Back to Journals » Patient Preference and Adherence » Volume 20
Dietary Management Experiences and Educational Needs of Patients in the Recovery Phase of Pancreatitis: A Descriptive Phenomenological Study
Authors Kuang L, Jiang S, Liu X, Xiong T, Luo X
Received 8 January 2026
Accepted for publication 24 March 2026
Published 8 April 2026 Volume 2026:20 594779
DOI https://doi.org/10.2147/PPA.S594779
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Lixia Kuang, Sheng Jiang, Xiaofang Liu, Tao Xiong, Xiao Luo
Department of Hepatobiliary, Chongqing University Fuling Hospital, Chongqing University, Chongqing, 408000, People’s Republic of China
Correspondence: Xiao Luo, Department of Hepatobiliary, Chongqing University Fuling Hospital, Chongqing University, Chongqing, 408000, People’s Republic of China, Email [email protected]
Purpose: To explore dietary management experiences and nursing education needs among patients in the recovery phase of pancreatitis from the patient perspective, and to provide evidence to inform the development of feasible, individualized, and continuous dietary management strategies.
Patients and Methods: A descriptive phenomenological qualitative design was adopted. Purposive sampling was used to recruit 15 patients in the recovery phase of pancreatitis who were treated in the hepatobiliary surgery department of a tertiary hospital in Chongqing, China, from June to September 2025. Semi-structured, in-depth interviews were conducted. Data were analyzed using thematic analysis.
Results: Four major themes were identified: (1) perceptions of the relationship between diet and disease; (2) limited access to dietary information and insufficient content; (3) challenges encountered during dietary management; and (4) specific needs regarding the content and delivery formats of dietary education.
Conclusion: Although patients in the recovery phase of pancreatitis recognize the importance of dietary control, the lack of specific, actionable guidance and ongoing support substantially limits long-term adherence to a low-fat diet. Clinical nurses should move beyond one-time, principle-based education and provide structured, staged, and individualized dietary guidance. Integrating digital health tools to support continuous follow-up may enhance patients’ dietary self-management, promote recovery, and reduce the risk of disease recurrence.
Keywords: pancreatitis, dietary management, qualitative research, patient education, nursing practice
Introduction
Pancreatitis is an inflammatory disease caused by the premature activation of pancreatic enzymes, leading to local tissue injury and systemic complications, and in severe cases, multi-organ dysfunction.1 In recent years, the global incidence of pancreatitis has continued to rise, largely driven by changing dietary patterns and the increasing prevalence of metabolic risk factors.2 Approximately 10–35% of patients experience recurrence after their first episode, which is associated with poorer clinical outcomes, increased healthcare utilization, and reduced quality of life.3 Therefore, effective management during the recovery phase is critical for preventing recurrence and promoting long-term health. Pancreatic diseases, including both pancreatitis and periampullary cancers, represent a significant burden on healthcare systems globally, with management strategies varying across different clinical contexts and geographical settings.4
Dietary factors play a pivotal role in both the onset and recurrence of pancreatitis.5,6 Evidence-based nutritional management can reduce pancreatic workload, improve nutritional status, and lower the risk of recurrence.7–9 This patient-centered perspective aligns with broader concepts of food and medicine homology, where dietary choices are inherently linked to health outcomes.10 However, in clinical practice, many patients struggle to maintain recommended low-fat dietary patterns after hospital discharge. Some patients overly restrict their diet due to fear of recurrence, resulting in inadequate energy and protein intake, whereas others find it difficult to sustain low-fat or triglyceride-lowering diets over time, which negatively affects recovery.11 These observations suggest that current dietary guidance during the recovery phase lacks sufficient specificity and practical applicability. Previous studies have reported that patients with pancreatitis often have limited health literacy, and their dietary self-management needs during the recovery phase remain largely unmet. Traditional discharge education is typically one-time and principle-based, with limited continuity, individualization, or digital support, making it difficult for patients to translate dietary recommendations into daily practice.12,13
Advances in disease modeling, such as patient-derived organoids, have opened new avenues for understanding pancreatic diseases—including pancreatitis—and for developing personalized therapeutic strategies.5,14 However, such approaches have not yet been integrated into dietary management research, which continues to rely on traditional patient education models. Understanding patients’ perceptions, challenges, and educational needs from their own perspectives is therefore essential for optimizing dietary management strategies. Furthermore, the transition from hospital to home during the recovery phase presents unique challenges. Patients must shift from strictly controlled hospital diets — often starting with nil-by-mouth or clear liquids—to self-managed dietary modifications at home, a period often characterized by uncertainty and fear of triggering a recurrence.
