Back to Journals » Journal of Pain Research » Volume 19
Differences in Experimental Pain Sensitivity Between Non-African and African American Healthy Individuals and Patients with Painful Chronic Pancreatitis
Authors Phillips AE ![]() , Faghih M, Ramsey ML, Han S, Hart PA, Afghani E, Bick BL, Easler JJ, Yadav D, Wilcox CM, Olesen SS, Drewes AM, Singh VK
, Faghih M, Ramsey ML, Han S, Hart PA, Afghani E, Bick BL, Easler JJ, Yadav D, Wilcox CM, Olesen SS, Drewes AM, Singh VK
Received 17 September 2025
Accepted for publication 20 January 2026
Published 25 February 2026 Volume 2026:19 562097
DOI https://doi.org/10.2147/JPR.S562097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Anna E Phillips,1,* Mahya Faghih,2,3,* Mitchell L Ramsey,4 Samuel Han,4 Phil A Hart,4 Elham Afghani,2,3 Benjamin L Bick,5 Jeffrey J Easler,6 Dhiraj Yadav,1 C Mel Wilcox,7 Søren Schou Olesen,8,9 Asbjørn M Drewes,8,9 Vikesh K Singh2,3 On behalf of the International Pancreatic Pain Consortium
1Department of Medicine, Division of Gastroenterology, Hepatology, and Nutrition, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA; 2Department of Medicine, Division of Gastroenterology, Johns Hopkins Medical Institutions, Baltimore, MD, USA; 3Pancreatitis Center, Johns Hopkins Medical Institutions, Baltimore, MD, USA; 4Department of Medicine, Division of Gastroenterology, Hepatology, and Nutrition, The Ohio State University Wexner Medical Center, College of Medicine, Columbus, OH, USA; 5Midwest Digestive Health and Nutrition, Des Plaines, IL, USA; 6Department of Medicine, Division of Gastroenterology and Hepatology, Indiana University Medical Center, Indianapolis, IN, USA; 7Digestive Health Institute, Orlando Health, Orlando, FL, USA; 8Department of Gastroenterology and Hepatology, Centre for Pancreatic Diseases and Mech-Sense, Aalborg University Hospital, Aalborg, Denmark; 9Department of Clinical Medicine, Aalborg University Hospital, Aalborg, Denmark
*These authors contributed equally to this work
Correspondence: Vikesh K Singh, Division of Gastroenterology, Pancreatitis Center, Department of Medicine, Johns Hopkins Medical Institutions, Johns Hopkins Hospital, 1830 E. Monument Street, Room 428, Baltimore, MD, 21205, USA, Tel +1-(410) 614-6708 ext 2, Fax +1 (410) 614-7631, Email [email protected]
Introduction: Pancreatic Quantitative Sensory Testing (P-QST) is a neurosensory evaluation used to characterize pancreatic pain. Given racial differences in experimental pain sensitivity, it is crucial to investigate this phenomenon before widespread P-QST adoption. We aimed to study experimental pain sensitivity in African American (AA) vs non-AA individuals with no abdominal pain or known pancreatic disease (controls), and AA controls vs AA participants with chronic pancreatitis (CP).
Methods: In this cross-sectional, multi-center study, race was dichotomized (AA and non-AA) and was self-reported. Participants underwent P-QST testing assessing pressure pain detection threshold (pPDT), pressure tolerance threshold (pPTT), cold pressor endurance (CPE), conditioned pain modulation (CPM), temporal summation (TS), and the Hospital Anxiety and Depression Scale (HADS).
Results: A total of 157 AA and 110 non-AA control participants were tested, as well as 35 AA participants with CP. No differences in P-QST testing were seen between racial groups in control participants. Compared to AA controls, AA participants with CP showed signs of impaired CPM, significantly lower pPTTs and suggestion of lower pPDTs, as well as increased TS scores of the upper abdomen. The lower pPDTs and pPTTs and decreased CPM in AA CP participants compared to AA controls are consistent with findings in other racial groups.
Conclusion: No significant differences in experimental pain results were found between AA and non-AA controls. Alterations in experimental pain sensitivity appear to mainly accompany the CP disease state in the group of AA participants studied.
Keywords: abdominal pain, chronic pancreatitis, African American, hyperalgesia, chronic pain, pain tolerance, pain threshold
Introduction
Quantitative sensory testing is a standardized set of experimental nerve stimulations designed to characterize nociceptive patterns and used in multiple diseases manifesting with chronic pain. Differences in experimental pain sensitivity have been previously reported in African American (AA) individuals, compared to other racial groups.1 Pancreatic Quantitative Sensory Testing (P-QST), a protocol designed for use in pancreatic disease to identify individuals with or without evidence of widespread hyperalgesia (suggesting central sensitization), has been increasingly used in the characterization of pancreatic pain.2–4 However, it is not known whether there are racial differences in the output from the test. This phenomenon is important to investigate prior to the broader dissemination of P-QST in clinical settings.
Chronic pancreatitis (CP) disproportionately affects AA individuals, compared to non-AA populations, in the United States.5,6 Compared to non-AA individuals with CP, AA individuals with CP have a higher frequency of pain as well as more constant and severe pain.7 Racial differences have been reported between AA and other groups in response to both experimental and clinical pain.8,9 However, many prior studies have been small or performed in young, healthy groups, limiting our ability to extrapolate these findings to larger and older age groups.10 Therefore, it is important to evaluate baseline sensory testing differences in AA individuals in an adequately sized and age-diverse group, to be able to apply this information to the future interpretation of sensory testing results in AA individuals with CP.
We hypothesize that there are differences in experimental pain sensitivity between AA and non-AA individuals. The aim of this study is to evaluate the sensory testing parameters of the P-QST protocol—including mechanical pain thresholds (pressure pain detection threshold [pPDT] and pressure pain tolerance threshold [pPTT]), cold pressor endurance (CPE), conditioned pain modulation (CPM), and temporal summation (TS) — in AA individuals without abdominal pain or known pancreas disease, to establish normative values in this specific population, compared to non-AA participants. The pPDT/pPTT measures reflect mechanical pain threshold/tolerance, while the CPM assessment reflects endogenous pain inhibition and TS is thought to reflect a “wind-up” phenomenon that reflects increased pain perception to repeated stimuli, a key mechanism in central sensitization An additional aim of this study is to evaluate these same sensory parameters in AA participants with no abdominal pain or pancreas disease (controls) versus AA participants with CP, to determine experimental pain sensitivity pattern differences between these groups.
