Back to Journals » Journal of Inflammation Research » Volume 18
Elevated Serum Podoplanin Levels Correlate with Disease Severity and Inflammation in Ulcerative Colitis: A Cross-Sectional Study
Received 16 March 2025
Accepted for publication 9 September 2025
Published 18 September 2025 Volume 2025:18 Pages 12989—13000
DOI https://doi.org/10.2147/JIR.S528624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Nadia Andrea Andreani
Xiaogang Huang,1 Caifang Tang2
1Department of Gastroenterology, Sijing Hospital, Shanghai, 201601, People’s Republic of China; 2Department of Nursing, Sijing Hospital, Shanghai, 201601, People’s Republic of China
Correspondence: Caifang Tang, Department of Nursing, Sijing Hospital, Songjiang District, No. 389, Sitong Road, Shanghai, 201601, People’s Republic of China, Tel +86-18917537805, Email [email protected]
Objective: Podoplanin is a transmembrane glycoprotein that is primarily expressed in lymphatic endothelial cells, fibroblasts, and certain epithelial cells. Although it has been implicated in various physiological and pathological processes, its role in ulcerative colitis (UC) remains unclear. This study aimed to investigate the association between serum podoplanin levels and disease severity in patients with UC, and its potential involvement in coagulation and inflammation in patients with UC.
Methods: This cross-sectional study compared serum podoplanin levels in patients with remission-UC (n = 115), active-UC (n = 94), and healthy controls (n = 150). Active-UC patients were further classified as mild (n = 37), moderate (n = 31), or severe (n = 26) based on their Mayo scores. Clinical, inflammatory, and coagulation markers were measured and analyzed using one-way ANOVA, ROC analysis, and Pearson’s correlation. Podoplanin expression in human tissues was examined using the BioGPS database (https://biogps.org/).
Results: Serum podoplanin levels were significantly elevated in patients with UC (n=209) compared to healthy controls (n=150), with higher levels observed in patients with moderate (n=31) and severe (n=26) disease than in those with mild UC (n=37). Correlation analysis revealed that serum podoplanin levels were positively associated with coagulation markers-platelet count (r=0.247, p< 0.001), erythrocyte sedimentation rate (ESR; r=0.695, p< 0.001), D-dimer (r=0.765, p< 0.001), and fibrinogen (r=0.490, p< 0.001) as well as inflammatory markers, including C-reactive protein (CRP; r=0.767, p< 0.001), interleukin-1beta (IL-1β; r=0.744, p< 0.001), interleukin-6 (IL-6; r=0.786, p< 0.001), interleukin-17A (IL-17A; r=0.788, p< 0.001), tumor necrosis factor-α (TNF-α; r=0.784, p< 0.001), and Mayo score (r=0.912, p< 0.001).
Conclusion: Elevated serum podoplanin levels are closely associated with disease activity, inflammation, and hypercoagulability in patients with UC, suggesting that it may serve as a reliable biomarker for monitoring disease severity and guiding clinical management.
Keywords: ulcerative colitis, severity, coagulation, inflammation, podoplanin
Introduction
Ulcerative colitis (UC) is a chronic inflammatory bowel disease (IBD) characterized by diffuse inflammation of the colonic mucosa, leading to symptoms such as abdominal pain, diarrhea, and rectal bleeding.1 The pathogenesis of UC involves a complex interplay of genetic, environmental, and immunological factors, resulting in dysregulated immune responses and chronic inflammation.2 Despite advances in our understanding of the disease, the mechanisms driving its severity and progression remain incompletely understood. Recent studies have highlighted the role of endothelial and epithelial markers, such as podoplanin, in inflammation and coagulation, which are key processes in patients with UC.3
Podoplanin, a transmembrane glycoprotein, is primarily expressed in lymphatic endothelial cells, fibroblasts, and certain epithelial cells.4 It is involved in various physiological and pathological processes, including lymphangiogenesis, inflammation, and thrombosis.5 In patients with UC, podoplanin may contribute to disease severity by promoting inflammation and coagulation, both of which are hallmarks of UC pathology.6 Moreover, previous research has reported a marked increase in podoplanin-expressing intestinal lymphatic vessels in IBD, suggesting their involvement in lymphangiogenesis and tissue remodeling during inflammation.7 Additionally, another study highlighted the broader role of podoplanin in inflammatory processes, including its interaction with immune cells and contribution to the tumor microenvironment.8 However, while these studies provide insight into tissue-level expression and biological function, the relationship between serum podoplanin levels and the clinical features of UC-such as disease severity, coagulation abnormalities, and inflammation, remains largely unexplored. This gap underscores the need for further research on serum podoplanin as a potential noninvasive biomarker for UC activity and complications.
This cross-sectional study aimed to explore the association between serum podoplanin levels and UC severity, as well as its potential role in coagulation and inflammation. By elucidating these relationships, we hope to provide new insights into the pathophysiology of UC and identify potential biomarkers for disease monitoring and therapeutic targeting. Understanding the role of podoplanin in patients with UC could pave the way for novel therapeutic strategies aimed at modulating inflammation and coagulation in this debilitating disease.
Methods
Study Population
A total of 209 patients with ulcerative colitis (UC) were recruited from the Department of Gastroenterology of our hospital between January 2021 and June 2024. The diagnosis of UC was established according to the 2017 European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines,9 based on clinical symptoms (abdominal pain, diarrhea, bloody stools, recurrent episodes, and excessive bowel sounds) and colonoscopic findings (vascular pattern loss, mucosal texture changes, purulent exudates, and intestinal wall sclerosis). The inclusion criteria were as follows: (1) age ≥ 18 years, (2) first-time diagnosis of UC, and (3) availability of complete clinical data. The exclusion criteria were as follows: (1) presence of other systemic inflammatory or infectious diseases, (2) family history of UC, (3) history of colorectal surgery, (4) abnormal liver or kidney function or impaired coagulation, (5) autoimmune diseases, and (6) history of malignancy. The control group comprised age- and sex-matched healthy individuals who underwent routine physical examinations. The study was approved by the Ethics Committee of our hospital, and all participants provided informed consent prior to participation. The overall study design is illustrated in Figure 1.
