Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Endocrine Therapy versus Chemotherapy After CDK4/6 Inhibitor Progression in HR+/HER2- Metastatic Breast Cancer: A Multicenter Real-World Study from Turkey
Authors Cangür C ![]() , Bülbül B
, Bülbül B ![]() , Yeğen IT, Ucun B
, Yeğen IT, Ucun B ![]() , Eren Oö, Başaran H, Erdoğan AP, Şahin Hafızoğlu E, Gökmen E, Özkan O, Araz M
, Eren Oö, Başaran H, Erdoğan AP, Şahin Hafızoğlu E, Gökmen E, Özkan O, Araz M ![]() , Oruç A, Yilmaz C, Gül G
, Oruç A, Yilmaz C, Gül G ![]() , Yildirim S
, Yildirim S
Received 30 September 2025
Accepted for publication 9 January 2026
Published 14 January 2026 Volume 2026:18 571246
DOI https://doi.org/10.2147/BCTT.S571246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Robert Clarke
Can Cangür,1 Büşra Bülbül,1 Irem Turgut Yeğen,1 Bekir Ucun,1 Orhan önder Eren,1 Hamit Başaran,2 Atike Pınar Erdoğan,3 Ece Şahin Hafızoğlu,3 Erhan Gökmen,4 Oğuzcan Özkan,4 Murat Araz,5 Ahmet Oruç,5 Cengiz Yilmaz,6 Gürkan Gül,6 Serkan Yildirim1
1Department of Medical Oncology, Selcuk University, Konya, Turkey; 2Department of Radiation Oncology, Selcuk University, Konya, Turkey; 3Department of Medical Oncology, Celal Bayar University, Manisa, Turkey; 4Department of Medical Oncology, Ege University, İzmir, Turkey; 5Department of Medical Oncology, Necmettin Erbakan University, Konya, Turkey; 6Department of Medical Oncology, Izmir City Hospital, İzmir, Turkey
Correspondence: Can Cangür, Department of Medical Oncology, Selcuk University, Konya, Turkey, Tel +90 535 3469301, Email [email protected]
Background: HR (hormone receptor)-positive, HER2 (Human Epidermal Growth Factor Receptor 2)-negative metastatic breast cancer represents the majority of advanced breast cancer cases. Although CDK4/6 (cyclin-dependent kinase) inhibitors combined with endocrine therapy have become the standard first-line approach, the optimal treatment strategy after disease progression remains unclear.
Methods: We conducted a multicenter retrospective study of 218 patients treated across five tertiary oncology centers in Turkey who progressed on CDK4/6 inhibitors and subsequently received either endocrine therapy (ET) or chemotherapy (CT).
Results: Endocrine therapy, administered in 65 patients—most commonly with everolimus-based combinations—was associated with a significantly longer overall survival (OS) compared with CT (18.0 vs 10.0 months, p = 0.011). While progression-free survival (PFS) showed a numerical advantage for ET (6.0 vs 4.9 months), the difference did not reach statistical significance. Multivariate analysis confirmed both treatment type and de novo metastatic presentation as independent predictors of survival.
Conclusion: These findings demonstrate that, in real-world clinical practice, continued endocrine therapy beyond CDK4/6 inhibitors progression yields superior survival compared to chemotherapy, particularly in patients with de novo metastatic disease. Our results support the prioritization of endocrine-based approaches over chemotherapy in this setting and underscore the urgent need for prospective trials to refine treatment sequencing strategies for this large patient population.
Plain Language Summary: Hormone receptor-positive, HER2-negative metastatic breast cancer is the most common subtype of advanced breast cancer, yet the best treatment strategy after progression on CDK4/6 inhibitors remains uncertain. Many patients are switched directly to chemotherapy, which is often associated with limited benefit and significant toxicity. In this large multicenter study from Turkey, we compared endocrine therapy with chemotherapy in women whose disease progressed after CDK4/6 inhibitors. We found that patients who continued endocrine therapy, particularly with mTOR-based combinations, lived significantly longer than those who received chemotherapy. Importantly, patients who presented with de novo metastatic disease also had better survival. These findings highlight that chemotherapy may not always be the best option after CDK4/6 inhibitor failure and support the continued use of endocrine-based strategies. Our results provide real-world evidence that could influence clinical decision-making and guide the design of future prospective trials.
Keywords: metastatic breast cancer, CDK4/6 inhibitor, endocrine therapy, chemotherapy, overall survival
Introduction
Breast cancer is the most common malignancy among women worldwide, accounting for 31% of all female cancer cases. In advanced stages, when the tumour metastasises to other organs such as the lungs, brain and bones, it poses a serious threat to patients’ lives.1–3 Approximately 70% of metastatic breast cancers express hormone receptors (oestrogen or progesterone receptor positive; HR) and do not express human epidermal growth factor receptor 2 (HER2).4 In the treatment of advanced HR-positive, HER2-negative breast cancer, endocrine-based therapies (ET) are recommended in the absence of visceral crisis.5,6 Since the approval of tamoxifen in the 1970s, an increasing number of patients have benefited from ET.7 The prognosis of patients with HR-positive advanced breast cancer has significantly improved with endocrine therapy (ET).8 With the approval of aromatase inhibitors (AIs; eg exemestane) and selective estrogen receptor downregulator (SERDs; eg fulvestrant and elacestrant), there are now additional ET options available for HR-positive breast cancer.9–12 However, most patients eventually develop resistance to ET.13–16
In randomised clinical trials of cyclin-dependent kinase 4/6 inhibitors (CDKi) used in combination with ET, CDKi have demonstrated a significant contribution to progression-free survival (PFS).17,18 Based on these results, the combination of CDKi and ET is the standard of care (SOC) for first- and second-line treatment in patients with HR-positive, HER2-negative advanced breast cancer.19 In randomised clinical trials of CDKI used in combination with ET, CDKI have been shown to significantly contribute to PFS.17,18 Based on these results, the combination of CDKi and ET is considered the standard of care (SOC) for first- and subsequent-line treatments in patients with HR-positive, HER2-negative advanced breast cancer.19
Following progression with combination therapy, there is no gold standard treatment option for the next systemic treatment step.20–22 Reasonable options include switching to another ET monotherapy, cytotoxic CT, everolimus with ET,23–25 olaparib26 or talazoparib27 for patients with germline BRCA mutations, alpelisib28 for patients with somatic PIK3CA mutations and capivasertib29 AKT pathway inhibitor. Additionally, in subsequent lines of therapy, antibody–drug conjugates such as trastuzumab deruxtecan30 may be used in patients with HER2 low metastatic breast cancer, whereas sacituzumab govitecan31 is an approved option for patients with HR–positive, HER2-negative metastatic breast cancer.
