Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Equivalent of Carbon Dioxide at the Anaerobic Threshold Predicts Acute Exacerbations in Patients with Chronic Obstructive Pulmonary Disease: A Retrospective Cohort Study
Authors Li Y, Li X ![]() , Lin F
, Lin F ![]() , Hu X, Liu S, Qiu M, Zhang J, Zhao R, Nie S, Xu B, Yan F, Yu G
, Hu X, Liu S, Qiu M, Zhang J, Zhao R, Nie S, Xu B, Yan F, Yu G
Received 2 April 2026
Accepted for publication 18 May 2026
Published 28 May 2026 Volume 2026:21 613925
DOI https://doi.org/10.2147/COPD.S613925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Yunxiao Li,1 Xiaona Li,1 Fang Lin,1 Xing Hu,1 Siqi Liu,1 Mengmeng Qiu,1 Jianxiong Zhang,2 Ranran Zhao,1 Shan Nie,1 Bo Xu,1 Fugui Yan,1 Ganggang Yu1
1Department of Respiratory Medicine, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Research Ward, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Ganggang Yu, Email [email protected] Fugui Yan, Email [email protected]
Purpose: To investigate the predictive value of the equivalent of carbon dioxide at the anaerobic threshold (EqCO2@AT) for acute exacerbations (AE) in patients with chronic obstructive pulmonary disease (COPD).
Patients and Methods: This retrospective cohort study included 79 patients with COPD who underwent baseline pulmonary function testing and cardiopulmonary exercise testing (CPET). EqCO2@AT = 30 was used only as an empirical threshold for descriptive stratification, rather than as an outcome-derived cutoff. Patients were also classified into non-AE and AE groups according to annualized exacerbation frequency. Baseline characteristics, pulmonary function, and CPET parameters were compared between groups. Logistic regression was used to evaluate the association between EqCO2@AT and AE risk. Predictive performance was assessed using receiver operating characteristic curves, calibration analysis, decision curve analysis, Kaplan–Meier analysis, and a simplified nomogram.
Results: Of the 79 patients, 16 were classified into the low EqCO2@AT group and 63 into the high EqCO2@AT group. Patients with higher EqCO2@AT were older, had lower BMI, greater smoking exposure, lower FEV1% predicted and DLCO% predicted, reduced exercise capacity, and higher ventilatory inefficiency parameters. Compared with the non-AE group, the AE group had worse lung function, lower exercise capacity, and higher VE/VCO2 slope and EqCO2@AT. EqCO2@AT was associated with AE risk in univariable analysis (OR 1.122, 95% CI 1.027– 1.226, P = 0.011) and remained significant after adjustment for age, BMI, and FEV1% predicted (OR 1.269, 95% CI 1.110– 1.450, P < 0.001). The AUC of EqCO2@AT alone was 0.739, whereas the combined model achieved an AUC of 0.850. Kaplan–Meier analysis showed significantly lower AE-free survival in the high EqCO2@AT group (log-rank P = 0.002). The simplified nomogram provided an individualized visual tool for AE risk estimation.
Conclusion: Elevated EqCO2@AT is associated with impaired ventilatory efficiency, reduced exercise capacity, and increased AE risk in COPD. A model incorporating EqCO2@AT, age, BMI, and FEV1% predicted showed good predictive performance and may support individualized AE risk stratification. These findings suggest that CPET-derived ventilatory efficiency parameters may provide clinically useful information beyond conventional pulmonary function assessment, although validation in larger multicenter prospective cohorts is still required.
Keywords: chronic obstructive pulmonary disease, acute exacerbation, anaerobic threshold, equivalent of carbon dioxide, cardiopulmonary exercise testing
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic respiratory disorder characterized by persistent respiratory symptoms and airflow limitation, and remains a major cause of disability and mortality worldwide.1 Acute exacerbations of COPD (AECOPD) are important events in disease progression because they may worsen symptoms, increase hospitalization risk, accelerate lung function decline, and raise mortality.1,2 Current global COPD management strategies emphasize future exacerbation risk assessment based on prior exacerbation history, symptom burden, and pulmonary function indices.1 However, these conventional measures mainly reflect disease severity at rest and may not fully capture abnormalities in ventilation, circulation, and metabolism during exercise. Therefore, dynamic cardiopulmonary parameters may provide additional value for refining risk stratification in stable COPD.
Cardiopulmonary exercise testing (CPET) enables integrated assessment of ventilation, gas exchange, circulatory reserve, and metabolic responses during incremental exercise, and is useful for clarifying mechanisms of exercise limitation and dyspnea.3–6 The equivalent of carbon dioxide at the anaerobic threshold (EqCO2@AT) reflects the ventilatory requirement for carbon dioxide elimination at a key metabolic transition point.7,8 In COPD, increased dead-space ventilation, ventilation/perfusion mismatch, and wasted ventilation increase the ventilatory cost of carbon dioxide elimination, leading to impaired ventilatory efficiency and exertional dyspnea.9,10 Although ventilatory inefficiency is associated with reduced exercise tolerance, evidence directly linking EqCO2@AT to future exacerbation risk remains limited. This retrospective cohort study therefore aimed to evaluate the predictive value of EqCO2@AT for AECOPD and its potential role in clinical risk stratification.
Materials and Methods
Study Design and Participants
This single-center retrospective cohort study enrolled patients with COPD who attended the Department of Respiratory Medicine, Beijing Friendship Hospital, Capital Medical University, between January 2020 and December 2025 and completed CPET during the stable phase. Baseline clinical data, pulmonary function, CPET parameters, and subsequent acute exacerbation events were retrospectively collected.
Eligible patients were aged ≥40 years, had COPD diagnosed according to GOLD criteria, defined as post-bronchodilator FEV1/FVC <0.70, had no acute exacerbation within 4 weeks before testing, and were able to complete CPET.1 Patients were excluded if they had severe cardiovascular disease, other severe pulmonary diseases, skeletal muscle or neurologic disorders affecting exercise performance, incomplete baseline data, or missing follow-up information. Of 91 patients initially screened, 79 were included in the final analysis. The study was approved by the Ethics Committee of Beijing Friendship Hospital, Capital Medical University (Approval No. 2024-P2-125-01) and complied with the Declaration of Helsinki.