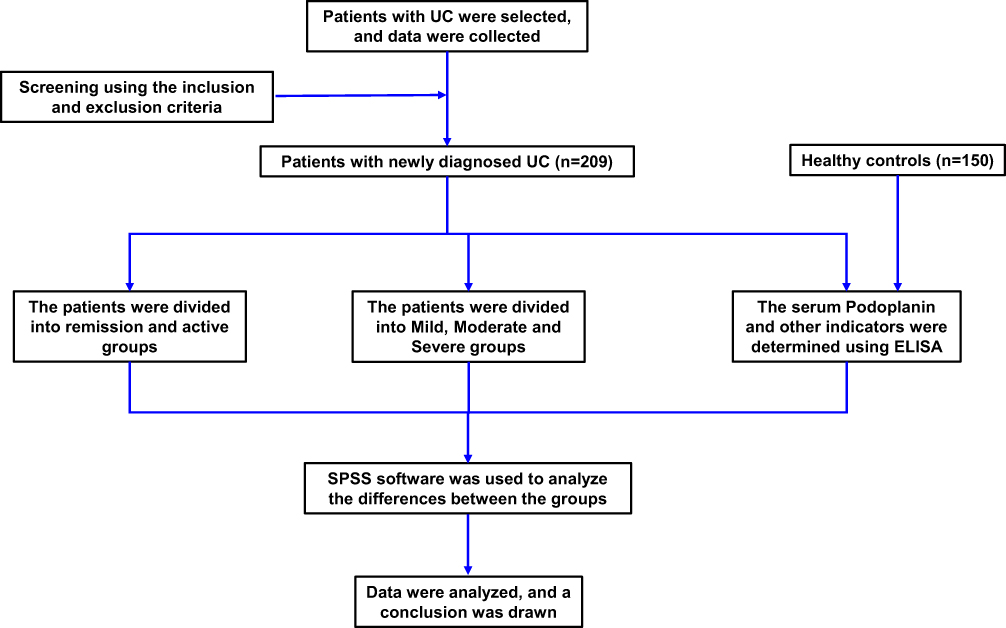 |
Figure 1 Research framework diagram. |
Podoplanin Expression Analysis in Different Human Tissues
To investigate the abundance of podoplanin expression across different human tissues, we queried the publicly available gene expression database BioGPS (http://biogps.org/). BioGPS compiles gene expression profiles from a wide range of human tissues and cell types based on microarray data primarily sourced from the GeneAtlas U133A dataset. The expression levels of podoplanin (Affymetrix probe ID: 203798_at) were retrieved and analyzed to identify tissues with relatively high or low transcript abundances.10
Severity Assessment of Disease
The disease severity of patients with UC were evaluated using the modified Mayo scoring system, which includes four items: rectal bleeding, frequency of bowel movements, physician evaluation, and endoscopic condition, with scores ranging from 0 to 3 for each item and a total score of 0 to 12. A score of 0–2 indicates clinical remission, while a score greater than 2 indicates the active phase, with 3–5 points indicating a mild active phase, 6–10 points indicating a moderate active phase, and 11–12 points indicating a severe active phase. A higher score indicates a more severe condition.11
Data Collection
Demographic and clinical characteristics were collected from each patient, including age, sex, and body mass index (BMI). Venous blood was obtained and measured within 24h after admission (fasting). Hemoglobin, white blood cell (WBC), platelet, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) levels were measured using an automatic biochemical analyzer (Beckman Coulter). D-dimer and fibrinogen levels were measured using an automated coagulation analyzer.
ELISA Assay
The collected fasting blood samples were centrifuged to separate the serum and stored in a refrigerator at −80°C. Serum biomarker levels in control subjects and patients with UC were measured using ELISA kits for Interleukin-1 beta (IL-1β; DLB50, R&D Systems), Interleukin-6 (IL-6; D6050B, R&D Systems), Interleukin-17A (IL-17A; D1700, R&D Systems), Tumor necrosis factor-alpha (TNF-α; DTA00D, R&D Systems), and podoplanin (BK-F98706, Shanghai Boke Biotechnology Co., Ltd).
Statistical Analysis
All statistical analyses were performed using SPSS software (version 20.0). Data are presented as mean ± standard deviation (SD) for continuous variables and as frequency (percentage) for categorical variables. The differences between the three groups were compared using one-way analysis of variance, followed by Tukey’s post-hoc test. The associations between categorical variables were assessed using the chi-square or Fisher exact test. The correlations between podoplanin and other continuous variables were evaluated using Pearson’s correlation analysis. The diagnostic value of podoplanin was assessed using ROC analysis to distinguish between remission and active UC. Statistical significance was set at *p< 0.05, **p<0.01, ***p<0.001.
