Back to Journals » Journal of Inflammation Research » Volume 19
Elevated Systemic Immune-Inflammation Index is Associated with Gestational Diabetes Mellitus: A Multicenter Retrospective Studies
Authors Li J, Li Q ![]() , Zhang Y
, Zhang Y ![]() , Chen X, Zhang C, Chen Y, Gu Y, Yue C
, Chen X, Zhang C, Chen Y, Gu Y, Yue C
Received 19 June 2025
Accepted for publication 27 January 2026
Published 5 February 2026 Volume 2026:19 548249
DOI https://doi.org/10.2147/JIR.S548249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Quan Zhang
Jingyang Li,1,* Qiong Li,2,* Yixuan Zhang,1 Xiaohu Chen,3 Chunyi Zhang,3 Yu Chen,1 Ying Gu,1 Chaoyan Yue3
1Department of Obstetrics, Wuxi Maternity and Child Health Hospital, Jiangnan University, Wuxi, People’s Republic of China; 2Department of Obstetrics and Gynecology, The First People’s Hospital of Chenzhou, Chenzhou, People’s Republic of China; 3Obstetrics & Gynecology Hospital of Fudan University, Shanghai Key Lab of Reproduction and Development, Shanghai Key Lab of Female Reproductive Endocrine Related Diseases, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chaoyan Yue, Obstetrics & Gynecology Hospital of Fudan University, Shanghai Key Laboratory of Reproduction and Development, Shanghai Key Laboratory of Female Reproductive Endocrine Related Diseases, Fang Xie Road, No. 419, Shanghai, People’s Republic of China, Email [email protected] Ying Gu, Department of Obstetrics, Wuxi Maternity and Child Health Hospital, Jiangnan University, No. 48, Huai Shu Lane, Wuxi, 214000, People’s Republic of China, Email [email protected]
Background: The systemic immune-inflammation index (SII), an integrative biomarker reflecting inflammatory and immune status, has been implicated in metabolic disorders. However, its association with gestational diabetes mellitus (GDM) remains unclear. This study aimed to investigate whether elevated SII is associated with an increased risk of GDM.
Objective: We aimed to clarify whether systemic SII is related to the occurrence of GDM and the relationship between changes in SII and adverse pregnancy outcomes associated with GDM.
Methods: This study analyzed 47,480 singleton pregnancies between 2018 and 2024, including 6599 GDM cases and 40,881 controls. SII was calculated before 24 weeks of gestation, and participants were categorized by SII quartiles. Multivariable logistic regression was used to assess associations between SII and GDM (primary outcome), insulin-requiring GDM (A2), preeclampsia, and large-for-gestational-age infants. In addition, interaction tests and smooth curve fitting methods were adopted to explore the relationship between SII and gestational diabetes mellitus (GDM) and related adverse pregnancy outcomes.
Results: After adjustment, higher SII quartiles showed a dose-dependent increase in GDM risk: Q2 (aOR = 1.19, 95% CI: 1.08– 1.30), Q3 (aOR = 1.26, 1.15– 1.38), Q4 (aOR = 1.56, 1.43– 1.71; P < 0.0001). Stronger associations were observed for GDM A2 and GDM with preeclampsia. The association with LGA was weaker and only significant in Q3. Subgroup analyses revealed consistent associations across age and BMI, though the effect was marginally stronger in multiparous women (interaction P=0.0213< 0.05). No significant interactions were found for BMI or age.
Conclusion: Elevated SII in early pregnancy is independently associated with an increased risk of GDM, supporting its potential utility as an early predictive marker for GDM screening.
Keywords: systemic immune-inflammation index, gestational diabetes mellitus, insulin resistance, retrospective studies
Introduction
Gestational diabetes mellitus (GDM) is one of the most common metabolic complications of pregnancy, affecting 5–20% of pregnancies worldwide, with significant variations across ethnicities and diagnostic criteria.1–3 It is characterized by glucose intolerance first recognized during pregnancy and is associated with adverse maternal and fetal outcomes, including preeclampsia, cesarean delivery, macrosomia, neonatal hypoglycemia, and long-term risks of type 2 diabetes for both mother and offspring.4–7 Globally, increasing maternal age and rising obesity rates among pregnant women have been observed in many countries. Such as in China, where family planning policies have evolved and living standards have improved, there has been a notable increase in maternal age and obesity rates among pregnant women. This worldwide trend makes the early identification of high-risk women crucial for timely intervention.8,9 The pathophysiology of GDM involves insulin resistance exacerbated by placental hormones, but growing evidence suggests that chronic low-grade inflammation plays a key role.10–12 During normal pregnancy, a controlled inflammatory response supports placental development; however, excessive activation of pro-inflammatory cytokines (eg, TNF-α, IL-6)13,14 and immune cells may contribute to β-cell dysfunction and insulin resistance.10,15,16 Recent studies highlight the involvement of neutrophils, lymphocytes, and platelets in this inflammatory cascade, yet a reliable, easily measurable biomarker to assess systemic inflammation in early pregnancy remains elusive.17–19
The Systemic Immune Inflammation Index (SII) is a complex biomarker that integrates three key immune cell types to assess the systemic inflammatory status.17,18,20 The SII is a composite index calculated based on complete blood count parameters using the formula: SII = platelet count × neutrophil count / lymphocyte count. In 2014, Hu et al21 initially proposed SII as an oncology prognostic tool.20,22,23 SII has demonstrated its clinical value beyond oncology. Through its unique ability to simultaneously assess inflammatory and thrombotic activities, it has shown predictive potential for cardiovascular and metabolic diseases.24,25 In obstetric studies, elevated SII levels are associated with adverse pregnancy outcomes including preterm birth and preeclampsia.26–28 However, its relationship with GDM remains controversial. It is worth noting that a recent retrospective study29 and a prospective cohort study30 both showed no significant correlation between SII levels and the development of GDM, suggesting that this potential relationship may need to be verified through larger-scale population studies. At present, most studies have focused on the research of SII levels in the middle and late stages of pregnancy (after 20 weeks of gestation), while the SII levels in the early stage of pregnancy have still not been fully studied17,31. Moreover, the existing GDM screening completely relies on the oral glucose tolerance test (OGTT) conducted at 24–28 weeks of gestation,32,33 resulting in the unmet demand for early risk stratification tools. Although inflammatory markers such as C-reactive protein (CRP) and white blood cell count have been studied for predicting GDM, their clinical application specificity is insufficient.34–36 The SII, as a comprehensive index, may offer superior predictive value by reflecting broader immune dysregulation. This study aims to fill these evidence gaps and further clarify the role of SII in the pathogenesis of GDM.