Methods
Control Participants
Participants who self-identified their race as Black or AA at a screening interview and via the demographic questionnaire (options: American Indian/Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, Black or African American, White, Unknown or Prefer not to respond) were recruited at four pancreas centers: The University of Pittsburgh Medical Center (Pittsburgh, PA, USA), The Johns Hopkins University Medical Center (Baltimore, MD, USA), Indiana University School of Medicine (Indianapolis, IN, USA), The Ohio State University Wexner Medical Center (Columbus, OH, USA). Institutional Review Board approval was obtained at each of these sites individually (University of Pittsburgh IRB Protocol PRO17060648, Johns Hopkins IRB 00143375, Indiana University School of Medicine IRB 1909843967, Ohio State University Wexner Medical Center IRB 2018H0444). This study is compliant with principles laid out in the Declaration of Helskinki. In addition, a total of 122 non-AA control participants (group who self-identified as one of the other categories on demographic questionnaire) were ascertained from International Pancreatic Pain Consortium (IPPC) studies who were recruited through advertisements and with the AA group.2 The study was registered with Clinicaltrials.gov (NCT03434392). Participants eligible for this study were ≥18 years of age and had no pancreatic disease and no abdominal pain. Participants were excluded from the study if they had abdominal pain more than six times within the past year, had evidence of medical or surgical disease of importance as judged by the investigators of each site, or were known to be pregnant at the time of screening. Recruitment efforts focused on obtaining equal numbers of men and women and equal numbers of younger adults and older adults. When a category was filled for age/sex group, recruitment for additional participants in that group ended. All participants (control and CP) underwent informed consent: a formal consent document was signed by all participants prior to any study activities being performed.
Participants with CP
A total of 35 AA participants with CP were included for evaluation in the sub-study of AA controls versus AA individuals affected with CP. Participants with CP were enrolled at all four centers during the period of control enrollment. Eligible CP participants were ≥ 18 years of age and met Cambridge III or IV criteria on cross-sectional imaging or met definitive M-ANNHEIM criteria for CP.11 CP participants were excluded if they had previously undergone pancreatic surgery or any organ transplantation. They were also excluded if they were affected by another abdominal pain condition that they were unable to distinguish from pancreatic pain. Additionally, CP participants were excluded if they were having an attack of acute pancreatitis at the time of enrollment.
Clinical Pain Assessment
The demographics for each participant, including the participant’s age; race; ethnicity; sex; and history of opioid, antidepressant, and gabapentinoids use, were recorded. The Hospital Anxiety and Depression Scale (HADS) was used to assess anxiety and depression.12,13
P-QST Procedures
All P-QST procedures were performed by trained study personnel, using the same equipment and standardized test sequence.
Static P-QST
The static P-QST included CPE (described below with CPM) and pressure stimulation thresholds that were tested using a pressure algometer with a 1.0 cm2 probe (Algometer Type II, SOMEDIC Electronics, Solna, Sweden). The pPDT and pPTT were obtained on the participant’s dominant side at 5 different sites: C5 (clavicula), T10 back (pancreatic viscerotome), T10 ventral (upper abdominal area – pancreatic viscerotome), L1 (anterior superior iliac crest), and L4 (the quadriceps 15 cm above the patella). The assessment parameter was the pressure at the predefined sensory threshold, measured in kPa. The pPDT and pPPT sums were calculated using the sum of pPDTs and pPTTs across the different stimulation sites (dermatomes). The pPDTs and pPTTs ratios were calculated by dividing mean pressure thresholds in pancreatic (T10 ventral and T10 back) dermatomes by mean pressure thresholds of C5, L1, and L4 dermatomes.
Dynamic P-QST
Assessment included temporal summation and conditional pain modulation (CPM). CPM can be experimentally induced by immersion of the dominant hand in ice-chilled water (2.0±0.3°C) for 120 seconds (the cold pressor test).14 If the pain became intolerable before this point, the participants were allowed to remove their hand from the water. The duration of hand immersion in cold water in seconds was recorded as CPE (a static QST test). The pPTT was measured on the L4 dermatome on the nondominant side before and immediately after the cold pressor test as test stimulus. The CPM capacity was measured as the absolute and relative changes (%) in pPTT before and after the conditioning stimulation.
Repetitive Pinprick Stimulation (Temporal Summation)
Recordings of TS to repetitive pinprick stimulations at the T10 ventral dermatome and dominant forearm (control area) were performed using an 8 mN PinPrick device (Pinprick Stimulatoren, MRC Systems GmbH, Heidelberg, Germany). Pain ratings using a 0–10 NRS were obtained verbally after a single stimulation at each site, followed by ten stimulations repeated at 1-second intervals. The difference between the ratings in the last and the first scores of the ten stimuli was recorded as the TS score.2
Statistics
Data are reported as medians (interquartile ranges [IQRs]) or numbers (%), unless otherwise specified. We compared demographics, clinical characteristics, and P-QST parameters between the AA and non-AA groups using Student´s test, Mann–Whitney test, or Fisher´s exact test as appropriate. The assumption of normality was checked by inspection of QQ-plots. We refrained from multiparameter analyses, as racial subgroups were intentionally well-balanced with respect to age and sex distributions (as well as other clinical characteristics). P-values were adjusted for a false discovery rate of 5% to account for multiple comparisons. In table form, the results of individual P-QST evaluations are shown in gray; results of the indices used in the P-QST algorithm to phenotype study subjects3 are shown in unshaded areas. Mediation analyses were performed to test whether anxiety or depression mediated P-QST findings in CP participants. Mediation was assessed via structural equation modeling with 1,000-sample bootstrapping; results are reported as coefficients with 95% bias-corrected CIs.15 We used Stata 17.0 (College Station, Texas, USA) for all statistical analyses.
Results
In total, 267 control participants were included in the study, of whom 157 (59%) were in the AA group and 110 (41%) in the non-AA group. The majority of non-AA participants self-identified as White. The mean age of participants was 48.0 (range 18–84) years, and 138 (52%) of the included participants were women. The AA and non-AA groups were well balanced with respect to age and sex distributions (Table 1). The prevalence of psychiatric co-morbidities was also similar between the two groups. Only a small fraction of participants received opioids and/or antidepressants.
