Back to Journals » Drug Design, Development and Therapy » Volume 20
Enhanced Recovery and Postoperative Analgesia After Laparoscopic Myomectomy: A Randomized Controlled Trial Comparing Total Intravenous Anesthesia, Transversus Abdominis Plane Block with Rectus Sheath Block, and Quadratus Lumborum Block
Authors Zeng C, Ling G, Huang C, Pan T, Tang Y, Kong F, Dai L, Xiao W, Liang Y, Gong Z
Received 6 May 2026
Accepted for publication 18 June 2026
Published 22 June 2026 Volume 2026:20 622304
DOI https://doi.org/10.2147/DDDT.S622304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Chunrong Zeng, Guoxu Ling, Caitao Huang, Tang Pan, Ying Tang, Fanli Kong, Luming Dai, Weiling Xiao, Yinsheng Liang, Zheng Gong
Department of Anesthesiology, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, People’s Republic of China
Correspondence: Zheng Gong, Department of Anesthesiology, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, People’s Republic of China, Email [email protected]
Objective: This study compares the effects of total intravenous anesthesia (TIVA, Group A), general anesthesia combined with transversus abdominis plane block and rectus sheath block (TAPB+RSB, Group B), and general anesthesia combined with quadratus lumborum block at the lateral supra-arcuate ligament (QLB-LSAL, Group C) on postoperative pain and recovery in patients undergoing laparoscopic myomectomy.
Methods: This was a prospective, single-center, randomized controlled trial involving 120 patients (1:1:1 randomization). The primary outcome was the visual analog scale (VAS) score for oxytocin-induced uterine contraction pain at 24 hours postoperatively (T16). Secondary outcomes included postoperative analgesic efficacy, intraoperative anesthetic consumption, hemodynamics, recovery indicators, and adverse reactions.
Results: Group C exhibited significantly lower oxytocin-induced contraction VAS scores than Groups B and A, with Group B also lower than A (all P< 0.05). Postoperatively, Group C had the lowest resting/exercise VAS scores, analgesic pump presses, and rescue analgesia needs within 48 hours (P< 0.05). Intraoperatively, Group C required the least propofol, remifentanil, and sufentanil, demonstrated superior hemodynamic stability, faster recovery/extubation, shorter PACU stays, better muscle strength, and higher QoR-15 scores (all P< 0.05). PONV incidence was lower in Group C than A (P< 0.05). No significant differences were found in patient demographics, operative/hospitalization time, or sleep quality, and no major block-related complications occurred.
Conclusion: General anesthesia combined with QLB-LSAL can effectively alleviate postoperative uterine contraction pain, reduce the need for anesthetic drugs during and after surgery, promote early recovery, and does not increase the risk of complications, making it an optimized anesthesia protocol for laparoscopic myomectomy.
Keywords: laparoscopic myomectomy, quadratus lumborum block, TAP block, rectus abdominis sheath block, multimodal analgesia, ERAS
Introduction
Uterine fibroids are the most common benign tumors in reproductive-aged women, with an incidence of approximately 20%–40%.1 Laparoscopic myomectomy has become the preferred surgical method due to its minimal invasiveness and rapid recovery.2 However, postoperative pain (resulting from incisions, pneumoperitoneum stimulation, and visceral pain)3 still severely affects the quality of recovery and increases the demand for opioids.4 Traditional opioid analgesia is accompanied by significant adverse reactions such as nausea, vomiting, and respiratory depression.5 In multimodal analgesic strategies, regional nerve block, as a key component, can effectively reduce opioid consumption and promote postoperative rehabilitation.6–8
Transversus abdominis plane block (TAPB) blocks the abdominal wall somatic nerves (T6–L1) and is effective for incisional pain.9,10 Rectus sheath block (RSB) blocks the anterior cutaneous branches of T7–T12, providing supplemental analgesia for midline incisions.9,10 Both have been widely used in abdominal surgery. Quadratus lumborum block (QLB) is believed to block both somatic and visceral pain through diffusion of local anesthetics into the paravertebral space and the thoracolumbar fascia.11 Among its approaches, the quadratus lumborum block at the lateral supra-arcuate ligament (QLB-LSAL) theoretically provides more extensive cephalad diffusion, potentially blocking the sympathetic trunks and visceral afferent fibers, which may be particularly beneficial for uterine contraction pain.12,13 Ultrasound-guided technology has further improved the accuracy and safety of the block.14
Despite these potential advantages, direct comparative studies of TAPB+RSB versus QLB-LSAL in laparoscopic myomectomy are insufficient, and their impact on the quality of postoperative recovery still requires high-level evidence.15–20 Moreover, acute postoperative pain, if poorly controlled, may transition to chronic pain; regional blocks may reduce this risk, an aspect rarely discussed in previous studies.
Therefore, this study aimed to compare the effects of three regimens (TIVA alone, general anesthesia combined with TAPB+RSB, and general anesthesia combined with QLB-LSAL) on perioperative analgesic efficacy, anesthetic consumption, postoperative recovery quality, and adverse reactions in patients undergoing laparoscopic myomectomy, to provide high-level clinical evidence for finding the optimal multimodal analgesic regimen.
