Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Efficacy and Safety of Negative Pressure Wound Therapy in Diabetic Foot Ulcers: A Cross-Sectional Analysis of Overlapping Meta-Analyses
Authors Du Y, Zhai T, Sheng Z, Xie W, Jia Z ![]() , Wen T, Zhao X, Tong X
, Wen T, Zhao X, Tong X
Received 13 September 2025
Accepted for publication 4 November 2025
Published 11 November 2025 Volume 2025:18 Pages 4099—4112
DOI https://doi.org/10.2147/DMSO.S565993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Ying Du,1,2,* Tiangang Zhai,1,3,* Zhujun Sheng,3 Weinan Xie,3 Zhiwei Jia,2 Tianlin Wen,2 Xiyan Zhao,3 Xiaolin Tong3
1Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Department of Orthopedics, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 3Department of Endocrinology, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tianlin Wen, Department of Orthopedics, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China, Email [email protected] Xiaolin Tong, Department of Endocrinology, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China, Email [email protected]
Objective: Negative pressure wound therapy (NPWT) is a key intervention for diabetic foot ulcers (DFUs). However, the body of meta-analytic evidence is fraught with conflicting findings, creating significant clinical uncertainty. This study was designed to harmonize the discordant evidence, identify the most methodologically robust meta-analysis, and formulate a clear, evidence-based recommendation for the clinical use of NPWT.
Methods: We conducted a comprehensive search of the PubMed, Embase, and Cochrane Library databases to identify all pertinent meta-analyses. The methodological quality of each included review was rigorously assessed using the Assessment of Multiple Systematic Reviews (AMSTAR) instrument. The Jadad decision algorithm was then employed to systematically select the most reliable and robust evidence.
Results: Eight meta-analyses met the inclusion criteria, with AMSTAR scores ranging from 6 to 9. The formal application of the Jadad decision algorithm identified the meta-analysis by Deng et al as the definitive source of best available evidence. This meta-analysis demonstrated that NPWT significantly improved wound healing rates (risk ratio = 1.46) and decreased amputation rates (risk ratio = 0.69) relative to conventional therapy, while also shortening granulation tissue formation time without increasing adverse events.
Conclusion: The highest-quality evidence, harmonized through this appraisal, confirms that NPWT is a safe and effective adjunctive therapy for DFUs. Its demonstrated ability to accelerate healing while reducing amputations provides a strong evidence base for consideration as a key component of standard clinical practice.
Keywords: diabetic foot ulcer, negative pressure wound therapy, vacuum-assisted closure, systematic review, meta-analysis
Introduction
Diabetic foot ulcers (DFUs) stand as a severe and pervasive complication of diabetes mellitus, with a lifetime incidence that affects up to a quarter of this patient population.1,2 These chronic wounds are a significant source of patient morbidity, precipitating frequent hospitalizations, a diminished quality of life, and a high risk of lower-extremity amputation and subsequent mortality.3,4 The established standard of care for DFUs necessitates a comprehensive, multidisciplinary strategy, integrating glycemic control, meticulous wound debridement, infection management, pressure off-loading, and the application of appropriate dressings.5
Although conventional therapy (CT) utilizing moist dressings remains a fundamental treatment component, its efficacy is often constrained, frequently resulting in protracted healing trajectories and a persistent risk of severe complications.3,6 Conventional wound management typically relies on passive dressings like gauze, cotton, films, and hydrocolloids. While these aim to protect the wound and maintain a moist environment, they possess inherent limitations.3,7,8 For instance, simple gauze dressings can adhere to the wound bed, causing secondary tissue trauma upon removal, and they offer suboptimal exudate management.3,7–9 More advanced options like hydrocolloids improve moisture retention but are primarily passive barriers that do little to actively stimulate the complex biological processes required for healing in compromised wounds like DFUs.10 These limitations have driven the field toward the development of advanced, active therapeutic modalities designed to modulate the wound environment and promote regeneration.7–9 This paradigm shift is evident in the extensive research into strategies such as the use of electrospun biomaterials that mimic the extracellular matrix, the incorporation of nanoparticles (eg, cerium oxide, titanium nanorods) to provide antioxidant and pro-angiogenic properties, and the development of systems for the controlled release of bioactive agents like nitric oxide and plant-derived compounds.11–14 In this context, negative pressure wound therapy (NPWT), also known as vacuum-assisted closure (VAC), has emerged as a leading advanced therapeutic modality.6 NPWT operates by applying a controlled sub-atmospheric pressure to the wound environment, which is believed to foster healing through multiple mechanisms, including the management of exudate, reduction of tissue edema, enhancement of local perfusion, and stimulation of granulation tissue proliferation.6,15
Reflecting its clinical significance, a substantial number of systematic reviews and meta-analyses have been published to synthesize the evidence on NPWT versus conventional therapy for DFUs.16–23 However, this body of literature is characterized by disparate and often contradictory conclusions, resulting in a state of clinical equipoise.24 This discordance is particularly evident for critical clinical outcomes and arises from key differences between reviews, including variations in study inclusion criteria, the date of literature searches, and the methodological quality of the reviews themselves.24–26 For example, regarding the pivotal issue of amputation, the meta-analysis by Chen et al20 found no statistically significant benefit for NPWT over standard care. This stands in stark contrast to other comprehensive reviews that have reported a significant reduction in amputation risk with NPWT.22 Similarly, the effect of NPWT on ulcer depth reduction remains a point of contention; a meta-analysis by Liu et al17 demonstrated a significant advantage for NPWT, whereas a subsequent analysis by Angulo et al23 reported no significant difference between the two therapies. This fractured evidence landscape creates considerable uncertainty for practitioners aiming to implement evidence-based medicine and impedes the formulation of a definitive, standardized therapeutic protocol.2,3
To resolve this ambiguity, the present study undertakes a formal critical appraisal of these overlapping meta-analyses. Our objective was to systematically deconstruct and harmonize the available evidence, apply the validated Jadad decision algorithm to identify the highest-quality and most dependable meta-analysis, and, consequently, provide a clear, evidence-based clinical recommendation on the role of NPWT in the treatment of diabetic foot ulcers.
