Back to Journals » Journal of Pain Research » Volume 15
Evaluation by Survival Analysis of Cold Pain Tolerance in Patients with Fibromyalgia and Opioid Use
Authors Deng EZ ![]() , Weikel DP, Martucci KT
, Weikel DP, Martucci KT ![]()
Received 1 April 2022
Accepted for publication 17 August 2022
Published 9 September 2022 Volume 2022:15 Pages 2783—2799
DOI https://doi.org/10.2147/JPR.S368805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Eden Z Deng,1– 3 Daniel P Weikel,3 Katherine T Martucci1– 3
1Human Affect and Pain Neuroscience Laboratory, Department of Anesthesiology, Duke University Medical Center, Durham, NC, USA; 2Center for Translational Pain Medicine, Duke University Medical Center, Durham, NC, USA; 3Biostatistics Group, Department of Anesthesiology, Duke University School of Medicine, Durham, NC, USA
Correspondence: Katherine T Martucci, Human Affect and Pain Neuroscience Laboratory, Duke University Medical Center, Durham, NC, 27710, USA, Tel +1 919-613-8023, Fax +1 919-684-2411, Email [email protected]
Purpose: The cold pressor test (CPT) is a clinical pain research method used to measure cold pain tolerance. During this test, participants immerse an extremity (ie, hand or foot) into cold water for as long as tolerable. The duration of the test (traditionally up to an experimentally imposed cut-off at 2 minutes) indicates the amount of cold pain tolerance by the participant. Prior research studies have investigated cold pain tolerance in patients with chronic pain. However, few of these studies have used survival analysis, which allows for proper handling of data censoring and is therefore, an optimal statistical method for CPT data analysis. The goal of the present study was to use survival analysis to evaluate cold pain tolerance in patients with fibromyalgia. Furthermore, we aimed to model relationships between psychological and clinical variables as well as opioid medication use and cold pain tolerance.
Patients and Methods: A total of 85 patients with fibromyalgia (42 who were taking opioids) and 47 healthy pain-free controls provided CPT and questionnaire data (collected across 2 study sites) for a case–control study. We used survival analysis using Cox regression to evaluate group differences (patients vs controls) in cold pain tolerance and to evaluate cold pain tolerance relationships with psychological, clinical, and medication use.
Results: As compared to healthy controls, patients with fibromyalgia exhibited significantly lower CPT survival (HR = 2.17, 95% CI: [1.42, 3.31], p = 0.00035). As indicated by Cox regression models, the significant group difference in CPT survival did not relate to our selected psychological and clinical measures (p > 0.05). The groups of non-opioid-taking patients and healthy controls showed consistent CPT survival across study sites. However, patients taking opioid pain medications showed differences in CPT survival across study sites.
Conclusion: By using survival analysis, an optimal method for time-to-event pain measures such as the CPT, we confirmed previously identified reductions in cold pain tolerance in patients with fibromyalgia. While our selected psychological and clinical measures were not significantly associated with cold pain tolerance, our data suggest that opioid medication use may impart greater cold pain tolerance in some patients.
Keywords: chronic pain, opiate, cold pressor test, hyperalgesia
Plain Language Summary
In clinical settings, cold pain tolerance is often measured using the Cold Pressor Test (CPT). For this test, participants place their hand or foot in cold water for as long as they can tolerate. The CPT is useful for studying chronic pain conditions, such as fibromyalgia, which impacts many individuals worldwide. Even though many researchers have used the CPT, a recent publication pointed out that most published studies using the CPT have used calculations that were not ideal for the data. In this analysis, researchers used survival analysis, a semiparametric method more suitable for CPT data, to study cold pain tolerance in women with fibromyalgia compared to women with no pain conditions. CPT data and psychological measures (for example, depression and anxiety scores) were collected from two separate studies to form a total group of 85 people with fibromyalgia and 47 people with no chronic pain. They reported the below conclusions:
- Similar to prior study results, women with fibromyalgia show lower tolerance to cold pain compared to pain-free women.
- The difference in cold pain tolerance between women with fibromyalgia and pain-free women cannot be entirely explained by differences in the included psychological factors (like anxiety and depression).
- Being prescribed an opioid pain medication for fibromyalgia may have different effects on tolerance to cold pain, depending on the patient. Data for this study were collected from patients who were at 2 different US locations. For the patients who were taking opioids, the group of patients at one of these locations showed greater cold pain tolerance compared to healthy controls, while the other group of patients who were taking opioids (at the other study location) did not. More research is needed to understand what these results mean.
Introduction
Chronic pain is highly prevalent across all demographics, is a major contributor to the current opioid epidemic, and imparts a major burden on society.1 As one method to clinically assess chronic pain, the cold pressor test (CPT) provides a way to measure cold pain tolerance. Broadly, both clinical practice and pain research use the CPT to measure pain tolerance across healthy individuals and chronic pain patient populations.2 While complex and interacting multi-system processes in the body driving chronic pain remain unclear, CPT-measured pain tolerance may provide useful insights into underlying mechanisms (eg, psychological and clinical drivers of pain sensitization) among individual patients and to characterize unique types and stages of chronic pain.
While many prior studies include CPT data, to date, most of these studies have used parametric statistical analysis which for time-to-event data does not involve proper handling of censoring. Censoring implies that not all data points (ie, survival times) are observed, and it must be accounted for during statistical inference.3 Despite censored data being more suitably analyzed by survival analysis, published studies of pain tolerance in patients with chronic pain have rarely used survival analysis methods to analyze CPT data.4 For example, such studies have used CPT data to study pain tolerance in adults with irritable bowel syndrome (IBS),5 to study psychological and genetic predictors of pain tolerance in healthy subjects,6 and to measure opioid-induced hyperalgesia (OIH) in opioid-dependent patients.7 However, these specific studies of pain tolerance represent a notable few involving survival analysis. Meanwhile, regarding pain tolerance in the fibromyalgia patient population, to our knowledge, no studies have reported CPT data as analyzed using survival analysis methods.
CPT data are “censored time-to-event data” which are appropriately analyzed by regression models. Of these models, the Cox proportional-hazards model is the most common. The Cox proportional-hazards model is a semiparametric model that uses a set of time-independent explanatory variables for prediction of risk.8 In the case of pain tolerance data collected using the CPT, the data are analyzed using the hazard function h(t) which represents an individual’s risk of removing their hand from the cold water at some time t. Survival analysis uses the hazard ratio (HR) to assess the individual risk experienced at any given time and provides a quantified value comparing survival probability between two groups.
In both healthy individuals and patients with chronic pain, such as fibromyalgia, pain tolerance may be affected by numerous health and psychological factors. Prior literature indicates that, compared to healthy individuals, patients with fibromyalgia demonstrate less cold pain tolerance.9–11 Differences in cold pain tolerance relate to changes in activity within brain sensorimotor, attentional, and executive control networks, as well as subcortical/brainstem areas,12–15 and such findings suggest that cold pain tolerance is modulated by cognitive and psychological processes. For example, in pain-free individuals and individuals with chronic pain, state anxiety, representing a major psychological factor, relates to greater pain sensitivity.16–19 Additionally, in patients with fibromyalgia, greater clinical pain intensity relates to both greater number of pain areas across the body and increased negative affective states.20 Moreover, pain intensity is related to positive and negative affect21,22 and affect balance.23
In addition to influences by psychological factors, the use of opioid medications may influence levels of pain tolerance. Opioid medication prescribed as long-term treatment for chronic pain poses risks of addiction, overdose, and opioid-induced hyperalgesia (ie, increased pain response when taking opioids).24,25 Concurrent with mechanisms of opioid-induced hyperalgesia, greater sensitivity and lower tolerance to cold stimuli have been observed in patients with opioid dependence7,26 as well as in patients with fibromyalgia.27
The present case–control study aimed to provide an analysis of CPT-evaluated cold pain tolerance in patients with fibromyalgia with enhanced rigor and reliability by using both survival analysis statistical methods. We compared CPT survival and psychological/clinical correlates in patients with fibromyalgia vs a healthy control group. We hypothesized that compared to healthy pain-free controls, patients with fibromyalgia would demonstrate less cold pain tolerance (ie, higher CPT survival hazard). We additionally hypothesized that in patients with fibromyalgia, factors of state anxiety, negative affect, number of pain areas in the body, and opioid use would be related to less pain tolerance. Lastly, we explored additional psychological and clinical factors and their relationship to cold pain tolerance in patients with fibromyalgia.
Material and Methods
Participants
The study included female patient and control participants who each participated in one of the two separate studies during which data were collected. Two different research teams collected data independently at different times and locations. For Study 1 which was conducted at Stanford University, the first research team collected CPT data from 35 patients and 17 controls, who were recruited from the regions surrounding Palo Alto, CA, between 2015 and 2018. Results from analyses of other non-CPT-related data collected from Study 1 have been reported previously.28–30 For Study 2 which was conducted at Duke University, the second research team collected data from 50 patients and 30 controls, who were recruited from the regions surrounding Durham, NC, between 2019 and 2021 (see Table 1 for demographic information).