Materials and Methods
Study Design and Ethics
This was a prospective, single-center, randomized controlled trial approved by the Ethics Committee of Guangxi Zhuang Autonomous Region People’s Hospital (approval number: KY-ZC-2024-008) and registered at ClinicalTrials.gov (registration number: ChiCTR2600118008). The study was conducted in accordance with the principles of the Declaration of Helsinki. All subjects signed written informed consent before participation.
Study Population
From September 2024 to June 2025, female patients scheduled for elective laparoscopic myomectomy were recruited. Inclusion criteria: aged 18–65 years, ASA physical status I–III, BMI 18–28 kg/m2. Exclusion criteria included: long-term use of analgesics/opioids, history of substance abuse, infection at the puncture site, coagulation disorders, allergy to study drugs, severe organ dysfunction, or inability to cooperate with assessments.
Randomization and Blinding
Using a computer-generated block randomization sequence (block size of 6), 120 patients were randomly divided into three groups in a 1:1:1 ratio (40 patients per group). The random allocation scheme was sealed in opaque envelopes. The operator performing the nerve block was aware of the grouping, but the researchers responsible for anesthesia management, data collection, postoperative follow-up, and statistical analysis were blinded to the grouping.
Anesthesia and Nerve Block Protocols
General Anesthesia Protocol
All patients received standardized general anesthesia. Induction: sequential intravenous injection of midazolam 0.04 mg/kg, etomidate 0.3 mg/kg, sufentanil 0.5 μg/kg, and rocuronium 0.8 mg/kg (Etomidate was chosen for induction for its hemodynamic stability, avoiding the hypotension often seen with propofol). Tracheal intubation was performed followed by mechanical ventilation. Maintenance: continuous intravenous infusion of propofol 4–12 mg/(kg·h) and remifentanil 0.1–0.4 μg/(kg·min), with intermittent intravenous boluses of sufentanil as needed during surgery to maintain hemodynamic fluctuations within 20% of the baseline value and BIS between 40–60.
Nerve Block Protocol
For Groups B and C, bilateral nerve blocks were performed by a senior anesthesiologist with more than 200 relevant block experiences under ultrasound guidance after general anesthesia induction and before surgical skin incision.
Group B (TAPB+RSB group): Inject 10 mL of 0.4% ropivacaine into the TAP plane and the posterior sheath of the rectus abdominis muscle on each side (a total of 20 mL on each side, with a total of 40 mL on both sides).
Group C (QLB-LSAL group): bilateral lumbar muscle block (QLB-LSAL) guided by ultrasound was performed in the lateral position. Inject 20 mL of 0.4% ropivacaine on each side (total amount of 40 mL on both sides).
Postoperative Analgesia
All patients received a uniform formula intravenous patient-controlled analgesia (PCA) pump postoperatively. Formula: sufentanil 2 μg/kg + dexmedetomidine 1.6 μg/kg + tropisetron 10 mg, diluted to 200 mL with normal saline. Settings: background infusion 4 mL/h, bolus dose 3 mL/time, lockout time 15 minutes. If the resting VAS score ≥4 points, PCA was used first; if ineffective after 5 minutes, 5 μg of sufentanil was intravenously injected in the post-anesthesia care unit (PACU), and 5 mg of dezocine was intravenously injected in the ward for rescue analgesia.
Outcome Measures
Time Points
Continuous observation time points were set as follows: T0 (before induction of anesthesia in the operating room), T1 (after intubation), T2 (5 minutes before skin incision), T3 (5 minutes after skin incision), T4 (30 minutes during surgery), T5 (end of surgery), T6 (awake), T7 (extubation), T8 (5 minutes after extubation), T9 (10 minutes after extubation), T10 (20 minutes after extubation), T11 (30 minutes after extubation), T12 (discharge from PACU to ward), T13 (2 hours postoperatively), T14 (6 hours postoperatively), T15 (12 hours postoperatively), T16 (24 hours postoperatively), T17 (48 hours postoperatively).
Outcome Indicators
Primary outcome: VAS score for uterine contraction pain at 24 hours postoperatively (T16). (Oxytocin was given as a 20 U intraoperative intravenous infusion, followed by a 24-hour postoperative maintenance infusion).
Secondary outcomes:
- Analgesic efficacy: Resting and movement (leg elevation 15° and abduction 30°) VAS scores at T8–T17; effective presses of PCA pump within 24 hours and 48 hours postoperatively; number of patients requiring rescue analgesia; cumulative dosage of rescue drugs (sufentanil, dezocine).
- Intraoperative and recovery conditions: Total intraoperative consumption of propofol, remifentanil, and sufentanil; mean arterial pressure and heart rate at T0–T11; time from the end of anesthesia to awakening (T0–T6), time from awakening to extubation (T6–T7), and PACU stay time; Ramsay sedation score (T6–T12), Lovett muscle strength score (T8–T17), QoR-15 score (postoperative day 1 and 2), AIS score (postoperative night 1 and 2); time of first PCA pump press, first ambulation time, first flatus time, and postoperative hospital stay.
- Safety: Occurrence of adverse reactions such as nausea, vomiting, dizziness, hypotension, and respiratory depression within 48 hours postoperatively; nerve block-related complications (eg., local anesthetic toxicity, hematoma, nerve injury).
Sample Size and Statistical Analysis
The sample size was calculated based on the intergroup difference in the primary outcome (VAS score for uterine contraction pain at 24 hours postoperatively). According to preliminary pilot studies, the expected means (standard deviations) of the three groups were: Group C 1.0 (0.5), Group B 2.0 (1.0), Group A 2.5 (1.0). Setting α=0.05 and power=90%, each group required at least 34 cases. Considering a 15% dropout rate, 40 cases were finally included in each group.