In this study, we aimed to determine the efficacy of subsequent systemic therapies in patients who progressed on CDKi therapy, to assess whether there were differences in overall survival (OS) and PFS between hormonal therapies (monotherapy vs mTOR-based) and CT, and to identify potential clinical and pathological factors associated with survival outcomes in these patients.
Materials and Methods
Study Design and Population
Our study is a multicentre, retrospective study conducted by the medical oncology clinics of Selçuk University Faculty of Medicine Hospital, İzmir City Hospital, Ege University Faculty of Medicine Hospital, Manisa Celal Bayar University Faculty of Medicine Hospital, and Necmettin Erbakan University Faculty of Medicine Hospital. The files of patients who applied to the relevant medical oncology outpatient clinics between 1 January 2019 and 1 May 2025 were reviewed and included in the study.
In our study, patients were categorized based on their metastatic status (de novo or systemic recurrence), metastatic sites (visceral, bone-only, or lymph node-only metastases), menopausal status (pre/perimenopausal or postmenopausal), and prior treatment with CT (CT or ET) before CDKi use. The effects of these parameters on survival were determined using univariate analysis, followed by multivariate analysis to examine their impact on survival.
The pathology reports of the patients included in the study were reviewed to determine their HER2 status. Patients with immunohistochemical Cerb2 levels of negative and + 1, as well as those with + 2 levels and a negative FISH test, were classified as HER2 negative.
Although categorization of endocrine resistance (primary vs secondary) was considered, the retrospective multicenter design limited the consistent availability of precise timelines required for this classification (eg, exact dates of progression on prior endocrine therapies). Therefore, this analysis was not performed.
Inclusion and Exclusion Criteria
Patients were eligible for inclusion if they had a diagnosis of metastatic breast cancer with hormone receptor–positive and HER2-negative disease, confirmed by a documented pathology report obtained either at the time of de novo metastatic presentation or from prior early-stage surgical specimens. All included patients had experienced disease progression following treatment with a CDK4/6 inhibitor and subsequently received at least one line of systemic therapy, either endocrine therapy or chemotherapy, in the metastatic setting.
Patients were excluded if they had hormone receptor–negative or HER2-positive breast cancer, non-metastatic disease, or had not received prior treatment with a CDK4/6 inhibitor. Patients who did not receive any subsequent systemic therapy following progression on CDK4/6 inhibitor–based treatment were also excluded. In addition, patients with incomplete clinical or pathological data that precluded reliable outcome assessment were not included in the analysis. Male patients were excluded to reduce biological and treatment-related heterogeneity.
Treatment
Patients included in the study progressed while receiving CDKi therapy in combination with ET and were divided into two treatment groups: the first group consisted of patients receiving CT, and the second group consisted of patients receiving ET alone or in combination.
Study Objectives
The primary endpoint of our study was the OS benefit of ET or CT initiated in patients who progressed under CDKi therapy, while PFS was defined as the secondary endpoint. OS was defined as the time from the start of treatment initiated after CDKi to death or follow-up end (confirmed last activity), while PFS was defined as the time from the start of treatment initiated after CDKi to progression (or death).
Ethical Considerations
Our study was conducted in accordance with the Helsinki Declaration and was reviewed and approved by the Ethics Committee of Selçuk University Faculty of Medicine (20/2025, dated 14 January 2025). Patient consent was waived due to the retrospective nature of the study. All patient data were anonymized, and confidentiality was strictly maintained in accordance with institutional and ethical guidelines.
Statistical Analysis
A formal sample size calculation was not performed for this study, as it was designed as a retrospective cohort analysis aiming to include all eligible patients treated at the participating centers during the specified study period to maximize the descriptive power and reflect real-world clinical practice in Turkey. All analyses were performed using the SPSS version 20.0 statistical software package for Windows. Continuous variables are presented as median (range), and categorical variables as numbers (percentages). The chi-square test was used to analyse differences in clinical characteristics between the two groups. Overall and progression-free survival were calculated using the Log rank test. We then used the Kaplan-Meier method to plot survival curves and the Cox proportional hazards regression model to identify statistically significant variables associated with overall survival. Differences were considered statistically significant when p < 0.05.
Results
A total of 218 patients were included in our study. Among the 65 (29.8%) patients who progressed during CDKi therapy with ET, 153 (70.2%) patients received CT-based therapy. The median age at diagnosis was 54.0 years (range, 26–89). In the CT group, the median age was 54.0 years (range, 26–88), while in the ET group, it was 55.0 years (range, 30–89). Among the study participants, 137 (62.8%) were postmenopausal and 81 (37.2%) were premenopausal at the start of ET plus CDKi therapy. The characteristics of the patients are presented in Table 1.