Clinical Data Collection
Baseline data were obtained from the electronic medical record system, including age, sex, height, weight, BMI, smoking history, comorbidities, previous exacerbation history, and pulmonary function variables. Smoking exposure was expressed as pack-years. For descriptive comparisons, patients were stratified into a low EqCO2@AT group (≤30) and a high EqCO2@AT group (>30) according to baseline EqCO2@AT.7
Pulmonary Function Testing
Pulmonary function testing was performed at baseline using a MasterScreen Body plethysmograph (CareFusion, San Diego, CA, USA) according to guideline-based procedures. The measured variables included vital capacity, forced vital capacity, forced expiratory volume in 1 second, FEV1% predicted, residual volume/total lung capacity, DLCO% predicted, and DLCO/VA% predicted.
Cardiopulmonary Exercise Testing
Baseline CPET was performed using an electronically braked cycle ergometer (ViaSprint, CareFusion, Höchberg, Germany). After 3 minutes of rest and 3 minutes of unloaded pedaling, patients underwent symptom-limited incremental exercise with an individualized work-rate increase of 5–20 W/min while maintaining a cadence of approximately 60 rpm. Electrocardiography, blood pressure, pulse oxygen saturation, minute ventilation, oxygen uptake, and carbon dioxide output were monitored continuously.5,6
EqCO2 was defined as VE/VCO2, and EqCO2@AT was defined as the VE/VCO2 value at the anaerobic threshold.8 AT was determined mainly by the V-slope method, with reference to the behavior of VE/VO2 and VE/VCO2.5,8 Other recorded CPET parameters included Peak VO2, peak work rate, ΔVO2/ΔWork slope, oxygen pulse, VE/VCO2 slope, Peak VCO2, peak heart rate, heart rate recovery, and chronotropic index.
The main derived indices were calculated as follows: VE/VCO2 slope was obtained from the linear relationship between VE and VCO2 during incremental exercise; ΔVO2/ΔWork slope was calculated as the change in VO2 divided by the change in work rate; oxygen pulse was calculated as VO2/heart rate; heart rate recovery was calculated as the difference between peak heart rate and early recovery heart rate; chronotropic index was calculated as (Peak HR − resting HR)/(age-predicted maximal HR − resting HR) × 100%; and BMI was calculated as weight divided by height squared.
Follow-Up and Outcome Definitions
The date of baseline CPET was defined as the start of observation. Because patients entered the cohort at different time points between January 2020 and December 2025, follow-up duration was not identical for all participants. Each patient was followed from baseline CPET until the first documented AE event, the last available follow-up visit, or the end of the study observation period, whichever came first. The maximum follow-up duration was 5 years.
AE was defined as an acute worsening of respiratory symptoms requiring additional antibiotics, systemic corticosteroids, or hospitalization.1 Annualized exacerbation frequency was calculated as the total number of AE events divided by follow-up duration. Patients were categorized into a non-AE group (AE <1/year) and an AE group (AE ≥1/year).1,11 For survival analysis, AE-free survival was defined as the time from baseline CPET to the first documented AE or censoring at the last follow-up visit.
EqCO2@AT = 30 was used only as an empirical threshold for descriptive stratification based on the ERS statement on standardized CPET in chronic lung diseases and the distribution of this cohort; it was not used as the outcome-derived predictive cutoff.7 The optimal cutoff for AE prediction was determined by ROC analysis and was used for Kaplan–Meier analysis. A combined model including age, BMI, FEV1% predicted, and EqCO2@AT was constructed and further evaluated using ROC, calibration, decision curve, and simplified nomogram analyses.
Data Completeness and CPET Interpretation
Data completeness was assessed before statistical analysis. Patients with incomplete baseline clinical data, pulmonary function results, CPET parameters, or missing follow-up information were excluded; therefore, no imputation was performed. CPET parameters, including AT determination, were interpreted according to standardized criteria by trained investigators. When uncertainty existed, results were reviewed by an experienced senior physician and resolved by consensus. Formal inter-observer variability analysis was not performed.
Statistical Analysis
All analyses were performed using R software, version 4.4.0. Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed variables are presented as mean ± standard deviation and were compared using the independent-samples t-test. Non-normally distributed variables are presented as median and interquartile range and were compared using the Mann–Whitney U-test. Categorical variables are presented as number and percentage and were compared using the chi-square test or Fisher’s exact test, as appropriate. A two-sided P < 0.05 was considered statistically significant.
Univariable and multivariable logistic regression analyses were performed to assess the association between EqCO2@AT and AE risk, with odds ratios and 95% confidence intervals calculated. ROC curves were used to evaluate the predictive performance of EqCO2@AT alone and the combined model. Calibration and decision curve analyses were used to assess model agreement and clinical utility. A simplified nomogram was constructed from the combined model to improve clinical interpretability. Kaplan–Meier analysis was performed using the ROC-derived cutoff, and group differences were compared with the Log rank test.
Results
A total of 79 patients with COPD were included. Using EqCO2@AT = 30 as the descriptive threshold, 16 patients were classified into the low EqCO2@AT group and 63 into the high EqCO2@AT group (Figure 1). Compared with the low EqCO2@AT group, the high EqCO2@AT group was older (67.9 ± 7.6 vs 61.6 ± 8.6 years, P = 0.014), had lower BMI (23.5 ± 3.4 vs 26.0 ± 3.8 kg/m2, P = 0.027), and had greater smoking exposure (26.3 ± 22.9 vs 10.9 ± 12.1 pack-years, P < 0.001). No significant between-group differences were observed in sex distribution, height, weight, GOLD stage, or major comorbidities, including hypertension, coronary artery disease, and diabetes (Table 1).
