Back to Journals » Drug Design, Development and Therapy » Volume 20
Precision Endocrine-Based Combinations After CDK4/6 Inhibitor Progression in HR-Positive Metastatic Breast Cancer
Authors Abdel-Razeq H ![]()
Received 23 March 2026
Accepted for publication 27 May 2026
Published 9 July 2026 Volume 2026:20 611371
DOI https://doi.org/10.2147/DDDT.S611371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Hikmat Abdel-Razeq1,2
1Section of Hematology and Medical Oncology, Department of Internal Medicine, King Hussein Cancer Center, Amman, 11941, Jordan; 2School of Medicine, the University of Jordan, Amman, 11941, Jordan
Correspondence: Hikmat Abdel-Razeq, Department of Internal Medicine King Hussein Cancer Center, 202 Queen Rania Al Abdullah Street, Amman, 11941, Jordan, Tel +962-6 5300460, Ext: 1000, Email [email protected]
Abstract: CDK4/6 inhibitors combined with endocrine therapy (ET) has significantly improved progression-free (PFS) and overall survival (OS) in patients with hormone receptor-positive (HR+), HER2-negative breast cancer, however, most patients ultimately develop acquired resistance and experience disease progression. Historically, this transition marked the point at which chemotherapy was initiated; however, advances in molecular profiling and drug development have fundamentally altered this paradigm.Resistance to endocrine therapy is mediated by distinct and therapeutically actionable mechanisms, most notably ESR1 mutations, activation of the PI3K/AKT/mTOR signaling pathway, and cell-cycle deregulation. These insights have led to the development of a new generation of targeted endocrine therapies that restore or prolong endocrine sensitivity. Oral selective estrogen receptor degraders (SERDs), particularly elacestrant and imlunestrant, have demonstrated clinically meaningful efficacy in patients with ESR1-mutant tumors progressing after CDK4/6 inhibitors. Additionally, targeted inhibitors of the PI3K and AKT pathways, such as alpelisib and capivasertib, when combined with appropriate endocrine backbones, have been shown to overcome resistance mechanisms.The emergence of circulating tumor DNA (ctDNA) testing has further refined therapeutic decision-making by enabling real-time detection of resistance mutations and guiding directed treatment selection. Several prospective trials have demonstrated that molecularly guided switching of endocrine therapy can delay clinical progression and extend disease control, highlighting a shift toward precision-based, adaptive strategies.Collectively, these advances support a new treatment paradigm in which endocrine-based combinations remain the preferred approach after progression, delaying the need for chemotherapy while maintaining efficacy and quality of life. This review summarizes the biology of endocrine resistance, evaluates current targeted endocrine therapies, and provides a practical framework for biomarker-driven sequencing in patients with HR+/HER2− advanced breast cancer following progression on prior endocrine therapy.
Keywords: metastatic breast cancer, endocrine therapy, CDK4/6 inhibitors, precision therapy, ESR1, ctDNA, PI3K/AKT/mTOR
Introduction
Hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2–) breast cancer accounts for approximately 70% of all metastatic breast cancers and remains largely driven by estrogen receptor (ER) signaling.1,2 Over the past decade, the integration of cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors with endocrine therapy (ET) has transformed the management of metastatic breast cancer (MBC), producing unparalleled improvements in progression-free survival (PFS) and overall survival (OS) compared with ET alone.3 Large Phase III trials, including MONALEESA-2/3/74–6 PALOMA-2,7 and MONARCH-3,8 have established CDK4/6 inhibitor–based regimens as the standard first-line therapy for HR+/HER2– MBC, achieving median PFS ranging approximately from 20–33 months and overall survival ranging from approximately 45 months to beyond 60 months in selected studies.4–8
Despite these major advances, most patients ultimately experience disease progression due to the development of endocrine resistance.9 Once resistance emerges, the therapeutic challenge shifts from simple endocrine substitution, or initiation of chemotherapy, to the rational deployment of molecularly targeted strategies that suppress escape pathways and restore ER sensitivity. Advances in genomic profiling, particularly circulating tumor DNA (ctDNA) analysis, have revealed that acquired resistance is driven by clonal evolution involving ER mutations (ESR1),10 activation of PI3K/AKT/mTOR signaling, and alterations in cell-cycle control.11 These insights have led to the development of novel oral selective estrogen receptor degraders (SERDs), PI3K and AKT inhibitors, and other targeted combinations that extend endocrine sensitivity beyond progression on first-line therapy.12
The current management of HR+/HER2– advanced breast cancer therefore requires a systematically informed approach to post-progression therapy, in which endocrine backbones are combined with targeted agents selected according to tumor biology.13,14 This review focuses on the evolving endocrine strategies for patients who progress after prior CDK4/6 inhibitors.
Biology of Endocrine Resistance After Endocrine Therapy
Advances in genomic profiling, particularly serial ctDNA analysis, have demonstrated that endocrine resistance is a dynamic and heterogeneous process involving both acquired subclonal alterations and pre-existing truncal genomic events.15 ESR1 mutations frequently emerge under selective therapeutic pressure and may expand during treatment, representing a classic mechanism of acquired endocrine resistance.16 In contrast, alterations such as PIK3CA mutations are often early truncal events that may persist throughout tumor evolution rather than arise exclusively at progression. Furthermore, activation of resistance pathways including PI3K/AKT/mTOR signaling may occur through non-mutational mechanisms such as signaling crosstalk, epigenetic adaptation, or compensatory pathway activation, which are not always fully captured by ctDNA-based genomic profiling alone.17 These observations highlight both the biological complexity of endocrine resistance and the limitations of relying solely on genomic mutation profiling to characterize functional pathway activation. Table 1 summarizes these mechanisms of endocrine resistance.18–23
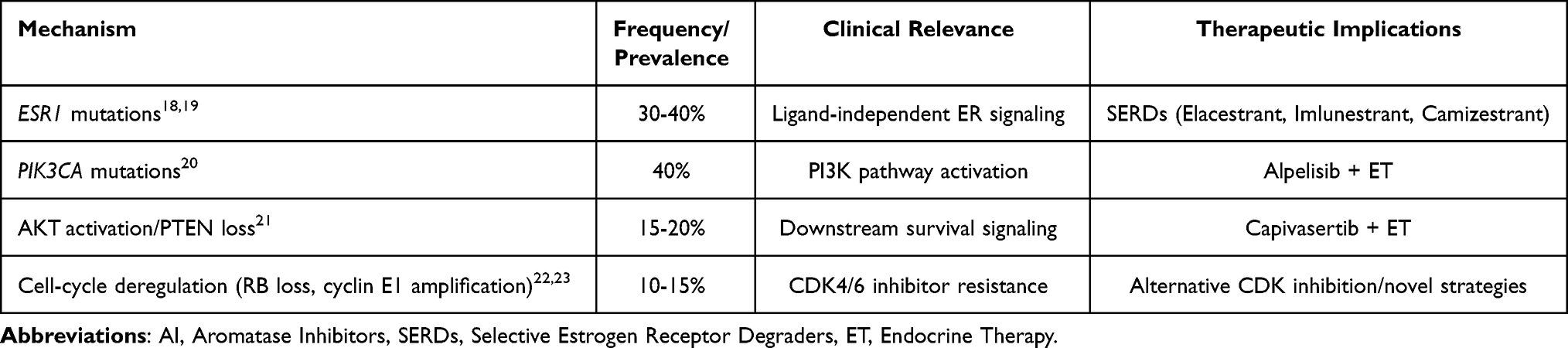 |
Table 1 Mechanisms of Endocrine Resistance |
The persistence of partial ER dependency in some resistant tumors supports the continued use of endocrine-based combinations after progression, particularly in biomarker-selected patients with actionable alterations such as ESR1 mutations or PI3K/AKT pathway activation. However, endocrine responsiveness generally diminishes with successive lines of therapy, especially in endocrine-refractory disease.24
ESR1 Mutations
Mutations in the ESR1 gene, which encodes the estrogen receptor α, represent one of the most important mechanisms of acquired resistance to endocrine therapy. These mutations, most commonly occurring in the ligand-binding domain, lead to constitutive, ligand-independent activation of ER signaling. ESR1 mutations are rare in primary breast cancer but emerge in approximately 40% of patients following prolonged exposure to AIs in patients with advanced stage disease.18
Functionally, ESR1 mutations confer resistance to estrogen deprivation by AIs, while retaining partial sensitivity to ER antagonists. Preclinical and clinical data demonstrate that SERDs, particularly oral SERDs, are more effective than AIs or tamoxifen in suppressing mutant ER signaling. The detection of ESR1 mutations in ctDNA has therefore become an essential biomarker guiding therapy selection following disease progression on AI.19
PI3K–AKT–mTOR Pathway Activation
Activation of the PI3K/AKT/mTOR signaling cascade is another major driver of endocrine resistance. PIK3CA mutations, which occur in approximately 30–45% of HR+/HER2– breast cancers promote estrogen-independent cell growth and survival.25
Resistance to CDK4/6 inhibitors is increasingly recognized as a biologically heterogeneous process involving both direct alterations of the cyclin D–CDK4/6–RB pathway and activation of compensatory signaling networks. Proposed resistance mechanisms include RB1 loss or dysfunction, cyclin E/CDK2 activation, CDK6 amplification, and adaptive activation of parallel pathways such as PI3K/AKT/mTOR, FGFR, and MAPK signaling.26,27 In addition, endocrine resistance may arise through ESR1 mutations, epigenetic reprogramming, and signaling crosstalk that promote estrogen-independent tumor growth. Importantly, not all resistance mechanisms are fully captured by genomic profiling alone, as functional pathway activation may occur through non-mutational processes.28
These biologic insights have important therapeutic implications in the post-CDK4/6 inhibitor setting. Selected patients may continue to benefit from endocrine-based strategies when combined with biomarker-directed targeted therapies, including oral SERDs for ESR1-mutant disease and PI3K/AKT/mTOR inhibitors for tumors harboring actionable pathway alterations.29 Other emerging approaches include continuation or switching of CDK4/6 inhibitors, development of CDK2-targeted therapies to overcome cyclin E–mediated resistance, and rational combination strategies designed to delay or reverse endocrine escape. These evolving treatment paradigms further support the growing role of precision medicine in guiding therapy selection after CDK4/6 inhibitor progression.