This study conducted a retrospective studies using this large-scale, multicenter clinical data to explore the relationship between the risk of SII and GDM in the early stage of pregnancy. After adjusting for relevant confounding factors, multivariate logistic regression analysis was used to evaluate the efficacy of SII in predicting the risk of GDM. Furthermore, after stratifying age, BMI and parity, we conducted subgroup analyses to evaluate whether these variables changed the association between SII and GDM. Furthermore, we employed interaction analyses and nonparametric smoothing techniques to comprehensively examine the association between SII and GDM risk, along with its potential impact on pregnancy complications. This study provides a new perspective for GDM prediction by utilizing the SII—measured before the 24th week of gestation—as a continuous and categorical variable to evaluate its relationship with GDM, an approach that differs from prior studies. Meanwhile, our research results may provide clinicians with a practical inflammatory marker in the early stage of pregnancy to identify high-risk women, thereby enabling timely intervention, such as strengthening blood glucose monitoring, changing lifestyles or adopting anti-inflammatory strategies, to alleviate GDM and its related complications. Furthermore, our research demonstrates that SII levels in early to mid-pregnancy can predict the later development of GDM. This identifies a crucial early time window for risk stratification and intervention, addressing the gap of lacking effective inflammatory markers for early prediction in pregnancy.
Materials and Methods
Design and Participants
This study adopted a multicenter retrospective cohort design, enrolling pregnant women who underwent prenatal examinations and participated in the cohort study at the Obstetrics and Gynecology Hospital of Fudan University, Wuxi Maternal and Child Health Hospital, and Chenzhou First People’s Hospital between February 2018 and April 2024. The inclusion criteria for pregnant women in this study are as follows: (1) singleton pregnancy; (2) maternal age ≥18 years; (3) no pre-existing diabetes and fasting blood glucose (FBG) <7 mmol/L at the first prenatal visit; (4) the gestational weeks of the pregnancies we included were 11.59 ± 3.98; (5) no history of cold or fever during early pregnancy; (6) no underlying diseases, such as hypertension, immune system disorders, or urinary system diseases; (7) no infectious diseases; (8) no use of medications affecting blood, liver function, or lipid levels before or during early pregnancy. Participants will be excluded if they have the following situations: (1) A history of diabetes (Type 1 or Type 2); (2) has a history of GDM in the past; (3) chronic inflammatory diseases (eg, rheumatoid arthritis, inflammatory bowel disease); (4) current use of corticosteroids or immunosuppressants; (5) multiple pregnancies; (6) with known chronic viral hepatitis (including Hepatitis B and C); 7) fetal developmental abnormalities detected at registration; (8) not sign broad informed consent.
Data Collection
Blood samples for the complete blood count (CBC), which was used to calculate the SII, were obtained during the routine first-trimester prenatal visit. As this visit included the measurement of fasting blood glucose and lipid levels, all samples were collected in the morning after a mandated fast of at least 8 hours. Fasting compliance was verbally confirmed by healthcare staff prior to venipuncture, ensuring standardized conditions across all participants.
Variables and Measurements
At the time of enrollment, the characteristics of the participants and pregnancy-related risk factors were obtained by completing the questionnaire survey. The questionnaires included the following information: demographic data (such as age and parity); anthropometric measurements such as pre-pregnancy body mass index (BMI), BMI was calculated by dividing weight in kilograms by the square of height in meters; conception through in vitro fertilization (IVF); medical history such as family history of diabetes, previous history of GDM, smoking and alcohol consumption history; measurement timing (eg, at first prenatal visit or before 24 weeks of gestation); pregnancy complications as preeclampsia; delivery outcomes such as large for gestational age (LGA).
Inflammatory Indicators and GDM
The calculation formula of the SII: SII = (platelet count × neutrophil count) / lymphocyte count, derived from complete blood count (CBC). Other biomarkers: fasting blood glucose (FBG), total cholesterol, triglycerides.
The diagnostic criteria for GDM are based on the International Association of Research Groups on Diabetes and Pregnancy (IADPSG):33 75-g oral glucose tolerance test (OGTT) at 24–28 weeks. Thresholds: fasting: ≥92 mg/dL (5.1 mmol/L), 1-hour: ≥180 mg/dL (10.0 mmol/L), 2-hour: ≥153 mg/dL (8.5 mmol/L).
Statistical Analysis
Statistical analyses were performed using IBM SPSS (version 21.0) and the R statistical package (Version 3.4.3). The baseline characteristics of the study participants were described and stratified according to quartiles (Q1–Q4) of the SII. Continuous variables with a normal distribution are presented as mean ± standard deviation (SD), and comparisons across SII quartiles were made using one-way analysis of variance (ANOVA). Categorical variables are summarized as numbers and percentages, and comparisons were made using the chi-square test. To assess the independent association between SII and GDM, we constructed multivariable logistic regression models. SII was analyzed both as a continuous variable (per unit increase) and as a categorical variable (quartiles). For subgroup analysis, GDM patients were categorized as GDM A1 (controlled by lifestyle modification) or GDM A2 (requiring pharmacologic therapy).37 The model was adjusted for potential confounders selected a priori based on clinical knowledge and previous literature. These included: age, parity (nulliparous vs multiparous), pre-pregnancy body mass index (BMI), gestational week at the time of SII measurement, fasting blood glucose level, total cholesterol level, triglyceride level, tobacco use (yes/no), alcohol consumption during pregnancy (yes/no), presence of polycystic ovary syndrome (PCOS, yes/no), conception by in vitro fertilization (IVF, yes/no), and family history of diabetes (yes/no). The results of the regression analyses are presented as adjusted odds ratios (ORs) with their corresponding 95% confidence intervals (CIs). The linearity assumption between continuous independent variables and the logit of the outcome was tested using the Box-Tidwell approach by including interaction terms between the variables and their natural logarithms. No significant deviations from linearity were detected for any of the continuous variables. Furthermore, we conducted stratified analyses by age (<35 years vs ≥35 years), pre-pregnancy BMI (<24 kg/m2 vs ≥24 kg/m2), and parity (primipara vs multipara) to evaluate the consistency of the association across different subgroups. Effect modification was formally tested by including multiplicative interaction terms in the logistic regression models. All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) and the REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines.38,39
Results
General Characteristics of the Study Population
The baseline characteristics of the study population stratified by systemic SII quartiles are present in Table 1. After excluding participants with incomplete prenatal records, threatened late miscarriage, twin pregnancies, pregestational diabetes, pregnancy complicated by urinary system diseases, pregnancy complicated by cardiovascular system diseases, and those with SII measured after 24 weeks of gestation, a total of 47,480 pregnant women met the inclusion and exclusion criteria and were enrolled in this study with nearly equal distribution across four SII quartiles (Q1-Q4). Since there is currently no globally unified consensus on the stratification criteria for SII, we categorized participants into four groups based on quartiles (Q1-Q4) of the study population’s SII distribution, referencing existing literature (eg: on tumor prognosis or infectious diseases). The participants were equally divided into four groups: low SII (Q1, <648.88), moderate-low SII (Q2, 648.88–838.33), moderate SII (Q3, 838.33–1079.54), high SII (Q4, >1079.54). As expected by design, significant differences were observed across quartiles for most measured parameters (all p<0.001 unless otherwise specified). The baseline characteristics across these groups are presented in Table 1, a total of 47,280 participants were included in the final analysis and were categorized into four groups based on SII quartiles (Q1-Q4), with nearly identical sample sizes (Q1: n=11,870; Q2: n=11,869; Q3: n=11,871; Q4: n=11,870). In pregnancy outcomes, all measured outcomes exhibited significant quartile dependent trends, GDM prevalence increased from 10.76% to 17.49%, GDM (A2) nearly doubled from 1.89% to 3.96%. GDM with PE tripled from 0.53% to 1.68%, LGA increased from 7.21% to 8.36%. The higher the SII value is, the higher the risk of occurrence of GDM, GDM&PE and LGA. These findings demonstrate that elevated SII quartiles are associated with distinct metabolic and inflammatory profiles early in pregnancy, along with progressively worse pregnancy outcomes. The consistent gradients across multiple parameters support the biological plausibility of SII as an integrative marker of metabolic-inflammatory dysregulation.
