")
Back to Journals » Clinical Ophthalmology » Volume 16
Autologous Platelet‐Rich Plasma Drops for Evaporative Dry Eye Disease from Meibomian Gland Dysfunction: A Pilot Study
Authors Murtaza F , Toameh D, Chiu HH , Tam ES , Somani S
Received 24 March 2022
Accepted for publication 22 June 2022
Published 6 July 2022 Volume 2022:16 Pages 2199—2208
DOI https://doi.org/10.2147/OPTH.S367807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fahmeeda Murtaza,1 Dana Toameh,2 Hannah H Chiu,2– 4 Eric S Tam,2– 4 Sohel Somani2– 4
1Temerty Faculty of Medicine, University of Toronto, Toronto, Ontario, Canada; 2Uptown Eye Specialists, Vaughan, Ontario, Canada; 3Division of Ophthalmology, William Osler Health System, Brampton, Ontario, Canada; 4Department of Ophthalmology & Vision Sciences, University of Toronto, Toronto, Ontario, Canada
Correspondence: Sohel Somani, 401-7900 Hurontario Street, Brampton, Ontario, L6Y 0P6, Canada, Tel +416 292-0330, Fax +416 292-0331, Email [email protected]
Purpose: To evaluate the effects of autologous platelet‐rich plasma (PRP) drops for evaporative dry eye (EDE) disease from meibomian gland dysfunction (MGD).
Methods: This is a retrospective, consecutive case series of 20 eyes of 10 patients with EDE from MGD treated with PRP drops from November 2020 to November 2021 at a single outpatient clinic in Ontario, Canada. PRP drops were prepared from whole blood using a two-step centrifugation method. Patients were instructed to instill these drops six times daily for 4 weeks. The Canadian Dry Eye Assessment (CDEA) questionnaire score, patient subjective assessment (PSA) score, first and average non-invasive break-up times (f/a NIBUT), tear meniscus height (TMH), bulbar redness (BR), and meibograph grade (MG) were measured before and after the treatment course.
Results: Significant improvements in dry eye symptoms and tear film parameters were observed. Dry eye symptoms significantly improved as per the CDEA (mean difference (MD) = − 5.45, 95% confidence interval (CI) = [− 7.9, − 3.1], p< 0.001) and PSA (MD = − 2.6, 95% CI = [− 3.9, − 1.2], p< 0.001). There were significant improvements in tear film parameters including fNIBUT (MD = 3.85s, 95% CI = [1.2, 6.8], p=0.006), aNIBUT (MD = − 6.81s, 95% CI = [5.7, 11.1], p< 0.001) and TMH (MD = 0.08, 95% CI = [0.003, 0.2], p=0.045). There was an improvement in conjunctival injection as measured by BR (MD = − 0.36, 95% CI = [− 0.4, − 0.15], p=0.373). Five eyes experienced a one-grade improvement in MG (p=0.453), and none experienced worsening in MG with treatment. No temporary or permanent adverse effects were noted.
Conclusion: Four weeks of PRP therapy resulted in significant functional improvements in dry eye symptoms and tear film quality and quantity. Improvements in conjunctival injection and microstructural improvements in meibomian glands were also observed in some eyes. Overall, PRP is a promising treatment option for patients with EDE from MGD refractory to conventional treatments.
Keywords: platelet-rich plasma, dry eye disease, meibomian gland dysfunction, hemoderivatives, ocular surface disease
Introduction
Evaporative dry eye (EDE) is the most common type of dry eye disease,1,2 resulting from a deficiency in the lipid layer of the tear film that causes increased tear evaporation. EDE is most commonly caused by meibomian gland dysfunction (MGD).1,2 Meibomian glands are small sebaceous glands located along eyelid margins that secrete meibum into the tear film, forming the tear film’s lipid layer. In MGD, atrophy of these glands, obstruction of gland orifices, and/or changes in meibum consistency can alter the lipid layer and cause increased tear evaporation.1–3 First-line treatments for patients with EDE from MGD include artificial tears, eyelid scrubs, and warm compresses. Patients with severe, refractory symptoms often require more advanced treatments such as punctal plugs, lifitegrast drops, cyclosporine drops, corticosteroid drops, antibiotic drops, omega-3 supplements, oral azithromycin or tetracyclines, intense pulsed light therapy or lipiflow thermal pulsation therapy.4–6 However, many patients still do not achieve complete or long-term relief with these treatments.
In the last decade, topical and injectable hemoderivatives have gained acceptance as more effective treatments for severe and refractory ocular surface diseases. Autologous serum (AS) drops are made from the patient’s own blood and are similar in composition to human tears.7 AS drops contain a higher concentration of vitamin A, lysozyme, transforming growth factor‐β (TGF‐β), and fibronectin.7 However, the preparation of AS drops involves the removal of a thick layer of platelets and growth factors that can provide additional benefits.8,9
Autologous platelet-rich plasma (PRP) drops contain 1.5 times as many platelets as AS drops, with platelet concentrations often exceeding 1 million/mL.10,11 PRP drops have been found to reduce inflammation, stimulate wound healing and promote ocular surface regeneration in patients with corneal ulcers and perforations,12,13 persistent epithelial defects,14 chemical burns,15,16 lacrimal gland dysfunction,17 ocular surface syndrome following refractive surgery,18 blepharoplasties,19 and graft-versus-host disease.20 Some studies have evaluated the effects of PRP drops in patients with dry eye disease and found significant improvements in dry eye symptoms, lacrimal meniscus, conjunctival hyperemia, corneal fluorescein staining and an increase in conjunctival goblet cells.8,21
To date, no studies have evaluated the effects of PRP drops on meibomian glands, which are important mediators in the development of EDE. Herein, we evaluate the effects of 4-weeks of topical PRP drops on tear film quantity and quality, conjunctival injection and meibomian gland health in patients with EDE from MGD.
