Back to Journals » International Journal of Women's Health » Volume 18
Epidemiological Risk Factor Analysis for Maternal Mortality Associated with Eclampsia: A Single-Center Study from Tertiary Hospital Garut
Authors Susandi D ![]() , Martani RA, Adriansyah PNA
, Martani RA, Adriansyah PNA ![]() , Nugrahani AD
, Nugrahani AD ![]() , Santoso DPJ, Sribudiani Y
, Santoso DPJ, Sribudiani Y ![]() , Anwar R
, Anwar R ![]() , Mose JC
, Mose JC
Received 22 September 2025
Accepted for publication 6 March 2026
Published 14 March 2026 Volume 2026:18 569262
DOI https://doi.org/10.2147/IJWH.S569262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Dadan Susandi,1,2 Rizky Alamsyah Martani,2 Putri Nadhira Adinda Adriansyah,1 Annisa Dewi Nugrahani,1 Dhanny Primantara Johari Santoso,1,2 Yunia Sribudiani,3 Ruswana Anwar,2 Johanes Cornelius Mose2
1Department of Obstetrics and Gynecology, Universitas Padjadjaran, Dr.Slamet General Hospital Garut, Garut, West Java, Indonesia; 2Department of Obstetrics and Gynecology, Universitas Padjadjaran, Hasan Sadikin General Teaching Hospital, Bandung, West Java, Indonesia; 3Molecular Genetic Division, Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Dadan Susandi, Department of Obstetrics and Gynecology, Universitas Padjadjaran, Dr.Slamet General Hospital Garut, Jl. Rumah Sakit, No. 12, Sukakarya, Tarogong Kidul, Garut, West Java, Indonesia, Tel +6281323015358, Email [email protected]
Background: Maternal mortality remains a major global health challenge, particularly in low- and middle-income countries. Eclampsia, a severe complication of hypertensive disorders in pregnancy, continues to contribute substantially to maternal and perinatal deaths despite advances in obstetric care. Previous studies have highlighted the role of clinical and laboratory abnormalities in worsening outcomes; however, evidence from developing settings remains limited. A clearer understanding of maternal mortality risk factors in eclampsia is essential to improve early detection, risk stratification, and clinical management.
Objective: To identify maternal mortality risk factors associated with eclampsia based on patient characteristics, clinical presentation, and laboratory findings.
Methods: A retrospective observational study was conducted using medical records of pregnant women diagnosed with eclampsia between January 2022 and March 2024 at a tertiary referral hospital. Demographic data, clinical features, and laboratory parameters were extracted systematically. Statistical analysis included univariate and bivariate analyses using the Chi-square test to assess associations between variables and maternal mortality. Multivariate logistic regression analysis was performed to determine independent risk factors and estimate odds ratios (OR) with corresponding p-values. Statistical significance was set at p ≤ 0.05.
Results: A total of 112 patients met the inclusion criteria. The eclampsia case fatality rate was 20.54%. Laboratory parameters demonstrated significant associations with maternal mortality. Severe proteinuria (+3) was associated with increased mortality risk (OR = 1.67; p = 0.05). Anemia, defined as hematocrit < 35%, showed a strong association with maternal death (OR = 2.25; p = 0.001). Additionally, HELLP syndrome significantly increased the risk of maternal mortality (OR = 2.82).
Conclusion: Laboratory abnormalities are key predictors of maternal mortality in eclampsia. Severe proteinuria, anemia, and HELLP syndrome should be promptly identified and managed to reduce adverse maternal outcomes.
Keywords: epidemiology, case fatality rate, eclampsia, risk factors
Introduction
Maternal mortality remains a critical indicator of health system performance, particularly in low- and middle-income countries. The World Health Organization defines maternal death as the death of a woman during pregnancy or within 42 days after the termination of pregnancy due to causes related to or aggravated by pregnancy.1 Despite global efforts to reduce maternal mortality, hypertensive disorders of pregnancy, especially preeclampsia and eclampsia, continue to be leading causes of maternal death worldwide.2,3
In Indonesia, maternal mortality has declined over recent decades; however, the burden remains substantial. A systematic review by Syairaji et al in 2024 reported a national maternal mortality ratio of 249 per 100,000 live births between 2016 and 2020, representing a 45% reduction compared to 1990.4 Importantly, the pattern of maternal death has shifted. While obstetric hemorrhage was previously the predominant cause, hypertensive disorders and non-obstetric complications now account for a large proportion of maternal deaths. Preeclampsia, eclampsia, and HELLP syndrome together contributed 14.6% of the maternal fatalities in Indonesia.4
Eclampsia is a severe and life-threatening pregnancy complication characterized by generalized tonic clonic seizures in women with hypertensive disorders of pregnancy.5 Although its incidence has decreased in high-income countries, eclampsia remains common in low-resource settings, with reported incidence rates ranging from 50 to 151 per 10,000 deliveries.6 Maternal mortality associated with preeclampsia and eclampsia remains high, with reported fatality rates of 5 to 20%, particularly among young women.7
Previous studies have identified several factors associated with increased mortality in eclampsia, including HELLP syndrome, disseminated intravascular coagulation, acute kidney injury, pulmonary edema, acute respiratory distress syndrome, and central nervous system hemorrhage.5,8 Laboratory abnormalities such as severe proteinuria, anemia, thrombocytopenia, and liver dysfunction have also been associated with poor maternal outcomes.9 However, the relative contribution of these factors may vary across institutions due to differences in patient characteristics, referral patterns, and available resources.
