Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Enhancing Creativity and Innovation in Medical Sciences Students Through Multidisciplinary Problem-Based Learning (MPBL): A Pre-Post Intervention Study
Authors Sarhadi M, Aliabadi F, Jiryaee N, Seidi M ![]()
Received 4 February 2026
Accepted for publication 2 July 2026
Published 10 July 2026 Volume 2026:19 601318
DOI https://doi.org/10.2147/JMDH.S601318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Maryam Sarhadi,1 Faezeh Aliabadi,1 Nasrin Jiryaee,2 Masoumeh Seidi3
1Hamadan University of Medical Sciences, Hamadan, Iran; 2Department of Social Medicine, School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran; 3Educational Development Center (EDC), Hamadan University of Medical Sciences, Hamadan, Iran
Correspondence: Masoumeh Seidi, Educational Development Center (EDC), Hamadan University of Medical Sciences, Hamadan, Iran, Tel +98 915 557 3059, Email [email protected]
Introduction: The growing complexity of healthcare systems requires the development of creativity and innovation among health professionals. These competencies are essential for professional growth and entrepreneurial thinking. Problem-Based Learning (PBL) and Multidisciplinary approaches have been recognized as effective strategies to foster such skills. This study aimed to evaluate the effectiveness of Multidisciplinary Problem-Based Learning (MPBL) in promoting creativity and innovation among medical sciences students.
Materials and Methods: This pre-post interventional study was conducted in 2024 with 70 students from various medical disciplines at Hamadan University of Medical Sciences. Participants engaged in three 4-hour MPBL workshops (12 hours total) featuring clinical scenarios on sepsis, cardiac arrest, and multiple trauma. The intervention incorporated higher-order thinking activities, structured group discussions, and debriefing sessions. Creativity was assessed using the abbreviated figural version of the Torrance Tests of Creative Thinking (TTCT), and innovation was measured using an adapted version of the Research and Innovation Competency Measure Questionnaire (RIC-MQ). Satisfaction was also evaluated. Data were analyzed using SPSS version 24.
Results: Participants had a mean age of 21.83 years, with 66.2% female. Overall, creativity and innovation scores increased significantly post-intervention (p < 0.05), except for innovation in the medical group and creativity in the midwifery group. High satisfaction was reported by 58.6% of participants. Although some changes reached statistical significance, the short intervention period limits the ability to infer sustained or educationally meaningful learning; thus, findings are presented as proof-of-concept.
Conclusion: MPBL may be associated with short-term improvements in creativity and innovation among medical sciences students. However, the pre-post design precludes causal attribution, and results should be interpreted as preliminary. Observed variations across disciplines underscore the need for further research with larger, more diverse samples and controlled designs to assess broader applicability.
Keywords: creativity, problem-based learning, multidisciplinary, education, students, undergraduate
Introduction
In today’s world, healthcare systems are confronted with emerging challenges and complexities that demand creative and innovative skills among physicians and healthcare professionals.1 Teaching creativity and innovation to medical sciences students is essential, as they are the future physicians who will play a central role in advancing medical discoveries and promoting health sciences. Moreover, the current medical knowledge taught to them is itself the product of creativity and innovation by previous generations of medical professionals.2 Given the rising unemployment rates among university graduates in developing countries, including ours, fostering creativity and innovation can contribute significantly to entrepreneurial mindset development. Creativity plays a vital role in the entrepreneurial process, as more creative individuals are better able to maintain self-confidence and a positive attitude.3 Globally, creativity and innovation have been increasingly recognized as essential competencies within competency-based medical education frameworks—such as the CanMEDS and ACGME models—which emphasize adaptability, problem solving, and creative leadership as core professional capabilities.4 Creativity involves divergent thinking (fluency, flexibility, originality, and elaboration,2 while innovation is the successful implementation of creative ideas4 and requires additional skills like planning and persistence. Both are essential in health professions education,1 necessitating effective educational strategies to cultivate them.