Cell-Cycle Deregulation
Resistance to CDK4/6 inhibition is increasingly recognized as a contributor to post-progression disease. Mechanisms include loss of retinoblastoma (RB) protein, amplification of cyclin E1 (CCNE1), and activation of CDK2, all of which allow tumor cells to bypass CDK4/6 blockade and continue proliferating.30 These alterations often coexist with endocrine resistance mechanisms, further underscoring the need for combination strategies that target both ER signaling and cell-cycle escape pathways.31
Targeted Endocrine Combinations After Progression on Endocrine Therapy
The therapeutic landscape of HR-positive/HER2-negative metastatic breast cancer following progression on CDK4/6 inhibitor-based therapy has evolved substantially in recent years. While antibody drug conjugates (ADCs), including sacituzumab govitecan and trastuzumab deruxtecan, have emerged as important standards of care for patients with endocrine-refractory disease and in later treatment lines, many patients retain partial endocrine sensitivity and may still benefit from biomarker-driven endocrine-based strategies.32 Consequently, increasing emphasis has been placed on identifying actionable molecular alterations such as PIK3CA, ESR1, AKT, and PTEN abnormalities to guide personalized treatment selection.33,34 This section focuses primarily on precision endocrine-based therapeutic approaches after CDK4/6 inhibitor progression, particularly in patients with preserved endocrine responsiveness, while acknowledging the growing role of ADCs and chemotherapy in endocrine-resistant disease.
Targeting ESR1 Mutations: Oral SERDs
Multiple studies have shown that ESR1 mutations detected in peripheral blood are strongly associated with resistance to AIs but retained sensitivity to SERDs.35, In the PADA-1 trial, patients receiving first-line AI plus palbociclib underwent serial ctDNA monitoring. Those who developed ESR1 mutations without radiological or clinical progression were randomized to switch to fulvestrant plus palbociclib or continue their regimen. Early switching significantly improved median PFS (11.9 vs 5.7 months), demonstrating for the first time that molecular progression can guide endocrine therapy adaptation and improve outcomes.36 Similarly, in the EMERALD trial as detailed below, the benefit of elacestrant was largely driven by patients with ESR1-mutant tumors, further validating ESR1 mutation status as a predictive biomarker rather than merely a prognostic factor.
Elacestrant (EMERALD Trial)
Elacestrant is the first oral selective estrogen receptor degrader (SERD) to demonstrate superiority over standard endocrine therapy in a randomized phase III trial. The EMERALD trial enrolled 478 patients with ER-positive, HER2-negative metastatic breast cancer whose disease had progressed after prior endocrine therapy and mandatory CDK4/6 inhibitor exposure. Patients were randomized to receive elacestrant or investigator’s choice of standard endocrine therapy (fulvestrant or an aromatase inhibitor). ESR1 mutation status was prospectively assessed using circulating tumor DNA (ctDNA) and used as a stratification biomarker for treatment evaluation.37
In the overall study population, elacestrant significantly improved progression-free survival (PFS) compared with standard endocrine therapy (HR 0.70; P=0.0018). The greatest benefit was observed in patients harboring ESR1 mutations, in whom median PFS was 3.8 months with elacestrant versus 1.9 months with standard therapy (HR 0.55; P=0.0005). Importantly, outcomes appeared particularly favorable among patients with prolonged prior exposure to CDK4/6 inhibitors. In the subgroup receiving ≥12 months of prior CDK4/6 inhibition, median PFS reached 8.6 months with elacestrant versus 1.9 months with standard therapy among patients with ESR1-mutant tumors (HR 0.41), Table 2.38 These findings suggest that patients with retained endocrine sensitivity may derive the greatest benefit from elacestrant-based therapy after CDK4/6 inhibitor progression. Elacestrant was generally well tolerated, with nausea, fatigue, and vomiting representing the most commonly reported adverse events. Treatment discontinuation rates due to toxicity were low.
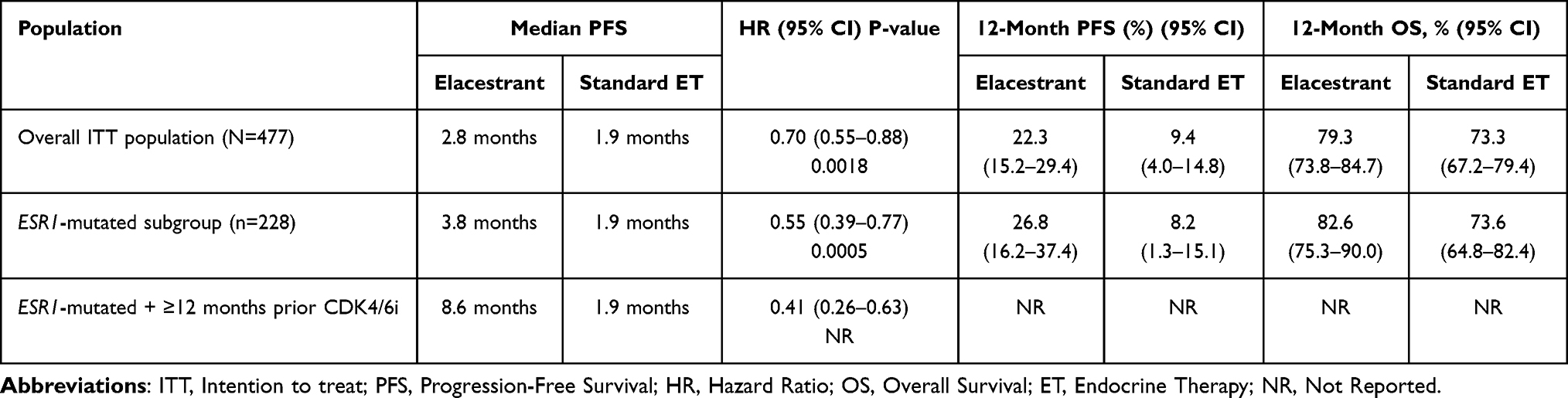 |
Table 2 EMERALD Trial, Elacestrant vs Standard Endocrine Therapy |
Collectively, EMERALD established elacestrant as an important biomarker-driven endocrine treatment option for patients with ESR1-mutated HR-positive/HER2-negative metastatic breast cancer following progression on CDK4/6 inhibitor-based therapy. The study also reinforced the clinical utility of ctDNA-based ESR1 mutation detection for therapeutic selection in endocrine-resistant disease. Based on these findings, elacestrant received regulatory approval in 2023 for ER-positive, HER2-negative, ESR1-mutated advanced breast cancer after progression on endocrine therapy.39
Imlunestrant (EMBER-3 Trial)
More recently, the EMBER-3 study has established imlunestrant, another oral SERD, as an effective drug in endocrine-pretreated ER+/HER2-negative MBC, particularly in tumors with ESR1 mutations. In this trial, 874 patients were randomized to receive single agent imlunestrant (n= 331), standard ET (investigator’s choice of fulvestrant or exemestane; n= 330), or imlunestrant in combination with abemaciclib (n= 213). Among the 256 patients with ESR1-mutated tumors, imlunestrant monotherapy significantly improved median PFS compared with standard therapy, 5.5 months vs 3.8 months, corresponding to a 38% reduction in the risk of progression or death (HR 0.62; 95% CI 0.46–0.82; P= 0.0008). Importantly, the imlunestrant–abemaciclib combination demonstrated even greater efficacy in the overall population, with median PFS of 10.9 versus 5.5 months (HR 0.59, 95% CI 0.47–0.74, nominal P< 0.0001) indicating a robust activity irrespective of prior CDK4/6 inhibitor exposure or ESR1 status. Updated analyses also suggest a clinically meaningful extension in median OS for imlunestrant monotherapy in ESR1-mutant disease (34.5 months vs 23.1 months; HR 0.60), although formal statistical boundaries were not met.40–42 These results reinforce imlunestrant as a potent oral SERD with significant clinical benefit in a biomarker-defined subset and support continued evaluation of combination strategies with CDK4/6 inhibitors. Based on these findings, the U.S. Food and Drug Administration (FDA) approved imlunestrant in September 2025 for patients with ER+, HER2-negative and ESR1-mutated advanced breast cancer whose disease has progressed after at least one line of ET. Detailed of Imlunestrant therapy in all patients and those with or without ESR1 mutation are summarized in Table 3.