Methods
Patient Selection
This retrospective, consecutive case series was approved by the William Osler Health System Research Ethics Board (WOHS REB) and adhered to the Declaration of Helsinki. Patient consent to review medical records was not required by the WOHS REB. Medical records of patients undergoing PRP treatment at a single outpatient clinic between November 2020 and November 2021 were extracted. All efforts were made to protect patient confidentiality.
Inclusion and Exclusion Criteria
Patients aged 18 and older, with evaporative dry eye (EDE) from meibomian gland dysfunction (MGD) refractory to conventional treatments were included. Patients were considered to have refractory dry eye if they experienced continued or worsening dry eye symptoms for 1 year or more with consistent use of first line treatments such as preservative-free artificial tears, eyelid scrubs, or warm compresses. EDE was diagnosed by an ophthalmologist (SS) based on the meibograph grade (MG), and only eyes with a MG ≥2 (out of 4) were included. Patients were excluded if they wore contact lenses, received cataract or refractive surgery within the last 6 months, were taking antiplatelet medications or had active allergies or ocular infections. Patients with blood-borne infectious diseases such as hepatitis, syphilis, or HIV were ineligible for PRP treatment. Only patients with complete baseline, pre-treatment and post-treatment data were included.
PRP Treatment Protocol
PRP was prepared using a 2-step centrifugation method illustrated in Figure 1.18,22 In brief, 22 mL of blood was drawn via venipuncture into sterile tubes containing 2 mL of acid-citrate-dextrose solution A, which prevents platelet activation. The citrated blood was centrifuged at 1500g for 10 minutes using Eclipse® Easy Spin Centrifuge (Model HW8M, Eclipse Med Global). Subsequently, the plasma layer (top) and buffy coat layer (middle) containing platelets were extracted and centrifuged again at 1500g for 10 minutes. The entire platelet-rich pellet (bottom layer) was extracted and resuspended with some platelet-poor plasma (top layer) to create an 11mL PRP suspension. This suspension was then aliquoted into the COL10 E-Drop system (Salient Medical Solutions, Canada), generating 10 vials. Patients were advised to shake vials prior to use and instill PRP drops 6 times a day for 4 weeks. Patients were also advised to keep used vials refrigerated and unused vials frozen. Patients were instructed to continue using any baseline topical medications or therapies for their dry eyes during the treatment course.
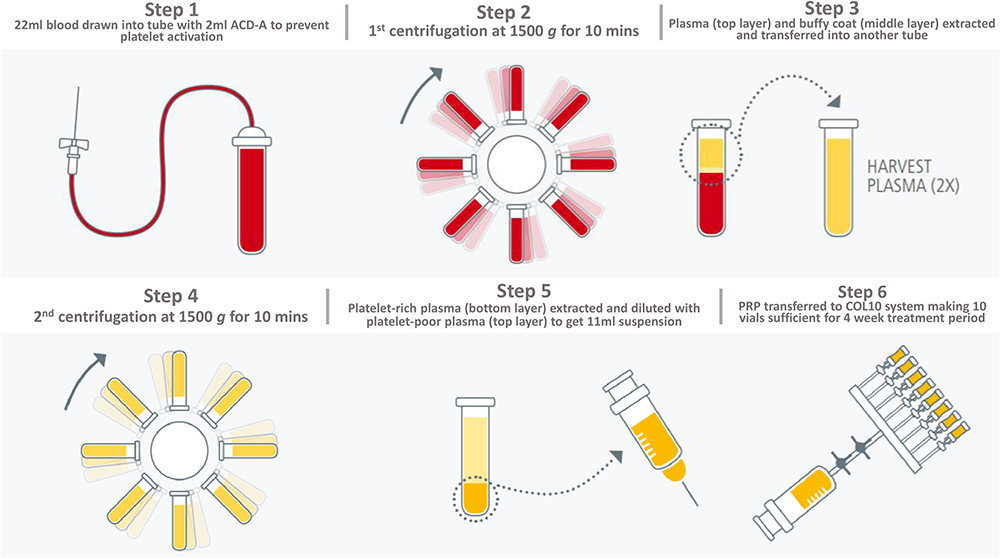 |
Figure 1 PRP was prepared using a 2-step centrifugation method.18,22 Step 1: 22 mL of blood was drawn into tubes containing 2mL of acid-citrate-dextrose solution A. Step 2: The citrated blood was centrifuged at 1500g for 10 minutes. Step 3: The plasma layer (top) and buffy coat layer (middle) containing platelets were extracted. Step 4: Both layers were centrifuged again at 1500g for 10 minutes. Step 5: The entire platelet-rich pellet (bottom layer) was extracted and resuspended with some platelet-poor plasma (top layer) to create an 11mL PRP suspension. Step 6: PRP suspension was aliquoted into vials for storage. |
Clinical Outcomes
The following clinical outcomes were measured before and after 4 weeks of PRP treatment: CDEA score, PSA score, first and average non-invasive break-up times (f/a NIBUT), tear meniscus height (TMH), bulbar redness (BR) and meibograph grade (MG).