SPSS 26.0 software was used for analysis. Measurement data conforming to normal distribution were expressed as mean±standard deviation, and intergroup comparison was performed using one-way analysis of variance (ANOVA) or repeated measures analysis of variance; those not conforming to normal distribution were expressed as median (interquartile range) and analyzed using Kruskal–Wallis H-test. Count data were expressed as number (percentage), and χ2-test or Fisher’s exact test was used. All tests were two-tailed, and P<0.05 was considered statistically significant.
Results
123 female patients who underwent elective laparoscopic myomectomy were included in the eligibility assessment. During the experiment, one patient in Group A requested to withdraw from the study midway, and one patient in Group B was excluded from the study due to switching to open surgery during the operation; One case in Group C was excluded from the study due to unclear ultrasound imaging, and ultimately 120 patients completed the experiment and were included in the analysis (Figure 1).
 |
Figure 1 CONSORT flow diagram of the randomized controlled trial. |
Baseline Characteristics
There were no statistically significant differences in general data including age, body mass index (BMI), and American Society of Anesthesiologists (ASA) physical status classification, as well as the duration of nerve block operation, surgical duration, and anesthetic duration among the three groups (P>0.05), indicating a well-balanced baseline and good comparability (Table 1).
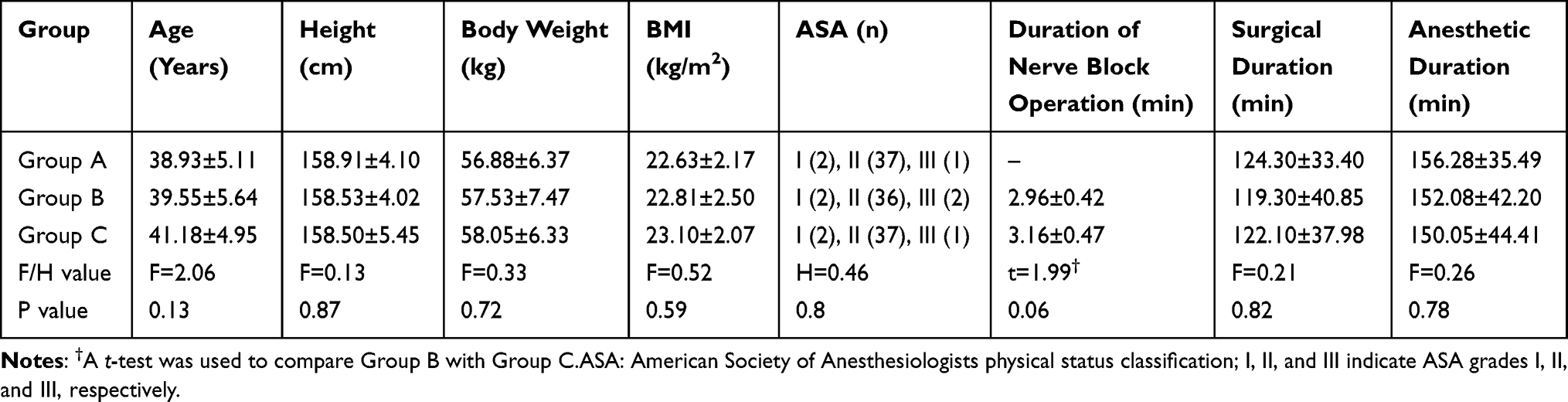 |
Table 1 Comparison of General Data Among the Three Groups ( |

Comparison of VAS Scores After Intravenous Oxytocin Infusion
The visual analog scale (VAS) scores of oxytocin-induced uterine contraction pain in Group C were significantly lower than those in Groups A and B at each time point from T9 to T16 postoperatively (P<0.05), and the scores in Group B were also lower than those in Group A (P<0.05) (Figure 2).
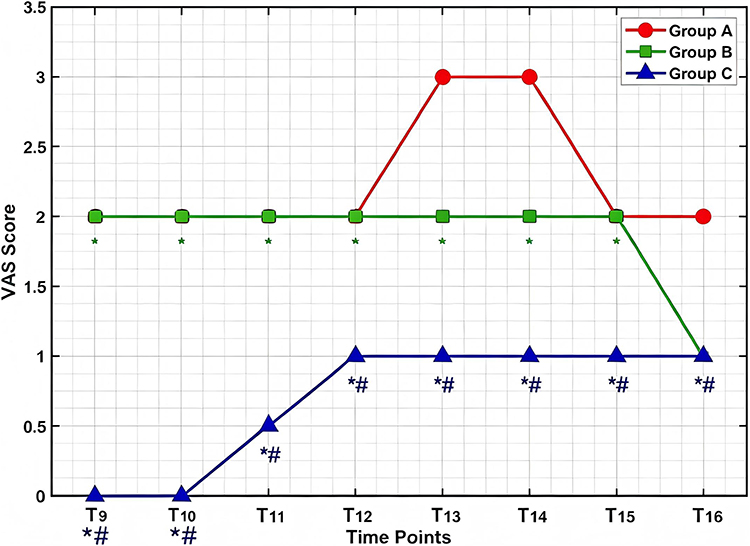 |
Figure 2 Comparison of VAS scores of uterine contraction pain after intravenous oxytocin infusion among the three groups. * Compared with Group A, P < 0.05; # Compared with Group B, P < 0.05. T9: 10 minutes after extubation; T10: 20 minutes after extubation; T11: 30 minutes after extubation; T12: discharge from PACU to ward; T13: 2 hours postoperatively; T14: 6 hours postoperatively; T15: 12 hours postoperatively; T16: 24 hours postoperatively. |
Comparison of Intraoperative Anesthetic Drug Consumption
There were statistically significant differences in the total consumption of intraoperative anesthetic drugs among the three groups (P<0.05). The intraoperative dosages of propofol (457.00±99.35 mg), remifentanil (0.88±0.21 mg) and sufentanil (31.13±4.23 μg) in Group C were significantly lower than those in Group A (propofol: 609.25±120.35 mg, remifentanil: 1.41±0.25 mg, sufentanil: 41.88±5.16 μg) and Group B (propofol: 549.25±138.37 mg, remifentanil: 1.19±0.29 mg, sufentanil: 37.00±4.96 μg). In addition, the intraoperative dosages of the above three anesthetic drugs in Group B were also significantly lower than those in Group A.
