Back to Journals » Journal of Pain Research » Volume 19
Evaluating the Effect of Electroacupuncture in Knee Osteoarthritis: Protocol for a Multicenter Randomized Controlled Trial
Authors Chen Y ![]() , Xie H, Ye M, Zhang L, Yuan A
, Xie H, Ye M, Zhang L, Yuan A ![]()
Received 3 March 2026
Accepted for publication 9 April 2026
Published 16 April 2026 Volume 2026:19 606479
DOI https://doi.org/10.2147/JPR.S606479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Yiming Chen,1,2 Hongyu Xie,1 Min Ye,1 Lele Zhang,1 Aihong Yuan1,2
1Department of Acupuncture, The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui, 230031, People’s Republic of China; 2Key Laboratory of Xin’an Medicine, Ministry of Education, Hefei, Anhui, 230038, People’s Republic of China
Correspondence: Aihong Yuan, Department of Acupuncture, The First Affiliated Hospital of Anhui University of Chinese Medicine, 117 Meishan Road, Shushan District, Hefei, Anhui, 230031, People’s Republic of China, Email [email protected]
Background & Objective: Knee osteoarthritis (KOA) is a degenerative disease of the knee joint. Current treatment strategies face considerable limitations. For thousands of years, acupuncture has been used in China to treat KOA due to its unique advantages. However, existing studies often rely excessively on subjective perception for outcome assessment, and the central neural mechanisms by which acupuncture alleviates chronic pain in KOA remain unclear. Our aim is to elucidate the efficacy and central mechanisms of acupuncture for KOA.
Methods: In this multicenter, patient- and assessor-blind, superiority, randomized controlled neuroimaging trial, 110 patients with KOA will be randomly assigned in a 1:1 ratio to an electroacupuncture group or a sham electroacupuncture group. Participants are patients with KOA aged between 50 and 75 years who have experienced chronic knee pain for the past three months. Participants will be randomized using a stratified block randomization method, followed by automatic allocation through an electronic system. The trial is scheduled to be conducted from March 2024 to September 2026, and participants will be recruited from the First Affiliated Hospital of Anhui University of Chinese Medicine, Anhui Provincial Hospital, and Bozhou Chinese Medicine Hospital. Treatment will be administered in six sessions over two weeks. Patients will undergo assessments and examinations at baseline and after the completion of treatment. The primary outcome measure is the Clinical Global Impressions scale - Improvement. Secondary outcomes include the Visual Analogue Scale, pressure pain threshold, Knee Injury and Osteoarthritis Outcome Score, Patients’ expectancy scale of acupuncture, Self-Rating Anxiety Scale, Self-Rating Depression Scale, functional magnetic resonance imaging (fMRI). A multimodal imaging protocol will be employed for fMRI. Differences in brain functional–structural information and brain network connectivity patterns before and after acupuncture will be comprehensively analyzed. Correlations between neural markers and patients’ subjective experiences will be examined. For clinical outcomes, categorical variables will use the chi-square test, and continuous variables will use the t-test or the Mann–Whitney U-test. For fMRI data, a general linear model will be used for between-group comparisons.
Discussion: This multicenter randomized controlled neuroimaging trial integrates validated subjective assessment tools with multimodal fMRI to multidimensionally evaluate the efficacy of acupuncture for KOA. We believe the forthcoming comprehensive results will provide a unified interpretation of the central effects of acupuncture.
Keywords: knee osteoarthritis, acupuncture, randomized controlled trial, CGI-I, fMRI
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Chen has been published for this article.
Introduction
Knee osteoarthritis (KOA) is a chronic degenerative disease characterized by knee pain and functional impairment.1 In 2021, an estimated 607 million individuals worldwide had osteoarthritis (OA), with an age-standardized prevalence rate of 7%.2 With the aging global population and rising obesity rates, the number of OA patients is projected to reach 1.2 billion by 2050, with 41.6 million years lived with disability.3 The high incidence and disability rate of KOA not only diminish patients’ quality of life (QoL) but also impose a substantial social burden.
Chronic pain in KOA is characterized by neuropathic mechanisms, involving dual sensitization of the peripheral and central nervous systems driven by inflammation and structural changes, and is associated with emotional, sensory, and cognitive factors.4–6 These processes may lead to the remodeling of brain structure and function, resulting in a vicious cycle of persistent pain.7 Due to this complex pain mechanism, current therapeutic strategies for KOA face major limitations. The mainstream treatment options for moderate-to-advanced KOA are medication and surgery. Although these interventions can alleviate symptoms, they have notable drawbacks regarding adverse effects and costs.8 Most importantly, they fail to reliably control chronic pain and improve joint function.
Acupuncture, a traditional therapeutic approach with a long history, is now widely accepted internationally.9 It has been used to treat KOA in China for thousands of years due to its unique advantages of effectiveness, convenience, and safety. A systematic review of international clinical practice guidelines for chronic musculoskeletal pain conditions found that 60% of the guidelines recommend acupuncture.10 Shuci theory, a guiding method in ancient Chinese medicine for treating Gubi, emphasizes deep needling of acupoints near the knee joint until reaching the bone surface to deliver a strong stimulus. Gubi, the ancient Chinese term for KOA, was considered a disease caused by long-term blood stasis blocking the knee joint, requiring strong stimulation for effective treatment.
Notably, modern acupuncturists have integrated it with controlled, regular electrical stimulation to develop electroacupuncture (EA), which further enhances its therapeutic efficacy.11 For KOA, although EA has inherent limitations such as considerable individual response variability and a lack of standardization of optimal stimulation parameters, its favorable safety, low cost, and multi-system, multi-target effects warrant greater attention. A review published in the Journal of Pain Research12 indicated that EA can directly relieve pain by modulating the central and peripheral nervous systems, as well as improve local inflammatory signals, hemodynamics, and cartilage metabolism in the knee joint.
However, in existing studies on acupuncture for KOA, outcome assessment has often relied excessively on various subjective perception scales, leading some to remain skeptical about the level of evidence for its effectiveness.13 An objective and quantifiable outcome assessment tool is needed to further enhance the credibility of the evidence.14 Meanwhile, the central neural mechanisms through which acupuncture improves chronic pain in KOA remain unclear, which limits its broader clinical adoption.15
With the widespread application of neuroimaging techniques in pain research, functional magnetic resonance imaging (fMRI) has demonstrated its advanced capabilities.16 For instance, using fMRI, researchers have observed robust activation in the dorsal anterior insula, midcingulate cortex, and medial frontal gyrus in patients with chronic primary pain.17 Cheng et al confirmed that patients with KOA exhibit reduced functional network connectivity (FNC) within the default mode network (DMN), visual network (VN), and cerebellar network, alongside increased FNC between the subcortical network and the VN.18 A randomized controlled trial (RCT) on acupuncture for migraine19 revealed that acupuncture can modulate neural activity within the DMN, VN, and sensory motor network (SMN), and that these neural changes are associated with improvements in pain and QoL. Multimodal fMRI, which simultaneously assesses neural features of structure, function, connectivity, and metabolism, provides a more comprehensive framework than single-sequence imaging and enables subsequent analysis for robust cross-validation.20 In summary, central biomarkers derived from multimodal fMRI enable us to interpret the effects of acupuncture on the brain from a neuroscientific perspective.