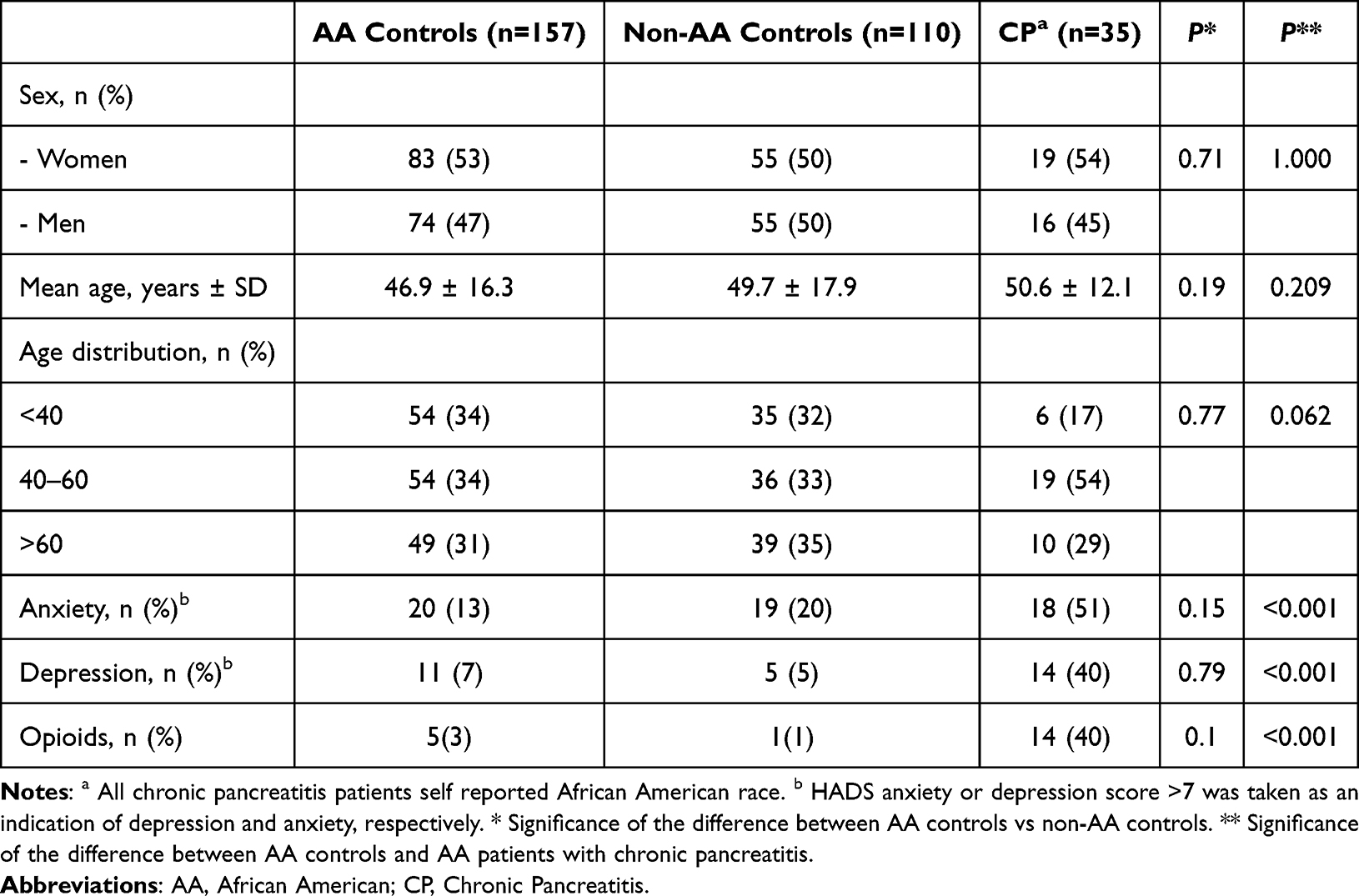 |
Table 1 Demographic and Clinical Characteristics of Control Subgroups and Chronic Pancreatitis (CP) Subgroup |
A total of 35 AA participants with CP were included in the study (female n=19 [54%]). The AA control and CP groups were well balanced with respect to age and sex distributions. However, compared to AA controls, a significantly higher proportion of the participants with CP had symptoms of anxiety (51% vs 13%), depression (40% vs 7%), and opioid use (40% vs 3%) (all p < 0.001).
P-QST Parameters in AA vs Non-AA Controls
No differences were seen between racial groups in any of the P-QST indices for either static or dynamic P-QST tests (unshaded areas of Table 2). Several statistically significant differences were seen in individual thresholds measured (greyed areas of Table 2), including the PPDTs at the abdomen and the L1 dermatome, as well as PPTTs at the T10 dermatome in both the abdominal and dorsal positions. No clear trend of higher or lower thresholds however was detected in AA versus non-AA controls.
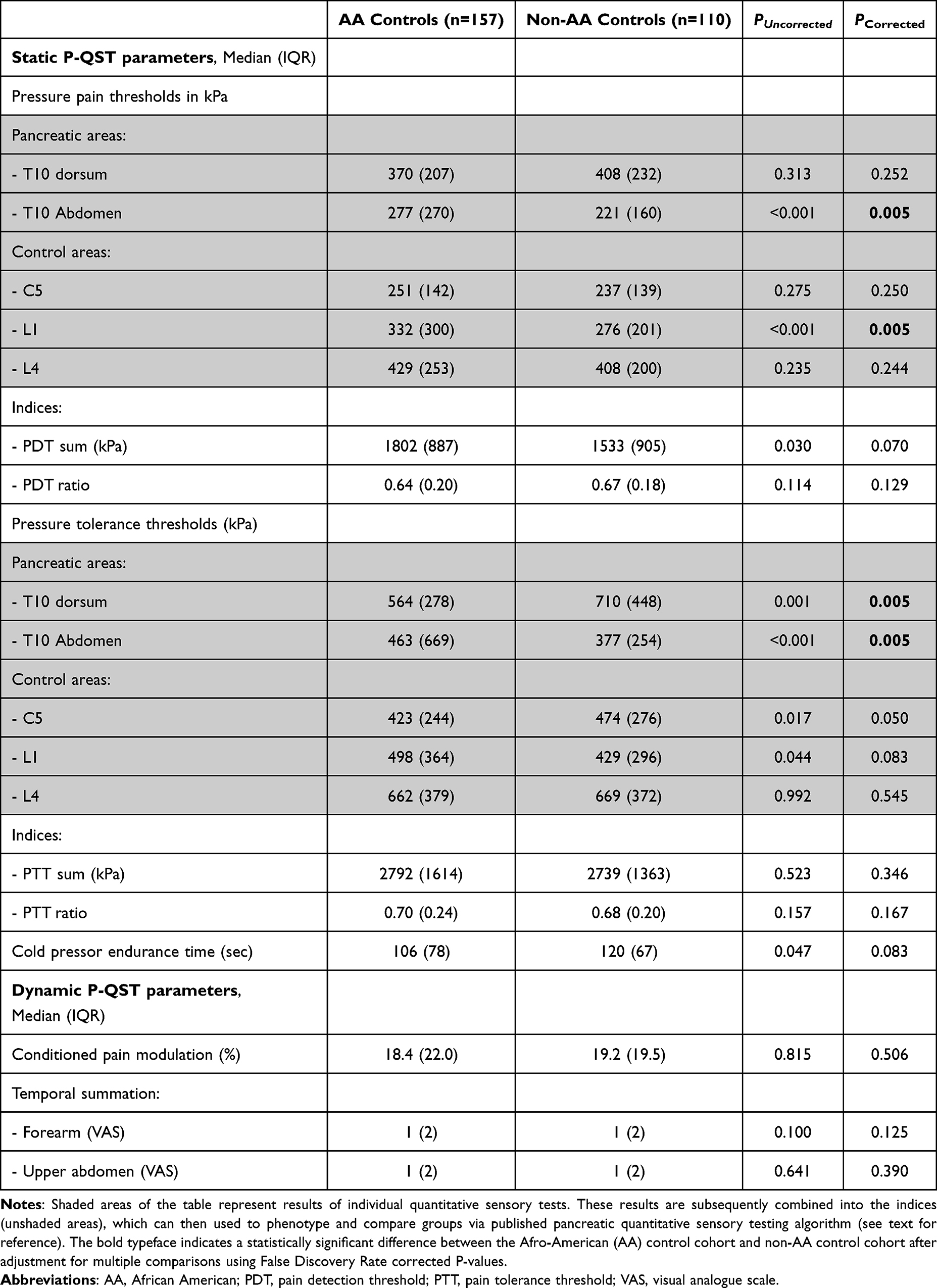 |
Table 2 Pancreatic Quantitative Sensory Testing (P-QST) Parameters in Control Subjects by Racial Subgroups |
P-QST Parameters in AA Controls vs AA Participants with CP
