Back to Journals » Clinical Ophthalmology » Volume 20
Ocular Surface Changes and Glaucoma: A Prospective Contralateral Study of IOP-Reducing Eyedrops versus iStent Inject Surgery
Authors Gundersen KG ![]() , Gundersen M
, Gundersen M ![]() , Nilsen C, Jensen PG
, Nilsen C, Jensen PG ![]()
Received 17 September 2025
Accepted for publication 4 December 2025
Published 8 January 2026 Volume 2026:20 568150
DOI https://doi.org/10.2147/OPTH.S568150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Kjell Gunnar Gundersen,1 Morten Gundersen,1,2 Christian Nilsen,1,2 Per Graae Jensen1,2
1IFocus Øyeklinikk AS, Haugesund, Rogaland, Norway; 2Department of Life Sciences and Health, Oslo Metropolitan University, Oslo, Norway
Correspondence: Kjell Gunnar Gundersen, IFocus Øyeklinikk AS, Sørhauggata, 111, Haugesund, 5527, Norway, Tel +47 91 64 87 07, Email [email protected]
Purpose: To compare ocular surface outcomes between interventional glaucoma treatment with trabecular micro-bypass stent implantation and continued topical intraocular pressure-lowering therapy.
Patients and Methods: A prospective, single-center, contralateral-eye study of patients with bilateral, mild-to-moderate open-angle glaucoma undergoing implantation of the iStent inject in the study eye, while the fellow eye (control eye) continued topical medications. Just over half the eyes in both groups underwent phacoemulsification. Ocular surface parameters were evaluated using objective tests and validated symptom questionnaires at baseline and at 1, 3, and 6 months.
Results: Fifty-six eyes were included, 28 in each group. At 6 months, medication use reduced significantly in study eyes (from 1.9± 1.0 preoperatively to 0.4± 0.6; p< 0.001), but not in control eyes (from 1.5± 0.9 to 1.4± 0.8; p=0.168). Study eyes demonstrated significant improvements in keratograph bulbar redness score (2.4± 0.6 to 2.0± 0.4; p=0.003), and Oxford ocular surface staining (OSS) score (1.6± 1.2 to 0.7± 1.0; p< 0.001) while control eyes did not; improvements in bulbar redness and OSS scores were significantly greater in study eyes (p=0.005 and p=0.045, respectively). Patient-reported symptoms improved significantly: OSDI (Ocular Surface Disease Index) scores decreased from 18.4 ± 16.4 to 9.3 ± 8.9 (p=0.007) and SPEED (Standard Patient Evaluation of Eye Dryness) II scores decreased from 8.0 ± 7.8 to 4.5 ± 4.1 (p=0.005).
Conclusion: Interventional glaucoma treatment with trabecular micro-bypass stent implantation significantly reduced medication burden, which was associated with improved signs and symptoms of ocular surface disease at 6 months. Compared to fellow eyes on topical therapy, stent-treated eyes showed better outcomes in selected ocular surface parameters, supporting the benefits of an interventional approach.
Keywords: ocular surface disease, glaucoma medications, iStent inject, dry eye disease, MIGS
Introduction
Despite advances in glaucoma treatment, topical medical therapy remains the established first-line treatment, effective in reducing intraocular pressure (IOP) and preventing progression to irreversible blindness.1 However, laser trabeculoplasty techniques—such as selective laser trabeculoplasty (SLT) and micropulse laser trabeculoplasty (MP-LT)—are increasingly being adopted as primary interventions for early or moderate glaucoma, as they effectively lower intraocular pressure while reducing the long-term burden and ocular surface toxicity associated with chronic topical therapy.2,3 Nevertheless, for many patients, the burden of lifelong topical therapy and complex multi-drug regimens remains considerable, often leading to poor treatment adherence, increased cost of care, and impaired quality of life (QoL).4 Another significant drawback is the risk of ocular surface toxicity.
Ocular surface disease (OSD) is widespread in glaucoma patients, showing a prevalence of 48–59% in various studies.5,6 Benzalkonium chloride, a common preservative in glaucoma medications, is known to cause corneal and conjunctival toxicity in patients on long-term topical glaucoma therapy. BAK can disrupt the corneal epithelium, reduce goblet cell density, and induce inflammation, thereby exacerbating ocular surface disease and potentially compromising surgical outcomes.7 Recent developments include the introduction of preservative-free formulations and alternative, less cytotoxic preservatives such as Polyquad®, potassium sorbate, and Purite®, which are associated with a lower risk of ocular surface toxicity. Although clinical evidence remains limited, these agents represent a useful strategy to minimize preservative-related ocular surface injury when preservative-free options are not available or affordable.8 In addition, the IOP-lowering active agents themselves can also be associated with ocular surface toxicity: prostaglandin analogs can cause conjunctival hyperemia and meibomian gland dysfunction, while beta-blockers can impair tear production, cause corneal epithelial disruption, and induce inflammatory changes in the conjunctiva.9 Several studies have shown an association between OSD severity and the number of glaucoma medications used.10,11
Ocular symptoms due to OSD, such as tearing, burning, or itching, can worsen adherence to glaucoma medications, increasing the risk of progressive glaucomatous vision loss.12,13 OSD in medically treated patients can also negatively affect QoL due to the ocular discomfort and associated visual disturbances, such as blurred vision, night vision difficulties, and trouble with near vision and reading.14,15 Additionally, increased subclinical conjunctival inflammation can increase the likelihood of failure of filtration surgery.16 Due to these significant drawbacks, glaucoma treatment aims to not only reduce IOP but also medication dependence.
Although filtration surgery such as trabeculectomy can achieve freedom from medications, it carries the risk of sight-threatening complications.17 Additionally, trabeculectomy itself has been associated with development of OSD in some studies.18,19 In comparison, minimally invasive glaucoma surgery (MIGS) has a more favorable safety profile, with proven efficacy in reducing IOP and medication use, making them an ideal alternative to invasive surgeries in mild to moderate glaucoma.20 However, the impact of MIGS on the ocular surface, either through medication reduction or through the surgical process itself, has yet to be established.
Interventional Glaucoma (IG) is a contemporary treatment paradigm that emphasizes early procedural intervention to reduce dependence on topical IOP-lowering medications.4 Within this framework, trabecular micro-bypass stents such as the iStent and iStent inject (Glaukos Corporation, Laguna Hills, CA) are commonly used MIGS devices. These biocompatible titanium implants create direct channels for aqueous outflow through the trabecular meshwork and have been shown to effectively decrease IOP and medication use in open-angle glaucoma (OAG).21,22 However, limited data are available on the impact of iStent surgery on ocular surface health.23,24 This study evaluated the effect of iStent inject implantation, with or without cataract surgery, on ocular surface parameters over six months, comparing outcomes to those of fellow eyes managed with ongoing topical therapy.
Patients and Methods
Study Design and Participants
This prospective nonrandomized contralateral-eye study recruited patients with bilateral glaucoma at a private eye clinic in Haugesund, Norway, from March 2022 to December 2023. The study complied with the tenets of the Declaration of Helsinki and Good Clinical Practice (GCP) and was approved by the Regional Committee for Medical and Health Research Ethics in Norway (reference number 2021/253,485). All participants provided written informed consent.
Inclusion criteria were age above 18 years, a diagnosis of bilateral OAG, visual field (VF) mean deviation better than –12 dB, and stable, well-controlled glaucoma on topical medications. Stability was defined as no progression on Standard Automated Perimetry (SAP) using the Zeiss Humphrey 24–2 program, with no worsening detected across three consecutive VF tests performed within six-months.
