Back to Journals » Journal of Pain Research » Volume 16
Can Myofascial Trigger Points Involve Nociplastic Pain? A Scoping Review on Animal Models
Authors Matuska W ![]() , Matuska J, Skorupska E
, Matuska J, Skorupska E ![]() , Siwek M, Herrero P
, Siwek M, Herrero P ![]() , Santafé MM
, Santafé MM ![]()
Received 25 May 2023
Accepted for publication 28 September 2023
Published 8 November 2023 Volume 2023:16 Pages 3747—3758
DOI https://doi.org/10.2147/JPR.S422885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Wiktoria Matuska,1 Jakub Matuska,2 Elżbieta Skorupska,2 Maria Siwek,3 Pablo Herrero,4 Manel M Santafé5
1Faculty of Veterinary Medicine and Animal Science, University of Life Sciences, Poznań, Poland; 2Department of Physiotherapy, University of Medical Sciences, Poznań, Poland; 3Department of Animal Biotechnology and Genetics, Faculty of Animal Breeding and Biology, University of Science and Technology, Bydgoszcz, Poland; 4Department of Physiatry and Nursing, Faculty of Health Sciences, IIS Aragon, University of Zaragoza, Zaragoza, Spain; 5Unit of Histology and Neurobiology, Department of Basic Medical Sciences, Faculty of Medicine and Health Sciences, Rovira I Virgili University, Reus, Spain
Correspondence: Manel M Santafé, Email [email protected]
Abstract: Nociplastic pain is a non-specific, regional pain lasting more than three months, characterised by the onset of hypersensitivity, despite no clear evidence of tissue damage. It is a relatively new classified type of pain. As a result, there has not yet been much work describing its precise modelling. The mechanism of its formation needs to be clearly explained. Authors point out that the occurrence of myofascial trigger points (MTrPs) can lead to this type of pain as one possibility. This paper summarises the available literature on modelling nociplastic pain and MTrPs. It complies with studies describing animal model creation and presents the results of performed experiments. The literature search was conducted in December 2022 and included the following databases: PubMed, Scopus, and Web of Science. In this scoping review, six studies were included. Two described the creation of animal models of nociplastic pain, one adapted old models to nociplastic pain, and three described the modelling of MTrPs. This is the first paper pointing in the possible direction of detecting and studying the correlation between MTrPs and nociplastic pain in animal models. However, there is currently insufficient evidence to describe MTrPs as nociplastic, as few studies with animal models exist.
Keywords: chronic pain, myofascial pain, autonomic nervous system, referred pain, hyperalgesia
Introduction
In 2017, the International Association for the Study of Pain (IASP) included nociplastic pain as a third pain mechanism besides neuropathic and nociceptive.1 It is described as “pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain”.2 To determine the presence of nociplastic pain, the patient must meet the following criteria: pain lasts more than three months, described more often as regional than discrete, with unexplained mechanisms, presenting with hypersensitivity.3 In addition, patients also present symptoms from the central nervous system, such as increased sensitivity to light/sound, sluggishness, frequent mood changes or tiredness.4
Nociplastic is one of the subtypes of chronic pain.2 ICD-11 classifies chronic pain as primary and secondary. Most, if not all, of primary pain subgroups include conditions with nociplastic pain.5–7 One of them is Chronic Primary Musculoskeletal Pain. Fitzcharles et al indicate that this category could contain the old concept, called Myofascial Pain, which is directly connected with myofascial trigger points (MTrPs).6 MTrPs are hypersensitive areas localised in a taut band in muscles causing sensory, motor and autonomic alterations.8 Authors distinguish active trigger points (ATrPs) that spontaneously can reproduce familiar pain, whereas symptoms provoked by latent trigger points (LTrPs) are not known to a patient. Some attempts have been already made in the available literature to link MTrPs with nociplastic pain.9–11 However, Treede does not fully follow Fitzcharles’ concept, pointing out that it is an interesting idea to integrate the mechanistic concept of “nociplastic pain” and the older term “myofascial pain”, but the conclusions are premature without further empirical evidence on autonomic, motor and sensory alterations in the zone of referred pain.5 On the contrary, De las Peñas et al proposed three subgroups of patients with Myofascial TrP Pain, stating that MTrPs are rather nociceptive than nociplastic – in nociplastic they are comorbid conditions. Nevertheless, it is unclear if the myofascial trigger points themselves can cause nociplastic pain.12
Interestingly, recent research suggests a possible connection between referred pain provoked by MTrPs and the nociplastic mechanism via abnormal autonomic nervous system activity.10 The researchers provoke noxiously amplified vasomotor reactivity within referred pain due to MTrPs stimulation with both active and latent MTrPs. The autonomic nervous system (ANS) dysregulation is perceived as a potentially important factor in the nociplastic pain development. Moreover, several authors have undertaken studies on asymptomatic individuals with myofascial trigger points (MTrPs), highlighting the presence of hypersensitivity – an essential criterion for nociplastic pain – in the corresponding referred pain zones.13,14 Thus, we hypothesise that maybe not all trigger points are related to nociplastic pain, but only these produce referred pain. Despite human studies indicate association between ANS, hypersensitivity and MTrPs-related referred pain, there is still a lack of a piece of evidence on the mechanism of referred pain and its link with nociplastic pain. Therefore, performing research on animal models would allow insightful analysis on the level of structural changes. There are several advantages of the animal models. The very first one is a uniform genetic background, which in the case of mouse inbred lines is almost identical.15 Yet another advantage is the possibility of generating high number of individuals of one gender as some studies pointed towards females being more prone to transition from temporary to nociplastic pain. Animal testing also allows for more invasive procedures. It is possible to collect tissues for histopathological and biochemical examination and to observe post-mortem changes. Animal testing is used extensively in the production of vaccines, research into human diseases such as diabetes and AIDS, drug distribution and transplantology.15,16 Animal modelling has also been applied to work on the investigation of the mechanism of pain.17
So far, many neuropathic and nociceptive pain models have been developed.18 Nociplastic pain models are still poorly explored, and more research needs to be produced on this issue. Hence, animal models can accelerate research in this field, especially in view of Fitzcharles’ concept.6
Scoping reviews are dedicated to discussing currently available evidence without targeting the clinical effectiveness of undertaken interventions. Such a review allows us to summarise current knowledge and identify future directions and perspectives. We opted to conduct a scoping review instead of a systematic review with meta-analysis due to the observed heterogeneity and limited data in the PICO analyses of these studies, making direct comparisons challenging.19 As far as we know, it is the first scoping review analysing animal models for nociplastic pain related to MTrPs. The aim of this paper is to summarise the current knowledge on animal modelling of nociplastic and MTrPs and to identify possible future directions.