Given the persistent contribution of eclampsia to maternal mortality in Indonesia, evaluating institution-specific risk factors is essential. This study aims to examine epidemiological, clinical, and laboratory risk factors associated with maternal death due to eclampsia at our institution to support earlier risk identification and improved clinical management strategies.
Materials and Methods
Study Design and Setting
This study employed an observational analytic design with a cross-sectional approach. The study was conducted at Dr. Slamet Garut Regional General Hospital. Data were collected retrospectively from medical records of patients treated between January 2022 and March 2024.
Study Population
The study population consisted of pregnant women diagnosed with eclampsia who were treated at the emergency maternal unit of Dr. Slamet Garut Regional General Hospital during the study period. Total sampling was applied to include all eligible cases that met the predefined inclusion criteria. The target population comprised all pregnant women attending the hospital, while the accessible population included patients with a confirmed diagnosis of eclampsia managed at the emergency maternal unit.
Inclusion and Exclusion Criteria
Inclusion criteria were pregnant women referred to or treated at Dr. Slamet Garut Regional General Hospital between 2022 and 2024 with a clinical diagnosis of eclampsia. Exclusion criteria included incomplete medical records, multiple pregnancies, seizures attributed to epilepsy, and patients with documented pre-existing neurological disorders prior to pregnancy.
Data Collection and Statistical Analysis
Data were extracted systematically from medical records and included patient demographic characteristics, clinical findings, and laboratory parameters. Data processing involved data editing to ensure completeness and accuracy, coding of variables, data entry into a master database, and tabulation. Statistical analysis was performed using IBM SPSS Statistics version 29.0.1.0. Univariate analysis was conducted to describe variable distributions. Bivariate analysis using the chi-square test was applied to assess associations between independent variables and maternal mortality. Multivariate logistic regression analysis was performed to identify independent risk factors and calculate odds ratios. Statistical significance was defined as a p value of 0.05 or less. Results are presented as proportions, odds ratios, p values, and tables.
Result
Table 1 presents the demographic and clinical characteristics of the study population. Most participants were aged 20–30 years (66.1%), and a large proportion were overweight or obese (78.5%). More than half of the participants were at a gestational age of ≥34 weeks (58.0%), while 15.2% were in the postpartum period. Primiparous women constituted 53.6% of the study population, and the majority had fewer than six antenatal care visits (63.4%). In terms of educational background, most participants had completed senior high school or lower (98.2%).
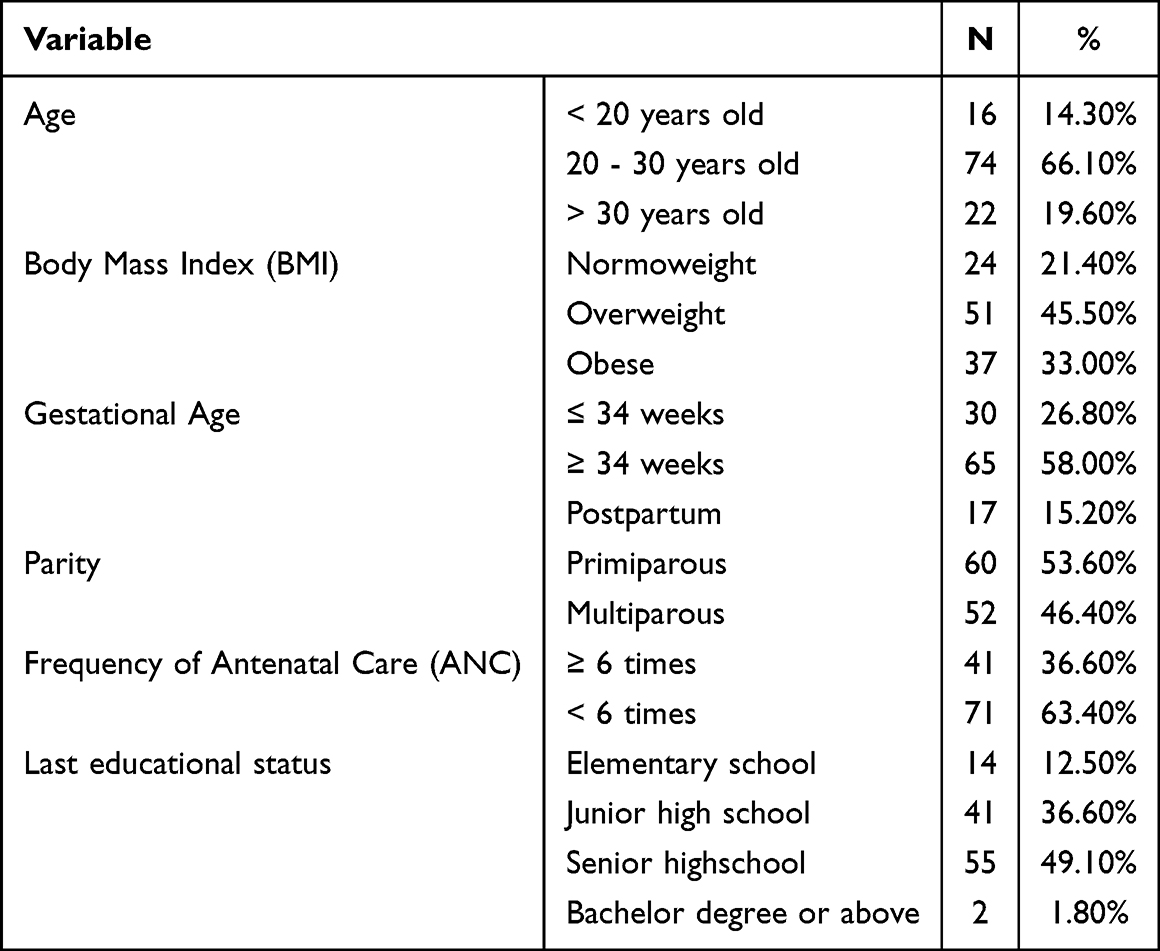 |
Table 1 Demographic and Clinical Characteristics of the Study Population |
Table 2 summarizes the clinical symptoms and blood pressure characteristics of the participants. Edema was present in 35.7% of cases, headache in 66.1%, upper abdominal pain in 33.0%, and blurred vision in 40.2%. Elevated systolic blood pressure (≥140 mmHg) was observed in 97.3% of participants, while diastolic blood pressure ≥90 mmHg was recorded in 93.8%, indicating a high prevalence of hypertension-related clinical features in the study population.