One of the key steps in this direction is selecting appropriate educational methods. Problem-Based Learning (PBL) has been widely used in higher education for its effectiveness in enhancing students’ creativity.5 PBL is a learner-centered approach grounded in real-life problems, providing an opportunity for individuals to engage in production and creative processes.6 Additionally, problem-solving-based learning strengthens skills such as teamwork and the development of creative solutions within an existing informational framework.7
In conventional PBL, students from just one discipline work in small groups to solve a problem, with learning occurring basically within that professional field. In contrast, the Multidisciplinary Problem-Based Learning (MPBL) approach applied in this study intentionally brings learners from five disciplines (including: medicine, nursing, midwifery, surgical technology, and anesthesiology) together to collaboratively address a shared clinical scenario. Unlike standard interprofessional education (IPE) which often focuses on role clarification and teamwork theory, MPBL embeds interprofessional interaction within the problem-solving process itself. Each workshop involved small groups of 4–5 learners (representing at least three of the five disciplines) who jointly identified learning objectives, shared discipline-specific perspectives, and negotiated an appropriate collaborative response related to clinical scenarios. The key distinction from conventional PBL is the explicit requirement for cross-disciplinary negotiation and integration of different professional knowledge to resolve the scenario, rather than independent learning followed by discipline-specific tutorials.
Beyond teaching methods, the interdisciplinary approach in medical education has also gained significant attention. Studies suggest that collaboration among different disciplines can foster creative capacity and innovative thinking. Given the dominance of specialization in education, integrating interdisciplinary strategies into specialized training may contribute to the development of innovative solutions for medical challenges.8 Recent international studies have highlighted that learner-centered and interdisciplinary approaches—particularly PBL—can stimulate higher-order cognitive processes, including divergent thinking, adaptive reasoning, and collaborative creativity, which are increasingly required in modern healthcare environments.9
This study is necessary because creativity and innovation are critical skills for future physicians. The global shift toward innovation-driven healthcare has underscored the need for physicians and allied health professionals to develop creative problem-solving skills capable of addressing rapidly evolving clinical and technological challenges.1 Also, with the increasing complexity of medical issues and the growing need for innovative health solutions, strengthening these skills in medical students is essential. Multidisciplinary Problem-Based Learning (MPBL) offers a potentially effective educational strategy for this purpose.
The research question guiding this study was: Does participation in a three-session MPBL lead to measurable changes in self-reported creativity and innovation scores among undergraduate healthcare students from medicine, nursing, midwifery, surgical technology, and anesthesiology? According to previous literature on collaborative problem-solving effect in higher-order thinking skills, we hypothesized that MPBL would be associated with an increase in both creativity and innovation scores from pre-test to post-test, although given the exploratory nature of the study and the absence of a control group, we did not assume causality. Therefore, the present study aimed to explore the potential contribution of MPBL to creativity and innovation among medical sciences students, rather than to establish any causal effects.
Conceptual Framework
This study draws on two complementary theories. First, Torrance’s theory defines creativity through four components: fluency, flexibility, originality, and elaboration—which directly inform the TTCT instrument used here. Second, Amabile’s Componential Theory posits that creativity emerges from domain-relevant skills, creativity-relevant processes, and task motivation; innovation (implementation of creative ideas) additionally requires environmental support.
Multidisciplinary Problem-Based Learning (MPBL) is expected to enhance creativity and innovation by: (a) exposing students to diverse disciplinary perspectives (stimulating flexibility and originality), (b) using ill-structured clinical ethical dilemmas (activating creativity-relevant processes), and (c) fostering collaborative group discussions (enhancing task motivation).
Materials and Methods
Study Design and Participants
This pre-post interventional study was conducted in 2024 among medical sciences students from the disciplines of medicine, nursing, midwifery, operating room, and anesthesia at Hamadan University of Medical Sciences. The study’s conceptual framework was based on the principles of problem-based learning (PBL) and multidisciplinary education. The single-group pre-post design was chosen as an exploratory proof-of-concept study; therefore, no causal claims are made.