Accordingly, this study aimed to explore dietary management experiences, perceived challenges, and education needs among patients in the recovery phase of pancreatitis using a qualitative phenomenological approach. The findings are intended to inform the development of feasible, individualized, and continuous nursing-led dietary management strategies to enhance patient self-management and reduce the risk of disease recurrence.
Methods
Study Design
A descriptive phenomenological qualitative study design was employed to explore patients’ lived experiences of dietary management during the recovery phase of pancreatitis.
Participants
Purposive sampling was used to recruit patients from June to September 2025 from the hepatobiliary surgery department of a tertiary hospital in Chongqing, China. Inclusion criteria were: (1) age ≥18 years; (2) a confirmed diagnosis of pancreatitis and being in the clinical recovery phase, defined as the period following the resolution of acute symptoms (eg., abdominal pain, nausea, vomiting), tolerance of oral diet, and discharge from the hospital to home care; (3) ability to communicate effectively; and (4) willingness to participate with written informed consent. Exclusion criteria included: (1) diagnosed cognitive impairment; and (2) hemodynamic instability or inability to complete the interview.
Data collection continued until thematic saturation was achieved, meaning that no new themes emerged from subsequent interviews. A total of 15 participants were included and anonymized using codes N1–N15. Participant characteristics are presented in Table 1.
 |
Table 1 Participant Characteristics (N = 15) |
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Chongqing Fuling Hospital (Approval No. 2025CDFSFLYYEC-29). All participants provided written informed consent prior to data collection, which included permission for audio-recording and the publication of anonymized direct quotations. To protect participant privacy, all transcripts were anonymized using participant codes (N1–N15), audio recordings were destroyed immediately after transcription verification, and all data were stored on a password-protected computer accessible only to the research team. Participants were informed of their right to withdraw at any time without affecting their medical care.
Data Collection
The interview guide (Supplementary Table 1) was developed based on a literature review of dietary management in chronic diseases and on discussions within the research team. The questions were designed to explore patients’ knowledge, experiences, barriers, and educational needs related to dietary management during the recovery phase of pancreatitis. Semi-structured, in-depth interviews were conducted by a nursing researcher with experience in qualitative interviewing and clinical nutrition. Prior to each interview, the researcher explained the study purpose and procedures and established rapport with participants. With permission, interviews were audio-recorded and lasted 20–45 minutes. All interviews were completed without withdrawal or loss to follow-up. Audio recordings were transcribed verbatim within 24 hours, and non-verbal observations were documented immediately after each interview.
Data Analysis
Data were analyzed using thematic analysis as described by Braun and Clarke.15 Two researchers independently read transcripts, conducted line-by-line open coding, and identified meaningful units. Codes were compared and discussed within the research team to develop themes. Discrepancies were resolved through discussion until consensus was reached. Data saturation was considered achieved when two consecutive interviews yielded no new codes or themes, and when the research team agreed through discussion that the existing themes were sufficiently rich and comprehensive to address the research aims.
Rigor
Methodological rigor was ensured through investigator triangulation, independent coding, and member checking with selected participants to enhance credibility. An audit trail documenting data collection, analysis, and coding decisions was maintained to support dependability. Reflexive journaling was used to minimize researcher bias and enhance confirmability.
Results
Four major themes emerged from the data analysis: (1) perceptions of the relationship between diet and disease; (2) limited access to dietary information and insufficient content; (3) challenges encountered during dietary management; and (4) specific needs regarding the content and delivery formats of dietary education. Figure 1 illustrates the thematic structure of these findings, providing a visual overview of the major themes and their corresponding subthemes.