Materials and Methods
Scoping Review
This review has been produced in accordance with the standards adopted for scoping review (Supplementary Table 1).20
Search Strategy
We used databases PubMed, Scopus and Web of Science. The search was conducted between 27 December and 28 December 2022 in the field of animal studies by analysing the following keywords: “nociplastic pain”, “trigger points”, “model”, “central sensitisation”, and “myofascial pain” and their various combinations depending on the database capabilities. References have been manually screened. Moreover, the option “similar articles” was used to expand the search strategy. All database search strategies are outlined in Table 1. MeSH was not used because of a lack of certain terms.
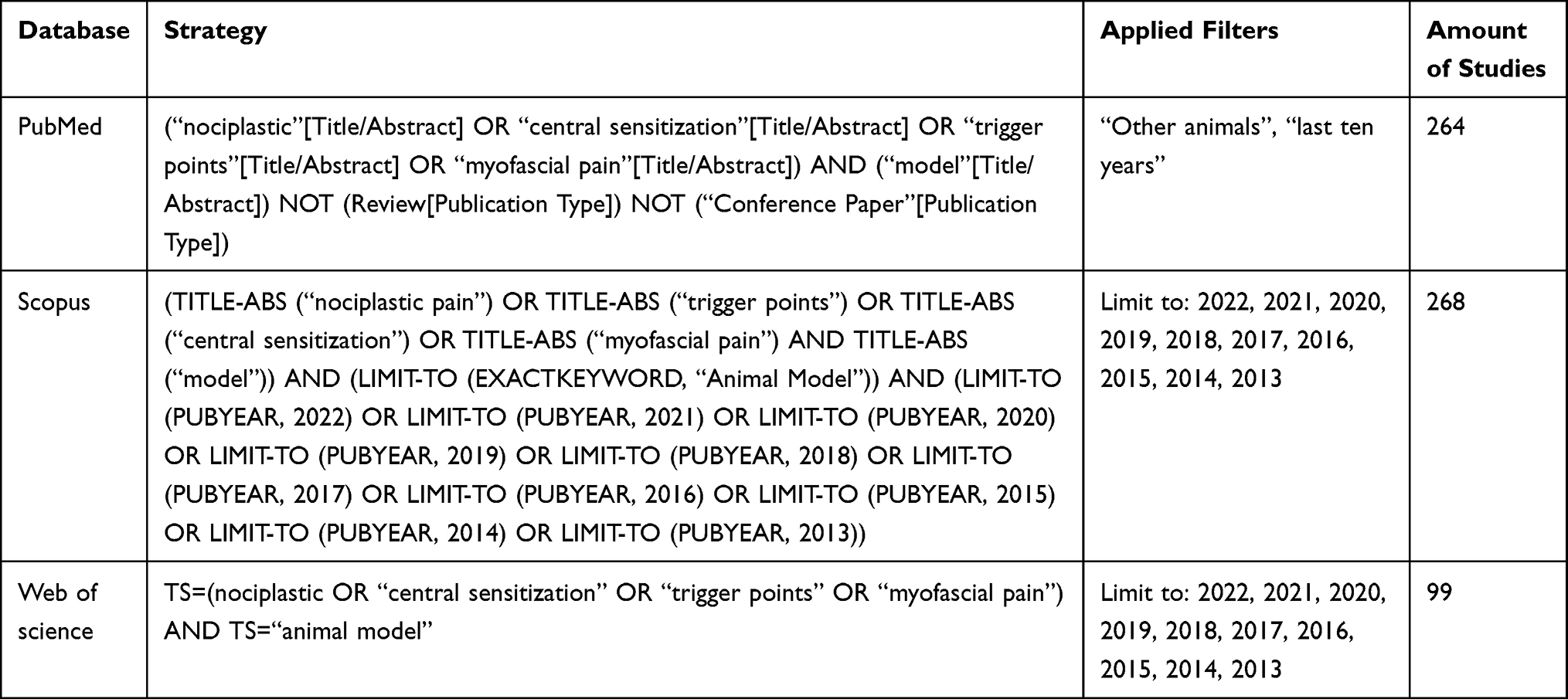 |
Table 1 Database Formulas During the Literature Search |
Eligibility Criteria
Two authors screened all the studies separately to verify whether they met the inclusion and exclusion criteria (Table 2) between 29 December 2022 and 15 January 2023. We have added, for example, systematic reviews as exclusion criteria. The inclusion of systematic reviews would have resulted in unnecessary duplication of the developed models as we were interested in original papers in which those models were created. Moreover, systematic reviews have their own objectives that can disturb this scoping review.
 |
Table 2 Inclusion and Exclusion Criteria |
Both researchers made a collective decision to include the paper in the scoping review. When there was no agreement to include a study, a third person supervising them decided if the studies were included or not.
Data Extraction
To extract the data, we used the online tool Covidence review software (Veritas Health Innovation). Obtained citation from databases has been imported to Covidence. Then, duplicates were automatically removed. Authors checked if the selected studies fulfilled the eligibility criteria in two steps, firstly by abstract and secondly by the full text. It took place from 15 February to 31 March 2023. For extracting data, we considered the following items: model creation, assessment of the animals, laboratory testing, type of the study, and main outcomes. We used the Systematic Review Tool of the Centre for Laboratory Animal Experimentation (SYRCLE) to conduct the critical appraisal.21 Assessment of the value and reliability may point out the gaps in the preclinical studies. The process of extraction and interpretation of obtained data was followed by dividing subjects into subsequent sections: Nociplastic Pain Models and Myofascial Trigger Points Models.
Results
Search results
In total, 633 studies were selected. The process of data extraction is presented in Figure 1. Two studies described novel nociplastic pain models, and three papers reported myofascial pain models. Moreover, one study presented two old models adapted to nociplastic pain. Animal models involved two animal species: rats and mice. Finally, three studies about the animal nociplastic pain model and three studies about the myofascial trigger points model were included.