 |
Table 3 EMBER-3 Trial, Imlunestrant vs Standard Endocrine Therapy |
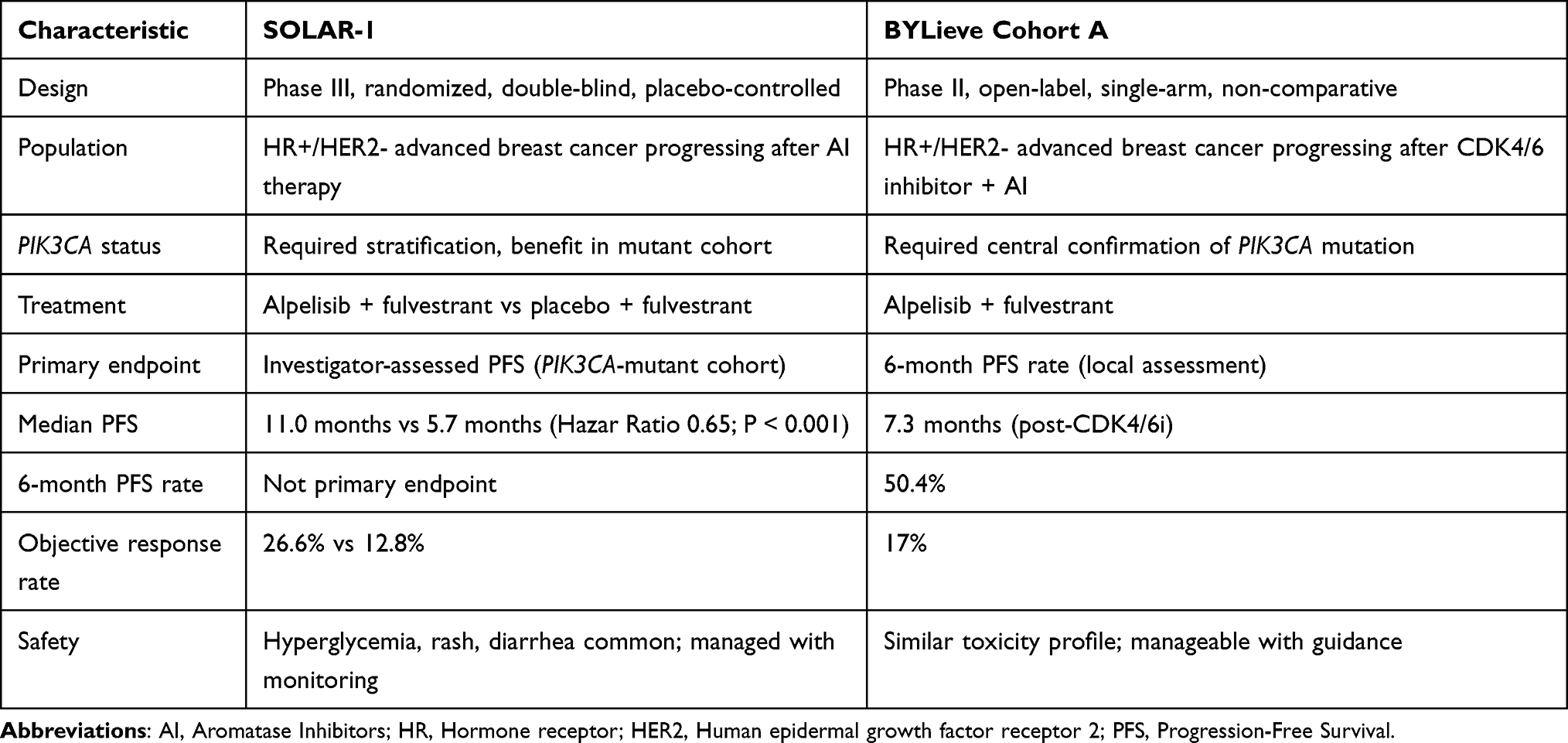 |
Table 4 Difference Between SOLAR-1 and BYLieve Trial Evaluating the Use of Alpelisib |
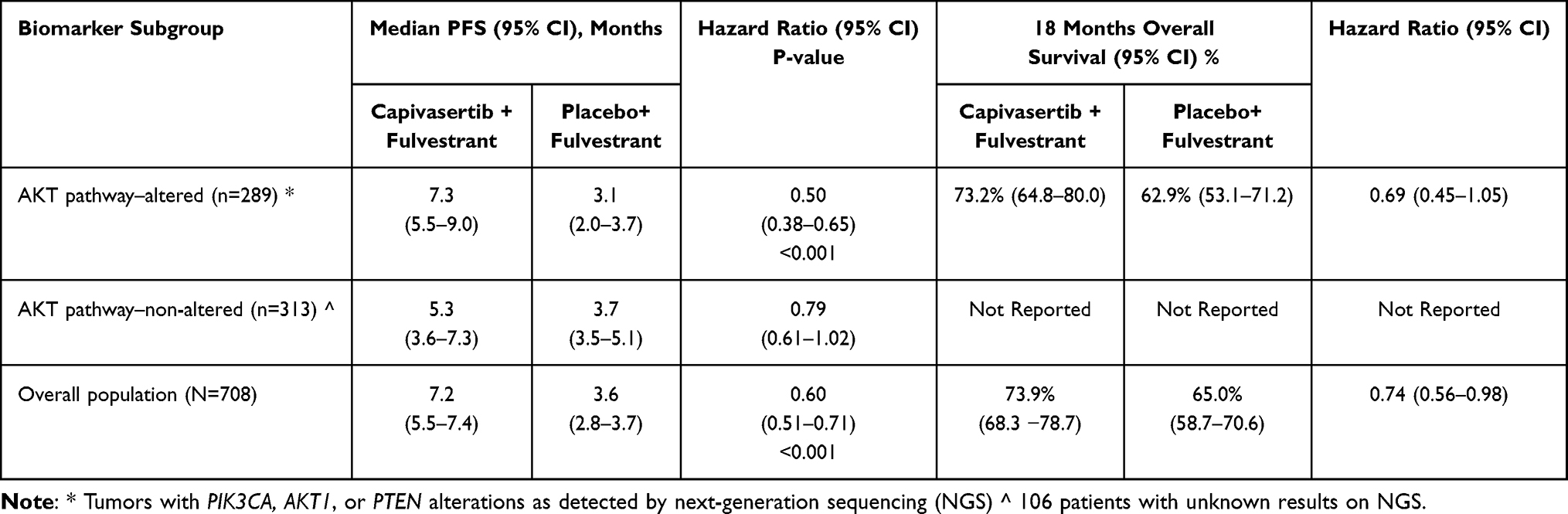 |
Table 5 CAPItello-291, Progression-Free Survival by PI3K/AKT Pathway Biomarker Status |
Amcenestrant (AMEERA-3 Trial)
The AMEERA-3 was a randomized, open-label Phase II trial that evaluated amcenestrant, another oral SERD, versus physician’s choice of standard ET (fulvestrant, AI, or tamoxifen) in patients with ER+, HER2-negative advanced breast cancer who had progressed after prior ET, including CDK4/6 inhibitors. The primary endpoint was PFS assessed by independent central review. In the overall population, amcenestrant did not significantly improve PFS compared with standard ET (median PFS 3.6 vs 3.7 months; HR 1.05). However, a numerical PFS advantage was observed in patients with ESR1-mutant tumors (3.7 vs 2.0 months; HR, 0.9) suggesting potential biological activity in this molecularly defined subgroup. The safety profile of amcenestrant was consistent with endocrine therapy and generally well tolerated. Although AMEERA-3 did not meet its primary endpoint, its results provided important insights into the role of oral SERDs and highlighted the need for biomarker-driven strategies in endocrine-resistant ER+ breast cancer.43
Targeting the PI3K Pathway
The phosphatidylinositol-3-kinase (PI3K)/AKT/mTOR pathway is one of the most frequently dysregulated signaling cascades in HR+, HER2-negative breast cancer, with activating PIK3CA mutations present in approximately 40% of tumors and strongly implicated in endocrine resistance.