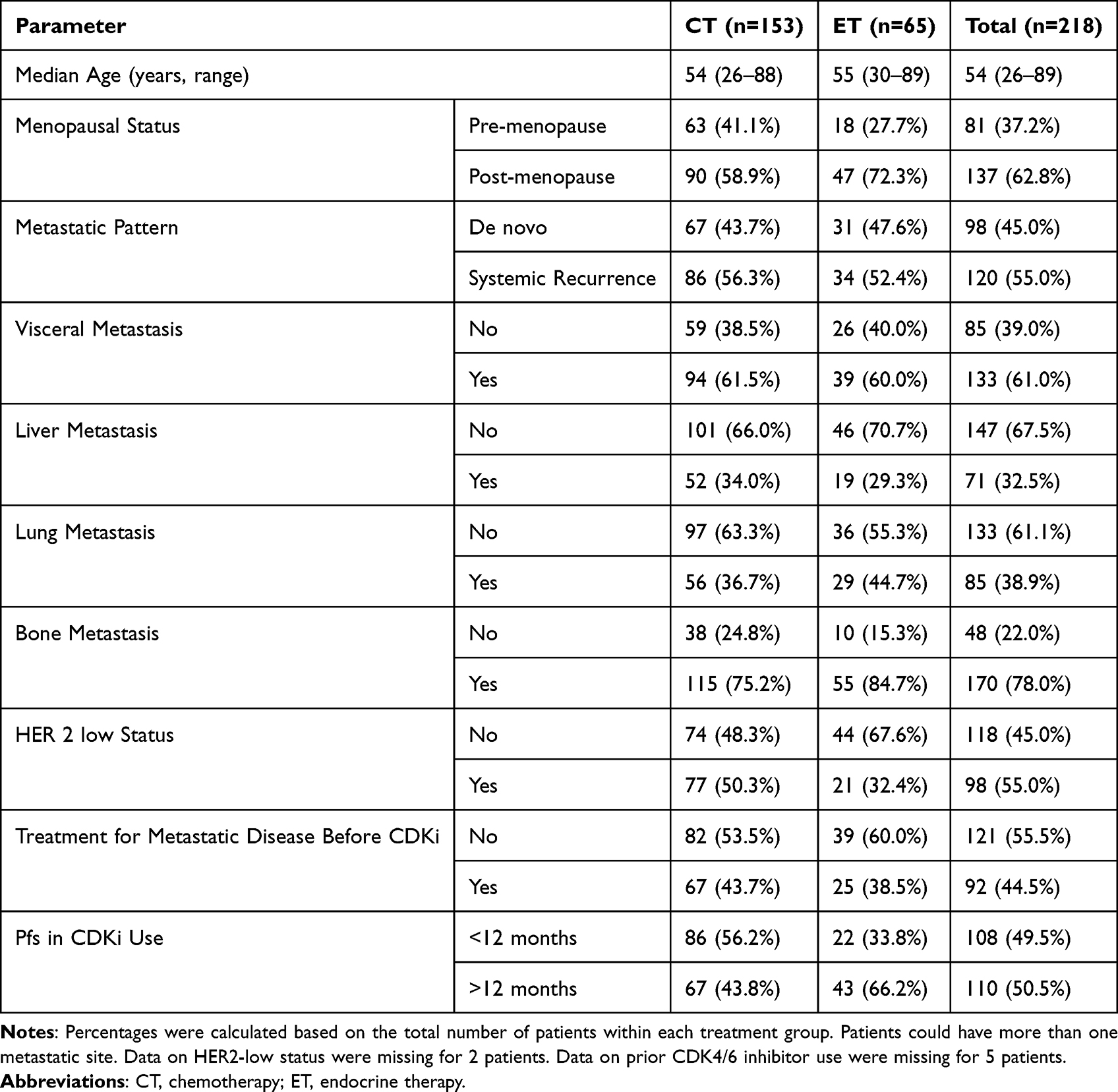 |
Table 1 General Characteristics of Patients |
In the ET group, 50 patients received everolimus plus exemestane, 4 patients received everolimus plus fulvestrant, and 11 patients received only ET (selective estrogen receptor inhibitors, aromatase inhibitors, etc). In the CT-based group, 89 patients received single or intravenous combination CT and 64 patients received oral CT (capecitabine or other drugs, alone or in combination). The most commonly used CT drugs were capecitabine and taxane. The treatments and numbers of patients assigned to treatment groups after CDKi therapy are shown in Table 2.
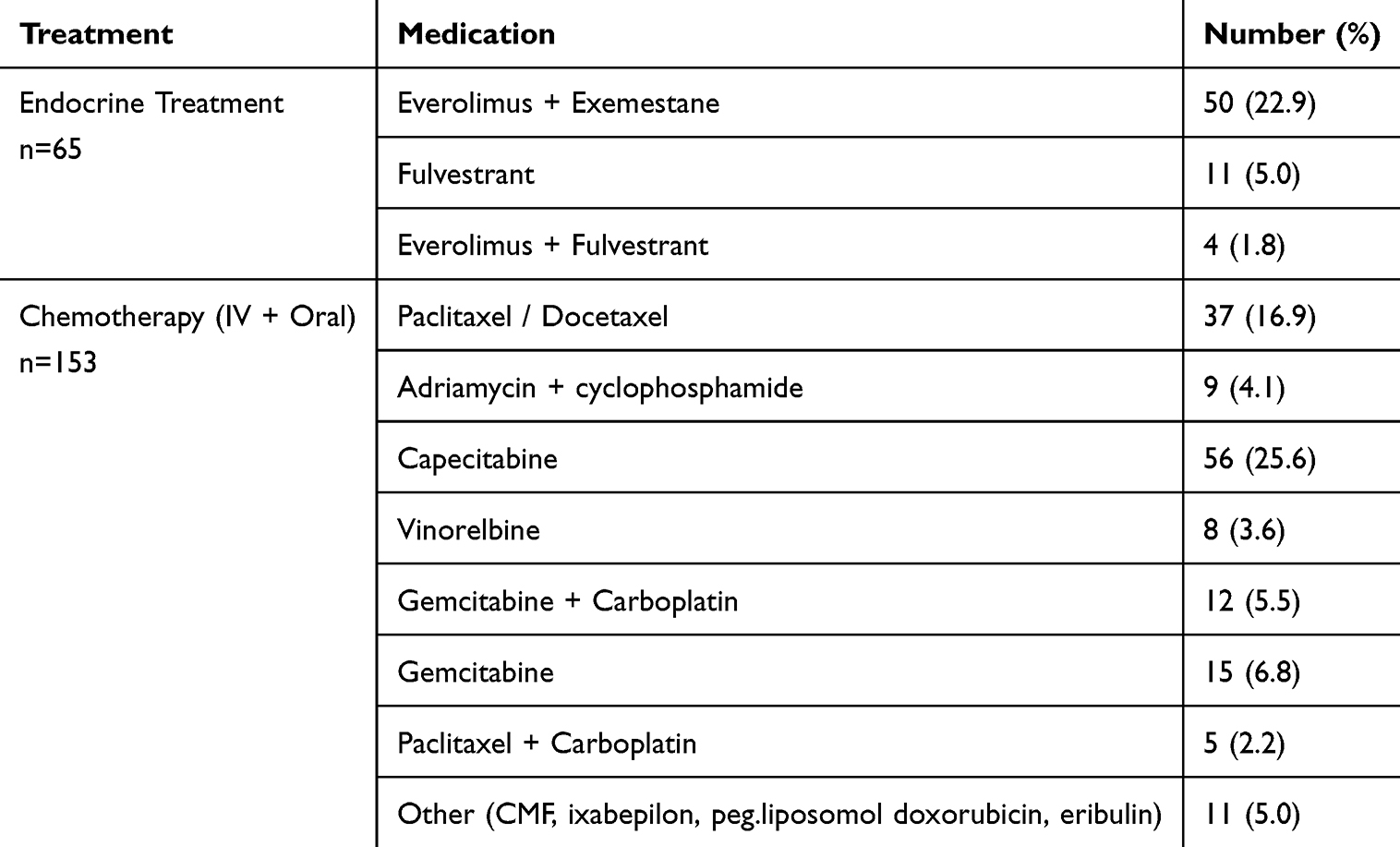 |
Table 2 Treatments Administered to Patients Who Progressed After CDKi |
At the time of diagnosis, 98 patients had de novo metastatic disease, while 120 patients developed systemic recurrence during the course of treatment. Visceral organ involvement was present in 133 patients. When visceral metastases were examined, liver metastases were observed in 52 patients, lung metastases in 56 patients, and brain metastases in 25 patients. Among the 170 patients with bone metastases, 36 had bone as the sole site of involvement.