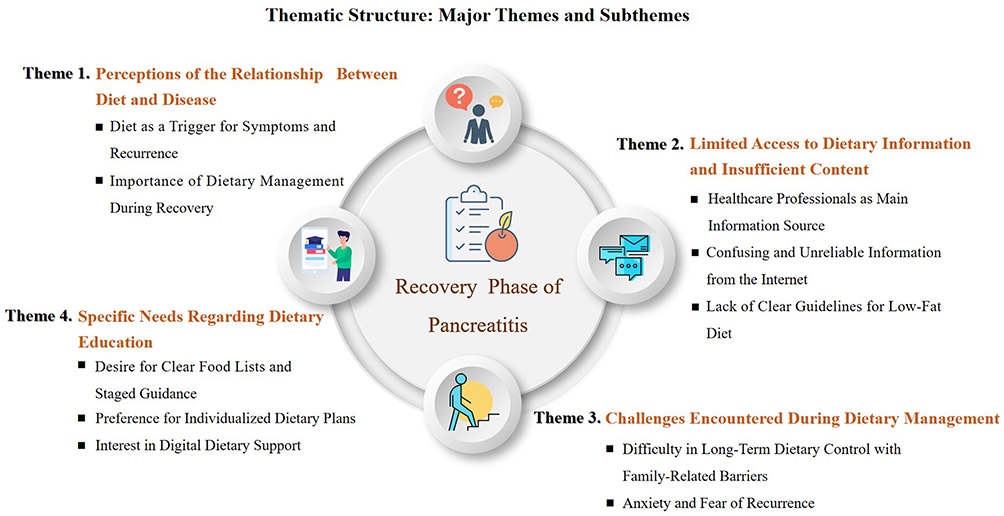 |
Figure 1 Thematic structure of dietary management experiences and educational needs among patients in the recovery phase of pancreatitis. Four major themes and their corresponding subthemes are displayed. |
Theme 1: Perceptions of the Relationship Between Diet and Disease
Diet as a Key Trigger for Symptoms and Recurrence
Most participants, particularly those with a history of recurrent pancreatitis, perceived diet as an important trigger for symptom exacerbation and disease recurrence. High-fat, greasy foods and overeating were commonly identified as precipitating factors. Participants described a clear temporal association between dietary indiscretion and the onset of discomfort or relapse.
My pancreatitis usually comes back when I eat too much or eat oily food. Not long after that, I start to feel uncomfortable, and once I go to the hospital, I know it has relapsed. (Participant N2)
I know diet is related to pancreatitis. Sometimes after recovery, when enough time passes, you feel like eating won’t affect you anymore. But after one big meal, pancreatitis comes back again. (Participant N4)
If I eat food that is too oily or too much, I can vaguely feel that something is wrong. (Participant N8)
The Importance of Dietary Management During Recovery
Participants generally believed that adhering to a low-fat, light diet was essential for reducing pancreatic burden and promoting recovery. Even those whose pancreatitis was not initially diet-related reported consciously adjusting their eating habits during the recovery phase.
The doctors and nurses emphasized many times that I must eat a low-fat diet during recovery and return to a normal diet gradually. I remember this very clearly. Diet definitely affects recovery. (Participant N1)
Even though my pancreatitis wasn’t caused by diet, I still pay attention to what I eat during recovery so my pancreas can heal properly. (Participant N5)
For patients like us, what we eat and what we don’t eat really has a big impact on recovery. (Participant N7)
Theme 2: Limited Access to Dietary Information and Insufficient Content
Healthcare Professionals as the Primary Source of Information
Most participants reported that their dietary knowledge came mainly from healthcare professionals during hospitalization. However, they often described the guidance they received as principle-based and lacking practical details.
Most of what I know about diet was told to me by doctors and nurses. They would say what I should eat, but usually just in general terms. (Participant N6)
The doctor said I needed a low-fat diet, but I didn’t really understand it at first. Later, after giving some examples, I understood better. (Participant N11)
Confusing and Unreliable Information from the Internet
Some participants attempted to seek dietary information online but found the content to be inconsistent, contradictory, or overly commercialized—which increased confusion rather than providing clarity.