The pivotal phase III SOLAR-1 trial evaluated the PI3Kα-selective inhibitor alpelisib in combination with fulvestrant in 572 patients with advanced HR+/HER2– MBC progressing on or after AI therapy, stratified by PIK3CA mutation status. In the PIK3CA-mutant cohort (n= 341), alpelisib significantly improved PFS compared with fulvestrant alone (11.0 vs 5.7 months; HR 0.65, p < 0.001), with higher objective response (26.6% vs 12.8%) and clinical benefit rates, whereas no benefit was observed in PIK3CA-wild-type tumors, confirming mutation-specific pathway dependence.44
Because few SOLAR-1 patients had prior CDK4/6 inhibitor exposure, the phase II BYLieve study specifically examined alpelisib plus fulvestrant in a real-world, post-CDK4/6 setting. In Cohort A (n = 121), which enrolled patients with PIK3CA-mutant tumors progressing on CDK4/6 inhibitor plus AIs, the combination achieved a 6-month PFS rate of 50.4% and a median PFS of 7.3 months, with an objective response rate of 17% and clinical benefit in 46%, confirming preserved PI3K pathway dependency after CDK4/6 inhibitor failure, Table 4.45 More recently, the phase III EPIK-B5 trial evaluated alpelisib plus fulvestrant in patients with PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer progressing after prior CDK4/6 inhibitor therapy. The study demonstrated a significant improvement in PFS with alpelisib–fulvestrant (7.4 months) compared with placebo–fulvestrant (2.8 months), HR: 0.52, 95% CI: 0.37,0.72, P<0.0001. These studies support continued targeting of the PI3K pathway in the post-CDK4/6 setting. However, the clinical utility of alpelisib is tempered by its toxicities, particularly hyperglycemia, rash, and diarrhea, necessitating careful metabolic screening, patient selection, and proactive toxicity management.46
Targeting AKT Signaling
AKT represents a key station in PI3K pathway signaling and provides an alternative target that may overcome some of the limitations of PI3K inhibition.
Capivasertib + Fulvestrant (CAPItello-291)
The phase III CAPItello-291 trial evaluated the addition of capivasertib, a selective AKT inhibitor, to fulvestrant compared with placebo plus fulvestrant in patients with HR+, HER2-negative advanced breast cancer who progressed during or after AI–based endocrine therapy, including a high proportion (69%) previously treated with CDK4/6 inhibitors. In this randomized, double-blind study of 708 patients, capivasertib plus fulvestrant produced a clinically meaningful and statistically significant improvement in PFS in the overall population, with a median PFS of 7.2 months versus 3.6 months for placebo plus fulvestrant (HR 0.60; 95% CI 0.51–0.71; P < 0.001), demonstrating nearly a 40% reduction in the risk of progression or death. In the prespecified AKT pathway–altered subgroup (defined by PIK3CA, AKT1, or PTEN alterations), the benefit was even more pronounced, with median PFS of 7.3 months versus 3.1 months (HR 0.50; 95% CI 0.38–0.65; P < 0.001), confirming that activation of the PI3K/AKT pathway confers enhanced sensitivity to AKT inhibition, Table 5.47 Importantly, benefit was observed across biomarker strata, including patients without documented alterations, although the magnitude was greatest in the altered cohort, positioning capivasertib as a broadly applicable targeted therapy in endocrine-resistant HR+ disease. The safety profile was consistent with AKT inhibition, with diarrhea, rash, and hyperglycemia among the most frequently reported toxicities, and adverse events leading to discontinuation occurring more often in the capivasertib arm. The median time to deterioration in quality of life as measured by QLQ-C30 score (defined as a sustained decrease of ≥10 points in the score from baseline) was 24.9 months in the capivasertib–fulvestrant group, as compared with 12.0 months in the placebo-fulvestrant group (HR, 0.70; 95% CI, 0.53–0.92). Based on these data, the combination has FDA approval in November 2023 for patients with AKT pathway alterations, with ongoing debates about its utility in unselected populations.48
Therapeutic Sequencing After Progression on Endocrine Therapy
The increasing availability of targeted endocrine therapies has transformed the post-progression landscape of HR+/HER2− advanced breast cancer from a linear sequence of treatments into a molecular-driven algorithm. Rather than viewing progression on endocrine therapy as endocrine failure, modern management emphasizes continued ER targeting combined with inhibition of resistance pathways, guided by molecular profiling. The optimal sequencing strategy depends primarily on prior therapies, ESR1 mutation status, PI3K/AKT pathway alterations, and clinical factors such as disease pace and patient comorbidities.49
First Progression After CDK4/6 Inhibitor-Based Therapy
For most patients, disease progression ultimately occurs after first-line therapy with an AI or fulvestrant combined with a CDK4/6 inhibitor. At this stage, ctDNA testing should be performed to identify actionable mutations. In patients with ESR1 mutations, AIs are no longer effective, and oral SERDs represent the preferred endocrine backbone. Elacestrant and imlunestrant are the only approved oral SERDs with phase III evidence in this setting. However, fulvestrant remains an option when oral SERDs are unavailable, though its efficacy is inferior in ESR1-mutant tumors. In the absence of ESR1 mutations, fulvestrant remains the standard endocrine partner for targeted therapy combinations.
Integration of PI3K and AKT Pathway Inhibitors
Patients with PIK3CA-mutant disease derive the greatest benefit from PI3K pathway inhibition. Alpelisib plus fulvestrant is appropriate when hyperglycemia and dermatologic adverse events can be managed. However, capivasertib plus fulvestrant is an attractive alternative, offering efficacy with improved tolerability and broader applicability.47
Later-Line Endocrine Strategies
After failure of SERDs and PI3K/AKT-directed therapy, additional endocrine-based combinations may still provide meaningful disease control. Everolimus plus exemestane remains a valid option, particularly in patients with indolent disease.50,51 Rechallenge with alternative endocrine backbones may be considered when chemotherapy is not yet indicated.