Among the 218 patients evaluated for HER 2 status, 98 patients with immunohistochemical Cerb2 levels of + 1 or + 2 and negative FISH test results were classified as HER2 low.
Prior to CDKi treatment, 92 patients had received ET or CT, while 121 patients were started on CDKi treatment as first-line therapy. All 92 patients who had previously received systemic treatment received this treatment in metastatic setting. In the univariate analysis, OS was found to be statistically significantly lower in these 92 patients who had previously received treatment (p = 0.032).
With a median follow-up of 32.2 months for the study cohort, when comparing the two groups of patients who progressed after ET plus CDKi therapy and subsequently received ET or CT, the median OS was calculated as 12.2 months (95% CI 9.3–15.1). In the CT arm, the median OS was 10.0 months (95% CI 7.9–12.1), while in the ET arm, it was 18.0 months (95% CI 13.3–22.7). A statistically significant difference was observed between the two groups (p = 0.011) (Figure 1)
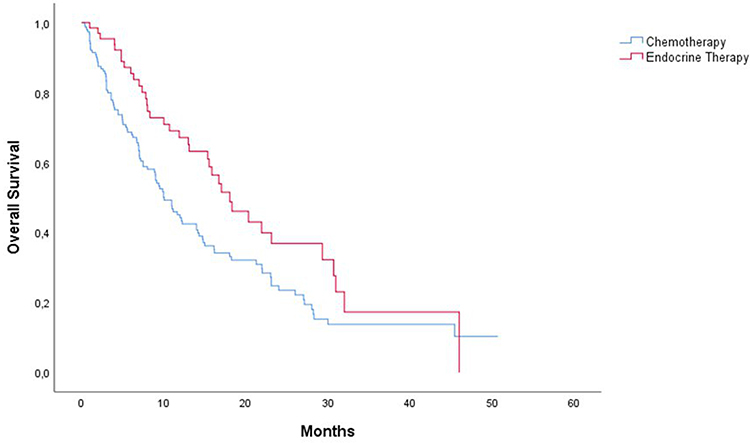 |
Figure 1 Overall survival by treatment group after progression on CDK4/6 inhibitor therapy. Kaplan-Meier curves comparing overall survival for patients receiving subsequent endocrine therapy (ET) versus chemotherapy (CT). Median OS was 18.0 months (95% CI 13.3–22.7) in the ET group and 10.0 months (95% CI 7.9–12.1) in the CT group (p = 0.011, Log rank test). |
When the two groups were compared in terms of PFS, the median PFS was found to be 5.2 months (95% CI 4.5–6.0), while in the CT arm, PFS was 4.9 months (95% CI 3.8–6.0), while in the ET arm, this duration was 6.0 months (95% CI 4.8–7.1), but this difference was not statistically significant (p = 0.06) (Figure 2).
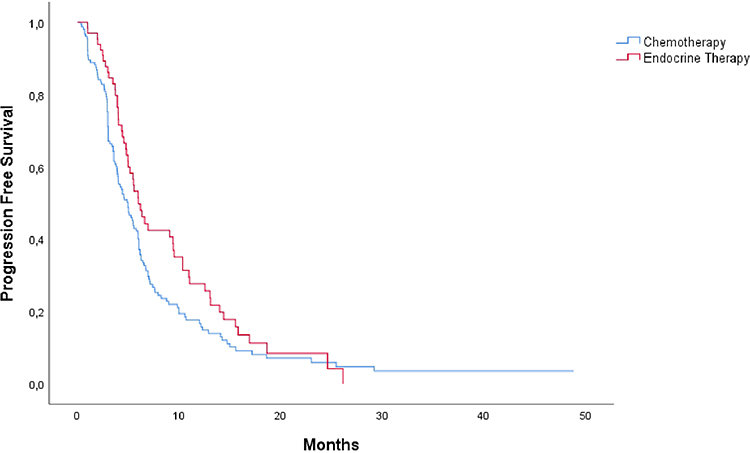 |
Figure 2 Progression-free survival (PFS) by treatment group after progression on CDK4/6 inhibitor therapy. Kaplan-Meier curves comparing progression-free survival for patients receiving subsequent endocrine therapy (ET) versus chemotherapy (CT). Median PFS was 6.0 months (95% CI 4.8–7.1) in the ET group and 4.9 months (95% CI 3.8–6.0) in the CT group (p = 0.06, Log rank test). |
The median PFS for CDKi therapy was 12.2 months. Among all patient groups, 110 patients had PFS > 12 months, while 108 patients had a CDKi treatment duration < 12 months. No significant difference was observed between these two groups in terms of response to subsequent treatments (p = 0.338).
The effects of various factors on OS were evaluated using univariate analysis, as summarised in Table 3. When these parameters were analysed using multivariate analysis, two parameters were found to significantly affect OS in patients: the metastatic status (p = 0.015) and the administration of systemic therapy (CT or ET) prior to CDKi treatment. The results of the multivariate analysis are presented in Table 4.
