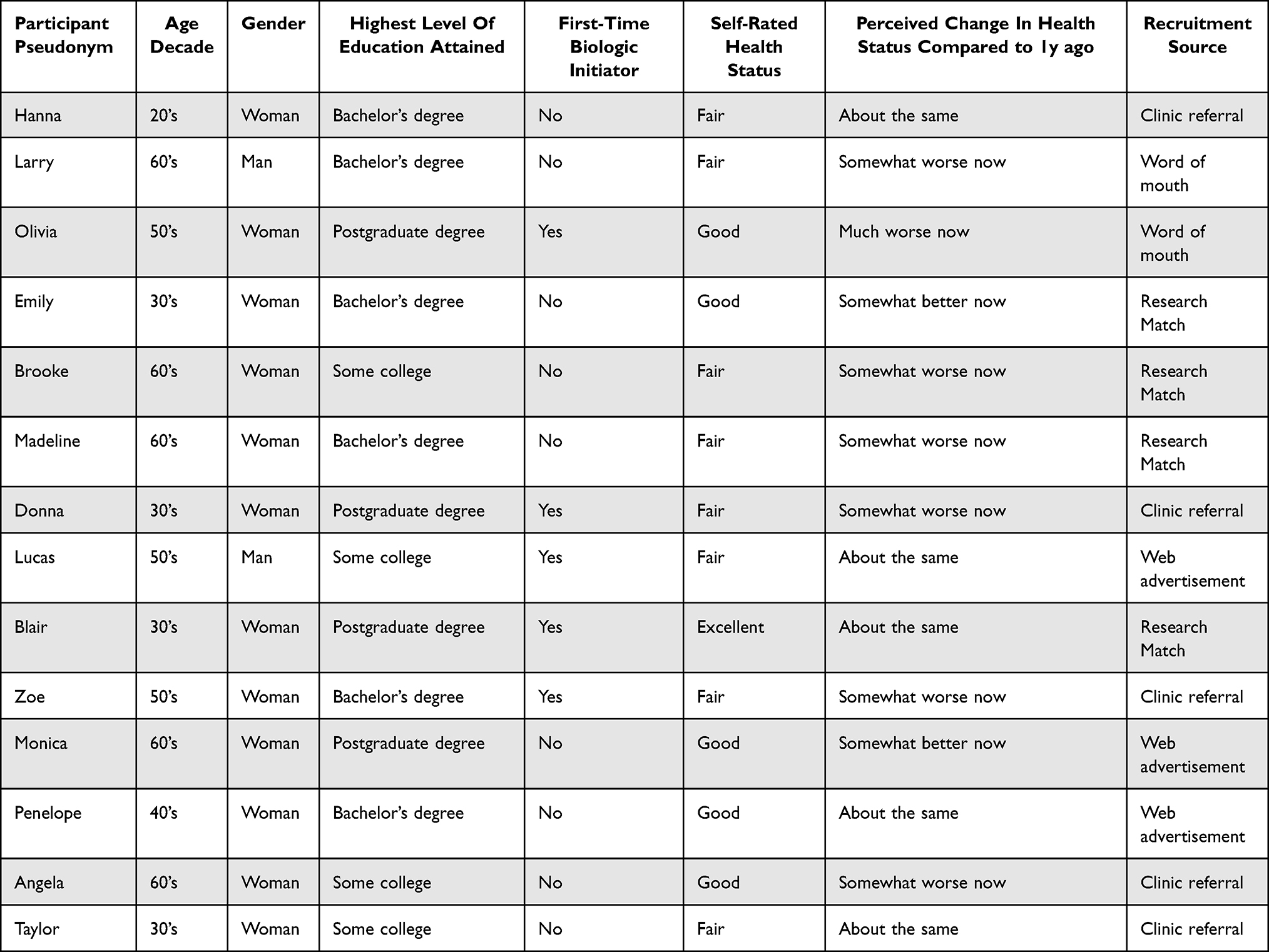 |
Table 1 Participant Characteristics |
Qualitative Themes
Theme 1: Treatment-Related Information Seeking Behavior
The first theme, treatment-related information seeking behavior, which encompassed how and where participants seek information about treatments for RA, comprised conceptual categories of: 1) gathering information from internet sources; 2) discussions with physicians or allied health providers; 3) talking with friends or close contacts with a chronic disease; 4) evaluating the credibility of information; and 5) other miscellaneous sources (Table 2). Gathering information from internet sources describes the various web-based sources that participants typically reviewed, including general searching, evidence-based or technical sources, and the pharmaceutical company’s website. Some participants described changes to their information needs as time passed after their initial diagnosis:
Most of it was just, you know, searching around, but my searches weren’t very focused, I mean in July when I was first diagnosed, I was in so much pain I didn’t care what he gave me. So it’s only since, you know, August, beginning to middle of August after I had, you know, steroid shots and everything else. So I started feeling better to where I actually could look at things to say ‘okay, what do I want to do.’ (Olivia, 50’s, first-time initiator)
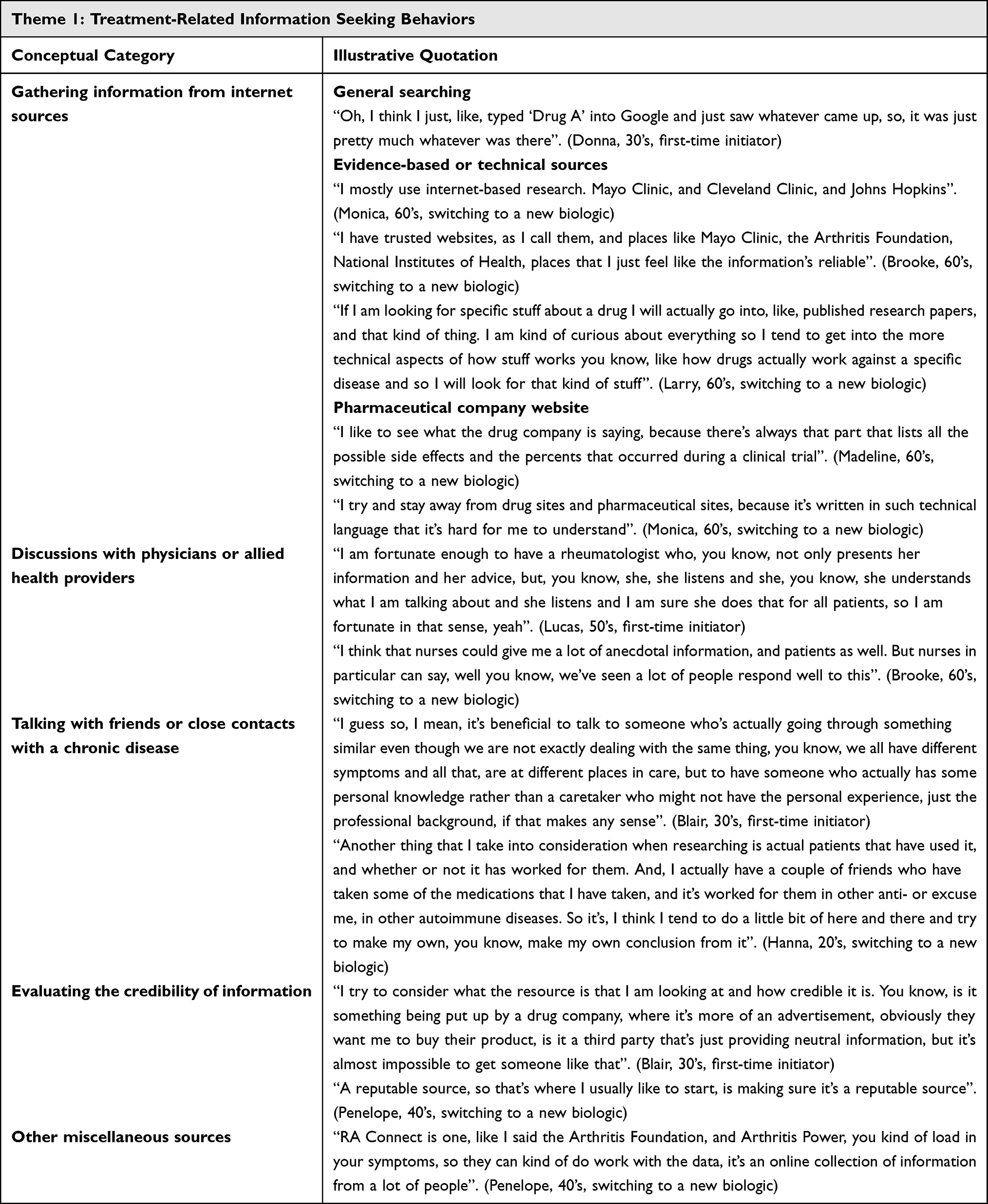 |
Table 2 Conceptual Categories and Illustrative Quotations from Participants for Theme 1 |
Other participants described utilizing specific scientific resources, which included websites maintained by established medical institutions, foundations, and government agencies, as well as technical sources such as peer-reviewed research literature. Finally, some individuals reviewed the information provided by pharmaceutical companies, which they felt presented a comprehensive list of side effects and corresponding statistics. Others did not share this perspective, instead feeling that this information was either too technical or contained some bias.
And I, I did, last week, look at the Drug A website, and the tools that they have, but I didn’t look at them extensively, because again, I have in my mind that the drug company wants you to take their drug, and your body to become acclimated to it, so that you can no longer live without this drug, and I have a hard time with that. (Zoe, 50’s, first-time initiator)
Discussions with physicians or allied health providers describes the conversations that participants have had with different healthcare providers. Many participants described gathering information from their rheumatologist, and they felt that it was important to have a rheumatologist who listened in addition to providing advice. Nurses were also suggested as a valuable resource for providing information about biologic use, particularly with respect to recounting anecdotal experiences of previous patients who initiated a biologic. Talking with friends or close contacts with a chronic disease describes how