Results
Demographic Characteristics of the Study Population
The investigation used a comprehensive method to compare patients with remission-UC (n=115) and active-UC (n=94) with healthy controls (n=150). The results from the one-way ANOVA analysis indicated that remission-UC and active-UC patients exhibited significantly higher levels of various health indicators, WBC, platelet, ESR, D-Dimer, Fibrinogen, CRP, IL-1β, IL-6, IL-17A, and TNF-α compared to healthy controls. In contrast, BMI and hemoglobin levels were significantly lower (p<0.05), as shown in Table 1. However, there were no significant differences in age and sex between healthy controls and either remission or active UC patients (p>0.05).
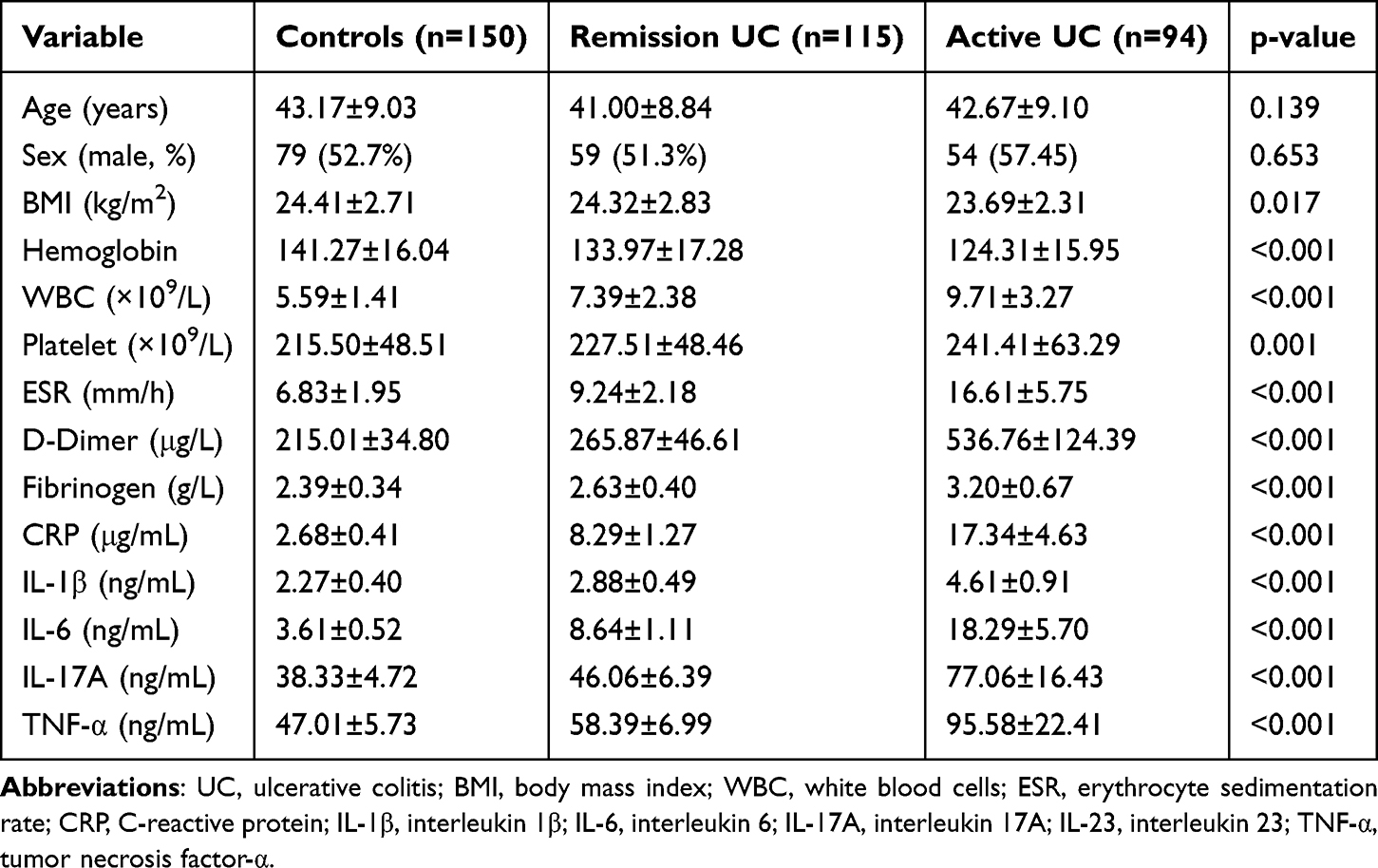 |
Table 1 Demographic, Clinic, and Laboratory Characteristics of the Study Population |
Furthermore, the data presented in Table 2 show how various clinical and laboratory parameters correlate with endoscopic severity (Mayo score) in patients with active ulcerative colitis (UC). The patients are grouped into three categories based on their Mayo endoscopic sub score: mild (3–5), moderate (6–10), and severe (11–12). One-way ANOVA revealed that patients in the moderate and severe groups had significantly elevated levels of inflammatory and coagulation markers, including WBC, platelet count, ESR, D-dimer, fibrinogen, CRP, IL-1β, IL-6, IL-17A, and TNF-α, compared to those in the mild group (p < 0.05). Conversely, BMI and hemoglobin levels were significantly lower in the moderate and severe groups (p < 0.05). However, there were no significant differences between the moderate and severe groups compared to the mild group regarding age and sex (p<0.05).
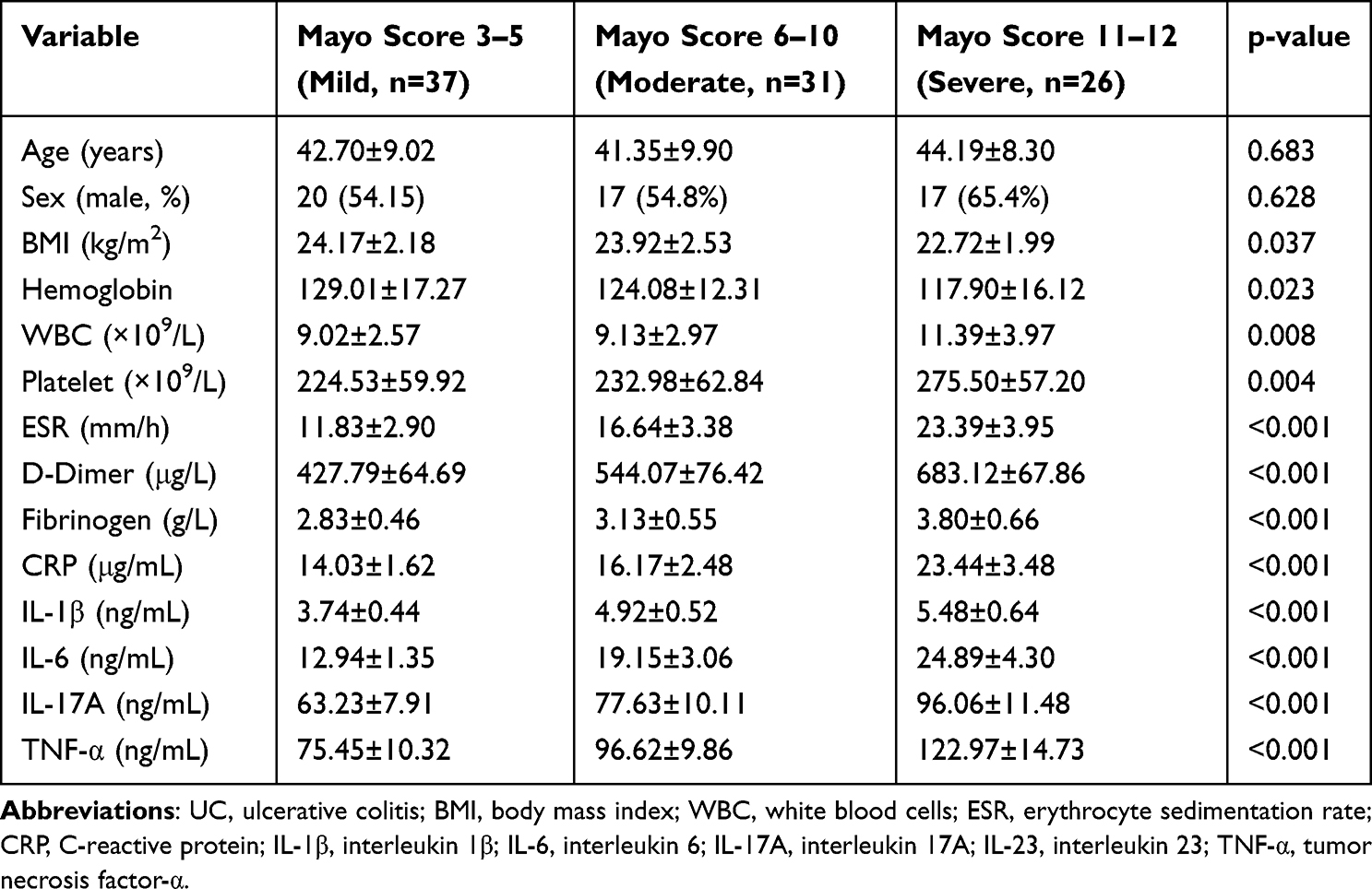 |
Table 2 Correlation Between Mayo Endoscopic Severity Scores and Clinical/Laboratory Parameters in Active UC Patients |
Podoplanin Expression is Abundant in Different Human Tissues
To investigate the expression of podoplanin in various human tissues, we utilized the online gene annotation and expression database BioGPS. The data from BioGPS revealed that podoplanin is extensively expressed in human tissues, with particularly high levels in the lymphatic endothelium, lungs, kidneys, and gastrointestinal tract (small intestine and colon) (Figure 2). The red arrow highlighting the small intestine and colon underlines the significance of podoplanin in these tissues, where it plays a role in epithelial function, immune regulation, and disease processes, such as cancer and inflammation.