Exclusion criteria were manifest corneal pathology or scarring, eyelid deformities, intra- or extra-ocular surgery in the preceding six months, pregnancy, and any acute or chronic illness that could confound the study outcomes (eg, autoimmune disorders, connective tissue disease, clinically significant atopy, diabetes).
The eye with higher IOP and/or worse VF damage was designated as the study eye and received iStent inject implantation. The fellow eye continued glaucoma medications and served as the control. Study and control eyes with visually significant cataract underwent phacoemulsification in addition to stent implantation or pharmacotherapy, respectively.
Preoperative and Postoperative Assessments
All patients underwent standard ophthalmological examination, including refraction and visual acuity measurements, at baseline, 1-month, 3-month, and 6-month visits. At each visit, OSD was evaluated using a battery of objective and subjective assessments, with a 3-minute break between tests for standardization of measurements. Temperature and humidity in the examination room were noted for the baseline and 6-month visits to account for the influence of environmental conditions.25
Patients were asked to discontinue any eyedrops two hours prior to OSD testing. Tests were performed in the following order:
- Tear osmolarity was measured using the TearLab Osmolarity system (Tearlab Corp, California, USA) with the test card touching the lower temporal tear meniscus. Values ≥308 mOsm/L or inter-eye difference >8 mOsm/L were defined as OSD.26 Osmolarity was graded from 0–3: 0 (< 308 mOsm/L), 1 (308–315 mOsm/L), 2 (316–335 mOsm/L), and 3 (≥336 mOsm/L).
- OSD symptoms were measured using two validated questionnaires:
- The Ocular Surface Disease Index (OSDI) questionnaire measures visual disability due to ocular symptoms. Symptoms are scored from 0 (none of the time) to 4 (all of the time), with total scores ranging from 0–100; a score of ≥13 was considered as cut-off for OSD.26 Scores were graded from 0–3 based on standard cutoffs for no, mild, moderate, and severe OSD: 0 (0–12), 1 (13–22), 2 (23–32), and 3 (>33).27
- The American Society of Cataract and Refractive Surgery (ASCRS)-modified Preoperative OSD SPEED II questionnaire is comprised of the original SPEED (Standard Patient Evaluation of Eye Dryness) questionnaire, which evaluates symptom frequency and severity, with additional questions designed to screen a preoperative population.28 Total scores range from 0–28, with values ≥4 considered as OSD. Scores were graded from 0 (< 4) to 1 (4–28).
- Bulbar conjunctival redness was measured using the Keratograph 5M (OculusOptikgeräte GmbH, Wetzlar, Germany). The software calculated redness scores (percentage area ratio between blood vessels and the rest of the analyzed area) from 0.0 to 4.0.29 Higher scores represent greater hyperemia.
- Tear meniscus height (TMH) and non-invasive keratograph tear break-up time (NIKBUT) were measured using the Keratograph 5M. NIKBUT was automatically measured by the device as time (seconds) from the last blink to the first tear film break-up (NIKBUT 1st) and average of all breakups (NIKBUT average) occurring in the measurement period set by the software (up to 24.98 s).30 NIKBUT < 10 seconds was considered OSD26 and given a score of 1, while NIKBUT measurements of 10–24 seconds were given a score of 0. TMH (millimeters) was measured at the central lower eyelid and a value ≤ 0.2 mm was considered OSD.
- Tear film thickness (TFT) was measured with the Lipiview II Interferometer (TearScience Inc., Morrisville, NC), with 75 nm used as cut-off for OSD.
- Tear production was measured with the Schirmer’s I test (without anesthetic). Wetting of the Schirmer paper strips (TearFlo, MDT, Krakow, Poland) by ≤ 5.0 mm in 5 minutes was considered as cut-off for OSD.
- Corneal sensitivity was measured in the center of the cornea with the Cochet–Bonnet esthesiometer (Aesthesiometer 12/100 mm; Luneau SAS, Pruneay-Le-Gillon, France). On a grading scale of 0–6 mm, a grade of ≤ 5 was considered abnormal.
- Ocular surface staining (OSS) was measured using the Oxford grading scheme (grades 0–5)31 after instillation of 5μL of 2% fluorescein sodium into the inferior fornix with a sterile-tip micro-pipette. Severity grades ≥ 2 were considered as OSD.
- Meibomian gland dropout was examined using the Keratograph 5M and meiboscore was calculated on a 0–3 scale: 0 (no dropout), 1 (< 1/3 of glands lost), 2 (1/3 – 2/3 glands lost) and 3 (>2/3 glands lost).32
- Meibum produced by the 5 central glands in the lower eyelid was assessed under the slit lamp by gently rolling a cotton swab towards the eyelid margin. Meibum expressibility was graded from 0–3: 0 (all glands expressible), 1 (3–4 glands were expressible), 2 (1–2 glands were expressible), and 3 (no glands were expressible). Meibum quality was graded from 0–3: 0 (clear fluid), 1 (cloudy meibum), 2 (granular meibum) and 3 (thick, toothpaste-like meibum).33
TFT, corneal sensitivity, meiboscore, meibum characteristics, and ocular symptoms (OSDI and SPEED II scores) were evaluated at baseline and 6-month visits. All other OSD tests were performed at every visit. A diagnosis of OSD was made as per the Tear Film & Ocular Surface Society Dry Eye (TFOS/DEWS) II criteria: OSDI ≥ 13 and at least one positive result for markers of homeostasis (osmolarity, OSS, NIKBUT).26
Additionally, patients selected for cataract surgery underwent standard biometric evaluation for intraocular lens (IOL) power calculation.
Anti-Glaucoma Topical Medication
Patients were on prostaglandin analog monotherapy or fixed-combination therapy at baseline. When additional IOP lowering was required, a second agent (eg, carbonic anhydrase inhibitors, beta blocker or alpha-agonists) was prescribed at the discretion of the treating physician. Variability existed in the specific brands used within each medication class due to differences in prior prescriptions and pharmacy availability. Both preservative-free and BAK-containing formulations were represented. No medication washout or changes to topical therapy were performed during the study, except when IOP exceeded 20 mmHg, in which case escalation was recorded.
Adherence was assessed at each follow-up visit through patient self-report of missed doses within the previous week and cross-checked with pharmacy dispensing records when available.
Surgical Intervention
Study eyes underwent surgery with the iStent inject, comprised of 2 second-generation stents. The preloaded injector was inserted through a corneal incision and the first stent was implanted in the inferior nasal trabecular meshwork as described in the literature.21,22 The second stent was implanted 2–3 clock hours away from the first.
In eyes undergoing cataract surgery, standard small-incision phacoemulsification was performed, followed by iStent inject implantation.
Sample Size Calculation
The sample size calculation was based on hyperosmolarity as the primary outcome measure, with reference to normative data reported by Epitropoulos et al.34 Using an alpha level of 0.05 and a power of 0.80, the estimated sample size was determined to be sufficient to detect clinically meaningful differences in tear osmolarity between groups.
Statistical Analysis
Statistical analyses were performed using SPSS version 24 (IBM SPSS, NY, USA). Primary outcomes were ocular surface parameters, while IOP and medications were secondary outcomes. Continuous variables were summarized using descriptive statistics. Baseline and 6-month data, as well as comparisons between the study and control eyes, were analyzed using the Wilcoxon signed-rank test. P value<0.05 was considered statistically significant.
