Back to Journals » Clinical Ophthalmology » Volume 20
Efficacy of Punctal Occlusion Techniques in Tear Drainage Disorders: A Systematic Review and Meta-Analysis
Authors Qutub MF, Almarwani S, Alsifri A ![]() , Alshareef W, Shaheen MH
, Alshareef W, Shaheen MH ![]() , Alajmi T, Alnashri R, Alharbi S, Ageel S, Aljadani HT
, Alajmi T, Alnashri R, Alharbi S, Ageel S, Aljadani HT ![]() , Alsulami MN
, Alsulami MN ![]()
Received 29 November 2025
Accepted for publication 12 May 2026
Published 29 June 2026 Volume 2026:20 584168
DOI https://doi.org/10.2147/OPTH.S584168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Mohammed F Qutub,1– 3 Salma Almarwani,1,2 Alanoud Alsifri,1,2 Wasan Alshareef,1,2 Marya Hassan Shaheen,1,2 Talal Alajmi,1,2 Rahaf Alnashri,1,2 Sereen Alharbi,1,2 Suzan Ageel,1,2 Hanan T Aljadani,1,2 Maria N Alsulami1,2
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia; 3Ophthalmology Department, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Jeddah, Saudi Arabia
Correspondence: Salma Almarwani, Email [email protected]
Introduction: Tear drainage dysfunction, presenting as epiphora or dry eye symptoms, significantly affects quality of life. Punctal occlusion, using temporary or permanent techniques, aims to retain tears and improve ocular surface health. However, the overall efficacy and safety of these techniques remain variably reported across studies.
Methods: This systematic review and meta-analysis followed PRISMA 2020 guidelines and was registered on PROSPERO (CRD42024607753). A comprehensive search of PubMed, MedLine, ScienceDirect, and the Cochrane Library yielded 1550 studies. After screening and eligibility assessment, 14 studies were included. Data extraction covered study design, plug type, follow-up duration, and clinical outcomes. Meta-analyses were performed using Review Manager 5.4.
Results: Fourteen studies involving 1537 patients (1155 eyes) were analyzed. Punctal occlusion techniques included silicone, collagen, SmartPlugs, and thermal cautery. Meta-analysis revealed no significant improvements in tear film break-up time (WMD = 0.37; 95% CI: − 0.94 to 1.67; p = 0.58), Schirmer scores (WMD = 0.61; 95% CI: − 0.96 to 2.18; p = 0.45), or fluorescein staining (WMD = − 0.38; 95% CI: − 0.92 to 0.16; p = 0.17) compared to controls. However, within group analysis based on follow up period of Schirmer test demonstrated significant improvement (p= 0.01). Reported adverse events were minor and self-limiting.
Conclusion: Punctal occlusion techniques offer consistent ocular surface benefits with minimal risks. While current evidence highlights positive clinical outcomes, high-quality randomized controlled trials with standardized metrics are necessary to establish definitive efficacy.
Keywords: punctal occlusion, punctal plugs, dry eye disease, ocular surface disease
Introduction
Epiphora, excessive tearing, arises when there is an imbalance between tear secretion and drainage. This disruption can lead to dry-eye symptoms.1 Dry eye syndrome (DES) is a condition in which the tear film that usually protects the surface of the eye becomes unstable and breaks down. Loss of the tear film in different places of the cornea and conjunctiva leads to irritation and reduced visual acuity.2 It can be due to systemic autoimmune diseases (Sjögren’s syndrome, graft-versus-host disease, lupus, and rheumatoid arthritis), dry weather, hormonal changes, contact lens use, and medications.3 One of the most frequent complaints in eye clinics is dry eye disease. Globally, the prevalence of DES varies widely ranging from approximately 5% to 50%, depending on diagnostic criteria, study design, and population characteristics.4 In Saudi Arabia, around 32.1% of adults have DES.5
First-line management consists of treating the underlying cause, followed by the use of artificial tears or lubricating eye drops.6 Punctal plugs are devices placed in the tear ducts to reduce tear drainage and increase tear retention on the ocular surface. They can be classified by duration into temporary (absorbable or silicone) and permanent (thermal cautery and laser ablation).7,8 Silicone punctal plugs have been used in various types of dry eye associated with aqueous tear deficiency, such as Sjögren’s syndrome, superior limbic keratoconjunctivitis, post-keratoplasty, and Stevens-Johnson syndrome.9–11 The primary indication for punctal plugs is moderate to severe aqueous-deficient dry eye. They may serve as adjuvant therapy for Sjögren’s syndrome, graft-versus-host disease, and for patients with poorly controlled disease by increasing contact time and tolerance to topical treatments through decreased tear drainage. However, clinical outcomes vary across patient populations, and complications such as plug extrusion, ocular discomfort, and epiphora have been reported. The effectiveness of punctal plugs remains debated, particularly in the absence of well-designed comparative trials.8,12,13 Despite the widespread clinical use of punctal occlusion, well designed comparative studies evaluating its effectiveness remains limited. This systematic review aims to determine the effectiveness of punctal occlusion techniques in improving symptoms and tear stability for patients with tear drainage disorder.
Methods
Protocol and Registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines.14 A protocol outlining the objectives, eligibility criteria, and analysis methods was developed and registered prior to the commencement of the review. The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number [CRD42024607753].
Eligibility Criteria
Studies were eligible for inclusion if they evaluated the use of punctal plugs in the treatment of dry eye disease or epiphora among human subjects. Both randomized controlled trials (RCTs) and non-randomized studies assessing clinical outcomes related to punctal plug use were considered. Eligible studies were required to be full-text articles published in English in peer-reviewed journals. Studies were excluded if they included irrelevant populations (such as non-ocular conditions), assessed interventions unrelated to punctal plugs, did not report relevant outcome data, or were not available in full-text English.
Information Sources
A comprehensive literature search was conducted across four electronic databases: PubMed, ScienceDirect, MedLine, and the Cochrane Library. The search retrieved 226 records from PubMed, 899 from ScienceDirect, 372 from MedLine, and 53 from the Cochrane Library. No publication date restrictions were applied, and the search included all literature available up to the date of screening.