participants connected with other individuals based on shared lived experiences. Participants detailed how they spoke with others living with chronic disease (including conditions other than RA) to learn about their symptoms and whether certain medications worked for them. They described feeling that this personal knowledge gained from lived experience was valuable. One participant countered this perspective by caveating that “everybody’s experience is different” and noted that
…. people with chronic illnesses, we carry a lot of other baggage (…) I don’t like the online support groups and that sort of thing, the negative that comes with it. (Brooke, 60’s, switching to a new biologic)
Evaluating the credibility of information encompasses how participants assessed the information they found. Participants described how they evaluated the trustworthiness of various sources, including considering its reputation (eg, Mayo Clinic) and whether the source had a financial incentive to provide specific information. Other miscellaneous sources encompassed additional resources that participants consulted, including programs run by pharmaceutical companies, books, and meetings held by professional organizations:
I had also ordered a bunch of books, I have followed a lot of stuff from the American College of Rheumatology, like … when they have their yearly conventions and stuff. (Taylor, 30’s, switching to a new biologic)
Theme 2: Helpful Aspects of the Decision Aid
The second theme, helpful aspects of the decision aid, which encompassed the positive and beneficial aspects that participants experienced while utilizing the decision aid, comprised conceptual categories of: 1) overall positive impressions of decision aid usability; 2) useful content presented in the decision aid; 3) feeling a sense of connection by hearing patient stories; and 4) perceived trustworthiness of information (Table 3). While describing their overall positive impressions of decision aid usability, participants indicated a high level of overall satisfaction with the decision aid:
I think that it is something that will be helpful for them to make their decision. I mean choosing something like a biologic is really a big decision, and it’s a scary decision. So I just feel that, yeah it would help a lot. (Madeline, 60’s, switching to a new biologic)
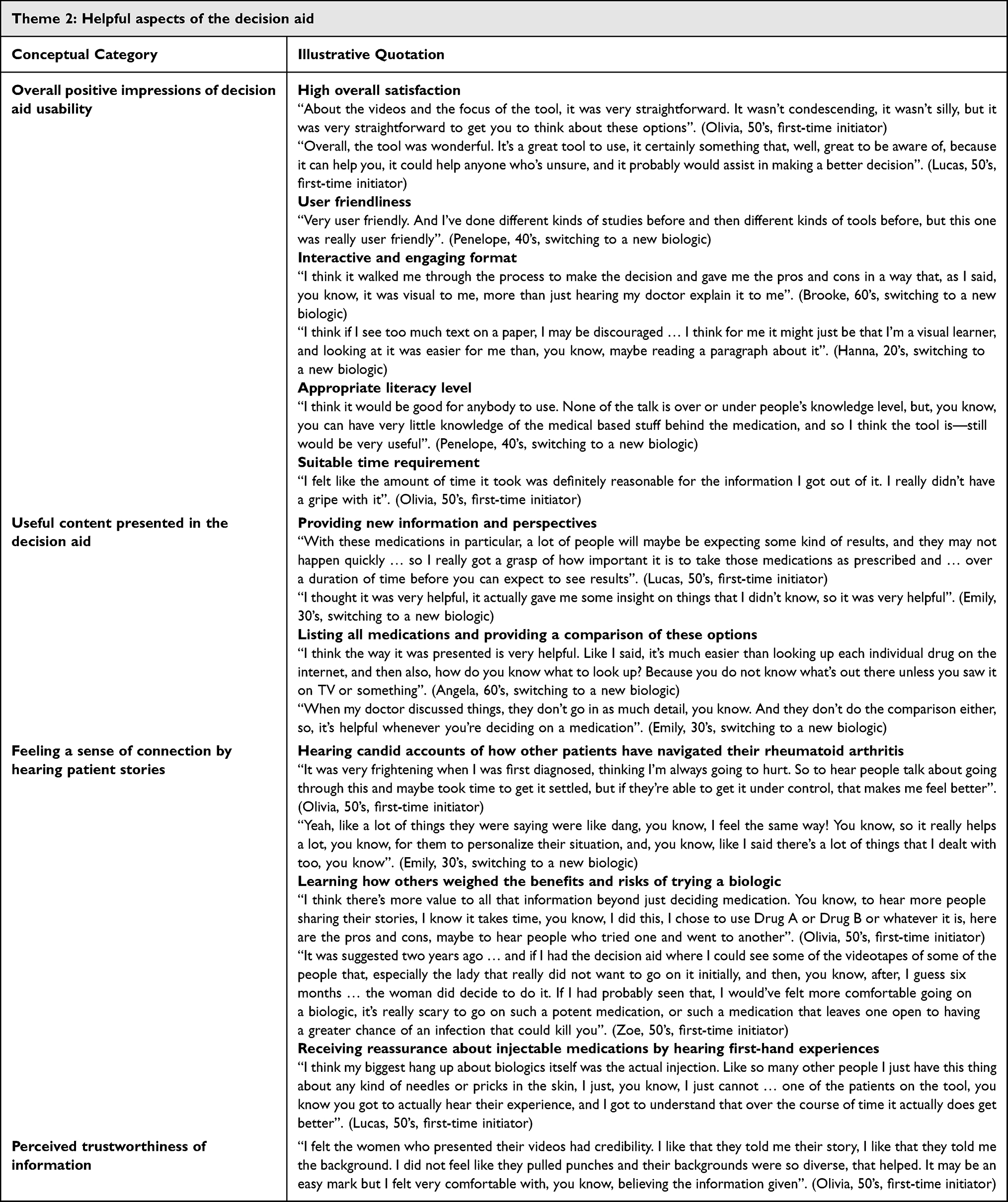 |
Table 3 Conceptual Categories and Illustrative Quotations from Participants for Theme 2 |
Participants felt that the decision aid was user friendly, delivered at an appropriate level, and required a reasonable amount of time. Moreover, participants felt that it was presented in an interactive and engaging format, and most individuals enjoyed the incorporation of videos as these added a “human” dimension to the decision aid:
I actually liked to look at the videos, because I like to hear more about it, there’s just something about having a human voice tell you rather than reading it. (Madeline, 60’s, switching to a new biologic)