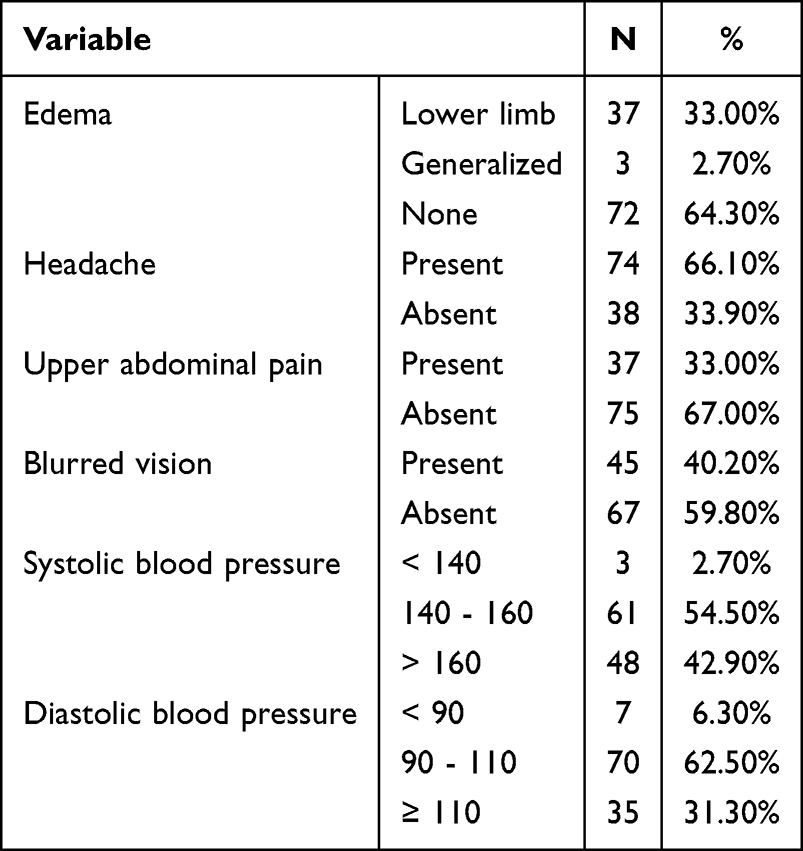 |
Table 2 Clinical Symptoms and Blood Pressure Characteristics of Study Participants |
Table 3 presents laboratory findings and the prevalence of HELLP syndrome among study participants. Proteinuria was detected at varying degrees, with 17% having 1+, 40.2% showing 2+, and 42.9% presenting with ≥3+. Hemoglobin levels were distributed almost equally, with 45.5% having levels ≥11 g/dL, while 54.5% had levels below 11 g/dL.