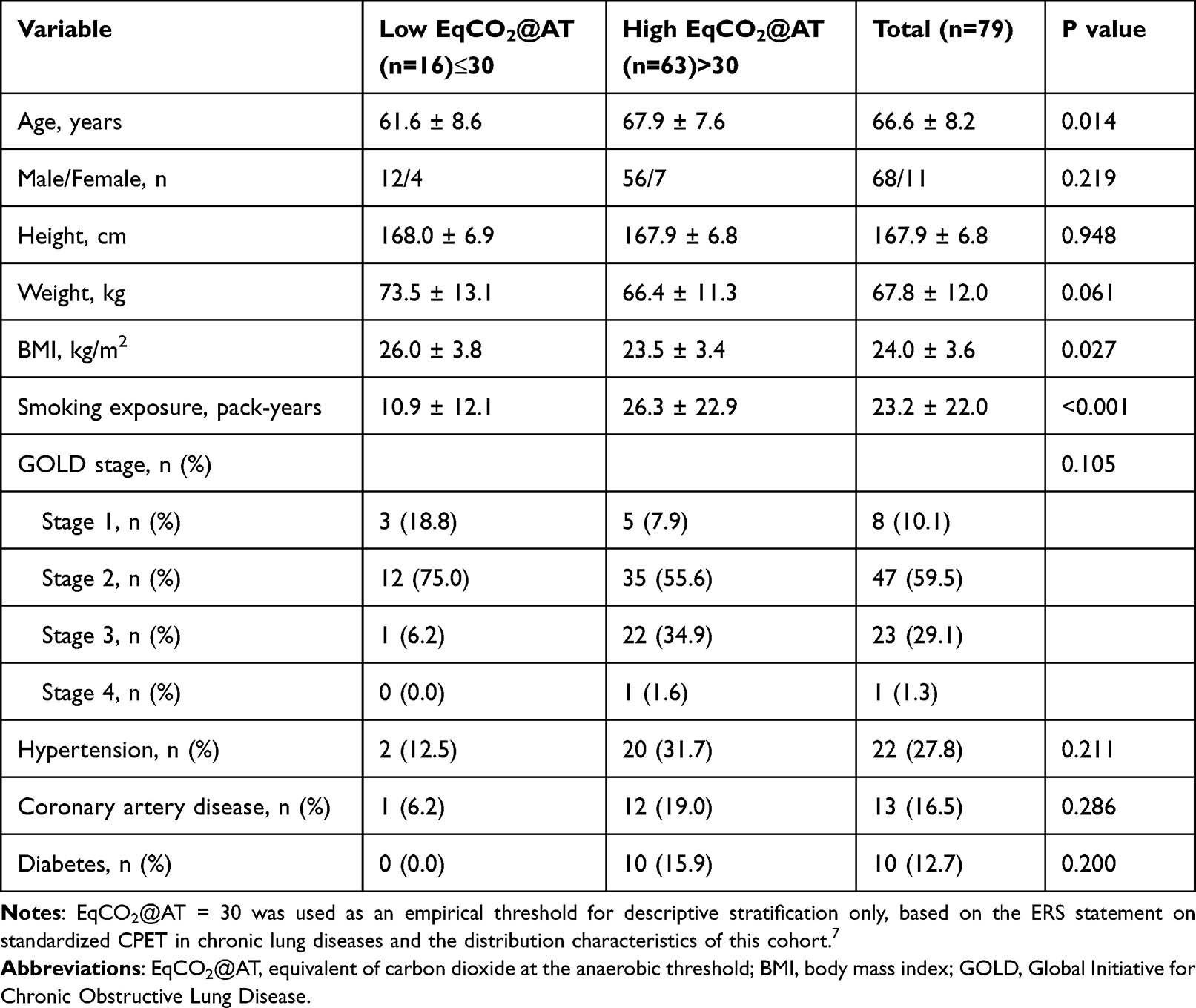 |
Table 1 Baseline Clinical Characteristics Stratified by EqCO2@AT |
 |
Figure 1 Flow chart showing patient inclusion and study grouping according to baseline EqCO2@AT and annualized acute exacerbation frequency. Patients with complete baseline cardiopulmonary exercise testing (CPET) and follow-up data were included in the final analysis. EqCO2@AT = 30 was used for descriptive stratification only. |
Static pulmonary function showed that patients with higher EqCO2@AT had lower FEV1% predicted (54.82 ± 14.06% vs 63.56 ± 14.23%, P = 0.030), lower DLCO% predicted (64.59 ± 15.03% vs 72.96 ± 9.68%, P = 0.038), and higher RV/TLC (66.98 ± 18.28% vs 59.25 ± 7.02%, P = 0.009) than those with lower EqCO2@AT. Other pulmonary function variables, including VC, FVC, FEV1, FEV1/FVC, and DLCO/VA% predicted, did not differ significantly between groups (Table 2).