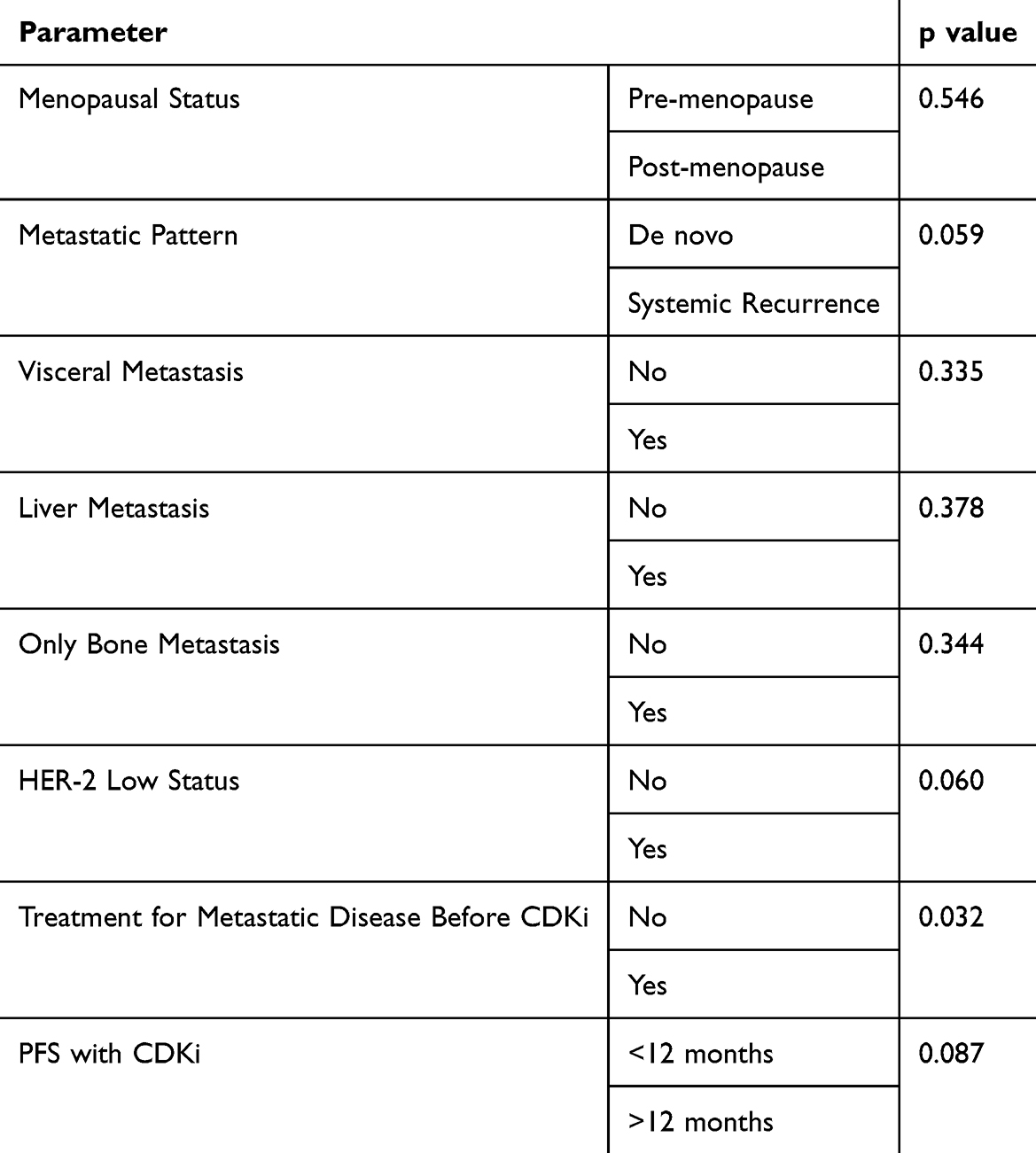 |
Table 3 Univariate Assessment of Factors Influencing the Contribution of Post-CDKi Treatments to OS |
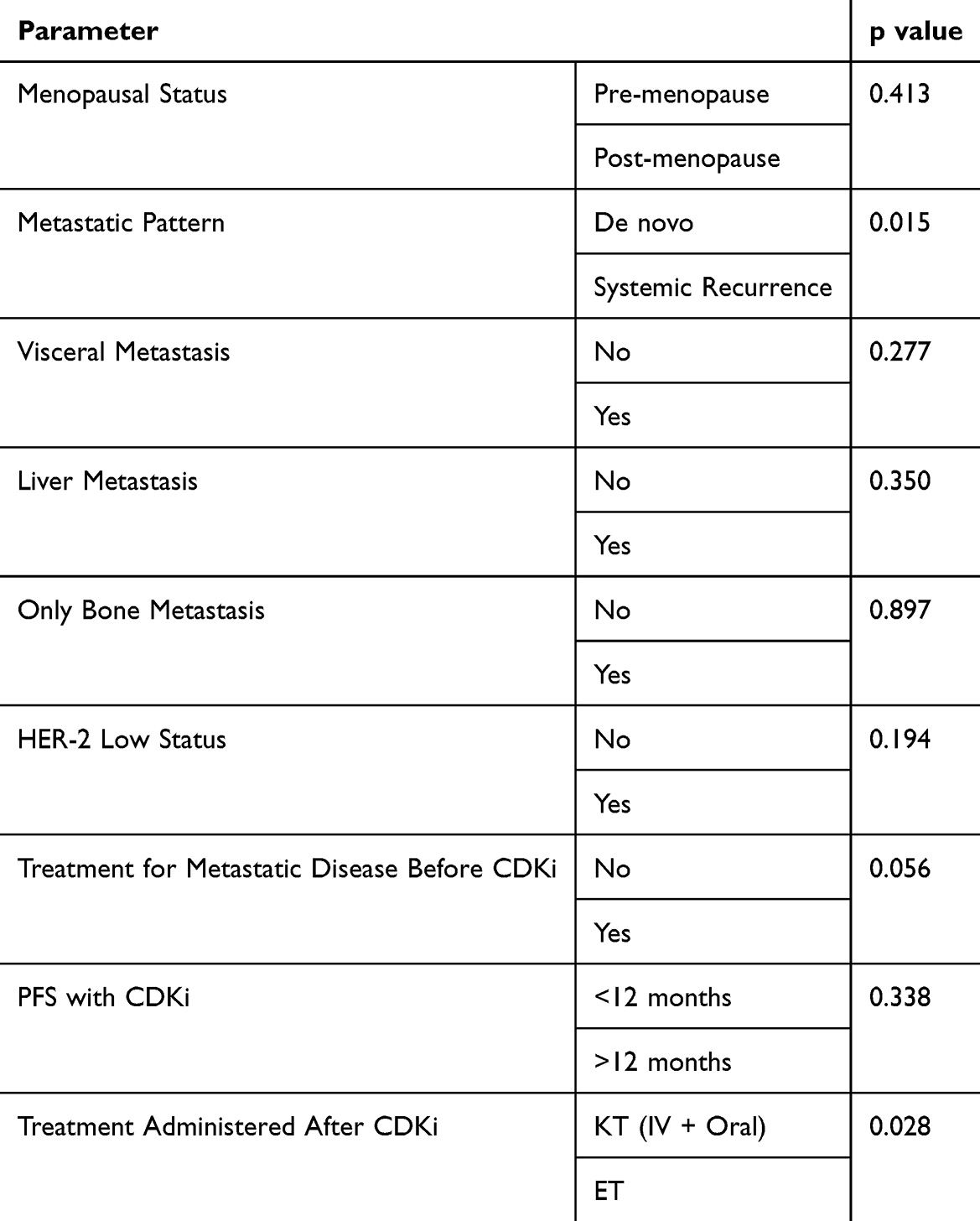 |
Table 4 Multivariate Analysis of Factors Influencing the Contribution of Post-CDKi Treatment to OS |
No statistically significant difference was observed in the distribution of patients who received systemic therapy prior to CDKi between the CT and ET groups (p = 0.260). Additionally, de novo metastatic patients were homogeneously distributed in both groups receiving CT or ET (p = 0.351).