The 12-item Canadian Dry Eye Assessment (CDEA) questionnaire is a modification of the validated Ocular Surface Disease Index (OSDI), used to determine the severity of dry eye symptoms.23,24 Total scores range from 0 to 48 and symptoms are interpreted as normal (<5), mild (5–20), moderate (21–30), or severe (31–48).24 The question “How much do your eyes bother you?” within the CDEA was evaluated independently and referred to as the “Patient Subjective Assessment (PSA)”. PSA scores range from 1 representing “not at all” to 10 representing “extremely and constantly”. A higher score indicates greater severity of symptoms.
The f/a NIBUT, TMH and BR scores were automatically generated by a Keratograph 5M (OCULUS, Wetzlar, Germany), equipped with a modified tear film scanning function. These ocular examinations were conducted by trained ophthalmic technicians blinded to the patients’ ocular or treatment status.
For non-invasive break-up time (NIBUT) measurements, patients were instructed to keep their eyes open for as long as possible. First NIBUT was measured as the time between the last complete blink and the first perturbation of a grid projected onto the surface of the cornea.25 Average NIBUT was calculated by averaging all break-up events. Generally, a break-up time of ≤5 seconds suggests dry eyes.26
The tear meniscus height (TMH) was measured as the distance between the darker edge of the lower eyelid and the tear strip. The final TMH was calculated from the average of the TMH measurements at the left, right and center of each eyelid (Figure 2). A TMH of <0.25 mm is suggestive of dry eye disease.27
 |
Figure 2 Tear meniscus height (TMH) measurements as generated by the Keratograph 5M. The final TMH is calculated from the average of the TMH measurements at the left, right and center of each eyelid. The final TMH in this eye is 0.36 mm. |
The bulbar redness (BR) score was determined by the area percentage ratio of vessels to the bulbar conjunctiva under illumination. The maximum ratio is 40%, therefore, BR scores range from 0.0 to 4.0. A higher score represents increased BR.28