Data Collection Tools
The instruments used in this study were adapted from previously validated questionnaires. Creativity was measured using an abbreviated administration of the TTCT-Figural. The Figural form is shorter and more suitable for time-limited educational settings compared to the full TTCT. Short-form or selected-task administrations of TTCT-Figural have been used in prior pre–post educational studies.10 Consistent with these studies, we used a reduced set of TTCT-Figural tasks to capture divergent thinking within the practical constraints of the workshop. Although the Persian version of the TTCT has previously demonstrated acceptable reliability in Iranian samples,11 we additionally calculated reliability coefficients in our own sample to ensure appropriateness for this specific study population (see Results section). Furthermore, recent research supports the use of the Figural form of TTCT in educational and multicultural contexts due to its enhanced culture-fairness and suitability for non-verbal assessment.12
Scoring procedures for the TTCT-Figural were as follows:
- Fluency (number of relevant responses)
- Flexibility (number of various categories of responses)
- Originality (statistical rarity of responses)
- Elaboration (amount of details added to responses)
Score ranges for each subscale were: fluency (0–20), flexibility (0–15), originality (0–10), and elaboration (0–10), with a total creativity score ranging from 0 to 55. Internal consistency (Cronbach’s alpha) for the abbreviated TTCT-Figural within this sample is reported in the Results section, along with 95% confidence intervals.
Innovation was assessed using an adapted version of Baer and Frese’s innovation scale.13 Although the original scale was developed for organizational settings, individual-level items from this instrument have been used in academic contexts. To ensure suitability for student-level assessment, we selected only the individual-oriented items and adapted them through expert review. Nevertheless, we recognize that the instrument was not originally designed to detect short-term changes and interpret results accordingly. For the adapted innovation scale, the total score range was 5 to 25, with higher scores indicating greater self-reported innovation. Cronbach’s alpha for this adapted scale within our sample, along with 95% confidence intervals, is reported in the Results section.
Both the abbreviated TTCT-Figural and the adapted innovation measure were originally validated for cross-sectional or longer-term assessments. Their sensitivity to detect short-term changes following a brief intervention is not established. This limitation is central to the interpretation of the findings. Also, due to underestimation of creativity and innovation among healthcare professionals, specifically related versions of these measures have not been applied among healthcare students.
Satisfaction with the educational intervention was evaluated using a scale adapted from a validated medical education study by Seidi et al.14 All instruments were translated from English into Persian through a forward–backward translation process, and minor cultural adaptations were made to enhance contextual relevance.
Data Analysis
Data were analyzed using SPSS version 24. Descriptive statistics (mean, standard deviation, frequency) were used. The Kolmogorov–Smirnov or Shapiro–Wilk tests assessed normality. Paired t-tests were used for normally distributed data, and Wilcoxon tests for non-normal data. The significance level was set at p < 0.05.
Reliability analysis: Internal consistency reliability was assessed using Cronbach’s alpha coefficient for all instruments in our sample (N=70). For each alpha estimate, 95% confidence intervals (CIs) were calculated using the bootstrap method with 1000 resamples.
Effect size calculation: For paired comparisons, effect sizes were calculated using Cohen’s d for paired samples, defined as d = (M_post - M_pre)/SD difference, where M_post and M_pre are the post-test and pre-test means, and SD difference is the standard deviation of the difference scores. According to Cohen’s conventions, d = 0.2, 0.5, and 0.8 indicate small, medium, and large effects, respectively. For non-normally distributed data (based on Shapiro–Wilk test), the effect size r was calculated as r = Z/√N, where Z is the Wilcoxon signed-rank test statistic.
Confidence intervals for effect sizes: For each Cohen’s d estimate, 95% confidence intervals were calculated using the non-central t distribution method (Cumming & Finch, 2001). This approach provides more accurate confidence intervals for effect sizes in paired designs compared to normal approximation methods.
Results
The total number of participants was 70: 24 (34.3%) in medicine, 14 (20%) in nursing, 13 (18.6%) in midwifery, 12 (17.1%) in operating room, and 7 (10%) in anesthesia. The mean age was 21.83 ± 1.03 years (range: 20–24 years). Most participants were female (66.2%, n=51), with 19 males (27.1%).
Reliability of Instruments and Pre-Post Correlations
Internal consistency reliability was assessed using Cronbach’s alpha for all instruments in our sample (N=70). To address both pre-test and post-test reliability separately, alpha coefficients were calculated for each time point. Additionally, pre-post Pearson correlation coefficients were computed to examine the stability of individual differences across time. All confidence intervals (95% CI) were estimated using the bootstrap method with 1000 resamples. The results are presented in Table 1.
 |
Table 1 Reliability Estimates (Cronbach’s α) and Pre-Post Correlations |
These results indicate acceptable to good internal consistency at both time points. The moderate to strong positive pre-post correlations suggest that participants’ relative standing on creativity and innovation was moderately stable across the intervention period, while still allowing for individual variation in the magnitude of change.