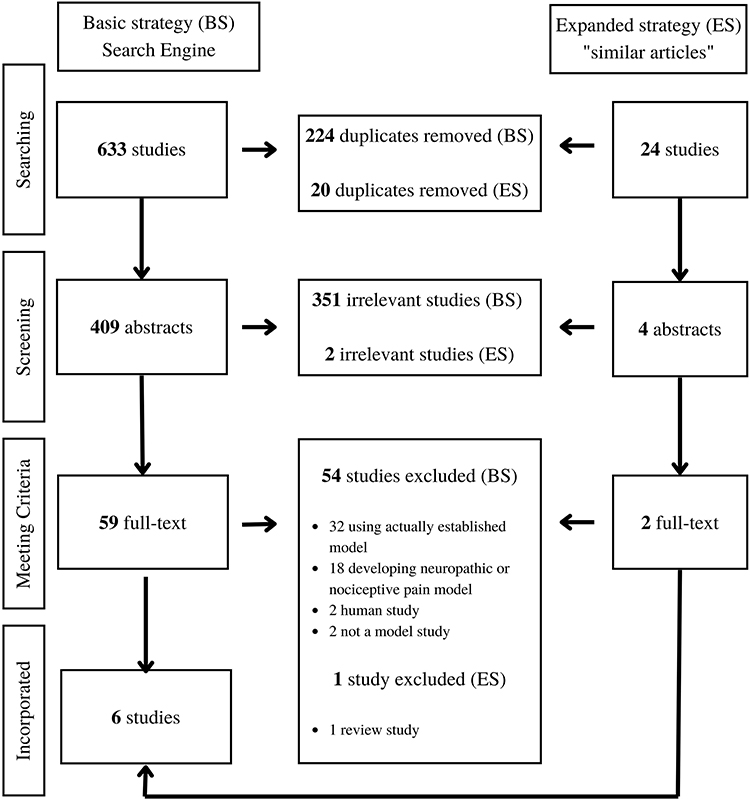 |
Figure 1 Flow chart of the data extraction process. Abbreviations: BS, Basic strategy; ES, Expanded strategy. |
Summary Findings
We analyzed the presented models in terms of their compatibility with nociplastic pain criteria. In Table 3 we have summarized the outcome of this analysis. We were unable to find a paper in which the developed model fully fits into the characteristics of nociplastic pain. The meaning of autonomic nervous system involvement was considered by Sugimoto et al and Hsieh et al.22,23 In addition, the work of Margalef et al was the only one to indicate the occurrence of pain without tissue damage.24
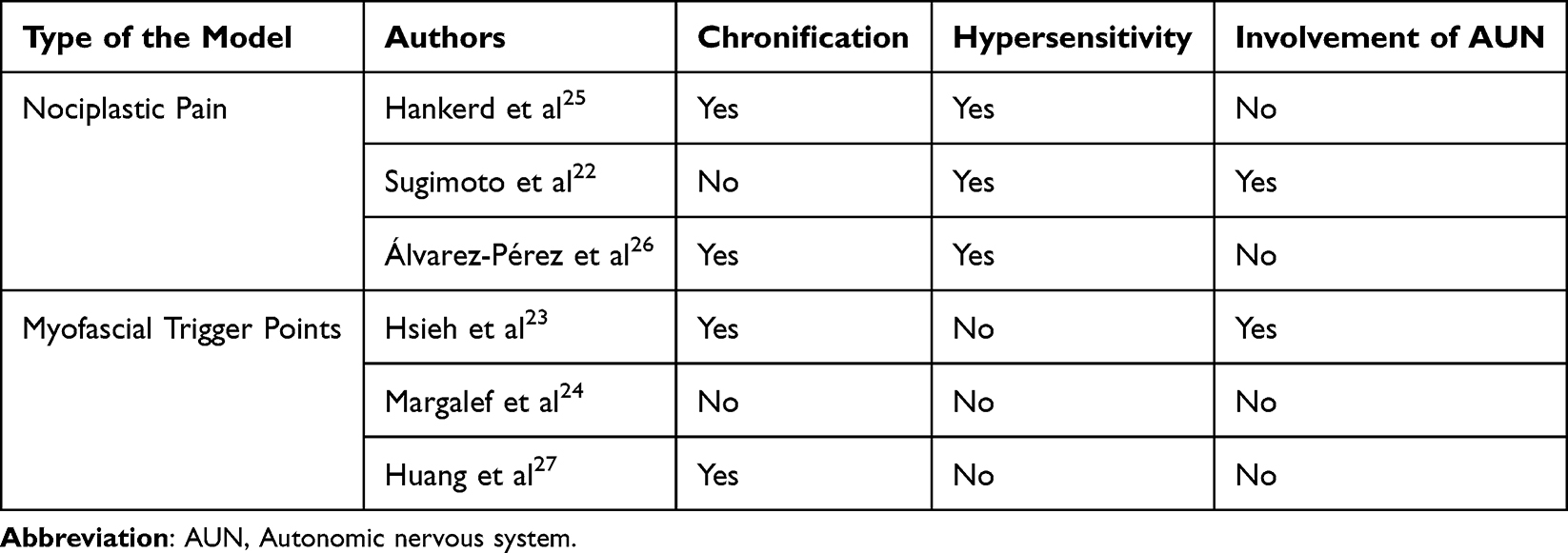 |
Table 3 Summary of the Investigation of Specific Features of Nociplastic Pain in Individual Articles |
Among the analyzed models, we selected two that possibly offered the best possibilities for creating a model that had all the features of nociplastic pain. The first describes the nociplastic pain model invented by Sugimoto et al and the second identifies myofascial trigger points created by Margalef et al.22,24 It seems to us that extending the included models to align fully with the attributes of nociplastic pain could lead to the development of a singular, comprehensive model.
Nociplastic Pain Models
During the creation of this scoping review, we only considered models that strictly described the development of nociplastic pain. This is a relatively new categorised type of pain. However, it is not excluded that older papers may also have contained models that can be adapted to study this type of pain in the future. We sum up all of the models (nociplastic) in Table 4.