The meibograph grade (MG) was determined by the degree of meibomian gland dropout or percentage of partial glands in the upper eyelids only. The MG was graded by an ophthalmologist (SS) blinded to the patient’s ocular or treatment status. The MG ranges from 1 to 4, where grade 1 represents no partial glands, grade 2 represents <25% partial glands, grade 3 represents 25%−75% partial glands, and grade 4 represents >75% partial glands.29
Statistical Analysis
Statistical analyses were performed using SPSS Statistics Version 27.0 (IBM, Armonk, NY). Continuous variables were described using means ± standard deviations (SD), mean differences (MD) with 95% confidence intervals (95% CI), and medians with interquartile ranges (IQR). Categorical variables were described using proportions. A linear mixed model was used to determine treatment effects. This model accounted for interrelationships between both eyes of the same patient. All tests were two-tailed. A p-value of <0.05 was used to confer statistical significance.
Results
Baseline Demographics
20 eyes of 10 patients met the inclusion criteria. The median age was 71 years (range 51–84), and the sample was 50.0% female (Table 1). The treatment interval was 4 weeks. The mean follow-up duration was 31.2 ± 2.74 days (range 28–35 days).
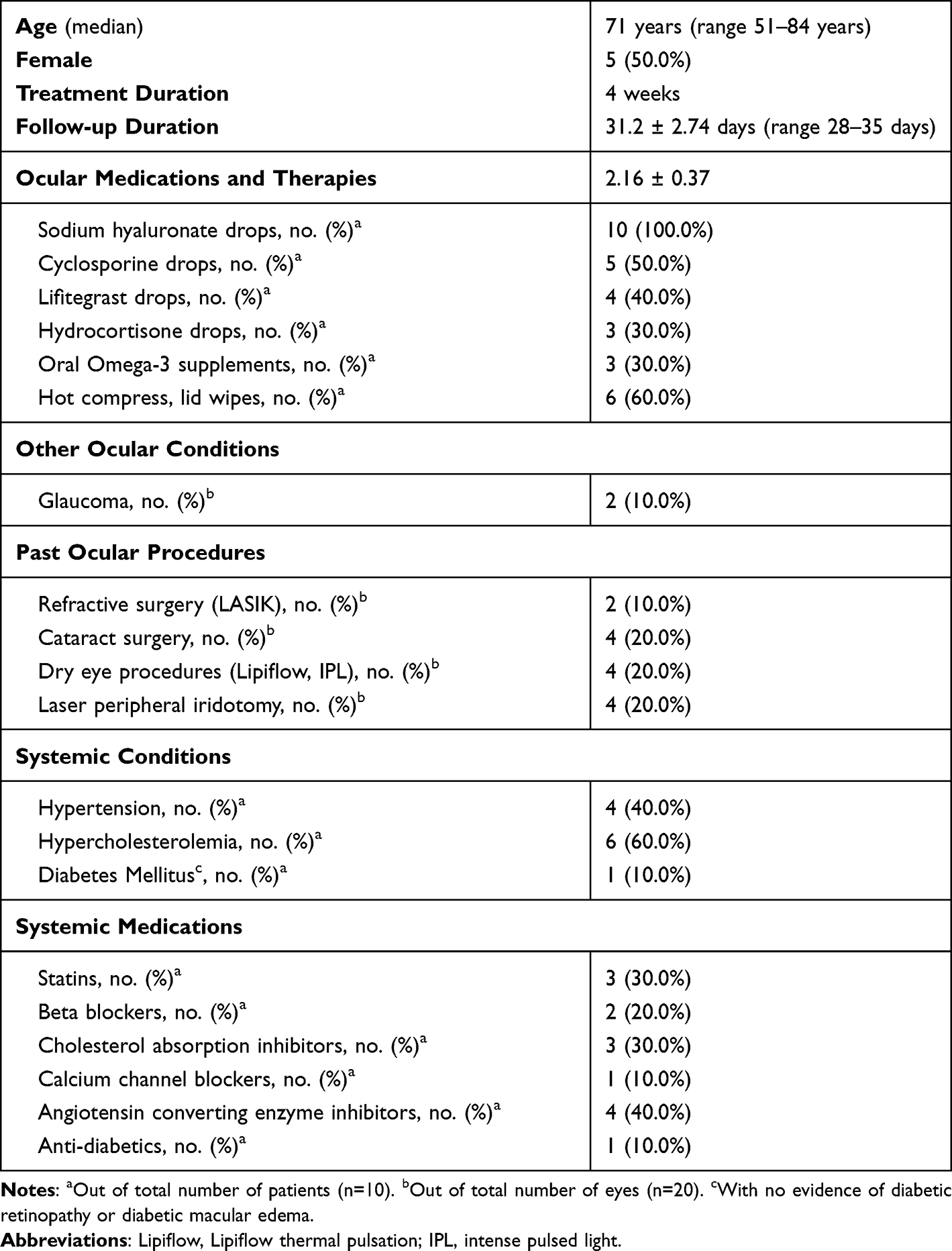 |
Table 1 Patient Demographics and Baseline Clinical Features |
On average, patients were using 2.16 ± 0.37 topical dry eye medications at baseline, including cyclosporine, sodium hyaluronate, lifitegrast and hydrocortisone drops. Three patients (30.0%) were concurrently using oral Omega-3 supplements. Four eyes (20.0%) had undergone cataract surgery, two eyes (10.0%) had undergone refractive (LASIK) surgery, and four eyes (20.0%) had undergone dry eye procedures, including lipiflow thermal pulsation therapy and intense pulsed light therapy. All eyes had undergone these procedures at least one year before starting the PRP treatment course.
With regards to systemic conditions, six (60.0%) patients had hypercholesterolemia, four (40.0%) had hypertension and one (10.0%) had type II diabetes mellitus but were not receiving treatment for diabetic retinopathy. On average, patients were taking 1.11 ± 0.18 oral medications to manage these conditions.
Clinical Outcomes