Participants described reviewing useful content presented in the decision aid. In addition to learning new information, one participant described how the material prompted her to think about her decision in a new way:
It was a question about how frequently would you want to take the biologic. And I think it was the woman who said ‘you have to do it everyday, because then if you need to change it, you can change it a lot faster instead of waiting every other week,’ which I thought was very interesting. I had never thought that way before. (Olivia, 50’s, first-time initiator)
Participants appreciated how the decision aid presented information about each biologic, including by providing a comprehensive list of different medications as well as providing information that allowed for direct comparisons between the different options. Participants described feeling a sense of connection by hearing patient stories, which included hearing candid accounts of how others have navigated their RA and learning how others weighed the benefits and risks of trying a biologic:
I think the new part to me was just the way it was presented, coming from an RA sufferer instead of from a doctor, or a drug company. And also to share the thought process of what choices they made. (Olivia, 50’s, first-time initiator)
Participants also described receiving reassurance about injectable medications by hearing these first-hand patient experiences in the videos:
I was most interested in the one that they had to inject themselves, because I thought that’s what I was going to end up doing … I remember that one woman talked about it, and how you just don’t have to jab it in your whole body, you just put it under your skin, or something like that … watching that video of the woman with the injection that had a drug she was injecting, that made me feel like, you know, it’s not that big of a deal after all, you know. It’s nothing to be afraid of, really. (Angela, 60’s, switching to a new biologic)
Finally, participants perceived the information contained in the decision as trustworthy; this was due, in part, to the patient stories which participants felt lent credibility to the content. Another participant remarked that the decision aid did not feel like an advertisement, which also created a feeling of trustworthiness:
Yeah, the fact that it was presented by – it didn’t reek of a commercial, so therefore it seemed reliable, so that kind of information is good because it sounds, it didn’t sound like someone was being paid to advertise. (Brooke, 60’s, switching to a new biologic)
Theme 3: Decision Aid Limitations and Potential Solutions
The third theme, decision aid limitations and potential solutions, included conceptual categories of: 1) perspectives on decision aid presentation; 2) identifying content preferences and gaps; and 3) concerns about accessibility and implementation (Table 4). Participants’ perspectives on decision aid presentation included feedback on the tool’s length and format. Some felt that the decision aid was long and included some redundant information, and others expressed a preference for reading written materials rather than watching the videos as this was felt to be quicker:
I don’t really enjoy the videos honestly. I just like to get, you know, into the written stuff. You know, in a lot of cases I find the videos are more of a time waster than informative. So, for me if it’s, you know, printed it’s just a lot easier and faster for me to get through. (Larry, 60’s, switching to a new biologic)
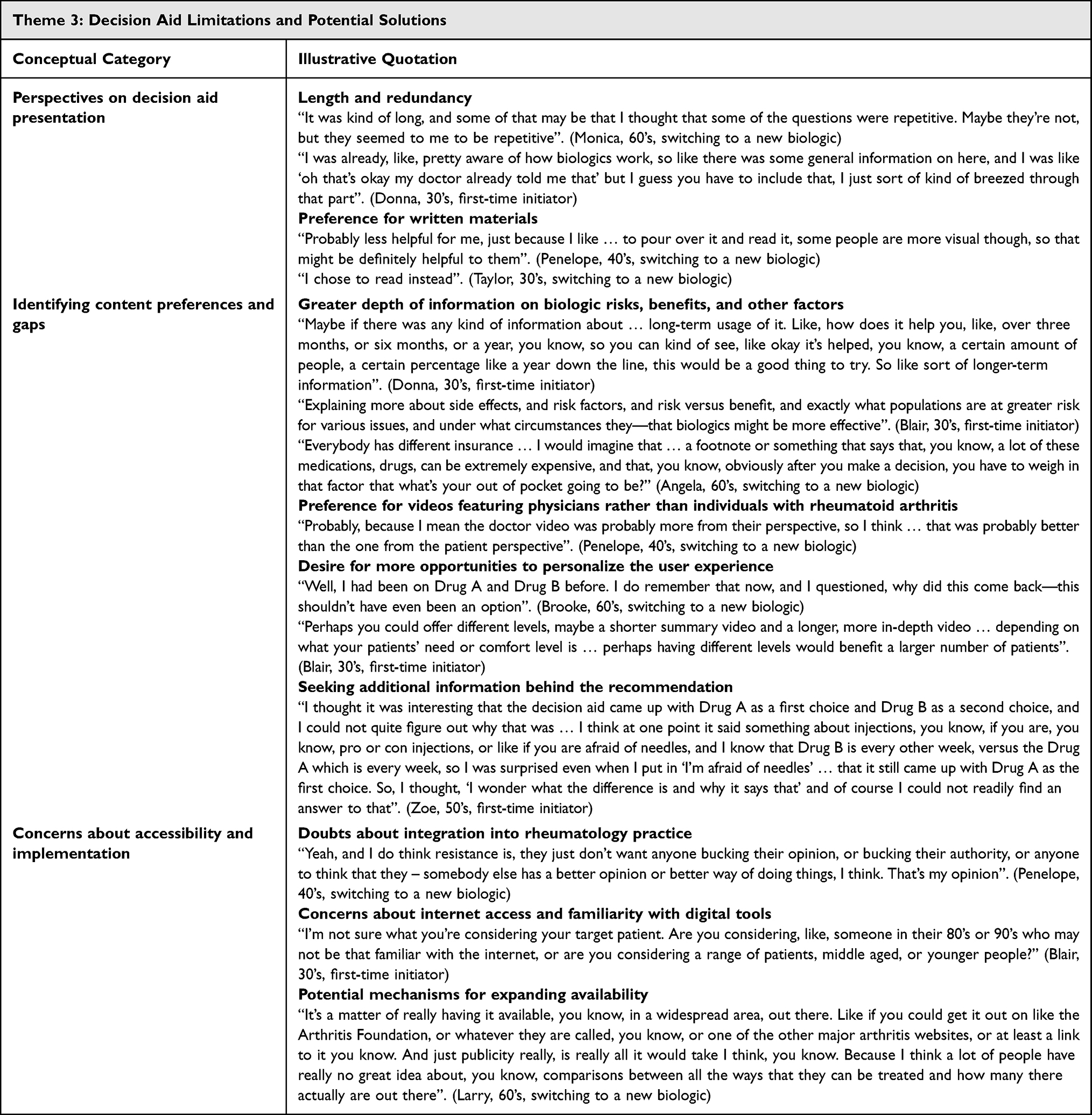 |
Table 4 Conceptual Categories and Illustrative Quotations from Participants for Theme 3 |
Participants identified several content preferences and gaps. Specifically, participants wanted to receive more information about the long-term use of biologics, potential side effects, specific populations who may be at a greater risk for complications, when biologics may be particularly beneficial, and the general risks versus benefits of these medications. Moreover, given the cost of biologics, participants suggested that adding information about insurance would be helpful. Some expressed an interest in more videos featuring physicians rather than patients. Finally, a few individuals who were switching to a new biologic indicated that they would have preferred if the decision aid could eliminate biologic recommendations that they had already tried previously:
Incorporate that rule that if you’d tried two TNF inhibitors previously, and they’re not working, then don’t offer it [as a recommendation] anymore. (Monica, 60’s, switching to a new biologic)
Lastly, participants expressed concerns about accessibility and implementation of the decision aid in a real-world rheumatology practice setting. Although nearly all participants described having positive relationships with their current care team, they felt that some rheumatologists may be resistant to incorporating a decision aid for several reasons, including a perceived threat to their expertise or authority, unwillingness to individualize treatment, resistance to trying something new, and lack of appointment time:
A rheumatologist that has very set opinions of how things work, and doesn’t see patients as being different from each other, they may just not want one more thing, or one more thing to take up any more time of their appointment. But I think this would be a time saver, because it actually kind of does some of their work for them. But I do feel like some doctors are resistant to anything new. (Penelope, 40’s, switching to a new biologic)
Participants also expressed concerns about internet access and familiarity with digital tools, particularly among older individuals living with RA: “Of course, the other piece is older folks don’t necessarily have access or have the capabilities to use these kinds of electronic tools” (Zoe, 50’s, first-time initiator). Nevertheless, the web-based format of the tool was also seen as a strength, and several ideas were suggested to increase its availability, including leveraging trusted organization websites such as the Arthritis Foundation as well as other major arthritis websites.