Many people online share their own experiences. Some say certain foods are okay, others say they aren’t. After reading, I just feel more confused. (Participant N13)
There’s too much mixed information online. Some opinions contradict each other, and many are advertisements selling products. (Participant N15)
Lack of Clear and Concrete Standards for a Low-Fat Diet
Several participants expressed uncertainty about what a “low-fat diet” specifically meant in practice. The absence of clear standards made dietary implementation difficult.
The health booklet only says ‘low-fat diet’ and lists some foods that might be allowed, but it doesn’t explain how to arrange three meals a day. (Participant N10)
Even now, I’m not very clear about what ‘low-fat’ actually means or what the standard is. (Participant N14)
Theme 3: Challenges Encountered During Dietary Management
Difficulty Maintaining Long-Term Dietary Control and Family-Related Barriers
Many participants reported that maintaining a low-fat diet over the long term was challenging, particularly when their own preferences—or those of family members—differed from dietary recommendations. Coordinating household meals was often described as difficult.
We usually eat fairly lightly, but we can’t eat boiled food or food with very little oil every day. Other family members aren’t used to it either. (Participant N4)
I can manage avoiding oily food for a week, but a month is really hard—the dishes become repetitive. (Participant N7)
It’s already hard enough for me to stick to it, and my family can’t eat the same bland food with me every day. (Participant N8)
Anxiety and Fear of Recurrence During Eating
Several participants described persistent anxiety related to eating, particularly those who had previously experienced relapse. Eating was often accompanied by fear of making mistakes that could trigger recurrence.
Every time I eat, I worry about whether I’ll eat something wrong and cause a relapse. (Participant N4)
After relapsing several times, I feel anxious. Eating feels like a time bomb—I never feel at ease. (Participant N12)
Theme 4: Specific Needs Regarding the Content and Delivery Formats of Dietary Education
Demand for Clear Food Lists and Staged Dietary Guidance
Participants expressed a strong desire for practical tools—such as clear food lists, staged dietary recommendations, and daily meal plans—to support implementation.
What we really care about is what we can eat, what we can’t eat, and how to arrange each meal. (Participant N3)
It would be great to have daily meal plans, so I wouldn’t have to eat the same things all the time. (Participant N6)
If possible, I’d like a staged meal plan based on my condition, telling me exactly what I can eat each day. (Participant N9)
Expectations for Individualized Dietary Plans
Participants consistently emphasized the need for dietary plans tailored to their individual symptoms, nutritional status, and comorbidities.
After fasting during this relapse, I lost a lot of weight. I hope a nutritionist can help me design a diet that really suits my situation. (Participant N2)
I already have diabetes, and I’m worried about eating the wrong foods. The recovery diet has its own requirements, so I definitely want a personalized meal plan, like diabetic diets. (Participant N12)
Strong Interest in Digital Dietary Support
Most participants expressed positive attitudes toward digital tools, such as mobile apps or mini-programs, for dietary guidance, nutritional assessment, and remote consultation.
My education level isn’t high, and there are many things I don’t understand. If there were an app that arranged meals based on my nutrition status, like cooking videos, it would be very helpful. (Participant N10)
I use a WeChat mini-program now to check what foods I can eat and when. It’s useful, but it requires payment. I hope there could be a more professional and comprehensive app that gives recommendations based on my real situation. (Participant N13)
If a mobile app could recommend recipes and cooking methods based on my preferences, I wouldn’t get tired of eating the same food so quickly and would be more likely to stick with it. (Participant N15)
Discussion
This qualitative study explored dietary management experiences and educational needs among patients in the recovery phase of pancreatitis from a patient-centered perspective. The findings indicate that although patients generally recognize the importance of dietary control—particularly low-fat intake—their ability to implement and sustain dietary recommendations is constrained by insufficiently specific guidance, limited access to reliable information, psychosocial concerns, and family-related factors. These results highlight critical gaps between dietary recommendations and patients’ real-world self-management practices during recovery.
Inadequate Dietary Understanding and Limitations of Health Beliefs
Participants in this study commonly identified high-fat intake and overeating as important triggers for symptom exacerbation and recurrence—a finding consistent with current evidence regarding the pathophysiology of pancreatitis and dietary risk factors.2,3,16 However, despite this awareness, most participants lacked a clear understanding of what constitutes a “low-fat diet” in practical terms. Their knowledge often remained at a conceptual or principle-based level, making it difficult to translate into concrete daily dietary decisions.