The study was designed and conducted independently by the investigators. Statistical analysis and medical writing support were provided by an independent writing agency funded by the study sponsor. The authors had full access to all study data, were responsible for data interpretation, and retained final authority over manuscript preparation and submission.
Results
Demographics
Thirty-two patients were enrolled. Four patients were excluded from the study: one due to panuveitis, one due to previous trabeculectomy, one for missing the follow-up visit, and one withdrew from the study. Fifty-six eyes of 28 patients (14 male and 14 female; mean age: 74.0±6.4 years) were included in the study. At baseline, patients were treated one of the following prostaglandin analogs or fixed combinations: tafluprost 0.15 mg/mL (3/28; 10.7%), bimatoprost 0.3 mg/mL (3/28; 10.7%), latanoprost 50 µg/mL (6/28; 21.4%), timolol/bimatoprost 5 mg/0.3 mg per mL (5/28; 17.9%), or timolol/tafluprost 5 mg/0.15 mg per mL (11/28; 39.3%). Tafluprost formulations used in this cohort were preservative-free, whereas most other agents contained benzalkonium chloride (BAK) as the preservative.
Regarding concomitant phacoemulsification, 16 study eyes (57%) underwent stent + phacoemulsification and 12 (43%) underwent standalone stent implantation. Out of 28 control eyes that continued glaucoma medications, 15 (54%) underwent phacoemulsification.
IOP and Medications
IOP was significantly higher in the study eyes at baseline and 6 months postoperatively (p<0.001), consistent with the selection of the worse eye for stent implantation (Figure 1). At 6 months, mean IOP reduced significantly in both study (20.5±4.7 to 17.7±4.3 mmHg, p=0.003) and control groups (15.9±3.7 to 14.3±3.1 mmHg, p=0.019), with comparable reductions between groups (p=0.125).
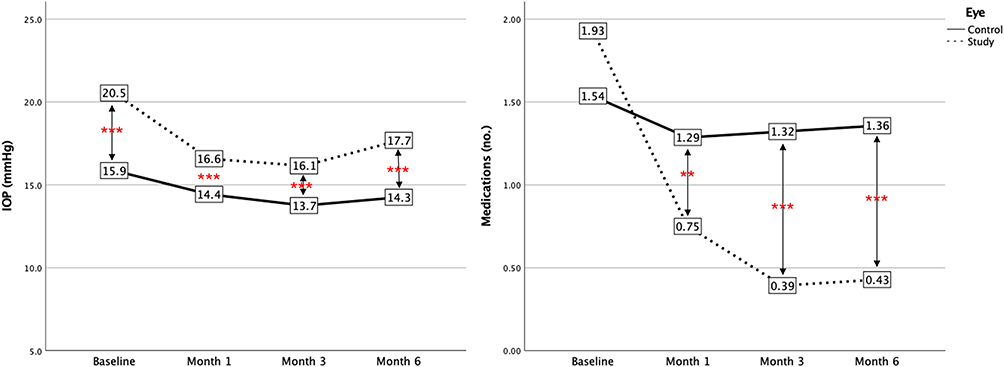 |
Figure 1 Line graphs showing intraocular pressure and medication usage of eyes in the control and study groups. Asterisks at a timepoint indicate statistically significant difference between the groups: *p<0.05, **p<0.01, ***p<0.001. |