Theme 4: Impacts on the Decision to Initiate a Biologic
The fourth and final theme, the impacts on the decision to initiate a biologic, included conceptual categories of: 1) feeling open to more treatment options; 2) generating questions for the rheumatologist; 3) feeling empowered to engage in shared decision-making; and 4) reinforced confidence in the decision (Table 5). After using the decision aid, participants described feeling open to more treatment options that they may have felt more reluctant to try previously:
Well, before I was just against it, really against it, now … I’ll say I’m on the fence, but I’m certainly leaning more towards, towards using the biologic because I understand the importance of it and how some, you know, some forms of the medication are not effective, or not as effective and the biologics could certainly be more effective, so, and if I take into consideration the minor discomfort that I may feel versus the relief that I could possibly gain, I don’t think it’s too big of a sacrifice. So I’m really leaning more towards just taking, you know, biologics. (Lucas, 50’s, first-time initiator)
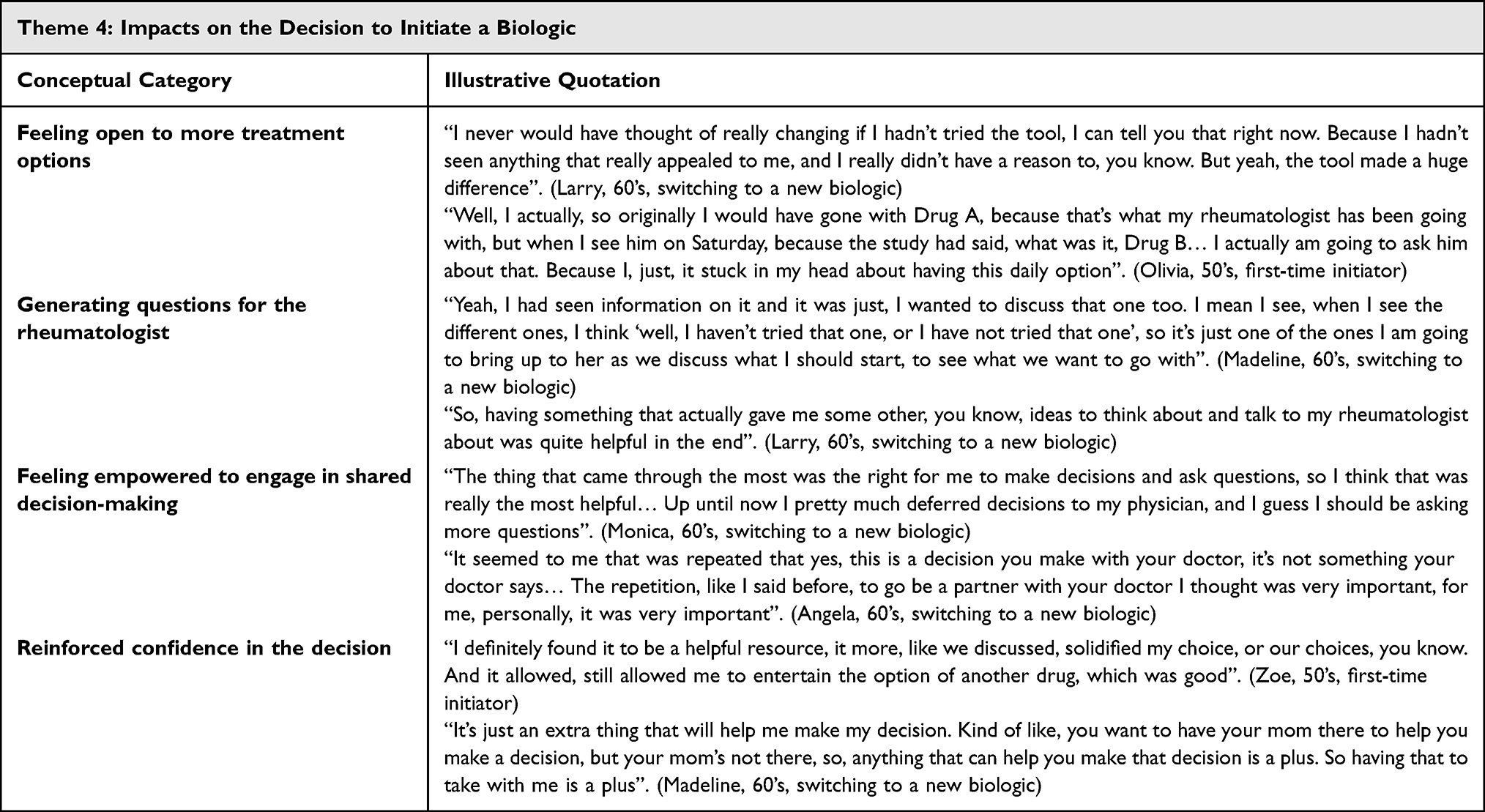 |
Table 5 Conceptual Categories and Illustrative Quotations from Participants for Theme 4 |
Participants also reported how the decision aid prompted them to consider a biologic that they had not previously thought of. Moreover, participants found that the content presented in the decision aid was useful for generating questions for their rheumatologist, leading to new questions to discuss at their next appointment. Participants reported feeling empowered to engage in shared decision-making after working through the decision aid. Specifically, individuals described how they had previously deferred to their physician’s recommendations, but now felt that they wanted to ask more questions and partner with their physician moving forward. One participant further noted how the decision aid-generated summary may help initiate these conversations with their physician. Finally, participants felt that the decision aid reinforced confidence in their decision of whether to initiate a given biologic. Individuals described the tool as helping to solidify or reinforce their choice:
It kind of reinforced my decision on my end. And I think, I think it was extremely helpful in feeling confident that I made the correct decision. (Hanna, 20’s, switching to a new biologic)
Discussion
We conducted a qualitative interview study to understand RA patients’ perspectives on the use of a decision aid regarding biologic initiation or switching. Findings include one theme describing treatment-related information seeking behaviors, specifically where individuals sought information about treatments for RA as well as how this information was evaluated for credibility, two themes related to the helpful aspects (eg, hearing patient stories) and limitations of the tool, and a fourth theme describing how the decision aid impacted the decision to initiate a biologic, including promoting feelings of empowerment to engage in shared decision-making.
Our findings build on prior literature describing medication-related information needs of RA patients. A 2018 qualitative synthesis of RA and spondyloarthritis (SpA) patient attitudes reported that participants felt that information from their physician was credible when it matched that received from other sources (eg, internet sources, pamphlets).17 Individuals also noted different types of information that they wanted to inform their decision, including information about alternative treatments as well as how DMARDs may impact their daily life (eg, whether to limit alcohol intake, how to time medications to minimize side effects during certain periods), although this study was not limited to those specifically considering biologic DMARDs.17 Another 2019 systematic review among individuals with inflammatory arthritis reported that participants desired information about their pharmacological management, including the rationale for medications, side effects, and alternative therapies.18 In addition to these well-characterized information needs and sources (eg, internet-based searching, discussions with a rheumatologist), our study further identified a key benefit to building relationships with other individuals living with a chronic