Discussion
The combination of CDKi and ET is the standard treatment for advanced HR-positive, HER2-negative metastatic breast cancer.32 For patients progressing on CDKi-based regimen, different options are available based on tumour mutation status, the patient’s clinical condition, and disease burden; however, a standard treatment has not yet been established. In our study, factors influencing subsequent treatment choices and the efficacy of these treatments were evaluated.
In our study of HR-positive HER2-negative metastatic breast cancer patients who showed progression after CDKi-based treatment, CT was compared with ET, and ET was found to provide a statistically significant survival advantage. Furthermore, although ET’s PFS was not statistically significant when compared to CT, it was numerically superior.
In a multicentre, retrospective, real-world study by Basile et al investigating post-CDKi treatment strategies for HR-positive metastatic breast cancer, patients who received CDKi-based regimen as first-line therapy followed by ET had significantly longer OS compared to those who were directed to CT.33 In this subgroup, the median OS for patients receiving ET was 30.7 months, while the OS for patients receiving CT was 19.1 months, and the difference was statistically significant (p = 0.002). A similar trend was observed in our study; the median OS was 18.0 months in patients who received ET after CDKi therapy and 10.0 months in the CT arm, and this difference was also significant (p = 0.011). However, although both studies aimed to evaluate the effect of treatment selection after CDKi on survival, they contained important design differences. In Basile et al’s study, analyses were performed only for patients who received CDKi-based regimen in the first line, whereas our study included all patients who received CDKi in either the first or second or later lines and subsequently progressed, comparing survival outcomes with ET or CT after treatment. Additionally, while patients who received CDKi-based regimen in the second line were included in Basile et al’s study, no separate OS analysis was presented for this group. When these results are considered together, the ET approach may be more advantageous than CT in terms of survival, especially when added to early CDKi use in the postprogression period.
In a multicentre, retrospective study conducted by Karaçin et al in 2023, no difference in PFS was observed between ET and CT treatments administered following progression under CDKi therapy. In the first-line setting, following progression under CDK4/6 inhibitor-based therapy, the median PFS was 5.3 months for CT and 9.5 months for ET, while in the second-line setting, following progression under CDK4/6 inhibitor-based therapy, the median PFS was 5.7 months and 6.7 months, respectively.34 In another retrospective study by Hanjie Mo et al, 79 patients received everolimus plus exemestane after CDK4/6 inhibitor-based therapy use, and PFS was 3.8 months (95% CI: 3.4–4.7) in these patients.35 Similarly, in our study, no significant difference was found between the two modalities; the median PFS was 4.9 months for CT and 6.0 months for ET (p = 0.06).
In our study, the majority of patients who progressed after CDKi and received ET were treated with this combination therapy in combination with everolimus. In a study analysing 839 patients who progressed after CDKi treatment, 249 (29.7%) received CT, 302 (36%) continued CDKi treatment, and 99 (11%) were treated with everolimus plus exemestane, with an estimated median PFS of 3.3 months.36 Everolimus treatment did not show a statistically significant difference in median PFS compared to CT (3.7 months vs 3.3 months). However, in terms of OS, treatment with everolimus demonstrated statistically significant better OS compared to CT (HR 0.61, 95% CI 0.51–0.74, p = 0.006).
In our study, no significant difference in OS was observed between patients who received CDKi for up to 12 months and those who received this treatment for more than 12 months, based on univariate and multivariate analyses. Similarly, in a study by Kubeczko et al from Poland involving 512 patients who developed progression after CDKi treatment37 and the BYLieve study,38 which evaluated the efficacy of ET plus alpelisib in patients with PIK3CA mutations, analyses were conducted based on a 12-month threshold for prior ET plus CDKi treatment duration, and no significant association was found between the efficacy of subsequent treatment and the duration of CDK4/6 inhibitor-based therapy exposure. On the other hand, contrary to our findings, a recent large multicentre study by Berton Giachetti et al reported that CDKi treatment duration exceeding 12 months was independently associated with longer overall survival in patients who progressed after first- or second-line therapy.39 The absence of a similar association in our study may be explained by the inclusion of patients who received CDKi beyond the second line in our cohort. These differing and sometimes conflicting findings suggest that the duration of ET plus CDKi therapy may be associated with the efficacy of different antitumour agents in various ways. However, the effect of CDK4/6 inhibitor-based therapy exposure duration on OS in HR positive, HER 2 negative metastatic breast cancer remains unclear, and further studies are needed in this area.
In our study, patients with de novo metastatic disease who received ET had significantly longer OS rates compared to those with systemic recurrence (p = 0.015). Similarly, in a multicentre retrospective study published by Karacin et al in 2023, de novo metastatic patients had significantly longer overall survival compared to recurrent metastatic patients (p < 0.05).34 One of the most important reasons for this difference may be that de novo patients were more sensitive to hormonal therapy because they had not previously received systemic treatment. Additionally, in this group, biological aggressiveness is generally lower due to the selection of treatment-resistant clones. On the other hand, patients with systemic recurrence may have a poorer prognosis due to the development of resistance mechanisms to treatment, as they have previously received adjuvant chemotherapy and endocrine therapy. Our findings indicate that the initial presentation of metastatic disease (de novo or systemic recurrence) is an independent prognostic factor for overall survival. The relatively high proportion of patients presenting with de novo metastatic disease in our cohort likely reflects real-world referral patterns to tertiary oncology centers and potential delays in diagnosis, and this variable was accounted for in the multivariate analysis as an independent prognostic factor.
In our study, among metastatic HR-positive HER2-negative breast cancer patients who progressed after CDKi treatment, a statistically significant difference was found in OS between the use of CDKi in the first line and subsequent lines in univariate analysis (p = 0.032). However, no statistically significant difference was found in multivariate analysis (p = 0.056). Since a statistically significant difference was observed in the univariate analysis, the distribution between groups was examined, and no statistically significant difference was found in the proportion of patients who had previously received systemic therapy between the CT and ET groups (p = 0.26). This result suggests that the early use of CDK4/6 inhibitor-based therapy may provide a survival advantage by more effectively suppressing tumour biology. Randomised studies directly addressing this issue are limited in the literature. Phase III studies such as PALOMA-218 and MONARCH-340 have demonstrated a survival advantage with the first-line use of CDKi, but they did not directly compare the effect of the order of use on OS. The SONIA-2 study compared the use of CDK4/6 inhibitor-based therapy as first- or second-line therapy and reported no significant difference in OS.41 On the other hand, in a Turkey-based multicentre retrospective study by Karaçin et al, ET demonstrated superiority over CT in terms of PFS when administered after CDK4/6 inhibitor-based therapy; however, OS data were not reported.34 Our study contributes real-world evidence regarding overall survival outcomes associated with treatment selection after progression on CDK4/6 inhibitor–based therapy. However, larger and prospective studies are needed to clarify the impact of post-progression treatment strategies and treatment sequence on long-term survival.