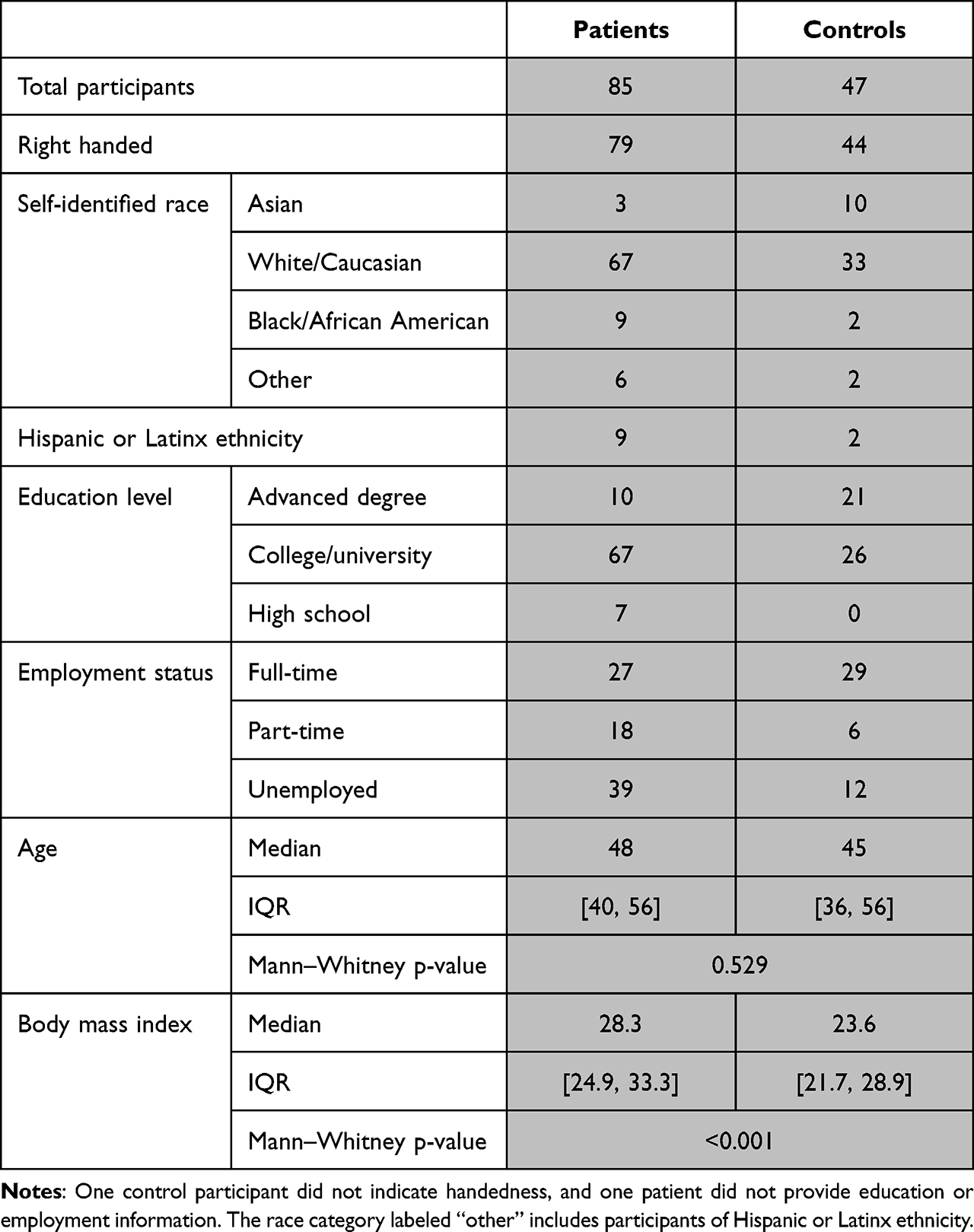 |
Table 1 Participant Demographics |
In Study 1 (Stanford University data collection site), all fibromyalgia patients met the modified American College of Rheumatology (ACR) 2011 criteria for fibromyalgia [widespread pain index (WPI) ≥7 + symptom severity (SS) ≥5, or WPI 3–6 + SS ≥ 9; symptoms present at a similar level for at least 3 months; no disorder that would otherwise explain the pain].31 In Study 2 (Duke University data collection site), fibromyalgia patients met the revised ACR 2016 criteria which includes a slight change in WPI criteria (range 4–6).32 Additional eligibility criteria required all fibromyalgia patients to have pain in all four quadrants of the body, have an average pain score over the past month of at least 2 on a 0–10 verbal scale, have no MRI contraindications, and not be pregnant or nursing. Healthy control eligibility criteria required individuals to have no history of chronic pain, not be pregnant or nursing, have no MRI contraindications, not be taking pain- or mood-altering medications at the time of the study, and have no depression or anxiety disorder. In total, 85 fibromyalgia patients and 47 healthy participants signed written informed consent indicating their willingness to participate in the study, understanding of all study procedures, and acknowledgement that they could withdraw from the study at any time. We conducted all study procedures in accordance with the Declaration of Helsinki, and all study procedures were approved by the Stanford University Institutional Review Board for Study 1 and the Duke University Institutional Review Board for Study 2. We conducted analysis for this study under a data use agreement that was established allowing the data collected at Stanford to be analyzed by the research team at Duke University (K.T.M. was the PI for both Study 1 and Study 2). We pre-registered data analysis plans including hypotheses and exploratory analyses, which were published on the Open Science Framework (OSF) website at: DOI: 10.17605/OSF.IO/H2KGW.
Medication Usage
In addition to the fibromyalgia eligibility criteria (described above), we enrolled patients with fibromyalgia into “opioid-taking” or “non-opioid” groups based on medication use criteria. Out of the 85 total patients with fibromyalgia, 43 patients were enrolled into the “non-opioid” (ie, opioid-naïve) group. The eligibility criteria for the non-opioid group required that the patients had never taken opioids for a period greater than 30 days, had not taken any opioids within the 90 days before study participation, and were not taking opioid medications as part of their pain treatment at the time of their study participation (of the 43 non-opioid patients, 17 patients were from Study 1 and 26 patients were from Study 2). The remaining 42 patients with fibromyalgia (out of the total 85 patients) were using prescribed opioid medications as part of their ongoing pain treatment at the time of the study. For enrollment into the opioid-taking patient group, these 42 patients met eligibility criteria that required them to have been taking opioid medications for at least 90 days prior to the study and at the time of their participation in the study (of the 42 opioid-taking patients, 18 patients were from Study 1 and 24 patients were from Study 2). For the opioid-taking patients, we recorded additional information about opioid medication dosage and duration of use, and all participants continued their medication use as prescribed during their participation in the study (see Table 2).
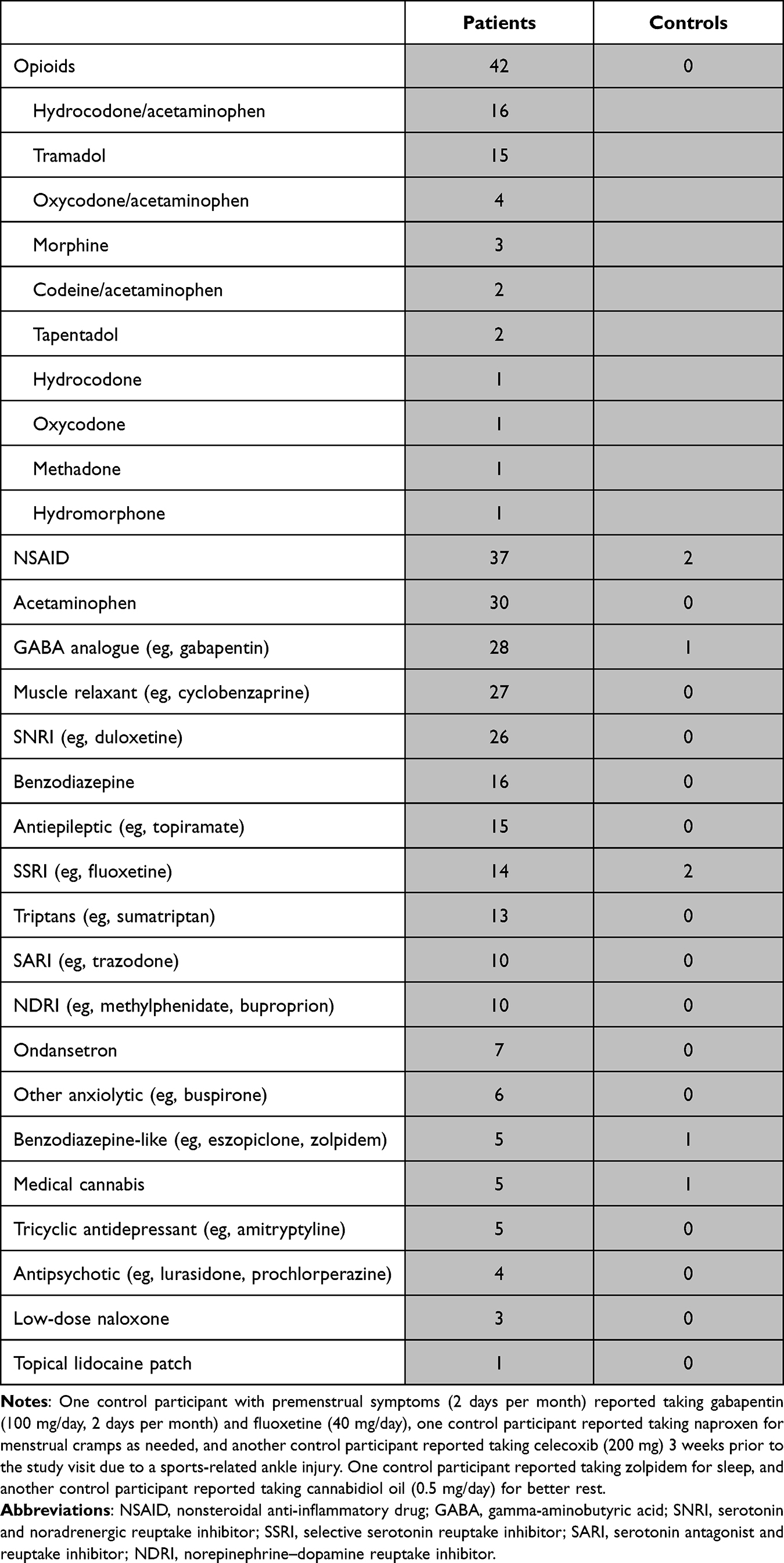 |
Table 2 Medications |
Study Procedures
Sample Size Calculation
We determined the total required sample size of the combined (Study 1 + Study 2) dataset based on the data collected in Study 1. Using the powerSurvEpi package in R, we calculated a sample size for Cox regression based on the hazard ratio (HR) between the fibromyalgia group and the healthy control group in the CPT data from Study 1 (HR = 2.83). To obtain a minimum power of 0.80 at the 0.05 alpha level for a targeted HR of 2.0 in the combined (Study 1 + Study 2) dataset, we determined that the combined dataset should have a minimum healthy control sample size of 39 (expecting 28 uncensored events; ie, time <120 seconds) and a minimum fibromyalgia sample size of 79 (expecting 73 uncensored events). Thus, the final combined study sample used in the analysis contained sufficient counts of healthy control (n = 47) and fibromyalgia (n = 85) participants.