Search Strategy and Study Selection
The search strategy combined Medical Subject Headings (MeSH) and relevant free-text terms such as “punctal plugs”, “dry eye”, “epiphora”, “lacrimal occlusion”, “ocular surface”, “punctal occlusion”, “tear drainage disorders”, “dry eye syndrome”, “efficacy”, “symptoms relief”, “tear stability”, and “ocular surface health”. Boolean operators (AND, OR) were employed to combine search terms, and the strategy was adapted according to each database’s indexing system. Because punctal occlusion is clinically used to modify tear retention and drainage, studies evaluating its use in both dry eye disease and epiphora were considered eligible despite the differing underlying pathophysiology of these conditions. 1550 articles were screened by title and abstract resulting in the exclusion of 1515 records. Full-text versions of 35 articles were retrieved for further assessment, and 14 studies met the inclusion criteria and were included in the final review. Two reviewers independently conducted the screening and selection process, resolving any discrepancies through discussion and consensus.
Data Collection
Data extraction was carried out independently by two reviewers using a standardized data collection form. The extracted information included the author’s name, year of publication, country, study design (RCT or non-randomized), sample size, patient demographics (age and gender), details of comparison groups, indications for punctal plug use (dry eye or epiphora), type and material of the plug, duration of follow-up, and measured outcomes such as symptom improvement, tear film parameters, plug retention, and adverse events. When reported, the number of eyes rather than the number of participants was used as the unit of analysis.
Risk of Bias Assessment and Critical Appraisal
The risk of bias in randomized controlled trials was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool, which evaluates five domains: the randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results (supplementary Figure1).15 For non-randomized studies, the ROBINS-I tool was used to assess bias across seven domains: confounding, participant selection, intervention classification, deviations from intended interventions, missing data, outcome measurement, and selective reporting (supplementary Figure2).16 For case-series, Joanna Briggs Institute’s (JBI) Critical appraisal checklist was used (supplementary Table1).17 Each study was independently evaluated by two reviewers, and any conflicts were resolved through discussion or with the involvement of a third reviewer.
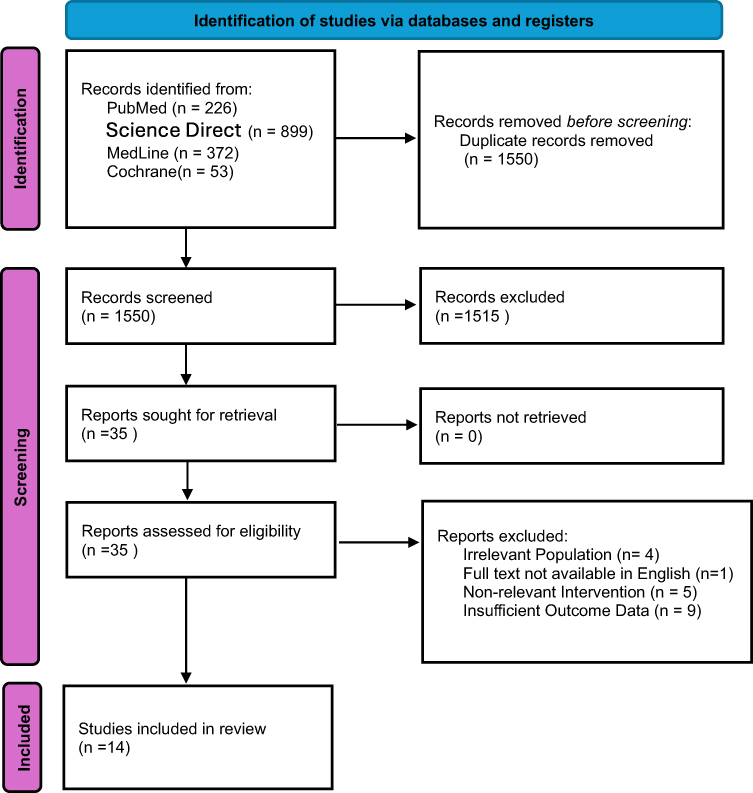 |
Figure 1 PPRISMA for screening and selection of included studies. |
 |
Figure 2 Forest plot for Tear film break up time (TFBUT). Forest plot comparing the mean change in TFBUT between the intervention group and the control group. Each green square represents the effect estimate for an individual study, and the size of the square reflects the weight assigned to that study in the meta-analysis. Horizontal lines indicate the 95% confidence intervals (CIs). The vertical line represents no effect between groups. The pooled overall effect (fixed/random effects model) demonstrated a significant improvement in TFBUT in the intervention group compared with the control group. Statistical heterogeneity among studies was assessed using the Chi2 test and I2 statistic. |
Synthesis and Statistical Analysis
Quantitative data were analyzed using Review Manager (RevMan) version 5.4 (Cochrane Collaboration). Meta-analyses were conducted using a random-effects model to account for potential heterogeneity among studies. Statistical significance was determined at the P < 0.05, threshold, and pooled outcomes were presented with 95% confidence intervals (CIs). Heterogeneity was assessed using the I2 statistic; values exceeding 50% indicate moderate to substantial heterogeneity. Forest plots were generated using the number of eyes as the unit of analysis, in line with the reporting in the included studies. Subgroup analyses were performed where data permitted; however, their interpretation was limited due to the small number of studies in certain categories, a limitation discussed further in the Discussion section.
Results
Systematic search initially identified 1550 potential studies across four databases: PubMed (n=226), ScienceDirect (n=899), MEDLINE (n=372), and the Cochrane Library (n=53). After a thorough process of removing duplicate papers and a rigorous eligibility assessment, 1515 studies were deemed ineligible for inclusion, leading to the final inclusion of 14 studies in accordance with the predetermined criteria (Figure 1).
Study Characteristics
The final set of included studies consisted of a diverse range of study designs, encompassing six randomized controlled trials (RCTs), four retrospective cohort studies, and four prospective or interventional case series. In total, these studies incorporated a collective sample of 1537 participants and 1155 eyes. In several studies, clinical outcomes were reported per eye rather than per participant, meaning that both eyes from some participants were included in the analysis. This approach may introduce inter-eye correlation, and therefore the results were interpreted with caution. The reported number of analyzed eyes may also represent an underestimate, as two included studies, Louis Tong et al and Rohan Bir Singh et al, did not clearly specify whether outcomes were reported for one eye or both eyes of enrolled participants, nor did they provide the exact number of eyes analyzed.10–18 Consequently, the precise unit of analysis could not be fully determined for these studies. This limitation has been acknowledged and considered. Among these, the majority underwent punctal plug implantation, with silicone and collagen plugs being the most commonly used types (Table 1).