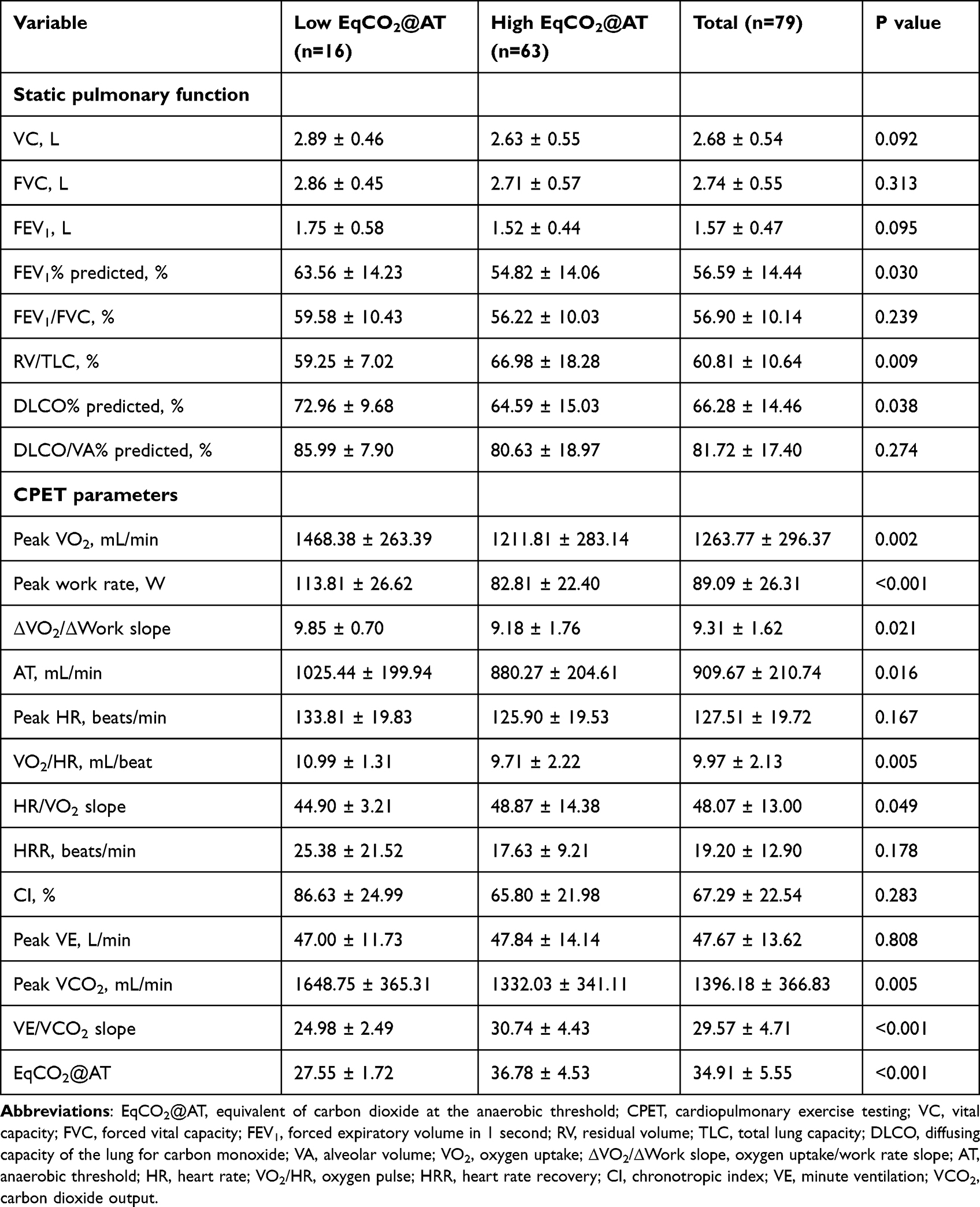 |
Table 2 Pulmonary Function and CPET Parameters Stratified by EqCO2@AT |
On CPET, the high EqCO2@AT group showed lower Peak VO2 (1211.81 ± 283.14 vs 1468.38 ± 263.39 mL/min, P = 0.002), peak work rate (82.81 ± 22.40 vs 113.81 ± 26.62 W, P < 0.001), ΔVO2/ΔWork slope (9.18 ± 1.76 vs 9.85 ± 0.70, P = 0.021), anaerobic threshold (880.27 ± 204.61 vs 1025.44 ± 199.94 mL/min, P = 0.016), VO2/HR (9.71 ± 2.22 vs 10.99 ± 1.31 mL/beat, P = 0.005), and Peak VCO2 (1332.03 ± 341.11 vs 1648.75 ± 365.31 mL/min, P = 0.005), but higher HR/VO2 slope (48.87 ± 14.38 vs 44.90 ± 3.21, P = 0.049), VE/VCO2 slope (30.74 ± 4.43 vs 24.98 ± 2.49, P < 0.001), and EqCO2@AT (36.78 ± 4.53 vs 27.55 ± 1.72, P < 0.001) than the low EqCO2@AT group. Peak HR, HRR, CI, and Peak VE were comparable between groups (Table 2).
According to annualized exacerbation frequency, 34 patients were classified into the non-AE group and 45 into the AE group. The AE group had lower FEV1% predicted than the non-AE group (52.27 ± 12.53% vs 59.38 ± 15.03%, P = 0.032), while other static pulmonary function variables were similar. CPET showed that the AE group had lower Peak VO2 (1170.65 ± 310.59 vs 1323.92 ± 273.46 mL/min, P = 0.024), Peak HR (121.84 ± 21.06 vs 131.17 ± 18.10 beats/min, P = 0.039), VO2/HR (9.65 ± 2.31 vs 10.17 ± 2.00 mL/beat, P = 0.029), and CI (49.24 ± 19.02 vs 71.53 ± 21.37%, P = 0.010), but higher VE/VCO2 slope (31.97 ± 4.96 vs 28.03 ± 3.87, P < 0.001) and EqCO2@AT (36.49 ± 5.75 vs 30.89 ± 5.24, P < 0.001) than the non-AE group (Table 3 and Figure 2). Peak work rate, ΔVO2/ΔWork slope, AT, HR/VO2 slope, HRR, Peak VE, and Peak VCO2 did not differ significantly between groups.