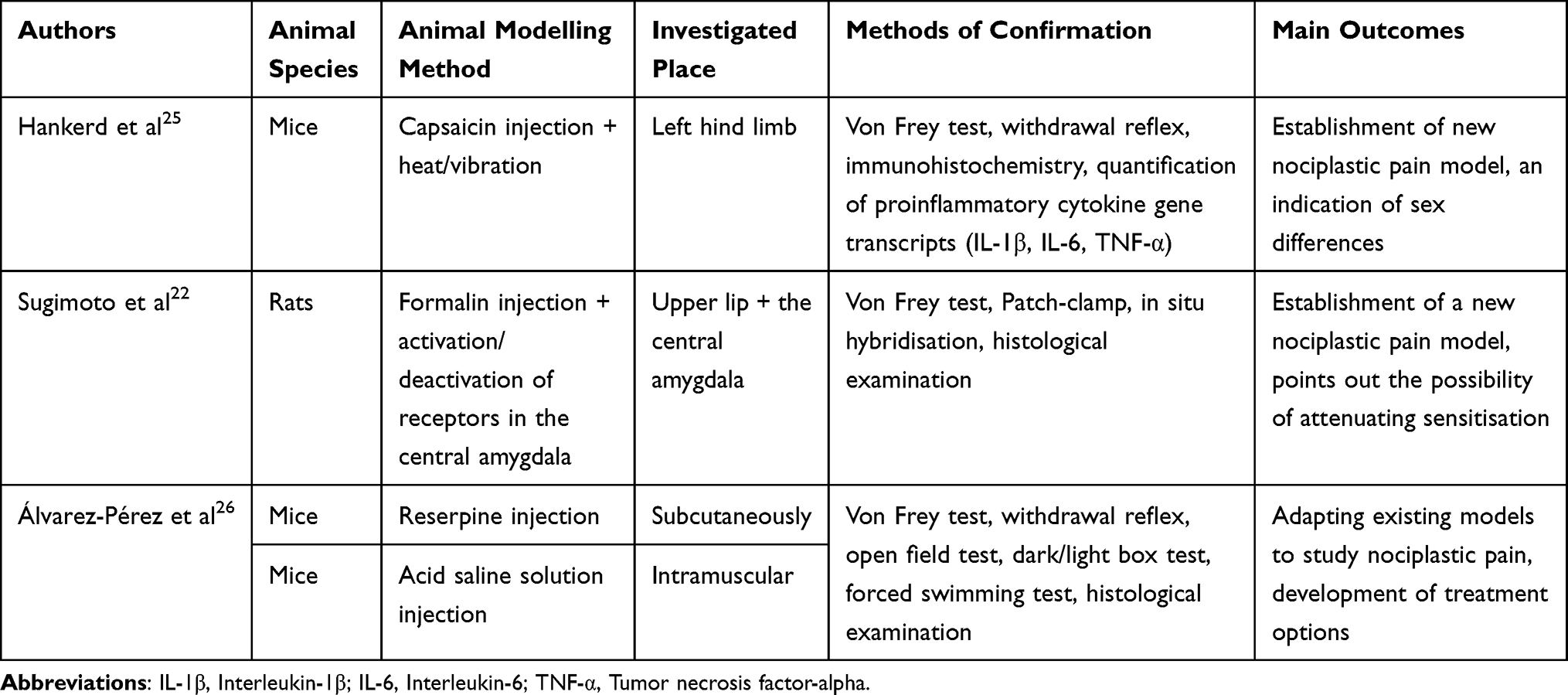 |
Table 4 Summary of the Nociplastic Pain Models Presented in the Scoping Review |
Description of the Nociplastic Pain Models
A novel model of postinjury transition to nociplastic pain has been constructed by Hankerd et al.25 The authors provoked injury with an injection of capsaicin in the left hind limb of the plantar area. In a group of mice, instead of capsaicin injection, the skin was incised and sutured at the level of the second-fourth digit of the plantar surface. Performed procedures were carried out under anaesthesia, for which 1.5–2.5% isoflurane was used. The pain chronification was sustained by heat (immersion in 40°C water at 10-minute intervals two hours after injection, where 30 seconds were underwater and 30 seconds rested). The control group has been exposed to air immersion (similar to a warm water bath), where the mice were dipped into an empty bath. A group of mice that underwent incision instead of capsaicin injection were stimulated with heat 23 hours after the procedure. In addition to heat stimulation, to induce pain chronification, the vibration was also used, which was achieved by applying a mini massager to the injected limb. In the research group, these were 10-second applications in 30-second intervals for 10 minutes, and in the control group, applications of the massager were turned off. After 7 to 10 days, mice were injected with the following drugs: (1) bupivacaine or saline – at the area of capsaicin injection, (2) morphine, gabapentin or saline – intraperitoneal; (3) saporin or Mac-1 saporin – intrathecal.
The rat model of Sugimoto et al presented an ectopic pain model in which hypersensitivity is present in areas not affected by the underlying inflammation.22 The injury was caused by formalin and was located in the orofacial area. Before that, three sets of experiments were performed. Two of them commanded the activation of hM4Di and hM3Dq by microinjection of adeno-associated virus vector into the central amygdala. Another procedure was to administer a calcitonin gene–related peptide receptor antagonist into the central amygdala. This resulted in the discovery of the location of widespread mechanical sensitisation.
The mice model used in the Álvarez-Pérez et al study has been described previously but was adapted here for the first time to a nociplastic pain model.26 It included two other models of fibromyalgia-like conditions, involving the administration of reserpine or intramuscular injection of acid saline solution.28,29 The solution for injection used in the first model was reserpine diluted with acetic acid and saline to a concentration of 0.5% acetic acid. This prepared solution was injected at a dose of 0.25 mg/kg via the subcutaneous route. Animals receiving reserpine were divided into groups according to the quantities of the injections: three, four and six. Mice received injections, respectively, on days 0, 1, 2 (RIM3 group), 0, 1, 2, 9 (RIM4 group), 0, 1, 2, 9, 16, 23 (RIM6 group). The control group consisted of animals receiving reserpine dilution vehicle on a six-day schedule. The second model was based on an intramuscular injection into the right gastrocnemius muscle of 10 µL of an acid saline solution (pH = 4) (ASI-group). The injection was carried out twice, on days 0 and 5. In the control group, a saline solution was used. Five days after the last injection, the drug treatment proceeded. Pregabalin was administered at doses of 5, 10, 20 and 40 mg/kg via intraperitoneal. In the control group, the medicine was replaced with saline solution.