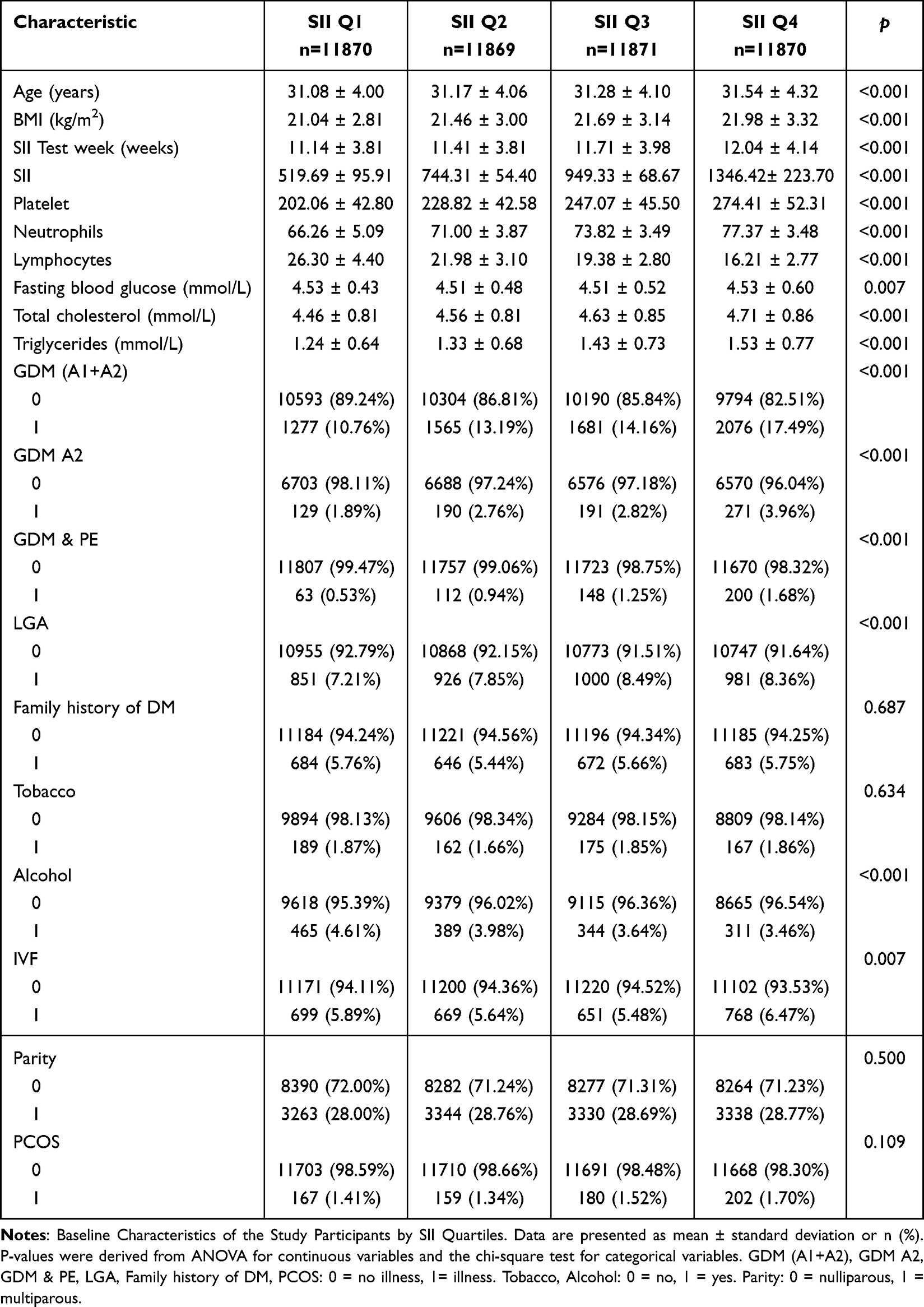 |
Table 1 Baseline Characteristic |
Baseline Participant Characteristics Based on the Quartiles of SII
After adjusting for confounding factors, such as age, parity, body mass index, test week of SII, fasting blood glucose, total serum cholesterol, tobacco, alcohol, PCOS, IVF, Triglycerides, family history of DM, the association between SII quartiles and pregnancy outcomes is presented in Table 2. For the primary outcome of GDM, including both diet-controlled (A1) and medication-requiring (A2) cases, we observed a significant dose-response relationship with increasing SII quartiles. Compared to the lowest quartile (Q1, reference), women in Q4 had the highest risk (17.49% vs 10.76% in Q1), with an adjusted odds ratio (aOR) of 1.56 (95% CI: 1.43–1.71, p<0.0001). The intermediate quartiles Q2 and Q3 showed progressively increasing risks (aOR respectively 1.19 and 1.26, both p<0.001). For secondary outcomes: GDM (A2) demonstrated particularly strong associations, with Q4 showing a 66% increased risk (aOR 1.66, 95% CI: 1.31–2.11) compared to Q1. The trend across quartiles was statistically significant (p<0.0001). The composite outcome of GDM with preeclampsia showed the most pronounced associations, with Q4 women having 2.61-fold higher risk (95% CI: 1.61–4.25) than Q1. Obviously, the adjusted risk estimates exceeded the unadjusted estimates in Q3 (aOR 2.82 vs crude OR 2.37). For LGA, the associations were more modest but still significant in Q3 (aOR 1.16, 95% CI: 1.05–1.29, p=0.0034). However, the highest quartile (Q4) did not maintain statistical significance after adjustment (aOR 1.09, p=0.1065). Furthermore, the dose-response relationship between SII and the risk of GDM was obtained through curve fitting. The results showed that after adjusting for confounding factors, the incidence of GDM significantly increased with the increase of SII (Figure 1).