Medication usage was comparable between groups at baseline (p=0.054) and lower in the study group at 6 months (p<0.001) (Figure 1). Medication burden was significantly reduced from baseline in study eyes (1.93±1.0 to 0.43±0.6, p<0.001) but not in control eyes (1.54±0.9 to 1.36±0.8, p=0.168), with greater reduction in study eyes (p<0.001).
Ocular Surface Outcomes
Tables 1, 2, and Figure 2 show ocular surface outcomes in study and control eyes. Baseline ocular surface parameters were similar between groups: tear osmolarity, NIKBUT, NIKBUT-first, tear lab grading, tear film thickness (TFT), corneal staining score, Schirmer I, corneal sensitivity, and meiboscore values showed no statistically significant differences between study and control eyes (Tables 1 and 2, all p > 0.05).
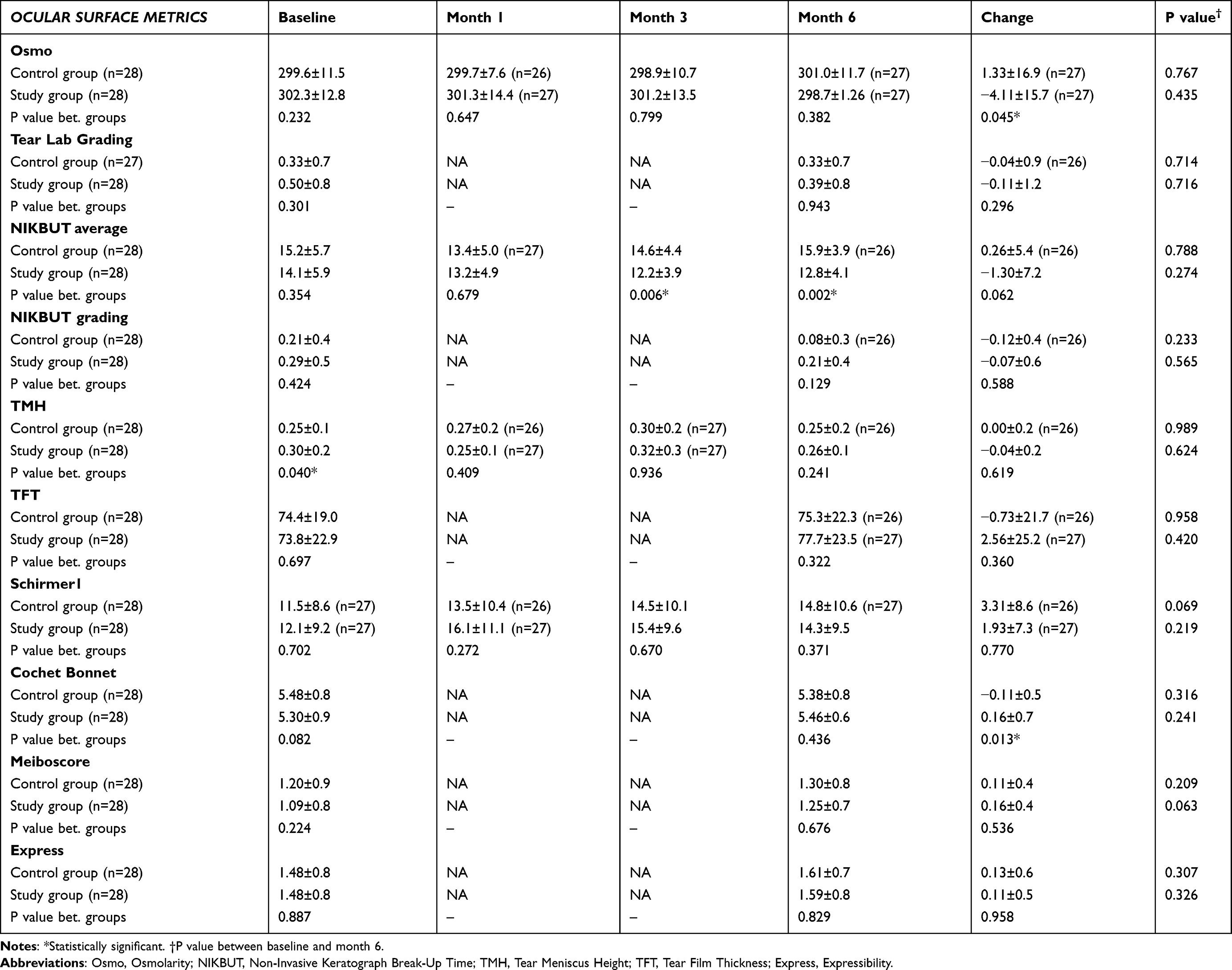 |
Table 1 Ocular Surface Metric Outcomes of Study vs Control Group Showing No Significant Change from Baseline to 6 Months. P values Between Baseline and 6 Months, and P values Between Groups Were Calculated Using Wilcoxon Signed-Rank Test |
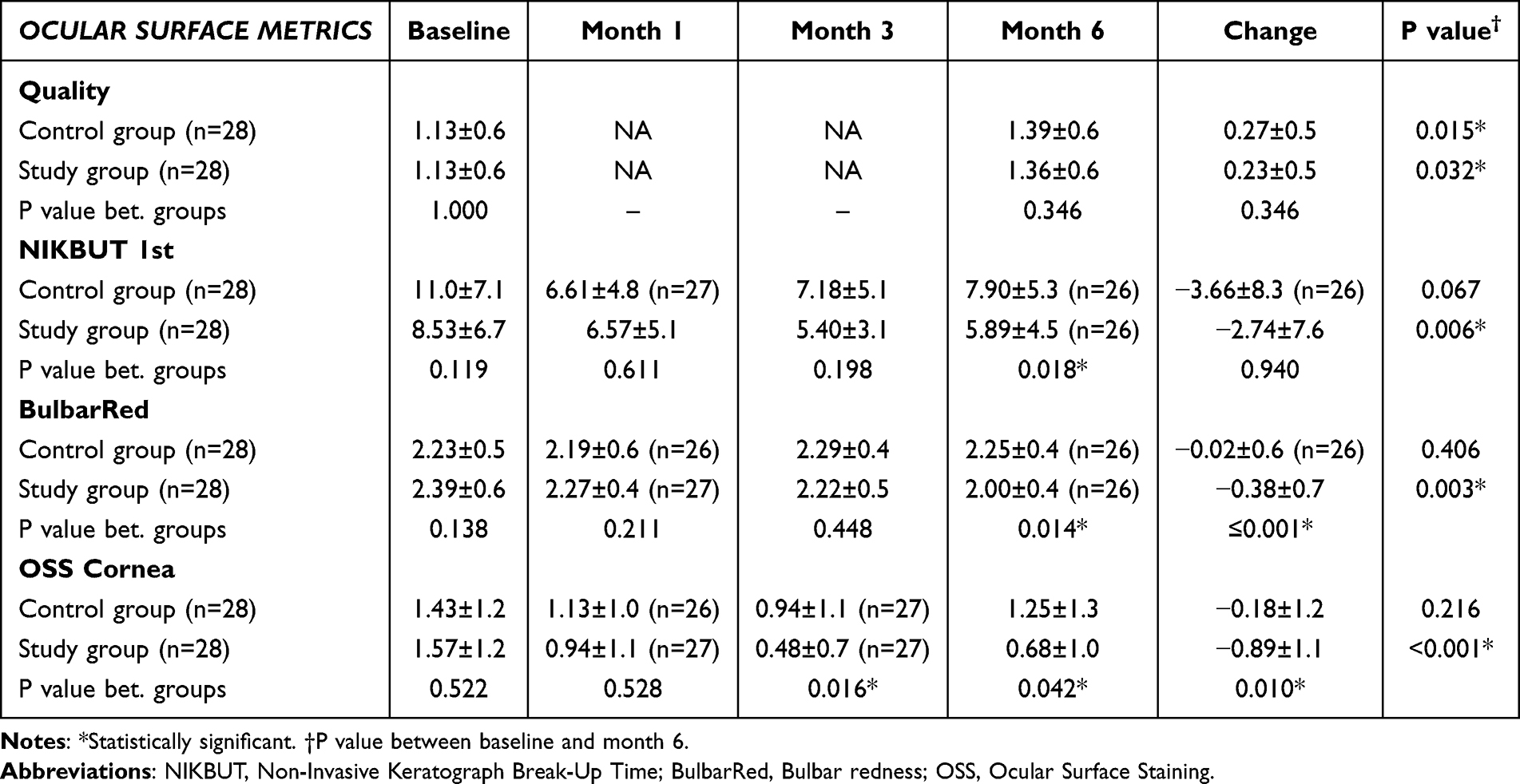 |
Table 2 Ocular Surface Metric Outcomes of Study vs Control Group Showing Significant Change from Baseline to 6 Months. P values Between Baseline and 6 Months, and P values Between Groups Were Calculated Using Wilcoxon Signed-Rank Test |
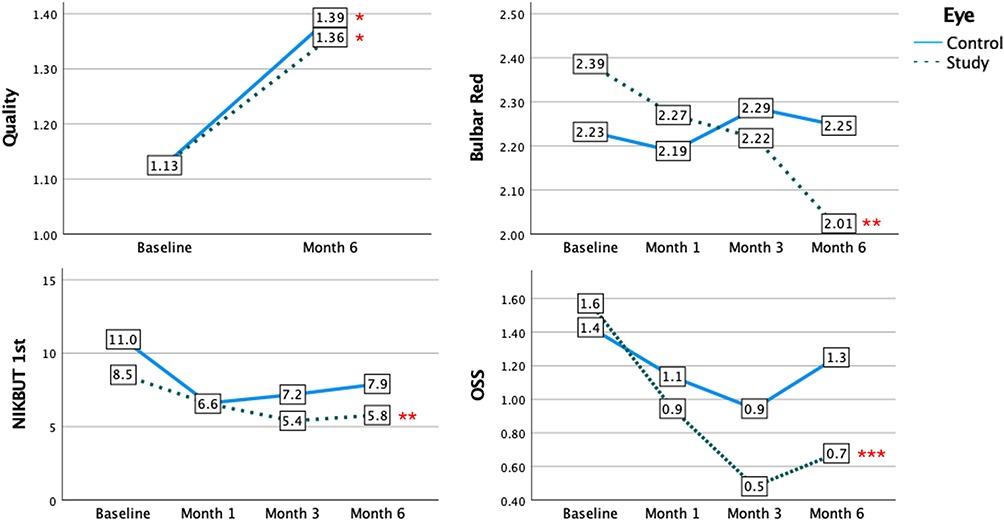 |
Figure 2 Ocular surface metric outcomes of eyes in the control and study groups showing significant change from baseline. Asterisks at a timepoint indicate statistical difference between baseline and Month 6. *p<0.05, **p<0.01, ***p<0.001. |
No significant changes from baseline to 6 months were observed in either group for tear osmolarity, tear meniscus height (TMH), TFT, Schirmer I test, meiboscore, meibum expressibility, or corneal sensitivity (Table 1). NIKBUT remained stable in the control group, while the study group showed transient reductions at months 3 and 6, although the overall baseline-to-6-month change was not statistically significant. Between-group comparisons at 6 months also revealed no differences in these parameters, except that the study group demonstrated a greater change in tear osmolarity (p=0.045) and higher Cochet–Bonnet esthesiometry values (p=0.013), indicating better corneal sensitivity.