Methods
Search Strategy
This cross-sectional analysis was designed in accordance with the methodologies of previously published similar studies,27–30 and structured according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.31 A comprehensive literature retrieval was performed on June 18, 2025, to identify all meta-analyses published up to that date, across the PubMed, Embase, and Cochrane Library databases. Search terms included negative, vacuum, NPWT, VAC, diabetic, foot, DFU, systematic review, and meta-analysis. The search was executed independently by two authors without language restrictions. To ensure comprehensiveness, the reference lists of included articles were manually screened for additional potential meta-analyses. Initial screening involved a review of titles and abstracts, with full-text articles being obtained for closer inspection when necessary. Any disagreements were resolved through discussion, with a third author serving as an arbitrator.
Eligibility Criteria
Inclusion parameters were as follows: (1) the study population consisted exclusively of patients with DFUs; (2) studies compared an intervention group (treated with NPWT or VAC) against a control group (treated with conventional therapy); (3) reported at least one quantifiable clinical outcome, such as healing time, healing rate, adverse events, or amputation rate; (4) the study was a meta-analysis.
Exclusion parameters were: (1) studies that were not meta-analyses (eg, narrative reviews, meeting abstracts, correspondence, or systematic reviews without a pooled analysis); (2) studies involving non-diabetic foot trauma; (3) articles lacking quantifiable outcome measures; (4) retracted articles.
Data Extraction
A standardized data collection form was used by two authors working independently to extract the following information from each eligible meta-analysis: first author, publication year, journal, number of primary studies included, number of randomized clinical trials (RCTs), search strategy details, methodological information (eg, software used, sensitivity analysis), I2 values, and principal meta-analytic results. A third author was consulted to resolve any discrepancies in extracted data.
Quality Assessment
The methodological quality of each included meta-analysis was appraised using two standardized instruments: the Oxford Levels of Evidence32 and the Assessment of Multiple Systematic Reviews (AMSTAR) tool.25 The AMSTAR instrument is a validated 11-item tool recognized for its reliability and validity in evaluating the quality of systematic reviews26 and is widely applied in this context.27–30 Two reviewers independently performed the quality appraisal, with disagreements resolved by consensus discussion or adjudication by a third reviewer.
Application of Jadad Decision Algorithm
The Jadad decision algorithm was utilized to systematically navigate the sources of discordance among the included reviews.24 This algorithm provides a structured framework for comparing meta-analyses based on differences in their clinical question, inclusion criteria, data extraction processes, quality appraisal, and statistical methods. It has been effectively used in prior studies to select the best evidence from a pool of conflicting meta-analyses.27–30 Three authors independently applied the algorithm to reach a consensus on which meta-analysis offered the most reliable evidence.
The application of the algorithm by three independent authors proceeds as follows: First, an assessment is made as to whether the included meta-analyses address the same clinical question (Step A). If they do, the degree of overlap among the primary trials included in each review is evaluated, typically by creating an evidence matrix (Step C). Depending on the degree of trial overlap and the similarity of study quality (Step D), the algorithm guides the user to compare specific aspects such as data extraction and synthesis (Step E) or to select the review with the highest overall quality (Step F). If the included trials are not the same, the algorithm directs an assessment of the selection criteria used by each review (Step G). Based on this assessment, the process may involve a focused comparison of search strategies (Step H) or, if criteria differ, a broader assessment of methodological quality, language restrictions, and the quality of primary trials to identify the most robust review (Step I). A consensus is reached among the authors to determine the final selection.