Study Limitations
Our study has some limitations. The most notable is the heterogeneous patient population. There was an imbalance in the number of patients between the CT and ET groups among patients receiving post-CDKi treatment. Additionally, the retrospective design and lack of data on patients’ molecular profiles limit the interpretation of results. Another limitation of our study is the lack of consistent data regarding primary versus secondary endocrine resistance patterns. This precluded a subgroup analysis based on resistance profiles, which are known to influence treatment outcomes in this patient population. Nevertheless, the inclusion of a large, real-world patient population is a strength of our study. Given the limited data examining the impact of post-CDKi treatment options on survival in real-world settings, our findings fill an important gap. Our findings suggest that treatment sequence and strategy may influence survival. However, larger, prospective, and molecularly detailed studies are needed to confirm this finding. Such data are critical for personalised treatment planning and determining optimal treatment strategies.
Conclusion
In conclusion, this real-world study demonstrates that continuing with ET, particularly everolimus-based combinations, after progression on CDKi provides a significant OS benefit compared to switching to CT. These findings offer robust evidence supporting current guideline recommendations to prioritize endocrine-based strategies before CT in this clinical setting. Multivariate analysis confirmed that both the treatment strategy (ET vs CT) and de novo metastatic presentation were independent predictors of overall survival. Prospective trials are needed to definitively establish the optimal treatment sequence in this setting and to integrate molecular profiling for personalized strategy selection.
Institutional Review Board Statement
This study was conducted in accordance with the Helsinki Declaration and was reviewed and approved by the Ethics Committee of Selçuk University Faculty of Medicine, Konya, Turkey (20/2025, dated 14 January 2025).
Abbreviations
AI, Aromatase Inhibitor; AKT, Protein Kinase B (Serine/Threonine Kinase); BRCA, Breast Cancer Gene; CDKi, Cyclin-Dependent Kinase 4/6 Inhibitor; CI, Confidence Interval; CMF, Cyclophosphamide, Methotrexate, 5-Fluorouracil; CT, Chemotherapy; ET, Endocrine Therapy; FISH, Fluorescence In Situ Hybridization; HER2, Human Epidermal Growth Factor Receptor 2; HR, Hormone Receptor; HR, Hazard Ratio; IV, Intravenous; mBC, Metastatic Breast Cancer; mTOR, Mammalian Target of Rapamycin; OS, Overall SurvivalPFS, Progression-Free Survival; PIK3CA, Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Alpha; SERD, Selective Estrogen Receptor Degrader/Downregulator; SOC, Standard of Care.
Data Sharing Statement
For access the data, interested parties can contact the corresponding author upon request.
Consent for Publication
This study utilized anonymized clinical data, and no identifiable individual patient images, data, or personal details are presented in this manuscript.
Informed Consent Statement
Patient consent was waived because of the retrospective nature of the study, as determined by the Ethics Committee.
Acknowledgments
The authors are grateful to all the patients and their families. We also thank the multidisciplinary teams at the participating oncology centers for their dedication and collaboration.
Author Contributions
All authors made a significant contribution to the work reported, including study conception and design, data acquisition, analysis and interpretation, drafting, revising, or critically reviewing the article. All authors approved the final version to be published, agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflict of interest.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–12. doi:10.3322/caac.21763
2. National Cancer Institute. Cancer stat facts: female breast cancer. 2019. Available from: https://seer.cancer.gov/statfacts/html/breast.html.
3. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
4. Howlader N, Altekruse SF, Li CI, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106(5):dju055. doi:10.1093/jnci/dju055
5. Gennari A, André F, Barrios C, et al. ESMO clinical practice guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475–1495. doi:10.1016/j.annonc.2021.09.019
6. Gradishar WJ. NCCN guidelines updates: management of patients with HER2-negative breast cancer. J Natl Compr Canc Netw. 2022;20(5.5):561–565. doi:10.6004/jnccn.2022.5016
7. Morgan LR, Schein PS, Woolley PV, et al. Therapeutic use of tamoxifen in advanced breast cancer: correlation with biochemical parameters. Cancer Treat Rep. 1976;60(10):1437–1443.
8. Nagini S. Breast cancer: current molecular therapeutic targets and new players. Anticancer Agents Med Chem. 2017;17(2):152–163. doi:10.2174/1871520616666160502122724
9. Simpson ER, Davis SR. Aromatase and the regulation of estrogen biosynthesis. Endocrinology. 2001;142(11):4589–4594. doi:10.1210/endo.142.11.8547
10. Nagaraj G, Ma C. Revisiting the estrogen receptor pathway and its role in endocrine therapy. Breast Cancer Res Treat. 2015;150(2):231–242. doi:10.1007/s10549-015-3316-4
11. Mauri D, Pavlidis N, Polyzos NP, Ioannidis JP. Survival with aromatase inhibitors vs. standard hormonal therapy in advanced breast cancer: meta-analysis. J Natl Cancer Inst. 2006;98(18):1285–1291. doi:10.1093/jnci/djj357
12. Li J, Wang Z, Shao Z. Fulvestrant in the treatment of HR+/HER2- advanced breast cancer: a review. Cancer Med. 2019;8(5):1943–1957. doi:10.1002/cam4.2095
13. Schiavon G, Smith IE. Endocrine therapy for advanced/metastatic breast cancer. Hematol Oncol Clin North Am. 2013;27(4):715–736. doi:10.1016/j.hoc.2013.05.004