The mean CDEA score decreased significantly from 16.89 ± 3.82 to 11.44 ± 3.47 out of 48 (mean difference (MD) = −5.45, 95% confidence interval (CI) = [−7.9, −3.1], p<0.001; Figure 3 and Table 2). The mean PSA score decreased significantly from 6.70 ± 2.63 to 4.10 ± 1.73 out of 10 (MD = −2.60, 95% CI = [−3.9, −1.2], p<0.001; Figure 3 and Table 2). All patients reported an improvement in the CDEA and PSA scores, with one patient experiencing no dry eye symptoms after treatment.
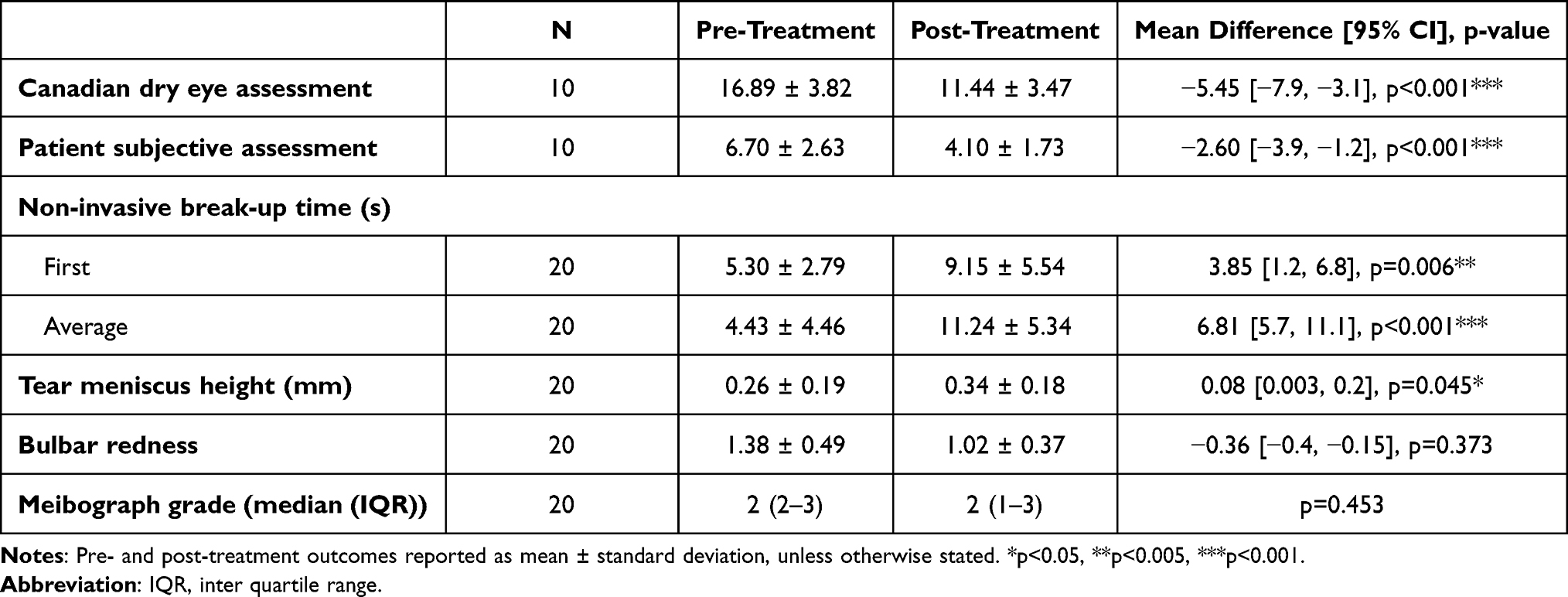 |
Table 2 Clinical Outcomes with 4 Weeks of Autologous Platelet-Rich Plasma Drops |
 |
Figure 3 PRP treatment resulted in significant improvements in patient-reported outcomes as measured by the Canadian dry eye assessment (CDEA, (A)) and patient subjective assessment (PSA, (B)). ***p<0.001. |
The mean fNIBUT and aNIBUT significantly improved from 5.30 ± 2.79s to 9.15 ± 5.54s (MD = 3.85, 95% CI = [1.2, 6.8], p=0.006) and from 4.43 ± 4.46s to 11.24 ± 5.34s (MD = 6.81, 95% CI = [5.7, 11.1], p<0.001), respectively (Figure 4 and Table 2). The mean TMH significantly increased from 0.26 ± 0.19mm to 0.34 ± 0.18mm (MD = 0.08, 95% CI = [0.003, 0.2], p=0.045; Figure 4 and Table 2). The mean BR decreased from 1.38 ± 0.49 to 1.02 ± 0.37 (MD = −0.36, 95% CI = [−0.4, −0.15], p=0.373; Figure 4 and Table 2). F/a NIBUT, TMH and BR did not worsen with PRP treatment in any of the patients.
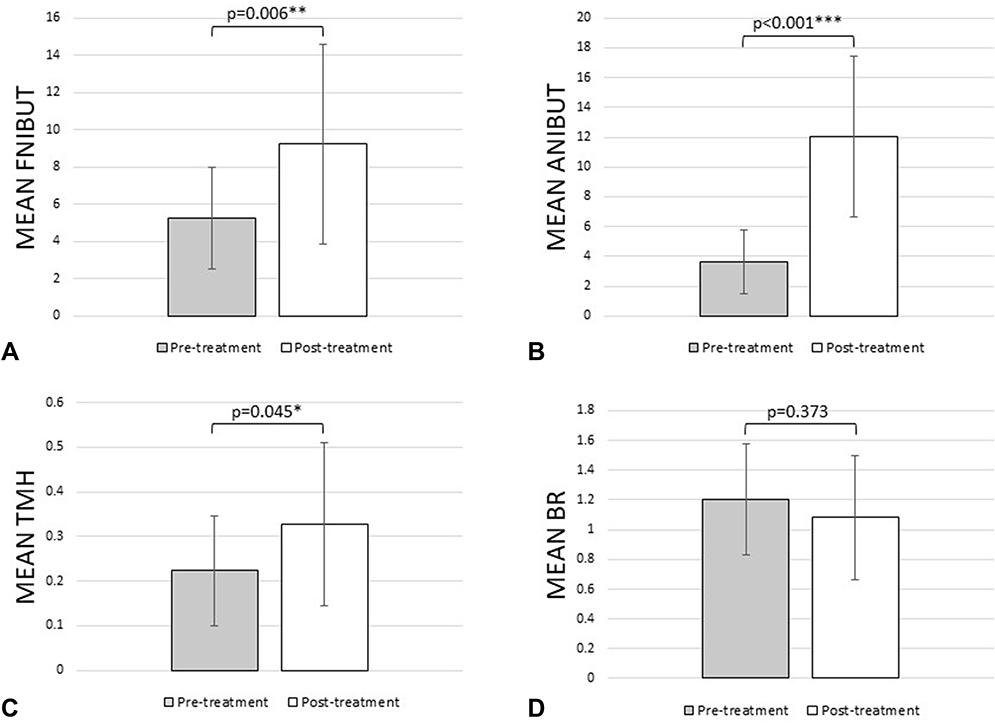 |
Figure 4 PRP treatment resulted in significant improvements in functional dry eye outcomes as measured by the change in mean first non-invasive break-up time (fNIBUT, (A)), mean average non-invasive break-up time (aNIBUT, (B)), mean tear meniscus height (TMH, (C)), and mean bulbar redness (BR, (D)). *p<0.05, **p<0.005, ***p<0.001. |
The median MG was unchanged from 2 (IQR 2–3) at baseline to 2 (IQR 1–3) after treatment (p=0.453; Table 2). Five eyes (25.0%) experienced an improvement in MG, all by one grade. There was no worsening of MG with treatment.
Safety
Patients reported no discomfort or irritation during PRP extraction or instillation. No temporary or permanent adverse events, including erythema, edema or pain were reported during or shortly after the treatment course.