Currently, few studies have integrated subjective assessment tools with multimodal fMRI to conduct a multi-dimensional analysis of the efficacy and mechanisms of acupuncture for KOA.15 Here, we designed the RCT protocol based on two interrelated scientific questions: whether EA can lead to clinically meaningful improvements in KOA compared to sham EA, and whether these improvements are associated with specific, measurable changes in brain structure and function. We will observe the effectiveness of acupuncture for KOA using various subjective perception scales, and then interpret its effects on the central nervous system based on neuroimaging. Finally, changes in subjective perception and the central system will be correlated. The hypothesis of the study is that, compared with sham EA, EA can better improve symptoms and quality of life in patients with KOA, and that this effect arises from the specific regulatory action of EA on the central system. We believe that this study will elucidate the efficacy and central mechanisms of acupuncture for KOA, provide evidence-based support for optimizing comprehensive treatment strategies, and offer KOA patients improved therapeutic options.
Methods and Design
Study Design
This trial will employ a multicenter, patient- and assessor-blind, superiority, randomized controlled design. Eligible patients with KOA will be recruited from three centers. Using a stratified block randomization method, participants will be allocated in a 1:1 ratio to either the EA group or the sham EA (SEA) group. The study is planned to be conducted from March 2024 to September 2026. Participants will undergo examinations and assessments at baseline (weeks 0) and after the completion of treatment at week 2. Additionally, 30 healthy adults will be recruited as a healthy control group for brain image standardization and auxiliary processing. This protocol adheres to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines Figure 1 presents the Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
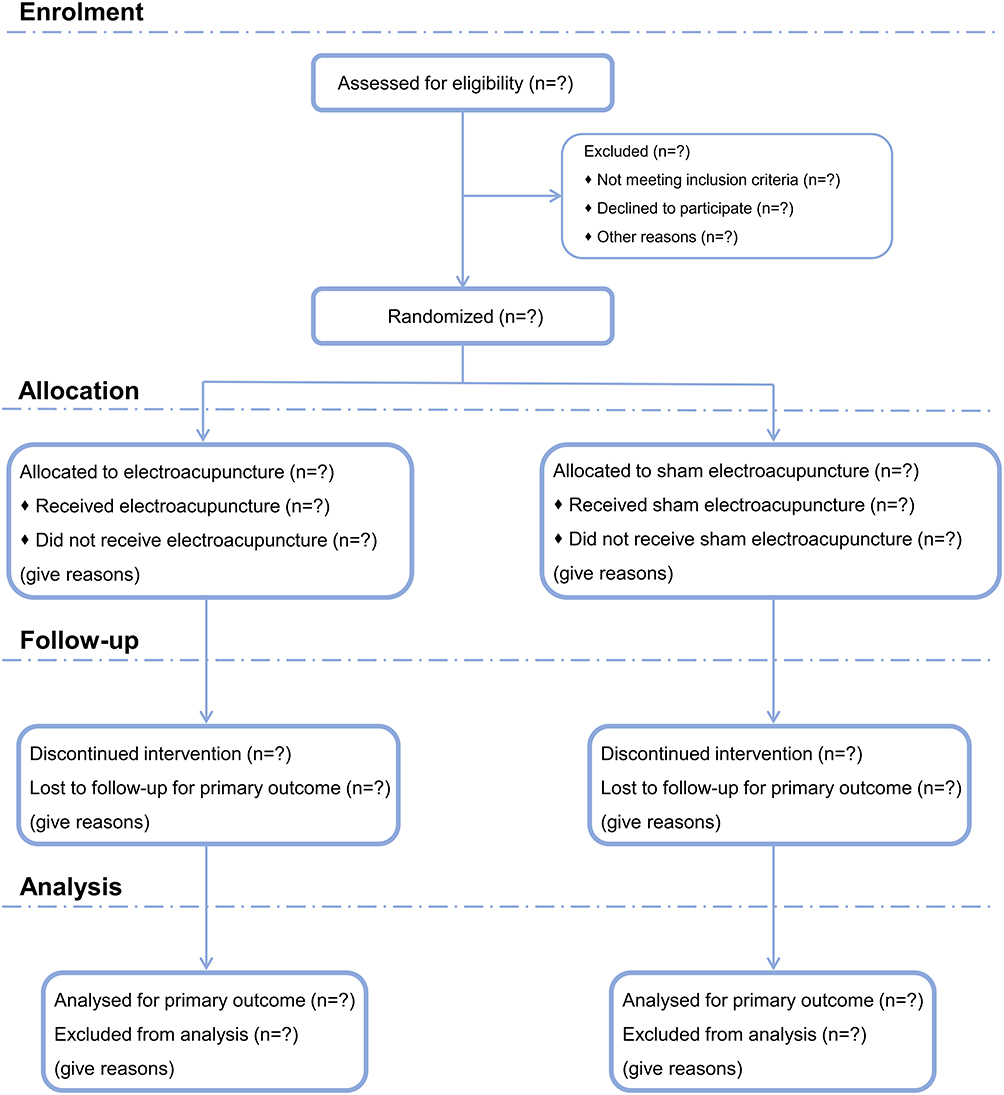 |
Figure 1 The Consolidated Standards of Reporting Trials flow diagram. Notes: The symbol “?” represents the number of uncertain cases in the trial (because of the current protocol phase). |
Ethics, Informed Consent, and Anonymization
All procedures in this trial were performed in accordance with the ethical requirements of the Declaration of Helsinki and all applicable governmental and institutional regulations regarding human volunteers. Protocol registration: https://www.chictr.org.cn, ChiCTR2300078135, 29 November 2023. The trial was approved by the Ethics Committee of the First Affiliated Hospital of Anhui University of Chinese Medicine (2023AH-61). All participants will provide written informed consent after being fully informed about all trial procedures and after having adequate time to consider their participation. All patient data were handled with the utmost confidentiality in accordance with applicable data protection regulations. Identifiable information was anonymized to ensure privacy and security throughout the research process.
Participants and Criteria
Participants in this trial will be patients recruited from the First Affiliated Hospital of Anhui University of Chinese Medicine, Anhui Provincial Hospital, and Bozhou Chinese Medicine Hospital. Recruitment advertisements will be disseminated through channels such as WeChat, websites, and hospitals. Eligibility of potential participants will be assessed by trained recruiters with extensive clinical experience using strict inclusion and exclusion criteria. All diseases will be diagnosed by senior specialist physicians at the time of recruitment after inquiring about and reviewing the patient’s symptoms, signs, laboratory tests, and medical history. Diagnoses will also refer to the patient’s previous medical records from any healthcare facility. These senior specialist physicians have more than ten years of clinical experience in their specialty and will not be involved in any other aspect of the trial.
Diagnosis Criteria
The diagnosis of KOA will be made with reference to the American College of Rheumatology’s Classification of Osteoarthritis of the Knee21 and the 2024 Chinese guidelines for diagnosis and treatment of osteoarthritis.22 The International Classification of Diseases 10th Revision codes for KOA include M17.0, M17.10, M17.11, and M17.12. Specifically, a diagnosis can be established if criterion ① is met, along with any two of the others:
① Recurrent knee pain within the last month;
② Age ≥ 50 years;
③ Morning knee stiffness ≤ 30 minutes;
④ Bony crepitus with knee joint movement;
⑤ X-ray showed narrowing of the knee joint space, subchondral bone sclerosis or cystic changes, and osteophyte formation at the joint margins.