This finding aligns with research in other chronic conditions demonstrating that limited dietary health literacy is a major barrier to effective self-management.17 According to health behavior theories, increasing risk awareness alone is insufficient to sustain long-term behavior change. Continued adherence depends on patients’ understanding of perceived benefits, self-efficacy, and their capacity to manage barriers encountered during daily implementation.18 These findings underscore a critical gap in current patient education models. The principle-based advice provided during hospitalization—such as “eat a low-fat diet”—is insufficient for patients with limited dietary health literacy. Without concrete guidance on what this means in daily practice, patients are left to interpret these principles on their own, often turning to the internet. However, as our findings show, online information is often contradictory and commercialized, leading to confusion rather than clarity. This highlights the need for healthcare providers not only to deliver dietary education but also to assess patients’ health literacy, provide actionable tools (such as food lists and meal plans), and guide patients toward authoritative information sources to discourage reliance on unverified online content. In the present study, several participants expressed strong motivation to restrict fat intake but struggled to operationalize this goal due to the absence of quantitative guidance and practical examples. When dietary education is limited to abstract recommendations such as “low-fat” or “light diet,” patients may find it difficult to apply these concepts within the context of household meal preparation and social eating. These findings underscore the need for dietary education that prioritizes clarity, specificity, and applicability in everyday life.
Barriers to Accessing Reliable Dietary Information Reveal Gaps in Current Education Models
Another prominent finding was the limited availability of reliable and consistent dietary information during the recovery phase. Participants relied primarily on healthcare professionals for dietary guidance during hospitalization; however, such education was typically delivered as brief, principle-based instructions, without detailed meal planning or staged progression. After discharge, many participants turned to online sources, where they encountered fragmented, contradictory, or commercially driven information that increased uncertainty rather than supporting informed decision-making.
These experiences are consistent with previous studies, which indicate that patients with pancreatitis often have unmet information needs and insufficient continuity of dietary education after discharge.12,13 International guidelines emphasize that nutritional support for pancreatitis should be continuous, explicit, and adapted to different recovery stages.9,19,20 Nevertheless, in routine clinical practice, dietary education is often limited to one-time verbal instructions, with few standardized tools or follow-up mechanisms. As a result, patients may struggle to maintain consistency between hospital-based recommendations and home-based self-management.
To address these gaps, future nursing practice should consider the development of structured dietary education systems, including standardized discharge materials, stage-specific dietary charts, sample meal plans, and access to authoritative information platforms. Such approaches may facilitate the translation of dietary knowledge into sustained self-management behaviors and reduce confusion arising from inconsistent information sources.
Dietary Adherence Influenced by Behavioral, Psychological, and Family Factors
The findings also highlight that dietary management during recovery is shaped by multiple interacting factors, including behavioral habits, psychological responses, and family environment. While participants acknowledged the importance of dietary control, many described difficulties maintaining long-term adherence, particularly when family members preferred regular or high-fat foods. The findings also reveal a dialectical tension within the family unit. On the one hand, family members provide essential emotional support and practical assistance, such as preparing meals. On the other hand, their own dietary preferences and habits can inadvertently become a significant barrier to adherence. As participants described, preparing separate meals was often impractical, and family members’ reluctance to adopt a low-fat diet created conflict. This places the patient in a difficult position: they must either isolate themselves by eating different food or compromise their dietary adherence to maintain family harmony. This finding suggests that dietary interventions need to target the family system as a whole—rather than just the individual patient—to align household dietary patterns with the patient’s medical needs. Consistent with previous research, family support emerged as a critical determinant of sustained dietary adherence.21 When household dietary patterns are misaligned with patient needs, adherence becomes more challenging—even among motivated individuals.
In addition, several participants reported heightened anxiety related to eating, especially those with a history of relapse. Fear of recurrence led to persistent vigilance and emotional distress during meals, which negatively affected their eating experience and confidence in dietary decision-making. Prior studies suggest that while knowledge may initiate behavior change, sustained adherence is more strongly influenced by self-efficacy, emotional regulation, and perceived social support.22,23
These findings indicate that dietary management interventions should not focus solely on nutritional knowledge but also incorporate skills training, emotional support, and family involvement. Addressing psychological distress and strengthening family-level support may help patients achieve more stable and sustainable dietary behaviors during recovery.