Meibum quality worsened slightly in both study and control eyes (p=0.032 and p=0.015, respectively). NIKBUT 1st was significantly reduced (worsened) from baseline in study eyes (p=0.006), but reductions from baseline were comparable between study and control eyes (−2.74±7.6 seconds versus −3.66±8.3 seconds, respectively; p=0.940) (Table 2). Room temperature and humidity were comparable between baseline and 6-month visits (23.6±0.7°C versus 23.9±0.8°C, p=0.213 and 33.3±10.2% versus 34.9±8.9%, p=0.718, respectively).
Bulbar conjunctival redness and Oxford ocular surface staining (OSS) scores improved significantly from baseline in the study eyes (p=0.003 and p<0.001, respectively), but not in the control eyes (p=0.406 and p=0.216, respectively) (Table 2). Study eyes showed significantly greater improvements in bulbar redness scores (−0.38±0.7 versus −0.02±0.6, p=0.001) and OSS scores (−0.89±1.1 versus −0.18±1.2, p=0.010).
Considering the results per patient (as opposed to study eye versus control eye), OSDI and SPEED scores were significantly improved from baseline to 6 months (p=0.007 and 0.005, respectively). Mean OSDI score reduced from 18.4±16.4 at baseline to 9.3±8.9 at 6 months (−9.1±14.9), while SPEED score reduced from 8.0±7.8 to 4.5±4.1 (−3.6±6.6). Inter-eye difference in osmolarity showed no significant change from baseline (7.82±7.4 to 11.1±9.5; p=0.055).
Subgroup Analysis without Cataract Surgery (iStent-Only vs Medications-Only)
In the subgroup analysis excluding all eyes that underwent cataract surgery, most ocular surface parameters showed no significant differences between the iStent-only and medications-only groups at baseline or month 6 (Table 3). Tear osmolarity, tear meniscus height, tear film thickness, meiboscore, meibum quality, and meibum expressibility remained comparable between groups across all time points.
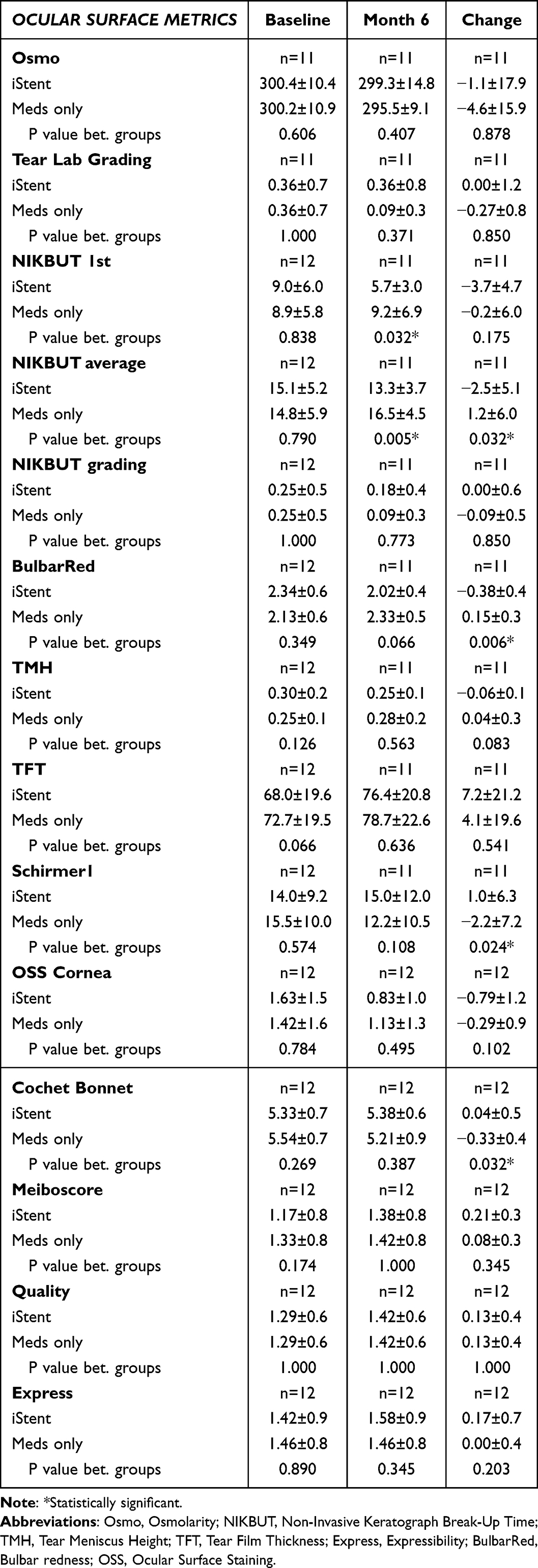 |
Table 3 Ocular Surface Metrics Outcomes of Eyes Grouped by Procedure (iStent Group vs No Procedure Group, Excluding Eyes That Underwent Cataract Surgery. P values Were Calculated Using the Wilcoxon Signed-Rank Test |
However, several NIKBUT parameters demonstrated significant between-group differences at month 6. The medications-only group maintained higher NIKBUT average values compared with the iStent group (16.5 ± 4.5 vs 13.3 ± 3.7; p = 0.005), with a corresponding difference in change from baseline (p = 0.032). NIKBUT-1st was also significantly higher in the medications-only group at month 6 (p = 0.032).
Bulbar hyperemia diverged between groups, showing a greater reduction in the iStent group while increasing slightly in the medications group, yielding a significant difference in change from baseline (p = 0.006). Schirmer I test also showed a significantly different change pattern, with an increase in the iStent group and a decrease in the medications group (p = 0.024). Corneal sensitivity demonstrated a small but statistically significant between-group difference in change from baseline, favoring the iStent group (p = 0.032).
Safety
Corrected distance visual acuity (CDVA) improved from baseline to 6 months in both groups (Figure 3), with statistically significant improvement in the study eyes (0.04±0.09 to −0.01±0.08 logMAR; p=0.003) but not in control eyes (0.02±0.09 to 0.00±0.07 logMAR; p=0.055). Study eyes showed greater improvement in CDVA, although differences between groups were not statistically significant (p=0.089). No intraoperative or postoperative complications related to stent implantation or cataract surgery were noted.
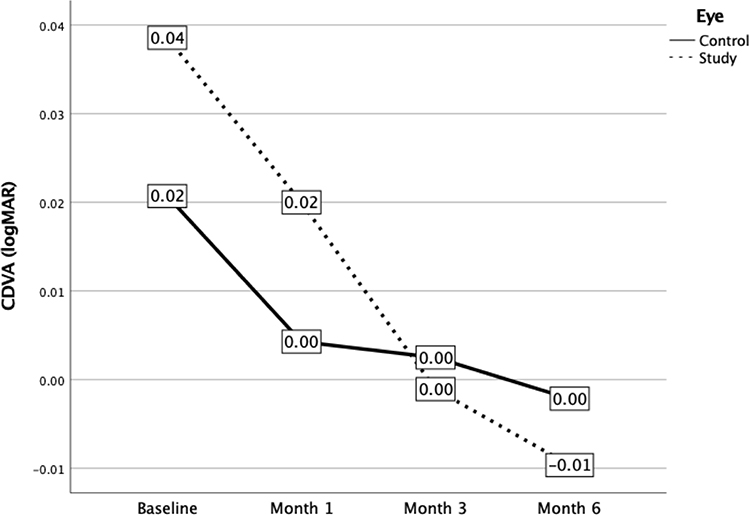 |
Figure 3 Line graphs showing visual outcomes of eyes in the control and study groups. |
Discussion
Following trabecular micro-bypass with the iStent inject, study eyes experienced a 79% reduction in glaucoma medication use (−1.5 ± 0.8 from a baseline of 1.9 ± 1.0) and a 13.95% IOP reduction, from 20.5±4.7 to 17.7±4.3 mmHg at 6 months. This was associated with statistically significant improvements in both objective and subjective ocular surface parameters, including bulbar redness, OSS, OSDI, and SPEED II scores. Notably, bulbar redness and OSS improved more in the study eyes than in the control eyes, supporting the contribution of reduced medication burden to enhanced ocular surface health. No adverse events were observed, and stent implantation did not compromise visual outcomes following cataract surgery.