Comparison of Hemodynamic Indicators
There were no significant differences in mean arterial pressure (MAP) and heart rate (HR) among the three groups at T0, T1, T4, and T5. At T3 and T6–T11 with obvious stress responses, the fluctuations of MAP and HR in Group C and Group B were smaller than those in Group A (P<0.05), while there was no significant difference between Group C and Group B (Figures 3 and 4).
 |
Figure 3 Trend of MAP changes at each time point among the three groups. *Comparison between Group A and Groups B and C, P<0.05, whereas the comparison between Group B and Group C, P>0.05.T0: before induction of anesthesia; T1: after intubation; T2: 5 minutes before skin incision; T3: 5 minutes after skin incision; T4: 30 minutes during surgery; T5: end of surgery; T6: awake; T7: extubation; T8: 5 minutes after extubation; T9: 10 minutes after extubation; T10: 20 minutes after extubation; T11: 30 minutes after extubation. |
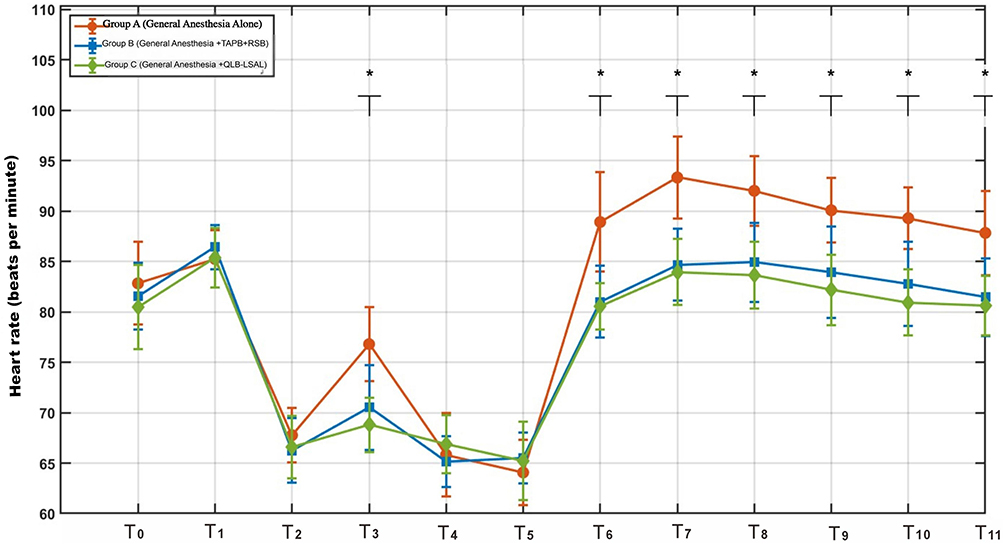 |
Figure 4 Trend of HR changes at each time point among the three groups. *Comparison between Group A and Groups B and C, P<0.05, whereas the comparison between Group B and Group C, P>0.05.T0: before induction of anesthesia; T1: after intubation; T2: 5 minutes before skin incision; T3: 5 minutes after skin incision; T4: 30 minutes during surgery; T5: end of surgery; T6: awake; T7: extubation; T8: 5 minutes after extubation; T9: 10 minutes after extubation; T10: 20 minutes after extubation; T11: 30 minutes after extubation. |
Comparison of Postoperative Pain and Analgesia-Related Indicators
From T8 to T17 postoperatively, the VAS scores at rest and during exercise in Group C were significantly lower than those in Groups A and B (P<0.05), and the scores in Group B were also lower than those in Group A (P<0.05). Specifically, the resting VAS score and exercise VAS score in Group C were 1.0 (1.0,1.0) and 3.0 (3.0,4.0) at 24 h postoperatively, and 1.0 (0.0,1.0) and 3.0 (2.0,3.0) at 48 h postoperatively, which were lower than those in Groups A and B at the corresponding time points. Moreover, the increase amplitude of VAS score during exercise in Group C was significantly smaller than that in the other two groups. The usage of postoperative patient-controlled analgesia (PCA) pump and rescue analgesia is shown in Table 2, with Group C showing the optimal outcomes in all related indicators. Specifically, at 24 h and 48 h postoperatively, the number of PCA pump presses in Group C was significantly lower than that in Groups A and B (P<0.05), and Group B also had fewer presses than Group A (P<0.05). The number of patients requiring rescue analgesia at 24 h and 48 h was significantly lower in Group C than in Groups A and B (P<0.05). No patient in Group C required sufentanil or dezocine for rescue analgesia, whereas the amounts of these rescue analgesics used in Groups A and B showed significant differences (P<0.05), with Group B requiring significantly less than Group A (P<0.05) (Table 2).