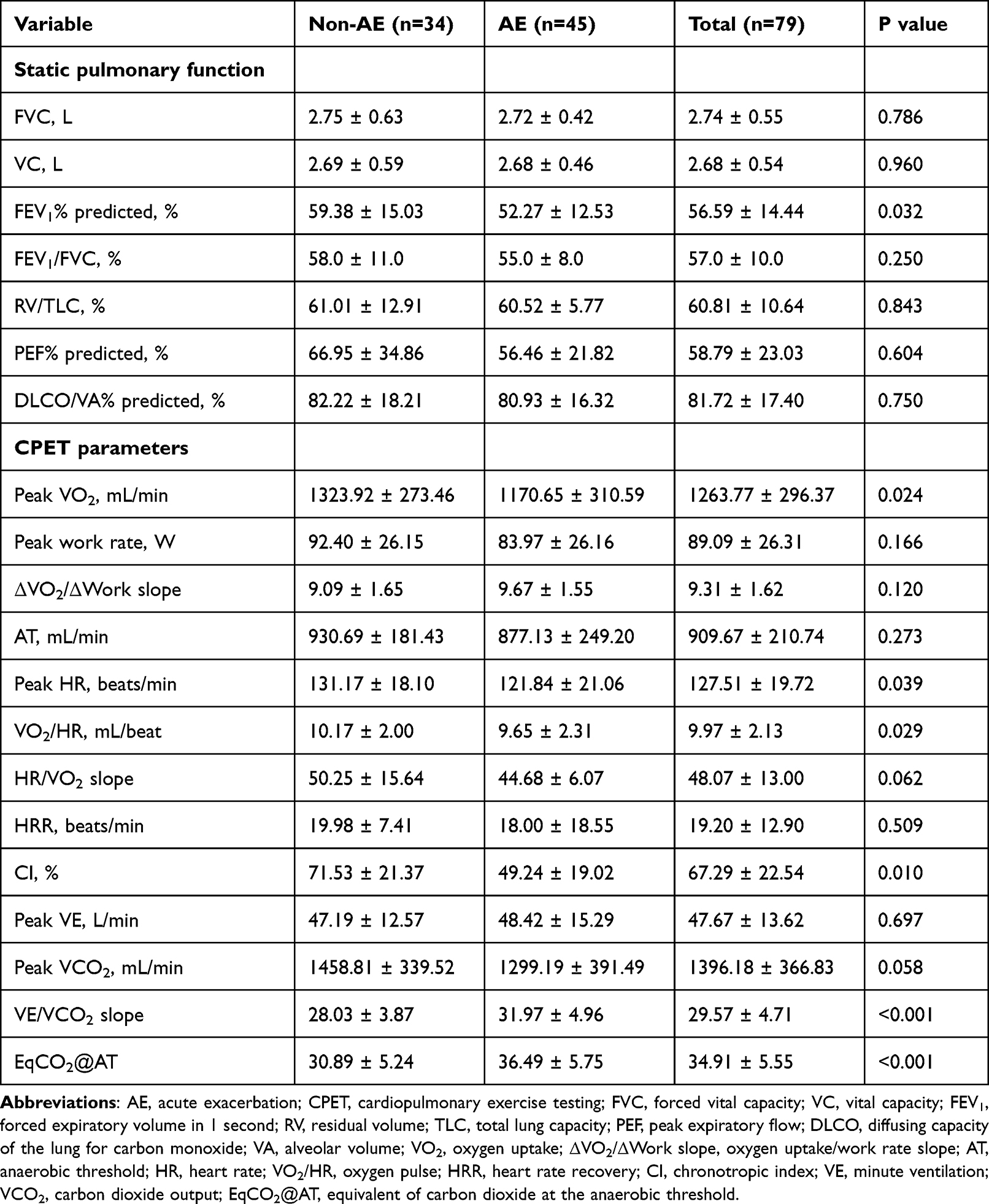 |
Table 3 Pulmonary Function and CPET Parameters in the Non-AE and AE Groups |
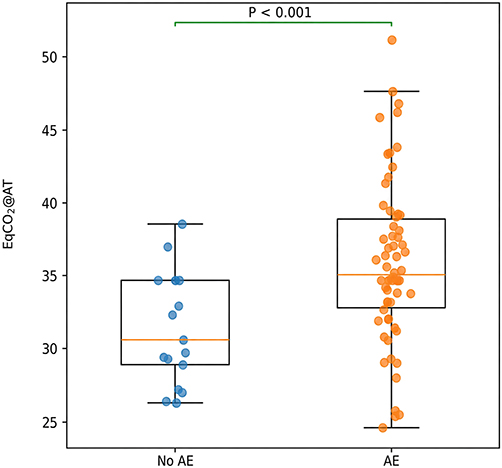 |
Figure 2 Comparison of EqCO2@AT between the non-AE and AE groups. The AE group showed significantly higher EqCO2@AT values than the non-AE group. AE, acute exacerbation; EqCO2@AT, equivalent of carbon dioxide at the anaerobic threshold. |
Correlation analysis showed that EqCO2@AT was negatively correlated with FEV1% predicted (r = −0.257, P = 0.023), peak work rate (r = −0.364, P = 0.00098), anaerobic threshold (r = −0.350, P = 0.00158), Peak VCO2 (r = −0.280, P = 0.0124), and Peak VO2 (r = −0.280, P = 0.0125), and positively correlated with VE/VCO2 slope (r = 0.701, P < 0.001) (Supplementary Figure S1). These findings suggest that elevated EqCO2@AT was associated with lower FEV1% predicted, impaired ventilatory efficiency, and reduced exercise capacity.
ROC analysis showed that the AUC of EqCO2@AT alone for predicting AE was 0.739, whereas the combined model incorporating age, BMI, FEV1% predicted, and EqCO2@AT achieved a higher AUC of 0.850 (Figure 3). Calibration analysis showed good agreement between predicted and observed probabilities (Figure 4). Decision curve analysis further indicated that the combined model provided greater net benefit than EqCO2@AT alone and the treat-all or treat-none strategies across a broad range of threshold probabilities (Figure 5).
 |
Figure 3 Receiver operating characteristic (ROC) curves of EqCO2@AT alone and Model B for predicting AE. Model B included age, body mass index (BMI), FEV1% predicted, and EqCO2@AT. The area under the curve (AUC) was 0.739 for EqCO2@AT alone and 0.850 for Model B. |
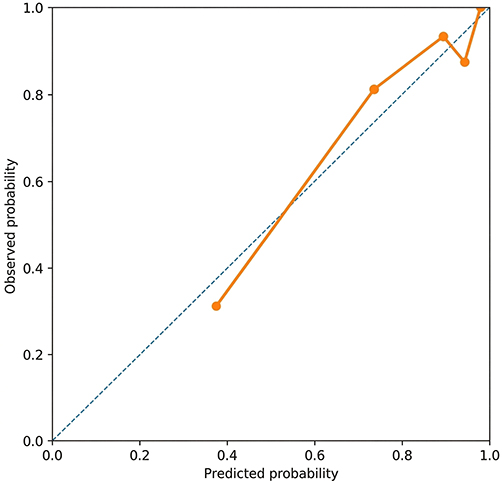 |
Figure 4 Calibration curve of Model B for predicting AE risk. The diagonal line represents ideal agreement between predicted and observed probabilities, and the model curve represents the observed calibration performance of Model B. |
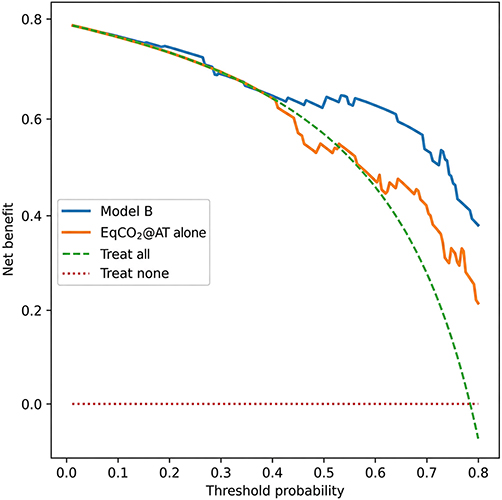 |
Figure 5 Decision curve analysis comparing Model B with EqCO2@AT alone for predicting AE. Model B provided greater net benefit than EqCO2@AT alone and than the treat-all or treat-none strategies across a broad range of threshold probabilities. |
In univariable logistic regression, EqCO2@AT was associated with increased AE risk (OR 1.122, 95% CI 1.027–1.226, P = 0.011), while higher FEV1% predicted was associated with lower AE risk (OR 0.960, 95% CI 0.933–0.987, P = 0.005). Age and BMI were not significantly associated with AE risk in univariable analysis. In multivariable analysis adjusted for age, BMI, and FEV1% predicted, EqCO2@AT remained independently associated with AE risk (OR 1.269, 95% CI 1.110–1.450, P < 0.001). BMI was positively associated with AE risk (OR 1.608, 95% CI 1.254–2.061, P < 0.001), whereas FEV1% predicted remained protective (OR 0.919, 95% CI 0.879–0.961, P < 0.001); age was not significant (OR 1.005, 95% CI 0.933–1.082, P = 0.895) (Table 4).