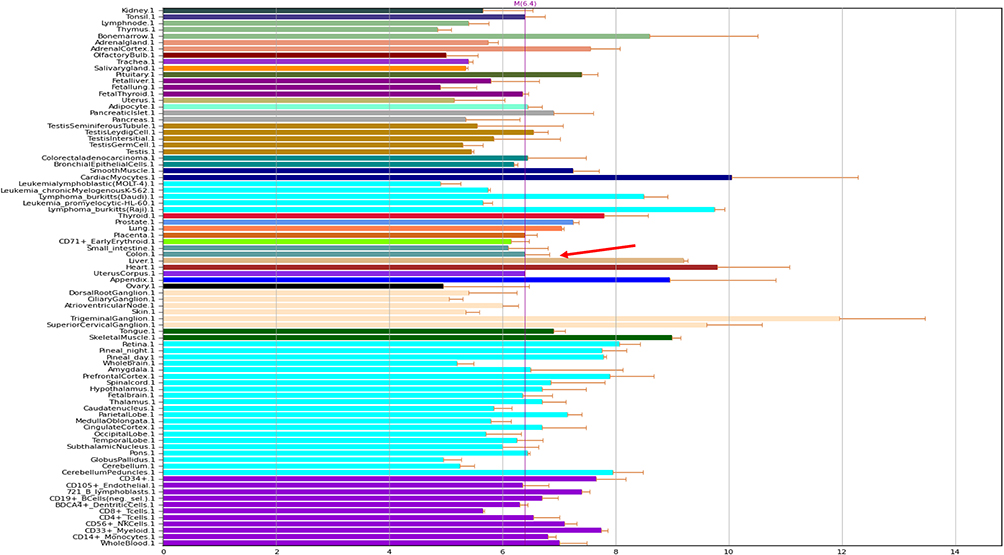 |
Figure 2 Abundance of podoplanin expression in different human tissues. The data were queried from the BioGPS database. The red arrow indicates the small intestine and colon. |
Comparison of Serum Podoplanin Levels in Healthy Controls and UC Patients
Serum podoplanin levels were measured using ELISA in patients with remission UC (n=115), active UC (n=94), and healthy controls (n=150). Active UC patients were further categorized into mild (n=37), moderate (n=31), and severe (n=26) subgroups. Initially, we compared serum podoplanin levels in healthy controls, UC in remission, and active UC patients. The levels were significantly higher in remission UC patients than in healthy controls and were further elevated in active UC patients (p < 0.001) (Figure 3A). Among active UC patients, podoplanin levels were significantly higher in the moderate group than in the mild group and were highest in the severe group (p < 0.001) (Figure 3B). ROC curve analysis demonstrated that serum podoplanin had excellent diagnostic performance in distinguishing active UC from remission and healthy controls, with an optimal cut-off value of 5.34 ng/mL (AUC = 0.926, 95% CI: 0.891–0.960, sensitivity = 80.9%, specificity = 88.7%) (Figure 3C). Among the evaluated biomarkers, podoplanin showed the highest AUC, outperforming conventional inflammatory markers such as ESR, CRP, fibrinogen, D-dimer, IL‑1β, and IL‑6 (Figure 3C). These findings indicate that serum podoplanin may serve as a reliable and sensitive biomarker for assessing disease activity in patients with UC.
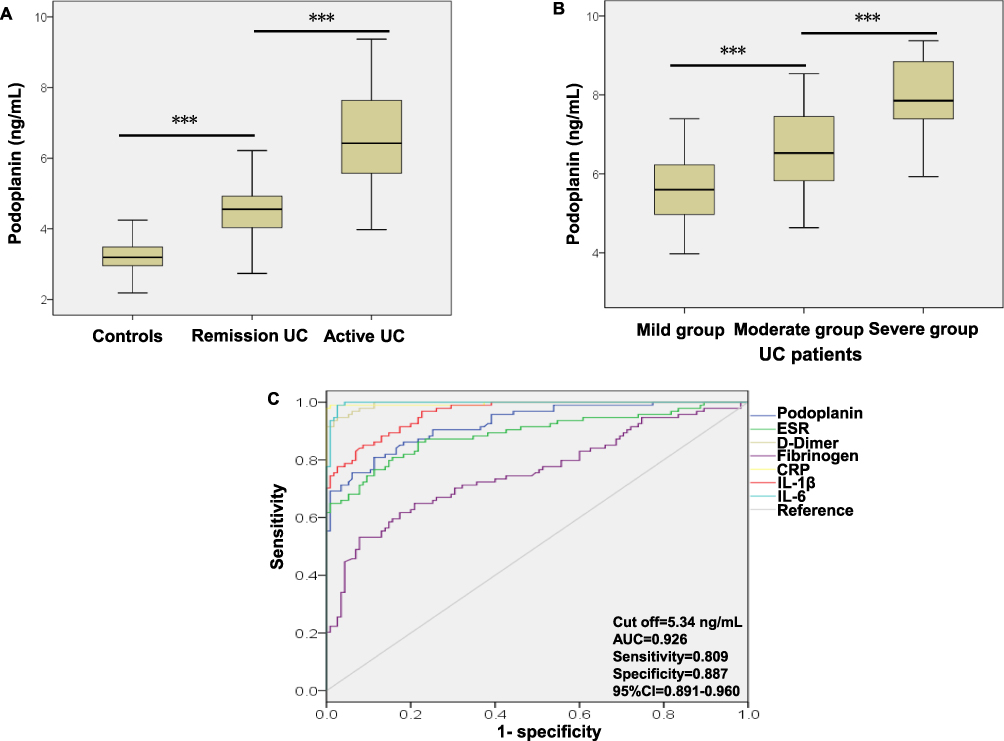 |
Figure 3 Comparison of serum podoplanin levels between healthy controls and patients with ulcerative colitis. (A) Serum podoplanin levels were compared between control subjects (n=150), remission UC patients (n=115), and active UC patients (n=94). Serum podoplanin concentration was measured using ELISA. (B) Serum podoplanin levels were compared in patients with UC in the mild (n = 37), moderate (n = 31), and severe (n = 26) groups. (C) The ROC curve was used to evaluate the diagnostic performance of serum podoplanin and to determine the optimal cutoff value for distinguishing active UC from remission and healthy controls. The optimal critical point was 5.34 ng/mL. The area under the curve was 0.926. ANOVA was used to compare the differences between the three groups. *** p<0.001. Abbreviation: UC, ulcerative colitis. |
Correlation Between Serum Podoplanin Levels and Coagulation-Related Indicators in Patients with UC
Pearson’s correlation analysis was used to investigate the relationship between serum podoplanin levels and coagulation-related indicators in patients with UC. We observed that serum podoplanin level is positively correlated with platelet count (r=0.247, p<0.001), ESR (r=0.695, p<0.001), D-Dimer (r=0.765, p<0.001), and fibrinogen (r=0.490, p<0.001) (Figure 4A–D).