Pre-Post Correlation of Measurements
To examine the stability of individual differences across time, Pearson correlation coefficients between pre-test and post-test scores were calculated:
- Creativity (TTCT): r = 0.68 (95% CI: 0.52–0.79), p < 0.001
- Innovation scale: r = 0.55 (95% CI: 0.36–0.70), p < 0.001
Discipline-specific comparisons of pre-test and post-test creativity and innovation scores are presented in Table 2. Due to the small and uneven sample sizes across disciplines (ranging from n=7 to n=24), subgroup comparisons should be interpreted with caution. In the anesthesia subgroup (n=7), all participants showed identical pre-post difference scores, resulting in a standard deviation of zero. This homogeneity may reflect a ceiling effect on the creativity measure, the very small sample size, or limited variability in this particular group. Therefore, effect sizes and confidence intervals could not be meaningfully calculated for this subgroup, and findings should be interpreted with extreme caution.
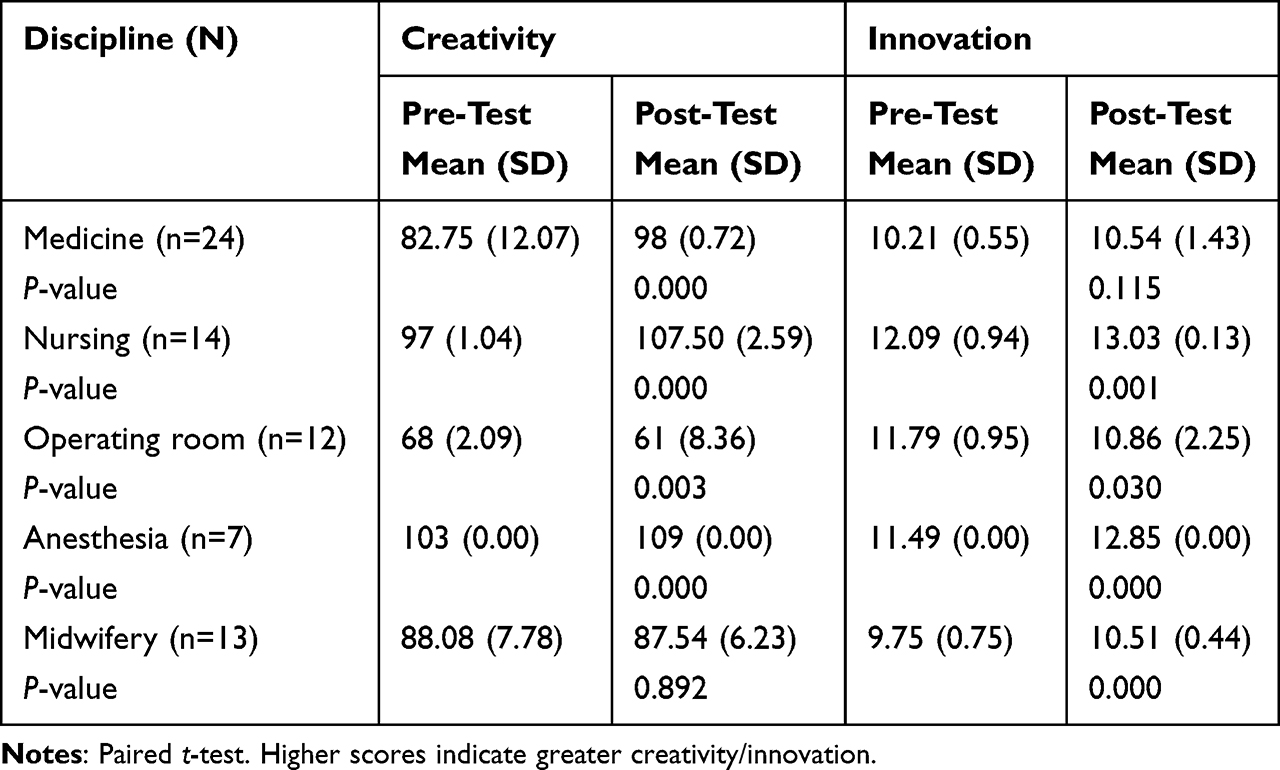 |
Table 2 Comparison of Pre-Test and Post-Test Creativity and Innovation Scores Between Disciplines |
The anesthesia subgroup consisted of only 7 participants, all of whom showed identical pre-post difference scores, resulting in a standard deviation of zero. This homogeneity may reflect a ceiling effect on the innovation measure, the very small sample size, or limited variability in this particular group. Therefore, effect sizes and confidence intervals could not be meaningfully calculated for this subgroup, and findings should be interpreted with extreme caution.