Transition to Chemotherapy
Chemotherapy should be reserved for patients with rapidly progressive disease, visceral crises or endocrine-refractory tumors. Multiple studies show that effective targeted endocrine therapy preserves quality of life and delays chemotherapy without compromising overall survival.52
Endocrine Therapy versus Chemotherapy After Endocrine Progression
Comparative Efficacy of Chemotherapy and Endocrine-Based Therapy
For decades, progression on endocrine therapy in HR+/HER2− metastatic breast cancer was viewed as a signal to switch to cytotoxic chemotherapy. However, recent data have challenged this concept as most patients retain endocrine sensitivity after progression, and that recently designed endocrine-based combinations can achieve disease control comparable to chemotherapy with substantially better tolerability and quality of life.53–56
Although direct randomized comparisons between targeted endocrine therapy and chemotherapy are limited, historical data indicate that single-agent chemotherapy in endocrine-resistant HR+ MBC typically produces median PFS of 3–5 months.57–59 In contrast, modern endocrine-based regimens such as capivasertib plus fulvestrant and elacestrant in biomarker-selected populations achieve similar or superior PFS with lower toxicity profile.51
Quality of Life and Toxicity Considerations
A key advantage of endocrine-based therapy is its favorable safety profile compared with chemotherapy. Cytotoxic regimens are associated with myelosuppression and infection risk, alopecia, neuropathy and fatigue; all of which negatively impact quality of life. In contrast, targeted endocrine combination therapy are generally manageable with dose modifications and supportive care.60,61
Analyses of patient-reported outcomes from trials of CDK4/6 inhibitors, SERDs, and AKT inhibitors consistently show better preservation of quality of life compared with chemotherapy, making prolonged endocrine-based treatment particularly important in this typically indolent disease.62,63
Clinical Implications
In the absence of visceral crisis or rapidly progressive disease, targeted endocrine therapy should remain the preferred treatment strategy after endocrine progression. Chemotherapy should be reserved for patients who have exhausted endocrine-based options or who require rapid tumor control due to life-threatening organ involvement. This approach maximizes disease control, minimizes toxicity, and aligns treatment with the biological reality that HR+/HER2− metastatic breast cancer remains fundamentally hormone driven even after multiple lines of therapy.64,65
Emerging Therapies
The rapid evolution of molecular understanding in HR+/HER2− advanced breast cancer has catalyzed the development of next-generation targeted and endocrine therapies with the purpose of prolonging endocrine sensitivity and overcoming resistance. Several innovative approaches have reshaped the treatment landscape beyond currently approved agents.
Next-Generation Oral SERDs
While imlunestrant and elacestrant validated oral SERDs as a therapeutic class, multiple next-generation drugs are in late-phase development with the goal of achieving greater activity against ESR1 mutations, deeper ER degradation, and better tolerability.66,67
Camizestrant
Camizestrant has demonstrated potent and deeper ER degradation and activity against ESR1-mutant tumors. In the phase II SERENA-2 trial, in patients previously treated with ET, camizestrant significantly improved PFS compared with fulvestrant with enhanced benefit observed in ESR1-mutant disease.68
The SERENA‑6 trial is randomized, double‑blind phase III landmark study designed to evaluate whether early switching from an AI to the next‑generation oral SERD camizestrant, upon detection of emergent ESR1 mutations in ctDNA, can extend clinical benefit over continued standard endocrine therapy in patients whose disease remains stable on first‑line AI plus CDK4/6 inhibitor therapy.
In this study, patients receiving first line AIs plus a CDK4/6 inhibitor underwent serial ctDNA monitoring; those found to have an emerging ESR1 mutation without radiographic progression were randomized to switch to camizestrant (75 mg once daily) with continued CDK4/6 inhibition versus continuing AI plus CDK4/6 inhibitor. At a median follow‑up of approximately 12.6 months, camizestrant significantly improved PFS, with a median PFS of 16.0 months (95% CI, 12.7–18.2), compared with 9.2 months (95% CI, 7.2–9.5) for the continued AI arm, (HR 0.44; 95% CI, 0.31–0.60; P < 0.0001). The benefit was consistent across subgroups and was reflected in PFS rates at 12 months (60.7% vs 33.4%) and at 24 months (29.7% vs 5.4%), underscoring the durability of disease control with camizestrant‑based therapy.69,70 Importantly, patient‑reported outcomes indicated a significant extension in quality of life, with the median time to deterioration in global health status delayed to 21–23 months versus 6.4 months in the AI arm with low discontinuation rates due to adverse events (1.3%).71 These outcomes support the notion that HR+/HER2− metastatic breast cancer can be more effectively managed with treatment adapted to evolving tumor biology rather than conventional imaging alone.
Giredestrant
Giredestrant, another SERD, has shown promising pharmacodynamic activity and clinical efficacy in multiple clinical settings. The lidERA adjuvant trial tested the use of giredestrant in patients with early-stage ER+/HER2-negative breast cancer. At the first prespecified analysis, giredestrant significantly improved invasive disease-free survival (iDFS) compared with standard-of-care endocrine therapy, reducing the risk of recurrence or death by approximately 30%, with favorable iDFS rates at 12, 24, and 36 months and trends toward better overall survival and distant recurrence-free interval. Safety was consistent with known profiles and discontinuation rates were modestly lower than standard endocrine treatment.72
In the advanced disease setting, updated phase III evERA demonstrated that giredestrant plus everolimus significantly improved PFS in patients with ER+/HER2-negative breast cancer previously treated with CDK4/6 inhibitors, including those with ESR1-mutated tumors. Overall survival data remain immature but suggest positive trends, and no new safety signals have emerged.73
Other ongoing phase III studies are evaluating giredestrant in combination with CDK4/6 inhibitors and also as monotherapy in early and resistant disease settings, seeking to define its role across lines of therapy and potentially position it as a new standard of care in ER-positive breast cancer.74,75
Estrogen Receptor Degraders Beyond SERDs: PROTACs and CERANs
Proteolysis-targeting chimeras (PROTACs) and complete estrogen receptor antagonists (CERANs) represent novel strategies to induce rapid and sustained ER degradation through the ubiquitin–proteasome system.76 These agents have demonstrated potent activity against both mutant and wild-type ER in early-phase clinical trials.77 By eliminating ER protein rather than merely inhibiting its activity, these compounds may overcome resistance even to current SERDs.
The Phase III VERITAC-2 trial of the oral PROTAC ER degrader vepdegestrant, compared daily oral vepdegestrant to intramuscular fulvestrant in adults with ER+/HER2-negative metastatic breast cancer post-CDK4/6 inhibitor and ET, with PFS as the primary. In this study, the ESR1-mutated subgroup achieved a significant PFS benefit (median 5.0 vs 2.1 months; HR 0.58, P<0.001) while the ITT analysis did not reach statistical significance, and OS data remain immature.78,79
Meanwhile, the OPERA-01 Phase III study of the oral CERAN/SERD palazestrant is designed as a randomized, open-label trial comparing palazestrant monotherapy to standard-of-care endocrine therapy (eg., fulvestrant or AI) in patients with ER+, HER2-negative locally advanced or metastatic breast cancer after progression on at least one CDK4/6 inhibitor plus ET, with PFS as its primary endpoint and OS, duration of response, safety, and patient-reported outcomes as secondary endpoints.80
ctDNA-Guided Adaptive Endocrine Therapy
The use of ctDNA to guide proactive treatment plans is perhaps the most transformative future direction. Trials such as SERENA-6 and PADA-1 demonstrated that switching endocrine therapy at the time of molecular progression, before radiographic progression, can significantly extend disease control. This innovative adaptive approach may allow continuous suppression of evolving resistant clones, effectively converting metastatic breast cancer into a chronically managed disease.
Conclusions and Future Directions
The management of HR-positive, HER2-negative advanced breast cancer following progression on endocrine therapy has fundamentally evolved significantly in recent years. Disease progression is now considered a biologically adaptive and therapeutically targetable process, with most tumors retaining estrogen dependence despite prior CDK4/6 inhibition and endocrine therapy. The introduction of mTOR-targeted therapies, oral SERDs, PI3K and AKT inhibitors has extended endocrine sensitivity and delayed the need for more aggressive chemotherapy. The integration of ctDNA enables real-time detection of resistance mechanisms and supports biomarker-guided treatment adaptation.
Together, these advances move endocrine-based precision therapy to the center of post-progression breast cancer management, offering preserved quality of life with durable disease control, while underscoring the importance of aligning economic sustainability with clinical innovation. This approach represents the preferred pathway specifically for patients with retained endocrine sensitivity, whereas those with endocrine-refractory disease generally require treatment with antibody-drug conjugates (ADCs) or chemotherapy.
Funding
This manuscript did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors. However, Article Publication Charges (APC) fees will be paid by the Office of Scientific Affair and Research (OSAR) at King Hussein Cancer Center.
Disclosure
The author has no relevant financial or non-financial interests to disclose.