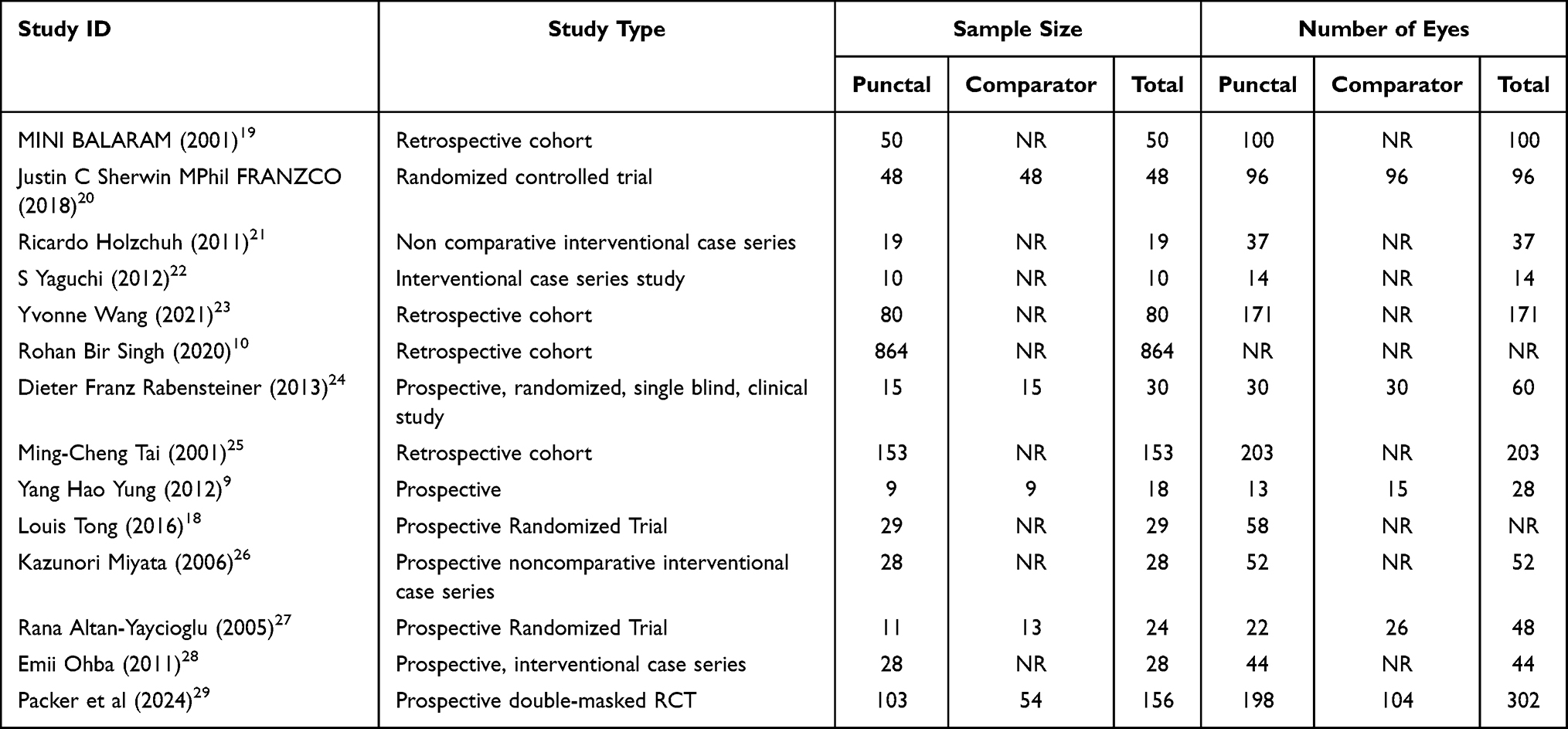 |
Table 1 Study Characteristics |
Tear Film Break-Up Time (TFBUT)
Four studies reported comparative data on tear film break-up time between punctal plug groups and control groups and were included in the meta-analysis (Figure 2). Where reported in the original studies, control groups consisted of either contralateral untreated eyes or separate control participants. However, not all studies hve specified the structure of the control group. The pooled analysis demonstrated no statistically significant difference between the punctal plug and control groups (WMD = 0.37; 95% CI: −0.94 to 1.67; p = 0.58). However, substantial heterogeneity was observed among studies (I2 = 85%). The subgroup analysis based on follow-up duration revealed no statistically significant difference at either less than 3 months (WMD = 1.20; 95% CI: −1.23 to 3.64; p = 0.33) or after 3 months follow-up (WMD = −0.24; 95% CI: −0.97 to 0.49; p = 0.53) (Figure 3).
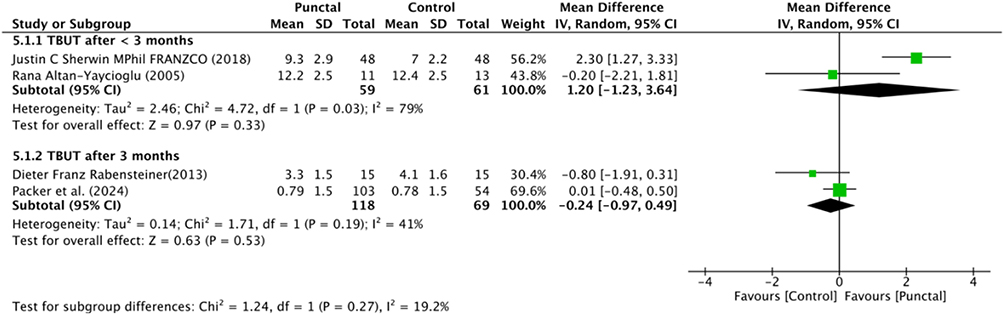 |
Figure 3 Forest plot for Tear film break up time (subgroup analysis). Subgroup analysis evaluating the effect of the intervention on TFBUT at different follow-up time points. Studies were grouped according to follow-up duration. Each square represents an individual study and the pooled effect within each subgroup is shown as a diamond. The analysis allows comparison of treatment effects across different follow-up periods and helps assess the consistency of the intervention effect over time. |
In addition to the comparative data, six studies provided within group, pre and post punctual plug data on TFBUT (Table 2). These studies consistently reported statistically significant improvements following punctal plug insertion. For instance, S. Yaguchi et al (2012) reported an increase in TFBUT from 2.6 ± 1.2 seconds at baseline to 8.1 ± 2.8 seconds post-intervention (p = 0.002).22 Similarly, Emii Ohba et al (2011) observed an improvement from 1.3 ± 1.1 seconds to 4.6 ± 2.4 seconds (p < 0.0001), and Ricardo Holzchuh et al (2011) reported an increase from 1.19 ± 1.68 to 2.49 ± 1.98 seconds (p = 0.006).21,28