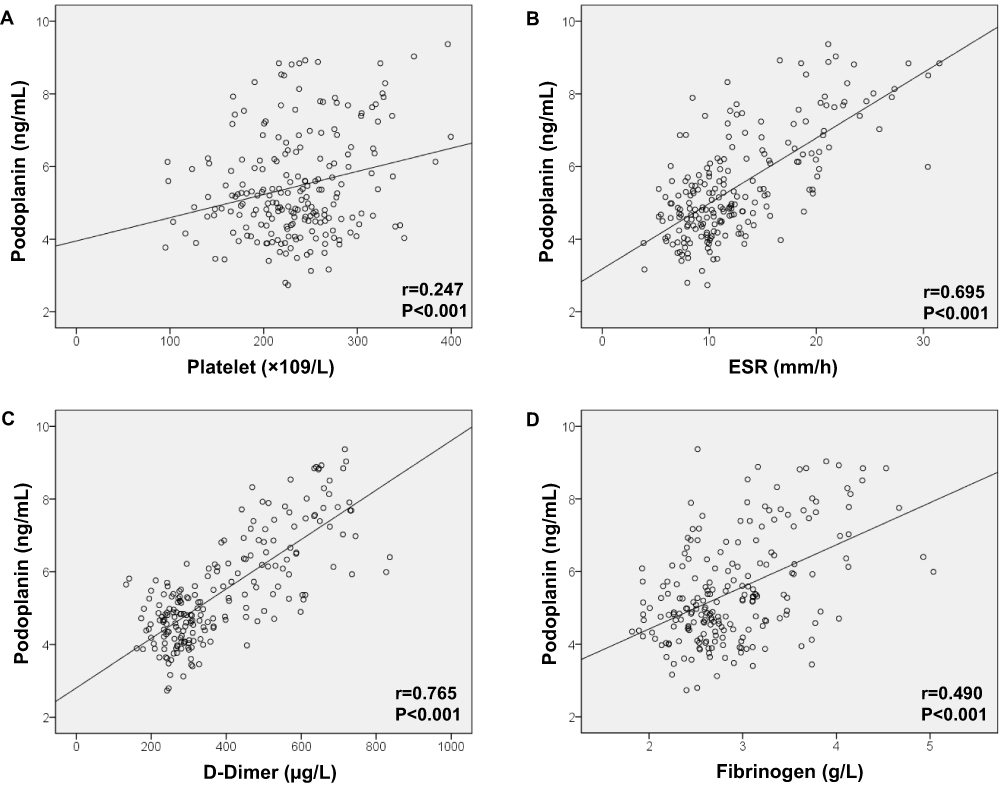 |
Figure 4 Correlation between serum podoplanin levels and coagulation-related indicators in patients with UC. Serum podoplanin levels were positively correlated with (A) platelet count, (B) ESR, (C) D-dimer, and (D) fibrinogen. Pearson’s correlation analysis was performed. Abbreviation: ESR, erythrocyte sedimentation rate. |
Correlation Between Serum Podoplanin Levels and Inflammatory Indicators of UC Patients
Pearson’s correlation analysis was also used to investigate the relationship between serum podoplanin levels and inflammatory indicators in patients with UC. We observed that serum podoplanin level is positively correlated with CRP (r=0.767, p<0.001), IL-1β (r=0.744, p<0.001), IL-6 (r=0.786, p<0.001), IL-17A (r=0.788, p<0.001), TNF-α (r=0.784, p<0.001), and Mayo score (r=0.912, p<0.001) (Figure 5A–F).
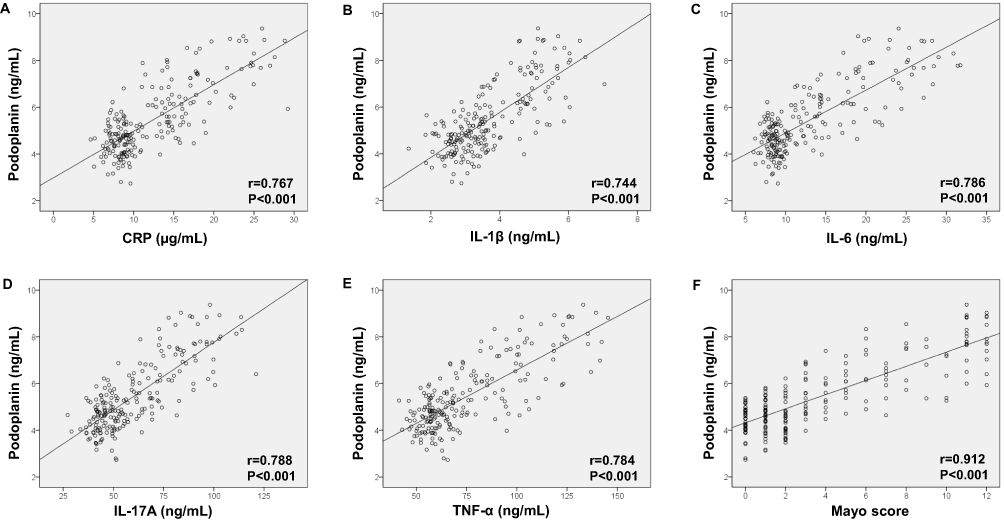 |
Figure 5 Correlation between serum podoplanin levels and inflammatory indicators in patients with ulcerative colitis. Serum podoplanin levels were positively correlated with (A) CRP, (B) IL-1β, (C) IL-6, (D) IL-17A, (E) TNF-α, and (F) Mayo score. Abbreviations: CRP, C-reactive protein; IL-1β, interleukin 1β; IL-6, interleukin 6; IL-17A, interleukin 17A; IL-23, interleukin 23; TNF-α, tumor necrosis factor-α. |
Regulation of Podoplanin in the Development of Ulcerative Colitis
Podoplanin is mainly expressed in the innate and adaptive immune systems during inflammation, and its expression is upregulated in macrophages following inflammatory stimulation by lipopolysaccharide (LPS), Toll-like receptor agonists, and tumor necrosis factor (TNF). Increased podoplanin levels in ulcerative colitis promote the release of inflammatory cytokines from the damaged intestinal mucosa, activate platelets, and increase platelet count, thereby exacerbating intestinal mucosal injury and the progression of ulcerative colitis. Therefore, the increase in podoplanin levels aggravates ulcerative colitis (Figure 6).