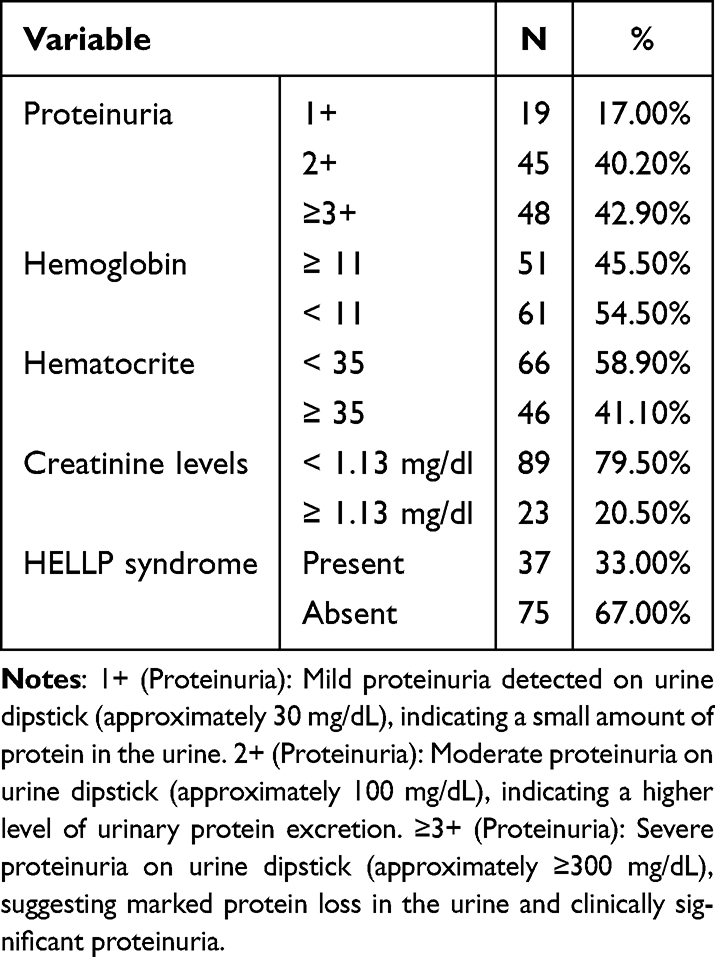 |
Table 3 Laboratory Parameters and HELLP Syndrome in Study Participants |
Regarding hematocrit levels, 58.9% of participants had values below 35, whereas 41.1% had levels ≥35. Serum creatinine levels were predominantly below 1.13 mg/dL (79.5%), with 20.5% having elevated levels (≥1.13 mg/dL). Additionally, HELLP syndrome was identified in 33% of participants, while 67% did not exhibit this condition.
Table 4 shows the case fatality rate of eclampsia among study participants. A total of 112 cases of eclampsia were recorded, with 23 deaths attributed to the condition. This results in a case fatality rate of 20.54%, indicating that approximately one in five patients with eclampsia did not survive. These findings highlight the significant mortality risk associated with eclampsia and underscore the importance of timely medical intervention and management to improve patient outcomes.
 |
Table 4 Case Fatality Rate of Eclampsia Cases |
Table 5 shows that several maternal factors are associated with perinatal mortality risk. The table presents a comparative analysis between deceased and surviving cases based on maternal age, body mass index (BMI), gestational age, parity, antenatal care visits, and education level. The odds ratio (OR) and p-value for each variable indicate the strength and significance of these associations.
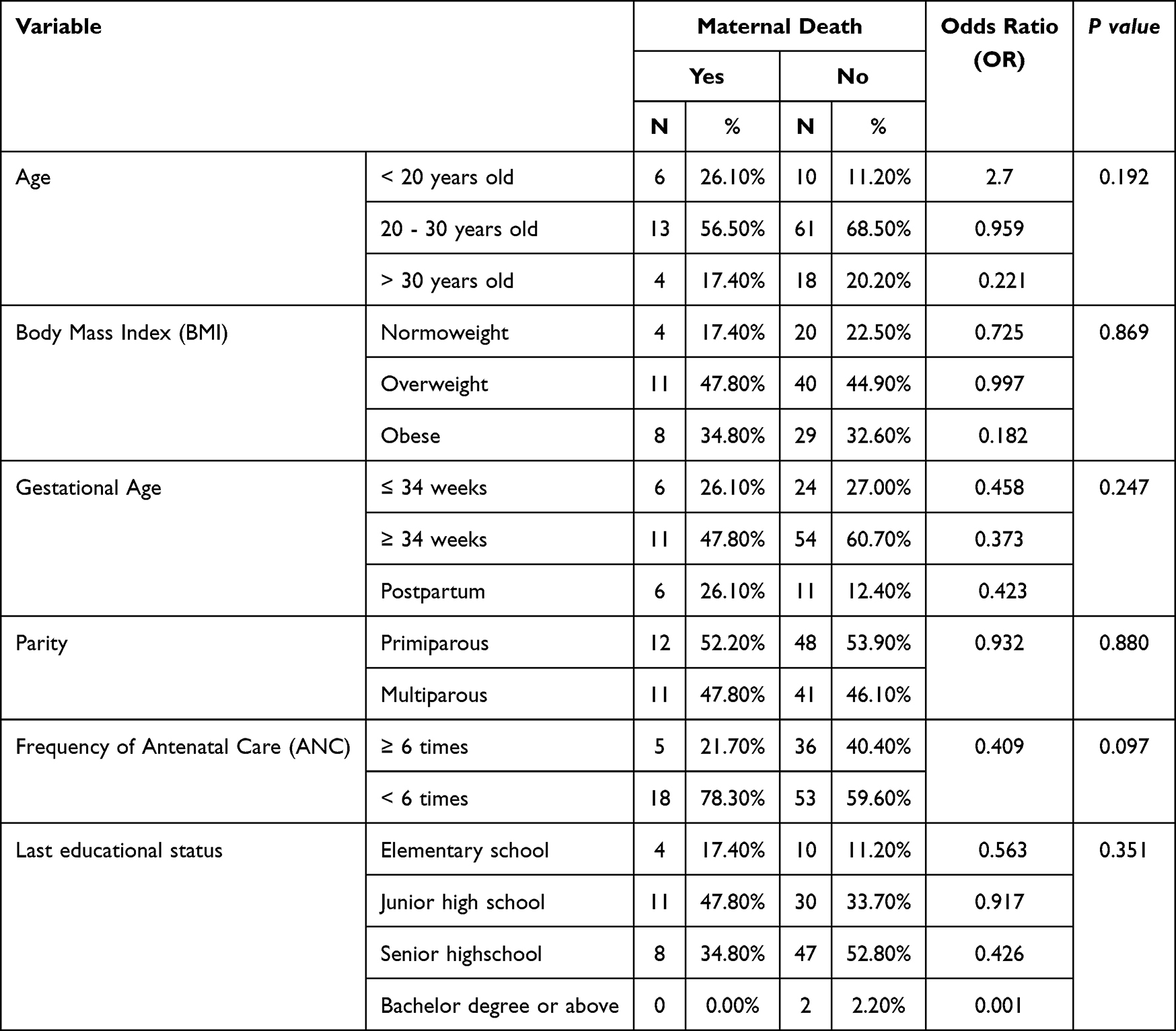 |
Table 5 Maternal Risk Factors Based on Demographic and Clinical Characteristics |
Younger mothers (<20 years) had a higher odds ratio (OR = 2.7) for mortality compared to older age groups, although the association was not statistically significant (p = 0.192). Regarding BMI, obese mothers had a lower odds ratio (OR = 0.182) compared to normoweight mothers, but this relationship was also not significant (p = 0.869). Gestational age at delivery did not show a significant impact on mortality outcomes (p = 0.247).