Cold Pressor Test Procedures
We conducted the cold pressor test in different facilities and by different experimenters in Study 1 and Study 2, with slight variations in protocol. In Study 1 (data collection site at Stanford University), we individually tailored the initial temperature of the cold water to each participant’s sensitivity. Specifically, we determined and used the temperature associated with each participant’s pain intensity rating of 3 on a 0–10 visual analog scale (VAS, anchors of “no pain” and “worst pain imaginable”).33 To determine the individually tailored cold water temperatures for each participant, patients and healthy controls each participated in a brief cold water immersion test of the left hand, which lasted up to 30 seconds in duration (5 minute inter-test interval) and was repeated up to 2 times as necessary at different temperatures. The cold water temperature evoking a pain intensity rating of VAS = 3 was used in the subsequent CPT assessment. In Study 2 (data collection site at Duke University), we standardized the temperature of the cold water used in the CPT for all participants to 5°C. Other than the individualized vs standardized temperatures described above, both studies involved the same CPT set up and procedures. To set up the CPT assessment, we filled a large plastic container with ice water, adjusted the temperature, removed any remaining ice, and recorded the final pre-test temperature of the water. Then, participants submerged their right hand in the cold water (with no remaining ice) for as long as tolerable (up to a 2-minute cut-off time to ensure patient safety and validity of the test). The CPT assessment began (and we started a digital timer) when the participant first immersed their hand into the water, and for the test, we allowed the participant to keep her hand in for up to a maximum of 2 minutes. The 2-minute cut-off is typically used in CPT studies to avoid changes in body temperature and other sources of experimental variability that may occur with longer durations of the test.2,4 After the CPT assessment, each participant rated their pain intensity and pain unpleasantness associated with the cold water experience on a 0–10 VAS sliding scale.
Psychological and Clinical Questionnaires
In addition to providing demographic and medication information, all subjects completed the following set of questionnaires: Beck Depression Inventory (BDI),34 Behavioral Inhibition System/Behavioral Approach System (BIS/BAS),35 Positive and Negative Affect Schedule (PANAS),36 Profile of Mood States (POMS),37 State-Trait Anxiety Inventory (STAI-State, STAI-Trait),38 Brief Pain Inventory (BPI),39 Fibromyalgia Assessment Status (FAS),40 and Patient-Reported Outcome Measurement Information System (PROMIS) Fatigue.41
Statistical Analyses
We stored questionnaire data in secure REDCap databases and manually entered (by double data confirmatory entry) CPT data from case report forms into digital spreadsheets prior to analysis. We pre-registered all analyses in the OSF registry (DOI: 10.17605/OSF.IO/H2KGW) and conducted the analyses in R version 3.6.0.
Because the CPT relies on time-to-event data, we fit the data with Cox proportional-hazards models which predict participants’ CPT survival hazard from their group status (patient or control), demographic information, behavioral and psychological measures, and medication information. Prior to analysis, we assessed variables for greater than 5% missingness to determine whether data imputation would be required. We did not impute missing values for variables with less than 5% missingness. All models used in this analysis contained an adjustment variable for starting temperature and a binary variable indicating Study (Study 1 or Study 2) to control for any systematic differences between trials. Nested Cox models were compared using the likelihood ratio test (LRT), and non-nested Cox models were compared using the plrtest function in R (created by Thomas Hielscher) which implements a partial LRT suited for non-nested Cox models.42
We first compared cold pain tolerance between patients (ie, combined opioid-taking and non-opioid patients) and healthy control groups using a Cox model to predict CPT hazard from fibromyalgia group status. To investigate the effect of demographic and psychological/clinical measures on the relationship between fibromyalgia and CPT hazard, we built a multivariate Cox model by selecting up to 4 additional covariates to add to the model (ie, in addition to group status) (Figure 1A). We selected the 4 additional covariates based on preliminary significance with CPT hazard (described below) from an array of a priori identified possible covariates, including age, body mass index (BMI), race (White, Asian, Black, other), BDI score, BAS reward responsiveness, BAS drive, BAS fun-seeking, BIS score, PANAS positive affect, PANAS negative affect, POMS total mood disturbance, STAI state anxiety, and STAI trait anxiety. We first individually modeled the CPT hazard function given by each covariate (including an adjustment variable for starting temperature and a binary variable for Study), and then we selected up to 4 of the most significant variables with coefficient p < 0.2. We tested these variables for high correlation (continuous variables: Pearson r > 0.7, categorical variables: x2 test p < 0.01), and we included in the model only the most significant variable of any group of highly correlated variables.
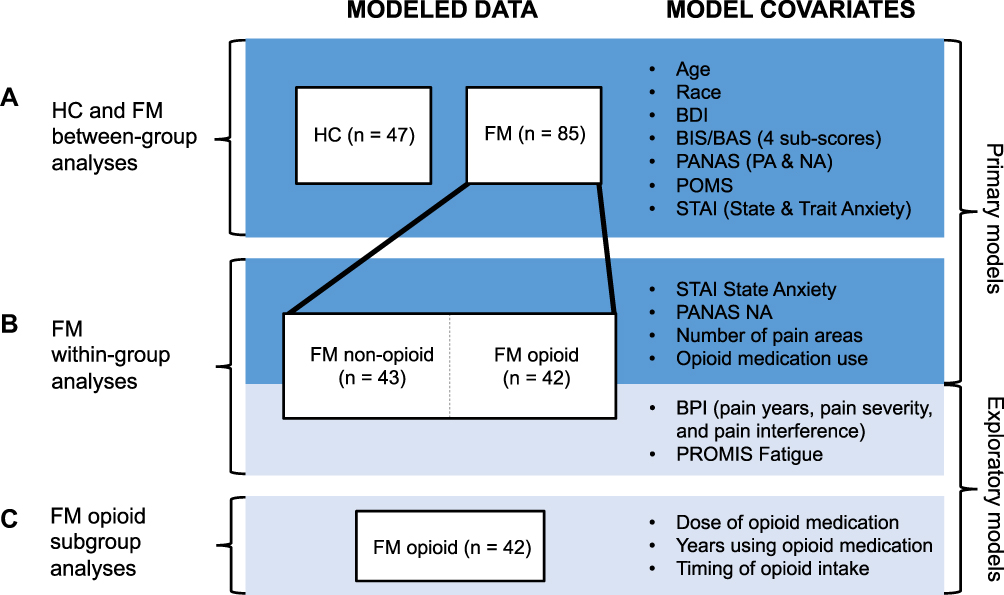 |
Figure 1 Diagram of statistical models. Abbreviations: BDI, Beck Depression Inventory; BIS/BAS, Behavioral Inhibition System/Behavioral Activation System; PANAS, Positive and Negative Affect Schedule; POMS, Profile of Mood States; STAI, State-Trait Anxiety Inventory; BPI, Brief Pain Inventory; PROMIS, Patient-Reported Outcome Measurement Information System. Notes: The primary hypotheses were first tested (A) across all participants [both healthy control (HC) and fibromyalgia (FM) groups] and (B) within the fibromyalgia group. Exploratory tests were then conducted (B) within the fibromyalgia group as well as (C) within the opioid-taking subgroup. All tests were conducted using Cox proportional hazards models. |
We hypothesized that state anxiety, negative affect, number of pain areas in the body, and opioid medication use would be correlated with decreased pain tolerance in patients with fibromyalgia. To test these hypotheses within the patient group, we modeled CPT hazard with each of STAI state anxiety, PANAS negative affect, FAS pain areas, and a binary variable indicating opioid medication use (Figure 1B).
Due to the non-normality of the data, we used the Mann–Whitney U-test to conduct all group comparisons of the psychological/clinical variables. We confirmed proportional hazards for all models using the cox.zph function in R, and we identified observations with deviance residuals greater than 2.5 or less than −2.5 as possible outliers.