In contrast, the fellow control eyes that continued anti-glaucoma medications showed a modest IOP reduction from 15.9 ± 3.7 to 14.3 ± 3.1 mmHg (10%), despite not receiving an iStent. This improvement is likely multifactorial. A proportion of control eyes also underwent phacoemulsification, which can lower IOP by approximately 1–3 mmHg.35,36 Additionally, better overall adherence following surgery in the study eye may have indirectly influenced IOP control in the fellow eye. Together, these factors likely explain the modest yet statistically significant IOP decrease observed in the control eyes in this contralateral-eye study.
Although the study eye was defined by higher IOP or worse visual field, baseline measures of ocular surface disease were comparable between groups; therefore, selection of the study eye did not produce a detectable baseline OSD imbalance that could account for the greater OSD improvement observed after surgery.
Previous studies have found OSDI and OSS to be significantly correlated with number of medications used.6,37 Consistent with the literature, we found OSS to be significantly improved at 6 months in the study eyes, with improvements noticed from the first month, showing that ocular health was rapidly restored following medication reduction. OSDI was significantly improved despite unilateral intervention. Mean OSDI score improved from mild OSD (score of 18.4±16.4) to normal (score of 9.3±8.9). Notably, this improvement (−9.1±14.9) was more than the minimal clinically important difference (MCID) defined for OSDI, which ranges from 4.5 to 7.3 for mild OSD, and 7.0 to 9.9 for all OSD grades.27 Additionally, improvements were observed in both objective and subjective OSD measures, which is significant when compared to previous literature showing low correlations between signs and symptoms of OSD.33,38,39 In our study, osmolarity did not show significant changes from baseline in either group, but this may be attributed to the baseline osmolarity in both groups being well below the cutoff for OSD (302.3±12.8 and 299.6±11.5 mOsm/L in study and control groups, respectively).
Compared to the broad evidence base on the IOP- and medication-lowering efficacy of the iStent devices, the assessment of ocular surface changes following trabecular micro-bypass has been limited. Samuelson et al found patient-reported QoL outcomes to be significantly improved over 24 months following iStent inject implantation with cataract surgery, with responders (patients that showed minimally important differences) found to be more likely to be medication-free than non-responders.40 Jones et al observed significantly improved glaucoma-specific and general health QoL, OSDI, tear break-up time (TBUT), and corneal staining at 4 months following iStent + phacoemulsification, with or without adjunctive endocyclophotocoagulation.24 Schweitzer et al found OSDI, ocular staining, and fluorescein TBUT to be significantly improved 3 months after iStent or iStent inject implantation with concomitant cataract surgery.23 Following reduction in medication burden by 60% from 1.5±0.9 to 0.6±0.8 medications, OSDI score reduced by 56% from 39.8±21.9 to 16.4±14.8, and Oxford ocular staining score showed a 71% reduction from 1.4±1.0 to 0.4±0.5 (p< 0.0001). Similarly, in the current study, mean OSDI score was reduced by 49% at 6 months (18.4±16.4 to 9.3±8.9; p=0.007) and mean OSS score reduced by 56% in the study group (1.6±1.2 to 0.7±1.0) (p<0.001). This was associated with medication reduction by 79% (1.9±1.0 to 0.4±0.6; p<0.001).
Contrary to Schweitzer et al and Jones et al, the current study found NIKBUT 1st to be significantly worsened from baseline to 6-month timepoints in the study eyes, despite non-significant differences in room temperature, humidity, and TFT between visits. The unexpected worsening of NIKBUT 1st in the study eyes may reflect a transient postoperative effect rather than a paradoxical deterioration. Corneal incisions, postoperative inflammation, and topical medications may transiently destabilize the tear film. In our series, NIKBUT 1st decreased markedly at 1 month but showed gradual improvement at 3 and 6 months, although values remained below baseline at the 6-month follow-up. This trend suggests that tear-film stability begins to recover after surgery but may require a longer period to fully normalize once postoperative factors resolve and topical medication burden is reduced. However, average NIKBUT measurement did not show a significant change from baseline (p=0.274). It must be noted that NIKBUT values show high between-visit variability due to various factors including keratograph precision and intrinsic variability in the tear film.41,42 The standard deviations of TBUT observed in the current study were greater than that noted by Schweitzer et al,23 which could also have contributed to increased variability of results, as keratograph measurements have been found to show lower repeatability at higher values.41
It must be noted that cataract surgery itself can also induce OSD due to factors including damage to corneal nerves, ocular surface drying/repeated irrigation, phototoxicity, and perioperative medications.43,44 Thus, it is possible that ocular surface parameters in the current study could have been confounded by concomitant phacoemulsification. However, a similar proportion of patients underwent phacoemulsification in the study and control groups (57% and 54%, respectively), and we can assume that confounding factors were comparably distributed between both groups. To address the potential confounding effect of phacoemulsification, we performed a subgroup analysis restricted to eyes that underwent iStent implantation alone compared with eyes that remained on topical therapy. After removing all eyes that had cataract surgery, most ocular surface parameters remained comparable between groups, indicating that the primary findings were not driven by phacoemulsification. Tear film stability indices (NIKBUT) remained higher in the medications-only group, whereas the iStent-only group demonstrated more favorable changes in bulbar hyperemia, Schirmer I, and corneal sensitivity. These patterns mirror the trends observed in the full cohort, supporting the conclusion that the differential effects observed between groups are attributable to the treatment modality rather than cataract surgery.
The current study allows the ocular surface-related changes following MIGS to be compared to traditional filtering surgery results reported in the scientific literature. Trabeculectomy can reduce ocular inflammation and improve ocular surface parameters by reducing medication dependence.45–47 However, the surgery itself may also worsen OSD: the filtering bleb can impair tear film distribution,19 while antimetabolite usage can cause limbal stem cell deficiency, and conjunctival trauma can impair ocular surface homeostasis.48 In comparison, iStent inject surgery preserves ocular tissue with a high safety profile demonstrated in previous studies as well as the current study. Our findings provide additional evidence that iStent inject implantation, with or without concomitant cataract surgery, does not impair ocular surface health, but rather improves it. As glaucoma patients have a higher risk of OSD, it is vital to consider the ocular surface benefits of a procedure in addition to its IOP- and medication-lowering efficacy during the decision-making process.
This study contributes some of the first evidence on the impact of MIGS on the ocular surface. The strengths of the study include its prospective design, which reduces selection bias. The contralateral-eye design was also valuable in removing bias due to inter-individual anatomic or physiological differences. Additionally, OSD was evaluated with a comprehensive slate of both objective and subjective measures, with the subjective parameters measured by widely used validated questionnaires (OSDI and SPEED II).