Effect Sizes and Practical Significance
To complement statistical significance testing and address practical significance, effect sizes were calculated using Cohen’s d for paired samples. According to Cohen’s conventions, d = 0.2 indicates a small effect, d = 0.5 a medium effect, and d = 0.8 a large effect. Table 3 presents effect sizes for overall and discipline-specific analyses.
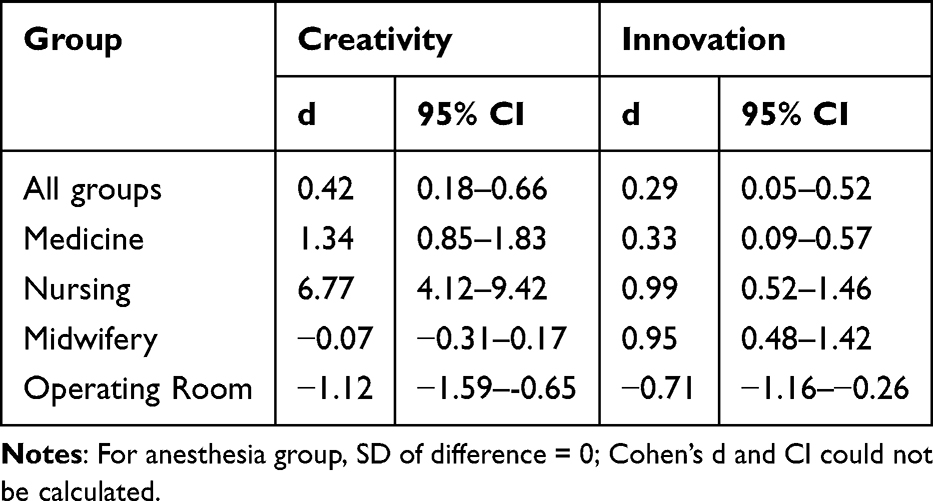 |
Table 3 Effect Sizes (Cohen’s d) with 95% Confidence Intervals for Creativity and Innovation |
Changes in Score Dispersion
To examine whether the intervention affected not only mean scores but also the variability of scores, we compared pre-test and post-test variances using Levene’s test for equality of variances.
For creativity, although the variance increased from pre-test (174.7) to post-test (280.3), this change was not statistically significant (F = 2.41, p = 0.12). This suggests that the MPBL intervention had a relatively consistent effect on creativity across participants.
For innovation, the variance increased significantly from 1.38 to 2.72 (F = 3.94, p = 0.049). This indicates that the intervention had a heterogeneous effect on innovation: some students improved substantially, while others showed little improvement or even decline. This finding complements the mean-based analysis and suggests that individual factors may moderate the effect of MPBL on innovation.
Coefficient of Variation (CV = SD/Mean) was also calculated to compare relative variability independent of scale:
- Creativity: pre-test CV = 0.15, post-test CV = 0.18
- Innovation: pre-test CV = 0.11, post-test CV = 0.15
As shown in Figure 1, the graphical results indicate an overall increase in creativity scores following the MPBL intervention. Although the variability of creativity scores increased from pre-test to post-test, the change in variance was not statistically significant (Levene’s test: p = 0.12). This pattern suggests that the intervention produced a relatively consistent effect across participants, with most students demonstrating a similar direction of change. The graphical representation complements the inferential analyses by illustrating both the upward shift in average creativity scores and the relatively stable distribution of responses.
 |
Figure 1 Mean creativity scores before and after the MPBL intervention (N = 70). Error bars represent ±1 standard deviation. |
As shown in Figure 2, the graphical results show an increase in innovation scores after the MPBL intervention. In contrast to creativity, innovation demonstrated a statistically significant increase in variability from pre-test to post-test (Levene’s test: p = 0.049). This finding suggests a heterogeneous intervention effect, whereby some students experienced substantial gains while others showed smaller improvements. The figure visually supports the variance analysis presented in Table 4 and highlights the differential responsiveness of participants to the MPBL experience.