Results
Literature Search
The study selection process is illustrated in Figure 1. An initial search yielded 414 records. After screening and eligibility assessment, eight meta-analyses were included in this critical appraisal.16–23 Table 1 summarizes the characteristics of these studies, which were published between 2014 and 2025. The included meta-analyses drew upon primary trials published from 2000 to 2021, with each review including between 8 and 14 primary studies (Table 2).33–71
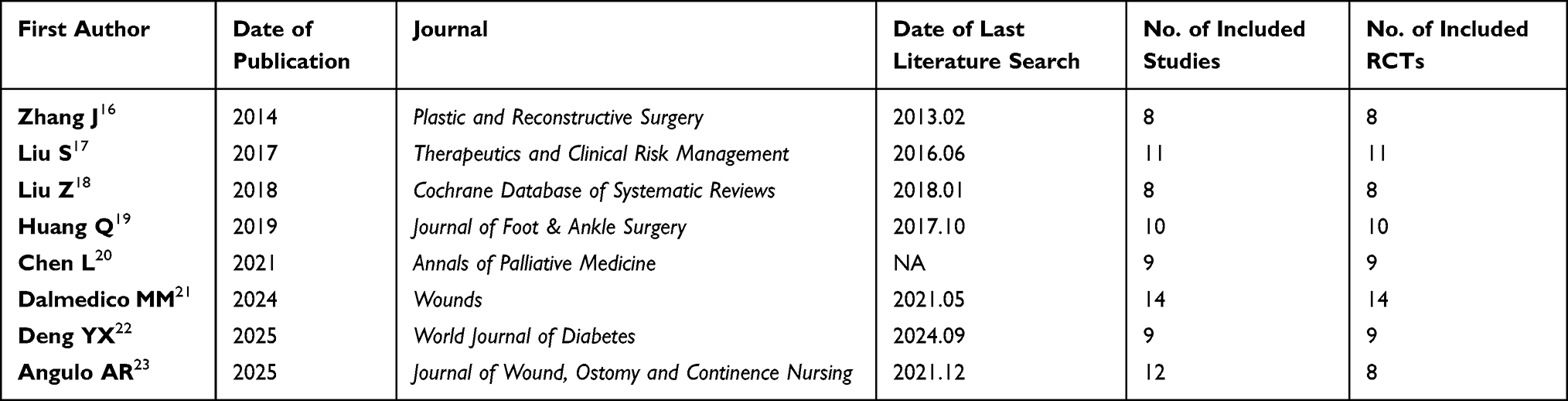 |
Table 1 Summary of Key Attributes of the Included Meta-Analyses |
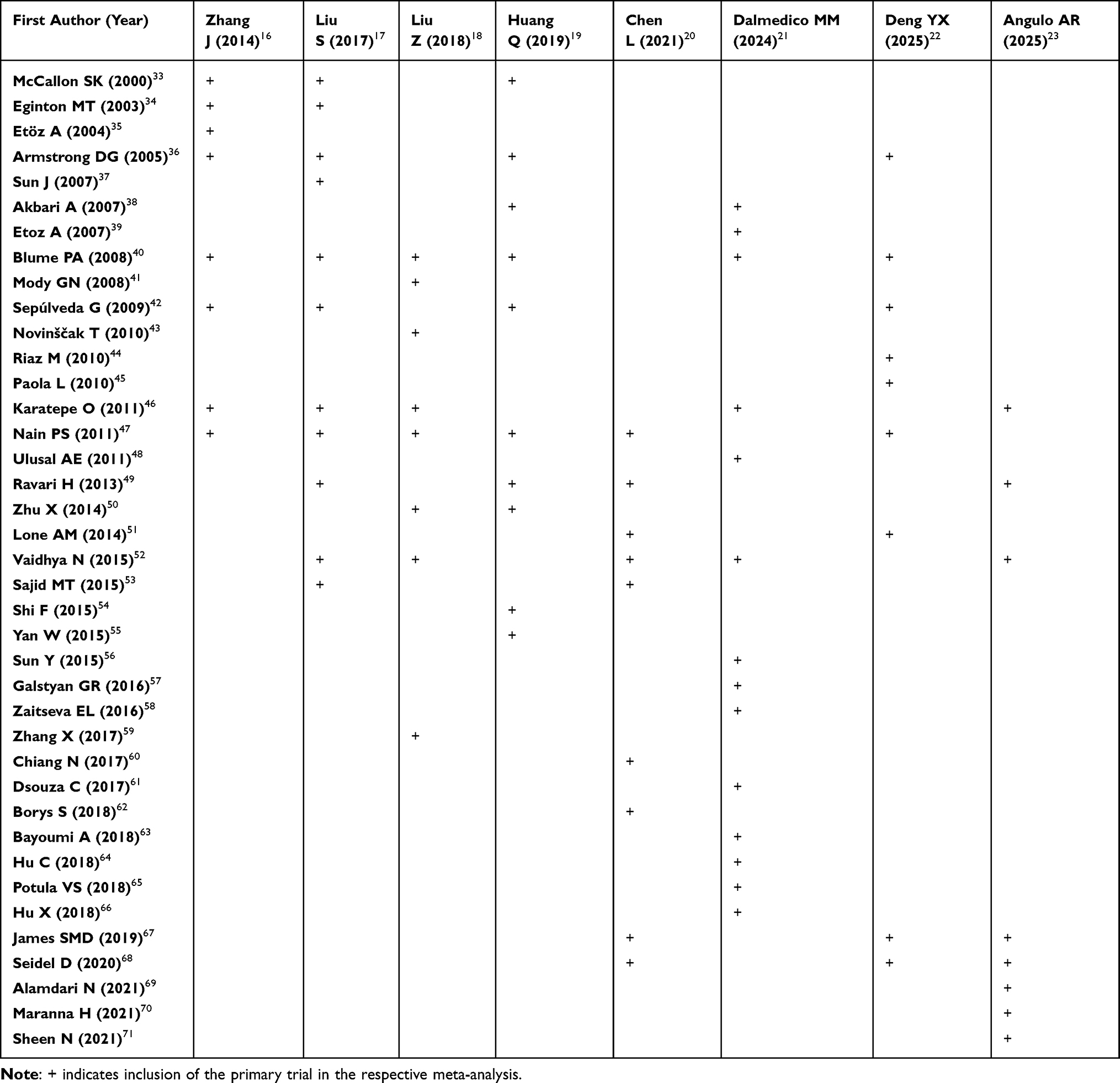 |
Table 2 Primary Trials Included in Each Meta-Analysis |