Inclusion Criteria
① Met the diagnostic criteria;
② Aged between 50 and 75 years;
③ Persistent knee pain over the past three months;
④ Visual Analogue Scale (VAS) ≥ 4.0;
⑤ No acupuncture treatment in the past three months;
⑥ Informed consent and good compliance.
Exclusion Criteria
① Presence of other musculoskeletal disorders;
② Presence of psychiatric, cerebrovascular, or neurological diseases;
③ Use of medications affecting mental state, cognition, pain perception, or brain function within the past three months;
④ Pregnancy, lactation, or plans for pregnancy in the near future;
⑤ Lower limb deformities or disabilities affecting normal walking;
⑥ Had undergone knee joint injection and surgery within the past six months;
⑦ Contraindications for fMRI examination;
⑧ Current or planned participation in other clinical trials.
Withdrawal Criteria
① Inability to cooperate or lost contact to various reasons;
② Severe adverse reactions, complications, or disease progression;
③ Poor compliance or failure to adhere to the treatment protocol;
④ Receipt of additional acupuncture, knee joint injections, or surgery during the study period;
⑤ Breaking of the blind.
Inclusion Criteria for Healthy Controls
① Aged between 50 and 75 years;
② No chronic pain in the past three months;
③ Free from musculoskeletal, psychiatric, cerebrovascular, or neurological diseases;
④ No use of medications affecting mental state, cognition, pain perception, or brain function in the past three months;
⑤ No acupuncture received in the past three months;
⑥ Willingness to undergo fMRI examination.
Enhancing Compliance
To mitigate the impact of participant withdrawal on study quality, we will enhance participant compliance through multiple strategies:
① Maintaining contact with participants to remind them of treatment schedules;
② Scheduling treatments and assessments at convenient times to minimize disruption to their daily lives;
③ Compensating participants for lost wages and travel expenses, while waiving all treatment fees;
④ Promptly addressing any study-related concerns raised by participants.
Randomization, Allocation Concealment, and Blinding
Table 1 presents the schedule of tasks for participants. Randomization in this study will be performed using a stratified block randomization method, with stratification factors being center and disease duration. Within each stratum, the block size is set to either 4 or 6, and the allocation ratio is 1:1. A statistician will generate random numbers and a random allocation table using a randomization system. The statistician will input the participants’ stratification data into the system, which will then automatically assign group allocations, denoted by the “A” or “B”.
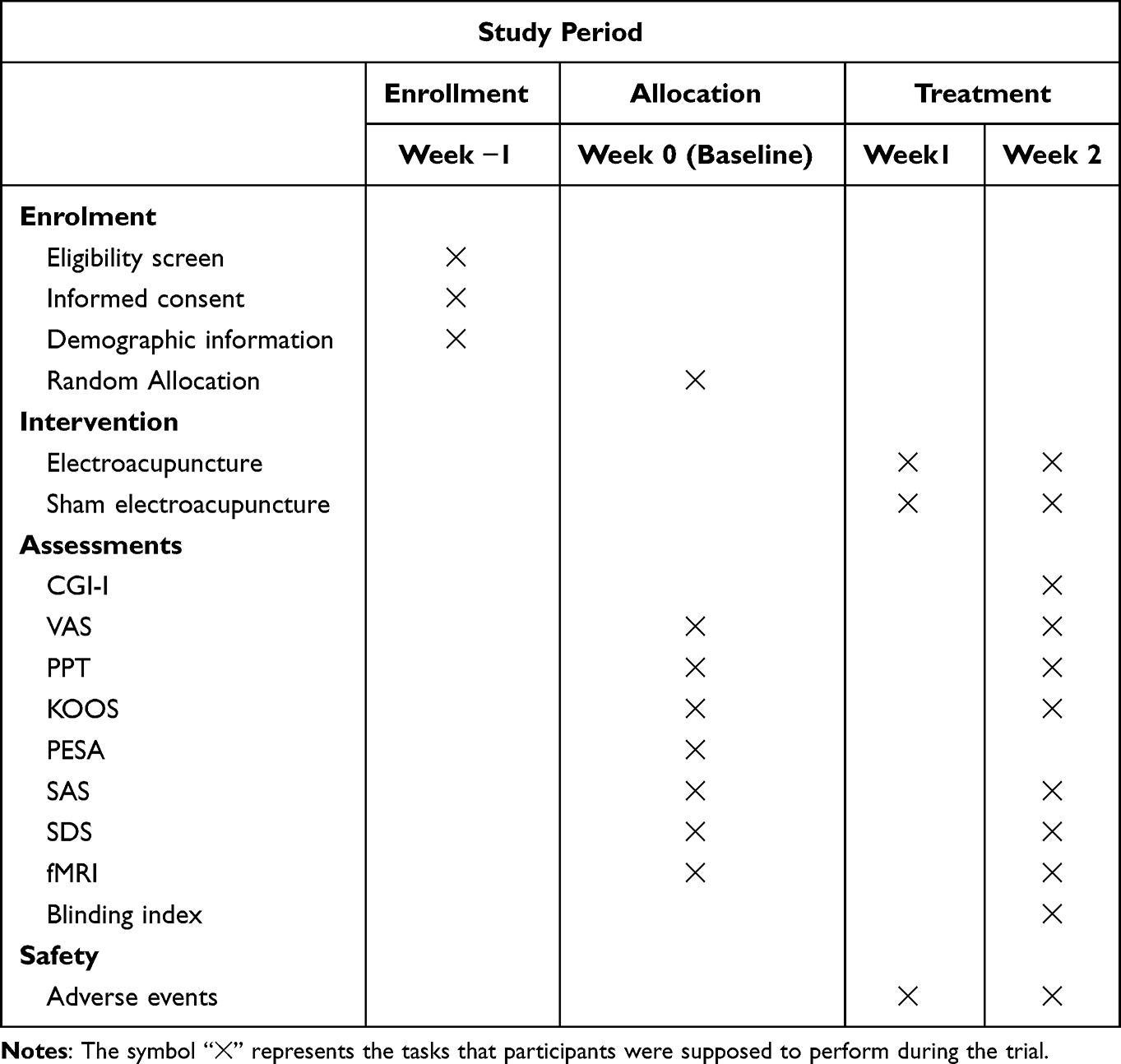 |
Table 1 Schedule of Tasks for Participants |
Due to the inherent nature of acupuncture, only the acupuncturists were aware of the participants’ letter group (“A” or “B”) and the corresponding treatment regimens. However, the acupuncturists were not involved in recruitment, allocation, assessment, or analysis. Outcome assessments were conducted by assessors, who completed the case report forms and entered the data into electronic spreadsheets. All personally identifiable information was concealed, with only the letter group retained. Finally, a statistician performed the statistical analysis. The recruiter, acupuncturists, assessors, and statisticians operated independently and did not communicate.