 |
Table 4 Changes in Score Dispersion (Variability) from Pre-Test to Post-Test |
 |
Figure 2 Mean innovation scores before and after the MPBL intervention (N = 70). Error bars represent ±1 standard deviation. |
Discussion
This study aimed to evaluate the effectiveness of Multidisciplinary Problem-Based Learning (MPBL) in enhancing creativity and innovation among undergraduate students across various medical sciences disciplines. The observed pre-post improvements should be interpreted as short-term activation or immediate effects following a brief 12-hour intervention, rather than evidence of sustained developmental change in creativity or innovation.
The discipline-specific differences observed in creativity and innovation scores should be interpreted cautiously. Although the results varied across fields, the present study was not designed to determine the underlying causes of these differences. Several alternative explanations may account for the patterns observed, including imbalanced group composition, variability in facilitator interaction, baseline score differences, differential sensitivity of the instruments, or ceiling effects in certain groups. Therefore, the observed variation across disciplines reflects descriptive differences rather than evidence of discipline-related determinants.
Given that neither TTCT nor the innovation scale was designed for assessing rapid change, the interpretation of short-term differences in scores must remain cautious. The instruments may reflect activation or test familiarity rather than meaningful developmental change.
While the workshop scenarios centered on clinical ethical dilemmas, such dilemmas require participants to generate multiple possible courses of action, consider competing values, and evaluate the consequences of different choices — processes that align closely with divergent thinking and creative problem-solving. Prior studies have shown associations between moral decision-making and divergent thinking, and have argued that ethical context can enhance creativity (Li et al, 2023). Therefore, although our intervention focused on ethical reasoning, it likely engaged cognitive mechanisms shared with general creativity, which may explain observed changes in TTCT scores. Nonetheless, ethical reasoning is only one subtype of creativity; this partial overlap should be borne in mind when interpreting our findings.
As shown in the Results section, post-intervention analyses demonstrated improvements in creativity and innovation for most groups. These results are supported by prior research that underscores the benefits of multidisciplinary and problem-based learning in medical education.15–19
Several mechanisms may explain how MPBL influences creativity and innovation:
- First, exposure to variable disciplinary perspectives (eg, medicine, nursing, midwifery, surgical technology, and anesthesiology) may stimulate cognitive flexibility by requiring students to integrate different professional viewpoints.
- Second, collaborative problem-solving within small groups activates social learning processes, including peer feedback and shared knowledge construction, which can foster higher-order thinking skills.
- Third, the use of ill-structured clinical ethical dilemmas creates cognitive disequilibrium as real-life disequilibrium that they almost definitely will be facing in professions, prompting learners to generate multiple solutions and evaluate alternative courses of action—processes closely aligned with creative thinking.
- Last but not the least, active engagement and task motivation, central to Amabile’s componential theory, are enhanced by the learner-centered nature of MPBL.
These mechanisms likely operate in combination rather than in isolation.
Statistical vs practical significance: While p-values (< 0.05) indicate statistical significance, effect sizes better reflect educational relevance. Creativity showed a medium effect (d = 0.42), indicating modest practical improvement, while innovation showed a small effect (d = 0.29), suggesting limited practical impact. Statistical significance alone can be misleading, especially with moderate sample sizes (N=70).
Changes in dispersion (variability): Beyond changes in mean scores, we examined whether the MPBL intervention affected the dispersion (variability) of creativity and innovation scores. While creativity showed no significant change in variance (p = 0.12), innovation scores demonstrated a significant increase in variance from pre-test to post-test (p = 0.049). This finding suggests that the intervention had heterogeneous effects on innovation: it worked well for some students but not for others. This heterogeneity may be explained by baseline differences in innovation capacity, prior exposure to multidisciplinary learning, or individual motivational factors. Future research should identify student characteristics that predict differential response to MPBL.