 |
Table 2 Comparison of Postoperative Analgesia-Related Indicators Among the Three Groups |
Comparison of Postoperative Recovery Indicators
Anesthesia Recovery-Related Indicators
The awakening time (25.08±7.16 min), extubation time (29.15±8.12 min) and post-anesthesia care unit (PACU) stay time (49.43±10.12 min) in Group C were significantly shorter than those in Group A (35.00±12.36 min, 38.05±13.35 min, 64.03±10.67 min) and Group B (32.88±9.26 min, 35.75±9.47 min, 58.45±12.23 min) (P<0.05), and there was no significant difference between Group A and Group B.
Muscle Strength and Sedation Scores
From T8 to T14, the Lovett muscle strength scores in Group C were significantly higher than those in Groups A and B (P<0.05), and this difference was particularly obvious from T8 to T12; the scores in Group B were also higher than those in Group A from T8 to T12 (P<0.05). Specifically, the Lovett muscle strength scores at T8 were 2.73±0.45 in Group A, 3.03±0.28 in Group B, and 3.28±0.45 in Group C; the scores at T10 were 2.93±0.35 in Group A, 3.10±0.30 in Group B, and 3.70±0.46 in Group C. The differences in scores among the three groups gradually narrowed from T15 onwards, and all reached 5.00±0.00 at T16 and T17 with no statistical significance.
From T6 to T12, the Ramsay sedation scores in Group C were significantly lower than those in Groups A and B (P<0.05), and the scores in Group B were also lower than those in Group A (P<0.05). The Ramsay sedation scores at T6 were 2.85±0.43 in Group A, 2.73±0.45 in Group B, and 2.45±0.38 in Group C; the scores at T12 were 2.70±0.46 in Group A, 2.58±0.45 in Group B, and 2.33±0.42 in Group C. This trend was consistent with the differences in intraoperative anesthetic drug consumption among the three groups.
Quality of Recovery and Rehabilitation Indicators
The scores of postoperative quality of recovery-15 (QoR-15) and Athens Insomnia Scale (AIS) among the three groups are shown in Table 3. On the 1st and 2nd days postoperatively, the QoR-15 scores in Group C were significantly higher than those in Groups A and B (P<0.05), and the scores in Group B were also higher than those in Group A (P<0.05); there were no significant differences in AIS scores among the three groups on the first two postoperative nights (Table 3).
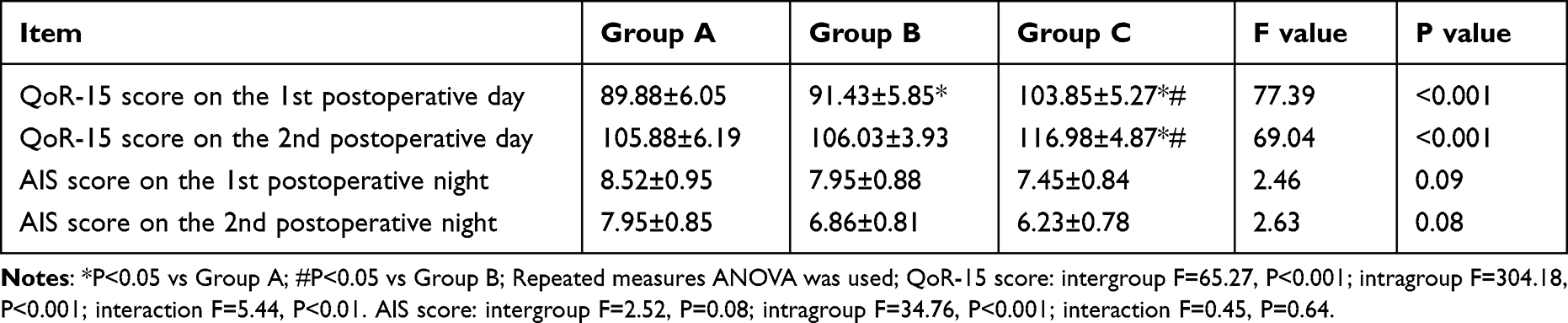 |
Table 3 Comparison of Postoperative Quality of Recovery and Sleep Quality Scores Among the Three Groups ( |

The first PCA pump press time in Group C (8.06±2.53 h) was significantly later than that in Group A (2.44±1.73 h) and Group B (3.38±2.44 h), and the duration of the first postoperative ambulation episode in Group C (4.15±0.73 min) was significantly longer than that in Group A (2.75±1.01 min) and Group B (3.45±0.85 min) (all P<0.05). There were no significant differences in the first flatus time (Group A: 34.91±7.69 h, Group B: 34.42±7.35 h, Group C: 32.06±8.42 h) and postoperative hospital stay (Group A: 107.46±17.68 h, Group B: 106.83±18.94 h, Group C: 103.55±14.90 h) among the three groups.