Table 5 also shows that antenatal care is an important factor in reducing mortality risk. Women who had fewer than six antenatal visits had a higher mortality rate (78.3%) than those with more visits (21.7%). The odds ratio for this variable (OR = 0.409) suggests a potential protective effect, with a borderline p-value (0.097). The last education status variable produced a p-value of 0.351 > 0.05, indicating no association between the last education status and eclampsia case mortality.
Table 6 shows that clinical symptoms such as edema, headache, upper abdominal pain, blurred vision, and blood pressure levels were analyzed as potential risk factors for mortality in eclampsia cases. The table presents the frequency and percentage of mortality cases in relation to these factors, along with the odds ratio (OR) and p-value for statistical significance based on the chi-square test.
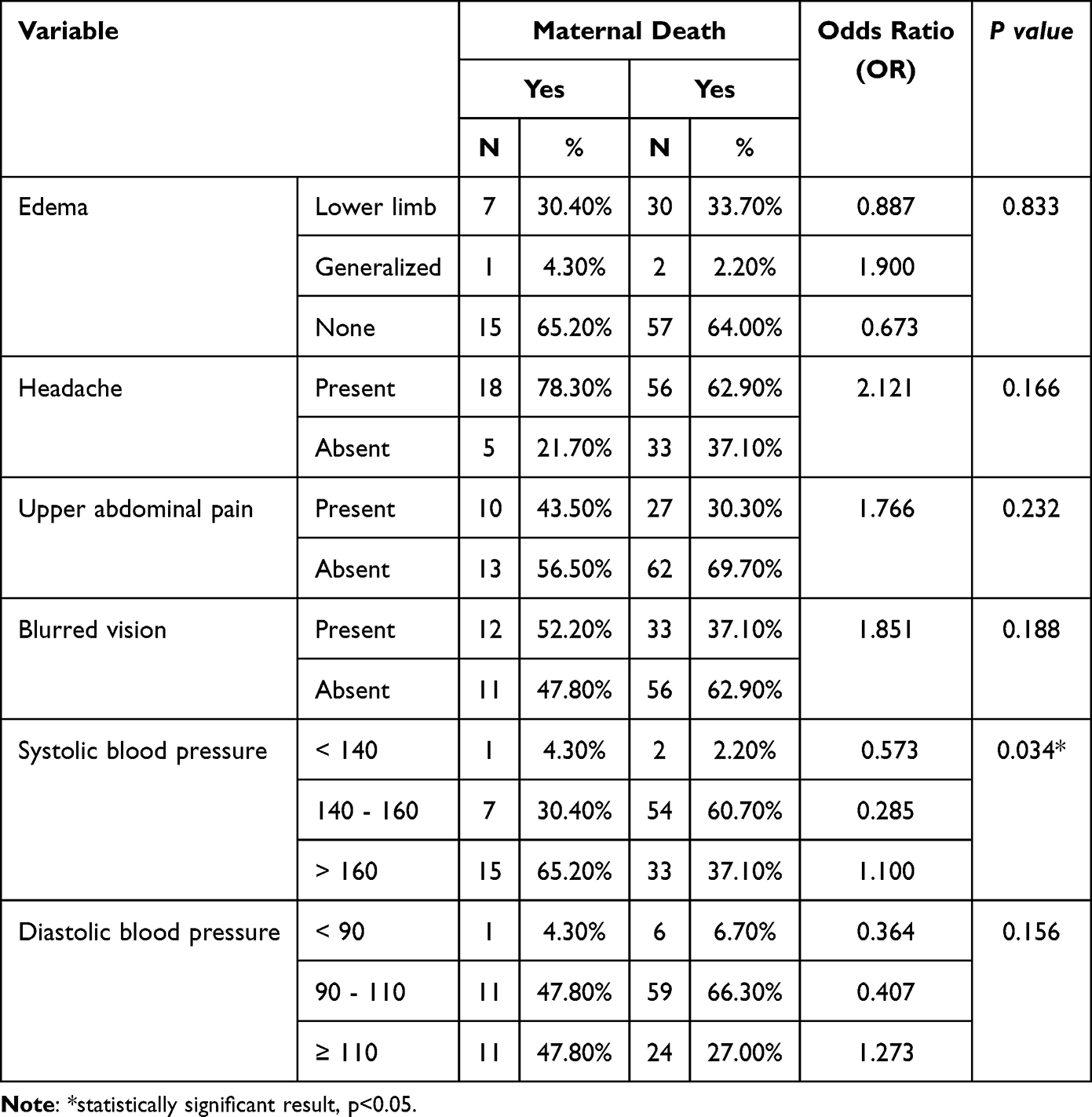 |
Table 6 Clinical Symptoms and Blood Pressure as Risk Factors for Maternal Mortality |
The results indicate that edema (p = 0.833), headache (p = 0.166), upper abdominal pain (p = 0.232), and blurred vision (p = 0.188) are not significantly associated with mortality in eclampsia cases, as their p-values exceed the 0.05 threshold. This suggests that these symptoms alone do not significantly contribute to the risk of death.