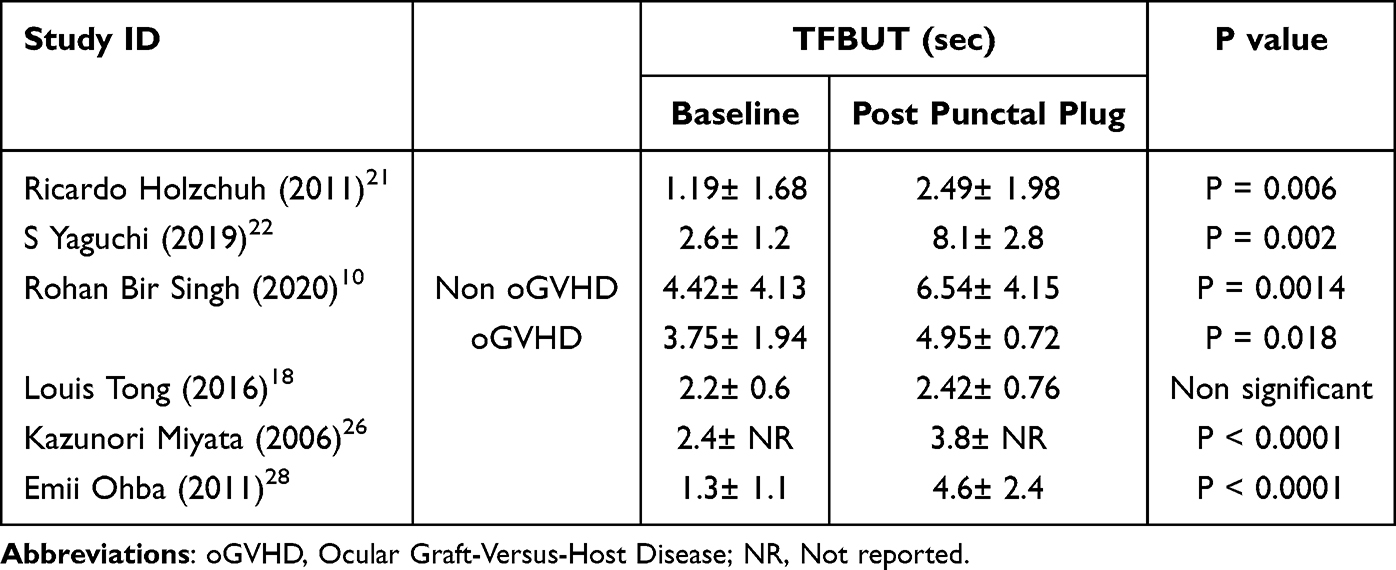 |
Table 2 Tear Film Break up Time (TFBUT) |
Schirmer Test
Three studies provided comparative data on Schirmer test scores and were included in the meta-analysis (Figure 4). The pooled analysis showed no statistically significant difference between punctal plug and control groups (WMD = 0.61; 95% CI: −0.96 to 2.18; p = 0.45). Subgroup analyses based on different follow-up duration showed no significant differences at less than 3 months (WMD = −0.19; 95% CI: −0.84 to 0.46; p = 0.57) and at 3 months it showed a borderline improvement favoring punctal plugs, though this did not reach statistical significance (WMD = 1.72; 95% CI: −0.04 to 3.48; p = 0.05). However, a statistically significant improvement favoring punctal plug insertion was observed at 6 months follow-up (WMD = 2.00; 95% CI: 0.32 to 3.68; p = 0.02), moderate heterogeneity was noted (Figure 5).
 |
Figure 4 Forest plot for Schirmer test. Forest plot comparing the mean change in Schirmer test results between intervention and control groups. Each green square indicates the mean difference for an individual study with its corresponding weight in the meta-analysis. Horizontal lines represent the 95% confidence intervals. The diamond represents the pooled mean difference with its 95% CI. The pooled analysis indicates an overall improvement in tear production in the intervention group compared with the control group. Heterogeneity among studies was evaluated using the Chi2 test and the I2 statistic. |
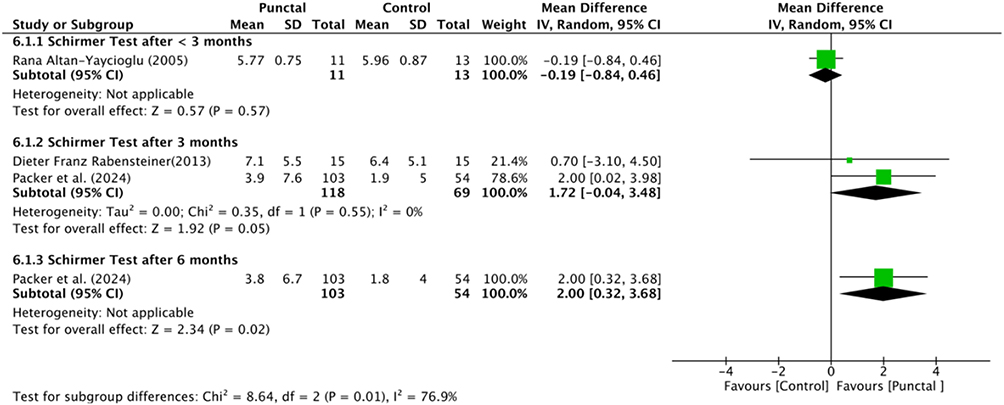 |
Figure 5 Forest plot for Schirmer test (subgroup analysis). Forest plot showing subgroup analysis of Schirmer test outcomes according to follow-up duration. Individual study results are presented as squares with corresponding 95% confidence intervals. The pooled estimates within each subgroup are represented by diamonds, illustrating the overall effect at different follow-up time points. |