To prevent communication between participants that could lead to unblinding, the two groups were treated at separate locations. After the treatment period, all participants were asked to guess which type of acupuncture they had received. The success of blinding was assessed using Bang’s Blinding Index (BBI).23 “BBI = 0” indicates completely random guessing, while “BBI ∈ [−0.2, 0.2]” or a similar absolute BBI value between the two groups suggests successful blinding. The BBI is calculated using the following formula:


Interventions
Electroacupuncture Group
Participants will wear an eye mask in the supine position, and the local skin will be sterilized. The acupoints Neixiyan (EX-LE4), Dubi (ST35), Yanglingquan (GB34), Yinlingquan (SP9), Zusanli (ST36), and Xuehai (SP10) be selected. The international standard locations of these acupoints are provided in Table 2. In accordance with the “Shuci” theory from traditional Chinese medicine (TCM) for treating KOA, the needles will be inserted towards the knee joint until reaching the periosteum. For patients with bilateral KOA, needles will be inserted bilaterally; for unilateral KOA, needles will be inserted only on the affected side. Sterile foam pads with adhesive surfaces (2 cm × 2 cm × 1 cm) will be affixed to the skin. Needles (0.35 mm × 50 mm) will then be inserted through the pads into the acupoints until contacting the periosteum. Twirling, lifting and thrusting of the needles will be performed to elicit the “deqi” sensation. Subsequently, an electroacupuncture device will be connected to the needles at Neixiyan and Dubi, with the parameters set to dense-and-sparse wave, frequency of 2/100 Hz, and intensity of 2 mA. Needles will be retained for 30 minutes. The treatment will be administered three times per week for two consecutive weeks. Acetaminophen was administered as needed, except 48 hours before outcome assessment.
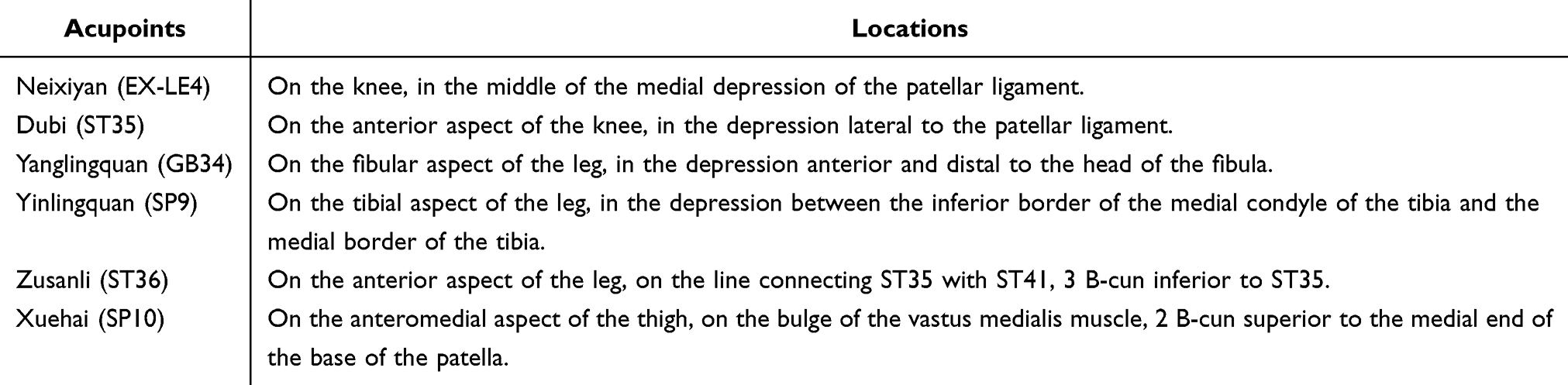 |
Table 2 The Location of the Acupoints |
Sham Electroacupuncture Group
SEA serves as a placebo-control, utilizing a customized blunt-tip needle. The needle will be inserted through pads to contact the skin surface without penetrating it, remaining upright via the pads and applying consistent pressure to the skin. The electroacupuncture device will also be connected and electrodes will be attached to the needles, but not powered. Patients will be able to hear the “click” of the device’s mechanical timer. To optimize blinding, all patients will be informed that the current intensity may be below the threshold of human perception. All other procedures for SEA will be identical to EA. Figure 2 illustrates the intervention for the two groups.
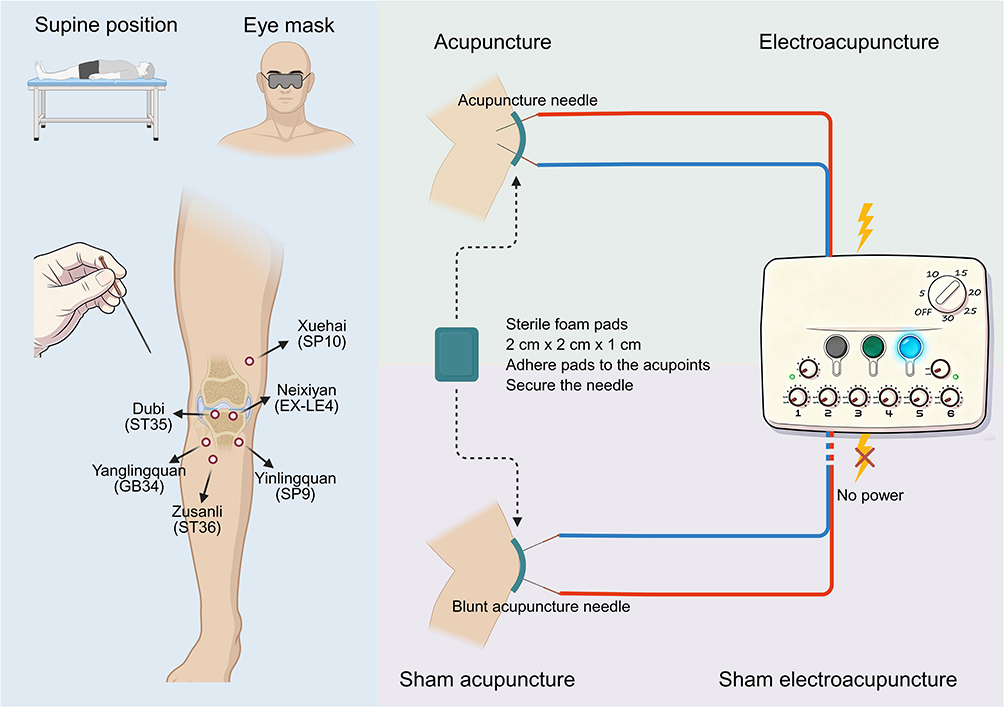 |
Figure 2 Schematic representation of the intervention for both groups. |
Outcomes
At baseline and after 2 weeks of treatment, an assessor will conduct face-to-face interviews with each participant, supervise the completion of the scales, and guide them through the examinations. All quantitative results will be entered into an electronic spreadsheet.
Primary Outcome
The primary outcome of this study is the self-assessment of treatment outcome measured by the Clinical Global Impressions scale - Improvement (CGI-I).24 The CGI-I is a single-item, 7-point scale originally published in the ECDEU Assessment Manual for Psychopharmacology25 by the U.S. Department of Health, Education, and Welfare in 1976. It is now primarily used to quantify a patient’s self-perceived global improvement of their condition following treatment. Specifically, a score of 1 indicates very much improved; 2, much improved; 3, minimally improved; 4, no change; 5, minimally worse; 6, much worse; and 7, very much worse. We define CGI-I ≤ 2 as indicating effective treatment. Time required: 1 minutes.