References
1. Huppert LA, Gumusay O, Idossa D, Rugo HS. Systemic therapy for hormone receptor-positive/human epidermal growth factor receptor 2-negative early stage and metastatic breast cancer. CA Cancer J Clin. 2023;73(5):480–13.PMID:36939293. doi:10.3322/caac.21777
2. Burstein HJ. Systemic therapy for estrogen receptor-positive, HER2-negative breast cancer. N Engl J Med. 2020;383(26):2557–2570.PMID:33369357. doi:10.1056/NEJMra1307118
3. O’Sullivan CC, Clarke R, Goetz MP, Robertson J. Cyclin-dependent kinase 4/6 inhibitors for treatment of hormone receptor-positive, ERBB2-negative breast cancer: a review. JAMA Oncol. 2023;9(9):1273–1282.PMID:37382948; PMCID: PMC11385778. doi:10.1001/jamaoncol.2023.2000
4. Tripathy D, Im SA, Colleoni M, et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised Phase 3 trial. Lancet Oncol. 2018;19(7):904–915.PMID:29804902. doi:10.1016/S1470-2045(18)30292-4
5. Hortobagyi GN, Stemmer SM, Burris HA, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016;375(18):1738–1748.PMID:27717303. doi:10.1056/NEJMoa1609709
6. Neven P, Fasching PA, Chia S, et al. Updated overall survival from the MONALEESA-3 trial in postmenopausal women with HR+/HER2- advanced breast cancer receiving first-line ribociclib plus fulvestrant. Breast Cancer Res. 2023;25(1):103. doi:10.1186/s13058-023-01701-9
7. Finn RS, Martin M, Rugo HS, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375(20):1925–1936.PMID:27959613. doi:10.1056/NEJMoa1607303
8. Goetz MP, Toi M, Campone M, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J Clin Oncol. 2017;35(32):3638–3646.PMID:28968163. doi:10.1200/JCO.2017.75.6155
9. Saatci O, Huynh-Dam KT, Sahin O. Endocrine resistance in breast cancer: from molecular mechanisms to therapeutic strategies. J Mol Med. 2021;99(12):1691–1710.PMID:34623477; PMCID:PMC8611518. doi:10.1007/s00109-021-02136-5
10. Betz M, Massard V, Gilson P, et al. ESR1 gene mutations and liquid biopsy in ER-positive breast cancers: a small step forward, a giant leap for personalization of endocrine therapy? Cancers. 2023;15(21):5169.PMID:37958343; PMCID:PMC10649433. doi:10.3390/cancers15215169
11. Zhang J, Wang Q, Wang Q, Cao J, Sun J, Zhu Z. Mechanisms of resistance to estrogen receptor modulators in ER+/HER2- advanced breast cancer. Cell Mol Life Sci. 2020;77(4):559–572.PMID:31471681; PMCID:PMC11105043. doi:10.1007/s00018-019-03281-4
12. Burstein HJ, Somerfield MR, Barton DL, et al. Endocrine treatment and targeted therapy for hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer: ASCO guideline update. J Clin Oncol. 2021;39(35):3959–3977.PMID:34324367; PMCID:PMC8659999. doi:10.1200/JCO.21.01392
13. Childs S, Semba R, Haggstrom L, Lim E. Integrating molecular phenotyping into treatment algorithms for advanced oestrogen receptor-positive breast cancer. Cancers. 2025;17(19):3174.PMID:41097702; PMCID:PMC12523997. doi:10.3390/cancers17193174
14. Shatsky R, Parker BA, Bui NQ, et al. Next-generation sequencing of tissue and circulating tumor DNA: the UCSanDiego moores center for personalized cancer therapy experience with breast malignancies. Mol Cancer Ther. 2019;18:1001–1011. doi:10.1158/1535-7163.MCT-17-1038
15. Razavi P, Chang MT, Xu G, et al. The genomic landscape of endocrine-resistant advanced breast cancers. Cancer Cell. 2018;34(3):427–438.e6.PMID:30205045; PMCID:PMC6327853. doi:10.1016/j.ccell.2018.08.008
16. Jeselsohn R, Buchwalter G, De Angelis C, Brown M, Schiff R. ESR1 mutations—a mechanism for acquired endocrine resistance in breast cancer. Nat Rev Clin Oncol. 2015;12(10):573–583.PMID:26122181; PMCID:PMC4911210. doi:10.1038/nrclinonc.2015.117
17. de Pinho IS, Abreu C, Gomes I, et al. Exploring new pathways in endocrine-resistant breast cancer. Explor Target Antitumor Ther. 2022;3(3):337–361.PMID:36045911; PMCID:PMC9400750. doi:10.37349/etat.2022.00086
18. Chandarlapaty S, Chen D, He W, et al. Prevalence of ESR1 mutations in cell-free DNA and outcomes in metastatic breast cancer: a secondary analysis of the BOLERO-2 clinical trial. JAMA Oncol. 2016;2(10):1310–1315.PMID:27532364; PMCID:PMC5063698. doi:10.1001/jamaoncol.2016.1279
19. Bardia A, Kaklamani V, Wilks S, et al. Phase I study of elacestrant (RAD1901), a novel selective estrogen receptor degrader, in ER-positive, HER2-negative advanced breast cancer. J Clin Oncol. 2021;39(12):1360–1370.PMID:33513026; PMCID:PMC8078341. doi:10.1200/JCO.20.02272
20. Yu L, Wei J, Liu P. Attacking the PI3K/Akt/mTOR signaling pathway for targeted therapeutic treatment in human cancer. Semin Cancer Biol. 2022;85:69–94.PMID:34175443. doi:10.1016/j.semcancer.2021.06.019
21. Glaviano A, Foo ASC, Lam HY, et al. PI3K/AKT/mTOR signaling transduction pathway and targeted therapies in cancer. Mol Cancer. 2023;22(1):138.PMID:37495903; PMCID:PMC10394894. doi:10.1186/s12943-023-01827-6
22. Ogata R, Kishino E, Saitoh W, et al. Resistance to cyclin-dependent kinase (CDK) 4/6 inhibitors confers cross-resistance to other CDK inhibitors but not to chemotherapeutic agents in breast cancer cells. Breast Cancer. 2021;28(2):206–215.PMID:32621815. doi:10.1007/s12282-020-01150-8
23. Xi J, Ma CX. Sequencing endocrine therapy for metastatic breast cancer: what do we do after disease progression on a CDK4/6 inhibitor? Curr Oncol Rep. 2020;22(7):57.PMID:32691068. doi:10.1007/s11912-020-00917-8
24. Le Saux O, Lardy-Cleaud A, Frank S, et al. Assessment of the efficacy of successive endocrine therapies in hormone receptor-positive and HER2-negative metastatic breast cancer: a real-life multicentre national study. Eur J Cancer. 2019;118:131–141. doi:10.1016/j.ejca.2019.06.014
25. Pogoda K, Pawlik H, Balata A, et al. Management Strategies and Outcomes in HR+/HER2- Metastatic Breast Cancer Receiving CDK4/6 Inhibitors and Subsequent Therapies. Breast Cancer. 2025:1307–1319.PMID: 41466771. doi:10.2147/BCTT.S567687
26. Álvarez-Fernández M, Malumbres M. Mechanisms of Sensitivity and Resistance to CDK4/6 Inhibition. Cancer Cell. 2020;37(4):514–529. doi:10.1016/j.ccell.2020.03.010
27. Wander SA, Cohen O, Gong X, et al. The genomic landscape of intrinsic and acquired resistance to cyclin-dependent kinase 4/6 inhibitors in patients with hormone receptor-positive metastatic breast cancer. Cancer Discov. 2020;10(8):1174–1193. doi:10.1158/2159-8290.CD-19-1390
28. Condorelli R, Spring L, O’Shaughnessy J, et al. Polyclonal RB1 mutations and acquired resistance to CDK 4/6 inhibitors in patients with metastatic breast cancer. Ann Oncol. 2018;29(3):640–645. doi:10.1093/annonc/mdx784
29. Lloyd MR, Spring LM, Bardia A, Wander SA. Mechanisms of resistance to cdk4/6 blockade in advanced hormone receptor-positive, her2-negative breast cancer and emerging therapeutic opportunities. Clin Cancer Res. 2022;28(5):821–830. doi:10.1158/1078-0432.CCR-21-2947
30. O’Leary B, Finn RS, Turner NC. Treating cancer with selective CDK4/6 inhibitors. Nat Rev Clin Oncol. 2016;13(7):417–430.PMID:26907292. doi:10.1038/nrclinonc.2016.26
31. Sharifi MN, Anandan A, Grogan P, O’Regan RM. Therapy after cyclin-dependent kinase inhibition in metastatic hormone receptor-positive breast cancer: resistance mechanisms and novel treatment strategies. Cancer. 2020;126(15):3400–3416.PMID: 32426848. doi:10.1002/cncr.32931