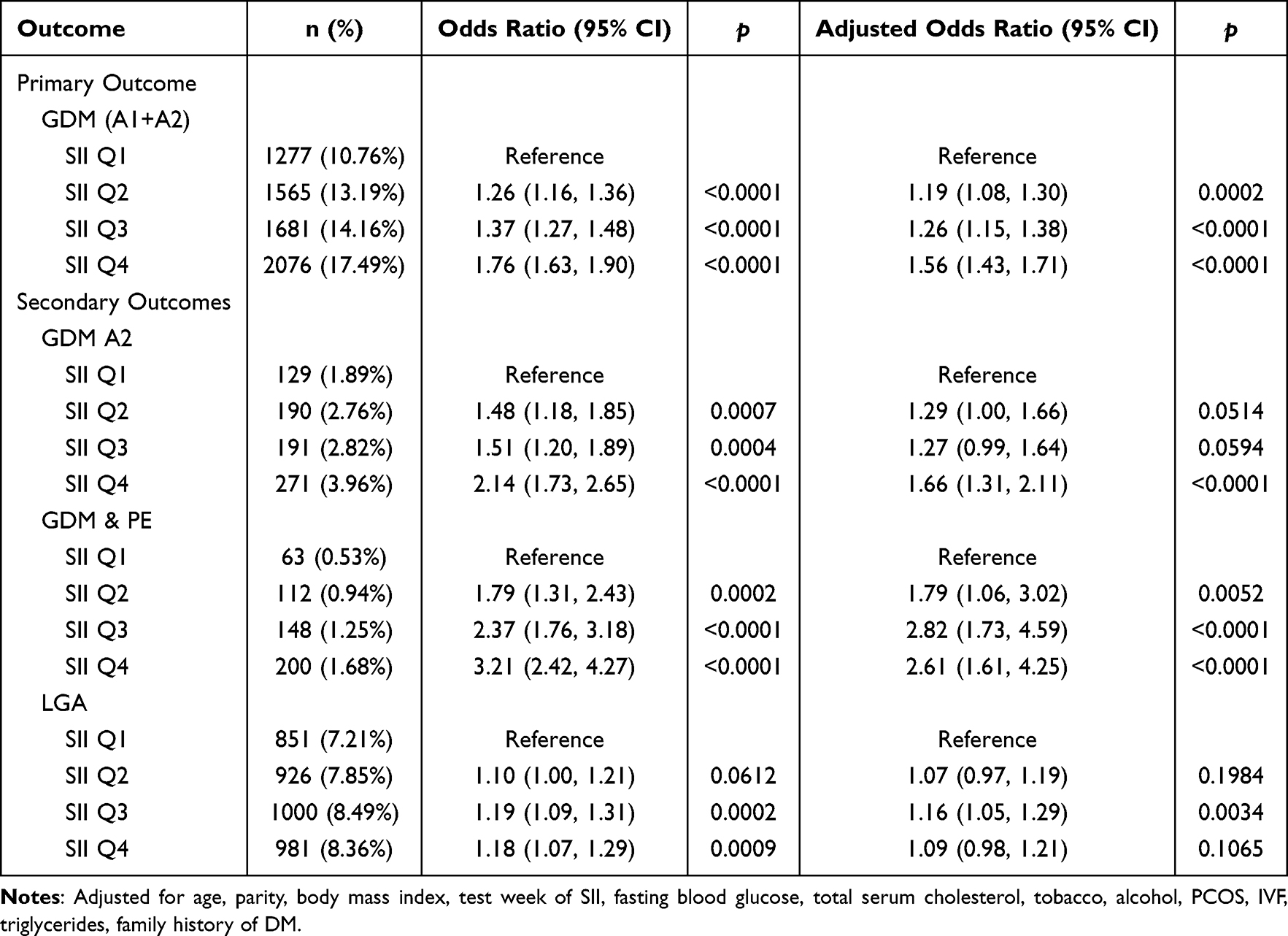 |
Table 2 Risk of Primary and Secondary Outcomes |
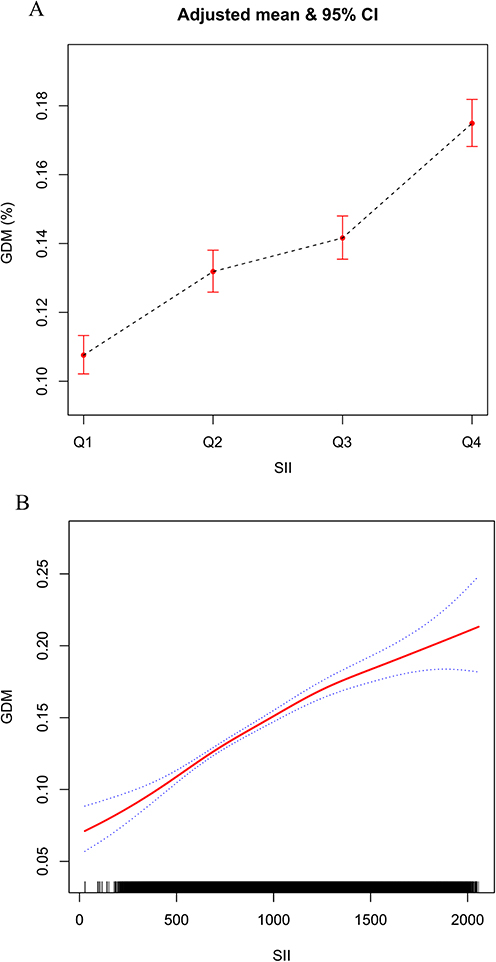 |
Figure 1 The dose-effect relationship between SII and the risk of GDM onset. (A) The overall relationship between SII and the risk of GDM based on the quartiles of SII. Age, parity, body mass index, test week of SII, fasting blood glucose, total serum cholesterol, tobacco, alcohol, PCOS, IVF, Triglycerides, family history of DM were adjusted. (B) The relationship between SII and GDM. Note: The dotted line represents the fitting curve of SII and GDM, and the red line represents the 95% confidence interval of the curve. |
Subgroup Analysis of GDM and SII
To better explore the relationship between SII and the risk of GDM occurrence, we conducted a subgroup analysis. After adjusting for confounding factors including age, parity, body mass index (BMI), gestational week at SII measurement, fasting blood glucose, serum total cholesterol, tobacco use, alcohol consumption, polycystic ovary syndrome, in vitro fertilization, triglycerides, and family history of diabetes, sensitivity analyses for age, BMI, and parity revealed that the association between SII and GDM remained largely consistent across subgroups in Table 3. As illustrated in Figure 2, visually depicts the stratified dose-response relationships across the analyzed subgroups.