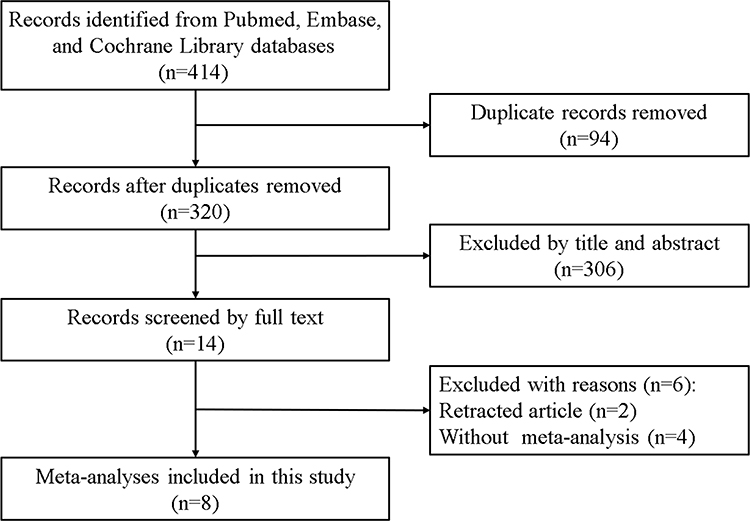 |
Figure 1 Visual summary of the study identification and screening pathway. |
Search Methodology
The search parameters varied across the included reviews. Three meta-analyses restricted their search to English-language publications,16,17,23 three imposed no language restrictions,18,21,22 and the remaining two did not specify their language criteria.19,20 Only two studies reported searching for unpublished literature (ie, no restriction on publication status).18,21 PubMed, Embase, and the Cochrane Library were consistently used across all reviews, while the inclusion of other databases like Web of Science was inconsistent. The search methodology for each study is detailed in Table 3.