However, systolic blood pressure (p = 0.034) is significantly associated with mortality, indicating that higher systolic blood pressure levels may play a critical role in determining fatal outcomes in eclampsia cases. In contrast, diastolic blood pressure does not show a significant association with mortality.
Table 7 shows that proteinuria is not significantly associated with mortality in eclampsia cases, as indicated by a p-value of 0.050 (p > 0.05). However, hemoglobin (p = 0.001), hematocrit (p = 0.001), creatinine (p = 0.001), and HELLP syndrome (p = 0.001) all demonstrated significant associations with mortality (p < 0.05). Patients with hemoglobin levels ≥11 g/dL had a 0.078 times lower risk of mortality compared to those with hemoglobin <11 g/dL. Similarly, patients with hematocrit <35% had 2.25 times higher odds of mortality than those with hematocrit ≥35%. Creatinine levels ≥1.13 mg/dL were linked to a 1.672 times greater risk of mortality, and individuals with HELLP syndrome had 2.825 times higher odds of death compared to those without it. These findings indicate that hematological and renal dysfunction, along with the presence of HELLP syndrome, are significant risk factors for mortality in eclampsia cases.
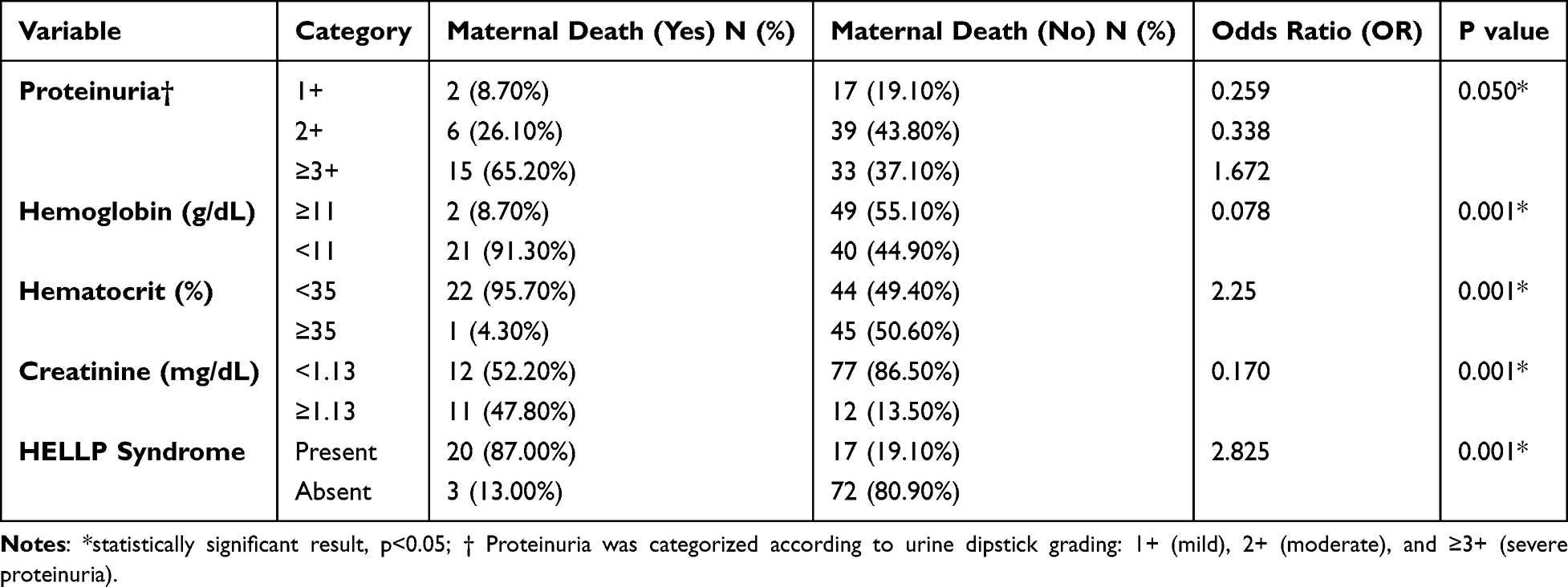 |
Table 7 Association Between Laboratory Parameters, HELLP Syndrome, and Maternal Mortality in Eclampsia Cases |
Discussion
This study identified several key predictors of maternal mortality among patients with eclampsia, with laboratory abnormalities and severe clinical manifestations showing the strongest associations. The causes of maternal death in eclampsia are closely linked to end organ dysfunction, including cerebral complications, renal failure, hematological disturbances, and hepatic involvement. These mechanisms are reflected in the statistically significant associations observed in this study.