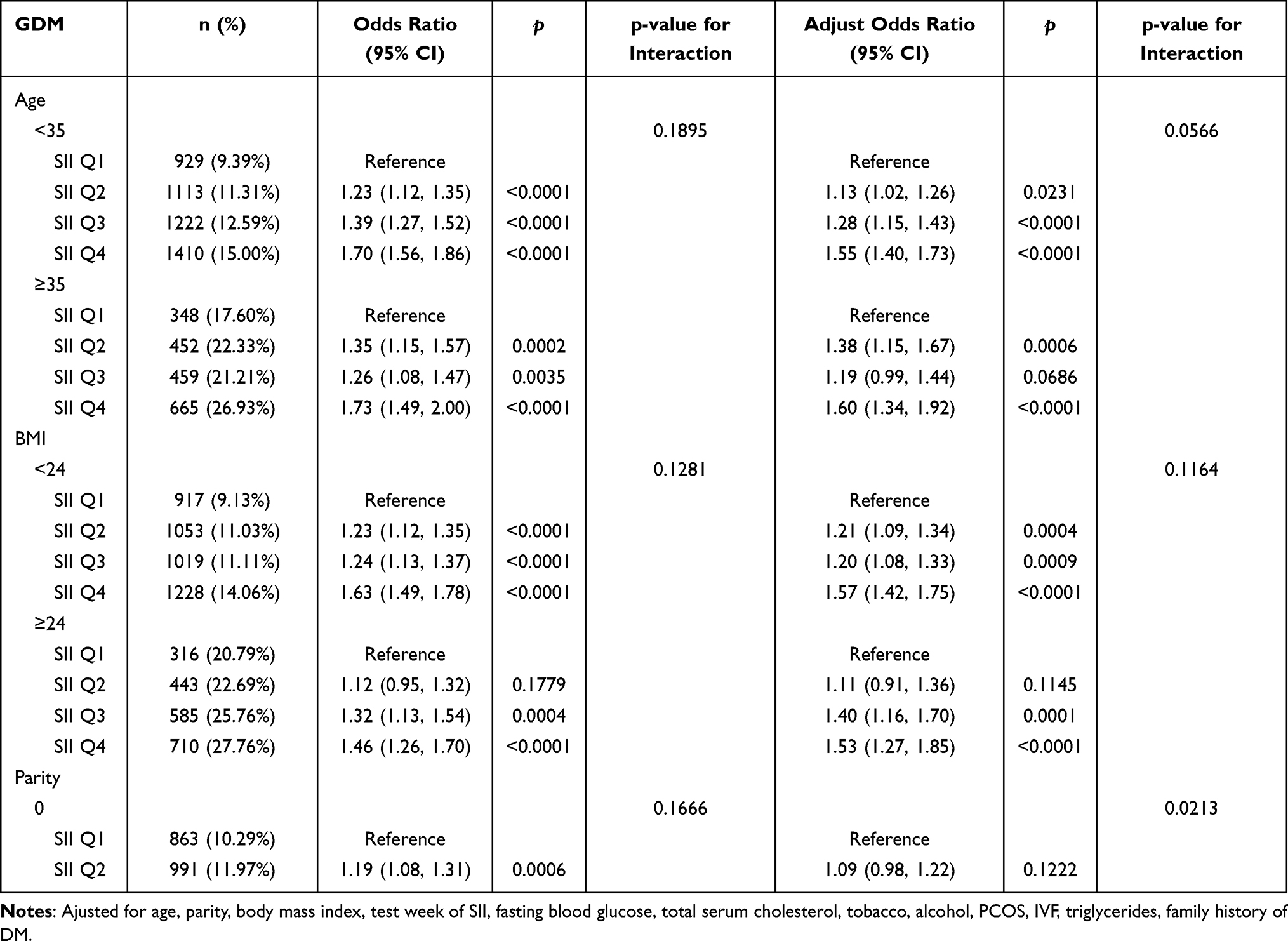 |
Table 3 Subgroup Analysis of GDM and SII |
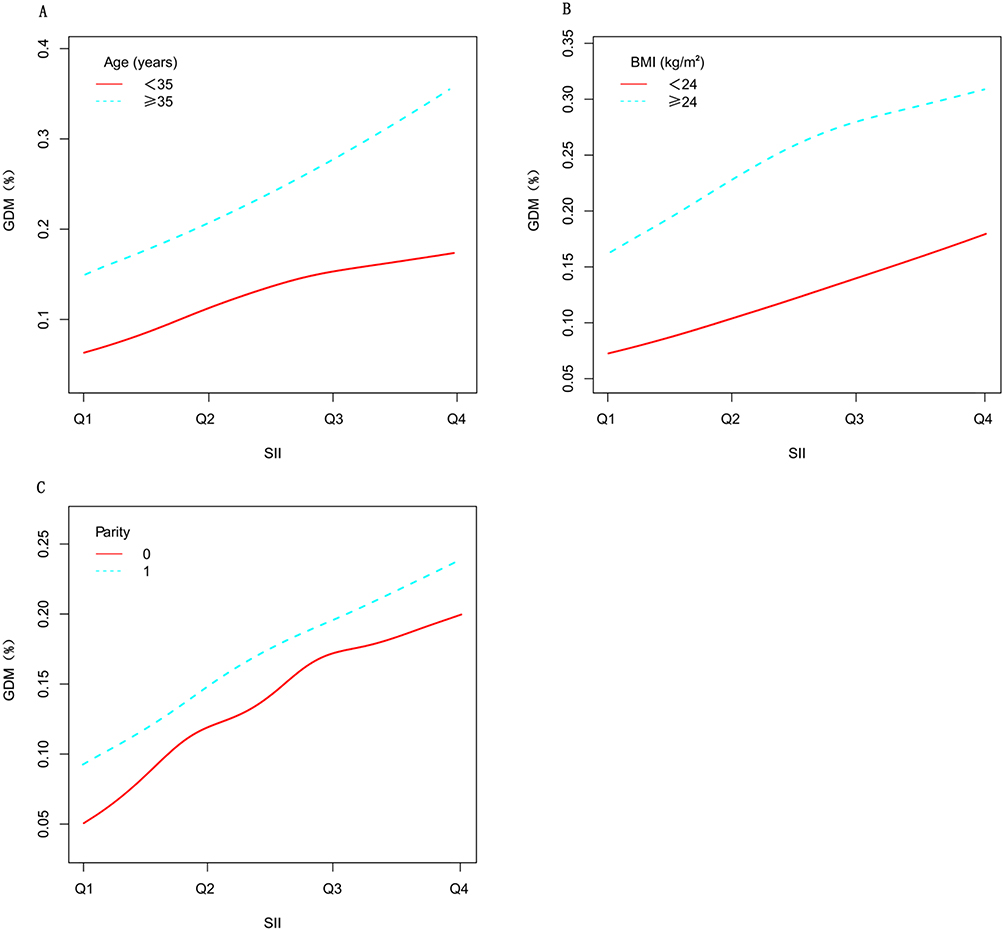 |
Figure 2 Stratified fitting curves among different subgroups. The results of the subgroup analyses were adjusted for age (A), BMI (B), and parity (C). |
Discussion
Main Results
Based on this retrospective birth cohort study involving 48,072 pregnant women, the research demonstrates that elevated SII levels during both early and mid-pregnancy are significantly associated with the development of GDM. Participants with increased SII in early pregnancy showed a higher risk of developing GDM during gestation. After adjusting for confounding factors including age, parity, BMI, gestational week at SII measurement, fasting blood glucose, serum total cholesterol, tobacco use, alcohol consumption, PCOS, IVF, triglycerides, and family history of diabetes, we found that elevated SII in early pregnancy was significantly correlated with age, BMI, GDM&preeclampsia, and large for gestational age LGA. Subgroup analysis further confirmed that this association remained statistically significant. It is proved that SII provides independent risk factors beyond traditional risk assessment.