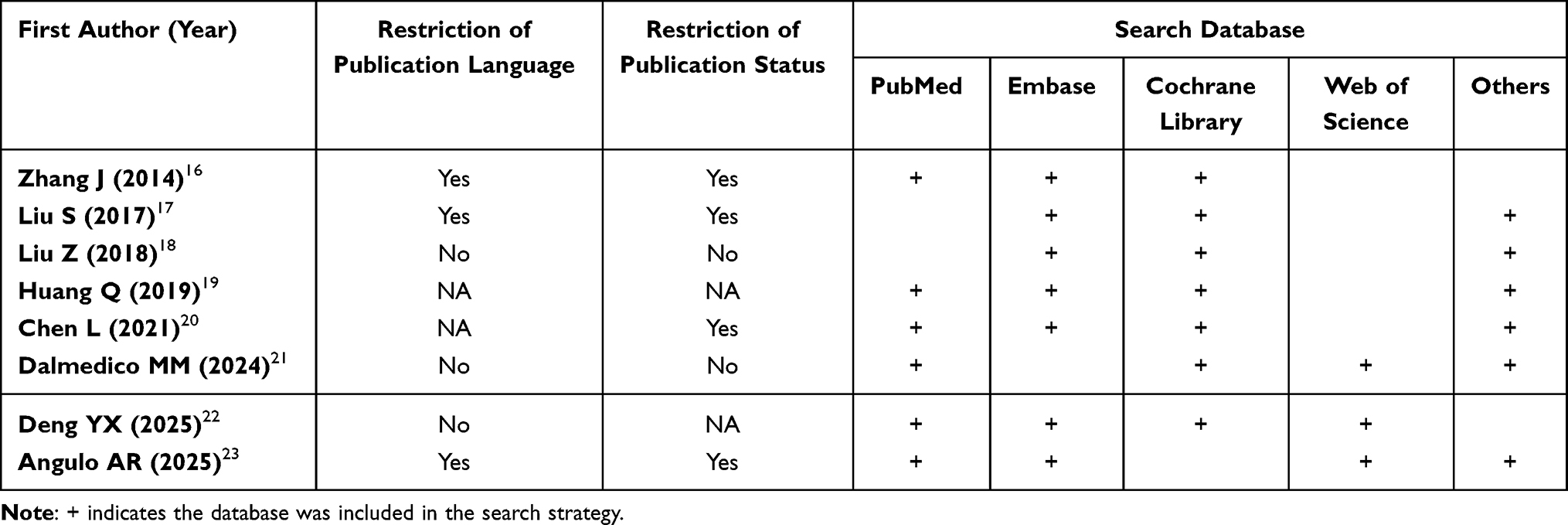 |
Table 3 Summary of Literature Search Strategies Employed by Each Meta-Analysis |
Methodological Quality
According to the Oxford Levels of Evidence, seven meta-analyses were classified as Level II evidence, as they exclusively included RCTs.16–22 One study was deemed Level III evidence due to its inclusion of both RCTs and cohort studies (Table 4).23 The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework was used in two reviews to assess the certainty of evidence.18,21 The most commonly used statistical software was RevMan. AMSTAR scores for the included reviews ranged from 6 to 9, with a median score of 7.5, indicating generally moderate to high methodological quality (Table 5).
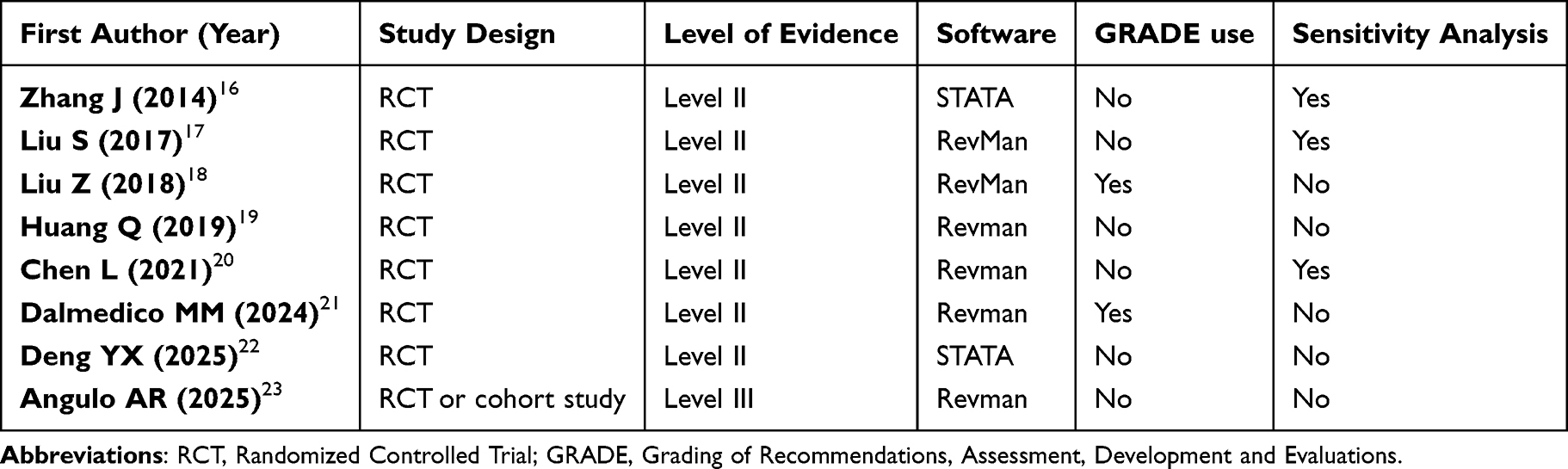 |
Table 4 Key Methodological Details of the Included Meta-Analyses |
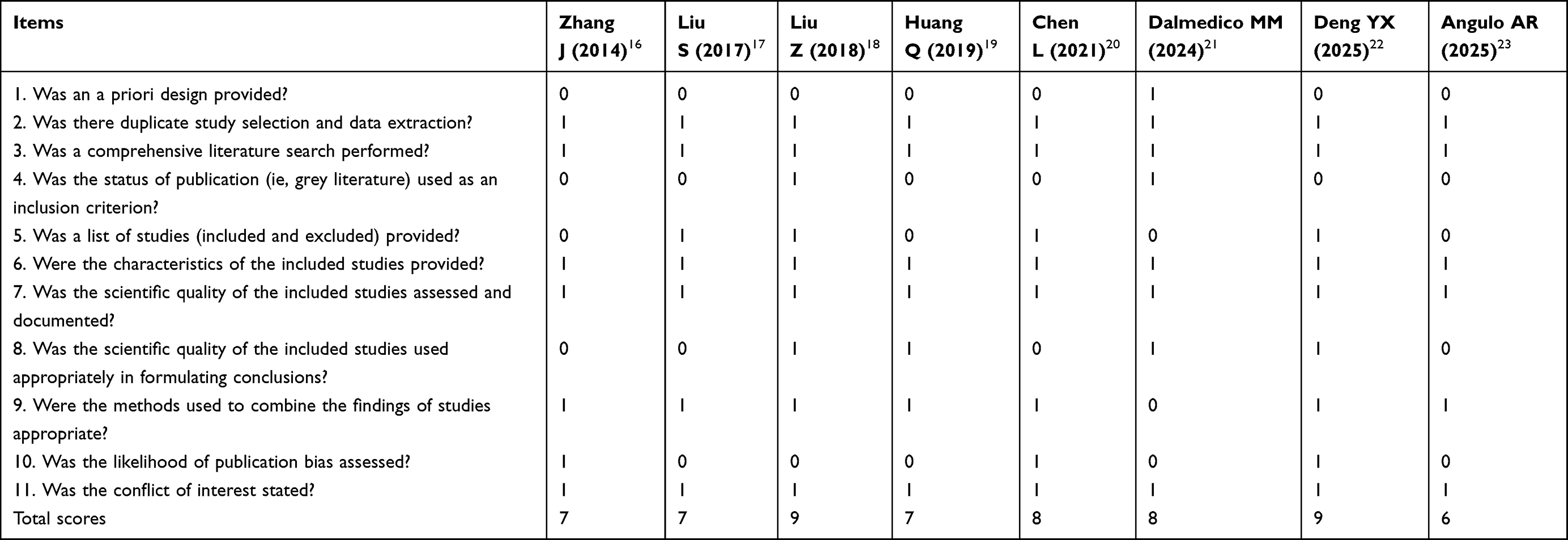 |
Table 5 Results of the AMSTAR Methodological Quality Assessment |
Heterogeneity Assessment
The I2 statistic was used in all included reviews to quantify inter-study heterogeneity for their pooled outcomes (Table 6). Three of the meta-analyses conducted sensitivity analyses to explore the impact of methodological quality on their results (Table 4).16,17,20
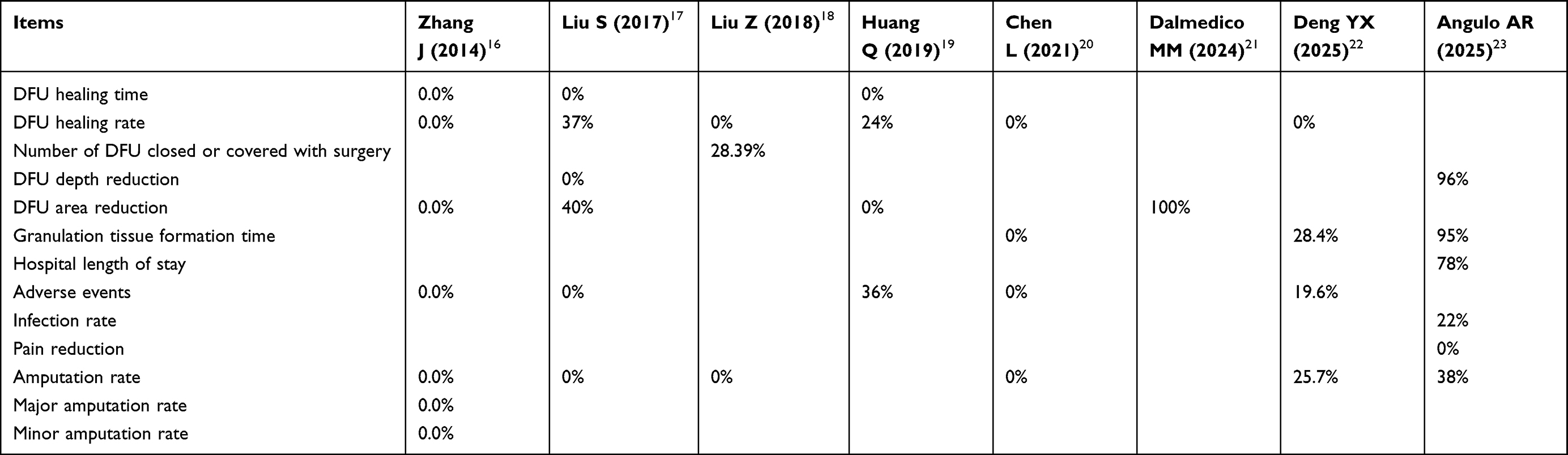 |
Table 6 Reported Statistical Heterogeneity (I2) for Key Outcomes in Each Meta-Analysis |
Results of Jadad Decision Algorithm