Additionally, significant improvements in tear production were consistently observed following punctal plug placement in five studies (Table 3). Ricardo Holzchuh et al (2011) reported a significant increase from 2.7 ± 2.55 mm at baseline to 8.92 ± 7.2 mm post-intervention (p < 0.0001).21 Similarly, S. Yaguchi et al (2019) documented improvement from 1.9 ± 2.1 mm to 6.3 ± 2.6 mm (p = 0.002), while Emii Ohba et al (2011) showed an increase from 2.6 ± 3.9 mm to 6 ± 5.3 mm (p = 0.0003).22,28
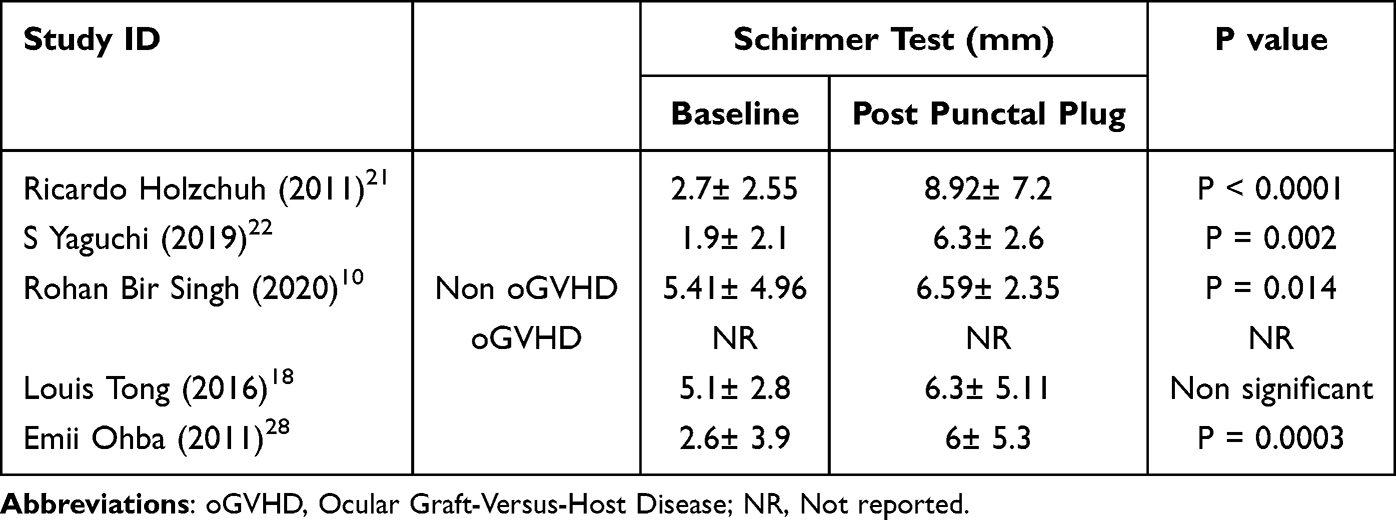 |
Table 3 Schirmer Test Score |
Corneal Fluorescence Staining
Two studies reported comparative data on corneal fluorescein staining scores and were included in the meta-analysis. The pooled analysis showed no statistically significant difference between groups (WMD = −0.38; 95% CI: −0.92 to 0.16; p = 0.17). (Figure 6).
 |
Figure 6 Forest plot for corneal Fluorescence Staining. Forest plot illustrating the comparison of fluorescein staining scores between the intervention and control groups. Each square corresponds to the effect size from an individual study, while the horizontal lines indicate the 95% confidence intervals. The pooled effect estimate suggests a reduction in fluorescein staining scores in the intervention group, indicating improvement in ocular surface integrity. The overall pooled effect and heterogeneity statistics are presented. |
Six studies have showed significant results after punctal plug insertion (Table 4). Ricardo Holzchuh et al (2011) reported a significant decrease in corneal staining scores from 4.08 ± 2.53 at baseline to 2.73 ± 0.074 post intervention (p = 0.003).21 S. Yaguchi et al (2019) observed a reduction from 6.1 ± 1.1 to 1.3 ± 0.8 (p = 0.002), and Emii Ohba et al (2011) showed improvement from 4.5 ± 2.8 to 1.1 ± 1.7 (p < 0.0001).22,28
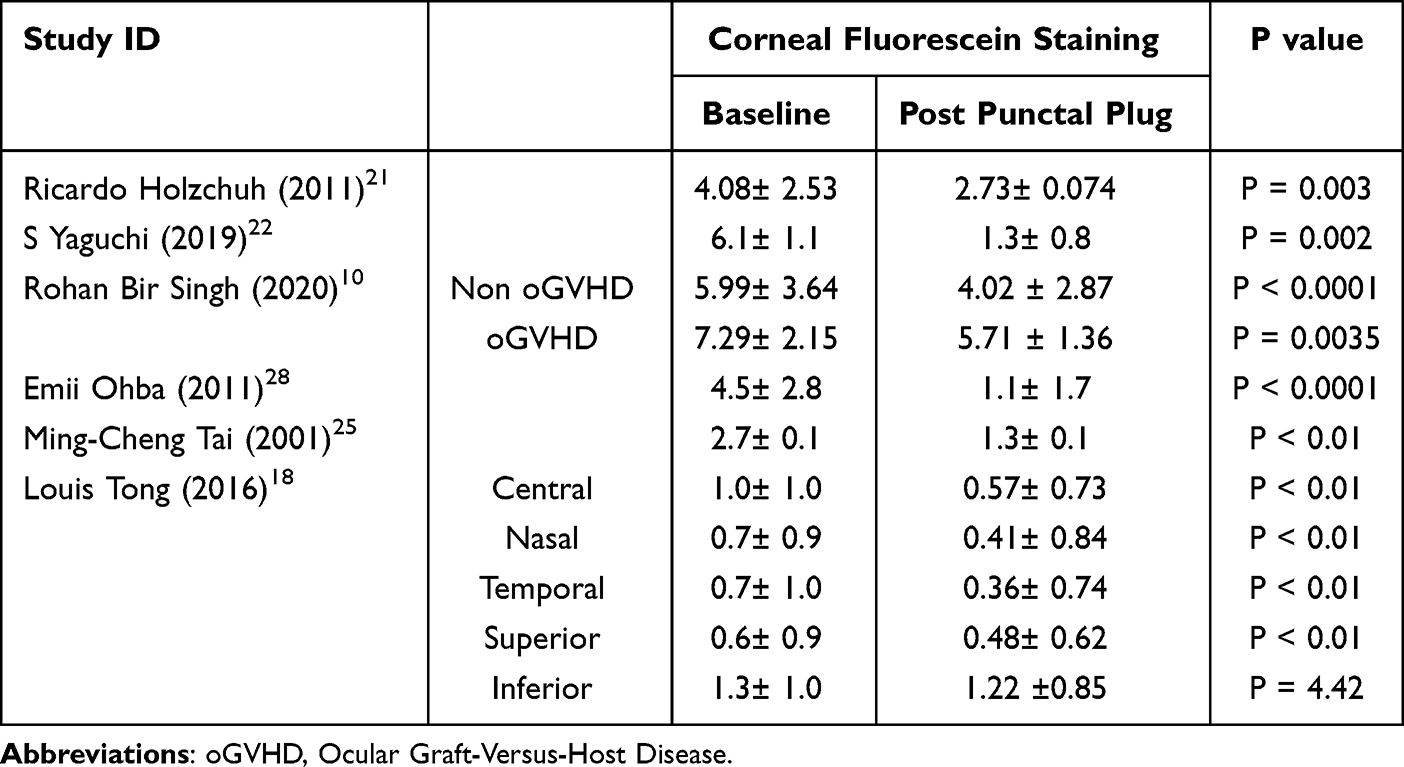 |
Table 4 Corneal Fluorescein Staining |
Rose Bengal Staining
The pooled analysis demonstrated no statistically significant difference between the two groups (WMD = −0.18; 95% CI: −0.75 to 0.40; p = 0.55). (Figure 7).