The P-QST parameters for AA controls vs AA participants with CP are reported in Table 3: similar to Table 2 the indices are reported in the unshaded areas and individual test results are reported in the grayed areas. There is a borderline difference in the pPDT ratio between the two groups (p = 0.066), but there is a highly significant difference in the pPTT ratio between these two groups (p = 0.004) with pPTT begin significantly reduced in those with CP compared to controls. The CPE time was reduced in CP participants compared to controls, though this was not significant. The median CPM response was reduced in CP participants vs controls (6.0 vs.18.4%, p<=0.009). CP participants had increased TS to repetitive pinprick stimulation of the upper abdomen (p=0.004). The combination of the differences in upper abdomen TS testing and the reduction in pPTT in CP patients compared to controls suggests a higher degree of segmental sensitization (around the pancreas) in participants with CP, compared to controls.
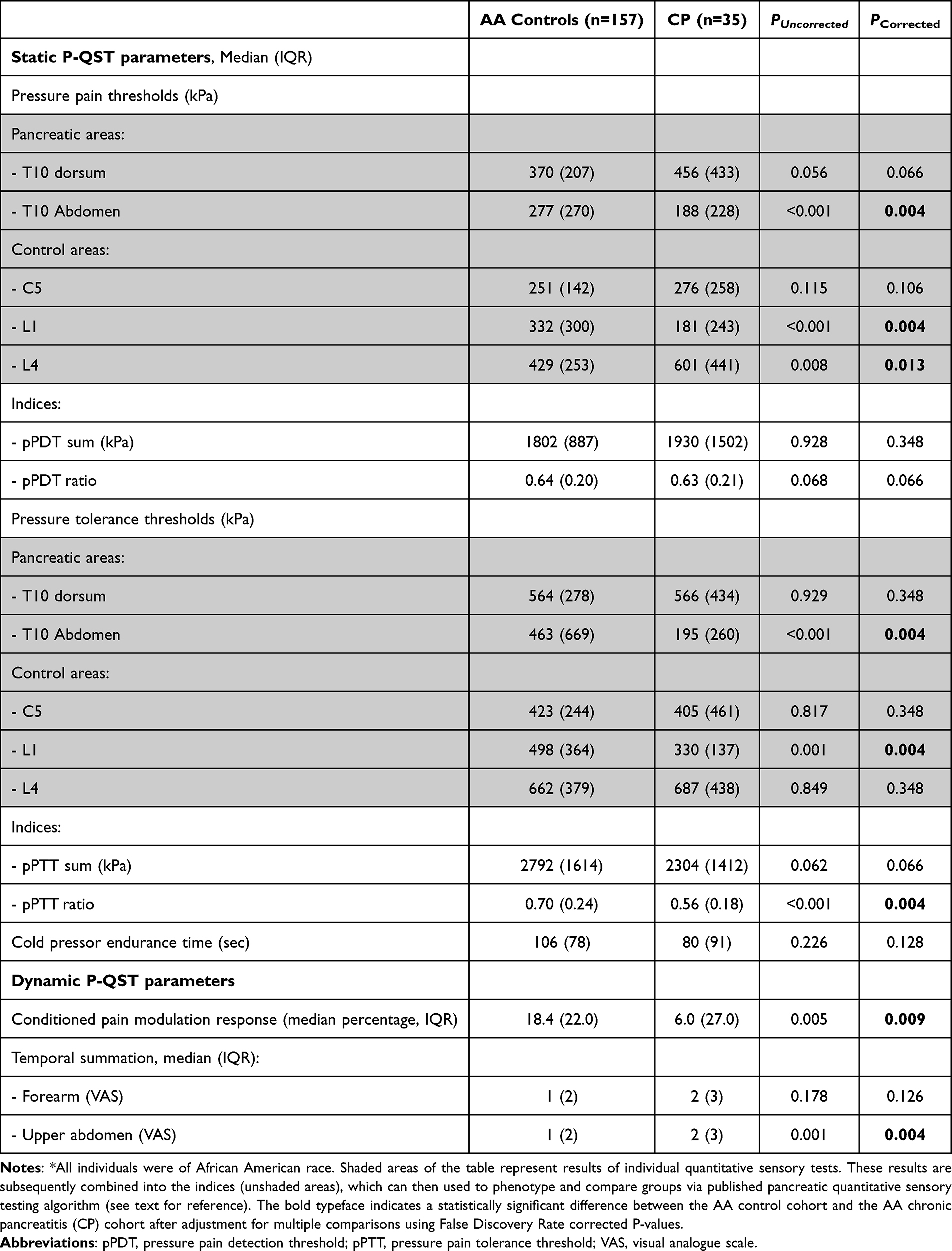 |
Table 3 Pancreatic Quantitative Sensory Testing (P-QST) Parameters in AA Controls vs Chronic Pancreatitis Patients* |
Because the CP subgroup of participants had a much higher prevalence of anxiety and depression than controls had, mediation analyses were performed. No significant mediation effects were identified (Table 4).