Exploratory Analyses
To validate the multivariate model and address the possibility of correlated groups of covariates in the model, we also used Lasso regression to identify variables predictive of CPT hazard. The Lasso approach tends to select one predictor out of a group of correlated predictors and discard the rest, and it can be more accurate than stepwise selection.43`
In addition to state anxiety, negative affect, number of body areas with pain, and opioid medication use, we also explored other factors potentially predictive of CPT survival within the patient group using Cox models. These exploratory variables included the covariates tested in the primary analysis as well as patients’ number of years with pain (BPI), average pain intensity (BPI), average pain interference (BPI), and PROMIS Fatigue score (Figure 1B). Because the study (ie, data collection site) effect on CPT survival was significant, we also separately analyzed Study 1 and Study 2 to evaluate CPT relationships with clinical/psychological variables. Additionally, compared to Study 1 we observed a stronger relationship between opioid medication use and CPT survival in Study 2. We sought to determine the factors that might account for this between-study difference. We hypothesized that such factors might include opioid dosage, duration of opioid use, or timing of last intake (ie, the opioid half-life range during which the CPT test was performed, calculated based on the time of the last opioid dose and the drug-specific half-life). Given this, we conducted a sub-analysis of the opioid-taking fibromyalgia group by testing for study differences in these three additional factors (opioid dose, opioid duration, and opioid intake timing), and we tested these factors as separate predictors of CPT survival (Figure 1C). Lastly, we conducted a post-hoc sensitivity analysis of opioid medication effects by re-evaluating the primary results on the dataset including only non-opioid-taking patients and healthy controls.
Results
Participant Demographics and Medication Use
We analyzed data from a total of 85 patients and 47 controls (see Table 1 for demographic information). Forty-three out of the 85 fibromyalgia participants were not taking opioid medications and were taking over-the-counter pain medications. The remaining 49% (n = 42) of the fibromyalgia patients were taking opioid pain medications. The opioid-taking sub-group had a median daily morphine equivalent dose (MED) of 20 mg morphine and a median opioid-taking duration of 5 years. Of the patients with fibromyalgia, 59% (n = 50) were taking anti-depressants, 26% (n = 22) were taking benzodiazepines or benzodiazepine-like medications, and 56% (n = 48) were taking muscle relaxants or anti-seizure medications. The number of patient and healthy control participants (from both Study 1 and Study 2) taking each medication type is shown in Table 2.
Psychological and Clinical Measures
Less than 5% of the questionnaire responses were missing from the data (Supplementary Figure 1). Among the patient group, participants reported number of body areas (FAS) with pain ranged from 3 (the minimum criteria) to 19 (maximum). The median pain severity was 5.8/10 and median pain interference was 6.4/10 (BPI). The patient vs healthy control groups showed significant differences in CPT time, STAI trait anxiety, STAI state anxiety, PANAS positive affect, PANAS negative affect, BAS fun-seeking, BIS score, POMS total mood disturbance, and BDI score (Table 3).
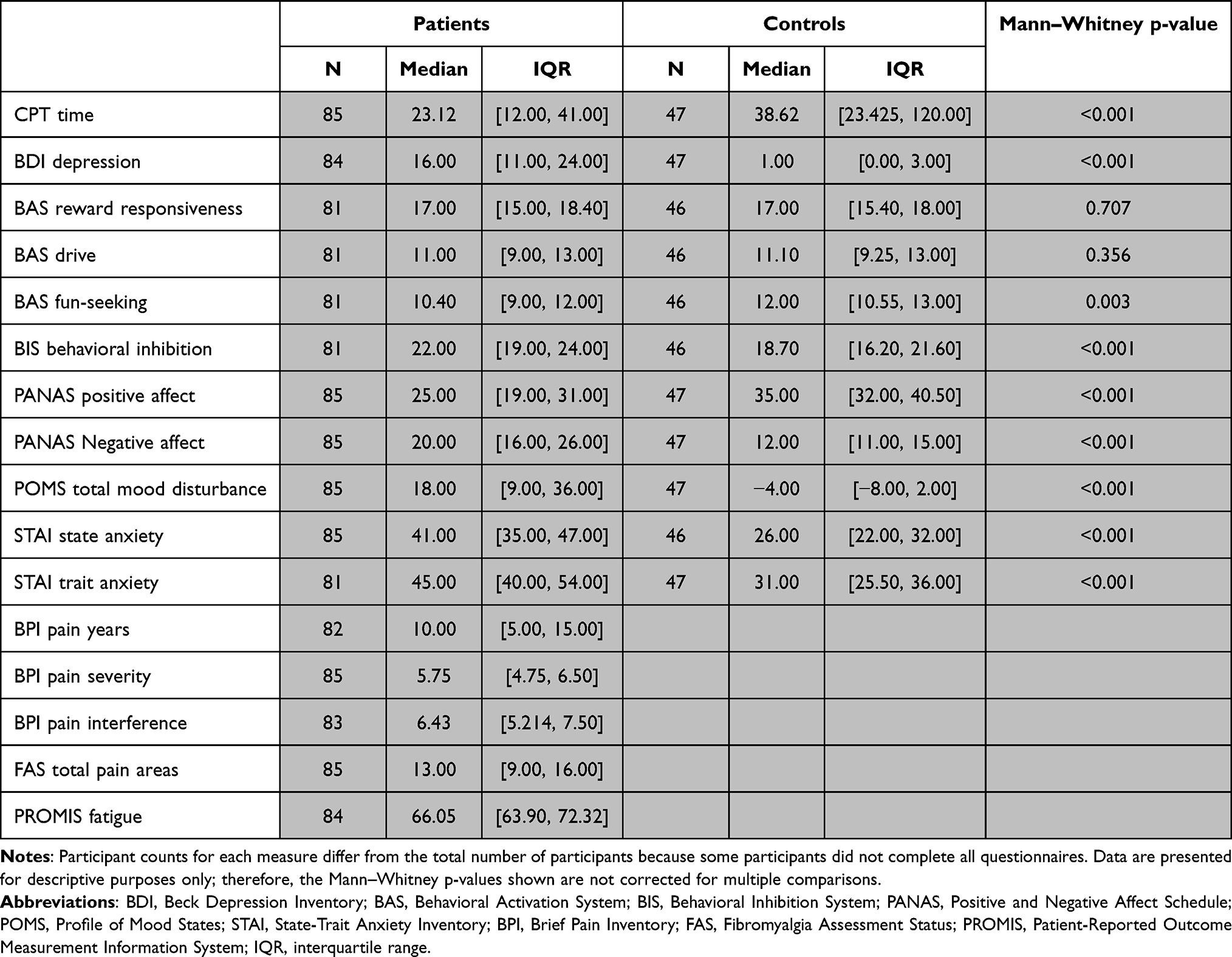 |
Table 3 Clinical and Psychological Measures Between Groups |
Group Comparison of CPT Survival
The distributions of CPT time by group are shown in Figure 2 (Mann–Whitney p = 0.00080). When including adjustment variables for Study 1 vs Study 2 and CPT starting temperature, patients with fibromyalgia had significantly lower CPT survival probability compared to controls (HR = 2.17, 95% CI [1.42, 3.31], p = 0.00035) (Figure 3). The starting temperature of the CPT was not significantly different across studies (Mann–Whitney = 0.39, median = 5.0°C, IQR = [4.7, 5.2]).
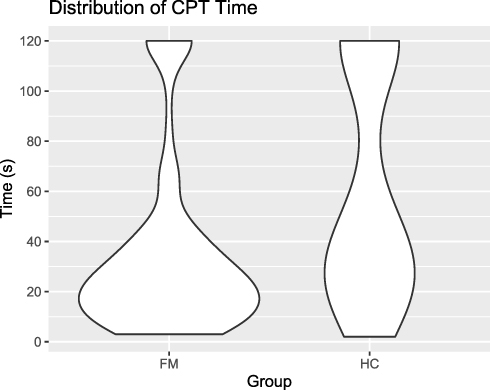 |
Figure 2 Distribution of CPT time by group. Notes: Distributions of raw CPT times from the fibromyalgia (FM) and healthy control (HC) groups are shown. The control group contained a larger proportion of censored times (CPT cut-off at 120 seconds) compared to the fibromyalgia group. |
 |
Figure 3 Kaplan–Meier curves of CPT assessment results by group. Notes: Kaplan–Meier curves with 95% confidence intervals show the difference in CPT survival probability over time between the fibromyalgia (FM) group and healthy control (HC) group. The p-value shown is for the group effect in the Cox regression model of CPT survival time with adjustments for starting temperature and study effect. Time-to-event data was censored at 120 seconds, and proportional hazards criteria were met for Cox regression. |
Regarding study-specific effects, between the fibromyalgia participants in Study 1 vs Study 2, CPT time was significantly different (p = 0.00079). Overall, the patients in Study 2 demonstrated a higher proportion of censored CPT times (16%) compared to the patients in Study 1 (3%). In contrast, healthy controls showed no significant differences in CPT time between studies. The proportion of censored times in Study 1 and Study 2 were 29% and 33%, respectively.
Results from the single-variable Cox models of CPT hazard, which each included a psychological/clinical variable, showed that none were significantly associated with CPT survival (p > 0.05) after accounting for starting temperature, study differences, and group status. However, both variables of Study 1 and fibromyalgia group status were significantly associated with greater hazard in each of these models. The multivariate Cox model included the variable for patient group status (HR = 1.99, p = 0.0020), selected variables which included BAS fun-seeking (HR = 0.94, p = 0.28), BAS drive (HR = 0.97, p = 0.50), and “other” race (HR = 1.78, p = 0.15), as well as an indicator variable for Study 2 and an adjustment variable for starting temperature (exact, measured before the CPT assessment). High collinearity was not detected between any covariates. The multivariate model did not improve the fit for the CPT data compared to the simpler model with no psychological predictors (LRT: p = 0.16).