Discussion
This is the first study to evaluate the effects of topical autologous platelet-rich plasma (PRP) on meibomian gland health. Our findings suggest that PRP leads to improvements in dry eye symptoms and tear film stability and quantity. There were also some improvements in conjunctival injection and structural improvements of the meibomian glands.
All patients in our study experienced an improvement in dry eye symptoms with treatment, which is consistent with findings in existing literature on dry eye patients.8,21,30–32 Dry eye symptoms are an important indicator of patient functionality and rehabilitation. Although associations between dry eye symptoms and clinical examinations are low and inconsistent,33 we believe the improvements in symptoms were attributable to improvements in NIBUT, TMH, BR and MG. All of our patients had mild to moderate dry eye symptoms before treatment but were using two or more topical medications in combination with oral supplements and dry eye therapies to manage their symptoms. While we encouraged our patients to continue their pre-treatment dry eye regimens after undergoing PRP therapy, our findings suggest that PRP drops have the potential to reduce treatment and medication burden in patients using multiple first-line therapies.
We observed a non-significant improvement in BR scores with PRP treatment. PRP contains anti-inflammatory molecules such as interleukin-1 receptor antagonists,12 which may directly reduce BR by limiting pro-inflammatory mediators at the ocular surface, and in doing so, indirectly dilute them and reduce the tear film osmolarity.
In keeping with the literature,8,21,34,35 we found a significant improvement in f/a NIBUT and TMH scores. PRP contains a high concentration of epitheliotropic growth factors including platelet-derived growth factor, fibroblast growth factor, epidermal growth factor, fibronectin, and platelet factor IV that target a variety of cells, including conjunctival goblet cells.36–39 Conjunctival goblet cells are simple, columnar cells within the conjunctival epithelium that secrete mucins into the tear film and are found to be decreased in dry eye disease.40–42 Alio et al21 found an increase in conjunctival goblet cells with 1 month of PRP drops. Although we did not perform impression cytology in our study, the improvements in f/a NIBUT and TMH may be attributable to the regeneration and proliferation of these cells. These improvements could also be attributable to changes in the meibomian gland structure.
We also observed a trend towards an improved MG, with 25% of eyes improving by one grade. In vivo studies have found that growth factors in PRP improve recruitment of dermal-derived stem cells in the regeneration of sweat glands, acinar and ductal cells.42 Meibomian glands are holocrine sebaceous glands that discharge meibum onto the lid margin and share similar structural features.40 In MGD, atrophy of the glands, obstruction of gland orifices, alteration of meibomian secretions or a combination of these processes affect tear film stability and quantity. The significant improvements observed in f/a NIBUT and TMH scores, in the context of clinical improvements in MG, suggest that PRP may stimulate the growth and regeneration of cells lining the meibomian gland orifices, thereby promoting meibum outflow. Anti-inflammatory mediators in PRP may also contribute to these improvements as they limit pro-inflammatory cytokines such as IL-1, IL-6, IL-17, and IL-22, which are known to cause lymphocyte infiltration and inflammation of gland orifices.44,45 However, our findings are limited by our measurement technique as MG scores were based on the percentage of partial glands in the upper eyelids only. Further, MG scores only quantify gross structural changes of the meibomian glands, which may underestimate the true effects of PRP therapy on meibomian gland health. We may have observed significant microstructural changes had we used other imaging modalities such as in-vivo confocal microscopy.
On the other hand, an injectable modality may be a more potent option for improving meibomian gland structure in patients with severe MGD. To date, only two studies have used injectable PRP for dry eye in the context of lacrimal gland dysfunction and found significant improvements in functional outcomes.17,34 However, some of these patients experienced temporary injection site inflammation. Although the risks associated with injectable PRP therapy may prevent its widespread adoption in routine ophthalmic practice, its efficacy in improving meibomian gland function merits further investigation.
Although we explored the short-term treatment effects of PRP therapy, the improvements in dry eye symptoms and tear film parameters suggest that long term or pulsed PRP therapy may have the potential to reduce treatment burden and improve quality of life in patients with dry eye resistant to conventional treatments. It is also important to recognize that our study findings are largely dependent on our treatment protocol. Currently, there is no standardized treatment protocol for PRP preparation. Studies on PRP for dry eye report a wide range of treatment parameters, including centrifugation speeds, storage temperatures, dilution concentrations, and clotting times. The preparation of hemoderivatives is an evolving field, and optimization of treatment parameters can bring PRP into mainstream ophthalmic practice.
Limitations
The small sample size of our study limits the applicability of our findings. Our treatment duration was only four weeks, and the average follow-up duration was one month, making it difficult to ascertain the long-term, sustained effects of PRP. Given the short follow-up, it was also difficult to determine the change in the number and types of oral and topical dry eye medications and therapies after PRP treatment. Patients were encouraged to continue their pre-treatment dry eye regimens after PRP treatment. Finally, investigating other clinical parameters such as tear film osmolarity and lipid layer thickness may have been useful in understanding the effects of PRP therapy on EDE and MGD.
Conclusion
This is the first study to explore the effects of topical autologous PRP drops on meibomian gland health in patients with EDE from MGD. We found significant improvements in dry eye symptoms, first and average tear break-up times, and tear meniscus height with 4 weeks of PRP therapy. There was a trend towards an improved bulbar redness and meibograph grade, with 25% of eyes improving by one grade. With its high concentration of platelets and growth factors, PRP is a promising treatment option for patients with dry eye refractory to conventional treatments such as artificial tears. Future research should investigate optimizing PRP preparation parameters and determining the long-term effects of PRP therapy.