 |
Figure 7 Forest plot for Rose bengal staining. Forest plot comparing Rose Bengal staining scores between intervention and control groups. Each green square represents the mean difference for an individual study, and the size reflects the relative study weight. Horizontal lines indicate the 95% confidence intervals. The pooled diamond shows the overall effect estimate. The analysis suggests a decrease in staining scores in the intervention group compared with the control group, indicating improvement in ocular surface damage. |
Three studies provided reported a significant decrease in staining after punctal insertion (Table 5). Ricardo Holzchuh et al (2011) showed a decrease in staining from 4.95 ± 2.73 at baseline to 3.16 ± 1.8 post-intervention (p = 0.0002).21 Similarly, S. Yaguchi et al (2019) observed a reduction from 5.6 ± 1.5 to 2.1 ± 2.0 (p = 0.002), and Emii Ohba et al (2011) reported an improvement from 4.4 ± 2.7 to 2.4 ± 1.6 (p = 0.02).28
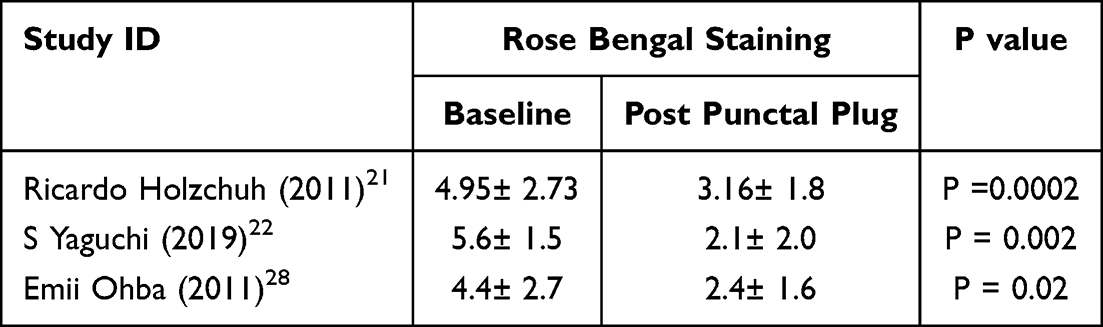 |
Table 5 Rose Bengal Staining |
Adverse Events
Adverse events associated with punctal plug insertion were reported in five studies (Table 6). The most frequently reported complications included ocular discomfort (n = 778), ocular redness (n = 221), ocular pain (n = 112), blurred vision (n = 101), and plug extrusion (total extrusion, n = 103; partial extrusion, n = 5). Other reported complications included epiphora, subconjunctival hemorrhage, conjunctival erosion, temporary eyelid pain, blepharitis, procedural pain, temporary swelling, and plug fragmentation. Most adverse events were mild and resolved spontaneously or required minimal intervention.
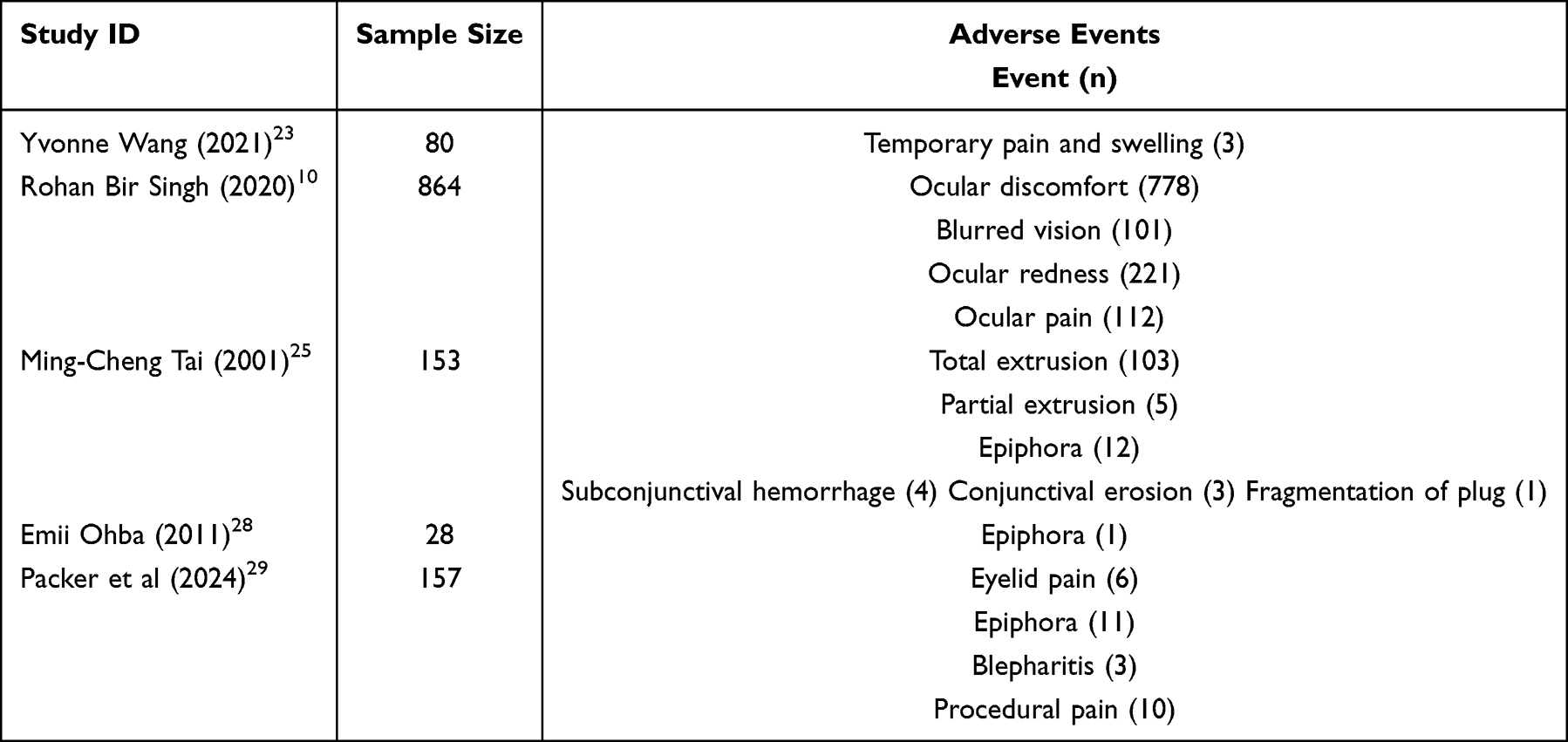 |
Table 6 Summary of Adverse Events |
Discussion
This systematic review of 14 studies involving 1567 participants, punctal occlusion (via silicone or collagen plugs, SmartPlugs, or thermal/surgical cautery) demonstrated variable outcomes across standard dry eye metrics.