32. Buonaiuto R, Fordellone M, Caltavituro A, et al. Efficacy and safety of systemic therapies following progression on CDK4/6 inhibitors in patients with HR+/HER2- metastatic breast cancer: a systematic review and network meta-analysis. EClinicalMedicine. 2025;89:103535. doi:10.1016/j.eclinm.2025.103535
33. De Santis P, Sanna V, Perrone M, et al. Antibody-drug conjugates in hr+ breast cancer: where are we now and where are we heading? J Clin Med. 2023;12(23):7325. doi:10.3390/jcm12237325
34. Ma J, Chan JJ, Toh CH, Yap YS. Emerging systemic therapy options beyond CDK4/6 inhibitors for hormone receptor-positive HER2-negative advanced breast cancer. NPJ Breast Cancer. 2023;9(1):74. doi:10.1038/s41523-023-00578-3
35. Dickinson K, Sharma A, Agnihotram RV, et al. Circulating tumor DNA and survival in metastatic breast cancer: a systematic review and meta-analysis. JAMA Network Open. 2024;7(3):e2431722.PMID:38976254. doi:10.1001/jamanetworkopen.2024.31722
36. Bidard FC, Hardy-Bessard AC, Dalenc F, et al. Switch to fulvestrant and palbociclib versus no switch in advanced breast cancer with rising ESR1 mutation during aromatase inhibitor and palbociclib therapy (PADA-1): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2022;23(9):1367–1377.PMID:35869350; PMCID:PMC9400221. doi:10.1016/S1470-2045(22)00555-1
37. Bidard FC, Kaklamani VG, Neven P, et al. Elacestrant versus standard endocrine therapy for estrogen receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: results from the randomized phase III EMERALD trial. J Clin Oncol. 2022;40(35):3246–3256.PMID:36133072. doi:10.1200/JCO.22.00338
38. Bardia A, Cortés J, Bidard FC, et al. Elacestrant in ER+, HER2− metastatic breast cancer with ESR1-mutated tumors: subgroup analyses from the phase III EMERALD trial. Clin Cancer Res. 2024;30(12):4299–4309. doi:10.1158/1078-0432.CCR-24-1073
39. Shah M, Lingam H, Gao X, et al. US Food and Drug Administration approval summary: elacestrant for estrogen receptor-positive, human epidermal growth factor receptor 2-negative, ESR1-mutated advanced or metastatic breast cancer. J Clin Oncol. 2024;42(10):1193–1201. doi:10.1200/JCO.23.02112
40. Jhaveri KL, Lim E, Jeselsohn R, et al. Imlunestrant, an oral selective estrogen receptor degrader, as monotherapy and in combination with targeted therapy in estrogen receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: phase Ia/Ib EMBER study. J Clin Oncol. 2024;42(19):4173–4186. doi:10.1200/JCO.23.02733
41. Jhaveri KL, Neven P, Casalnuovo ML, et al. Imlunestrant with or without abemaciclib in advanced breast cancer. N Engl J Med. 2025;392:1189–1202. doi:10.1056/NEJMoa2410858
42. Jhaveri KL, Neven P, Casalnuovo ML, et al. Imlunestrant with or without abemaciclib in advanced breast cancer: updated efficacy results from the phase 3 EMBER-3 trial. Ann Oncol. 2025;36. doi:10.1016/j.annonc.2025.11.018
43. Tolaney SM, Chan A, Petrakova K, et al. AMEERA-3: randomized phase II study of amcenestrant versus standard endocrine monotherapy in estrogen receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer. J Clin Oncol. 2023;41(34):4014–4024. doi:10.1200/JCO.22.02746
44. André F, Ciruelos E, Rubovszky G, et al. Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced breast cancer. N Engl J Med. 2019;380(21):1929–1940.PMID:30861129. doi:10.1056/NEJMoa1813904
45. Rugo HS, Lerebours F, Ciruelos E, et al. Alpelisib plus fulvestrant in PIK3CA-mutated, hormone receptor-positive advanced breast cancer after a CDK4/6 inhibitor (BYLieve): one cohort of a Phase 2, multicentre, open-label, non-comparative study. Lancet Oncol. 2021;22(4):489–498.PMID:33510835. doi:10.1016/S1470-2045(21)00034-6
46. De Laurentiis M, Ferreira AM, Gligorov J, et al. Alpelisib plus fulvestrant for PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer after a CDK4/6 inhibitor (EPIK-B5): phase III, randomized, double-blind, placebo-controlled, multicenter study [abstract]. In: proceedings of the San Antonio Breast Cancer Symposium 2025; 2025 Dec 9-12; San Antonio, TX. Philadelphia (PA). 2026;32(4 Suppl).
47. Turner NC, Oliveira M, Howell SJ, et al. Capivasertib in hormone receptor-positive advanced breast cancer. N Engl J Med. 2023;388:2058–2070. doi:10.1056/NEJMoa2214131
48. Dilawari A, Buturla J, Osgood C, et al. US Food and Drug Administration approval summary: capivasertib with fulvestrant for hormone receptor-positive, human epidermal growth factor receptor 2-negative locally advanced or metastatic breast cancer with PIK3CA/AKT1/PTEN alterations. J Clin Oncol. 2024;42:4103–4113. doi:10.1200/JCO.24.00427
49. Chan JCH, Chow JCH, CHM H, et al. Clinical application of circulating tumor DNA in breast cancer. J Cancer Res Clin Oncol. 2021;147:1431–1442. doi:10.1007/s00432-021-03588-5
50. Dhillon S. Everolimus in combination with exemestane: a review of its use in postmenopausal hormone receptor-positive, HER2-negative advanced breast cancer. Drugs. 2013;73:475–485. doi:10.1007/s40265-013-0034-2
51. Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med. 2012;366:520–529. doi:10.1056/NEJMoa1109653
52. Cardoso F, Paluch-Shimon S, Schumacher-Wulf E, et al. 6th and 7th international consensus guidelines for the management of advanced breast cancer (ABC guidelines 6 and 7). Breast. 2024;76:103756. doi:10.1016/j.breast.2024.103756
53. Corbaux P, Lardy-Cleaud A, Alexandre M, et al. Progression-free survival on endocrine therapy, before or after chemotherapy, in hormone receptor-positive HER2-negative metastatic breast cancer. Breast Cancer Res Treat. 2022;191:191–207. doi:10.1007/s10549-021-06382-6
54. Liu Q, Qiu J, Lu Q, et al. Comparison of endocrine therapy and chemotherapy as different systemic treatment modes for metastatic luminal HER2-negative breast cancer patients: a retrospective study. Front Oncol. 2022;12:873570. doi:10.3389/fonc.2022.873570
55. Jacquet E, Lardy-Cléaud A, Pistilli B, et al. Endocrine therapy or chemotherapy as first-line therapy in hormone receptor-positive HER2-negative metastatic breast cancer patients. Eur J Cancer. 2018;95:93–101. doi:10.1016/j.ejca.2018.03.013
56. Werutsky G, Reinert T, Rosa ML, Barrios CH. Real-world data on first-line systemic therapy for hormone receptor-positive HER2-negative metastatic breast cancer: a trend shift in the era of CDK 4/6 inhibitors. Clin Breast Cancer. 2021;21:e688–e692. doi:10.1016/j.clbc.2021.04.003
57. Chainitikun S, Long JP, Rodriguez-Bautista R, et al. The efficacy of first-line chemotherapy in endocrine-resistant hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer. Breast Cancer Res Treat. 2020;183:729–739. doi:10.1007/s10549-020-05837-6
58. Bender L, Pflumio C, Trensz P, et al. Capecitabine efficacy after cyclin-dependent-kinase 4/6 inhibitor plus endocrine therapy in metastatic hormone receptor-positive breast cancer. Cancer Treat Res Commun. 2023;36:100738. doi:10.1016/j.ctarc.2023.100738