Variable selection with Lasso regression revealed similar results: the binary variables for patient group status (HR = 1.71, p = 0.048) and Study 2 (HR = 0.61, p = 0.017) were significant covariates selected by Lasso (10-fold cross-validation using Harrell’s C-index, and coefficients were extracted at the value of ƛ giving the minimum mean cross-validation error). The Lasso model also selected BAS fun-seeking, BIS score, “other” race, and STAI state anxiety, but these were not significant predictors of CPT survival. The Lasso-selected Cox model was neither a significant improvement upon the p-value-selected multivariate Cox model (partial LRT: p = 0.82) nor upon the original simple Cox model with no psychological/clinical predictors (LRT: p = 0.23).
Psychological and Clinical Predictors of CPT Survival in Fibromyalgia Patients
Within the patient group, STAI state anxiety, PANAS negative affect, number of pain areas, and opioid medication use were all not significantly associated with CPT survival probability (p > 0.0125). Other exploratory variables, including BAS fun-seeking (HR = 0.86, p = 0.014) and BAS drive (HR = 0.89, p = 0.021), indicated trends for stronger relationships (ie, larger effect sizes, but note these were not corrected for multiple comparisons) with CPT survival in fibromyalgia patients (but not in healthy controls). We report Cox regression statistics within the fibromyalgia patient group (n = 85) for covariates selected for a priori tests (opioid medication use, PANAS negative affect, number of pain areas, and STAI state anxiety) as well as exploratory covariates (BAS fun-seeking and BAS drive) in Table 4 and Supplementary Table S1.
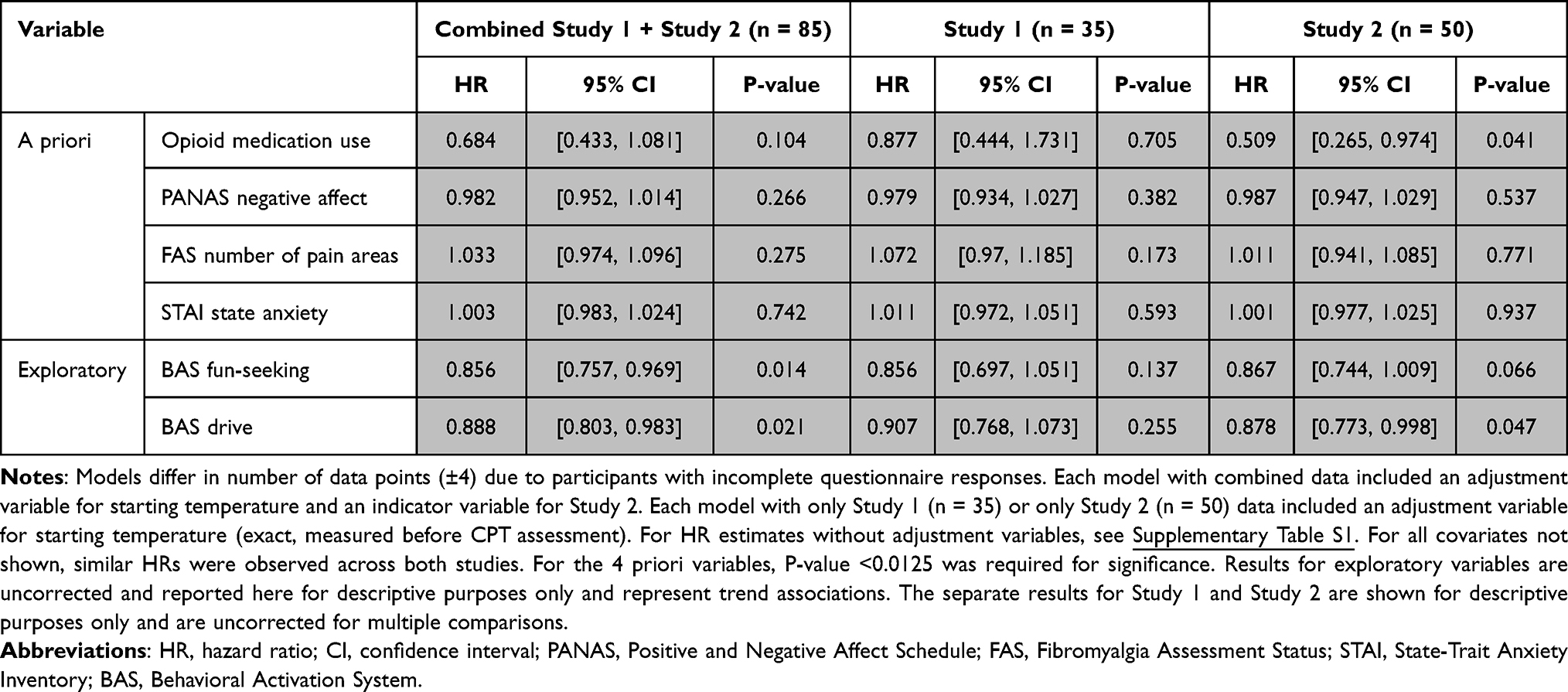 |
Table 4 CPT Covariates in Patients: Cox Regression HRs and P-values Stratified by Study |
The CPT survival rate in Study 2 patients was greater compared to Study 1 patients (HR = 0.48, 95% CI [0.30, 0.77], p = 0.0026) even when accounting for CPT starting temperature [Note: This study difference in CPT survival was absent in the healthy control group (HR = 0.83, p = 0.62)]. Because we observed significant between-study CPT differences in the patient group, the effects of covariates on CPT survival are also reported by the study in Table 4. No demographic, psychological, or clinical variables were significant predictors of CPT survival in the patient group of either study after correction for multiple comparisons, and most variables showed consistent effects (direction and magnitude) between studies. The use of opioid medication was associated with greater CPT survival in Study 2 (HR = 0.51, 95% CI [0.27, 0.97], p = 0.041) but not in Study 1 (HR = 0.88, p = 0.71), and no interaction effect was detected between study and opioid medication use (p = 0.26).
Between-Study Variability in the Opioid-Taking Patient Subgroup
As noted above, the data showed a positive trend (non-significant) between opioid medication use and CPT survival among fibromyalgia patients in Study 2 (Table 4). The direction of this effect was independent of any demographic, psychological, or clinical differences between the opioid-taking patients of Study 2 and their non-opioid-taking counterparts (Supplementary Table S2); for instance, the positive trend between opioid medication use and CPT survival was preserved even when analyses were stratified by age group or patients’ number of years with pain.
CPT times did not differ significantly between studies for the subgroup of patients with fibromyalgia who were not taking opioids (p = 0.11) nor for the healthy control group (p = 0.52). However, in the subgroup analysis of opioid-taking patients, these patients demonstrated significantly different CPT times in Study 1 vs Study 2 (p = 0.0028). Meanwhile, neither the duration of opioid medication use (p = 0.97), nor the daily opioid dose (p = 0.96), nor the distribution of intake timing (x2 test p = 0.091) significantly differed between studies (Table 5). The demographic, psychological, and clinical profiles of the opioid-taking subgroups were also consistent between studies.
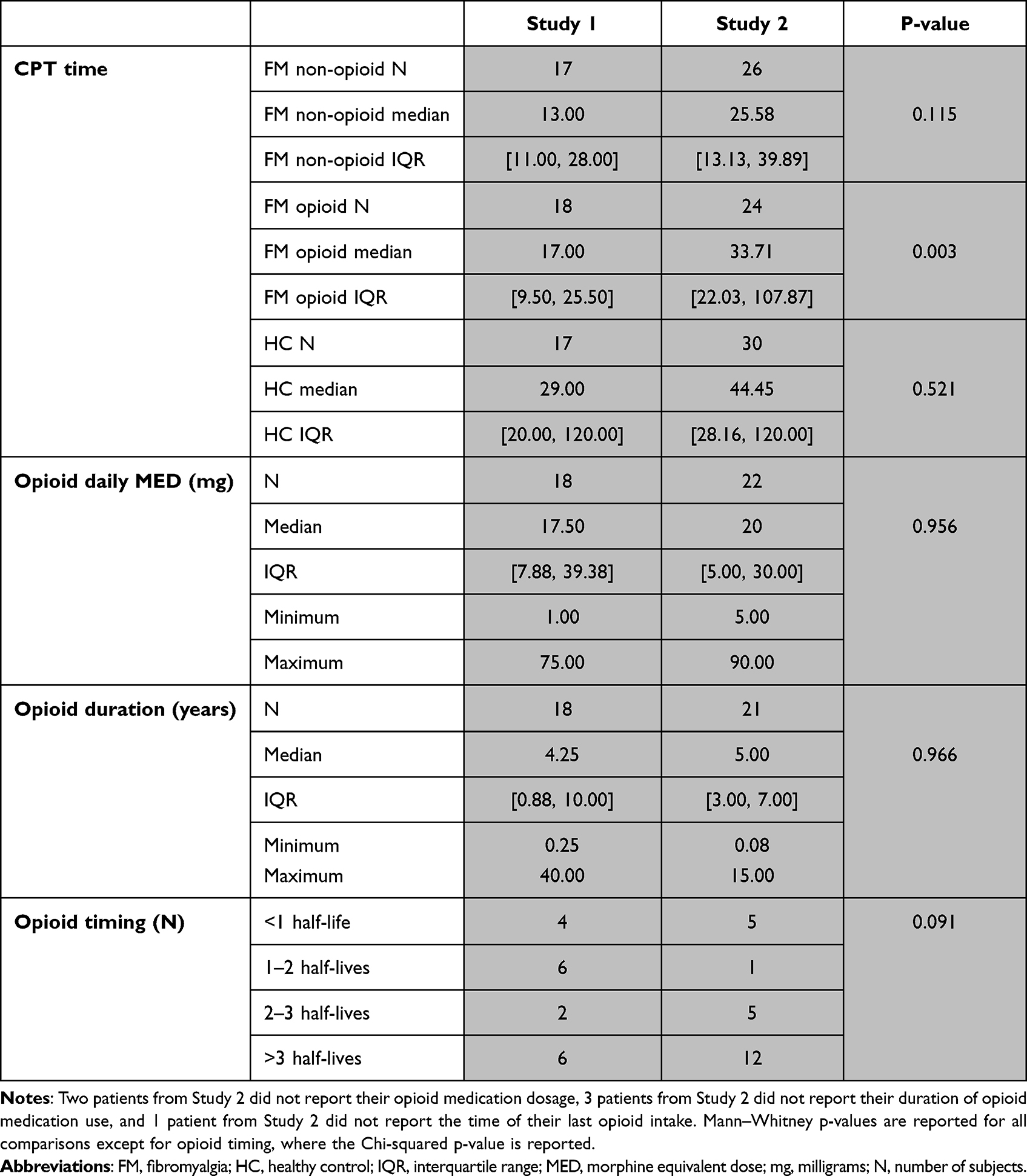 |
Table 5 Comparison of CPT Time and Opioid Dose, Duration, and Timing Across Studies |
Post-Hoc Sensitivity Analysis of Opioid Medication Relationships
When assessing study differences in CPT survival within each group/subgroup separately, Study 2 showed a stronger association with higher CPT survival probability in opioid-taking patients (HR = 0.40, p = 0.013) compared to non-opioid patients (HR = 0.60, p = 0.12) and healthy controls (HR = 0.83, p = 0.62). Due to this additional between-study variation present in the subgroup of opioid-taking patients compared to the rest of the sample (Figure 4), we conducted a separate analysis with the opioid-taking subgroup removed in order to identify any changes in the group and study effects on CPT survival. In Table 6 and Supplementary Table S3, we report the Cox regression statistics for group effect for all fibromyalgia patients (n = 85) vs healthy controls (n = 47) (top row, also refer to Figure 3), and for comparison to non-opioid-taking fibromyalgia patients (n = 43) vs healthy controls (bottom row). After removing the opioid-taking subgroup, the group effect between the non-opioid patient subgroup with healthy controls increased (HR = 2.70, p = 0.000054), and the Cox model indicated that the study effect was no longer significant (HR = 0.67, p = 0.11).