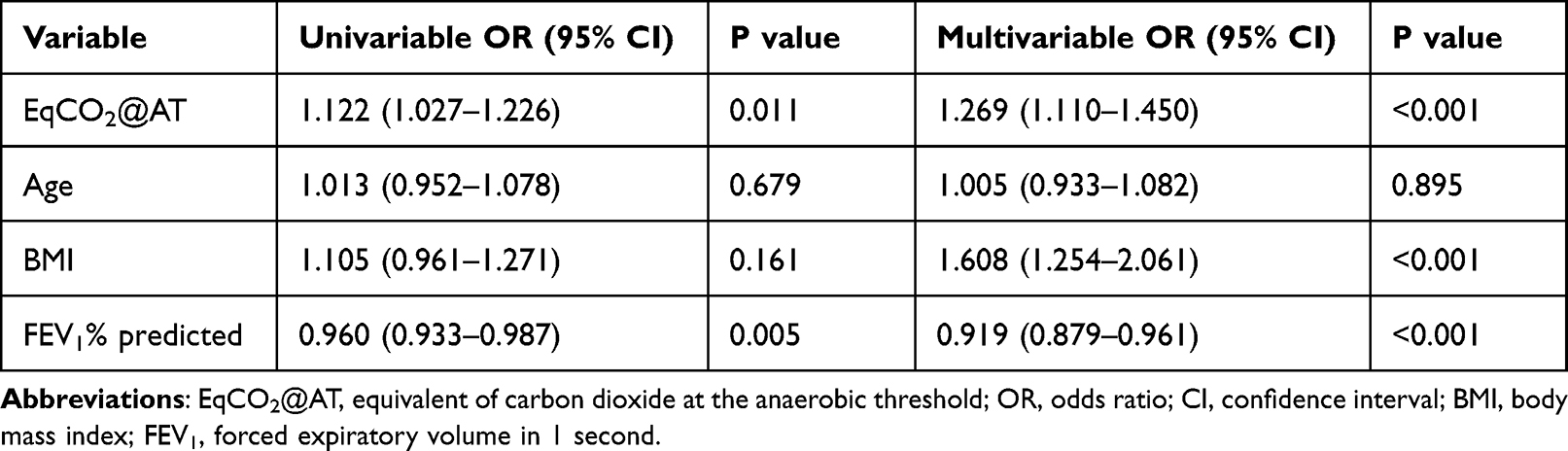 |
Table 4 Logistic Regression Analysis of EqCO2@AT and Acute Exacerbation Risk |
A simplified nomogram based on the combined model was constructed to improve clinical interpretability (Figure 6). BMI contributed the largest point score, followed by FEV1% predicted and EqCO2@AT, while age contributed minimally. The nomogram visually integrates clinical, pulmonary function, and CPET-derived variables for individualized AE risk estimation.
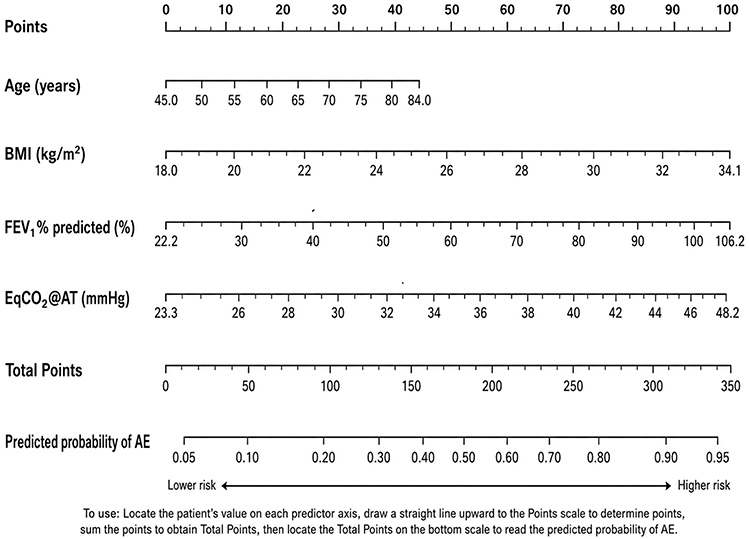 |
Figure 6 Simplified nomogram based on Model B for individualized AE risk estimation. The nomogram integrates age, BMI, FEV1% predicted, and EqCO2@AT. Each predictor corresponds to a point score, and the total points can be mapped to the predicted probability of AE. AE, acute exacerbation; BMI, body mass index; FEV1, forced expiratory volume in 1 second; EqCO2@AT, equivalent of carbon dioxide at the anaerobic threshold. |
Using the ROC-derived optimal cutoff of EqCO2@AT = 34.88, Kaplan–Meier analysis showed significantly lower AE-free survival in the high EqCO2@AT group than in the low EqCO2@AT group (log-rank P = 0.002; Figure 7).