Growing Demand for Individualized and Digital Dietary Support
Beyond challenges related to knowledge and behavior, participants expressed a strong preference for individualized dietary guidance—tailored to their symptoms, nutritional status, and comorbidities. Personalized dietary plans were viewed as more relevant and achievable than generic recommendations. This preference reflects a broader trend in patient-centered care, where individualized approaches are increasingly recognized as essential for improving adherence and engagement.
Notably, most participants demonstrated strong interest in digital health tools, such as mobile applications and mini-programs, to support dietary management. Digital platforms were perceived as convenient, accessible, and capable of providing real-time guidance, nutritional assessment, and professional feedback. This enthusiasm for digital tools can be understood through the lens of the Technology Acceptance Model (TAM), which posits that perceived usefulness and perceived ease of use are primary drivers of technology adoption.24 For patients in this study, the perceived usefulness of apps lay in their potential to provide concrete meal plans and reduce uncertainty about what to eat. The perceived ease of use was enhanced by the familiarity of platforms like WeChat, which many patients already used in daily life. However, barriers also emerged—such as cost (as mentioned by participant N13) and concerns about the reliability of information—suggesting that future interventions must address both acceptance factors and practical barriers to ensure sustained engagement. Previous studies have shown that mobile health interventions can improve dietary quality, self-management behaviors, and patient engagement through integrated mechanisms of monitoring, feedback, and professional interaction.25–27 In chronic disease management, digital nursing interventions have also demonstrated promising outcomes by enabling continuous support beyond traditional clinical encounters.28
These findings suggest that digital tools may serve as effective complements to conventional dietary education by extending support into patients’ daily lives. Future interventions could explore the development of integrated dietary management models incorporating baseline assessment, individualized dietary prescriptions, digital tracking, professional feedback, and early warning of recurrence risk. By leveraging patient data and intelligent algorithms, such systems may enhance precision, convenience, and continuity in dietary self-management during the recovery phase of pancreatitis.
Implications for Nursing Practice
Overall, this study demonstrates that although patients in the recovery phase of pancreatitis recognize the importance of dietary control, significant barriers remain: understanding low-fat dietary standards, accessing reliable information, and sustaining adherence over time. Current dietary education practices are often principle-based, insufficiently targeted, and lacking in continuous support, limiting their effectiveness in real-world self-management.
Clinical nurses play a pivotal role in addressing these gaps. Nursing-led interventions should emphasize structured, staged, and individualized dietary education, actively involve family members, and integrate digital health tools to support continuous follow-up. By adopting a multi-level approach that addresses cognitive, behavioral, emotional, and contextual factors, nursing practice may enhance patients’ dietary self-management capacity, improve adherence to low-fat diets, reduce recurrence risk, and ultimately improve long-term outcomes and quality of life.
Limitations
This study has several limitations. First, as a qualitative study conducted in a single tertiary hospital in Chongqing, China, the findings may reflect local cultural and healthcare contexts and may not be directly transferable to other settings. Second, while we achieved data saturation with 15 participants, the sample was self-selecting and may not represent the experiences of all patients in the recovery phase, particularly those with lower health literacy or those living alone without family support. Third, despite efforts to bracket preconceptions through reflexive journaling, the interpretation of data remains susceptible to researcher bias inherent in phenomenological inquiry. Future quantitative or mixed-methods research is needed to validate and generalize these findings across broader populations.
Conclusion
This study provides patient-centered insights into dietary management during the recovery phase of pancreatitis. The findings reveal that while patients recognize the importance of dietary control, they face significant barriers: confusion about what “low-fat” means in practice (Theme 1), limited access to reliable information (Theme 2), challenges in long-term adherence due to family dynamics and anxiety (Theme 3), and a strong desire for personalized and digital support (Theme 4). In response to these specific needs, nursing practice should move beyond principle-based, one-time education. Interventions must provide structured, stage-specific dietary plans with clear food lists and meal examples to address patients’ confusion; actively involve family members to mitigate household-level barriers; and integrate digital tools to enable the continuous follow-up and authoritative guidance that patients currently lack. By directly targeting the gaps identified in this study, such comprehensive approaches may enhance patients’ dietary self-management capacity and ultimately reduce the risk of disease recurrence.