The limitations of this study include a relatively small sample size from a single-center population in Norway, limiting the generalizability of results to other ethnicities. Examiners were unmasked to the study groups, which could have introduced some bias. Additionally, a history of lubricant eyedrop use was not an exclusion criterion, which could have underestimated OSD severity in patients using such drops. A further limitation is the heterogeneity of preservative exposure across brands of topical therapy prior to enrolment. While the primary focus was on drug class and medication burden, different preservative formulations may have contributed variably to ocular surface disease. In addition, although we assessed self-reported adherence and logged any medication modifications, recall bias and unrecorded changes cannot be entirely excluded. Further studies with longer durations of follow-up are required to investigate the longer-term effects and the durability of iStent inject implantation on the ocular surface and possible late changes.
Conclusion
In summary, this study evaluated the impact of an interventional glaucoma approach—specifically, trabecular micro-bypass stent implantation—on ocular surface parameters in patients with open-angle glaucoma. At 6 months postoperatively, marked reduction in medication burden and achievement of IOP control were accompanied by significant improvements in both signs and symptoms of ocular surface disease. Objective improvements, in particular, reductions in bulbar conjunctival redness and Oxford ocular surface staining scores, occurred in parallel with decreased medication use. Similarly, subjective assessments such as the OSDI and SPEED II scores showed clinically meaningful improvements. While these results support the potential of interventional glaucoma strategies to alleviate ocular surface toxicity associated with long-term topical pharmacotherapy, the findings should be interpreted with caution given the modest sample size, single-center design, and short follow-up period. Future multicenter studies with larger cohorts and longer follow-up are warranted to confirm these results and further explore the long-term ocular surface effects of MIGS.
Acknowledgments
Writing and editing support was provided by Dana Hornbeak, MD, MPH (Glaukos) and GP Communications, and was funded by Glaukos.
Disclosure
The authors have no financial interests in the materials and methods mentioned in this study. K.G.G is a consultant for Glaukos. The study was funded by Glaukos Corp. The funder was not involved in the study design, data collection, analysis and interpretation.
References
1. Vass C, Hirn C, Sycha T, Findl O, Bauer P, Schmetterer L. Medical interventions for primary open angle glaucoma and ocular hypertension. Cochrane Database Syst Rev. 2007;2007(4):CD003167. doi:10.1002/14651858.CD003167.pub3
2. Yener HI, Ozcimen M. Effectiveness of selective laser trabeculoplasty as initial or adjunctive treatment for primary open-angle glaucoma. Beyoglu Eye J. 2020;5(3):199–14. doi:10.14744/bej.2020.85866
3. Phan R, Bubel K, Fogel J, Brown A, Perry H, Morcos M. Micropulse laser trabeculoplasty and reduction of intraocular pressure. Saudi J Ophthalmol. 2021;35(2):122–125. doi:10.4103/1319-4534.337860
4. Radcliffe NM, Shah M, Samuelson TW. Challenging the “Topical medications-first” approach to glaucoma: a treatment paradigm in evolution. Ophthalmol Ther. 2023;12(6):2823–2839. doi:10.1007/s40123-023-00831-9
5. Fechtner RD, Godfrey DG, Budenz D, Stewart JA, Stewart WC, Jasek MC. Prevalence of ocular surface complaints in patients with glaucoma using topical intraocular pressure-lowering medications. Cornea. 2010;29(6):618–621. doi:10.1097/ICO.0b013e3181c325b2
6. Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma. 2008;17(5):350–355. doi:10.1097/IJG.0b013e31815c5f4f
7. Goldstein MH, Silva FQ, Blender N, Tran T, Vantipalli S. Ocular benzalkonium chloride exposure: problems and solutions. Eye. 2022;36(2):361–368. doi:10.1038/s41433-021-01668-x
8. Kahook MY, Rapuano CJ, Messmer EM, Radcliffe NM, Galor A, Baudouin C. Preservatives and ocular surface disease: a review. Ocul Surf. 2024;34:213–224. doi:10.1016/j.jtos.2024.08.001
9. Zhou X, Zhang X, Zhou D, Zhao Y, Duan X. A narrative review of ocular surface disease related to anti-glaucomatous medications. Ophthalmol Ther. 2022;11(5):1681–1704. doi:10.1007/s40123-022-00557-0
10. Pérez-Bartolomé F, Martínez-de-la-Casa JM, Arriola-Villalobos P, Fernández-Pérez C, Polo V, García-Feijoó J. Ocular surface disease in patients under topical treatment for glaucoma. Eur J Ophthalmol. 2017;27(6):694–704. doi:10.5301/ejo.5000977
11. Baudouin C, Renard JP, Nordmann JP, et al. Prevalence and risk factors for ocular surface disease among patients treated over the long term for glaucoma or ocular hypertension. Eur J Ophthalmol. 2013;23(1):47–54. doi:10.5301/ejo.5000181
12. Wolfram C, Stahlberg E, Pfeiffer N. Patient-Reported Nonadherence with Glaucoma Therapy. J Ocul Pharmacol Ther. 2019;35(4):223–228. doi:10.1089/jop.2018.0134
13. Newman-Casey PA, Niziol LM, Gillespie BW, Janz NK, Lichter PR, Musch DC. The association between medication adherence and visual field progression in the collaborative initial glaucoma treatment study. Ophthalmology. 2020;127(4):477–483. doi:10.1016/j.ophtha.2019.10.022
14. Skalicky SE, Goldberg I, McCluskey P. Ocular surface disease and quality of life in patients with glaucoma. Am J Ophthalmol. 2012;153(1):1–9.e2. doi:10.1016/j.ajo.2011.05.033
15. Nordmann JP, Auzanneau N, Ricard S, Berdeaux G. Vision related quality of life and topical glaucoma treatment side effects. Health Qual Life Outcomes. 2003;1:75. doi:10.1186/1477-7525-1-75
16. Broadway DC, Grierson I, O’Brien C, Hitchings RA. Adverse effects of topical antiglaucoma medication. II. The outcome of filtration surgery. Arch Ophthalmol. 1994;112(11):1446–1454. doi:10.1001/archopht.1994.01090230060021
17. Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814.e1. doi:10.1016/j.ajo.2011.10.024
18. Sagara H, Sekiryu T, Noji H, Ogasawara M, Sugano Y, Horikiri H. Meibomian gland loss due to trabeculectomy. Jpn J Ophthalmol. 2014;58(4):334–341. doi:10.1007/s10384-014-0324-6
19. Ji H, Zhu Y, Zhang Y, Li Z, Ge J, Zhuo Y. Dry eye disease in patients with functioning filtering blebs after trabeculectomy. PLoS One. 2016;11(3):e0152696. doi:10.1371/journal.pone.0152696
20. Balas M, Mathew DJ. Minimally invasive glaucoma surgery: a review of the literature. Vision. 2023;7(3):54. doi:10.3390/vision7030054
21. Samuelson TW, Katz LJ, Wells JM, Duh YJ, Giamporcaro JE. Randomized evaluation of the trabecular micro-bypass stent with phacoemulsification in patients with glaucoma and cataract. Ophthalmology. 2011;118(3):459–467. doi:10.1016/j.ophtha.2010.07.007
22. Samuelson TW, Sarkisian SRJ, Lubeck DM, et al. Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology. 2019;126(6):811–821. doi:10.1016/j.ophtha.2019.03.006
23. Schweitzer JA, Hauser WH, Ibach M, et al. Prospective Interventional cohort study of ocular surface disease changes in eyes after trabecular Micro-Bypass Stent(s) Implantation (iStent or iStent inject) with phacoemulsification. Ophthalmol Ther. 2020;9(4):941–953. doi:10.1007/s40123-020-00290-6
24. Jones L, Maes N, Qidwai U, Ratnarajan G. Impact of minimally invasive glaucoma surgery on the ocular surface and quality of life in patients with glaucoma. Ther Adv Ophthalmol. 2023;15. doi:10.1177/25158414231152765:doi
25. Alves M, Asbell P, Dogru M, et al. TFOS lifestyle report: impact of environmental conditions on the ocular surface. Ocul Surf. 2023;29:1–52. doi:10.1016/j.jtos.2023.04.007
26. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
27. Miller KL, Walt JG, Mink DR, et al. Minimal clinically important difference for the ocular surface disease index. Arch Ophthalmol. 2010;128(1):94–101. doi:10.1001/archophthalmol.2009.356
28. Starr CE, Gupta PK, Farid M, et al. An algorithm for the preoperative diagnosis and treatment of ocular surface disorders. J Cataract Refract Surg. 2019;45(5):669–684. doi:10.1016/j.jcrs.2019.03.023
29. Pérez Bartolomé F, Martínez de la Casa JM, Arriola Villalobos P, et al. Ocular redness measured with the keratograph 5M in patients using anti-glaucoma eye drops. Semin Ophthalmol. 2018;33(5):643–650. doi:10.1080/08820538.2017.1395891