Severe systolic hypertension was significantly associated with maternal death. Patients with systolic blood pressure greater than 160 mmHg had higher mortality compared to those with lower systolic values, with a statistically significant association (p = 0.034). The odds ratio for maternal death in patients with systolic blood pressure above 160 mmHg was 1.10. This finding highlights the role of uncontrolled hypertension in precipitating fatal complications such as intracranial hemorrhage and hypertensive encephalopathy.
Severe systolic hypertension was significantly associated with maternal death. Patients with systolic blood pressure greater than 160 mmHg had higher mortality compared to those with lower systolic values, with a statistically significant association (p = 0.034). The odds ratio for maternal death in patients with systolic blood pressure above 160 mmHg was 1.10. This finding highlights the role of uncontrolled hypertension in precipitating fatal complications such as intracranial hemorrhage and hypertensive encephalopathy.10,11
Similar findings were reported in the CLIP trials, where increasing systolic and diastolic blood pressure levels were associated with higher maternal and perinatal mortality and morbidity.10 Vigil et al also demonstrated an independent association between severe systolic hypertension and maternal mortality in eclamptic patients.12 These findings support current recommendations for careful but timely blood pressure control in eclampsia.8,13
Anemia was one of the strongest predictors of maternal mortality in this study. Hemoglobin <11 g/dL was significantly associated with maternal death (OR for hemoglobin ≥11 g/dL = 0.078, p = 0.001). Low hematocrit was also strongly associated with maternal death, with hematocrit <35% increasing the odds of mortality (OR = 2.25, p = 0.001). These findings suggest that reduced oxygen carrying capacity may worsen the effects of severe hypertension and increase susceptibility to multiorgan failure.14,15 Previous studies have reported similar associations between anemia and maternal mortality in eclampsia and severe preeclampsia.16,17
Renal dysfunction also contributed significantly to maternal mortality. Creatinine ≥1.13 mg/dL was significantly associated with maternal death (OR = 0.170, p = 0.001). Elevated creatinine reflects impaired renal perfusion and glomerular injury, which may progress to acute kidney failure and systemic metabolic derangements.18 Although evidence on creatinine thresholds is inconsistent, the present results support renal impairment as an important predictor of adverse outcomes in eclampsia.18,19
HELLP syndrome emerged as the strongest predictor of maternal mortality in this study. The presence of HELLP syndrome significantly increased the odds of maternal death (OR = 2.825, p = 0.001). HELLP syndrome contributes to maternal death through mechanisms such as disseminated intravascular coagulation, hepatic failure, pulmonary edema, and multiorgan dysfunction.20 This finding is consistent with previous studies identifying HELLP syndrome as a major determinant of maternal mortality in eclamptic patients.12,19 Early diagnosis and aggressive management are essential to reduce fatal outcomes.16,20
Overall, this study demonstrates that laboratory-based indicators of organ dysfunction, including anemia, renal impairment, and HELLP syndrome, are more strongly associated with maternal mortality than demographic characteristics or isolated clinical symptoms. These findings emphasize the importance of comprehensive laboratory evaluation and early risk stratification in patients with eclampsia. However, the cross-sectional design limits causal inference and may introduce selection bias. Future prospective studies are needed to further clarify causal pathways and improve predictive models for maternal mortality.
Conclusion
This study underscores the importance of comprehensive laboratory evaluation in patients presenting with eclampsia. Severe proteinuria, low hemoglobin levels, and HELLP syndrome were associated with increased maternal mortality. These findings are particularly relevant in low- and middle-income countries, where resource and logistical constraints may limit the availability and frequency of laboratory investigations, potentially delaying risk stratification and timely intervention. Future studies using stronger study designs are warranted to confirm these findings and further clarify independent predictors of maternal death in eclampsia.
Data Sharing Statement
Datasets used in this article are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study complies with the Declaration of Helsinki and was approved by the Health Research Ethics Committee of RSUD Dr. Slamet Garut with approval number 00001/KEP/RSUD/B/VIII/2025. Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cresswell J. Maternal deaths. World Health Organization. Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/4622.
2. Centers for Disease Control and Prevention (CDC). Preventing pregnancy-related deaths. Maternal Mortality Prevention. 2024. Available from: https://www.cdc.gov/maternal-mortality/preventing-pregnancy-related-deaths/index.html.
3. World Health Organization. Trends in Maternal Mortality: 1990 to 2015: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: World Health Organization; 2015.