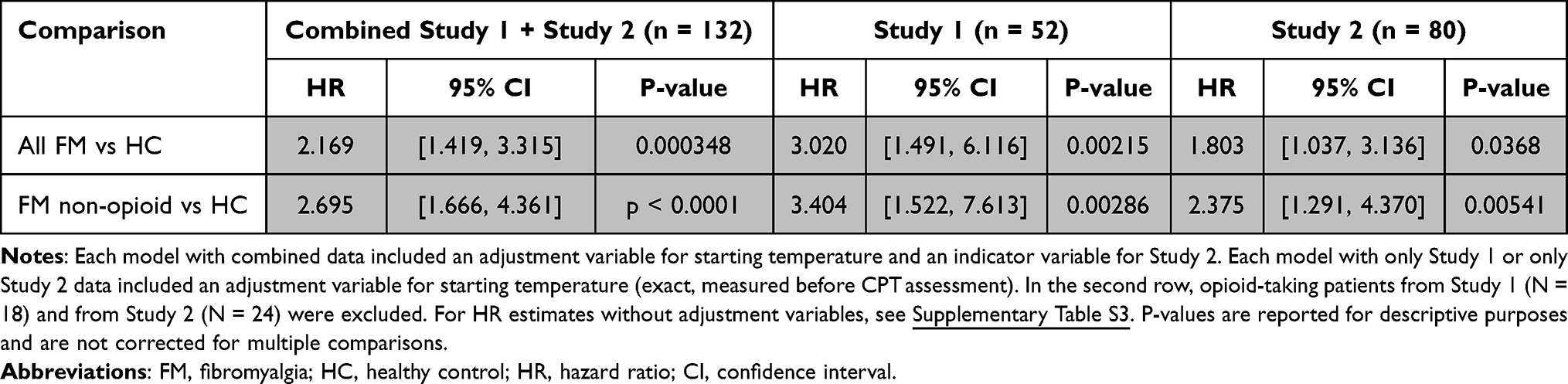 |
Table 6 Group Effect HRs from Sensitivity Analysis |
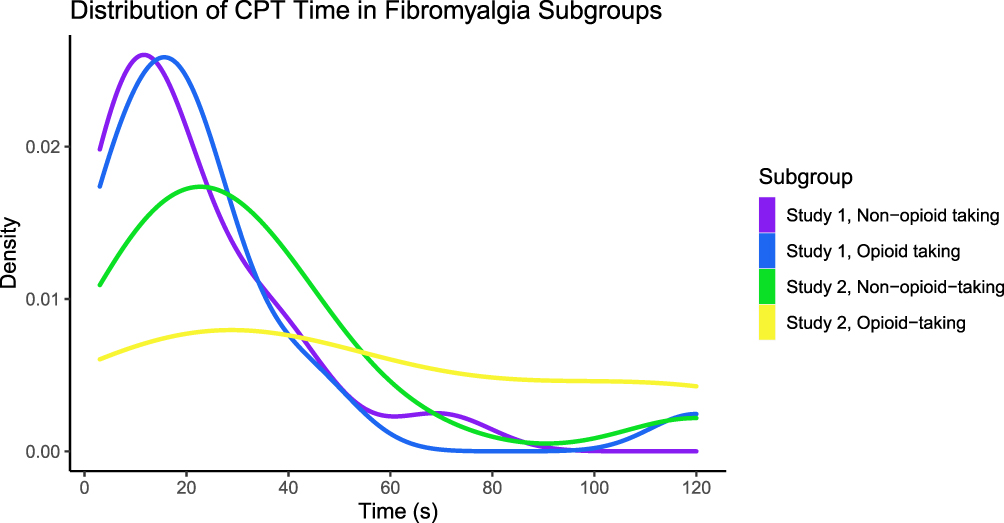 |
Figure 4 Distributions of patient CPT times by study and opioid medication use. Notes: CPT times of fibromyalgia patients in Study 1 and Study 2 are shown by subgroups (opioid-taking vs non-opioid-taking). The distribution of CPT times for opioid-taking patients in Study 2 is shown to be more uniform compared to the right-skewed distributions of CPT times in all other fibromyalgia subgroups. |
Discussion
To our knowledge, we present the first survival analysis and Cox regression modeling of CPT data in patients with fibromyalgia vs healthy controls. Our study analyzed data across combined datasets and evaluated cold pain tolerance differences in patients with fibromyalgia who take opioids vs those who do not take opioids. We conducted this analysis to respond to the need to re-evaluate the statistical methods used in clinical pain tolerance research.4 Most previous analyses of CPT data have used parametric methods to form conclusions about cold pain tolerance. However, such approaches do not account for censored data (eg, CPT time), which are almost always not normally distributed and cannot be effectively normalized with data transformations.4 By considering survival probability instead of time, survival analysis allows us to conduct inference with the censored data points despite not having observed their true values. Furthermore, multivariate methods (as opposed to single-variable comparisons) are needed to more accurately model the complex, interacting processes involved in pain tolerance. In this study, we analyzed CPT data with the Cox proportional-hazards model, a semiparametric model which is widely used in various disciplines to analyze right-censored, time-to-event data with covariates. By comparing patients with fibromyalgia vs healthy controls, we observed group differences in cold pain tolerance which were significant. While the effects of psychological and clinical variables appeared limited, among patients with fibromyalgia who take opioids, our data suggest that opioid medication use may influence cold pain tolerance for a proportion of patients.
Reduced CPT Survival in Fibromyalgia and Potential Contributors
In alignment with previous pain tolerance data in patients with fibromyalgia,9–11 our data demonstrate that patients with fibromyalgia have lower rates of survival in the CPT assessment. Under both p-value-based and Lasso regression variable selection methods, fibromyalgia status was the most significant predictor of CPT survival probability even when accounting for psychological measures including anxiety, depression, and negative affect. This suggests that fibromyalgia may impair cold pain tolerance in ways beyond such psychological processes alone; for example, cold pain tolerance may be altered in conjunction with underlying neurobiological mechanisms. In this study, we did not evaluate neuropathic measures of chronic pain that may be potentially related to pain tolerance. Meanwhile, it is important to note that pain sensitivity in fibromyalgia may be attributed to biological alterations spanning both peripheral and central nervous systems.44,45 Among different patients, fibromyalgia can be characterized by varying amounts of peripheral nociceptor pathologies46,47 and central alterations such as altered descending control of pain and central sensitization.48,49 The sensation of cold pain, specifically, is mediated by transient receptor potential melastatin 8 (TRPM8), and alterations to this receptor may account for cold hyperalgesia in a variety of chronic pain conditions, including fibromyalgia.50,51 Nerve fiber diameter, collected via skin biopsy, has also been shown to be reduced in some fibromyalgia patients.52 In future studies of cold pain tolerance, measures of neuropathic pain should be collected in both patients and healthy controls to complement data collected via questionnaires.