59. Choong GM, Liddell S, Ferre RAL, et al. Clinical management of metastatic hormone receptor-positive, HER2-negative breast cancer after CDK4/6 inhibitors: a retrospective single-institution study. Breast Cancer Res Treat. 2022;196:229–237. doi:10.1007/s10549-022-06713-1
60. Kahan Z, Gil-Gil M, Ruiz-Borrego M, et al. Health-related quality of life with palbociclib plus endocrine therapy versus capecitabine in postmenopausal patients with hormone receptor-positive metastatic breast cancer: patient-reported outcomes in the PEARL study. Eur J Cancer. 2021;156:70–82. doi:10.1016/j.ejca.2021.07.004
61. Oliveira M, Rugo HS, Howell SJ, et al. Capivasertib and fulvestrant for patients with hormone receptor-positive, HER2-negative advanced breast cancer (CAPItello-291): patient-reported outcomes from a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2024;25:1231–1244. doi:10.1016/S1470-2045(24)00373-5
62. Di Lauro V, Barchiesi G, Martorana F, et al. Health-related quality of life in breast cancer patients treated with CDK4/6 inhibitors: a systematic review. ESMO Open. 2022;7:100629. doi:10.1016/j.esmoop.2022.100629
63. Freedman RA, Tolaney SM. Efficacy and safety in older patient subsets in studies of endocrine monotherapy versus combination therapy in patients with HR+/HER2− advanced breast cancer: a review. Breast Cancer Res Treat. 2018;167:607–614. doi:10.1007/s10549-017-4560-6
64. Goldschmidt D, Dalal AA, Romdhani H, et al. Current treatment patterns among postmenopausal women with HR+/HER2− metastatic breast cancer in US community oncology practices: an observational study. Adv Ther. 2018;35:482–493. doi:10.1007/s12325-018-0676-2
65. Moy B, Rumble RB, Come SE, et al. Chemotherapy and targeted therapy for patients with human epidermal growth factor receptor 2-negative metastatic breast cancer that is either endocrine-pretreated or hormone receptor-negative: ASCO guideline update. J Clin Oncol. 2021;39:3938–3958. doi:10.1200/JCO.21.01374
66. Rej RK, Thomas JE 2nd, Acharyya RK, Rae JM, Wang S. Targeting the estrogen receptor for the treatment of breast cancer: recent advances and challenges. J Med Chem. 2023;66:8339–8381. doi:10.1021/acs.jmedchem.3c00136
67. Pagliuca M, Donato M, D’Amato AL, et al. Novel endocrine-based therapies in metastatic breast cancer: selective estrogen receptor degraders and proteolysis-targeting chimeras. Drugs. 2024;84:213–232. doi:10.1007/s40265-024-01998-0
68. Curigliano G. The role of CDK4/6 inhibitors in the treatment of hormone receptor-positive advanced breast cancer: focus on patient-reported outcomes. Ther Adv Med Oncol. 2020;12:1758835920933871. doi:10.1177/1758835920933871
69. Cardoso F, Kyriakides S, Ohno S, et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann Oncol. 2020;31:1623–1649. doi:10.1016/j.annonc.2020.09.010
70. Bidard FC, Mayer EL, Park YH, et al. First-line camizestrant for emerging ESR1 -mutated advanced breast cancer. N Engl J Med. 2025;393(6):569–580. doi:10.1056/NEJMoa2502929
71. Jacob L, Klein J, Kostev K. Treatment patterns in metastatic breast cancer: a retrospective analysis of real-world data. Breast. 2022;62:79–85. doi:10.1016/j.breast.2022.01.005
72. Bardia A, Schmid P, Martín M, et al. Selective estrogen degrader giredestrant (GDC-9545) vs standard-of-care endocrine therapy in patients with ER-positive, HER2-negative early breast cancer: results from the Phase III lidERA Breast Cancer trial (NCT04961996). In:
73. Rugo HS, Tolaney SM, Jhaveri KL, et al. Clinical and biomarker subgroup analysis from the phase III evERA Breast Cancer trial (NCT05306340): giredestrant plus everolimus vs standard-of-care endocrine therapy plus everolimus in ER-positive advanced breast cancer after CDK4/6 inhibitor therapy. In:
74. Liang J, Zbieg JR, Blake RA, et al. A potent and orally bioavailable selective estrogen receptor antagonist and degrader with an exceptional preclinical profile for ER+ breast cancer. J Med Chem. 2021;64(16):11841–11856. doi: 10.1021/acs.jmedchem.1c00847
75. A Phase III, Randomized, Open-label study evaluating efficacy and safety of giredestrant compared with fulvestrant, both combined with a CDK4/6 inhibitor, in patients with ER-positive, HER2-negative advanced breast cancer resistant to prior adjuvant endocrine therapy (pionERA breast cancer). ClinicalTrials.gov. NCT06065748. Available from: https://clinicaltrials.gov/study/NCT06065748.
76. Min J, Liu X, Peng R, Chen CC, Wang W, Guo RT. New generation estrogen receptor-targeted agents in breast cancer: present situation and future prospectives. Acta Mater Med. 2024;3(1):57–71. doi: 10.15212/amm-2024-0006
77. Flanagan JJ, Neklesa TK. Targeting nuclear receptors with PROTAC degraders. Mol Cell Endocrinol. 2019; 493:110452. doi: 10.1016/j.mce.2019.110452
78. Hamilton EP, Ma C, De Laurentiis M, et al. (VERITAC-2): a Phase III study of vepdegestrant, a PROTAC ER degrader, versus fulvestrant in ER+/HER2- advanced breast cancer. Future Oncol. 2024;20(32):2447–2455. doi: 10.1080/14796694.2024.2377530
79. Campone M, De Laurentiis M, Jhaveri K, et al; Patsouris A (VERITAC-2 Study Group). Vepdegestrant, a PROTAC estrogen receptor degrader, in advanced breast cancer. N Engl J Med. 2025;393(6):556–568. doi: 10.1056/NEJMoa2505725
80. Pistilli B, Bellet Ezquerra M, Del mastro L, et al. OPERA-01: a phase III study of palazestrant for ER+, HER2- advanced breast cancer after CDK4/6 inhibitor therapy. Future Oncol. 2025:1–10. doi: 10.1080/14796694.2025.2608863
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Differences in Treatment Outcomes Between Patients with HER2-Low versus HER2-Zero, Hormone Receptor-Positive Advanced-Stage Breast Cancer Treated with Ribociclib
Sharaf B, Abu-Fares H, Tamimi F, Al-Sawajneh S, Salama O, Daoud R, Alhajahjeh A, Al-Lababidi S, Abdel-Razeq H
Breast Cancer: Targets and Therapy 2023, 15:541-548
Published Date: 28 July 2023
Clinical Outcomes of Patients Treated with Ribociclib in Combination with Aromatase Inhibitors or Fulvestrant for HR-Positive, HER2-Negative Metastatic Breast Cancer, Real-World Data from a Low-Resourced Country
Abdel-Razeq H, Sharaf B, Khater S, Baidoun HJ, Bani Hani H, Taqash A, El Khatib O, Edaily S, Abunasser M, Tamimi F, Al-Masri YN, Al-Batsh TMW, Zayed A, Ghatasheh T, Radaideh T
ImmunoTargets and Therapy 2024, 13:501-512
Published Date: 29 September 2024
Management Strategies and Outcomes in HR+/HER2− Metastatic Breast Cancer Receiving CDK4/6 Inhibitors and Subsequent Therapies
Pogoda K, Pawlik H, Balata A, Czopowicz M, Bak A, Twardowska I, Meluch M, Wojda M, Mlodzinska A, Szombara E, Sienkiewicz R, Konieczna A, Brewczynska E, Lemanska I, Majstrak-Hulewska A, Gorniak A, Niwinska A, Nowecki Z
Breast Cancer: Targets and Therapy 2025, 17:1307-1319
Published Date: 24 December 2025
Endocrine Therapy versus Chemotherapy After CDK4/6 Inhibitor Progression in HR+/HER2- Metastatic Breast Cancer: A Multicenter Real-World Study from Turkey
Cangür C, Bülbül B, Yeğen IT, Ucun B, Eren Oö, Başaran H, Erdoğan AP, Şahin Hafızoğlu E, Gökmen E, Özkan O, Araz M, Oruç A, Yilmaz C, Gül G, Yildirim S
Breast Cancer: Targets and Therapy 2026, 18:571246
Published Date: 14 January 2026