Secondary outcomes
① VAS:26 One of the most common methods for quantifying pain perception. Patients are asked to mark their perceived pain level on a 10 cm straight line, with 0 representing no pain and 10 representing the most intense pain. Time required: 1 minutes.
② Pressure pain threshold (PPT):27 PPT is the minimum pressure value applied that first elicits a sensation of pain in the participant, measured using an algometer. It serves as an objective indicator for assessing mechanical pain sensitivity and directly reflects the degree of pain sensitization. Time required: 3 minutes.
③ Knee injury and osteoarthritis outcome score (KOOS):28 It is a self-reported instrument specifically designed for patients with knee injury and osteoarthritis, assessing function and quality of life. It comprises five subdomains: Pain, Symptoms, Activities of Daily Living, Sport and Recreation Function, and Knee-related Quality of Life. This scale provides a comprehensive evaluation of knee condition and function. Each domain is scored on a 100-point scale, where 100 indicates no problems. Time required: 5 minutes.
④ Patients’ expectancy scale of acupuncture (PESA):29 PESA is a tool specifically designed to assess patients’ expectations regarding acupuncture treatment before its initiation. It helps clarify the influence of psychological effects on treatment outcomes and aids in isolating the specific physiological effects of acupuncture. The scale comprises 11 items, each with 5 options corresponding to scores of 1 to 5. Higher scores indicate a more positive attitude toward acupuncture. Time required: 2 minutes.
⑤ Self-rating anxiety scale (SAS):30 A widely used instrument for assessing the severity of a patient’s subjective feelings of anxiety. Standardized scores range from 25 to 100, with higher scores indicating more severe anxiety. Time required: 3 minutes.
⑥ Self-rating depression scale (SDS):31 One of the most widely used self-report instruments for depression internationally. Standardized scores range from 25 to 100, with higher scores indicating more severe depression. Time required: 3 minutes.
fMRI
In the 72 hours prior to the scan, participants are required to maintain a regular lifestyle and refrain from consuming alcohol, coffee, and tea. Thirty minutes before the scan, participants need to rest in quiet solitude. Foam earplugs and sponge padding will be used to attenuate scanner noise and minimize head motion, respectively. Participants are instructed to keep their eyes closed, remain awake, and hold their body still. If unbearable discomfort is experienced during the scan, the procedure will be immediately terminated. All data were acquired on a Siemens Prisma 3.0 T MRI scanner using a multimodal imaging protocol. The specific sequences and parameters are as follows:
High-resolution three-dimensional T1-weighted (T1W): Serves as the anatomical basis for fine brain structure segmentation, cortical thickness analysis, and multimodal image registration. The acquisition parameters are as follows: TR/TE/TI ≈ 8 ms/3 ms/900 ms; flip angle: 8°-12°; spatial resolution: 1.0 mm3 isotropic; FOV: 256 mm × 256 mm; matrix: 256 × 256; slices/thickness: 176 slices/1.0 mm. The scan duration is 5 minutes.
Resting-state fMRI (rs-fMRI): Assess changes in spontaneous neural activity and functional connectivity before and after acupuncture. The acquisition parameters are as follows: TR/TE: 2000 ms/30 ms; flip angle: 90°; spatial resolution: 3.0 mm3 or 3.5 mm3 isotropic; FOV: 224 mm × 224 mm; matrix: 64 × 64; slices/thickness: 40–45 slices/3.0 mm (no gap). The scan duration is 10 minutes.
Diffusion-weighted imaging (DWI): Assess the integrity and connectivity of white matter tracts. The acquisition parameters are as follows: TR/TE: 8000–10000 ms/80-90 ms; spatial resolution: 2.0 mm3 isotropic; FOV: 256 mm × 256 mm; matrix: 128 × 128; slices/thickness: 70 slices/2.0 mm (no gap). For b-values, at least 5–10 volumes without diffusion weighting (b = 0 s/mm2) are acquired, and diffusion gradients are applied in 64 non-collinear directions at b = 1000 s/mm2. The scan duration is 10 minutes.
Meshcher-Garwood point resolved spectroscopy (MEGA-PRESS): To quantify neurotransmitter concentrations in specific brain regions (eg., anterior cingulate cortex, thalamus, primary sensorimotor cortex). TR/TE: 2000 ms/68 ms. Voxel size: 3.0 cm × 3.0 cm × 3.0 cm (27 mL). Number of acquisitions: 192–256 averages. Scan duration: 12 minutes.
Adverse Events and Safety Assessment
Common adverse events (AEs) include post-needling pain, dizziness, and subcutaneous hemorrhage. In the event of an AE, we will promptly take necessary measures to ensure patient safety. All AEs will be assessed and documented by the acupuncturist (CTCAE v5.0) and reported to the ethics committee within 12 hours. The incidence of AEs will be compared between groups to determine the safety of acupuncture.
Sample Size Calculation
Considering the superiority design of this study, we estimated the sample size based on the response rates defined by CGI-I ≤ 2. The calculation was performed using the R package TrialSize. According to previous studies on acupuncture for KOA,11,32 the response rate ranged from 45.0% to 60.3% in trial group and from 30.8% to 47.3% in control group. A clinically meaningful difference in response rate was considered to be at least 20%. Using a two-sided chi-square test with α = 0.05 and 80% power, the calculated sample size was at least 94 participants (47 per group). Accounting for a 15% dropout rate, the final sample size was set at 110 participants (55 per group).
Monitoring and Amendments
A two-level quality review system will be established to ensure project implementation and quality. Independent monitors at each center will conduct quality reviews monthly, and the monitoring team will conduct reviews quarterly. Following each quality review, a quality control report shall be submitted to the ethics committee, which will decide whether to continue or terminate the trial. The independent monitors and monitoring team will not participate in any trial procedures other than monitoring.
Standardized training sessions will be provided to all centers to ensure adherence to the study protocol and familiarity with the management procedures. All personnel must possess the relevant qualifications and have completed the training. All study documents will be retained for five years after trial completion. Any modifications to the study protocol will be reported to and approved by the ethics committee.
Dissemination
The study findings will be published in peer-reviewed journals or presented at scientific conferences.
Data Processing & Statistical Analysis
Preprocessing of high-resolution T1W structural images (bias field correction, skull stripping, segmentation of gray matter/white matter/cerebrospinal fluid, and cortical surface reconstruction) will be performed using FSL and FreeSurfer software. These processed images will provide spatial templates for subsequent multimodal data fusion.
Preprocessing of rs-fMRI data will be conducted using SPM12 and the CONN toolbox. The first 10 time points will be discarded to account for magnetic field instability, followed by slice-timing correction and head motion correction. Head motion will be assessed using framewise displacement (FD) calculated from the six rigid-body motion parameters. The following exclusion criteria will be applied: any scan with a mean FD > 0.5 mm will be excluded; any time point (volume) with FD > 0.2 mm will be removed from the time series (scrubbing); if the proportion of removed time points exceeds 10% of the total time points, the entire scan will be excluded. Functional images will be co-registered to each individual’s T1-weighted structural image and further normalized to MNI space, resampled to 3 mm3 voxels. For functional connectivity analysis, seed regions related to pain processing (eg., default mode network, salience network, anterior cingulate cortex, thalamus) will be selected. Temporal correlations between the time series of these seeds and all other voxels across the whole brain will be computed to generate seed-based functional connectivity maps at the individual level. To remove confounding signals from the data, the following nuisance regressors will be included in the general linear model: head motion parameters, white matter signal, cerebrospinal fluid signal, linear and quadratic trends, and scrubbed volumes. All nuisance regressors will be applied before bandpass filtering (0.01–0.1 Hz).