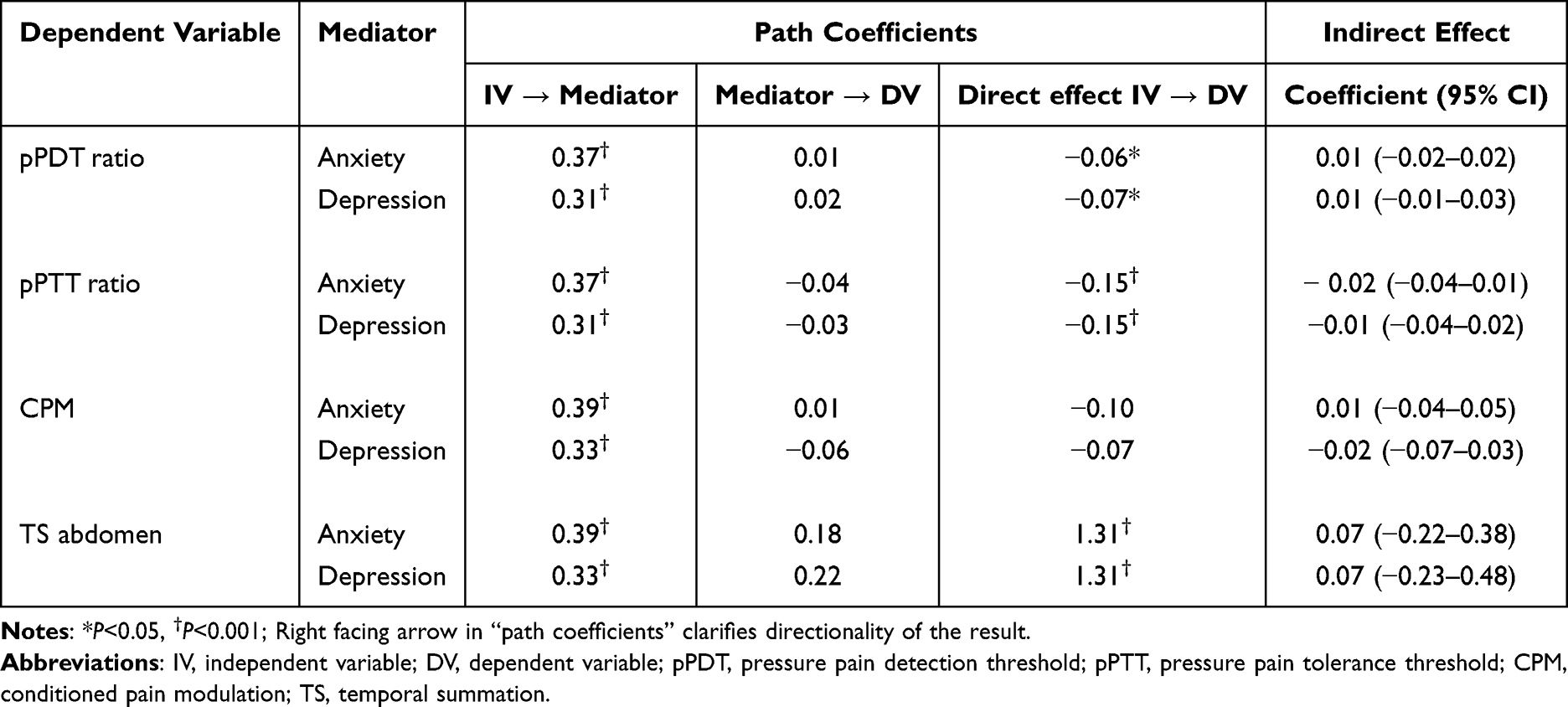 |
Table 4 Summary of the Significance of Direct and Indirect (Mediated) Effects for Sequential Mediation Models in Which the Association Between Chronic Pancreatitis (vs Controls) and Pancreatic Quantitative Sensory Testing (P-QST) Assessment Parameters (pPDT-Ratio, pPTT Ratio, CPM and TS Abdomen) is Mediated by Psychologic Distress (Anxiety and Depression) |
Discussion
The present study evaluated racial differences in experimental pain sensitivity in a group of 157 AA and 110 non-AA control participants, as well as differences in pain sensitivity between the AA control participants and 35 AA participants with CP. Neither the individual experimental pain parameters nor the static or dynamic P-QST indices results showed any consistent differences between AA and non-AA control participants. Compared to AA controls, AA participants with CP showed signs of impaired CPM, significantly lower pPTTs and suggestion of lower pPDTs, as well as increased TS scores of the upper abdomen. No mediation effects from anxiety or depression on experimental pain sensitivity were identified. Together, these findings suggest that alterations in experimental pain sensitivity accompany the CP disease state in this group of AA participants.
Racial differences in clinical pain perception have been shown across various clinical pain conditions (eg, migraine headache,16 glaucoma,17 AIDS,18 postoperative pain,19 traumatic stress exposures,20 angina pectoris,21 joint pain, and arthritis22), with AA participants often reporting greater pain-related symptoms and disabilities independent of baseline characteristics such as age, sex, socioeconomic status, and duration of disease.23–25 While prior studies have shown the risk of CP is 2–3 folds higher in AA individuals compared to Caucasians,5,26–28 differences in pain patterns and experimental pancreatic pain sensitivity in AA individuals have remained unexplored until this study.
Results from prior studies that have examined experimental pain sensitivity in other conditions are too heterogeneous to draw simple conclusions. In studies that evaluated thermal-cold and thermal-heat experimental pain thresholds between AA and non-AA healthy participants, tolerance of thermal-cold and thermal-heat pain have been shown to be lower in healthy AA participants than non-AA participants10,29 and in participants with knee osteoarthritis (OA).30 In most studies using mechanical-ischemic experimental pain models (using submaximal effort tourniquet test), no difference has been reported for pain thresholds, but pain tolerance was found to be lower in AA participants than in non-AA participants.10 Studies examining mechanical cutaneous pain (administered with calibrated nylon monofilaments) showed higher pain scores in AA, compared to non-AA in middle-aged and older adults31 and participants with knee OA.30,32 In mechanical pressure-pain models using pressure algometers, previous studies have shown that healthy AA participants9 and AA participants with knee OA exhibit either lower thresholds30,33 or no difference,31,34,35 compared to non-AA healthy participants and non-AA participants with knee OA. TS has been more pronounced in AA than non-AA healthy participants36 and participants with knee OA.30,32 In other studies, no differences have been reported between the AA and non-AA in healthy middle-aged and older adults,31 and AA healthy youth participants had higher thresholds than non-AA participants - findings more similar to our own.37 A study by Goodin et al of 225 participants with knee OA did show additional clinical relevance in that TS results were able to predict clinical outcomes for pain in non-AA but not AA participants, suggesting that these differences could predict clinically meaningful outcomes for specific groups of participants.32 CPM findings in other studies have been mixed, with greater pain reduction being seen in non-AA participants, compared to AA participants, in one study of 57 healthy adults,38 whereas a second study of 78 healthy youth (ages 10 to 17) showed a greater reduction in pain scores in AA participants, compared to non-AA participants.37 Still other studies have shown no significant differences between CPM results in AA and non-AA participants.9 Overall, there are no consistent patterns in the racial differences reported between AA and non-AA groups across multiple studies, which aligns with our findings in AA versus non-AA healthy participants.