Comparative meta-analyses revealed no significant improvements in tear film break-up time (TFBUT) or Schirmer test values compared with control groups, reflecting high inter-study heterogeneity, small sample sizes, and inconsistent protocols. However, within-group pre–post analyses consistently showed significant enhancements in both TFBUT and tear production, indicating potential individual-level benefits. These within-group improvements should nonetheless be interpreted with caution, as they are susceptible to placebo effects, regression to the mean, and the influence of concomitant treatments, all of which may contribute to apparent gains independent of the intervention itself. In contrast, corneal fluorescein staining scores were markedly improved in patients receiving punctal occlusion (mean difference ≈ -0.47; p < 0.00001), with substantial reductions documented at both short- and longer-term follow-up. This supports the notion that punctal occlusion meaningfully enhances ocular surface integrity. Although pooled analysis of Rose Bengal staining did not demonstrate significant changes, descriptive pre- and post-data consistently suggested clinical benefits that may not be captureable in aggregated metrics.
The observations align with previous reviews: Ervin et al concluded that evidence for plug efficacy remains inconclusive due to study limitations, although some ocular surface improvements were noted;30 and the more recent review by Chen et al (2025) reported moderate-to-high certainty evidence supporting substantial gains in TFBUT, Schirmer scores, symptom relief, and staining, with high retention and low heterogeneity.31 Notably, punctal cautery, especially with high-heat devices, has shown low recanalization (< 2%) and robust improvements in objective and subjective outcomes, as in Ohba et al (2011) 28 and Yaguchi et al (2012) demonstrated positive outcomes in chronic GVHD patients.22 A broader review of thermal/surgical methods further confirmed gains in tear volume and stability, with recanalization rates up to 39%.32
Adverse events were generally mild and transient, including ocular discomfort, redness, pain, blurred vision, and plug extrusion without serious or vision-threatening complications reported, which is consistent with findings from Ervin et al.30
Limitations of this review include the predominance of nonrandomized, small-scale, and open-label designs; inconsistent definitions of outcomes; substantial heterogeneity in interventions and patient populations; and reliance on pre-post studies lacking controls. These factors limit the ability to draw definitive conclusions about comparative efficacy. Clinically, punctal occlusion appears to offer ocular surface benefits and symptomatic relief, particularly for moderate-to-severe aqueous-deficient dry eye (eg, Sjögren’s, GVHD), and may serve as a valuable adjunct to conventional therapies. Permanent cautery may be preferable in cases of recurrent plug extrusion.
Conclusion
Though comparative meta-analysis did not show statistically significant improvements in tear production or film stability, punctal occlusion, especially thermal/surgical approaches, demonstrated consistent ocular surface and symptomatic benefits when assessed within individuals and had favorable safety profiles. Permanent cautery provides durable occlusion with low recanalization rates, though recanalization remains a risk even with single-use devices. Future research should prioritize large-scale, blinded RCTs with standardized interventions and outcomes, including robust patient-reported measures and long-term follow-up.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Funding
There is nofunding to report.
Disclosure
The authors declare that have no competing interest in this work.
References
1. Price KM, Richard MJ. The tearing patient: diagnosis and management. EyeNet Magazine [Internet]. 2009 Jun 1, [cited November 19, 2025]. Available from: https://www.aao.org/eyenet/article/tearing-patient-diagnosis-management.
2. Patel AS, Bustos DE. Dry eye syndrome [Internet]. EyeWiki; 2025 Feb 11, [cited June 13, 2025]. Available from: https://eyewiki.org/Dry_Eye_Syndrome#Overview.
3. Britten-Jones AC, Wang MTM, Samuels I, Jennings C, Stapleton F, Craig JP. Epidemiology and risk factors of dry eye disease: considerations for clinical management. Medicina. 2024;60(9):1458. doi:10.3390/medicina60091458
4. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334–11. doi:10.1016/j.jtos.2017.05.003 PMID: 28736337.
5. Alshamrani AA, Almousa AS, Almulhim AA, et al. Prevalence and risk factors of dry eye symptoms in a Saudi Arabian population. Middle East Afr J Ophthalmol. 2017;24(2):67–73. doi:10.4103/meajo.meajo_281_16
6. Agarwal P, Craig JP, Rupenthal ID. Formulation considerations for the management of dry eye disease. Pharmaceutics. 2021;13(2):207. doi:10.3390/pharmaceutics13020207
7. Baxter SA, Laibson PR. Punctal plugs in the management of dry eyes. Ocular Surf. 2004;2(4):255–265. doi:10.1016/S1542-0124(12)70113-1
8. Best A, Labetoulle M, Legrand M, M’garrech M, Barreau E, Rousseau A. Punctal and canalicular plugs: indications, efficacy and safety. J Fr Ophtalmol. 2019;42(3):e95–e104. doi:10.1016/j.jfo.2018.12.003
9. Yung YH, Toda I, Sakai C, Yoshida A, Tsubota K. Punctal plugs for treatment of post-LASIK dry eye. Jap J Ophthalmol. 2012;56(3):208–213. doi:10.1007/s10384-012-0125-8
10. Singh RB, Yung A, Coco G, et al. Efficacy and retention of silicone punctal plugs for treatment of dry eye in patients with and without ocular graft-versus-host disease. Ocular Surf. 2020;18(4):731–735. doi:10.1016/j.jtos.2020.07.018
11. Sjögren’s Syndrome Association B, Cheung G, Rauz S. Punctal plugs and dry eyes. Sjögren’s Today Magazine. 2007;22. Available from: https://sjogrensuk.org/wp-content/uploads/2023/08/punctal-plugs.pdf.