DWI data will be preprocessed and analyzed using MRtrix3 and FSL. Whole-brain white matter fiber tracts will then be reconstructed using deterministic fiber tracking algorithms. Microstructural indices, including fractional anisotropy and mean diffusivity, will be calculated for voxel-based or tract-based statistical analysis.
Single-voxel MEGA-PRESS spectroscopy data will be processed using the Gannet toolbox to obtain final neurotransmitter concentrations.
Based on the existing literature on neurobiological studies for KOA,14,33–35 we propose the following a priori hypotheses: compared with SEA, ① EA will significantly increase functional connectivity between DMN and sensorimotor network; ② EA will increase fractional anisotropy in the corpus callosum and cingulate gyrus, reflecting improved structural integrity of pain-related pathways; ③ EA will increase GABA levels and decrease glutamate levels in the anterior cingulate cortex, reflecting enhanced inhibitory neurotransmission.
For voxel-level analysis, the significance level was set at cluster-level family-wise error corrected p<0.05, with an initial voxel-level threshold of p<0.001. For a priori defined regions (anterior cingulate cortex, thalamus, primary sensorimotor cortex, default mode network, sensorimotor network, and salience network), the significance level was set at p<0.05 after Bonferroni correction (corrected for the number of regions). For DWI data, threshold-free cluster enhancement with 5000 permutations and correction for multiple comparisons was used, with significance set at p<0.05.
In this study, all 110 patients will be included in the intention-to-treat set and analyzed. The intention-to-treat set includes all participants in the analysis according to their original group assignment, regardless of whether they completed the treatment protocol, withdrew early, or violated the protocol. This intention-to-treat principle preserves the advantages of randomization, maintains baseline comparability between groups, avoids bias due to dropout, and reflects the realities of incomplete adherence and protocol deviations in clinical practice. Under the missing-at-random assumption, multiple imputation will be used to handle missing data. For the primary outcome, response defined by CGI-I, a Z-test for proportions will be used to compare the difference between the two groups and calculate the confidence interval. For secondary outcomes with repeated measurements, a mixed-effects model will be used, with treatment and time as fixed effects, with particular focus on the treatment × time interaction. Center and participants will be included as random intercepts, and baseline data will be included as covariates. Adjusted between-group differences and their confidence intervals will be reported. Confidence intervals will be established at the 95% level, and the significance level will be set at 0.05. Continuous data will be presented as mean ± standard deviation if normally distributed; otherwise, they will be reported as median (interquartile range). For baseline characteristics and clinical outcomes, categorical variables will use the chi-square test, and continuous variables will use the t-test or the Mann–Whitney U-test. For fMRI data, a general linear model will be used for between-group comparisons. If baseline variables differ significantly between groups, these unbalanced variables will be included as covariates in regression models. The strength of relationships between variables will be assessed using correlation analysis and association rule algorithms. The correlation analyses are exploratory; all correlations between neural biomarkers and clinical outcomes will be analyzed to identify unknown associations. If necessary, sensitivity analyses will be performed. Pre-planned subgroup analyses include: (1) KL grade II or III; (2) baseline PESA > 30 or ≤ 30.
Discussion
KOA is a common degenerative joint disease and a frequent cause of disability.36 A growing body of clinical evidence supports acupuncture as an effective treatment for improving chronic pain and joint function in KOA.37 In this study, we plan to conduct a multicenter RCT. Based on the “Shuci” theory for treating KOA in the TCM system, we selected six acupoints around the knee. In the EA group, acupuncture needles will be inserted at these acupoints, directed toward the knee joint, reaching the periosteum. The primary outcome measure we plan to observe is the CGI-I, which quantifies the patient’s self-perceived global improvement following treatment. We define CGI-I ≤ 2 (at least much improved) as indicating effective acupuncture treatment.
In addition to EA or SEA intervention, both groups will be provided with conventional oral acetaminophen, which can be taken as needed when knee pain becomes uncontrollable. Because using EA or SEA alone and completely discontinuing all analgesic medications would be unethical, potentially causing unnecessary suffering and increasing the risk of dropout. Acetaminophen is a first-line analgesic for KOA, and we have set a 48-hour washout period before outcome assessments to ensure that its acute analgesic effects do not influence the evaluations.
A meta-analysis of 20 clinical studies38 showed that the EA group had a higher response rate compared with the analgesic group (p < 0.00001). The EA group also showed greater improvement in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) stiffness scores (p < 0.0001). However, the effects of EA on improving VAS, WOMAC pain, and WOMAC joint function were not superior to those of analgesics.
The effects of acupuncture are multifaceted. Assessments based solely on patients’ subjective feelings and quality of life cannot fully elucidate the mechanisms of acupuncture in KOA. In recent years, acupuncture researchers have turned their attention to its influence on the central nervous system. Acupuncture may precisely transmit stimulation from acupoints on the skin to central neural networks via the “skin-brain axis”39 Specifically, acupuncture stimulates cutaneous nerve ending receptors, transmitting signals through the dorsal root ganglia to key central nuclei, such as the nucleus tractus solitarius and the hypothalamus. It can then dynamically modulate neural networks involved in pain and emotion, and improve the activity of immune cells and the levels of inflammatory factors. This “acupoint-periphery-central” mechanism partially explains both the immediate effects of acupuncture and the sustained effects mediated by neuroplasticity and functional remodeling of brain networks. However, only a limited number of studies have holistically dissected the integrative mechanisms of acupuncture for chronic pain in KOA. More advanced techniques are required to gain clear insights into the precise neuromodulatory mechanisms of acupuncture.
Multimodal fMRI, characterized by its high resolution, lack of radiation, and rapid imaging capabilities, is exceptionally well-suited for investigating the central neural effects of acupuncture.40 Single sequences can only capture limited aspects of brain activity, whereas multimodal integration allows simultaneous assessment of functional connectivity, white matter microstructure, and neurotransmitter metabolism within a unified framework. This comprehensive approach enables cross-validation among different neural biomarkers, distinguishes structural plasticity from functional plasticity, and provides a more complete mechanistic explanation for the central pain-modulating effects of acupuncture. We will integrate multiple fMRI sequences and comprehensively analyze differences in brain functional-structural information and brain network connectivity patterns before and after acupuncture. Finally, we will correlate identified neural markers with patients’ subjective experiences, aiming to obtain integrated evidence regarding the brain mechanisms underlying the clinical effects of acupuncture.