disease, as they may provide a rich perspective on medication use that is informed by a shared lived experience. This is consistent with prior work showing that individuals with RA will utilize online support groups to discuss their disease experiences (including medication use).19 Conversely, a recent study in Belgium evaluated the need and potential format of a peer mentoring program for individuals newly diagnosed with RA; while participants did seek more information about medication use, this was perceived to be primarily the responsibility of the healthcare team rather than a peer mentor.20 While the participants in our study largely described benefiting from talking with peers, one noted that the views shared in online support groups may be more negative than encouraging. It would be valuable for future research to examine how best to integrate peer connections to support medication decision-making.
In the current study, participants described their experiences using a decision aid, encompassing both aspects they found helpful and its perceived limitations. Several participants highlighted the visual components of the decision aid as being particularly beneficial, which is consistent with prior research on the use of audiovisual aids and improved health literacy.21 Accordingly, similar approaches have been applied in the development of decision aids for other conditions, including a biologic decision aid for individuals with inflammatory bowel disease (IBD) that incorporated video content and other visual aids to overcome varying levels of numeracy among end users,22 as well as fully video-based decision aid for pediatric IBD patients to improve risk communication.23 At the same time, selected participants in the current study instead expressed a preference for more written content as well as greater depth of certain information (eg, medication risks), suggesting that it may be beneficial to offer individuals the opportunity to select from different media formats and lengths (eg, full length vs. abbreviated summary) where feasible. Next, participants in the current study overwhelmingly responded positively to hearing patient stories as part of the decision aid. Interestingly, although research suggests that hearing another patient’s experience helps with understanding one’s own chronic illness and the adjustment to treatment, findings are mixed with respect to the potentially beneficial role of patient stories in medication decision-making.24 Further research in this area is warranted. Participants also wondered whether a decision aid could be implemented in community rheumatology practices, citing time constraints and anticipated reluctance of rheumatologists. Indeed, while rheumatologists agree that patient decision aids could enhance patient care, they have also outlined practical challenges with their implementation, thereby highlighting the need to develop strategies to support their integration into clinical practice.25 Such strategies may be multipronged, including the use of different formats (eg, print, basic digital, or electronic health record-integrated), availability of training, and the use of clinical champions. As rheumatologists and other healthcare providers are key stakeholders of patient decision aids such as this one, it is imperative that future studies continue to survey and interview these providers to ensure feasible implementation of digital tools.
Finally, participants in our study reported feeling empowered to engage in shared decision-making. This is particularly important in light of a qualitative synthesis of RA and SpA patient attitudes toward DMARD use, which reported that patients wished to maintain a sense of control and feel ownership over the decision to take both conventional and biologic DMARDs.17 Moreover, participants in the current study described feeling confident in their decision. This is consistent with a recent interview study among psoriatic arthritis patients which identified “gaining confidence” as a key theme toward medication decision-making, which included feeling empowered from gaining knowledge about treatment options as well as experiencing first-hand various physical function benefits after initiating treatment.26 Future longitudinal studies should examine whether the use of such decision aids translates to lower rates of discontinuation.