Comparison with Findings of Previous Studies
The association between elevated SII and GDM observed in this study adds to the growing body of evidence linking systemic inflammation to GDM pathogenesis. Our results are consistent with those of previous studies, suggesting that the increase in the activation of circulating immune inflammatory cells may be related to glucose metabolism disorders in pregnant women.10,12,17,36,40 For example, in the research of Ye et al, their study, which evaluated inflammatory indices during the early-to-middle pregnancy period, compared with healthy women, pregnant women with GDM show significantly higher blood cell parameters, such as WBC (aOR 2.38, 95% CI 1.76–3.20), neut (aOR 2.47, 95% CI 1.82–3.36), lymph (aOR 1.40, 95% CI 1.06–1.85) or mono (aOR 1.69, 95% CI 1.27–2.24), in the early or middle stages of pregnancy.36 Xie et al17 found that the systemic inflammatory response index (SIRI) is a potential independent risk factor for the onset of GDM, ror the Q2 through Q4, the ORs (95% CIs) were 1.24 (1.12–1.38), 1.41 (1.27–1.57), and 1.64 (1.48–1.82), respectively. Furthermore, although our research results widely support the inflammation-GDM hypothesis, the differences from some negative studies are worth discussing. A recent retrospective studies showed that there was no significant association between SII and the risk of GDM occurrence.29 In all three adjusted models (Model 1 to Model 3), the four quartiles (Q1-Q4) of SII showed no statistically significant association with GDM risk (all P > 0.05), such as Model 3 (Fully adjusted model, Q4 aORs 0.90, 95% CI 0.78–1.03). Another prospective cohort study conducted on pregnant women in Iran also supports this view,30 their research results indicate that SII has no significant association with the development of GDM (RR = 3.7, 95% CI:1.5–8.8). The observed discrepancies with prior studies may stem from racial variations in immune responses and baseline inflammatory levels. Notably, our Asian cohort demonstrated higher GDM susceptibility at lower BMI thresholds, suggesting ethnic differences in metabolic-inflammatory interactions.41 Importantly, unlike previous models limited to age, parity and BMI adjustments, our analysis incorporated key confounders including fasting blood glucose, total serum cholesterol, tobacco, alcohol, PCOS, IVF, triglycerides, family history of diabetes, thereby minimizing residual confounding.
Possible Underlying Mechanisms
We observed that the association between elevated SII and GDM likely arises through multiple interrelated biological pathways linking chronic low-grade inflammation with impaired glucose metabolism. The following interconnected mechanisms may underlie this relationship. First, chronic low-grade inflammation drives insulin resistance (IR), the core pathological feature of GDM.12,17 The SII—which integrates neutrophils, lymphocytes, and platelets—serves as a marker of systemic immune activation and inflammatory burden. Pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) disrupt insulin signaling by promoting serine phosphorylation of insulin receptor substrate-1 (IRS-1), thereby impairing glucose uptake in insulin-sensitive tissues including skeletal muscle and adipose tissue. This inflammatory interference with insulin action results in hyperglycemia and contributes to GDM pathogenesis. Second, immune cell imbalance exacerbates metabolic dysfunction. Such as white blood cells (WBCs), particularly neutrophils and monocytes, play key roles in inflammation-mediated IR through the secretion of pro-inflammatory factors.12,42 Additionally, lymphocytes, which regulate adaptive immunity, may demonstrate an altered Th1/Th2 balance in GDM, further perpetuating a pro-inflammatory state. The SII combined measurement of these immune components provides a more robust assessment of inflammation-related metabolic disruption than individual cell counts alone.40 Third, platelet activation and vascular dysfunction contribute to disease progression. Beyond their coagulation functions, platelets act as inflammatory mediators. Inflammation-induced vascular injury promotes platelet activation and aggregation, leading to endothelial dysfunction and microvascular impairment.43 Given the critical role of vascular health in insulin-mediated glucose delivery, platelet-driven inflammation may exacerbate IR. The incorporation of platelet counts in the SII enhances its ability to reflect this thrombotic-inflammatory axis in GDM development.44 Finally, obesity and other risk factors interact with inflammatory pathways. Adipose tissue, especially visceral fat, secretes pro-inflammatory adipokines (eg TNF-α, IL-6, leptin) while reducing anti-inflammatory adiponectin, creating an inflammatory milieu that worsens insulin sensitivity.5,14,30,31 Advanced maternal age correlates with increased baseline inflammation and declining metabolic efficiency, potentially explaining the higher SII levels and GDM susceptibility observed in older pregnant women. Multiparity may induce a “metabolic memory effect” where repeated pregnancies cause cumulative β-cell stress and persistent subclinical inflammation, predisposing women to glucose intolerance in subsequent pregnancies. Notably, our study found that SII remained significantly associated with GDM even after BMI adjustment, suggesting inflammation contributes to GDM risk both independently and synergistically with obesity.
The SII emerges as a comprehensive biomarker that captures multiple pathological processes—innate immune activation, platelet-mediated vascular dysfunction, adipose tissue inflammation, and metabolic dysregulation—that collectively promote GDM. Our findings suggest that early-pregnancy SII assessment could enhance GDM risk stratification and highlight potential avenues for anti-inflammatory interventions in high-risk populations. Future research should investigate whether modulation of these inflammatory pathways can prevent or mitigate GDM onset.
Clinical Implications
Our findings carry significant clinical implications, as the SII offers practical advantages for early pregnancy risk assessment. Derived from routine complete blood count parameters, SII provides a cost-effective screening tool without requiring additional testing, enabling timely identification of high-risk women before conventional GDM diagnosis at 24–28 weeks. Its quantitative nature may further refine risk stratification and guide personalized prevention strategies. The study’s strengths—including its large multicenter retrospective cohort design, standardized GDM diagnosis (IADPSG criteria)33 and comprehensive adjustment for confounders—enhance the validity of these findings. Moving forward, critical questions remain, such as whether anti-inflammatory interventions (eg dietary modifications, exercise) in women with elevated first-trimester SII can reduce GDM incidence.26,35,45 Additionally, future research should explore the longitudinal dynamics of SII throughout pregnancy, its relationship with postpartum metabolic outcomes, and the mechanistic pathways linking SII components to pancreatic β-cell dysfunction and insulin resistance in pregnancy.17,29,31 These investigations could deepen our understanding of GDM pathogenesis and inform targeted therapeutic strategies.
Strengths and Limitations
Our findings are noteworthy, with the key strength being that this was a multicenter cohort study conducted in collaboration with three tertiary Grade-A hospitals. This population-based retrospective studies demonstrated the association between SII and the risk of GDM development, involving long-term follow-up of a large population. Such a design is optimal for evaluating the relationship between SII levels and GDM risk. Following adjustment for potential confounders, we also collected detailed information, including age, BMI, parity, history of GDM, and monitoring of blood lipids and liver enzymes, further confirming that the observed association in our study remains robust.
However, several limitations warrant consideration: First, although we adjusted for known major confounding factors, residual confounding by unmeasured variables (such as dietary patterns, dietary habits, trimester-specific weight gain, physical activity, and other potential confounders) cannot be excluded. Although we excluded patients with known hepatitis, universal serological screening for HBV and HCV was not performed for all participants. Therefore, we cannot entirely rule out the potential influence of undetected chronic hepatitis infections on SII values in some individuals, which may represent a potential confounding factor in our results. Second, while our study included patients from three medical centers, this may limit generalizability to other populations with different environmental exposures or ethnic groups at varying baseline risks of GDM. Although temporal sequence and biological plausibility support a potential causal relationship, the findings should not be considered definitive. Finally, peripheral blood inflammatory biomarkers may be influenced by infections, steroid therapy, or other medications, which were not systematically assessed in this study.