Multimodal neuroimaging presents several inherent challenges that must be addressed to ensure data quality and interpretability. Motion artifacts are a major concern, particularly in older adults with KOA who may experience discomfort during prolonged scanning sessions. To mitigate this issue, we will use foam pads to reduce head motion, implement real-time motion monitoring, and exclude scan data with framewise displacement exceeding 0.5 mm or a proportion of time points with framewise displacement >0.2 mm exceeding 10%. Second, participant attrition may increase due to the time burden of multiple scanning sessions. We will reduce this risk by scheduling scans at convenient times, reimbursing travel expenses, and maintaining regular contact with participants. The integration of heterogeneous data introduces analytical complexity. We will address this issue by using validated software pipelines (FSL, FreeSurfer, CONN, MRtrix3) and registering all modalities to individual T1-weighted anatomical images, ensuring spatial alignment across sequences. These strategies aim to maximize data quality and robustness while minimizing bias and data loss.
The findings of our study could be considered for translation into clinical practice in the future. The outcome system that integrates subjective experience and multimodal fMRI enables clinicians to assess disease status and treatment response in KOA patients from multiple perspectives. Identifying specific neural biomarkers associated with clinical improvement may, in the long term, help achieve precision medicine for KOA. Reliable results would ultimately support the inclusion of EA as an evidence-based non-pharmacological treatment option in KOA management.
Our strengths are as follows: (1) This is a multicenter RCT designed to validate the efficacy of “Shuci” theory in TCM, which will provide high-level evidence for the clinical promotion of acupuncture in KOA. (2) We integrate subjective assessment tools with multimodal fMRI to evaluate and analyze the brain mechanisms of acupuncture for KOA from a multidimensional perspective.
The limitations of this study are as follows: (1) Due to the operational nature of acupuncture, a double-blind design is not feasible. However, we will maximize blinding to the greatest extent possible; only the acupuncturists must be aware of the participants’ letter group and corresponding treatment. The acupuncturists will not be involved in recruitment, allocation, assessment, or analysis. (2) The intervention duration is short, only 2 weeks. After completing this RCT, we plan to conduct a follow-up study to compare the effects of different acupuncture intervention durations, with the aim of identifying the optimal treatment duration.
Abbreviations
AE, adverse event; BBI, Bang’s Blinding Index; CGI-I, Clinical Global Impressions scale - Improvement; CONSORT, Consolidated Standards of Reporting Trials; DMN, default mode network; DWI, Diffusion-weighted imaging; EA, electroacupuncture; FD, framewise displacement; fMRI, functional magnetic resonance imaging; FNC, functional network connectivity; KOA, Knee osteoarthritis; KOOS, Knee injury and osteoarthritis outcome score; MEGA-PRESS, Meshcher-Garwood point resolved spectroscopy; OA, osteoarthritis; PESA, Patients’ expectancy scale of acupuncture; PPT, Pressure pain threshold; QoL, quality of life; RCT, randomized controlled trial; rs-fMRI, Resting-state fMRI; SAS, self-rating anxiety scale; SDS, self-rating depression scale; SEA, sham EA; SMN, sensory motor network; SPIRIT, Standard Protocol Items: Recommendations for Interventional Trials; T1W, High-resolution three-dimensional T1-weighted; TCM, traditional Chinese medicine; VAS, visual analog scale; VN, visual network.
Data Sharing Statement
The data used in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The trial was approved by the Ethics Committee of the First Affiliated Hospital of Anhui University of Chinese Medicine (2023AH-61). All participants will provide written informed consent after being fully informed about all trial procedures and after having adequate time to consider their participation.
Consent for Publication
This paper is our original work. We certify that this manuscript has not been published in part or whole elsewhere in any language, and it has not been submitted to any other journal for reviews. We certify that all authors named deserve authorship, and that all authors have agreed to be so listed and have read and approved the manuscript.
Funding
This work was supported by the Special Project for Clinical Medical Research Transformation of Anhui Province (202304295107020100), National Excellent Clinical Talents Training Program for TCM (National Administration of TCM (2022) No. 1), Health Innovative Talents Project of Anhui Province Special Support Program (Organization Department of Anhui Provincial Committee (2023) No. 35). The grantee of the funded project was Aihong Yuan. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Moseng T, Vliet Vlieland TPM, Battista S, et al. EULAR recommendations for the non-pharmacological core management of Hip and knee osteoarthritis: 2023 update. Ann Rheumatic Dis. 2024;83(6):730–14. doi:10.1136/ard-2023-225041
2. Dell Isola A, Recenti F, Giardulli B, et al. Osteoarthritis year in review 2025: epidemiology and therapy. Osteoarthritis Cartilage. 2025;33(11):1300–1306. doi:10.1016/j.joca.2025.08.015
3. Chen M, Chen S, Xie C, et al. Global prevalence, incidence, and years lived with disability (YLDs) of osteoarthritis: trends from 1990 to 2021 and projections to 2050. J Orthopaed Transl. 2026;56:101029. doi:10.1016/j.jot.2025.11.005
4. Jiao J, Dong B, Han Y, et al. Acupuncture in knee osteoarthritis: a narrative review of clinical efficacy and neuroimmune-endocrine mechanisms. J Pain Res. 2025;18:4989–4998. doi:10.2147/JPR.S546687
5. Sariyildiz A, Coskun Benlidayi I, Olmez Engizek S, et al. The relation of psychological status and type D personality with central sensitization in knee osteoarthritis: everything is in your mind! Rheumatol Int. 2023;43(12):2261–2269. doi:10.1007/s00296-023-05471-7
6. He C, Li Q, Huang R, et al. Pain phenotype in knee osteoarthritis: implications for mechanism-based therapy. Orthopaed Surg. 2025;17(11):3007–3021. doi:10.1111/os.70161
7. Mathew S, Ashraf S, Shorter S, et al. Neurobiological correlates of rheumatoid arthritis and osteoarthritis: remodelling and plasticity of nociceptive and autonomic innervations in synovial joints. Neuroscientist. 2025;31(4):425–444. doi:10.1177/10738584241293049
8. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2020;72(2):149–162. doi:10.1002/acr.24131
9. Liu C, Duan Y, Zhou H, et al. Clinical effect and contributing factors of acupuncture for knee osteoarthritis: a systematic review and pairwise and exploratory network meta-analysis. BMJ Evidence Based Med. 2024;29(6):374–384. doi:10.1136/bmjebm-2023-112626
10. Ho L, Lai CNT, Chen H, et al. Systematic review of clinical practice guidelines on acupuncture for chronic musculoskeletal pain. BMC Complement Med Therap. 2025;25(1):322. doi:10.1186/s12906-025-05070-y
11. Tu JF, Yang JW, Shi GX, et al. Efficacy of intensive acupuncture versus sham acupuncture in knee osteoarthritis: a randomized controlled trial. Arthritis Rheumatol. 2021;73(3):448–458. doi:10.1002/art.41584
12. Wu X, Li S, Wu M. Advances in electroacupuncture for treatment of knee osteoarthritis: mechanisms, efficacy, and future directions. J Pain Res. 2025;18:5083–5108. doi:10.2147/JPR.S543346
13. Liu X, Ma Y, Huang Z, et al. The efficacy of acupuncture, exercise rehabilitation, and their combination in the treatment of knee osteoarthritis: a randomized controlled trial. J Pain Res. 2024;17:2837–2849. doi:10.2147/JPR.S465058
14. Wei X, Wang Z, Shi G, et al. Effect of acupuncture treatment for patients with knee osteoarthritis on brain fluctuation amplitude and functional connectivity: a randomized three-armed fMRI study. BMC Complement Med Therap. 2025;25(1):244. doi:10.1186/s12906-025-04985-w
15. Qu Y, Peng Y, Xiong Y, et al. Acupuncture-Related therapy for knee osteoarthritis: a narrative review of neuroimaging studies. J Pain Res. 2024;17:773–784. doi:10.2147/JPR.S450515
16. Lehtinen P, Stenroos P, Salo R, et al. Functional MRI following sensory stimulation in rat monosodium iodoacetate model of osteoarthritis pain as a tool for drug therapy discovery. NeuroImage. 2026;325:121670. doi:10.1016/j.neuroimage.2025.121670
17. Al-Faraj K, Hanel PHP, Valentini E. Brain Responses during provoked pain in Patients with Chronic Primary Pain: a systematic review and meta-analysis of fMRI studies. J Pain. 2026;106218. doi:10.1016/j.jpain.2026.106218
18. Cheng S, Zeng F, Zhou J, et al. Altered static and dynamic functional brain network in knee osteoarthritis: a resting-state functional magnetic resonance imaging study. NeuroImage. 2024;292:120599. doi:10.1016/j.neuroimage.2024.120599
19. Xie C, Zhang Z, Zhang Y, et al. Multi-Spatial Voxel-scale modulation of acupuncture on abnormal brain activity in migraine patients without aura: a randomized study neuroimaging trial. Brain Behav. 2025;15(5):e70536. doi:10.1002/brb3.70536
20. Chowdhury A, Bianciardi M, Chapdelaine E, et al. Multimodal neurophenomenology of advanced concentration absorption meditation: an intensively sampled case study of Jhana. NeuroImage. 2025;305:120973. doi:10.1016/j.neuroimage.2024.120973
21. Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Arthritis Rheum. 1986;29(8):1039–1049. doi:10.1002/art.1780290816
22. Osteoarthritis E G O C, Association T P D B. Chinese guidelines for diagnosis and treatment of osteoarthritis (2024 edition). Chin J Painol. 2024;20(3):323–338.