The Way of the Model Confirmation – Laboratory Testing
The impact of the treatments was verified by behavioural tests such as Von Frey filaments and the withdrawal reflex. To check mechanical sensitivity, Von Frey filaments were used in the hind paw after injection of capsaicin in the mice model, after upper lip formalin injection in the rat model and in the fibromyalgia mice models.22,25,26 The withdrawal reflex was measured by targeting a heat laser under the centre of the hind paw, automatically turning off when the mouse retracted a limb.25,26
To determine the occurrence of inflammation, it can be used to examine the concentration of Evans Blue dye in glamorous skin samples after intravenous injection.25 This shows plasma extravasation that accompanies inflammation. In addition, for this purpose, it is also possible to perform immunohistochemistry or quantification of proinflammatory cytokine gene transcripts (such as IL-1β, IL-6, and TNF-α).25 The reactivity of astrocytes and microglial cells from the spinal cord might be analysed through histological methods based on Zamboni solution.26
To assess acute nocifensive behaviour, rats were left in cages with mirrors for an hour, and their actions were recorded.22 The evaluation was based on the time taken to rub the injection site into the upper lip. Electrophysiological recordings (Patch-clamp) were made on brain slices 5 to 8 weeks after adeno-associated virus injection to confirm activation of the appropriate receptors. Laboratory tests also include in situ hybridisation and histological examination followed by injection of clozapine N-oxide to the somatic expression of mCherry and FluoSphere fluorescence.22 To evaluate nonreflexive pain responses, the following tests were used: open field, dark/light box, and forced swimming.26
Outcomes of the Studies
In a mice model developed by Hankered et al, for the first time, a post-injury stimulation had also been performed before initial injury-induced hypersensitivity to ensure the transition to nociplastic pain.25 Post-injury stimulation in both sexes was shown to extend the evoked hypersensitivity mechanically, but not thermally, for up to three weeks. Interestingly, when a lower-intensity stimulus was applied, chronification occurred only in female mice. These results indicate that females transition more easily from temporary to nociplastic pain after an injury. This study shows that risk factors for pain chronification are acute post-injury pain and female gender, indicating the importance of post-injury pain treatment to prevent the progression to nociplastic pain. However, further research into this model is required.
Sugimoto et al studies have shown that mechanical allodynia in the hind paw lasting >13 days was obtained after the injection of formalin in the upper lip.22 Therefore, it is possible to attenuate senescence by blocking calcitonin gene-related peptide receptors or inhibiting gamma-aminobutyric neurons in the right central amygdala. Besides, bilateral hind paw sensitisation in rats without inflammation was caused by chemogenetic stimulation of gamma-aminobutyric acid neurons in the right central amygdala. Because of the authors’ findings and the models developed, attempts have been made to use analgesics to treat nociplastic pain.
A study by Álvarez-Pérez et al was the first to adapt existing models to study nociplastic pain.26 They used two previously described animal models for fibromyalgia. In addition, these researchers showed that acute pregabalin therapy could result in reduced pain responses.
Myofascial Trigger Points Models
The models describing myofascial trigger points have been thoroughly characterised. There has been repeated replication and confirmation of them by other researchers. In our work, we presented the three established models. A summary of the studies is presented in Table 5.
 |
Table 5 Summary of the Myofascial Pain Models Presented in the Scoping Review |
Description of the Myofascial Trigger Points Models
Hsieh et al presented a model of masticatory myofascial pain (MMP) in rats.23 Authors developed MMP by repetitive tetanic eccentric contractions. Animals in the experimental group were anaesthetised and then stimulated with an electrical stimulator to maximum tetanic eccentric contraction with jaw opening. The procedure lasted 14 days. Everyday 30s with 10s breaks in stimuli for 20 min was performed. Subjects in the experimental group were anaesthetised, and then the electrode was inserted into the masseter. However, the control group did not receive any electrical stimulation.
Margalef et al worked out another novel model for developing MTrPs in mice and rats.24 Authors conducted in vivo and ex vivo experiments that investigated the influence of anticholinesterase agents (neostigmine methyl sulfate (NTG), pyridostigmine (PTG), fasciculin II (FII) and rivastigmine (RTG)) on the emergence of MTrPs. In ex vivo, part of the experiment levator auris longus muscle (LAL) and diaphragm with their nerve supply was excised from previously euthanised animals. The extracted muscles were exposed to anticholinesterasic agent (NTG or FII) for 60 minutes before the recordings started. For in vivo experiments, NTG, PTG and RTG were injected subcutaneously. The authors expected a cholinergic syndrome that would occur 30 min after injection. If it did not appear, the subjects were excluded from the study. As mentioned above, the sample was dissected when acute cholinergic syndrome disappeared. Finally, in both groups, authors obtained the best results using NTG.
Huang et al have established a model of myofascial trigger point creation in rats.27 The authors divided rats into two groups: experimental and control. Rats in the experimental group were subjected to injury by dropping a stick from a height of 20 cm into the vastus medialis (VM) muscle with a kinetic energy of 2.352 J. On the second day, they were subjected to eccentric exercise by running on the treadmill for 90 min at a 16° downward angle and with 16m/min. This procedure was repeated once a week for eight weeks. Animals in the control group were not exposed to the abovementioned practices.
The Way of the Model Confirmation – Laboratory Testing
Electrophysiological methods – especially endplate noise (EPN) recordings – were used in all three studies to confirm spontaneous electrical activity characteristics for MTrPs.23,24,27 Intramuscular electromyography was performed in the area of the taut band that was previously manually palpated. Additionally, Margalef et al used intracellular recordings – spontaneous miniature endplate potentials (mEPPs) – to confirm spontaneous neurotransmissions.24
In 2 out of 3 studies, ultrasonography has been used.23,24 Hsieh et al pointed out the taut band as a hypoechoic region with an elliptical appearance.23 On the other hand, Margalef et al used ultrasound imaging to investigate the local twitch response during the dry needling procedure of the MTrPs in rats’ gastrocnemius.24
Histological techniques were also widely used in the studies. Hsieh et al indicated that each muscle fibre was surrounded by undifferentiated endomysium.23 Therefore, aberrant, big muscular fibres with circular or/and elliptical forms in cross-section (indirect for MTrPs) were found. However, Margalef et al confirmed the presence of muscle knots after subcutaneous NTG injection using the Periodic acid Schiff (PAS)-Alcian technique.24 Moreover, the authors used methylene blue to exclude potential muscle damage due to repeated treatment. At last, a histochemical method (rhodaminated α-bungarotoxin) was performed to investigate an area of muscle knots (presence of neuromuscular synapses).
Immunohistochemistry was used only in one study.23 The authors investigated substance P-like immunoreactivity (SP-LI) in parabrachial nuclei (PBN) and amygdaloid nuclei (AN). To do so, they took 20 samples each from the region PBN and AN. After the whole laboratory procedure, obtained images were computer-based analysed to quantify SP-LI.