14. Dowsett M. Endocrine resistance in advanced breast cancer. Acta Oncol. 1996;35(Suppl 5):91–95. doi:10.3109/02841869609083979
15. Razavi P, Chang MT, Xu G, et al. The genomic landscape of endocrine-resistant advanced breast cancers. Cancer Cell. 2018;34(3):427–438.e6. doi:10.1016/j.ccell.2018.08.008
16. Hanker AB, Sudhan DR, Arteaga CL. Overcoming endocrine resistance in breast cancer. Cancer Cell. 2020;37(4):496–513. doi:10.1016/j.ccell.2020.03.009
17. Hortobagyi GN, Stemmer SM, Burris HA, et al. Ribociclib as first-line therapy for HR+ advanced breast cancer. N Engl J Med. 2016;375(18):1738–1748. doi:10.1056/NEJMoa1609709
18. Finn RS, Martin M, Rugo HS, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375(20):1925–1936. doi:10.1056/NEJMoa1607303
19. Cardoso F, Paluch-Shimon S, Senkus E, et al. ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann Oncol. 2020;31(12):1623–1649. doi:10.1016/j.annonc.2020.09.010
20. Mittal A, Molto Valiente C, Tamimi F, et al. Novel endocrine and biologic options post-CDK4/6 inhibitors. Cancers. 2023;15(7):2015. doi:10.3390/cancers15072015
21. Ashai N, Swain SM. Post-CDK4/6 inhibitor therapy: current agents and novel targets. Cancers. 2023;15(6):1855. doi:10.3390/cancers15061855
22. Ma J, Chan JJ, Toh CH, Yap YS. Emerging therapy options beyond CDK4/6 inhibitors in HR+/HER2- breast cancer. NPJ Breast Cancer. 2023;9(1):1–16. doi:10.1038/s41523-023-00578-3
23. Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal HR+ advanced breast cancer. N Engl J Med. 2012;366(6):520–529. doi:10.1056/NEJMoa1109653
24. Kornblum N, Zhao F, Manola J, et al. Fulvestrant plus everolimus vs placebo in HR+/HER2- AI-resistant mBC: prE0102. J Clin Oncol. 2018;36(16):1556–1563. doi:10.1200/JCO.2017.76.9331
25. Schmid P, Zaiss M, Harper-Wynne C, et al. Fulvestrant-based combinations in HR+ mBC: MANTA trial. JAMA Oncol. 2019;5(11):1556–1564. doi:10.1001/jamaoncol.2019.2526
26. Robson M, Im SA, Senkus E, et al. Olaparib for metastatic breast cancer in Patients with a germline BRCA mutation. N Engl J Med. 2017;377(6):523–533. doi:10.1056/NEJMoa1706450
27. Litton JK, Rugo HS, Ettl J, et al. Talazoparib in Patients with advanced breast cancer and a germline BRCA mutation. N Engl J Med. 2018;379(8):753–763. doi:10.1056/NEJMoa1802905
28. André F, Ciruelos E, Rubovszky G, et al. Alpelisib for PIK3CA -mutated, hormone receptor–positive advanced breast cancer. N Engl J Med. 2019;380(20):1929–1940. doi:10.1056/NEJMoa1813904
29. Turner NC, Oliveira M, Howell SJ, et al. Capivasertib in HR+ advanced breast cancer. N Engl J Med. 2023;388(22):2058–2070. doi:10.1056/NEJMoa2214131
30. Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
31. Rugo HS, Bardia A, Marmé F, et al. TROPiCS-02: sacituzumab govitecan vs TPC in HR+/HER2- breast cancer. J Clin Oncol. 2022;40(17_suppl):LBA1001. doi:10.1200/JCO.2022.40.17_suppl.LBA1001
32. Rashmi KR, Schonfeld R, Gradishar WJ, et al. NCCN Guidelines Version 2.2024: breast Cancer.
33. Basile D, Gerratana L, Corvaja C, et al. Post-CDKi treatment strategies in HR+/HER2- mBC: real-world study. Breast. 2021;57:104–112. doi:10.1016/j.breast.2021.02.015
34. Karacin C, Oksuzoglu B, Demirci A, et al. Post-CDKi therapies in HR+ advanced breast cancer. BMC Cancer. 2023;23(1):1–10. doi:10.1186/s12885-022-10466-x
35. Mo H, Renna CE, Moore HCF, et al. Real-world outcomes of everolimus plus exemestane after CDKi. Clin Breast Cancer. 2022;22(2):143–148. doi:10.1016/j.clbc.2021.10.002
36. Martin JM, Handorf EA, Montero AJ, et al. Post-CDKi systemic therapies: real-world data. Oncologist. 2022;27(6):441–446. doi:10.1093/oncolo/oyac075
37. Kubeczko M, Polakiewicz-Gilowska A, Świderska K, et al. Post-CDKi treatment patterns in ABC: polish real-world data. Front Oncol. 2024;14:1408664. doi:10.3389/fonc.2024.1408664
38. Chia SKL, Ruiz-Borrego M, Drullinsky P, et al. BYLieve: impact of prior CDKi duration on alpelisib benefit. J Clin Oncol. 2021;39(15_suppl):1060. doi:10.1200/JCO.2021.39.15_suppl.1060
39. Berton Giachetti PPM, Morganti S, Gandini S, et al. Survival following CDK4/6 inhibitor therapy for hormone receptor–positive, ERBB2–negative metastatic breast cancer. JAMA Network Open. 2025;8(2):e2461067. doi:10.1001/jamanetworkopen.2024.61067
40. Johnston SRD. MONARCH 3: abemaciclib plus ET in HR+/HER2− mBC—Final OS. J Clin Oncol. 2023;41(18_suppl):LBA500.
41. Turner NC, Im SA, Boyle FM, et al. SONIA: ribociclib plus ET vs ET alone—final OS. Lancet Oncol. 2023;24(5):561–574.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ribociclib Plus Letrozole in Italian Male Patients with Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative Advanced Breast Cancer: Case Studies of Phase 3b CompLEEment-1 Trial
Caputo R, Fabi A, Romagnoli E, Baldini E, Grasso D, Fenderico N, Michelotti A
Breast Cancer: Targets and Therapy 2022, 14:351-362
Published Date: 18 October 2022
Pembrolizumab in Lymphopenic Metastatic Breast Cancer Patients Treated with Metronomic Cyclophosphamide: A Clinical and Translational Prospective Study
Mery B, Ménétrier-Caux C, Montané L, Heudel PE, Ray-Coquard I, Bachelot T, Derbel O, Augereau P, Treilleux I, Berthet J, Nkodia A, Bardin-Dit-Courageot C, Attignon V, Ferrari A, Garin G, Perol D, Caux C, Dubois B, Trédan O
Breast Cancer: Targets and Therapy 2023, 15:311-325
Published Date: 27 April 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Clinical Efficacy and Security Analysis of CDK4/6 Inhibitors Combined with ET in Patients with HR+HER2− Advanced Breast Cancer
Wang Y, Chen D, Wang Z, Jin X, Zhang J, Lv Y
Cancer Management and Research 2026, 18:579562
Published Date: 22 May 2026
Precision Endocrine-Based Combinations After CDK4/6 Inhibitor Progression in HR-Positive Metastatic Breast Cancer
Abdel-Razeq H
Drug Design, Development and Therapy 2026, 20:611371
Published Date: 9 July 2026