Ethical Approval
This study was approved by the Ethics Committee of Chongqing Fuling Hospital, School of Medicine, Chongqing University (Approval No. 2025CDFSFLYYEC-29). Written informed consent was obtained from all participants prior to data collection. All procedures were conducted in accordance with the Declaration of Helsinki. Privacy and confidentiality were ensured through anonymization of transcripts, secure data storage, and restricted access to study materials.
Acknowledgments
The authors sincerely thank all participants for sharing their valuable experiences and perspectives, which greatly contributed to the success of this study. The authors also express their gratitude to the clinical and administrative staff of Chongqing Fuling Hospital for their assistance in participant recruitment and support during data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Voronina S, Chvanov M, De Faveri F, et al. Autophagy, acute pancreatitis and the metamorphoses of a trypsinogen-activating organelle. Cells. 2022;11(16):2565. doi:10.3390/cells11162565
2. Trikudanathan G, Yazici C, Evans Phillips A, Forsmark CE. Diagnosis and management of acute pancreatitis. Gastroenterology. 2024;167(4):673–10. doi:10.1053/j.gastro.2024.02.052
3. Sun Y, Jin J, Zhu A, et al. Risk factors for recurrent pancreatitis after first episode of acute pancreatitis. Int J Gen Med. 2022;15:1319–1328. doi:10.2147/IJGM.S348860
4. Xiao AY, Tan ML, Wu LM, et al. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol. 2016;1(1):45–55. doi:10.1016/S2468-1253(16)30004-8
5. Mao X, Huang C, Wang Y, et al. Association between dietary habits and pancreatitis among individuals of European ancestry: a two-sample Mendelian randomization study. Nutrients. 2023;15(5):1043. doi:10.3390/nu15051043
6. Zhou C, Geng J, Huang H, et al. Adherence to the Mediterranean diet is associated with reduced chronic pancreatitis risk: a longitudinal cohort study. Food Funct. 2024;15(22):11072–11082. doi:10.1039/d4fo03547a
7. Becker U, Timmermann A, Ekholm O, et al. Alcohol drinking patterns and risk of developing acute and chronic pancreatitis. Alcohol Alcohol. 2023;58(4):357–365. doi:10.1093/alcalc/agad012
8. Dugum M, Gougol A, Paragomi P, et al. Association of dietary habits with severity of acute pancreatitis. Curr Dev Nutr. 2018;2(12):nzy075. doi:10.1093/cdn/nzy075
9. Arvanitakis M, Ockenga J, Bezmarevic M, et al. ESPEN practical guideline on clinical nutrition in acute and chronic pancreatitis. Clin Nutr. 2024;43(2):395–412. doi:10.1016/j.clnu.2023.12.021
10. Li MY, Zhang Q, Li J, Zengin G. Food and medicine homology in cancer treatment: traditional thoughts collide with scientific evidence. Food Med Homol. 2025;2(3):9420120. doi:10.26599/FMH.2025.9420120
11. Xu X, Ding L, Chen T, et al. Efficacy and safety of intensive triglyceride-lowering therapy on reducing recurrence of hypertriglyceridemia-associated pancreatitis (REDUCE): protocol for a multicentre, randomised controlled trial. BMJ Open. 2025;15(7):e093011. doi:10.1136/bmjopen-2024-093011
12. Su X, Ma S, Yang X, et al. Health literacy needs of acute pancreatitis patients during the diagnosis and treatment process under the lens of the Timing It Right theory: a qualitative study. Patient Prefer Adherence. 2024;18:507–517. doi:10.2147/PPA.S447389
13. Zhang X, Guo Y, Dang X, et al. Self-management challenges among young and middle-aged patients with recurrent acute pancreatitis: a qualitative study. Chin J Mod Nurs. 2024;30(6):743–748. doi:10.3760/cma.j.cn115682-20231008-02314
14. Song S, Liu Z, Wang Y, Gong B. Human organoids and their application in tumor models, disease modeling, and tissue engineering. Med Bull. 2025;1:17–36. doi:10.1002/mdb2.70001
15. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
16. Wang YX, Ge P, Chen HL. Induction of hyperlipidemic pancreatitis by different fatty acids: a narrative review. World J Gastroenterol. 2025;31(22):106575. doi:10.3748/wjg.v31.i22.106575
17. Lambert K. Designing dietary education materials for people with chronic kidney disease: recommendations for improving the quality of resources. J Ren Nutr. 2023;33(1):208–213. doi:10.1053/j.jrn.2022.07.003
18. Yang S, Zhang F, Zhu R, et al. Effects of a multidisciplinary intervention based on an integrated theory of health behavior change on medication adherence in patients with gastrointestinal stromal tumors. Chin J Pract Nurs. 2024;40(33):2561–2569. doi:10.3760/cma.j.cn211501-20240109-00076
19. National Institute for Health and Care Excellence (NICE). Pancreatitis: diagnosis and management. London: NICE; 2018 [updated 2024]. (NICE Guideline, NG104). Available from: https://www.nice.org.uk/guidance/ng104.