Outcomes of the Studies
Hsieh et al presented increased SP-LI in PBN and Central Amygdala (CeA).23 It points out that MMP is linked to PBN and CeA activity. It indicates that the development of myofascial pain may be related to the central sensitisation process, emotions and autonomic control.
Margalef et al created myofascial trigger points that were visible only for three days, probably due to a lack of chronification.24 Additionally, extracellular glycosaminoglycans (GAGs) were found in the area of MTrPs for the first time, which could be contributing to the symptoms caused by MTrPs.
Huang et al established a myofascial trigger points animal model created by blunt trauma and eccentric exercise.27 They showed differences in electrical activity and muscle morphology in model animals compared to the control group. This was associated with an increased amount of taut bands and the appearance of mixed-phase and multiphase potentials with short wavelengths in myoelectrical activity recording.
Critical Appraisal
The outcomes of the critical appraisal are available in Supplementary Table 2.21
Discussion
According to our best knowledge, it is the first time that nociplastic pain and myofascial trigger points (myofascial pain) in animal models were compared using Scoping Review (PRISMA-ScR).20 We have found some similarities between nociplastic pain and myofascial pain models: chronicfications, biomarkers as hypersensitivity and ANS involvement.
Both models used chronification as a primary factor to obtain nociplastic and myofascial pain except (i) Margalef et al, in whose study MTrPs disappeared after three days, probably due to lack of chronification; (ii) Sugimoto et al, in whose study examined responses following activation/deactivation of receptors in the central amygdala.22,24 In 5 out of 6 studies, the researchers used a distinctive agent (excessive overloading of the muscles, initial damage to the tissue) that led to the initiation of the alterations in the tissue.22,23,25–27 Whereas, Margalef et al stated that they created MTrPs despite any muscle damage confirmed in histology.24 Lastly, tree models (two nociplastic and one MTrPs) investigated changes in the Central Nervous System.22,23,26 Only Hankerd et al, Sugimoto et al, and Álvarez‑Pérez et al assessed hyperalgesia and allodynia among the mentioned models.22,25,26 In one of the described studies, the researchers used already existing mice models.26 The animal model we consider when assessing trigger points as potentially dependent on nociplastic pain would require confirmation in the following features: chronification, the occurrence of hypersensitivity (sensory alterations) and the involvement of ANS.
Chronification of Painful Stimuli
Four out of six authors conducted a repeated procedure to chronify the painful stimuli.23,25–27 In nociplastic and myofascial models, primary injury or overloading was applied, followed by chronification.23,25–27 That involved multiple repetitions of carried procedures,23,26 eccentric exercises,27 and use of heat/vibration.25 Kosek et al proposed chronicity as one of the main nociplastic pain features.1 It seems a very important element that should be included in the creation of models. Among the described papers, two of them did not include this feature.22,24 Inhibition/excitation of neurons in the central amygdala in Sugimoto’s study appears to be chronification.22 However, the observation in the study was too short to clearly determine this. In our opinion, the model developed by Margalef et al should be extended by including this essential component for further improvement.24
Occurrence of Hypersensitivity – Sensory Alterations
In all of the studies on nociplastic pain, authors used Von Frey filaments to assess hyperalgesia and allodynia remote from the primary induced injury.22,25,26 On the contrary, these symptoms were not investigated in MTrPs’ models.23,24,27 According to Treede, it is necessary to confirm this feature in MTrPs models to characterise them as nociplastic.7 Nevertheless, referred pain zone characteristics for MTrPS, in which potentially hypersensitivity could appear, should also be determined. In human studies, Quantitative Sensory Testing (QST) has already been used to assess latent MTrPs and myofascial pain.13,14 Suzuki et al and Ambite-Quesada et al go along with each other and state QST as a possibility to assess sensory alterations locally in MTrPs area and referred pain zone.13,14 Due to the fact that the patient works closely with the examiner during the QST, this test cannot be included in animal modelling.30 In animal models hypersensitivity is mainly verified by performing the mentioned behavioural tests. Therefore, it would be reasonable to develop a more precise method.
Involvements of ANS
Both Sugimoto and Hsieh investigated changes in the autonomic nervous system.22,23 Sugimoto et al have pointed out that through inhibition and excitation of the neurons in the central amygdala it is possible to control widespread mechanical sensitisation.22 Due to that, researchers claim the central amygdala is necessary in nociceptive pathways. Hsieh et al localised increased substance P-like immunoreactivity in central amygdala and parabrachium nuclei.23 Moreover, in their another study, authors confirm this association by decreasing substance P-like level due to therapy of MTrPs.31 Mentioned regions play an essential role in chronic pain processing and are also related to emotional processes.32 Therefore, Cao et al conducted a study on sympathetic nerve distribution and its activity in MTrPs based on a model established by Hsieh et al23,33 Researchers have demonstrated local hyperinnervation in MTrPs. These findings align with Rodrigues et al, who indicated that the sympathetic nervous system might also play an essential role in acetylcholine receptor stability.34 Depending on the Integrated Trigger Points Hypothesis, autonomic nervous system is involved in MTrPs phenomena.8 Both Hsieh et al and Sugimoto et al are going along with those findings as they stated the involvement of the Amygdala (and Parabrachial Nuclei in Hsieh et al), which partially regulates the autonomic nervous system.22,23 The involvement of the autonomic nervous system in MTrPs has also been investigated in human studies. Skorupska et al proposed a new method that demonstrates the autonomic vasomotor dysfunction due to dry needling of the MTrPs.35 These findings are preliminary, and demand further studies. The implementation of this method into animal models could be useful in imaging the area of pain sensation accompanied MTrPs. The studies mentioned previously point to the involvement of autonomic nervous systems in relation to myofascial trigger points and associated referred pain. In our opinion, these connections should be the main focus of future research models.
Involvement of CNS
Only one included study on nociplastic pain investigated the CNS involvement.26 Álvarez et al showed alterations in astrocyte activation in the spinal cord.26 The authors concluded that pain might cause subsequent synthesis and release of inflammatory mediators causing those changes. Therefore, increased neuronal activity can cause chronic pain by activating astrocytes.36 Widyadharma in his review suggested that alterations in astrocyte activation and reactive astrogliosis are sufficient in MTrPs creation.37 Models used by Álvarez et al were previously described as fibromyalgia pain models.26 In human studies, there was a confirmation that conditions like fibromyalgia are said to have greater comorbidity, eg higher number of MTrPs. In this case, it is in line with De las Peñas et al that myofascial trigger points are rather comorbidity in nociplastic states than the cause.12 It would be interesting to investigate this hypothesis, especially if myofascial trigger points itself can cause changes in CNS without previously induced conditions like fibromyalgia. This topic still remains unclear and needs further investigation.