12. Marcet MM, Shtein RM, Bradley EA, et al. Safety and efficacy of lacrimal drainage system plugs for dry eye syndrome. Ophthalmology. 2015;122(8):1681–1687. doi:10.1016/j.ophtha.2015.04.034
13. Ervin A, Law A, Pucker AD. Punctal occlusion for dry eye syndrome. Cochrane Lib. 2017;2017(6). doi:10.1002/14651858.CD006775.pub3
14. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
15. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
16. Sterne JAC, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
17. Munn Z, Barker T, Moola S, et al. Methodological quality of case series studies. JBI Evidence Synth. 2020. doi:10.11124/JBISRIR-D-19-00099
18. Tong L, Beuerman R, Simonyi S, Hollander DA, Stern ME. Effects of punctal occlusion on clinical signs and symptoms and on tear cytokine levels in patients with dry eye. Ocul Surf. 2016;14(2):233–241. doi:10.1016/j.jtos.2015.12.004.
19. Balaram M, Schaumberg DA, Dana MR. Efficacy and tolerability outcomes after punctal occlusion with silicone plugs in dry eye syndrome. Am J Ophthalmol. 2001;131(1):30–36. doi:10.1016/s0002-9394(00)00620-6 PMID: 11162976.
20. Sherwin JC, Ratnarajan G, Elahi B, Bilkiewicz-Pawelec A, Salmon JF. Effect of a punctal plug on ocular surface disease in patients using topical prostaglandin analogues: a randomized controlled trial. Clin Exp Ophthalmol. 2018;46(8):888–894. doi:10.1111/ceo.13311 PMID: 29700925.
21. Holzchuh R, Villa Albers MB, Osaki TH, et al. Two-year outcome of partial lacrimal punctal occlusion in the management of dry eye related to Sjögren syndrome. Curr Eye Res. 2011;36(6):507–512. doi:10.3109/02713683.2011.569870 PMID: 21591859.
22. Yaguchi S, Ogawa Y, Kamoi M, et al. Surgical management of lacrimal punctal cauterization in chronic GVHD-related dry eye with recurrent punctal plug extrusion. Bone Marrow Transplant. 2012;47(11):1465–1469. doi:10.1038/bmt.2012.50
23. Wang Y, Carreno-Galeano JT, Singh RB, Dana R, Yin J. Long-term outcomes of punctal cauterization in the management of ocular surface diseases. Cornea. 2021;40(2):168–171. doi:10.1097/ICO.0000000000002384 PMID: 32467449; PMCID: PMC7704919.
24. Rabensteiner DF, Boldin I, Klein A, Horwath-Winter J. Collared silicone punctal plugs compared to intracanalicular plugs for the treatment of dry eye. Curr Eye Res. 2013;38(5):521–525. doi:10.3109/02713683.2013.765487 PMID: 23402650.
25. Tai MC, Cosar CB, Cohen EJ, Rapuano CJ, Laibson PR. The clinical efficacy of silicone punctal plug therapy. Cornea. 2002;21(2):135–139. doi:10.1097/00003226-200203000-00001 PMID: 11862081.
26. Miyata K, Otani S, Miyai T, Nejima R, Amano S. Atelocollagen punctal occlusion in dry eye patients. Cornea. 2006;25(1):47–50. doi:10.1097/01.ico.0000164783.10667.a4 PMID: 16331041.
27. Altan-Yaycioglu R, Gencoglu EA, Akova YA, Dursun D, Cengiz F, Akman A. Silicone versus collagen plugs for treating dry eye: results of a prospective randomized trial including lacrimal scintigraphy. Am J Ophthalmol. 2005;140(1):88–93. doi:10.1016/j.ajo.2005.02.031 PMID: 15939391.
28. Ohba E, Dogru M, Hosaka E, et al. Surgical punctal occlusion with a high heat-energy releasing cautery device for severe dry eye with recurrent punctal plug extrusion. Am J Ophthalmol. 2011;151(3):483–487.e1. doi:10.1016/j.ajo.2010.08.045
29. Packer M, Lindstrom R, Thompson V, et al. Effectiveness and safety of a novel crosslinked hyaluronate canalicular gel occlusive device for dry eye. J Cataract Refract Surg. 2024;50(10):1051–1057. doi:10.1097/j.jcrs.0000000000001505 PMID: 38875184.
30. Ervin AM, Law A, Pucker AD. Punctal occlusion for dry eye syndrome: summary of a Cochrane systematic review. Br J Ophthalmol. 2019;103(3):301–306. doi:10.1136/bjophthalmol-2018-313267
31. Chen KY, Chan HC, Chan CM. How effective and safe are punctal plugs in treating dry eye disease? A systematic review and meta-analysis. Contact Lens Anterior Eye. 2025. doi:10.1016/j.clae.2025.102438
32. Ranjan A, Basu S, Singh S. Punctal cautery in dry eye disease: a systematic review. Ocular Surf. 2024;34:235–240. doi:10.1016/j.jtos.2024.08.006
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Autologous Platelet‐Rich Plasma Drops for Evaporative Dry Eye Disease from Meibomian Gland Dysfunction: A Pilot Study
Murtaza F, Toameh D, Chiu HH, Tam ES, Somani S
Clinical Ophthalmology 2022, 16:2199-2208
Published Date: 6 July 2022
Engaging Stakeholders to Develop a Roadmap for Dry Eye and MGD PCORI-Funded Research
Warren NA, Maskin SL, Gurupur V, Rector DA, Adelman D, Howell S, McAree J, Dibble R, Carlisano C, Maconi DP, Schrotenboer D, Jaimes M, Marte N, Carlisano T, Toland C, Chung J, Cremers SL, Corbin GS
Patient Related Outcome Measures 2024, 15:143-186
Published Date: 12 May 2024
Shelf-Stable, Cryopreserved Amniotic Membrane for the Management of Ocular Surface Disease: A Retrospective Assessment
Cushman S
Clinical Optometry 2025, 17:409-415
Published Date: 21 December 2025
Low-Level Light Therapy as a Potential Adjunctive Approach in Mucus Fishing Syndrome: Report of Two Clinical Cases
Mancini A, Carnovale-Scalzo G, Mancini M, Borselli M, Taloni A, Chisari D, Lucisano A, Carnevali A, Meduri A, Aragona P, Scorcia V, Giannaccare G
International Medical Case Reports Journal 2025, 18:1679-1684
Published Date: 28 December 2025
Ocular Surface Changes and Glaucoma: A Prospective Contralateral Study of IOP-Reducing Eyedrops versus iStent Inject Surgery
Gundersen KG, Gundersen M, Nilsen C, Jensen PG
Clinical Ophthalmology 2026, 20:568150
Published Date: 8 January 2026