The strengths of our study deserve comment. The application of a qualitative interview approach allowed for the identification of detailed perspectives on the decision aid, including among five individuals who were newly initiating a biologic, which is a practically challenging treatment window to capture in research. Indeed, it would be valuable for future work among more patients to examine whether these perspectives surrounding decision-making differed between those who are newly starting a biologic versus those who are switching to a different biologic. Our topic guide was developed and refined using an iterative process, and our iterative analysis ceased upon agreement among the research team that no new codes or themes had emerged.27,28 Finally, we leveraged several web-based resources to expand our study beyond the Boston area and successfully enrolled individuals across the United States. Our study is also not without limitations. Our sample was restricted to English-speaking individuals living in the US, and >70% of participants had obtained a bachelor’s degree or higher. Moreover, our study population was comprised largely of women, and we did not collect data on race/ethnicity, occupation, or other demographic factors. As there are potential demographic differences in the health information needs among those with inflammatory arthritis,18 it is imperative that future work intentionally recruit individuals from many types of diverse backgrounds, particularly given the critical role that education and health literacy can play in the successful uptake of education tools. Moreover, although RA disproportionately affects women, it would be valuable for future studies to explore potential gender differences in treatment decision-making; indeed, a study among individuals considering hemodialysis found that men and women approach treatment decisions differently and prioritize different expectations for a given treatment.29 Nevertheless, the current findings do continue to extend our understanding of RA patient decision-making surrounding biologic therapy.
In conclusion, we conducted a qualitative interview study to understand the information needs of individuals with RA who are living in the US, as well as their experiences with a web-based decision aid in the context of considering biologic therapy. We identified key information needs, including participants’ desire for more detailed information on potential long-term side effects, as well as an important role for connecting with peers living with chronic disease who can provide information to RA patients considering a biologic that is informed by a shared lived experience. Moreover, we identified unique perspectives on the use of different media, broader decision aid format, and the inclusion of patient voices. Finally, our findings suggest that the current decision aid facilitated feelings of empowerment to engage in shared decision-making. Future work ought to ensure that healthcare provider (particularly rheumatologist) perspectives are evaluated to ensure feasible strategies for implementation, examine perspectives among key subpopulations, and evaluate real-world effectiveness. Taken together, our findings highlight key factors to consider for the design/refinement and implementation of patient decision aids in the US to appropriately meet the needs of patients who are considering a biologic.
Data Sharing Statement
Due to the sensitive nature of the research, these data are not openly available in a central repository. Data sharing requests may be made to the corresponding authors and will be subject to an institutional data use agreement and relevant institutional review board approvals.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Dr. Rai is supported by a Postdoctoral Fellowship from the Canadian Institutes of Health Research. Dr. McCormick is supported by a Career Development Award from the National Institutes of Health (K99-AR080243). Dr. Yokose is supported by a Career Development Award from the National Institutes of Health (K23-AR081425). Dr. De Vera is supported by a Tier 2 Canada Research Chair in Health Outcomes and Treatment Adherence. This qualitative study was funded by Pfizer Inc. through the Independent Grants for Learning & Change (IGLC) program (grant identification number 17924525). Pfizer Inc. had no role in the development of the decision aid, study design, data analysis, drafting of the manuscript, or decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Finckh A, Gilbert B, Hodkinson B, et al. Global epidemiology of rheumatoid arthritis. Nat Rev Rheumatol. 2022;18(10):591–14. doi:10.1038/s41584-022-00827-y
2. Hsieh P-H, Wu O, Geue C, McIntosh E, McInnes IB, Siebert S. Economic burden of rheumatoid arthritis: a systematic review of literature in biologic era. Ann Rheumatic Dis. 2020;79(6):771. doi:10.1136/annrheumdis-2019-216243
3. Chen C-I, Wang L, Wei W, Yuce H, Phillips K. Burden of rheumatoid arthritis among US Medicare population: co-morbidities, health-care resource utilization and costs. Rheumatol Adv Pract. 2018;2(1). doi:10.1093/rap/rky005
4. Romano S, Salustri E, Ruscitti P, Carubbi F, Penco M, Giacomelli R. Cardiovascular and metabolic comorbidities in rheumatoid arthritis. Curr Rheumatol Rep. 2018;20(12):81. doi:10.1007/s11926-018-0790-9
5. Scheiman-Elazary A, Duan L, Shourt C, et al. The rate of adherence to antiarthritis medications and associated factors among patients with rheumatoid arthritis: a systematic literature review and metaanalysis. J Rheumatol. 2016;43(3):512–523. doi:10.3899/jrheum.141371
6. Balsa A, García de Yébenes MJ, Carmona L. Multilevel factors predict medication adherence in rheumatoid arthritis: a 6-month cohort study. Ann Rheumatic Dis. 2022;81(3):327. doi:10.1136/annrheumdis-2021-221163
7. Marengo MF, Suarez-Almazor ME. Improving treatment adherence in patients with rheumatoid arthritis: what are the options? Int J Clin Rheumtol. 2015;10(5):345–356. doi:10.2217/ijr.15.39
8. Akuffo-Addo E, Udounwa T, Chan J, Cauchi L. Exploring biologic treatment hesitancy among black and indigenous populations in Canada: a review. J Racial Ethn Health Disparities. 2023;10(2):942–951. doi:10.1007/s40615-022-01282-x
9. Kottak N, Tesser J, Leibowitz E, Rosenberg M, Parenti D, DeHoratius R. Ethnographic observational study of the biologic initiation conversation between rheumatologists and biologic-naive rheumatoid arthritis patients. Arthritis Care Res. 2018;70(7):997–1004. doi:10.1002/acr.23527
10. Rai SK, Howren A, Wilcox ES, et al. Exploring strategies to support medication adherence in patients with inflammatory arthritis: a patient-oriented qualitative study using an interactive focus group activity. Patient Prefer Adherence. 2018;12:2015–2025. doi:10.2147/ppa.S174672
11. Stacey D, Lewis KB, Smith M, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2024;1(1):Cd001431. doi:10.1002/14651858.CD001431.pub6
12. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
13. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
14. Li LC, Shaw CD, Lacaille D, et al. Effects of a web-based patient decision aid on biologic and small-molecule agents for rheumatoid arthritis: results from a proof-of-concept study. Arthr Care Res. 2018;70(3):343–352. doi:10.1002/acr.23287
15. White RE, Cooper K. Chapter 9: grounded Theory. In: Qualitative Research in the Post-Modern Era: Critical Approaches and Selected Methodologies. Springer; 2022.