In our study, AA CP participants were seen to have significantly higher rates of abnormal CPM than AA control participants had. Together with the borderline significant difference in pPDT ratio and the difference seen in TS of the upper abdomen suggests a pattern of generalized or segmental neuronal sensitization. Some of these differences in results may be explained by coping mechanisms in this particular cohort, levels of vigilance among the individuals tested, or simply (and potentially most likely) the CP disease process at play.39 The use of any quantitative sensory testing protocol in different racial populations will be most accurate if first tested in control participants, to understand any underlying racial differences.40–42
Disparities in pain sensitivity have been frequently associated with various psychological factors such as anxiety and depression.10,43 However, the present study found that these psychological variables that were assessed did not have any significant differences between AA and non-AA participants. The prevalence of anxiety and depression symptoms are higher in the CP population studied here than in healthy controls, a finding that is consistent with prior work.44 However, a mediation analysis performed to assess whether these factors were influential on experimental pain sensitivity found that psychological distress was not responsible for the differences seen between AA controls and AA CP participants in this study. This is also consistent with prior work showing that anxiety and depression symptoms were not independent predictors of the specific pain phenotypes characterized by patterns of hyperalgesia.3 Nevertheless, it is possible that other unmeasured psychological or socioeconomic factors could have contributed to the findings. Further research is needed to elucidate these factors and their potential impact on pain sensitivity across different racial groups.
Recent translational research indicates that differences in pain perception may be related to specific nucleotide polymorphisms (SNPs) such as catechol-O-methyl-transferase (COMT), Delta-opioid receptor (OPRD1), Mu-opioid receptor (OPRM1), and Vanilloid receptor subtype-1 gene (TRPV1).45–47 In addition, the interaction between race and the OPRM1 gene has been found to influence pain sensitivity. One study showed that participants of African ancestry who possess a certain genetic variant in the OPRM1 gene experience increased thermal and ischemic pain sensitivity, compared to those without the variant. These findings highlight the potential role of genetic factors and ethnicity in pain perception and suggest the need for personalized pain management strategies.34
This study has many strengths including its performance across multiple centers and its large cohort of participants. The findings of this study inhabit an important space in the literature, shedding some light into the knowledge gap about AA patients with CP,7 and also helping to elucidate whether any specific (and different) patterns of sensitivity using P-QST testing exist in self-identified AA participants compared to the initial cohort of primarily Caucasian participants who were tested.2 The limitations of the study must however also be acknowledged. Racial identification in this study was self-reported and was analyzed as a dichotomous variable, leaving little room for nuance in this regard. Racial identification is also not a biologic construct even though historically it may have been regarded in this way. With respect to these issues we have attempted to follow expert guidance in relation to the discussion herein wherever possible.48 While details of ancestry and ethnicity may have helped to inform our findings more thoroughly, unfortunately this information was not available to us. This was a multi-center study with deep phenotyping of all of the included participants; however, the studied group still represents a small sample size. Future studies validating these findings with larger sample sizes will be essential to helping further clarify these results. Several statistically significant differences in individual P-QST parameters were seen between AA and non-AA controls; however, the significance of these findings is questionable given the lack of consistent directionality. For this reason, we focused on the P-QST indices incorporated in the algorithm used to phenotype study subjects that has previously been published.3 This work also focused on comparison of AA healthy controls with non-AA healthy controls, and also AA healthy controls with AA CP patients. Not included here are any comparisons between AA CP patients and non-AA CP patients, as this is outside the scope of the current work. Also importantly, the lack of differences in experimental pain findings between AA and non-AA healthy controls should not be utilized to shed light on existing research related to racial differences in clinical pain as there is a lack of consensus on how the results of experimental pain testing translate to the clinical treatment of pain.
Conclusions
In conclusion, the present study found that there were no consistent experimental pain testing differences between AA control participants and non-AA control participants. AA participants with CP had a significantly higher prevalence of abnormal CPM than AA control participants had, along with lower pressure thresholds and increased abdominal sensitivity, suggesting that these patterns in experimental pain sensitivity in the studied group may be related mostly to the CP disease state. The study adds to a growing body of literature highlighting racial differences in experimental pain sensitivity. There is a need for further research to elucidate environmental, genetic, and socioeconomic status and their impact on pain sensitivity in diverse populations.
Acknowledgments
The authors would like to thank Pearl V. Nielsen, PhD, for her assistance in editing for clarity and phrasing.
Collaborators
The authors would also like to thank the additional members of the International Pancreatic Pain Consortium for their thoughtful feedback on this work: Louise Kuhlmann (Department of Gastroenterology and Hepatology, Centre for Pancreatic Diseases & Mech-Sense, Aalborg University Hospital, Aalborg, Denmark), Suzette Schmidt (Division of Gastroenterology and Hepatology, Indiana University Medical Center, Indiana, USA), Paul Tarnasky and Elaina Vivian (Methodist Digestive Institute, Dallas, Texas, USA), Juan Gurria (Division of Pediatric General and Thoracic Surgery, Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio, USA), Maisam Abu-el-Haija (Division of Gastroenterology Hepatology and Nutrition, Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio, USA), Rupjyoti Talukdar and Misbah Unnisa (Department of Gastroenterology, Asian Institute of Gastroenterology, Hyderabad, Telangana, India), Pramod Garg and Soumya Jagannath (Department of Gastroenterology, All India Institute of Medical Sciences, New Delhi, India), Jonas Rosendahl and Marko Damm (Department of Internal Medicine I, Martin Luther University, Halle (Saale), Germany), Peter Hegyi (Institute for Translational Medicine, Medical School, University of Pécs, Pécs, Hungary; Center for Translational Medicine, Semmelweis University, Budapest, Hungary; Institute of Pancreatic Diseases, Semmelweis University, Budapest, Hungary), Zoltan Hajnády (Semmelweis University, Budapest, Hungary), Patrick Michl (Department of Internal Medicine I, Martin-Luther-University Halle-Wittenberg, Halle (Saale), Germany) and Ana Dugic (Department of Internal Medicine IV, Heidelberg University Hospital, Heidelberg, Germany).