Satisfaction ratings reflect participants’ perceptions of the workshop experience rather than actual learning effectiveness. Although overall satisfaction was moderate to high, such measures do not provide evidence of improved creativity or innovation. Moreover, the observed differences in satisfaction across disciplines were not examined, and the study did not collect data on factors such as perceived relevance, prior experience, or group dynamics that might explain these variations. It is important to emphasize that satisfaction reflects participants’ subjective perceptions of the workshop experience and does not constitute evidence of learning or educational effectiveness. High satisfaction does not validate that creativity or innovation improved; these are distinct constructs requiring separate measurement. Readers should avoid interpreting satisfaction as an indicator for learning outcomes.
Overall, the study provides preliminary evidence that MPBL may support creative and innovative thinking in health sciences students. However, methodological limitations—including short intervention duration, measurement constraints, lack of control group, and absence of process evaluation—necessitate cautious interpretation and highlight directions for future research.
Limitations
This study has several limitations that should be considered when interpreting the findings.
First, the pre–post design without a control group prevents causal inference; therefore, the observed changes may be influenced by factors other than the MPBL intervention, including maturation, exposure to concurrent educational experiences, novelty effects, testing effects, or other uncontrolled influences associated with repeated measurement.
Second, the 12-hour intervention duration across two weeks is relatively too brief for fostering stable or sustained changes in creativity and innovation, which typically develop over longer periods. Short-term effects may reflect temporary activation, motivation, or testing familiarity rather than sustained development. Results should be interpreted as short-term immediate effects only.
Third, subgroup analyses by discipline are potentially underpowered due to the small and uneven sample sizes across disciplines (ranging from n=7 to n=24). These analyses are presented as exploratory and should be interpreted with caution; they require confirmation in larger and more vast studies.
Fourth, both the abbreviated TTCT-Figural format and the adapted innovation measure were originally validated for cross-sectional or longer-term assessments. Their sensitivity to detect short-term changes following a brief intervention is not established. This limitation is central to the interpretation of the findings.
Conclusions
It is important to distinguish three levels of evidence provided by this study. First, regarding feasibility: MPBL was implementable within existing curriculum structures and was well-received by most participants (58.6% high satisfaction). Second, regarding short-term score changes: statistically significant increases in creativity and innovation were observed at the aggregate level immediately following the intervention. Third, regarding meaningful educational impact: due to the absence of a control group, short intervention duration, and measurement limitations, this study cannot provide evidence of sustained or educationally meaningful change. The observed effects should be interpreted as short-term activation rather than long-term developmental improvement.
This study provides preliminary evidence that MPBL may be associated with short-term improvements in creativity and innovation among medical sciences students. MPBL may therefore be considered as a promising approach for further exploration in undergraduate and postgraduate health sciences education. The results highlight the potential value of MPBL as an exploratory approach, but further research using larger samples, validated instruments, and longitudinal or controlled designs is required before firm conclusions or curricular recommendations can be drawn.
The observed variability across disciplines should be interpreted as descriptive and hypothesis-generating only. This study was not designed to explain why differences occurred, and no causal or explanatory claims regarding disciplinary mechanisms are made. These patterns may inform future research questions but should not be overinterpreted.
Notably, variability in outcomes across disciplines suggests the need for tailored approaches to optimize MPBL’s effectiveness for specific groups. High satisfaction levels among participants further reinforce the feasibility and acceptance of MPBL in diverse educational settings.
Data Sharing Statement
The datasets used and analyses during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki. Participants received complete information about the study objectives and methods and provided written informed consent. All personal data were kept confidential and used exclusively for research purposes. Participants were allowed to withdraw at any time without consequence. The study received approval from the Ethics Committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1402.222).
Consent for Publication
Not applicable, as this study does not involve any individual person’s data or image.
Acknowledgments
The authors thank Hamadan University of Medical Sciences for their financial and administrative support of this project (Grant No. 140208307389). We also appreciate the cooperation of the Education Development Center and all participating students.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Vice-Chancellor for Research and Technology, Hamadan University of Medical Sciences (Grant No. 140208307389). The Education Development Center of Hamadan University of Medical Sciences also provided administrative and logistic support.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–10. doi:10.1016/S0140-6736(10)61854-5
2. Amabile TM. Creativity in Context. Boulder (CO): Westview Press; 1996:336.
3. Torrance EP. Torrance Tests of Creative Thinking: Norms-Technical Manual. Bensenville (IL): Scholastic Testing Service; 1974:104.