Comparison of Postoperative Adverse Reactions
The incidence of nausea and vomiting in Group A (45.0%, 18/40) was significantly higher than that in Group B (27.5%, 11/40) and Group C (12.5%, 5/40) (P<0.05), and the incidence in Group C was significantly lower than that in Group B (P<0.05). The incidence of dizziness was 10.0% (4/40) in Group A, 7.5% (3/40) in Group B and 2.5% (1/40) in Group C, with no significant difference among the three groups.
No adverse reactions such as somnolence, hypotension, urinary retention, pruritus, delirium, or respiratory depression were observed in all patients. No complications related to nerve block such as local anesthetic toxicity, hematoma, or nerve injury occurred in Groups B and C after the nerve block operation.
Discussion
This study confirmed that in patients undergoing laparoscopic myomectomy, general anesthesia combined with quadratus lumborum block at the lateral supra-arcuate ligament (QLB-LSAL) is significantly superior to TIVA alone or general anesthesia combined with TAPB+RSB in controlling postoperative visceral pain and promoting early recovery. The core advantage lies in the potent inhibition of oxytocin-induced uterine contraction pain by QLB-LSAL (from 10 minutes after extubation to 24 hours postoperatively). We hypothesize that QLB-LSAL achieves specific blocking of visceral nociceptive stimulation by blocking the thoracolumbar sympathetic trunks or visceral afferent fibers.21,22 In contrast, TAPB+RSB mainly acts on the abdominal wall somatic nerves and has limited effect on visceral pain,23,24 explaining why Group B was inferior to Group C for contraction pain.
Excellent visceral analgesia brought comprehensive perioperative benefits to the QLB-LSAL group. The preemptive analgesic effect significantly reduced intraoperative propofol and opioid requirements,21,25 leading to more stable hemodynamics and faster awakening and extubation.26 Continuous adequate postoperative analgesia translated into the lowest PCA pump usage, rescue analgesia needs, and opioid consumption, thereby reducing opioid-related adverse events. Consequently, patients in the QLB-LSAL group achieved better early lower limb muscle strength recovery,27,28 higher QoR-15 scores, and earlier first ambulation,29,30 underscoring its key role in accelerated rehabilitation.
Regarding safety, the significant reduction in opioid dosage in Group C resulted in a markedly lower incidence of postoperative nausea and vomiting compared to Group A.31,32 No complications were attributed to any ultrasound-guided nerve block, consistent with the high safety profile of ultrasound-guided regional blocks reported in the literature.33,34 Although the QLB-LSAL group showed advantages in many recovery indicators, hospital stay did not differ significantly among groups, suggesting that discharge decisions may be influenced by non-pain factors (eg., institutional protocols, social reasons).
Limitations
Several limitations should be acknowledged. First, sensory blockade could not be assessed immediately after the block because the procedure was performed under general anesthesia. Nonetheless, all blocks were performed by experienced anesthesiologists (>200 prior procedures) under ultrasound guidance, and no clinical signs of block failure (eg., hemodynamic responses to skin incision or excessive incisional pain) were observed. Thus, the actual failure rate is likely negligible. Future studies could perform blocks before anesthesia induction or assess sensory levels after emergence. Second, the 48-hour follow-up is too short to evaluate long-term analgesic effects or acute-to-chronic pain transition. Third, the sample size, while adequate for the primary outcome, is underpowered to detect rare complications. Fourth, we did not perform subgroup analyses based on ropivacaine dosage. Further research should optimize local anesthetic protocols, extend follow-up, and assess chronic pain outcomes.
Risk-Benefit Consideration
The use of QLB-LSAL involves injection of a relatively large volume of local anesthetic (40 mL of 0.4% ropivacaine), which carries a potential risk of local anesthetic systemic toxicity (LAST). In our study, no signs of LAST were observed, likely due to ultrasound guidance, slow intermittent injection, and the use of ropivacaine, which has a lower cardiac toxicity profile. The benefits – reduced opioid consumption, better pain control, earlier mobilization – outweighed these theoretical risks in our patient population. However, clinicians should remain vigilant.
Conclusion
In conclusion, general anesthesia combined with QLB-LSAL provides specific analgesia for visceral pain in patients undergoing laparoscopic myomectomy. By reducing perioperative anesthetic requirements, it may promote early functional recovery and improve the quality of recovery without increasing surgical risks. These findings suggest that this regimen is a viable anesthetic option for laparoscopic myomectomy.
Data Sharing Statement
The data of observational studies cannot be made publicly available because of ethical and legal considerations. It may be provided upon reasonable request to corresponding author Dr. Zheng Gong.
Author Contributions
Chunrong Zeng, Guoxu Ling, Caitao Huang, and Tang Pan are co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is funded by the Key Project of Guangxi Natural Science Foundation (No. 2024GXNSFDA010058), the General Project of Guangxi Natural Science Foundation (No. 2023GXNSFAA026324), the Exploration Plan of Wuhan Natural Science Foundation (No.2025020701020277), the Research Special Fund of Wu Jieping Medical Foundation (No.320.6750.2024-15-68), the New Rui Research Comfort Medicine Special Fund of Hubei Chen Xiaoping Science and Technology Development Foundation (No.CXPJJH124001-38), and a self-funded research project of Guangxi Zhuang Autonomous Region Health Commission (No. Z-A20240097).