16. Hewlett S, de Wit M, Richards P, et al. Patients and professionals as research partners: challenges, practicalities, and benefits. Arthritis Rheum. 2006;55(4):676–680.
17. Kelly A, Tymms K, Tunnicliffe DJ, et al. Patients’ attitudes and experiences of disease-modifying antirheumatic drugs in rheumatoid arthritis and spondyloarthritis: a qualitative synthesis. Arthritis Care Res. 2018;70(4):525–532. doi:10.1002/acr.23329
18. Connelly K, Segan J, Lu A, et al. Patients’ perceived health information needs in inflammatory arthritis: a systematic review. Semin Arthritis Rheum. 2019;48(5):900–910. doi:10.1016/j.semarthrit.2018.07.014
19. Des Bordes JKA, Foreman J, Westrich-Robertson T, et al. Interactions and perceptions of patients with rheumatoid arthritis participating in an online support group. Clin Rheumatol. 2020;39(6):1775–1782. doi:10.1007/s10067-020-04967-y
20. Van der Elst K, De Cock D, Bangels L, et al. ‘More than just chitchat’: a qualitative study concerning the need and potential format of a peer mentor programme for patients with early rheumatoid arthritis. RMD Open. 2021;7(3). doi:10.1136/rmdopen-2021-001795
21. Mbanda N, Dada S, Bastable K, Ingalill GB, Ralf WS. A scoping review of the use of visual aids in health education materials for persons with low-literacy levels. Patient Educ Couns. 2021;104(5):998–1017. doi:10.1016/j.pec.2020.11.034
22. Almario CV, Keller MS, Chen M, et al. Optimizing selection of biologics in inflammatory bowel disease: development of an online patient decision aid using conjoint analysis. Off J Am College Gastroenterol. 2018;113(1):58–71. doi:10.1038/ajg.2017.470
23. Newman NE, Williams KL, Zikmund-Fisher BJ, Adler J. A new video aid for communicating risk in the treatment of pediatric inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2020;70(2):e33–e36. doi:10.1097/MPG.0000000000002557
24. Bekker HL, Winterbottom AE, Butow P, et al. Do personal stories make patient decision aids more effective? A critical review of theory and evidence. BMC Med Inform Decis Mak. 2013;13 Suppl 2(Suppl 2):S9. doi:10.1186/1472-6947-13-s2-s9
25. Zong JY, Leese J, Klemm A, et al. Rheumatologists’ views and perceived barriers to using patient decision aids in clinical practice. Arthr Care Res. 2015;67(10):1463–1470. doi:10.1002/acr.22605
26. Sumpton D, Oliffe M, Kane B, et al. Patients’ perspectives on shared decision-making about medications in psoriatic arthritis: an interview study. Arthr Care Res. 2022;74(12):2066–2075. doi:10.1002/acr.24748
27. Leese J, Li LC, Nimmon L, Townsend AF, Backman CL. Moving beyond “Until Saturation Was Reached”: critically examining how saturation is used and reported in qualitative research. Arthr Care Res. 2021;73(9):1225–1227. doi:10.1002/acr.24600
28. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quantity. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
29. Beckwith H, Thomas N, Adwaney A, et al. Gender differences in experiences and expectations of hemodialysis in a frail and seriously unwell patient population. Kidney Int Rep. 2022;7(11):2421–2430. doi:10.1016/j.ekir.2022.08.023
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Rheumatoid Vasculitis, an Uncommon Complication of Non-Deforming Rheumatoid Arthritis: A Case Report
Taha ZI, Abdalla YA, Hamza SB, Eltagalawi MF, Abubakr ME, William J, Abdalgadir SA
Open Access Rheumatology: Research and Reviews 2022, 14:141-146
Published Date: 18 July 2022
Rapidly Progressive Felty Syndrome After Sudden Discontinuation of Methotrexate: A Case Report and Review of Literature
Hamsho S, Alannouf I, Ashour AA
International Medical Case Reports Journal 2022, 15:473-477
Published Date: 2 September 2022
Expectations and Experiences of a Group of Patients Enrolled in an Educational Program for Rheumatoid Arthritis at a Specialized Care Center in Colombia
Castiblanco-Montañez RA, Buitrago-Garcia D, Arévalo Velandia A, Garzón-Cepeda JD, Rodríguez-Florido F, Sánchez Vanegas G, Santos-Moreno P
Journal of Multidisciplinary Healthcare 2023, 16:483-492
Published Date: 22 February 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Dietary Management Experiences and Educational Needs of Patients in the Recovery Phase of Pancreatitis: A Descriptive Phenomenological Study
Kuang L, Jiang S, Liu X, Xiong T, Luo X
Patient Preference and Adherence 2026, 20:594779
Published Date: 8 April 2026