4. Amabile TM, Pratt MG. The dynamic componential model of creativity and innovation in organizations: making progress, making meaning. Res Organ Behav. 2016;36:157–183.
5. Barrows HS. Problem-based learning in medicine and beyond: a brief overview. New Dir Teach Learn. 1996;68:3–12. doi:10.1002/tl.37219966804
6. Schmidt HG, Rotgans JI, Yew EHJ. The process of problem-based learning: what works and why. Med Educ. 2011;45(8):792–806. doi:10.1111/j.1365-2923.2011.04035.x
7. Dolmans DHJM, De Grave W, Wolfhagen IHAP, van der Vleuten CPM. Problem-based learning: future challenges for educational practice and research. Med Educ. 2005;39(7):732–741. doi:10.1111/j.1365-2929.2005.02205.x
8. Tang C, Werner A. Interdisciplinary education and creativity. Innov Educ Teach Int. 2017;54(3):245–253.
9. Jorm C, Roberts C, Lim R, et al. A large-scale interprofessional learning activity. J Interprof Care. 2016;30(5):654–657.
10. Kim KH. The Torrance Tests of Creative Thinking (TTCT). In: Sternberg RJ, Kaufman JC, editors. Handbook of Creativity Assessment. Cambridge (UK): Cambridge University Press; 2017:117–138.
11. Rezaei A, Hosseini M, Ghasemi N, et al. Reliability of Persian version of TTCT. J Psychol Stud. 2015;11(2):45–58.
12. Saeki N, Fan X, Van Dusen L. A comparative study of creative thinking of American and Japanese college students. J Creat Behav. 2001;35(1):24–36. doi:10.1002/j.2162-6057.2001.tb01219.x
13. Baer M, Frese M. Innovation in organizations. Annu Rev Organ Psychol Organ Behav. 2015;2:403–437.
14. Seidi M, Ramezani-Aliakbari F, Doosti-Irani A, et al. Effectiveness of the flipped classroom method using clinical scenarios and Educational Technology versus Subject-Based Lectures in a gastrointestinal physiology course for medical students. BMC Med Educ. 2024;24:858. doi:10.1186/s12909-024-05863-8
15. Salari M, Shokri A, Naderi F, et al. PBL strategies and higher-order cognitive skills. Med Teach. 2018;40(5):489–495.
16. Yelavarthi S. Creative thinking modules in medical education. Acad Med. 2022;97(3):412–418.
17. Liu F, Qu S, Fan Y, et al. Scientific creativity and innovation ability and its determinants among medical postgraduate students in Fujian province of China: a cross sectional study. BMC Med Educ. 2023;23(1):444. doi:10.1186/s12909-023-04408-9
18. Safin S, Zare M, Hosseini A, et al. Creativity-based learning in medical education. BMC Med Educ. 2024;24(1):89–97. doi:10.1186/s12909-024-05055-4
19. Foushee JA, Everhart KM, Stoner AM, Tjiattas-Saleski L, Redden D, et al. Student correlates with interprofessional attitudes within undergraduate medical education. BMC Med Educ. 2025;25(1):13. doi:10.1186/s12909-024-06480-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Integration of Case-Based Dialogue to Enhance Medical Students’ Understanding of Using Health Communication to Address Social Determinants of Health
King J, Taylor J
Advances in Medical Education and Practice 2023, 14:237-244
Published Date: 15 March 2023
Integrated Educational Technology in Teaching Anatomy Using the ASIC Framework: A Case Study from VinUniversity
Ha TM, Hoang D, Huynh CD, Le L
Advances in Medical Education and Practice 2023, 14:669-681
Published Date: 29 June 2023
Physician-Chef-Dietitian Partnerships for Evidence-Based Dietary Approaches to Tackling Chronic Disease: The Case for Culinary Medicine in Teaching Kitchens
Wood NI, Stone TA, Siler M, Goldstein M, Albin JL
Journal of Healthcare Leadership 2023, 15:129-137
Published Date: 24 July 2023
Enhancing Surgical Nursing Student Performance: Comparative Study of Simulation-Based Learning and Problem-Based Learning
Ma L, Yan R, Wang X, Gao X, Fan N, Liu L, Kang H
Journal of Multidisciplinary Healthcare 2024, 17:991-1005
Published Date: 7 March 2024