30. OCULUS Optikgeräte GmbH. Oculus Keratograph Instruction Manual.
31. Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–650. doi:10.1097/00003226-200310000-00008
32. Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology. 2008;115(5):911–915. doi:10.1016/j.ophtha.2007.06.031
33. Graae Jensen P, Gundersen M, Nilsen C, et al. Prevalence of dry eye disease among individuals scheduled for cataract surgery in a norwegian cataract clinic. Clin Ophthalmol. 2023;17:1233–1243. doi:10.2147/OPTH.S407805
34. Epitropoulos AT, Matossian C, Berdy GJ, Malhotra RP, Potvin R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672–1677. doi:10.1016/j.jcrs.2015.01.016
35. Hussein O, Musleh A, Abukhaled Y, Hammad A, Feras R, Abu Serhan H. Does standalone phacoemulsification lower intraocular pressure in glaucomatous eyes? A systematic review and meta-analysis. Eye. 2025;39(13):2518–2526. doi:10.1038/s41433-025-03927-7
36. Carolan JA, Liu L, Alexeeff SE, Amsden LB, Shorstein NH, Herrinton LJ. Intraocular pressure reduction after phacoemulsification: a matched cohort study. Ophthalmol Glaucoma. 2020;4(3):277. doi:10.1016/J.OGLA.2020.10.002
37. Guarnieri A, Carnero E, Bleau AM, Alfonso-Bartolozzi B, Moreno-Montañés J. Relationship between OSDI questionnaire and ocular surface changes in glaucomatous patients. Int Ophthalmol. 2020;40(3):741–751. doi:10.1007/s10792-019-01236-z
38. Sullivan BD, Crews LA, Messmer EM, et al. Correlations between commonly used objective signs and symptoms for the diagnosis of dry eye disease: clinical implications. Acta Ophthalmol. 2014;92(2):161–166. doi:10.1111/aos.12012
39. Nichols KK, Nichols JJ, M MPH, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004;23(8):762–770. doi:10.1097/01.ico.0000133997.07144.9e
40. Samuelson TW, Singh IP, Williamson BK, et al. Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ-25 and OSDI from the istent inject® pivotal trial. Am J Ophthalmol. 2021;229:220–229. doi:10.1016/j.ajo.2021.03.007
41. Cox SM, Nichols KK, Nichols JJ. Agreement between automated and traditional measures of tear film breakup. Optom Vis Sci. 2015;92(9):e257–63. doi:10.1097/OPX.0000000000000648
42. García-Marqués JV, Martínez-Albert N, Talens-Estarelles C, García-Lázaro S, Cerviño A. Repeatability of non-invasive keratograph break-up time measurements obtained using oculus keratograph 5M. Int Ophthalmol. 2021;41(7):2473–2483. doi:10.1007/s10792-021-01802-4
43. Naderi K, Gormley J, O’Brart D. Cataract surgery and dry eye disease: a review. Eur J Ophthalmol. 2020;30(5):840–855. doi:10.1177/1120672120929958
44. Jensen P, Nilsen C, Gundersen M, et al. A preservative-free approach - effects on dry eye signs and symptoms after cataract surgery. Clin Ophthalmol. 2024;18:591–604. doi:10.2147/OPTH.S446804
45. Tong L, Hou AH, Wong TT. Altered expression level of inflammation-related genes and long-term changes in ocular surface after trabeculectomy, a prospective cohort study. Ocul Surf. 2018;16(4):441–447. doi:10.1016/j.jtos.2018.06.005
46. Vaajanen A, Nättinen J, Aapola U, Gielen F, Uusitalo H. The effect of successful trabeculectomy on the ocular surface and tear proteomics—a prospective cohort study with 1‐year follow‐up. Acta Ophthalmol. 2021;99(2):160–170. doi:10.1111/aos.14526
47. Agnifili L, Brescia L, Oddone F, et al. The ocular surface after successful glaucoma filtration surgery: a clinical, in vivo confocal microscopy, and immune-cytology study. Sci Rep. 2019;9(1):11299. doi:10.1038/s41598-019-47823-z
48. Lam J, Wong TT, Tong L. Ocular surface disease in posttrabeculectomy/mitomycin C patients. Clin Ophthalmol. 2015;9:187–191. doi:10.2147/OPTH.S70721
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Autologous Platelet‐Rich Plasma Drops for Evaporative Dry Eye Disease from Meibomian Gland Dysfunction: A Pilot Study
Murtaza F, Toameh D, Chiu HH, Tam ES, Somani S
Clinical Ophthalmology 2022, 16:2199-2208
Published Date: 6 July 2022
Engaging Stakeholders to Develop a Roadmap for Dry Eye and MGD PCORI-Funded Research
Warren NA, Maskin SL, Gurupur V, Rector DA, Adelman D, Howell S, McAree J, Dibble R, Carlisano C, Maconi DP, Schrotenboer D, Jaimes M, Marte N, Carlisano T, Toland C, Chung J, Cremers SL, Corbin GS
Patient Related Outcome Measures 2024, 15:143-186
Published Date: 12 May 2024
Shelf-Stable, Cryopreserved Amniotic Membrane for the Management of Ocular Surface Disease: A Retrospective Assessment
Cushman S
Clinical Optometry 2025, 17:409-415
Published Date: 21 December 2025
Low-Level Light Therapy as a Potential Adjunctive Approach in Mucus Fishing Syndrome: Report of Two Clinical Cases
Mancini A, Carnovale-Scalzo G, Mancini M, Borselli M, Taloni A, Chisari D, Lucisano A, Carnevali A, Meduri A, Aragona P, Scorcia V, Giannaccare G
International Medical Case Reports Journal 2025, 18:1679-1684
Published Date: 28 December 2025
Long-Term Evaluation of Autologous Serum Eye Drops in Dry Eye Disease
Velier M, Champoussin J, Dambricourt L, Bec C, Darque A, Lento C, Veran J, Dumoulin C, Dignat-George F, David T, Sabatier F, Magalon J
Clinical Ophthalmology 2026, 20:589337
Published Date: 9 April 2026