CPT Survival, Behavioral Activation System, and Reward Response
Overall, we did not observe clear relationships between CPT survival and the psychological and clinical questionnaire data collected. However, some relationships became more distinct when we performed survival analyses separately for fibromyalgia or healthy control groups. For instance, higher scores in BAS drive and BAS fun-seeking were slightly predictive of higher CPT survival among fibromyalgia patients, but not among healthy individuals. These results suggest that the psychological contributors to pain tolerance may differ between fibromyalgia patients and healthy individuals. For example, pain tolerance in fibromyalgia patients, compared to healthy controls, may be more susceptible to individuals’ intrinsic drive to achieve goals (ie, BAS drive), and/or willingness to engage in unknown but possibly rewarding activities (ie, BAS fun-seeking). Previous research has proposed the BIS-BAS model of chronic pain, suggesting that pain responses can be predicted by individual perceptions of reward and punishment.53 Furthermore, prior neuroimaging research in patients with fibromyalgia has demonstrated that BAS drive is related to differences in regional brain response to anticipation of rewards28 and avoidance of punishment.30 Thus, alterations in recruited CNS activities ongoing during the CPT assessment may contribute to the observed differences in CPT survival between healthy controls and patients with fibromyalgia.
Opioid Medication and CPT Survival
CPT survival times were significantly longer in opioid-taking patients compared to non-opioid-taking patients in one cohort of patients (Study 2), but not both. Furthermore, there was no evidence to suggest that these differences could be explained by patients’ daily dose of opioid medication, duration of opioid medication use, or the timing of their last opioid intake. Meanwhile, in line with CPT survival relationships with BAS measures as described above, it is possible that changes in reward response in patients with fibromyalgia who take opioids30 may relate to increased cold pain tolerance. Nonetheless, the observed inconsistencies across studies suggest that the relationship between opioid medication use and cold pain tolerance in fibromyalgia patients is tenuous, in that it may vary across patient cohorts and requires further investigation. Prior research has shown that individuals (with and without chronic pain) taking opioids demonstrate lower cold pain tolerance when measured prior to a scheduled opioid dose.54 In another study, compared to non-opioid patients, opioid-taking patients with chronic pain had similar cold pain tolerance when measured within several hours after their morning analgesic dose.55 The timing of opioid dose prior to CPT was variable in the present analysis, therefore, timing effects of opioids are unclear, yet given such prior evidence, opioid timing may be an important variable in assessing cold pain tolerance. Additionally, other studies in individuals with opioid use disorder (ie, opioid-addicted individuals without noted presence of chronic pain) have shown decreased opioid tolerance (by survival analysis) when individuals were tested at a time when opioids (eg, heroin and methadone) were present in their system.56 Together, these prior research findings suggest potential differences in opioid effects on cold pain tolerance in patients with vs without chronic pain.
Study Limitations
In this analysis, we combined two separate CPT studies to maximize statistical power. However, differences between the two studies significantly affected survival rates in the CPT. As compared to Study 1 which used individually tailored starting temperature, Study 2, in which the testing temperature was standardized to 5°C, was associated with lower CPT hazard when accounting for group status (ie, patient vs healthy control). Although the group effect was the most salient predictor of CPT survival in both studies (when each study was analyzed separately), the study effect in the combined analysis was nearly as notable as the group effect. Such significant differences in CPT survival between studies suggest limitations regarding the generalizability of CPT findings across different geographic/demographic cohorts and indicate that slight differences in CPT procedures (ie, starting water temperature) may influence the generalizability of results across studies.
Aside from our a priori modeled factors of opioid medication use, PANAS negative affect, number of pain areas, and STAI state anxiety, the within-group analyses for CPT survival relationships with clinical/psychological factors were exploratory and, as such, can only suggest trend relationships that may be relevant for future investigation. Additionally, we did not collect information on participants’ vital signs (eg, blood pressure) which may be related to differences in pain perception.57 Lastly, as described above, for patients who take opioids, timing of opioid intake prior to the CPT assessment was not controlled in these studies, yet opioid intake timing may be an important variable to consider in future investigations of opioid effects on cold pain tolerance.
Conclusion
By using survival analysis to analyze time-to-event CPT data, we confirm previous findings that, compared to healthy individuals without chronic pain, individuals with fibromyalgia demonstrate less tolerance to cold pain as evoked by hand immersion into cold water. To further understand cold pain tolerance relationships to clinical/psychological factors in individuals with fibromyalgia, future investigations should include measures to evaluate the presence of peripheral neuropathy and compare, in the same patients, results from the CPT and other tests of CNS-related pain processing function. Furthermore, as suggested by our results, some fibromyalgia patients who take opioid medications may be associated with greater cold pain tolerance as compared to patients who do not take opioids. In patients with fibromyalgia, cold pain tolerance may be related to differences in reward response and motivation, to regionally influenced variables such as prescribing practices and local geographic climate, and to timing of opioid intake. As such, to delineate contributions of these and other variables as well as effects of opioids on cold pain tolerance, future investigations using appropriate survival analysis methods of CPT data need to be conducted to study the intersecting realms of chronic pain and opioid use.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, K.T.M., upon reasonable request.
Acknowledgments
We thank Erin Perrine, Christina Cojocaru, and Elizabeth Cha for their assistance with recruitment, data collection, data organization, and analysis for Study 1. We thank Lindsie Boerger, Meghna Nanda, and Drs Anne Baker and Su Hyoun Park for their assistance with recruitment, data collection, and data organization for Study 2. Special thanks to Dr Sean Mackey, Stanford University for resources supporting Study 1 data collection. Lastly, we thank all the study participants for their time and contribution to advance clinical research and knowledge.
Author Contributions
All authors made a significant contribution to the work reported, whether that is the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. All authors took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
For this study, the authors received funding from the National Institutes of Health via K99/R00 DA040154 (KTM) and from the Redlich Pain Research Endowment (Dr Sean Mackey, Stanford University).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships, other than the described funding sources, that could be construed as a potential conflict of interest.
References
1. Sicras-Mainar A, Rejas J, Navarro R, et al. Treating patients with fibromyalgia in primary care settings under routine medical practice: a claim database cost and burden of illness study. Arthritis Res Ther. 2009;11(2):R54. doi:10.1186/ar2673
2. Modir JG, Wallace MS. Human experimental pain models 2: the cold pressor model. Methods Mol Biol. 2010;617:165–168. doi:10.1007/978-1-60327-323-7_13
3. Schober P, Vetter TR. Survival analysis and interpretation of time-to-event data: the tortoise and the hare. Anesth Analg. 2018;127(3):792–798. doi:10.1213/ANE.0000000000003653
4. Treister R, Nielsen CS, Stubhaug A, et al. Experimental comparison of parametric versus nonparametric analyses of data from the cold pressor test. J Pain. 2015;16(6):537–548. doi:10.1016/j.jpain.2015.03.001
5. Stabell N, Stubhaug A, Flægstad T, Nielsen CS. Increased pain sensitivity among adults reporting irritable bowel syndrome symptoms in a large population-based study. Pain. 2013;154(3):385–392. doi:10.1016/j.pain.2012.11.012
6. Patanwala AE, Norwood C, Steiner H, et al. Psychological and genetic predictors of pain tolerance. Clin Transl Sci. 2019;12(2):189–195. doi:10.1111/cts.12605
7. Krishnan S, Salter A, Sullivan T, Gentgall M, White J, Rolan P. Comparison of pain models to detect opioid-induced hyperalgesia. J Pain Res. 2012;5:99–106. doi:10.2147/JPR.S27738
8. Cox DR. Regression models and life-tables. Journal of the Royal Statistical Society: Series B (Methodological). 1972;34(2):187–220. doi:10.1111/j.2517-6161.1972.tb00899.x
9. Brusselmans G, Nogueira H, De Schamphelaere E, Devulder J, Crombez G. Skin temperature during cold pressor test in fibromyalgia: an evaluation of the autonomic nervous system? Acta Anaesthesiol Belg. 2015;66(1):19–27.