 |
Figure 7 Kaplan–Meier curve of AE-free survival stratified by the ROC-derived optimal cutoff of EqCO2@AT. AE-free survival was significantly lower in the high EqCO2@AT group than in the low EqCO2@AT group (log-rank P = 0.002). |
Discussion
In this retrospective cohort study, elevated EqCO2@AT was associated with impaired ventilatory efficiency, reduced exercise capacity, and increased acute exacerbation (AE) risk in patients with COPD. This association remained significant after adjustment for age, BMI, and FEV1% predicted, suggesting that EqCO2@AT may provide prognostic information beyond conventional clinical and spirometric indices. The combined model incorporating EqCO2@AT, age, BMI, and FEV1% predicted showed better discrimination than EqCO2@AT alone, and the simplified nomogram provided an intuitive format for individualized AE risk estimation.
The physiological relevance of EqCO2@AT is consistent with the known mechanisms of ventilatory inefficiency in COPD. EqCO2@AT reflects the ventilatory requirement for carbon dioxide elimination at the anaerobic threshold, a key metabolic transition during exercise. In COPD, increased dead-space ventilation, ventilation/perfusion mismatch, abnormal gas exchange, and dynamic hyperinflation may increase the ventilatory cost of exercise, contributing to exertional dyspnea and exercise intolerance.4–6,9,10,12 Compared with resting spirometry, exercise-derived indices may better capture integrated abnormalities in ventilation, gas exchange, circulation, and metabolic reserve.4–6 Therefore, EqCO2@AT may serve as a dynamic marker of ventilatory burden and reduced physiological reserve.
The association between EqCO2@AT and AE risk may be explained by several mechanisms. Higher EqCO2@AT indicates poorer ventilatory compensation during exercise, which may reflect limited reserve when patients encounter infection, inflammation, or other stressors. Ventilation/perfusion mismatch and impaired gas exchange may also indicate broader pulmonary parenchymal, pulmonary vascular, or cardiopulmonary dysfunction, thereby increasing vulnerability to exacerbations.13–16 In addition, ventilatory inefficiency often coexists with exertional symptoms, reduced physical activity, and deconditioning, all of which are associated with adverse COPD outcomes.6,14,17
The clinical value of the combined model lies in integrating CPET-derived ventilatory efficiency with conventional clinical and pulmonary function variables. GOLD-based assessment mainly relies on prior exacerbation history, symptom burden, and lung function.1 Our findings suggest that EqCO2@AT may refine risk stratification by adding dynamic functional information. The simplified nomogram translates the multivariable model into a clinically interpretable format. However, because it was derived from a single-center retrospective cohort, it should be regarded as an exploratory risk-visualization tool rather than a validated decision instrument.
BMI also contributed substantially to the multivariable model. The relationship between BMI and COPD outcomes is complex and may depend on disease stage, body composition, nutritional status, and systemic metabolic phenotype. Previous studies have emphasized the prognostic significance of underweight status, BMI decline, and low fat-free mass index in COPD.18–21 In the present cohort, higher BMI was associated with increased AE risk after adjustment. This finding should be interpreted cautiously. Higher BMI may increase ventilatory mechanical load, reduce chest wall compliance, increase work of breathing, and contribute to obesity-related inflammation or metabolic dysfunction. Conversely, low BMI or cachexia may reflect muscle wasting and systemic catabolism. Future studies should incorporate body composition, fat-free mass index, inflammatory biomarkers, and physical activity data to clarify BMI-related risk mechanisms.
From a clinical perspective, EqCO2@AT is derived from routine CPET and may help evaluate ventilatory burden and gas-exchange stress during exercise. These findings provide hypothesis-generating evidence that CPET-derived ventilatory efficiency parameters may be useful for exacerbation risk assessment, pulmonary rehabilitation planning, and individualized follow-up.22 Nevertheless, prospective validation is required before clinical implementation.
This study has several limitations. First, it was a single-center retrospective study with a relatively small sample size, so selection bias, residual confounding, and limited statistical power cannot be excluded. Second, although patients with incomplete baseline data or missing follow-up information were excluded, follow-up intervals, treatment adjustments, pulmonary rehabilitation exposure, and AE ascertainment could not be fully standardized. Third, inflammatory biomarkers, imaging variables, body composition measurements, and objective physical activity data were unavailable, limiting mechanistic interpretation. Fourth, the combined model and simplified nomogram have not been externally validated. Finally, annualized exacerbation frequency may not fully reflect exacerbation severity, phenotype, or temporal clustering. Larger multicenter prospective studies are needed to validate EqCO2@AT-based models and assess their value in COPD management.
In conclusion, elevated EqCO2@AT was associated with poorer lung function, lower exercise tolerance, and higher AE risk in patients with COPD. A combined model incorporating EqCO2@AT, age, BMI, and FEV1% predicted showed good performance for individualized AE risk stratification and was translated into a simplified nomogram. EqCO2@AT may provide dynamic information beyond static pulmonary function alone, but larger prospective multicenter studies are needed before incorporation into standardized COPD management algorithms.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The Ethics Committee of Beijing Friendship Hospital approved the study protocol (No. 2024-P2-125-01, Date: 2024–04-19). This study was conducted in accordance with the Declaration of Helsinki. All participants were provided with written and oral information about the study and signed informed consent forms.
Author Contributions
Y.L. and X.L. conceived and designed the study. Y.L., F.L., X.H., S.L., M.Q., J.Z., R.Z., S.N., and B.X. contributed to patient recruitment, data collection, and data curation. Y.L., X.L., F.Y., and G.Y. performed data analysis, interpreted the results, and revised the manuscript. F.Y. and G.Y. supervised the study and provided critical intellectual input. All authors contributed to the work, participated in drafting or revising the manuscript, approved the final version, agreed on the target journal, and accept accountability for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 82000043) and the Capital’s Funds for Health Improvement and Research (Grant No. 2024-2-1101).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2026 report. Available from: https://goldcopd.org/2026-gold-report-and-pocket-guide/.