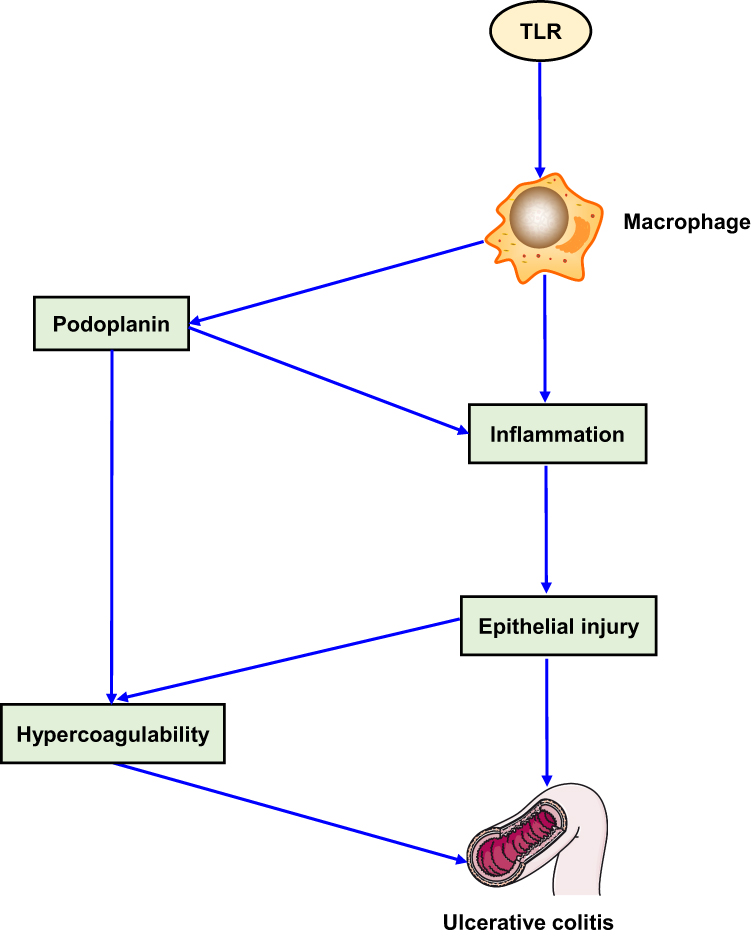 |
Figure 6 Schematic diagram of podoplanin in the development of ulcerative colitis. |
Discussion
In this study, we observed significantly elevated serum podoplanin levels in patients with UC, particularly in those with active disease compared to those in remission and healthy controls. This pattern was consistent with elevated levels of inflammatory markers (CRP, IL-1β, IL-6, IL-17A, and TNF-α) and coagulation-related indicators (platelets, D-dimer, ESR, and fibrinogen), suggesting a potential role of podoplanin as a biomarker for both inflammation and coagulation status in patients with UC. Our data further demonstrated a strong positive correlation between serum podoplanin levels and disease severity, as assessed by the Mayo score, as well as a gradual increase in podoplanin levels across the mild, moderate, and severe UC groups. These findings reinforce the hypothesis that podoplanin contributes to UC pathogenesis by mediating inflammation and coagulative responses.
Podoplanin is a transmembrane glycoprotein that plays a role in lymphatic vessel formation, inflammation, and thrombosis.12 Its expression has been linked to various inflammatory and thrombotic conditions, making it a potential biomarker for UC, a chronic inflammatory bowel disease characterized by mucosal inflammation and an increased risk of thrombosis.13,14 The results of this study align with current knowledge, suggesting that podoplanin levels reflect UC severity. Elevated serum podoplanin levels were observed in patients with moderate-to-severe disease activity compared to those with mild disease or healthy controls. This is consistent with the understanding that podoplanin expression is upregulated in inflamed tissues, including the colonic mucosa of patients with UC, where it may contribute to lymphatic dysfunction and immune cell recruitment.14 The correlation between podoplanin levels and disease severity underscores its potential as a biomarker for monitoring UC progression.
Previous studies have reported similar patterns of inflammation and hypercoagulability in patients with UC. For instance, a prior investigation highlighted the role of inflammatory cytokines, such as TNF-α, IL-6, and IL-1β, in patients with UC progression and their contribution to mucosal damage.15 Likewise, hypercoagulable states characterized by elevated platelet and fibrinogen levels have been well-documented in patients with UC and are considered to increase the risk of thromboembolic complications.16 The current findings add to this knowledge by positioning podoplanin as a molecule that bridges inflammatory and thrombotic pathways in patients with UC. Its positive correlation with CRP, D-dimer, and cytokine levels supports its involvement in the inflammatory response and coagulation cascade, consistent with previous research describing podoplanin as a platelet-activating molecule that facilitates thrombosis in inflammatory diseases.17
The relationship between serum podoplanin levels and the Mayo score further underscores its clinical relevance. The Mayo score remains the standard index for evaluating UC severity, integrating clinical, endoscopic, and physician-assessed components.18 Elevated podoplanin levels in patients with higher Mayo scores suggest that this marker may reflect both mucosal inflammation and broader vascular or fibroblast activation. This finding is consistent with previous research implicating podoplanin in tissue remodeling, leukocyte migration, and thrombogenesis in inflammatory settings.19
ROC curve analysis further demonstrated the strong diagnostic performance of podoplanin for distinguishing active UC from remission and healthy states (AUC = 0.926; optimal cutoff value = 5.34 ng/mL). Podoplanin outperformed conventional inflammatory markers (ESR, CRP, fibrinogen, and D‑dimer) and cytokines (IL‑1β and IL‑6) in terms of both sensitivity (80.9%) and specificity (88.7%). Although established markers such as CRP and fecal calprotectin are widely used to monitor UC, they often lack sufficient accuracy to differentiate active from quiescent disease.20,21 Given its biological role in inflammatory signaling and platelet activation,14,22 incorporating podoplanin measurements alongside established inflammatory markers could further enhance diagnostic precision, potentially improving disease monitoring and guiding timely therapeutic intervention.
Our proposed model (Figure 6) indicates that podoplanin may contribute to the pathogenesis of UC by promoting the release of inflammatory cytokines and platelet activation, thereby sustaining mucosal injury. This is in line with previous findings showing that podoplanin expression is upregulated in inflamed tissues, where it facilitates leukocyte recruitment and disrupts epithelial barrier integrity.22 Through its interactions with Toll-like receptors (TLRs) and TNF-α signaling pathways, podoplanin likely amplifies inflammatory responses, making it a potential therapeutic target.22,23 Although direct investigations of serum podoplanin levels in patients with UC are limited, our results align with those of studies on other inflammatory and thrombotic disorders. For example, elevated podoplanin levels have been associated with both inflammation and thrombosis in conditions such as rheumatoid arthritis and various malignancies,24 suggesting a common pathogenic mechanism in chronic inflammatory diseases. Nevertheless, longitudinal studies are warranted to determine causality and assess the potential of podoplanin as a biomarker for disease monitoring and treatment response in patients with UC.