Critical Appraisal of the Models
We conducted a critical appraisal based on SYRCLE’s risk of bias tool for animal studies (detailed assessment available in Supplementary Table 2).21 Answers to most signalling questions in our opinion was unclear. This increases the risk of bias. In the case of the works of Álvarez et al and Huang et al, this may be because the guidelines were created after the models had already been established.26,27 When creating new studies/models, it is important to follow the guidelines to improve the value and reliability of the study.
Strengths and Limitations
The strength of this work is a solid review of all available literature on this subject. We selected the most important results and drafted the methodology that was used. We relied on strict inclusion and exclusion criteria and presented a thorough search and data extraction process. In addition, we have shown the results obtained in the form of accessible tables and diagrams.
On the other hand, we found some limitations in our work. We did not analyse models describing disorders previously known as neuropathic or nociceptive but, actually, are classified as nociplastic (eg temporomandibular disorder, fibromyalgia, irritable bowel syndrome). However, the purpose of our study was to synthesise the outcomes of the studies on MTrPs and directly nociplastic pain. At last, we analysed only six papers. It is due to the novelty of the topic. In the future, review should be expanded and include new studies adapted to nociplastic pain.
Conclusion
This scoping review aims to bring all animal models on nociplastic pain and its connection to myofascial trigger points. As a result, we have systematised the current level of knowledge in this field. We compared all the papers with each other and pointed out possible correlations between nociplastic and myofascial pain. This type of pain is a relatively young field in medicine, and so far, how it occurs has yet to be developed. Our work can be used for research on developing a universal model that merges myofascial and nociplastic pain.
We consider that existing animal models are insufficient. It is reasonable to work on developing a new model that can be used to study nociplastic pain in accordance with MTrPs. Many studies point to the involvement of ANS in the pathomechanism of this type of pain. We know that tackling the study of AUN in animals is quite difficult. For example, the first work that demonstrated the existence of sympathetic innervation in neuromuscular synapses was published in 2016 and has only been reproduced in 2 more articles since then.38 The occurrence of referred pain could also be essential. An in vivo human study may be inaccurate and fraught with difficulties. We propose to refine the models outlined above to make them more reliable and trackable. Moreover, only Margalef et al presented modelling of MTrPs without muscle damage, which fits into the nociplastic pain definition.24 Perhaps adding a chronification factor to this model and using methods present in other studies will allow the creation of a universal model for nociplastic pain research.
In conclusion, there is insufficient evidence to describe myofascial trigger points as nociplastic. Further studies on animal models in the perspective of defining myofascial pain as nociplastic are demanded. It can lead to faster and more accessible research on this issue.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kosek E, Clauw D, Nijs J, et al. Chronic nociplastic pain affecting the musculoskeletal system: clinical criteria and grading system. Pain. 2021;162(11):2629–2634. doi:10.1097/J.PAIN.0000000000002324
2. Kosek E, Cohen M, Baron R, et al. Do we need a third mechanistic descriptor for chronic pain states? Pain. 2016;157(7):1382–1386. doi:10.1097/J.PAIN.0000000000000507
3. Nijs J, Lahousse A, Kapreli E, et al. Nociplastic pain criteria or recognition of central sensitization? Pain phenotyping in the past, present and future. J Clin Med. 2021;10(15):3203. doi:10.3390/jcm10153203
4. Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet. 2021;397(10289):2098–2110. doi:10.1016/S0140-6736(21)00392-5
5. Treede RD. Chronic musculoskeletal pain: traps and pitfalls in classification and management of a major global disease burden. Pain Rep. 2022;7(5):E1023. doi:10.1097/PR9.0000000000001023
6. Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Chronic primary musculoskeletal pain: a new concept of nonstructural regional pain. Pain Rep. 2022;7(5). doi:10.1097/PR9.0000000000001024
7. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/J.PAIN.0000000000001384
8. Travell JG, Simons DG. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual.
9. Skorupska E, Jokiel M, Rychlik M, Łochowski R, Kotwicka M. Female Overrepresentation in Low Back-Related Leg Pain: a Retrospective Study of the Autonomic Response to a Minimally Invasive Procedure. J Pain Res. 2020;13:3427–3435. doi:10.2147/JPR.S282233
10. Skorupska E, Dybek T, Rychlik M, Jokiel M, Zawadziński J, Dobrakowski P. Amplified Vasodilatation within the Referred Pain Zone of Trigger Points Is Characteristic of Gluteal Syndrome-A Type of Nociplastic Pain Mimicking Sciatica. J Clin Med. 2021;10(21):5146. doi:10.3390/JCM10215146
11. Doménech-García V, Peirotén AR, Imaz ML, Palsson TS, Herrero P, Bellosta-López P. Not just sensitization: sympathetic mechanisms contribute to expand experimental referred pain. Korean J Pain. 2022;35(3):240–249. doi:10.3344/KJP.2022.35.3.240
12. Fernández-de-las-Peñas C, Nijs J, Cagnie B, et al. Myofascial Pain Syndrome: a Nociceptive Condition Comorbid with Neuropathic or Nociplastic Pain. Life. 2023;13(3):694. doi:10.3390/life13030694
13. Ambite-Quesada S, Arias-Buría JL, Courtney CA, Arendt-Nielsen L, Fernández-De-Las-Peñas C. Exploration of Quantitative Sensory Testing in Latent Trigger Points and Referred Pain Areas. Clin J Pain. 2018;34(5):409–414. doi:10.1097/AJP.0000000000000560
14. Suzuki H, Tahara S, Mitsuda M, et al. Current Concept of Quantitative Sensory Testing and Pressure Pain Threshold in Neck/Shoulder and Low Back Pain. Healthcare. 2022;10(8):1485. doi:10.3390/HEALTHCARE10081485
15. Barré-Sinoussi F, Montagutelli X. Animal models are essential to biological research: issues and perspectives. Future Sci OA. 2015;1(4). doi:10.4155/FSO.15.63
16. Robinson NB, Krieger K, Khan F, et al. The current state of animal models in research: a review. Int J Surgery. 2019;72:9–13. doi:10.1016/J.IJSU.2019.10.015
17. Abboud C, Duveau A, Bouali-Benazzouz R, et al. Animal models of pain: diversity and benefits. J Neurosci Methods. 2021;348:108997. doi:10.1016/J.JNEUMETH.2020.108997
18. Kaliyaperumal S, Wilson K, Aeffner F, Dean C. Animal Models of Peripheral Pain: biology Review and Application for Drug Discovery. Toxicol Pathol. 2020;48(1):202–219. doi:10.1177/0192623319857051
19. Huang X, Lin J, Demner-Fushman D. Evaluation of PICO as a Knowledge Representation for Clinical Questions. AMIA Ann Symposium Proce. 2006;2006:359.
20. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
21. Hooijmans CR, Rovers MM, De Vries RBM, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol. 2014;14(1). doi:10.1186/1471-2288-14-43
22. Sugimoto M, Takahashi Y, Sugimura YK, Tokunaga R, Yajima M, Kato F. Active role of the central amygdala in widespread mechanical sensitization in rats with facial inflammatory pain. Pain. 2021;162(8):2273–2286. doi:10.1097/j.pain.0000000000002224
23. Hsieh YL, Wu BT, Yang CC. Increased substance P-like immunoreactivities in parabrachial and amygdaloid nuclei in a rat model with masticatory myofascial pain. Exp Brain Res. 2020;238(12):2845–2855. doi:10.1007/s00221-020-05942-4
24. Margalef R, Sisquella M, Bosque M, et al. Experimental myofascial trigger point creation in rodents. J Appl Physiol. 2019;126(1):160–169. doi:10.1152/japplphysiol.00248.2018
25. Hankerd K, McDonough KE, Wang J, Tang SJ, Chung JM, La JH. Postinjury stimulation triggers a transition to nociplastic pain in mice. Pain. 2022;163(3):461–473. doi:10.1097/j.pain.0000000000002366
26. Álvarez-Pérez B, Deulofeu M, Homs J, et al. Long-lasting reflexive and nonreflexive pain responses in two mouse models of fibromyalgia-like condition. Sci Rep. 2022;12(1). doi:10.1038/s41598-022-13968-7
27. Huang QM, Ye G, Zhao ZY, Lv JJ, Tang L. Myoelectrical activity and muscle morphology in a rat model of myofascial trigger points induced by blunt trauma to the vastus medialis. Acupuncture Med. 2013;31(1):65–73. doi:10.1136/acupmed-2012-010129
28. Nagakura Y, Takahashi M, Noto T, et al. Different pathophysiology underlying animal models of fibromyalgia and neuropathic pain: comparison of reserpine-induced myalgia and chronic constriction injury rats. Behav Brain Res. 2012;226(1):242–249. doi:10.1016/j.bbr.2011.09.023
29. Sharma NK, Ryals JM, Liu H, Liu W, Wright DE. Acidic Saline-Induced Primary and Secondary Mechanical Hyperalgesia in Mice. J Pain. 2009;10(12):1231–1241. doi:10.1016/j.jpain.2009.04.014
30. Mücke M, Cuhls H, Radbruch L, et al. Quantitative sensory testing (QST). English version. Schmerz. 2021;35(Suppl 3):153–160. doi:10.1007/S00482-015-0093-2
31. Hsieh YL, Yang CC, Yang NP. Ultra-Low Frequency Transcutaneous Electrical Nerve Stimulation on Pain Modulation in a Rat Model with Myogenous Temporomandibular Dysfunction. Int J Mol Sci. 2021;22(18):9906. doi:10.3390/IJMS22189906
32. Kato F, Sugimura YK, Takahashi Y. Pain-Associated Neural Plasticity in the Parabrachial to Central Amygdala Circuit: pain Changes the Brain, and the Brain Changes the Pain. Adv Exp Med Biol. 2018;1099:157–166. doi:10.1007/978-981-13-1756-9_14
33. Cao L, Gao Y, Wu K, Li Y, Chen C, Yuan S. Sympathetic hyperinnervation in myofascial trigger points. Med Hypotheses. 2020;139. doi:10.1016/J.MEHY.2020.109633
34. Rodrigues ACZ, Messi ML, Wang ZM, et al. The sympathetic nervous system regulates skeletal muscle motor innervation and acetylcholine receptor stability. Acta Physiol. 2019;225(3). doi:10.1111/APHA.13195
35. Skorupska E, Dybek T, Rychlik M, Jokiel M, Dobrakowski P. The Automatization of a New Thermography Method Using Invasive Nociceptive Stimulation to Confirm an Autonomic Phenomenon within a Trigger Point Referred Pain Zone. Brain Sci. 2021;11(7):893. doi:10.3390/brainsci11070893
36. Lu HJ, Gao YJ. Astrocytes in Chronic Pain: cellular and Molecular Mechanisms. Neurosci Bull. 2022;39(3):425–439. doi:10.1007/s12264-022-00961-3
37. Widyadharma IPE. The role of oxidative stress, inflammation and glial cell in pathophysiology of myofascial pain. Postepy Psychiatrii i Neurologii. 2021;29(3):180–186. doi:10.5114/PPN.2020.100036
38. Majid Khan M, Lustrino D, Silveira WA, et al. Sympathetic innervation controls homeostasis of neuromuscular junctions in health and disease. Proc National Acad Sci. 2016;113(3):746. doi:10.1073/pnas.1524272113
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation by Survival Analysis of Cold Pain Tolerance in Patients with Fibromyalgia and Opioid Use
Deng EZ, Weikel DP, Martucci KT
Journal of Pain Research 2022, 15:2783-2799
Published Date: 9 September 2022
Sympathetic-Sensory Coupling as a Potential Mechanism for Acupoints Sensitization
Cui X, Zhang Z, Xi H, Liu K, Zhu B, Gao X
Journal of Pain Research 2023, 16:2997-3004
Published Date: 30 August 2023
Differences in Experimental Pain Sensitivity Between Non-African and African American Healthy Individuals and Patients with Painful Chronic Pancreatitis
Phillips AE, Faghih M, Ramsey ML, Han S, Hart PA, Afghani E, Bick BL, Easler JJ, Yadav D, Wilcox CM, Olesen SS, Drewes AM, Singh VK
Journal of Pain Research 2026, 19:562097
Published Date: 25 February 2026