Conclusion
This retrospective studies provides compelling evidence that an elevated systemic SII during early pregnancy is significantly associated with subsequent development of GDM. Our findings contribute to the growing body of evidence supporting the crucial role of subclinical inflammation in the pathogenesis of GDM, while introducing SII as a novel, clinically accessible biomarker for early risk stratification.
Abbreviations
GDM, gestational diabetes mellitus; SII, immune-inflammation index; FBG, fasting blood glucose; LGA, large for gestational age; PCOS, polycystic ovary syndrome; IVF, in vitro fertilization; BMI, body mass index; IR, insulin resistance; PSM, propensity score matching; SD, standard deviation; RR, relative risks.
Data Sharing Statement
Due to the consideration of the privacy of the research participants, the datasets generated and analyzed during the research period have not been made public yet. However, if the corresponding author makes a reasonable request, it can be provided to them. The datasets used and analyzed during the current study are available from the corresponding author (Ying Gu), upon reasonable request.
Ethical Approval
This study was conducted in accordance with the guiding principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Obstetrics and Gynecology Hospital of Fudan University, Wuxi Maternal and Child Health Hospital and Chenzhou First People’s Hospital. All individual participants provided broad informed consent to participate in this study. Ethical Approval: Approved by the Ethics Committees of the Obstetrics and Gynecology Hospital of Fudan University (No. 2024-189), Wuxi Maternal and Child Health Hospital (No. 2024-06-1024-54), and Chenzhou First People’s Hospital (No. 2024021).
Funding
The Appropriate Technology Promotion Project of Wuxi Municipal Health Commission (FYTG202404); Wuxi Municipal Health Commission youth project (Q202468).
Disclosure
The authors declare no potential conflicts of interest.
References
1. Sweeting A, Wong J, Murphy HR, et al. A clinical update on gestational diabetes mellitus. Endocr Rev. 2022;43(5):763–13. doi:10.1210/endrev/bnac003
2. Kautzky-Willer A, Winhofer Y, Kiss H, et al. [Gestational diabetes mellitus (Update 2023)]. Wien Klin Wochenschr. 2023;135(Suppl 1):115–128. German. doi:10.1007/s00508-023-02181-9
3. Wang H, Li N, Chivese T, et al. IDF diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabet Res Clin Pract. 2022;183:109050. doi:10.1016/j.diabres.2021.109050
4. Chen L, Zhu Y. Gestational diabetes mellitus and subsequent risks of diabetes and cardiovascular diseases: the life course perspective and implications of racial disparities. Curr Diab Rep. 2024;24(11):244–255. doi:10.1007/s11892-024-01552-4
5. Hornova M, Simjak P, Anderlova K. Preeclampsia and diabetes mellitus. Ceska Gynekol. 2023;88(6):467–471. doi:10.48095/cccg2023467
6. Yang Y, Wu N. Gestational diabetes mellitus and preeclampsia: correlation and influencing factors. Front Cardiovasc Med. 2022;9:831297. doi:10.3389/fcvm.2022.831297
7. Moon JH, Jang HC. Gestational diabetes mellitus: diagnostic approaches and maternal-offspring complications. Diabetes Metab J. 2022;46(1):3–14. doi:10.4093/dmj.2021.0335
8. Wicklow B, Retnakaran R. Gestational diabetes mellitus and its implications across the life span. Diabetes Metab J. 2023;47(3):333–344. doi:10.4093/dmj.2022.0348
9. Artzi NS, Shilo S, Hadar E, et al. Prediction of gestational diabetes based on nationwide electronic health records. Nat Med. 2020;26(1):71–76. doi:10.1038/s41591-019-0724-8
10. Pinto Y, Frishman S, Turjeman S, et al. Gestational diabetes is driven by microbiota-induced inflammation months before diagnosis. Gut. 2023;72(5):918–928. doi:10.1136/gutjnl-2022-328406
11. Pradhan AD, Manson JE, Rifai N, et al. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA. 2001;286(3):327–334. doi:10.1001/jama.286.3.327
12. Rehman K, Akash MS. Mechanisms of inflammatory responses and development of insulin resistance: how are they interlinked? J Biomed Sci. 2016;23(1):87. doi:10.1186/s12929-016-0303-y
13. Kristiansen OP, Mandrup-Poulsen T. Interleukin-6 and diabetes: the good, the bad, or the indifferent? Diabetes. 2005;54(Suppl 2):S114–S124. doi:10.2337/diabetes.54.suppl_2.S114
14. Liu Y, Sun R, Lin X, et al. Procyanidins and its metabolites by gut microbiome improves insulin resistance in gestational diabetes mellitus mice model via regulating NF-kappaB and NLRP3 inflammasome pathway. Biomed Pharmacother. 2022;151:113078. doi:10.1016/j.biopha.2022.113078
15. Esser N, Legrand-Poels S, Piette J, et al. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabet Res Clin Pract. 2014;105(2):141–150. doi:10.1016/j.diabres.2014.04.006
16. Cao Z, Chen H, Chen Q, et al. Baseline plasma GPX3 level predicts efficacy of insulin-sensitization drug Chiglitazar in type 2 diabetes. Phenomics. 2025;5(3):338–342. doi:10.1007/s43657-025-00266-1
17. Xie S, Zhang E, Gao S, et al. Associations of systemic immune-inflammation index and systemic inflammation response index with maternal gestational diabetes mellitus: evidence from a prospective birth cohort study. Chin Med J. 2025;138(6):729–737. doi:10.1097/CM9.0000000000003236
18. Sahin R, Tanacan A, Serbetci H, et al. First-trimester neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), and systemic immune-response index (SIRI) as predictors of composite adverse outcomes in pregnant women with Familial Mediterranean fever. Z Geburtshilfe Neonatol. 2024;228(2):156–160. doi:10.1055/a-2125-0973
19. Wu J, Huang Y, Zhang S, et al. Association between healthy lifestyles and adverse health outcomes, and the mediating role of inflammation. Phenomics. 2025;5:461–465. doi:10.1007/s43657-025-00265-2
20. Albany C. Systemic immune-inflammation index in germ-cell tumours: search for a biological prognostic biomarker. Br J Cancer. 2018;118(6):761–762. doi:10.1038/bjc.2018.7
21. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
22. Wang A, Wang F, Huang Y, et al. Association between systemic inflammatory markers and all-cause mortality in patients with stroke: a prospective study using data from the UK Biobank. J Stroke Cerebrovasc Dis. 2024;33(12):108076. doi:10.1016/j.jstrokecerebrovasdis.2024.108076