The findings of our study suggest that serum podoplanin is a promising multifaceted biomarker for the clinical evaluation of UC, reflecting disease severity, inflammation, and coagulation status. Elevated levels of this protein may help guide risk stratification and therapeutic strategies, potentially improving patient outcomes. However, podoplanin is not a disease-specific marker; it is known to be upregulated in various inflammatory and neoplastic conditions, such as rheumatoid arthritis, squamous cell carcinoma, gliomas, and cardiovascular diseases, which may limit its specificity for UC diagnosis.25,26 Despite this limitation, emerging evidence indicates that podoplanin plays an active role in thrombosis via its interaction with C-type lectin-like receptor 2 (CLEC-2) on platelets, promoting platelet aggregation and thrombus formation.27 These characteristics, while biologically insightful, emphasize the need for cautious interpretation of podoplanin levels in patients with UC and highlight the necessity of multimodal biomarker strategies.
Compared with other emerging UC biomarkers, podoplanin has certain advantages. Although non-invasive and highly correlated with neutrophil infiltration and mucosal healing, fecal calprotectin lacks utility in predicting extraintestinal manifestations and complications.28 Similarly, serum CRP and ESR, although broadly reflective of systemic inflammation, lack specificity for colonic disease activity.29 Newer candidates, such as cytokines (OSM, IL-6, IL-8), have shown associations with treatment response but are limited by assay complexity and standardization challenges.30,31 MicroRNAs (eg, miR-21, miR-155) and metabolomic markers are mechanistically promising but not yet clinically routine.32,33 In contrast, podoplanin detection via ELISA is relatively accessible and reproducible, with the potential to bridge mechanistic relevance and clinical feasibility pending further validation.
Limitations
This study had several limitations that need to be acknowledged. First, as a cross-sectional study, it did not establish causality between serum podoplanin levels and the severity, coagulation state, and inflammation of UC. Second, the study was limited by the relatively small sample size, which could have reduced the statistical power and generalizability of the findings. Third, we used the publicly available gene expression database BioGPS for podoplanin expression analysis in different human tissues. Future studies should validate this using additional databases. Fourth, we failed to address some key confounding factors, including smoking, disease duration, and medications, which can potentially influence the inflammatory and coagulation profiles of patients with UC. Fifth, the current analysis did not include multivariate regression; therefore, the findings should be interpreted with caution, particularly in terms of the independent prognostic value of podoplanin. Sixth, although this study identified associations between podoplanin and UC severity, coagulation, and inflammation, the underlying mechanisms were not investigated in vitro and in vivo. Finally, this study relied on serum podoplanin as a single biomarker, which may not comprehensively capture the multifactorial nature of UC pathology. Future longitudinal studies with larger and more diverse cohorts and a broader range of biomarkers are needed to validate these findings and explore the mechanisms underlying these associations.
Conclusions
In summary, our study demonstrates that serum podoplanin levels are significantly elevated in patients with UC, correlate with disease severity, and are strongly associated with inflammatory and coagulation markers. These findings suggest that podoplanin may play a pathogenic role in patients with UC by promoting inflammation and thrombosis, highlighting its potential as a diagnostic and prognostic biomarker of UC. A more extensive population-based prospective study is needed to validate the potential role of serum podoplanin as a predictive biomarker in patients with UC.
Data Sharing Statement
The datasets used/analyzed during the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Ethics Committee of the Sijing Hospital approved this study (2024-SH-06). The authors followed all standard protocols in accordance with the 1964 Declaration of Helsinki. Informed consent was obtained from all participated subjects’ parents/legal guardians in the study.
Acknowledgment
We sincerely thank all of the participants in our study.
AI Declaration
We have used AI tool (DeepSeek) to prepare this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet. 2017;389(10080):1756–1770. doi:10.1016/S0140-6736(16)32126-2
2. Neurath MF. Current and emerging therapeutic targets for IBD. Nat Rev Gastroenterol Hepatol. 2017;14(5):269–278. doi:10.1038/nrgastro.2016.208
3. Astarita JL, Cremasco V, Fu J, et al. The CLEC-2–podoplanin axis controls the contractility of fibroblastic reticular cells and lymph node microarchitecture. Nat Immunol. 2015;16(1):75–84. doi:10.1038/ni.3035
4. Schacht V, Ramirez MI, Hong YK, et al. T1 /podoplanin deficiency disrupts normal lymphatic vasculature formation and causes lymphedema. EMBO J. 2003;22(14):3546–3556. doi:10.1093/emboj/cdg342
5. Suzuki-Inoue K, Kato Y, Inoue O, et al. Involvement of the snake toxin receptor CLEC-2, in podoplanin-mediated platelet activation, by cancer cells. J Biol Chem. 2007;282(36):25993–26001. doi:10.1074/jbc.M702327200
6. Danese S, Sans M, Fiocchi C. Inflammatory bowel disease: the role of environmental factors. Autoimmun Rev. 2004;3(5):394–400. doi:10.1016/j.autrev.2004.03.002
7. Geleff S, Schoppmann SF, Oberhuber G. Increase in podoplanin-expressing intestinal lymphatic vessels in inflammatory bowel disease. Virchows Archiv. 2003;442(3):231–237. doi:10.1007/s00428-002-0744-4
8. Quintanilla M, Montero-Montero L, Renart J, et al. Podoplanin in inflammation and cancer. Int J Mol Sci. 2019;20(3):707. doi:10.3390/ijms20030707
9. Bischoff SC, Bager P, Escher J, et al. ESPEN guideline on clinical nutrition in inflammatory bowel disease. Clin Nutr. 2023;42(3):352–379. doi:10.1016/j.clnu.2022.12.004