Disclosure
All authors declare no potential conflicts of interest.
References
1. Ahmad A, Kumar M, Bhoi NR, et al. Diagnosis and management of uterine fibroids: current trends and future strategies. J Basic Clin Physiol Pharmacol. 2023;34(3):291–11. doi:10.1515/jbcpp-2022-0219
2. Krishnan M, Narice B, Cheong YC, et al. Surgery and minimally invasive treatments for uterine fibroids. Cochrane Database Syst Rev. 2024;6(6):CD015650. doi:10.1002/14651858.CD015650
3. Song T, Kim TJ, Lee SH, Kim TH, Kim WY. Laparoendoscopic single-site myomectomy compared with conventional laparoscopic myomectomy: a multicenter, randomized, controlled trial. Fertil Steril. 2015;104(5):1325–1331. doi:10.1016/j.fertnstert.2015.07.1137
4. Kwack JY, Ahn KH, Kwon YS. Postoperative pain control with ropivacaine following laparoscopic myomectomy: a randomized double-blind, pilot study. J Obstet Gynaecol Res. 2019;45(4):871–876. doi:10.1111/jog.13910
5. Munro A, Sjaus A, George RB. Anesthesia and analgesia for gynecological surgery. Curr Opin Anaesthesiol. 2018;31(3):274–279. doi:10.1097/ACO.0000000000000584
6. Yin H, Tong X, Huang H. Dural puncture epidural versus conventional epidural analgesia for labor: a systematic review and meta-analysis of randomized controlled studies. J Anesth. 2022;36(3):413–427. doi:10.1007/s00540-022-03061-8
7. Delgado A, Katz L, Melo RS, Amorim M, Lemos A. Effectiveness of the peanut ball use for women with epidural analgesia in labour: a systematic review and meta-analysis. J Obstet Gynaecol. 2022;42(5):726–733. doi:10.1080/01443615.2021.1997959
8. Anim-Somuah M, Smyth RM, Cyna AM, Cuthbert A. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database Syst Rev. 2018;5(5):CD000331. doi:10.1002/14651858.CD000331.pub4
9. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in Enhanced Recovery After Surgery (ERAS) guidelines. Anesthesiol Clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
10. Gan TJ, Habib AS, Miller TE, White W, Apfelbaum JL. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin. 2014;30(1):149–160. doi:10.1185/03007995.2013.860019
11. Ma K, Bebawy JF, Hemmer LB. Multimodal Analgesia and Intraoperative Neuromonitoring. J Neurosurg Anesthesiol. 2023;35(2):172–176. doi:10.1097/ANA.0000000000000904
12. Fiore JF, El-Kefraoui C, Chay MA, et al. Opioid versus opioid-free analgesia after surgical discharge: a systematic review and meta-analysis of randomised trials. Lancet. 2022;399(10343):2280–2293. doi:10.1016/S0140-6736(22)00582-7
13. Prabhakar A, Mancuso KF, Owen CP, et al. Perioperative analgesia outcomes and strategies. Best Pract Res Clin Anaesthesiol. 2014;28(2):105–115. doi:10.1016/j.bpa.2014.04.005
14. Schricker T, Lattermann R. Perioperative catabolism. Can J Anaesth. 2015;62(2):182–193. doi:10.1007/s12630-014-0274-y
15. Van der Meulen JF, Fisch C, Dreessen JRJ, Coppus SFPJ, Kok HS, Bongers MY. Procedural sedation and analgesia with propofol (PSA) for gynecologic surgery: a systematic review of the literature. Eur J Obstet Gynecol Reprod Biol. 2023;287:137–146. doi:10.1016/j.ejogrb.2023.05.035
16. Bos EME, Hollmann MW, Lirk P. Safety and efficacy of epidural analgesia. Curr Opin Anaesthesiol. 2017;30(6):736–742. doi:10.1097/ACO.0000000000000516
17. Vicari JJ. Sedation and analgesia. Gastrointest Endosc Clin N Am. 2002;12(2):297–311. doi:10.1016/S1052-5157(01)00006-8
18. Bongiovanni T, Lancaster E, Ledesma Y, et al. Systematic review and meta-analysis of the association between non-steroidal anti-inflammatory drugs and operative bleeding in the perioperative period. J Am Coll Surg. 2021;232(5):765–790. doi:10.1016/j.jamcollsurg.2021.01.012
19. Wang J, Chu T, Sun R, et al. Analgesic efficacy of quadratus lumborum block in patients undergoing nephrectomy: a systematic review and meta-analysis. Pain Med. 2023;24(5):476–487. doi:10.1093/pm/pnac185
20. Kim S, Kim H, Kim N, et al. Effectiveness of quadratus lumborum block for postoperative pain: a systematic review and meta-analysis. Minerva Anestesiol. 2020;86(5):554–564. doi:10.23736/S0375-9393.20.14112-2
21. Chin KJ, McDonnell JG, Carvalho B, et al. Essentials of our current understanding: abdominal wall blocks. Reg Anesth Pain Med. 2017;42(2):133–183. doi:10.1097/AAP.0000000000000545
22. Balocco AL, López AM, Kesteloot C, et al. Quadratus lumborum block: an imaging study of three approaches. Reg Anesth Pain Med. 2021;46(1):35–40. doi:10.1136/rapm-2020-101647