Author Contributions
Vikesh K. Singh, MD, MSc is the guarantor of the article. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
DY reports personal fees from Pfizer, Inc, outside the submitted work. VKS is a consultant for AbbVie and Nestlée Health Science; medical advisory board participant for Envara; receives grant support from AbbVie; personal fees from Amgen and Zenas BioPharma; grants from Panafina; equity holder for Kyttaro, Solv Endotherapy and Origin Endoscopy. These financial interests do not pertain directly to this work. For the remaining authors, no conflict of interest was declared.
The abstract of this paper was presented at the European Pancreas Club as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Pancreatology in November 2023 (DOI:10.1016/j.pan.2023.06.542).
References
1. Rahavard BB, Candido KD, Knezevic NN. Different pain responses to chronic and acute pain in various ethnic/racial groups. Pain Manag. 2017;7(5):427–12. doi:10.2217/pmt-2017-0056
2. Phillips AE, Faghih M, Kuhlmann L, et al. A clinically feasible method for the assessment and characterization of pain in patients with chronic pancreatitis. Pancreatology. 2020;20(1):25–34. doi:10.1016/j.pan.2019.11.007
3. Faghih M, Phillips AE, Kuhlmann L, et al. Pancreatic QST Differentiates Chronic Pancreatitis Patients into Distinct Pain Phenotypes Independent of Psychiatric Comorbidities. Clin Gastroenterol Hepatol. 2022;20(1):153–161e152. doi:10.1016/j.cgh.2020.10.036
4. Olesen SS, Phillips AE, Faghih M, et al. Overlap and cumulative effects of pancreatic duct obstruction, abnormal pain processing and psychological distress on patient-reported outcomes in chronic pancreatitis. Gut. 2022;71(12):2518–2525. doi:10.1136/gutjnl-2021-325855
5. Yang AL, Vadhavkar S, Singh G, Omary MB. Epidemiology of alcohol-related liver and pancreatic disease in the United States. Arch Intern Med. 2008;168(6):649–656. doi:10.1001/archinte.168.6.649
6. Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013;144(6):1252–1261. doi:10.1053/j.gastro.2013.01.068
7. Wilcox CM, Sandhu BS, Singh V, et al. Racial Differences in the Clinical Profile, Causes, and Outcome of Chronic Pancreatitis. Am J Gastroenterol. 2016;111(10):1488–1496. doi:10.1038/ajg.2016.316
8. Edwards RR, Doleys DM, Fillingim RB, Lowery D. Ethnic differences in pain tolerance: clinical implications in a chronic pain population. Psychosom Med. 2001;63(2):316–323. doi:10.1097/00006842-200103000-00018
9. Goodin BR, Kronfli T, King CD, Glover TL, Sibille K, Fillingim RB. Testing the relation between dispositional optimism and conditioned pain modulation: does ethnicity matter? J Behav Med. 2013;36(2):165–174. doi:10.1007/s10865-012-9411-7
10. Kim HJ, Yang GS, Greenspan JD, et al. Racial and ethnic differences in experimental pain sensitivity: systematic review and meta-analysis. Pain. 2017;158(2):194–211. doi:10.1097/j.pain.0000000000000731
11. Schneider A, Lohr JM, Singer MV. The M-ANNHEIM classification of chronic pancreatitis: introduction of a unifying classification system based on a review of previous classifications of the disease. J Gastroenterol. 2007;42(2):101–119. doi:10.1007/s00535-006-1945-4
12. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
13. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52(2):69–77. doi:10.1016/S0022-3999(01)00296-3
14. Walsh NE, Schoenfeld L, Ramamurthy S, Hoffman J. Normative model for cold pressor test. Am J Phys Med Rehabil. 1989;68(1):6–11. doi:10.1097/00002060-198902000-00003
15. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. doi:10.3758/BRM.40.3.879
16. Heckman BD, Britton AJ. Headache in African Americans: an Overlooked Disparity. J Natl Med Assoc. 2015;107(2):39–45. doi:10.1016/S0027-9684(15)30023-7
17. Sherwood MB, Garcia-Siekavizza A, Meltzer MI, Hebert A, Burns AF, McGorray S. Glaucoma’s impact on quality of life and its relation to clinical indicators. A pilot study. Ophthalmology. 1998;105(3):561–566. doi:10.1016/S0161-6420(98)93043-3
18. Breitbart W, McDonald MV, Rosenfeld B, et al. Pain in ambulatory AIDS patients. I: pain characteristics and medical correlates. Pain. 1996;68(2–3):315–321. doi:10.1016/S0304-3959(96)03215-0
19. Thurston KL, Zhang SJ, Wilbanks BA, Billings R, Aroke EN. A Systematic Review of Race, Sex, and Socioeconomic Status Differences in Postoperative Pain and Pain Management. J Perianesth Nurs. 2023;38(3):504–515. doi:10.1016/j.jopan.2022.09.004
20. Beaudoin FL, Zhai W, Merchant RC, et al. Persistent and Widespread Pain Among African-Americans Six Weeks after MVC: emergency Department-based Cohort Study. West J Emerg Med. 2020;22(2):139–147. doi:10.5811/westjem.2020.8.47450
21. Sheffield D, Kirby DS, Biles PL, Sheps DS. Comparison of perception of angina pectoris during exercise testing in African-Americans versus Caucasians. Am J Cardiol. 1999;83(1):106–108,A108. doi:10.1016/S0002-9149(98)00790-5
22. Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58(1):26–35. doi:10.1002/art.23176
23. Cano A, Mayo A, Ventimiglia M. Coping, pain severity, interference, and disability: the potential mediating and moderating roles of race and education. J Pain. 2006;7(7):459–468. doi:10.1016/j.jpain.2006.01.445
24. Edwards RR, Moric M, Husfeldt B, Buvanendran A, Ivankovich O. Ethnic similarities and differences in the chronic pain experience: a comparison of African American, Hispanic, and white patients. Pain Med. 2005;6(1):88–98. doi:10.1111/j.1526-4637.2005.05007.x
25. Meints SM, Miller MM, Hirsh AT. Differences in Pain Coping Between Black and White Americans: a Meta-Analysis. J Pain. 2016;17(6):642–653. doi:10.1016/j.jpain.2015.12.017
26. Yadav D, Muddana V, O’Connell M. Hospitalizations for chronic pancreatitis in Allegheny County, Pennsylvania, USA. Pancreatology. 2011;11(6):546–552. doi:10.1159/000331498