10. Gormsen L, Bach FW, Rosenberg R, Jensen TS. Differential pain modulation in patients with peripheral neuropathic pain and fibromyalgia. Scand J Pain. 2012;3(3):116–123. doi:10.1016/j.sjpain.2012.01.002
11. Reyes del paso GA, Garrido S, Pulgar Á, Duschek S. Autonomic cardiovascular control and responses to experimental pain stimulation in fibromyalgia syndrome. J Psychosom Res. 2011;70(2):125–134. doi:10.1016/j.jpsychores.2010.09.012
12. Moont R, Crispel Y, Lev R, Pud D, Yarnitsky D. Temporal changes in cortical activation during conditioned pain modulation (CPM), a LORETA study. Pain. 2011;152(7):1469–1477. doi:10.1016/j.pain.2011.01.036
13. Nahman-Averbuch H, Martucci KT, Granovsky Y, Weissman-Fogel I, Yarnitsky D, Coghill RC. Distinct brain mechanisms support spatial vs temporal filtering of nociceptive information. Pain. 2014;155(12):2491–2501. doi:10.1016/j.pain.2014.07.008
14. Bogdanov VB, Viganò A, Noirhomme Q, et al. Cerebral responses and role of the prefrontal cortex in conditioned pain modulation: an fMRI study in healthy subjects. Behav Brain Res. 2015;281:187–198. doi:10.1016/j.bbr.2014.11.028
15. Jarrahi B, Martucci KT, Nilakantan AS, Mackey S. Cold water pressor test differentially modulates functional network connectivity in fibromyalgia patients compared with healthy controls. Conf Proc IEEE Eng Med Biol Soc. 2018;2018:578–582. doi:10.1109/EMBC.2018.8512350
16. Cimpean A, David D. The mechanisms of pain tolerance and pain-related anxiety in acute pain. Health Psychol Open. 2019;6(2):2. doi:10.1177/2055102919865161
17. Lauriola M, Tomai M, Palma R, et al. Intolerance of uncertainty and anxiety-related dispositions predict pain during upper endoscopy. Front Psychol. 2019;10. doi:10.3389/fpsyg.2019.01112
18. Tang J, Gibson SJ. A psychophysical evaluation of the relationship between trait anxiety, pain perception, and induced state anxiety. J Pain. 2005;6(9):612–619. doi:10.1016/j.jpain.2005.03.009
19. Zeidan F, Gordon NS, Merchant J, Goolkasian P. The effects of brief mindfulness meditation training on experimentally induced pain. J Pain. 2010;11(3):199–209. doi:10.1016/j.jpain.2009.07.015
20. Staud R, Price DD, Robinson ME, Vierck CJ. Body pain area and pain-related negative affect predict clinical pain intensity in patients with fibromyalgia. J Pain. 2004;5(6):338–343. doi:10.1016/j.jpain.2004.05.007
21. Finan PH, Garland EL. The role of positive affect in pain and its treatment. Clin J Pain. 2015;31(2):177–187. doi:10.1097/AJP.0000000000000092
22. Thong ISK, Tan G, Jensen MP. The buffering role of positive affect on the association between pain intensity and pain related outcomes. Scand J Pain. 2017;14(1):91–97. doi:10.1016/j.sjpain.2016.09.008
23. Sibille KT, Kindler LL, Glover TL, Staud R, Riley JL, Fillingim RB. Affect balance style, experimental pain sensitivity, and pain-related responses. Clin J Pain. 2012;28(5):410–417. doi:10.1097/AJP.0b013e3182324799
24. Crofford LJ. Adverse effects of chronic opioid therapy for chronic musculoskeletal pain. Nat Rev Rheumatol. 2010;6(4):191–197. doi:10.1038/nrrheum.2010.24
25. Volkow ND, McLellan AT, Longo DL. Opioid abuse in chronic pain–Misconceptions and mitigation strategies. N Engl J Med. 2016;374(13):1253–1263. doi:10.1056/NEJMra1507771
26. Doverty M, White JM, Somogyi AA, Bochner F, Ali R, Ling W. Hyperalgesic responses in methadone maintenance patients. Pain. 2001;90(1–2):91–96. doi:10.1016/s0304-3959(00)00391-2
27. Jackson D, Singh S, Zhang-James Y, Faraone S, Johnson B. The effects of low dose naltrexone on opioid induced hyperalgesia and fibromyalgia. Front Psychiatry. 2021;12:593842. doi:10.3389/fpsyt.2021.593842
28. Martucci KT, Borg N, MacNiven KH, Knutson B, Mackey SC. Altered prefrontal correlates of monetary anticipation and outcome in chronic pain. Pain. 2018;159(8):1494–1507. doi:10.1097/j.pain.0000000000001232
29. Martucci KT, Weber KA, Mackey SC. Altered cervical spinal cord resting-state activity in fibromyalgia. Arthritis Rheumatol. 2019;71(3):441–450. doi:10.1002/art.40746
30. Martucci KT, MacNiven KH, Borg N, Knutson B, Mackey SC. Apparent effects of opioid use on neural responses to reward in chronic pain. Sci Rep. 2019;9(1):9633. doi:10.1038/s41598-019-45961-y
31. Wolfe F, Clauw DJ, Fitzcharles MA, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR preliminary diagnostic criteria for fibromyalgia. J Rheumatol. 2011;38(6):1113–1122. doi:10.3899/jrheum.100594
32. Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319–329. doi:10.1016/j.semarthrit.2016.08.012
33. Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45–56. doi:10.1016/0304-3959(83)90126-4
34. Beck AT, Steer RA, Carbin MG. Psychometric properties of the beck depression inventory: twenty-five years of evaluation. Clin Psychol Rev. 1988;8(1):77–100. doi:10.1016/0272-7358(88)90050-5
35. Carver CS, White TL. Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: the BIS/BAS scales. J Pers Soc Psychol. 1994;67(2):319–333. doi:10.1037/0022-3514.67.2.319
36. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063–1070. doi:10.1037//0022-3514.54.6.1063
37. McNair DM, Lorr M, Droppleman LF. Manual for the Profile of Mood States. San Diego, CA: Education and Industrial Testing Service; 1971.
38. Spielberger CD, Gorsuch RL, Lushene RE. Manual for the State-Trait Anxiety Inventory; 1970.
39. Keller S, Bann CM, Dodd SL, Schein J, Mendoza TR, Cleeland CS. Validity of the brief pain inventory for use in documenting the outcomes of patients with noncancer pain. Clin J Pain. 2004;20(5):309–318. doi:10.1097/00002508-200409000-00005
40. Salaffi F, Sarzi-Puttini P, Girolimetti R, Gasparini S, Atzeni F, Grassi W. Development and validation of the self-administered fibromyalgia assessment status: a disease-specific composite measure for evaluating treatment effect. Arthritis Res Ther. 2009;11(4):R125. doi:10.1186/ar2792
41. Cella D, Riley W, Stone A, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J Clin Epidemiol. 2010;63(11):1179–1194. doi:10.1016/j.jclinepi.2010.04.011
42. Fine JP. Comparing nonnested cox models. Biometrika. 2002;89(3):635–647. doi:10.1093/biomet/89.3.635
43. Tibshirani R. The lasso method for variable selection in the Cox model. Stat Med. 1997;16(4):385–395. doi:10.1002/(sici)1097-0258(19970228)16:4<385::aid-sim380>3.0.co;2-3
44. Sluka KA, Clauw DJ. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience. 2016;338:114–129. doi:10.1016/j.neuroscience.2016.06.006
45. Martucci KT, Mackey SC. Neuroimaging of pain: human evidence and clinical relevance of central nervous system processes and modulation. Anesthesiology. 2018;128(6):1241–1254. doi:10.1097/ALN.0000000000002137
46. Oaklander AL, Herzog ZD, Downs H, Klein MM. Objective evidence that small-fiber polyneuropathy underlies some illnesses currently labeled as fibromyalgia. Pain. 2013;154(11):2310–2316. doi:10.1016/j.pain.2013.06.001
47. van de Donk T, van Velzen M, Dahan A, Niesters M. Cornea nerve fibre state determines analgesic response to tapentadol in fibromyalgia patients without effective endogenous pain modulation. Eur J Pain. 2019;23(9):1586–1595. doi:10.1002/ejp.1435
48. Potvin S, Marchand S. Pain facilitation and pain inhibition during conditioned pain modulation in fibromyalgia and in healthy controls. Pain. 2016;157(8):1704–1710. doi:10.1097/j.pain.0000000000000573
49. Bosma RL, Mojarad EA, Leung L, Pukall C, Staud R, Stroman PW. FMRI of spinal and supra-spinal correlates of temporal pain summation in fibromyalgia patients. Hum Brain Mapp. 2016;37(4):1349–1360. doi:10.1002/hbm.23106
50. Xing H, Chen M, Ling J, Tan W, Gu JG. TRPM8 mechanism of cold allodynia after chronic nerve injury. J Neurosci. 2007;27(50):13680–13690. doi:10.1523/JNEUROSCI.2203-07.2007
51. MacDonald DI, Wood JN, Emery EC. Molecular mechanisms of cold pain. Neurobiol Pain. 2020;7:100044. doi:10.1016/j.ynpai.2020.100044
52. Doppler K, Rittner HL, Deckart M, Sommer C. Reduced dermal nerve fiber diameter in skin biopsies of patients with fibromyalgia. Pain. 2015;156(11):2319–2325. doi:10.1097/j.pain.0000000000000285
53. Jensen MP, Ehde DM, Day MA. The behavioral activation and inhibition systems: implications for understanding and treating chronic pain. J Pain. 2016;17(5):
54. Hay JL, White JM, Bochner F, Somogyi AA, Semple TJ, Rounsefell B. Hyperalgesia in opioid-managed chronic pain and opioid-dependent patients. J Pain. 2009;10(3):316–322. doi:10.1016/j.jpain.2008.10.003
55. Ram KC, Eisenberg E, Haddad M, Pud D. Oral opioid use alters DNIC but not cold pain perception in patients with chronic pain - new perspective of opioid-induced hyperalgesia. Pain. 2008;139(2):431–438. doi:10.1016/j.pain.2008.05.015
56. Pud D, Cohen D, Lawental E, Eisenberg E. Opioids and abnormal pain perception: new evidence from a study of chronic opioid addicts and healthy subjects. Drug Alcohol Depend. 2006;82(3):218–223. doi:10.1016/j.drugalcdep.2005.09.007
57. Ghione S. Hypertension-associated hypalgesia. Evidence in experimental animals and humans, pathophysiological mechanisms, and potential clinical consequences. Hypertension. 1996;28(3):494–504. doi:10.1161/01.hyp.28.3.494
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Hypnotic Analgesia and Transcranial Direct Current Stimulation on Pain Tolerance and Corticospinal Excitability in Individuals with Fibromyalgia: A Cross-Over Randomized Clinical Trial
Schein B, Beltran G, França BR, Sanches PR, Silva DP Jr, Torres IL, Fegni F, Caumo W
Journal of Pain Research 2023, 16:187-203
Published Date: 24 January 2023
Can Myofascial Trigger Points Involve Nociplastic Pain? A Scoping Review on Animal Models
Matuska W, Matuska J, Skorupska E, Siwek M, Herrero P, Santafé MM
Journal of Pain Research 2023, 16:3747-3758
Published Date: 8 November 2023
Differences in Experimental Pain Sensitivity Between Non-African and African American Healthy Individuals and Patients with Painful Chronic Pancreatitis
Phillips AE, Faghih M, Ramsey ML, Han S, Hart PA, Afghani E, Bick BL, Easler JJ, Yadav D, Wilcox CM, Olesen SS, Drewes AM, Singh VK
Journal of Pain Research 2026, 19:562097
Published Date: 25 February 2026