2. Xu Z, Li F, Xin Y, et al. Prognostic risk prediction model for patients with acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Res. 2024;25(1):410. doi:10.1186/s12931-024-03033-4
3. Poparcea D, Corlateanu A, Ceasovschih A, et al. Cardiopulmonary exercise testing in chronic obstructive pulmonary disease. Physiol Int. 2025;112(4):428–13. doi:10.1556/2060.2025.00704
4. Glaab T, Taube C. Practical guide to cardiopulmonary exercise testing in adults. Respir Res. 2022;23(1):9. doi:10.1186/s12931-021-01895-6
5. Stickland MK, Neder JA, Guenette JA, et al. Using cardiopulmonary exercise testing to understand dyspnea and exercise intolerance in respiratory disease. Chest. 2022;161(6):1505–1516. doi:10.1016/j.chest.2022.01.021
6. Behnia M, Sietsema KE. Utility of cardiopulmonary exercise testing in chronic obstructive pulmonary disease: a review. Int J Chron Obstruct Pulmon Dis. 2023;18:2895–2910. doi:10.2147/COPD.S432841
7. Radtke T, Crook S, Kaltsakas G, et al. ERS statement on standardisation of cardiopulmonary exercise testing in chronic lung diseases. Eur Respir Rev. 2019;28(154):180101. doi:10.1183/16000617.0101-2018
8. Wasserman K, Hansen JE, Sue DY, et al. Principles of Exercise Testing and Interpretation: Including Pathophysiology and Clinical Applications.
9. Neder JA, Santyr G, Zanette B, et al. Beyond spirometry: linking wasted ventilation to exertional dyspnea in the initial stages of COPD. COPD. 2024;21(1):2301549. doi:10.1080/15412555.2023.2301549
10. James MD, Berton DC, Neder JA. Activity-related dyspnea and exercise intolerance in chronic obstructive pulmonary disease: recent insights. Curr Opin Pulm Med. 2025;31(2):145–155. doi:10.1097/MCP.0000000000001146
11. Duong ML, Qian C, Talukdar M, et al. Frequency and severity of COPD exacerbations and future risk of exacerbations and mortality: an observational cohort study in Canada. BMJ Open Respir Res. 2025;12(1):e002976. doi:10.1136/bmjresp-2024-002976
12. O’Donnell DE, Laveneziana P, Webb KA, Neder JA. Chronic obstructive pulmonary disease: clinical integrative physiology. Clin Chest Med. 2014;35(1):51–69. doi:10.1016/j.ccm.2013.09.008
13. Maeda T, Dransfield MT. Chronic obstructive pulmonary disease and cardiovascular disease: mechanistic links and implications for practice. Curr Opin Pulm Med. 2024;30(2):141–149. doi:10.1097/MCP.0000000000001040
14. Daniels K, Lanes S, Tave A, et al. Risk of death and cardiovascular events following an exacerbation of COPD: the EXACOS-CV US study. Int J Chron Obstruct Pulmon Dis. 2024;19:225–241. doi:10.2147/COPD.S438893
15. Simons SO, Heptinstall AB, Marjenberg Z, et al. Temporal dynamics of cardiovascular risk in patients with chronic obstructive pulmonary disease during stable disease and exacerbations: review of the mechanisms and implications. Int J Chron Obstruct Pulmon Dis. 2024;19:2259–2271. doi:10.2147/COPD.S466280
16. Matsunaga K, Yoshida Y, Makita N, et al. Increased risk of severe cardiovascular events following exacerbations of chronic obstructive pulmonary disease: results of the EXACOS-CV study in Japan. Adv Ther. 2024;41(8):3362–3377. doi:10.1007/s12325-024-02920-y
17. Vaes AW, Burtin C, Casaburi R, et al. Prevalence and prognostic importance of exercise limitation and physical inactivity in COPD. Breathe. 2024;20(2):230179. doi:10.1183/20734735.0179-2023
18. Wang M, Ni X, Yu F. Impact of body mass index on the risk of exacerbation in patients with COPD: a systematic review and meta-analysis. Chronic Obstr Pulm Dis. 2024;11(5):524–533. doi:10.15326/jcopdf.2024.0507
19. Putcha N, Anzueto AR, Calverley PMA, et al. Mortality and exacerbation risk by body mass index in patients with COPD in TIOSPIR and UPLIFT. Ann Am Thorac Soc. 2022;19(2):204–213. doi:10.1513/AnnalsATS.202006-722OC
20. Kim EK, Singh D, Park JH, et al. Impact of body mass index change on the prognosis of chronic obstructive pulmonary disease. Respiration. 2020;99(11):943–953. doi:10.1159/000511022
21. Hu C, Song B, Liu X. The association between COPD, acute exacerbations of COPD, and survival in COPD with fat-free body mass index: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2025;20:2025–2040. doi:10.2147/COPD.S526194
22. Nici L. Pulmonary rehabilitation: mechanisms of functional loss and benefits of exercise. Respir Care. 2024;69(6):640–650. doi:10.4187/respcare.11705
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Multivariable Prediction Model to Identify Acute Exacerbation of COPD and Its Severity for COPD Management in China (DETECT Study): A Multicenter, Observational, Cross-Sectional Study
Yin Y, Xu J, Cai S, Chen Y, Chen Y, Li M, Zhang Z, Kang J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2093-2106
Published Date: 5 September 2022
The Influence of Influenza Virus Infections in Patients with Chronic Obstructive Pulmonary Disease
Liao KM, Chen YJ, Shen CW, Ou SK, Chen CY
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2253-2261
Published Date: 14 September 2022
Analyses of Factors Associated with Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Review
Qian Y, Cai C, Sun M, Lv D, Zhao Y
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2707-2723
Published Date: 24 November 2023
The Relationship of Fractional Exhaled Nitric Oxide in Patients with AECOPD
Xu X, Zhou L, Tong Z
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:3037-3046
Published Date: 21 December 2023
Glucocorticoid Use in Patients Hospitalized with Chronic Obstructive Pulmonary Disease Exacerbations
Yu S, Li S, Zhang J, Fang Q
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:431-438
Published Date: 12 February 2024