27. Yadav D, O’Connell M, Papachristou GI. Natural history following the first attack of acute pancreatitis. Am J Gastroenterol. 2012;107(7):1096–1103. doi:10.1038/ajg.2012.126
28. Lowenfels AB, Maisonneuve P, Grover H, et al. Racial factors and the risk of chronic pancreatitis. Am J Gastroenterol. 1999;94(3):790–794. doi:10.1111/j.1572-0241.1999.00952.x
29. Moss KO, Wright KD, Tan A, et al. Race-Related Differences Between and Within Sex to Experimental Thermal Pain in Middle and Older Adulthood: an Exploratory Pilot Analysis. Front Pain Res. 2021;2:780338. doi:10.3389/fpain.2021.780338
30. Cruz-Almeida Y, Sibille KT, Goodin BR, et al. Racial and ethnic differences in older adults with knee osteoarthritis. Arthritis Rheumatol. 2014;66(7):1800–1810. doi:10.1002/art.38620
31. Riley III JL, Cruz-Almeida Y, Tl G, et al. Age and race effects on pain sensitivity and modulation among middle-aged and older adults. J Pain. 2014;15(3):272–282. doi:10.1016/j.jpain.2013.10.015
32. Goodin BR, Bulls HW, Herbert MS, et al. Temporal summation of pain as a prospective predictor of clinical pain severity in adults aged 45 years and older with knee osteoarthritis: ethnic differences. Psychosom Med. 2014;76(4):302–310. doi:10.1097/PSY.0000000000000058
33. Glover TL, Goodin BR, Horgas AL, et al. Vitamin D, race, and experimental pain sensitivity in older adults with knee osteoarthritis. Arthritis Rheum. 2012;64(12):3926–3935. doi:10.1002/art.37687
34. Ba H, Jl RIII, Kaplan L, et al. Ethnicity interacts with the OPRM1 gene in experimental pain sensitivity. Pain. 2012;153(8):1610–1619. doi:10.1016/j.pain.2012.03.022
35. Rahim-Williams FB, Riley III JL, Herrera D, Campbell CM, Hastie BA, Fillingim RB. Ethnic identity predicts experimental pain sensitivity in African Americans and Hispanics. Pain. 2007;129(1–2):177–184. doi:10.1016/j.pain.2006.12.016
36. Mechlin B, Morrow AL, Maixner W, Girdler SS. The relationship of allopregnanolone immunoreactivity and HPA-axis measures to experimental pain sensitivity: evidence for ethnic differences. Pain. 2007;131(1–2):142–152. doi:10.1016/j.pain.2006.12.027
37. Morris MC, Walker L, Bruehl S, Hellman N, Sherman AL, Rao U. Race effects on temporal summation to heat pain in youth. Pain. 2015;156(5):917–922. doi:10.1097/j.pain.0000000000000129
38. Campbell CM, France CR, Robinson ME, Logan HL, Geffken GR, Fillingim RB. Ethnic differences in diffuse noxious inhibitory controls. J Pain. 2008;9(8):759–766. doi:10.1016/j.jpain.2008.03.010
39. Campbell CM, Edwards RR, Fillingim RB. Ethnic differences in responses to multiple experimental pain stimuli. Pain. 2005;113(1–2):20–26. doi:10.1016/j.pain.2004.08.013
40. Helms JE, Jernigan M, Mascher J. The meaning of race in psychology and how to change it: a methodological perspective. Am Psychol. 2005;60(1):27–36. doi:10.1037/0003-066X.60.1.27
41. Comstock RD, Castillo EM, Lindsay SP. Four-year review of the use of race and ethnicity in epidemiologic and public health research. Am J Epidemiol. 2004;159(6):611–619. doi:10.1093/aje/kwh084
42. Corbie-Smith G, St George DM, Moody-Ayers S, Ransohoff DF. Adequacy of reporting race/ethnicity in clinical trials in areas of health disparities. J Clin Epidemiol. 2003;56(5):416–420. doi:10.1016/S0895-4356(03)00031-3
43. Ruehlman LS, Karoly P, Newton C. Comparing the experiential and psychosocial dimensions of chronic pain in African Americans and Caucasians: findings from a national community sample. Pain Med. 2005;6(1):49–60. doi:10.1111/j.1526-4637.2005.05002.x
44. Phillips AE, Faghih M, Drewes AM, Singh VK, Yadav D, Olesen SS. Psychiatric Comorbidity in Patients With Chronic Pancreatitis Associates With Pain and Reduced Quality of Life. Am J Gastroenterol. 2020;115(12):2077–2085. doi:10.14309/ajg.0000000000000782
45. Xu F, Yin J, Xiong E, et al. COMT gene variants and beta-endorphin levels contribute to ethnic differences in experimental pain sensitivity. Mol Pain. 2020;16:1744806920908474. doi:10.1177/1744806920908474
46. Diatchenko L, Slade GD, Nackley AG, et al. Genetic basis for individual variations in pain perception and the development of a chronic pain condition. Hum Mol Genet. 2005;14(1):135–143. doi:10.1093/hmg/ddi013
47. Fillingim RB, Kaplan L, Staud R, et al. The A118G single nucleotide polymorphism of the mu-opioid receptor gene (OPRM1) is associated with pressure pain sensitivity in humans. J Pain. 2005;6(3):159–167. doi:10.1016/j.jpain.2004.11.008
48. Flanagin A, Frey T, Christiansen SL. Committee AMAMoS. Updated Guidance on the Reporting of Race and Ethnicity in Medical and Science Journals. JAMA. 2021;326(7):621–627. doi:10.1001/jama.2021.13304
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation by Survival Analysis of Cold Pain Tolerance in Patients with Fibromyalgia and Opioid Use
Deng EZ, Weikel DP, Martucci KT
Journal of Pain Research 2022, 15:2783-2799
Published Date: 9 September 2022
Effects of Hypnotic Analgesia and Transcranial Direct Current Stimulation on Pain Tolerance and Corticospinal Excitability in Individuals with Fibromyalgia: A Cross-Over Randomized Clinical Trial
Schein B, Beltran G, França BR, Sanches PR, Silva DP Jr, Torres IL, Fegni F, Caumo W
Journal of Pain Research 2023, 16:187-203
Published Date: 24 January 2023
Can Myofascial Trigger Points Involve Nociplastic Pain? A Scoping Review on Animal Models
Matuska W, Matuska J, Skorupska E, Siwek M, Herrero P, Santafé MM
Journal of Pain Research 2023, 16:3747-3758
Published Date: 8 November 2023
Best Practices for Chronic Pancreatitis Pain Management: A Comprehensive Evidence-Based Review
Huang PY, Xiao AF, Ren ZQ, Chen L, Ding L, Li C
Journal of Inflammation Research 2025, 18:5087-5096
Published Date: 15 April 2025