20. Crockett SD, Wani S, Gardner TB, et al. American Gastroenterological Association Institute guideline on initial management of acute pancreatitis. Gastroenterology. 2018;154(4):1096–1101. doi:10.1053/j.gastro.2018.01.032
21. Pamungkas RA, Chamroonsawasdi K, Vatanasomboon P. Family support integrated with diabetes self-management among uncontrolled type 2 diabetes mellitus patients: a systematic review. Behav Sci. 2017;7(3):62. doi:10.3390/bs7030062
22. Glick AA, Winham DM, Heer MM, Shelley MC, Hutchins AM. Health belief model predicts likelihood of eating nutrient-rich foods among US adults. Nutrients. 2024;16(14):2335. doi:10.3390/nu16142335
23. Chen J, Tian Y, Yin M, et al. Relationship between self-efficacy and adherence to self-management and medication among patients with chronic diseases in China: a multicentre cross-sectional study. J Psychosom Res. 2023;164:111105. doi:10.1016/j.jpsychores.2022.111105
24. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989;13(3):319–340. doi:10.2307/249008
25. Scarry A, Rice J, O’Connor EM, et al. Usage of mobile applications or mobile health technology to improve diet quality in adults: a systematic review. Nutrients. 2022;14(12):2459. doi:10.3390/nu14122459
26. Keum J, Chung MJ, Kim Y, et al. Usefulness of smartphone apps for improving nutritional status of pancreatic cancer patients: randomized controlled trial. JMIR mHealth uHealth. 2021;9(8):e21088. doi:10.2196/21088
27. Han CY, Lim SL, Ong KW, Johal J, Gulyani A. Behavioral lifestyle intervention program using mobile application improves diet quality in adults with prediabetes (D’LITE study): a randomized controlled trial. J Acad Nutr Diet. 2024;124(3):358–371. doi:10.1016/j.jand.2023.10.005
28. Xu Y, Huang H, Cao Q, et al. Scope of application of electronic health interventions in Chronic disease management: a scoping review. J Nurs Sci. 2022;36(23):96–101. doi:10.3870/j.issn.1001-4152.2022.23.096
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Expectations and Experiences of a Group of Patients Enrolled in an Educational Program for Rheumatoid Arthritis at a Specialized Care Center in Colombia
Castiblanco-Montañez RA, Buitrago-Garcia D, Arévalo Velandia A, Garzón-Cepeda JD, Rodríguez-Florido F, Sánchez Vanegas G, Santos-Moreno P
Journal of Multidisciplinary Healthcare 2023, 16:483-492
Published Date: 22 February 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Exploring Information Needs and Perspectives on a Patient Decision Aid for Biologic Therapy: A Qualitative Interview Study Among Individuals with Rheumatoid Arthritis
Rai SK, McCormick N, Yokose C, De Vera MA, Li LC, Choi HK
Patient Preference and Adherence 2026, 20:565490
Published Date: 23 June 2026