10. Wu C, Orozco C, Boyer J, et al. BioGPS: an extensible and customizable portal for querying and organizing gene annotation resources. Genome Biol. 2009;10(11):R130. doi:10.1186/gb-2009-10-11-r130
11. Wang Y, Li C, Wang W, et al. Serum albumin to globulin ratio is associated with the presence and severity of inflammatory bowel disease. J Inflamm Res. 2022;15:1907–1920. doi:10.2147/JIR.S347161
12. Carrasco-Ramírez P, Greening DW, Andrés G, et al. Podoplanin is a component of extracellular vesicles that reprograms cell-derived exosomal proteins and modulates lymphatic vessel formation. Oncotarget. 2016;7(13):16070–16089. doi:10.18632/oncotarget.7445
13. Hellmann J, Ta A, Ollberding NJ, et al. Patient-reported outcomes correlate with microbial community composition independent of mucosal inflammation in pediatric inflammatory bowel disease. Inflamm Bowel Dis. 2023;29(2):286–296. doi:10.1093/ibd/izac175
14. Astarita JL, Acton SE, Turley SJ. Podoplanin: emerging functions in development, the immune system, and cancer. Front Immunol. 2012;3:283. doi:10.3389/fimmu.2012.00283
15. Danese S, Papa A, Saibeni S, Repici A, Malesci A, Vecchi M. Inflammation and coagulation in inflammatory bowel disease: the clot thickens. Am J Gastroenterol. 2007;102(1):174–186. doi:10.1111/j.1572-0241.2006.00943.x
16. Papa A, Laterza L, Papa V, et al. Vascular complications in hospitalized patients with inflammatory bowel disease and acute gastroenteritis and colitis: a propensity score-matched study. Dig Liver Dis. 2025;57(5):547–555. doi:10.1016/j.dld.2025.01.195
17. Martín-Villar E, Scholl FG, Gamallo C, et al. Characterization of human PA2.26 antigen (T1alpha-2, podoplanin), a small membrane mucin induced in oral squamous cell carcinomas. Int J Cancer. 2005;113(6):899–910. doi:10.1002/ijc.20656
18. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987;317(26):1625–1629. doi:10.1056/NEJM198712243172603
19. Suzuki H, Kaneko MK, Kato Y. Roles of podoplanin in malignant progression of tumor. Cells. 2022;11(3):575. doi:10.3390/cells11030575
20. Henriksen M, Jahnsen J, Lygren I, et al. C-reactive protein: a predictive factor and marker of inflammation in inflammatory bowel disease. Results from a prospective population-based study. Gut. 2008;57(11):1518–1523. doi:10.1136/gut.2007.146357
21. Taghvaei T, Maleki I, Nagshvar F, et al. Fecal calprotectin and ulcerative colitis endoscopic activity index as indicators of mucosal healing in ulcerative colitis. Intern Emerg Med. 2015;10(3):321–328. doi:10.1007/s11739-014-1144-x
22. Yu J, Xu W, Gao J, et al. The role of podoplanin in the immune system and inflammation. J Inflamm Res. 2022;15:3561–3572. doi:10.2147/JIR.S366620
23. Kerrigan AM, Navarro-Nuñez L, Pyz E, et al. Podoplanin-expressing inflammatory macrophages activate murine platelets via CLEC-2. J Thromb Haemost. 2012;10(3):484–486. doi:10.1111/j.1538-7836.2011.04614.x
24. Wicki A, Christofori G. The potential role of podoplanin in tumour invasion. Br J Cancer. 2007;96(1):1–5. doi:10.1038/sj.bjc.6603518
25. Martín-Villar E, Megías D, Castel S, Yurrita MM, Vilaró S, Quintanilla M. Podoplanin binds ERM proteins to activate RhoA and promote epithelial-mesenchymal transition. J Cell Sci. 2006;119(21):4541–4553. doi:10.1242/jcs.03218
26. Krishnan H, Rayes J, Miyashita T, et al. Podoplanin: an emerging cancer biomarker and therapeutic target. Cancer Sci. 2018;109(5):1292–1299. doi:10.1111/cas.13580
27. Suzuki-Inoue K, Fuller GL, García A, et al. A novel Syk-dependent mechanism of platelet activation by the C-type lectin receptor CLEC-2. Blood. 2006;107(2):542–549. doi:10.1182/blood-2005-05-1994
28. Rokkas T, Portincasa P, Koutroubakis IE. Fecal calprotectin in assessing inflammatory bowel disease endoscopic activity: a diagnostic accuracy meta-analysis. J Gastrointestin Liver Dis. 2018;27(3):299–306. doi:10.15403/jgld.2014.1121.273.pti
29. Vermeire S, Van Assche G, Rutgeerts P. C-reactive protein as a marker for inflammatory bowel disease. Inflamm Bowel Dis. 2004;10(5):661–665. doi:10.1097/00054725-200409000-00026
30. West NR, Hegazy AN, Owens BMJ, et al. Oncostatin M drives intestinal inflammation and predicts response to tumor necrosis factor–neutralizing therapy in patients with inflammatory bowel disease. Nat Med. 2017;23(5):579–589. doi:10.1038/nm.4307
31. Bertani L, Caviglia GP, Antonioli L, et al. Serum interleukin-6 and −8 as predictors of response to vedolizumab in inflammatory bowel diseases. J Clin Med. 2020;9(5):1323. doi:10.3390/jcm9051323
32. Wu F, Guo NJ, Tian H, et al. Peripheral blood MicroRNAs distinguish active ulcerative colitis and Crohnʼs disease. Inflamm Bowel Dis. 2011;17(1):241–250. doi:10.1002/ibd.21450
33. Huang H, Vangay P, McKinlay CE, Knights D. Multi-omics analysis of inflammatory bowel disease. Immunol Lett. 2014;162(2):62–68. doi:10.1016/j.imlet.2014.07.014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Role of Podoplanin in the Immune System and Inflammation
Zhang Z, Zhang N, Yu J, Xu W, Gao J, Lv X, Wen Z
Journal of Inflammation Research 2022, 15:3561-3572
Published Date: 17 June 2022
Prognostic Role of Serum Soluble Tim-3 in Severe Traumatic Brain Injury: A Prospective Observational Study
Zhang H, Lv QW, Zheng ZQ, Shen LJ, Zhou J, Guo M
Neuropsychiatric Disease and Treatment 2023, 19:153-169
Published Date: 18 January 2023
Evaluation of Serum NLRC4 as a Potential Prognostic Biochemical Marker in Humans with Severe Traumatic Brain Injury: A Prospective Cohort Study
Tang B, Zhong Z, Wu J, Ma J, Li L, Zhong X, Lin D, Hu J, Yu P
Risk Management and Healthcare Policy 2023, 16:439-454
Published Date: 23 March 2023
The Impact of Obesity on the Host–Pathogen Interaction with Influenza Viruses – Novel Insights: Narrative Review
Miron VD, Drăgănescu AC, Pițigoi D, Aramă V, Streinu-Cercel A, Săndulescu O
Diabetes, Metabolic Syndrome and Obesity 2024, 17:769-777
Published Date: 13 February 2024
Quzhou Aurantii Fructus Flavonoids Ameliorate Inflammatory Responses, Intestinal Barrier Dysfunction in DSS-Induced Colitis by Modulating PI3K/AKT Signaling Pathway and Gut Microbiome

Wang H, Huang W, Pan X, Tian M, Chen J, Liu X, Li Q, Qi J, Ye Y, Gao L
Journal of Inflammation Research 2025, 18:1855-1874
Published Date: 6 February 2025