23. de Rooij L, Becker LM, Teuwen LA, et al. The pulmonary vasculature in lethal COVID-19 and idiopathic pulmonary fibrosis at single-cell resolution. Cardiovasc Res. 2023;119(2):520–535. doi:10.1093/cvr/cvac139
24. Xu B, Wu Q, La R, et al. Is systemic inflammation a missing link between cardiometabolic index with mortality? Evidence from a large population-based study. Cardiovasc Diabetol. 2024;23(1):212. doi:10.1186/s12933-024-02251-w
25. Tort M, Sevil FC, Sevil H, et al. Evaluation of systemic immune-inflammation index in acute deep vein thrombosis: a propensity-matched. J Vasc Surg Venous Lymphat Disord. 2023;11(5):972–977. doi:10.1016/j.jvsv.2023.02.008
26. Hrubaru I, Motoc A, Moise ML, et al. The predictive role of maternal biological markers and inflammatory scores NLR, PLR, MLR, SII, and SIRI for the risk of preterm delivery. J Clin Med. 2022;11(23):6982. doi:10.3390/jcm11236982
27. Cakir U, Tayman C, Tugcu AU, et al. Role of Systemic Inflammatory Indices in the Prediction of Moderate to Severe Bronchopulmonary Dysplasia in Preterm Infants. Arch Bronconeumol. 2023;59(4):216–222. doi:10.1016/j.arbres.2023.01.003
28. Zhuang Y, Xiao Y, Bai R, et al. The association of peripheral blood immunoinflammatory markers with PE and adverse outcomes in preeclampsia: a retrospective study. J Inflamm Res. 2025;18:4359–4366. doi:10.2147/JIR.S504552
29. Qiu J, Song R, Chen L, et al. The association between inflammatory indices in early pregnancy and the risk of gestational diabetes mellitus in Chinese population. BMC Pregnancy Childbirth. 2025;25(1):151. doi:10.1186/s12884-025-07238-3
30. Hashemipour S, Kalantarian SS, Panahi H, et al. The association of inflammatory markers in early pregnancy with the development of gestational diabetes: qazvin maternal and neonatal metabolic study (QMNS). BMC Pregnancy Childbirth. 2025;25(1):135. doi:10.1186/s12884-025-07267-y
31. Duo Y, Song S, Qiao X, et al. The association of hematological parameters in early and middle pregnancy with the risk of gestational diabetes mellitus. Diabetes Metab Syndr Obes. 2024;17:633–646. doi:10.2147/DMSO.S445927
32. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy: a World Health Organization Guideline. Diabet Res Clin Pract. 2014;103(3):341–363. PMID: 24847517. doi:10.1016/j.diabres.2013.10.012
33. Metzger BE, Gabbe SG, Persson B, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–682. doi:10.2337/dc10-0719
34. Amirian A, Rahnemaei FA, Abdi F. Role of C-reactive Protein (CRP) or high-sensitivity CRP in predicting gestational diabetes mellitus: systematic review. Diabetes Metab Syndr. 2020;14(3):229–236. doi:10.1016/j.dsx.2020.02.004
35. Rizo-Tellez SA, Sekheri M, Filep JG. C-reactive protein: a target for therapy to reduce inflammation. Front Immunol. 2023;14:1237729. doi:10.3389/fimmu.2023.1237729
36. Ye YX, Wang Y, Wu P, et al. Blood cell parameters from early to middle pregnancy and risk of gestational diabetes mellitus. J Clin Endocrinol Metab. 2023;108(12):e1702–e1711. doi:10.1210/clinem/dgad336
37. Ye W, Luo C, Huang J, et al. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2022;377:e67946. doi:10.1136/bmj-2021-067946
38. Langan SM, Schmidt SA, Wing K, et al. The reporting of studies conducted using observational routinely collected health data statement for pharmacoepidemiology (RECORD-PE). BMJ. 2018;363:k3532. doi:10.1136/bmj.k3532
39. Fitchett E, Seale AC, Vergnano S, et al. Strengthening the Reporting of Observational Studies in Epidemiology for Newborn Infection (STROBE-NI): an extension of the STROBE statement for neonatal infection research. Lancet Infect Dis. 2016;16(10):e202–e213. doi:10.1016/S1473-3099(16)30082-2
40. Kong M, Zhang H, Liu X, et al. Association of maternal neutrophil count in early pregnancy with the development of gestational diabetes mellitus: a prospective cohort study in China. Gynecol Endocrinol. 2022;38(3):258–262. doi:10.1080/09513590.2021.2025216
41. ElSayed NA, Aleppo G, Aroda VR, et al. 2. Classification and diagnosis of diabetes: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S19–S40. doi:10.2337/dc23-S002
42. Shin G, Jang K, Kim M, et al. Inflammatory markers and plasma fatty acids in predicting WBC level alterations in association with glucose-related markers: a cross-sectional study. Front Immunol. 2020;11:629. doi:10.3389/fimmu.2020.00629
43. Scherlinger M, Richez C, Tsokos GC, et al. The role of platelets in immune-mediated inflammatory diseases. Nat Rev Immunol. 2023;23(8):495–510. doi:10.1038/s41577-023-00834-4
44. Hessami K, Tabrizi R, Homayoon N, et al. Gestational diabetes mellitus and inflammatory biomarkers of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio: a systematic review and meta-analysis. Biomarkers. 2021;26(6):491–498. doi:10.1080/1354750X.2021.1926542
45. Ureyen OE, Buyuk GN, Erol KE, et al. Gestational diabetes and c-reactive protein/albumin ratio in pregnancy: a prospective study. Yonsei Med J. 2024;65(7):413–417. doi:10.3349/ymj.2023.0334
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Lower ATG7 Levels are Associated with a Higher Risk of Gestational Diabetes Mellitus: A Cross-Sectional Study
Lu L, Ma Y, Deng J, Xie J, Huang C
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2335-2343
Published Date: 4 August 2022
First-Trimester Triglyceride-Glucose Index and Triglyceride/High-Density Lipoprotein Cholesterol are Predictors of Gestational Diabetes Mellitus Among the Four Surrogate Biomarkers of Insulin Resistance
Ma N, Bai L, Lu Q
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1575-1583
Published Date: 8 April 2024
Deciphering the Role of CD36 in Gestational Diabetes Mellitus: Linking Fatty Acid Metabolism and Inflammation in Disease Pathogenesis
Huang L, Zhang T, Zhu Y, Lai X, Tao H, Xing Y, Li Z
Journal of Inflammation Research 2025, 18:1575-1588
Published Date: 4 February 2025
Insulin Resistance as a Biomarker for Pelvic Organ Prolapse in Gestational Diabetes Mellitus: Stratification by Delivery Modes
Jiao Y, Dai Y, He L, Fei Z
International Journal of General Medicine 2025, 18:6377-6385
Published Date: 21 October 2025
The Role of METS-IR in Early Screening for Gestational Diabetes Mellitus in Chinese Women: A Two-Center Prospective Study
Gao J, Song S, Duo Y, Wang S, Qiao X, Zhang Y, Xu J, Zhang J, Nie X, Sun Q, Yang X, Wang A, Sun W, Fu Y, Zhang M, Dong Y, Lu Z, Yuan T, Zhao W
Diabetes, Metabolic Syndrome and Obesity 2025, 18:3967-3984
Published Date: 25 October 2025