Acknowledgments
This paper was a presented as an e-poster at the European Society of Cataract and Refractive Surgeons (ESCRS) Winter Meeting, February 18–20, 2022 (Virtual) and American Society of Cataract and Refractive Surgeons (ASCRS) Annual Meeting, April 22–26, 2022 (Virtual).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
2. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
3. Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2011;52(4):2050–2064. doi:10.1167/iovs.10-6997g
4. Qiao J, Yan X. Emerging treatment options for meibomian gland dysfunction. Clin Ophthalmol. 2013;7:1797–1803. doi:10.2147/OPTH.S33182
5. Kojima T, Dogru M, Kawashima M, Nakamura S, Tsubota K. Advances in the diagnosis and treatment of dry eye. Prog Retin Eye Res. 2020;78:100842. doi:10.1016/j.preteyeres.2020.100842
6. Murtaza F, Toameh D, Al-Habib S, et al. Safety and efficacy of broadband intense pulsed light therapy for dry eye disease with meibomian gland dysfunction. Clin Ophthalmol. 2021;15:3983–3991. doi:10.2147/OPTH.S331289
7. Pan Q, Angelina A, Marrone M, Stark WJ, Akpek EK. Autologous serum eye drops for dry eye. Cochrane Database Syst Rev. 2017;2(2):CD009327. doi:10.1002/14651858.CD009327.pub3
8. Alio JL, Rodriguez AE, Ferreira-Oliveira R, Wróbel-Dudzińska D, Abdelghany AA. Treatment of dry eye disease with autologous platelet-rich plasma: a prospective, interventional, non-randomized study. Ophthalmol Ther. 2017;6(2):285–293. doi:10.1007/s40123-017-0100-z
9. Cole BJ, Seroyer ST, Filardo G, Bajaj S, Fortier LA. Platelet-rich plasma: where are we now and where are we going? Sports Health. 2010;2(3):203–210. doi:10.1177/1941738110366385
10. Wroblewski AP, Mejia HA, Wright VJ. Application of platelet-rich plasma to enhance tissue repair. Oper Tech Orthop. 2010;20(2):98–105. doi:10.1053/j.oto.2009.10.006
11. Brass L. Understanding and evaluating platelet function. Hematology Am Soc Hematol Educ Program. 2010;2010:387–396. doi:10.1182/asheducation-2010.1.387
12. Alio JL, Abad M, Artola A, Rodriguez-Prats JL, Pastor S, Ruiz-Colecha J. Use of autologous platelet-rich plasma in the treatment of dormant corneal ulcers. Ophthalmology. 2007;114(7):1286–1293.e1. doi:10.1016/j.ophtha.2006.10.044
13. Alio JL, Rodriguez AE, Martinez LM. Bovine pericardium membrane (tutopatch) combined with solid platelet-rich plasma for the management of perforated corneal ulcers. Cornea. 2013;32(5):619–624. doi:10.1097/ICO.0b013e31825a6d9a
14. Ronci C, Ferraro AS, Lanti A, et al. Platelet-rich plasma as treatment for persistent ocular epithelial defects. Transfus Apher Sci. 2015;52(3):300–304. doi:10.1016/j.transci.2014.12.027
15. Marquez De Aracena Del Cid R, Montero De Espinosa Escoriaza I. Subconjunctival application of regenerative factor-rich plasma for the treatment of ocular alkali burns. Eur J Ophthalmol. 2009;19(6):909–915. doi:10.1177/112067210901900603
16. Panda A, Jain M, Vanathi M, Velpandian T, Khokhar S, Dada T. Topical autologous platelet-rich plasma eyedrops for acute corneal chemical injury. Cornea. 2012;31(9):989–993. doi:10.1097/ICO.0b013e3182114661
17. Avila MY. Restoration of human lacrimal function following platelet-rich plasma injection. Cornea. 2014;33(1):18–21. doi:10.1097/ICO.0000000000000016
18. Alio JL, Pastor S, Ruiz-Colecha J, Rodriguez A, Artola A. Treatment of ocular surface syndrome after LASIK with autologous platelet-rich plasma. J Refract Surg. 2007;23(6):617–619. doi:10.3928/1081-597X-20070601-13
19. Vick VL, Holds JB, Hartstein ME, Rich RM, Davidson BR. Use of autologous platelet concentrate in blepharoplasty surgery. Ophthalmic Plast Reconstr Surg. 2006;22(2):102–104. doi:10.1097/01.iop.0000202092.73888.4c
20. Pezzotta S, Del Fante C, Scudeller L, Cervio M, Antoniazzi ER, Perotti C. Autologous platelet lysate for treatment of refractory ocular GVHD. Bone Marrow Transplant. 2012;47(12):1558–1563. doi:10.1038/bmt.2012.64
21. Alio JL, Colecha JR, Pastor S, Rodriguez A, Artola A. Symptomatic dry eye treatment with autologous platelet-rich plasma. Ophthalmic Res. 2007;39(3):124–129. doi:10.1159/000100933
22. Bernabei F, Roda M, Buzzi M, Pellegrini M, Giannaccare G, Versura P. Blood-based treatments for severe dry eye disease: the need of a consensus. J Clin Med. 2019;8(9):1478. doi:10.3390/jcm8091478
23. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
24. Jackson WB. Management of dysfunctional tear syndrome: a Canadian consensus. Can J Ophthalmol. 2009;44(4):385–394. doi:10.3129/i09-015
25. Hong J, Sun X, Wei A, et al. Assessment of tear film stability in dry eye with a newly developed keratograph. Cornea. 2013;32(5):716–721. doi:10.1097/ICO.0b013e3182714425
26. Alfaro-Juárez A, Caro-Magdaleno M, Montero-Iruzubieta J, et al. Keratograph 5M as a useful and objective tool for evaluating the ocular surface in limbal stem cell deficiency. Clin Ophthalmol. 2019;13:2025–2033. doi:10.2147/OPTH.S218313
27. Yokoi N, Komuro A. Non-invasive methods of assessing the tear film. Exp Eye Res. 2004;78(3):399–407. doi:10.1016/j.exer.2003.09.020
28. Wu S, Hong J, Tian L, Cui X, Sun X, Xu J. Assessment of Bulbar redness with a newly developed keratograph. Optom Vis Sci. 2015;92(8):892–899. doi:10.1097/OPX.0000000000000643
29. Nichols JJ, Berntsen DA, Mitchell GL, Nichols KK. An assessment of grading scales for meibography images. Cornea. 2005;24(4):382–388. doi:10.1097/01.ico.0000148291.38076.59
30. García-Conca V, Abad-Collado M, Hueso-Abancens JR, et al. Efficacy and safety of treatment of hyposecretory dry eye with platelet-rich plasma. Acta Ophthalmol. 2019;97(2):e170–e178. doi:10.1111/aos.13907
31. Sanchez-Avila RM, Merayo-Lloves J, Riestra AC, et al. The effect of immunologically safe plasma rich in growth factor eye drops in patients with Sjögren syndrome. J Ocul Pharmacol Ther. 2017;33(5):391–399. doi:10.1089/jop.2016.0166
32. Fea AM, Aragno V, Testa V, et al. The effect of autologous platelet lysate eye drops: an in vivo confocal microscopy study. Biomed Res Int. 2016;2016:8406832. doi:10.1155/2016/8406832
33. Kyei S, Dzasimatu SK, Asiedu K, Ayerakwah PA. Association between dry eye symptoms and signs. J Curr Ophthalmol. 2018;30(4):321–325. doi:10.1016/j.joco.2018.05.002
34. Avila MY, Igua AM, Mora AM. Randomised, prospective clinical trial of platelet-rich plasma injection in the management of severe dry eye. Br J Ophthalmol. 2018;103(5). doi:10.1136/bjophthalmol-2018-312072
35. Ribeiro MVMR, Barbosa FT, Ribeiro LEF, et al. Platelet-rich plasma in diabetic dry eye disease. Rev Bras Oftalmol. 2016;75(4):308–313. doi:10.5935/0034-7280.20160061
36. Watanabe K, Nakagawa S, Nishida T. Stimulatory effects of fibronectin and EGF on migration of corneal epithelial cells. Invest Ophthalmol Vis Sci. 1987;28(2):205–211.
37. Klenkler B, Sheardown H, Jones L. Growth factors in the tear film: role in tissue maintenance, wound healing, and ocular pathology. Ocul Surf. 2007;5(3):228–239.
38. Mandić JJ, Kozmar A, Kusačić-Kuna S, et al. The levels of 12 cytokines and growth factors in tears: hyperthyreosis vs euthyreosis. Graefes Arch Clin Exp Ophthalmol. 2018;256(4):845–852. doi:10.1007/s00417-017-3892-6
39. Lubkowska A, Dolegowska B, Banfi G. Growth factor content in PRP and their applicability in medicine. J Biol Regul Homeost Agents. 2012;26(2Suppl 1):3S–22S.
40. Holland EJ, Mannis MJ, Lee WB. Ocular Surface Disease: Cornea, Conjunctiva and Tear Film: Expert Consult-Online and Print. Elsevier Health Sciences; 2013.
41. Barbosa FL, Xiao Y, Bian F, et al. Goblet cells contribute to ocular surface immune tolerance-implications for dry eye disease. Int J Mol Sci. 2017;18(5):978. doi:10.3390/ijms18050978
42. Gipson IK. Goblet cells of the conjunctiva: a review of recent findings. Prog Retin Eye Res. 2016;54:49–63. doi:10.1016/j.preteyeres.2016.04.005
43. Roubelakis MG, Trohatou O, Roubelakis A, et al. Platelet-rich plasma (PRP) promotes fetal mesenchymal stem/stromal cell migration and wound healing process. Stem Cell Rev Rep. 2014;10(3):417–428. doi:10.1007/s12015-013-9494-8
44. Luo L, Li DQ, Doshi A, Farley W, Corrales RM, Pflugfelder SC. Experimental dry eye stimulates production of inflammatory cytokines and MMP-9 and activates MAPK signaling pathways on the ocular surface. Invest Ophthalmol Vis Sci. 2004;45(12):4293–4301. doi:10.1167/iovs.03-1145
45. Tan X, Sun S, Liu Y, et al. Analysis of Th17-associated cytokines in tears of patients with dry eye syndrome. Eye. 2014;28(5):608–613. doi:10.1038/eye.2014.38
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.