23. Bang H. Random guess and wishful thinking are the best blinding scenarios. Contemp Clin Trials Commun. 2016;3:117–121. doi:10.1016/j.conctc.2016.05.003
24. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. 2007;4(7):28–37.
25. Guy W. ECDEU Assessment Manual for Psychopharmacology (DHEW Publication No. ADM 76–338). Rockville, MD: U.S. Department of Health, Education, and Welfare; 1976.
26. Downie WW, Leatham PA, Rhind VM, et al. Studies with pain rating scales. Ann Rheumatic Dis. 1978;37(4):378–381. doi:10.1136/ard.37.4.378
27. Lorusso L, Salerno M, Sessa F, et al. Autoalgometry: an important tool for pressure pain threshold evaluation. J Clin Med. 2018;7(9):273. doi:10.3390/jcm7090273
28. Roos EM, Roos HP, Lohmander LS, et al. Knee Injury and Osteoarthritis Outcome Score (KOOS)—development of a self-administered outcome measure. J Orthop Sports Phys Ther. 1998;28(2):88–96. doi:10.2519/jospt.1998.28.2.88
29. Yang X, Xia W, Xu Y, et al. Patients’ expectancy scale of acupuncture: development and clinical performance test. Complement Therap Clin Pract. 2023;53:101797. doi:10.1016/j.ctcp.2023.101797
30. Zung WWK. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
31. Zung WWK. A self-rating depression scale. Arch Gen Psychiatry. 1965;12(1):63. doi:10.1001/archpsyc.1965.01720310065008
32. Zheng A, Zheng F, Jin K, et al. Manual acupuncture at LI11, local points and both for knee osteoarthritis: a pilot randomized controlled trial. J Pain Res. 2023;16:4393–4404. doi:10.2147/JPR.S445770
33. Nie Q, He F, Dong L, et al. Effects of transcranial direct current stimulation combined with acupuncture therapy on brain network functional connectivity in patients with knee osteoarthritis: a single-center randomized controlled trial. J Neuroeng Rehabil. 2025;22(1):160. doi:10.1186/s12984-025-01692-y
34. Cheng S, Dong X, Zhou J, et al. Alterations of the white matter in patients with knee osteoarthritis: a diffusion tensor imaging study with tract-based spatial statistics. Front Neurol. 2022;13:835050. doi:10.3389/fneur.2022.835050
35. Tan X, Zheng D, Lin Q, et al. Confirmation of pain-related neuromodulation mechanism of Bushen Zhuangjin Decoction on knee osteoarthritis. J Ethnopharmacol. 2024;324:117772. doi:10.1016/j.jep.2024.117772
36. Ding Y, Liu X, Chen C, et al. Global, regional, and national trends in osteoarthritis disability-adjusted life years (DALYs) from 1990 to 2019: a comprehensive analysis of the global burden of disease study. Public Health. 2024;226:261–272. doi:10.1016/j.puhe.2023.10.030
37. Zhu R, Li X, Yan Z, et al. Efficacy and safety of acupuncture with moxibustion for knee osteoarthritis: a meta-analysis of randomized controlled trials. Syst Rev. 2025;14(1):15. doi:10.1186/s13643-025-02762-x
38. Li P, Zhang Y, Li F, et al. The efficacy of electroacupuncture in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Adv Biol. 2023;7(10):2200304. doi:10.1002/adbi.202200304
39. He T, Zheng Y, Yan J, et al. Skin-Brain Axis: neural pathways in acupuncture treatment. ChinMed. 2025;20(1):163. doi:10.1186/s13020-025-01213-y
40. Liu S, Bai Y, Liu J, et al. Decoding the mechanisms of acupuncture by neuroimaging: an integrated review from networks to molecules. Front Human Neurosci. 2026;20:1704570. doi:10.3389/fnhum.2026.1704570
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
Evaluating the Efficacy and Underlying Mechanisms of Acupuncture for Chronic Subjective Tinnitus Using Functional Near-Infrared Spectroscopy: Study Protocol for a Randomized Controlled Trial
Hu H, Lin X, Fang L, Li Y, Gao H
Journal of Pain Research 2023, 16:3367-3378
Published Date: 4 October 2023
Effect of Traditional Chinese Non-Pharmacological Therapies on Knee Osteoarthritis: A Narrative Review of Clinical Application and Mechanism
Liu ZF, Zhang Y, Liu J, Wang YY, Chen M, Liu EY, Guo JM, Wang YH, Weng ZW, Liu CX, Yu CH, Wang XY
Orthopedic Research and Reviews 2024, 16:21-33
Published Date: 26 January 2024
Exploring the Analgesic Effect of Acupuncture on Knee Osteoarthritis Based on MLT/cAMP/PKA/CREB Signaling Pathway
Zhang C, Yu M, Zhang L, Zhou X, Han J, Fu B, Xue H, Zhang C
Journal of Inflammation Research 2025, 18:237-249
Published Date: 7 January 2025
Therapeutic Potential of Acupuncture in Knee Osteoarthritis: Clinical Efficacy and Mechanistic Insights
Yao K, Shamim MF, Xia J, Liu TT, Guo Y, Lin X
Journal of Inflammation Research 2025, 18:12169-12190
Published Date: 5 September 2025