23. Canikli Adıgüzel E, Akyurt D, Bahadır Altun H, et al. Posterior quadratus lumborum block or thoracolumbar interfascial plane block and postoperative analgesia after spinal surgery: a randomized controlled trial. J Clin Med. 2023;12(23):7312. doi:10.3390/jcm12237312
24. Farag E, Seif J, Kolli S. Quadratus lumborum block versus transversus abdominal plane block – the debate is still going on. J Clin Anesth. 2020;66:109969. doi:10.1016/j.jclinane.2020.109969
25. Takeda Y, Tsujimoto K, Okamoto T, et al. Efficacy of anterior quadratus lumborum block and pain after total Hip arthroplasty: a randomized controlled trial. J Arthroplasty. 2023;38(11):2386–2392. doi:10.1016/j.arth.2023.05.031
26. Mostafa M, Mousa MS, Hasanin A, et al. Erector spinae plane block versus subcostal transversus abdominis plane block in patients undergoing open liver resection surgery: a randomized controlled trial. Anaesth Crit Care Pain Med. 2023;42(1):101161. doi:10.1016/j.accpm.2022.101161
27. Elsayed Elashry H, Abdelbadie M, Ali Elshabacy A, et al. Analgesic effect of quadratus lumborum block type III and type II versus lateral transversus abdominis plane block in cesarean section: a randomized controlled multicenter trial. Anesth Pain Med. 2024;14(1):e140464. doi:10.5812/aapm-140464
28. Aoyama Y, Sakura S, Abe S, et al. Analgesic effects and distribution of cutaneous sensory blockade of quadratus lumborum block type 2 and posterior transversus abdominis plane block: an observational comparative study. Korean J Anesthesiol. 2020;73(4):326–333. doi:10.4097/kja.20094
29. Li J, Dai F, Ona Ayala KE, et al. Transmuscular quadratus lumborum and lateral femoral cutaneous nerve block in total Hip arthroplasty. Clin J Pain. 2021;37(5):366–371. doi:10.1097/AJP.0000000000000925
30. Tran DQ, Bravo D, Leurcharusmee P, et al. Transversus abdominis plane block: a narrative review. Anesthesiology. 2019;131(5):1166–1190. doi:10.1097/ALN.0000000000002828
31. Huang Q, Wang F, Liang C, et al. Fosaprepitant for postoperative nausea and vomiting in patients undergoing laparoscopic gastrointestinal surgery: a randomised trial. Br J Anaesth. 2023;131(4):673–681. doi:10.1016/j.bja.2023.06.058
32. Hansen CK, Steingrimsdottir GE, Dam M, et al. Anterior quadratus lumborum catheters for elective cesarean section: a double-blind, randomized, placebo-controlled trial. Acta Anaesthesiol Scand. 2024;68(2):254–262. doi:10.1111/aas.14348
33. Lee PS, Brunette LL, Sriprasert I, et al. Benefits of the Enhanced Recovery After Surgery (ERAS) pathway with quadratus lumborum blocks for minimally invasive gynecologic surgery patients: a retrospective cohort study. Cureus. 2023;15(11):e49183. doi:10.7759/cureus.49183
34. Zhu R, Xiang S, Chen D. Combined lumbar muscle block and perioperative comprehensive patient-controlled intravenous analgesia with butorphanol in gynecological endoscopic surgery. World J Clin Cases. 2021;9(34):10540–10548. doi:10.12998/wjcc.v9.i34.10540
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Erector Spinae Plane Block for Perioperative Pain Management in Lumbar Spinal Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Fu MY, Hao J, Ye LH, Jiang W, Lv YW, Shen JL, Fu T
Journal of Pain Research 2023, 16:1453-1475
Published Date: 3 May 2023
Comparison of Quadratus Lumborum Plus Modified Erector Spinae Plane Block versus Pericapsular Nerve Group Block Plus Lateral Femoral Cutaneous Block on Postoperative Analgesia and Functional Recovery in Total Hip Arthroplasty: A Retrospective Propensity Score-Matched Study
Wu X, Wang M, Du M, Wang Y, Chen X, Zhang D, Xu Y
Journal of Pain Research 2026, 19:567827
Published Date: 13 January 2026
The Effect of Cocktail Formula Solution for Erector Spinae Plane Block on Postoperative Pain After Laparoscopic Major Upper Abdominal Surgery: A Single-Center Randomized Controlled Study
Lu D, Chen H, Hu J, He X, Bao L, Xu B, Zhang S, Fan J, Wang R
Journal of Pain Research 2026, 19:566625
Published Date: 24 January 2026
Effect of Intrathecal Hydromorphone on the Duration and Efficacy of Postoperative Analgesia in Patients Undergoing Benign Anorectal Surgery: Protocol for a Randomized, Double-Blind, Controlled Trial
Cao Y, Zhou Y, Zhou D, Xiong C, Fu L, Chen X, Zhang X
Journal of Pain Research 2026, 19:569284
Published Date: 26 February 2026
Modified Single-Side-Lying Quadratus Lumborum Block Combined with Liposomal Bupivacaine versus Transversus Abdominis Plane Block for Post-Cesarean Analgesia: A Randomized Controlled Trial
Rao J, Xiao J, Li B, Zong Y, Song J, Hu S, Luo A, Zeng L, Zhou Q
Drug Design, Development and Therapy 2026, 20:580472
Published Date: 8 June 2026