4. Syairaji M, Nurdiati DS, Wiratama BS, Prüst ZD, Bloemenkamp KWM, Verschueren KJC. Trends and causes of maternal mortality in Indonesia: a systematic review. BMC Pregnancy Childbirth. 2024;24(1):515. doi:10.1186/s12884-024-06687-6
5. Fishel Bartal M, Sibai BM. Eclampsia in the 21st century. Am J Obstet Gynecol. 2022;226(2):S1237–9. doi:10.1016/j.ajog.2020.09.037
6. Sriyanti R, Aldhi A, Permatasari R. Atypical eclampsia: a case report. Andalas Obstet Gynecol J. 2022;6(2):167–172. doi:10.25077/aoj.6.2.167-172.2022
7. Laskowska M. Eclampsia: a critical pregnancy complication demanding enhanced maternal care: a review. Med Sci Monit. 2023;29:e939919. doi:10.12659/MSM.939919
8. ACOG. Gestational hypertension and preeclampsia: ACOG practice bulletin, number 222. Obstet Gynecol. 2020;135(6):e237–e60. doi:10.1097/AOG.0000000000003891
9. Lei T, Qiu T, Liao W, et al. Proteinuria may be an indicator of adverse pregnancy outcomes in patients with preeclampsia: a retrospective study. Reprod Biol Endocrinol. 2021;19(1):71. doi:10.1186/s12958-021-00751-y
10. Magee LA, Bone J, Owasil SB, et al. Pregnancy outcomes and blood pressure visit-to-visit variability and level in three less-developed countries. Hypertension. 2021;77(5):1714–1722. doi:10.1161/HYPERTENSIONAHA.120.16851
11. Hannola K, Hoppu S, Mennander S, Huhtala H, Laivuori H, Tihtonen K. Obstetric early warning system to predict maternal morbidity of pre-eclampsia, postpartum hemorrhage and infection after birth in high-risk women: a prospective cohort study. Midwifery. 2021;99:103015. doi:10.1016/j.midw.2021.103015
12. Vigil‐De Gracia P, Rojas‐Suarez J, Ramos E, et al. Incidence of eclampsia with HELLP syndrome and associated mortality in Latin America. Int J Gynaecol Obstet. 2015;129(3):219–222. doi:10.1016/j.ijgo.2014.11.024
13. Balahura A-M, Moroi Ș-I, Scafa-Udrişte A, et al. The management of hypertensive emergencies—is there a “magical” prescription for all? Clin Med. 2022;11(11):3138. doi:10.3390/jcm11113138
14. Ali AA, Rayis DA, Abdallah TM, Elbashir MI, Adam I. Severe anaemia is associated with a higher risk for preeclampsia and poor perinatal outcomes in Kassala hospital, eastern Sudan. BMC Res Notes. 2011;4(1):311. doi:10.1186/1756-0500-4-311
15. Johnson A, Vaithilingan S, Avudaiappan SL. The interplay of hypertension and anemia on pregnancy outcomes. Cureus. 2023;15(10):e46390. doi:10.7759/cureus.46390
16. Bano E, Mahar T, Malhi P, Hashmi S, Soomro A, Khoso S. Risk factors of eclampsia and its maternal and perinatal effects at a tertiary hospital: a retrospective study: risk factors of eclampsia and its maternal effects at a tertiary hospital. Pakistan J Health Sci. 2022;194–198. doi:10.54393/pjhs.v3i05.202
17. Gupta G. A case control study to evaluate correlation of anemia with severe preeclampsia. Int J Reproduct Contracept Obstet Gynecol. 2018;7(7):2773. doi:10.18203/2320-1770.ijrcog20182879
18. Selamat A. Clinical and laboratory profiles relationships of preeclampsia-eclampsia patients with maternal mortality in Dr. Soetomo Hospital, Surabaya. Surabaya Majalah Obstetri Ginekologi. 2012;20(1):35–39.
19. Khusen D. Factors influencing maternal mortality from severe preeclampsia and eclampsia. Indonesian Obste Gynecol. 2012.
20. Lam MC, Dierking E. Intensive care unit issues in eclampsia and HELLP syndrome. Int J Critical Illness Injury Sci. 2017;7(3):136–141. doi:10.4103/IJCIIS.IJCIIS_33_17
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Scoping Review on the Status of Female Breast Cancer in Asia with a Special Focus on Nepal
Dhakal R, Noula M, Roupa Z, Yamasaki EN
Breast Cancer: Targets and Therapy 2022, 14:229-246
Published Date: 26 August 2022
Burden of Metabolic Syndrome Among a Low-Income Population in China: A Population-Based Cross-Sectional Study
Bao J, Wang L, Hu P, Liu J, Tu J, Wang J, Li J, Ning X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2713-2723
Published Date: 3 September 2022
Clinical Features of Human Brucellosis and Risk Factors for Focal Complications: A Retrospective Analysis in a Tertiary-Care Hospital in Beijing, China
Zhang Z, Zhang X, Chen X, Cui X, Cai M, Yang L, Zhang Y
International Journal of General Medicine 2022, 15:7373-7382
Published Date: 19 September 2022
Prevalence and Associated Factors of Urinary Tract Infection in Patients with Diabetic Neuropathy: A Hospital-Based Cross-Sectional Study
Wang X, Wang Y, Luo L, Tan L, Cai W, Chen L, Ren W
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1261-1270
Published Date: 3 May 2023
Prevalence, Risk Factors, and Impact on Life of Female Urinary Incontinence: An Epidemiological Survey of 9584 Women in a Region of Southeastern China
Wang Q, Que YZ, Wan XY, Lin CQ
Risk Management and Healthcare Policy 2023, 16:1477-1487
Published Date: 9 August 2023