The Jadad decision algorithm was applied to determine which of the eight meta-analyses provided the best available evidence.24 The pooled results from all included studies are visualized in Figure 2. The specific application of the algorithm to the eight included meta-analyses proceeded as follows (Figure 3): All studies were determined to address the same clinical question (Step A: Yes). Examination of the primary trial evidence matrix (Table 2) revealed that the studies did not include the same trials (Step C: No). A further assessment of the search strategies and methodological details (Tables 3 and 4) showed that the selection criteria were not the same (Step G: No). This path led to Step I, which mandates the selection of the best evidence based on a comprehensive comparison of methodological quality, search comprehensiveness, and the quality of included primary trials. Based on this final assessment, the 2025 meta-analysis by Deng et al22 was selected (Figure 3). This review demonstrated a statistically significant improvement in wound healing rate (risk ratio = 1.46, 95% confidence interval 1.22–1.76) and a reduction in amputation rate with NPWT (risk ratio = 0.69, 95% confidence interval 0.50–0.96). Additionally, it found that the time to granulation tissue formation was significantly shortened. The incidence of adverse events, however, was not significantly different between NPWT and control groups. Therefore, NPWT is a safe and effective therapy that enhances healing and reduces amputations in patients with DFUs.
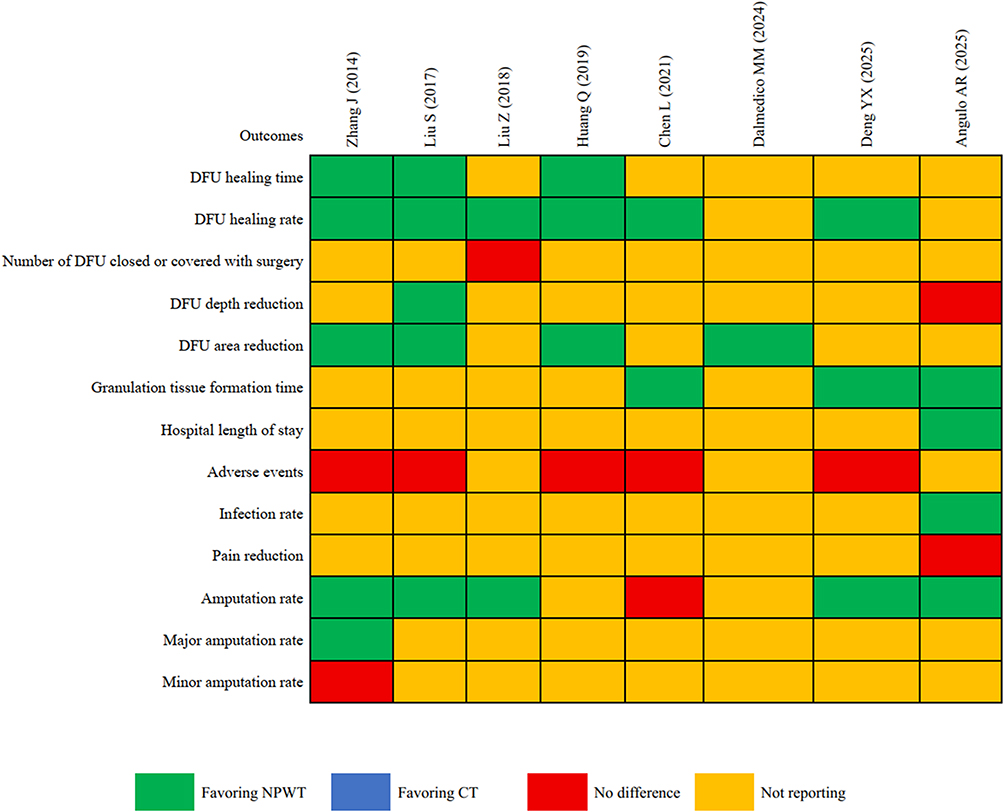 |
Figure 2 Comparative summary of findings from the included meta-analyses. |
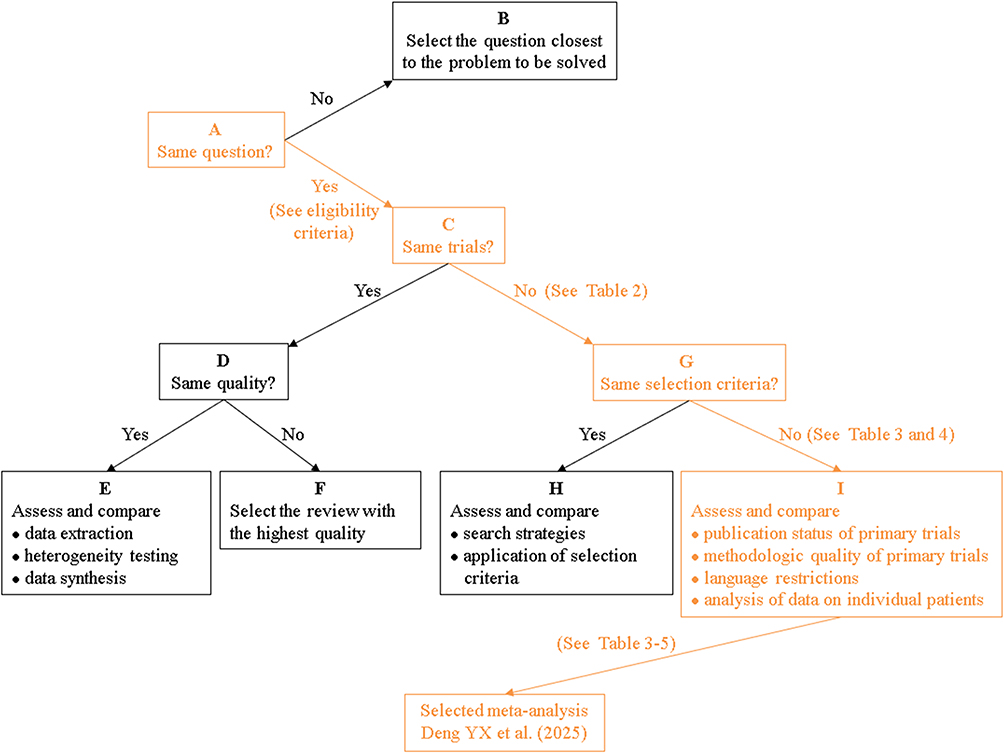 |
Figure 3 Schematic representation of the Jadad decision algorithm application. |
Discussion
This study represents, to our knowledge, the first critical appraisal designed to synthesize and harmonize the overlapping body of meta-analytic evidence on NPWT for DFUs. In a clinical area characterized by multiple, often contradictory, high-level meta-analyses, such an investigation is essential for providing clarity and guiding evidence-based practice.27–30 This methodological approach is particularly valuable in modern evidence-based medicine, where clinicians are often overwhelmed by an ever-increasing volume of publications.24–26 Instead of requiring practitioners to individually appraise multiple complex reviews with varying conclusions, our work provides a single, methodologically vetted directive, thereby enhancing the practical application of evidence at the point of care. Through a comprehensive evaluation of eight meta-analyses and the formal application of the Jadad decision algorithm, our work identifies the 2025 meta-analysis by Deng et al22 as the most methodologically robust and reliable source of evidence currently available. This selection was not an arbitrary choice, but the direct result of a systematic process that evaluated multiple quality-related domains. Specifically, the selection of Deng et al22 was predicated on its superior AMSTAR score, its comprehensive search strategy which did not impose language bias, and its inclusion of a greater number of recent and high-quality RCTs, making it the most up-to-date and methodologically sound synthesis available.
The central conclusion derived from this best-evidence analysis is that NPWT confers substantial clinical benefits over conventional therapy in the management of DFUs.22 The evidence demonstrates that NPWT leads to a significantly higher rate of complete wound closure and a clinically important reduction in the risk of amputation.22 Moreover, NPWT accelerates a critical phase of healing by markedly shortening the time to granulation tissue formation.22 Importantly, these therapeutic gains are not accompanied by an increased risk of adverse events, underscoring a favorable safety profile for the intervention.22 However, the conclusion of a favorable safety profile must be interpreted with some caution. While the best-evidence analysis found no significant increase in overall adverse events, safety reporting across the primary trials included in these meta-analyses is often inconsistent and incomplete.22 Important adverse events like bleeding or periwound maceration may be underreported, a common limitation in wound care trials that should be acknowledged.22
The discordance among the eight included meta-analyses is attributable to several identifiable factors. Chronological differences in publication are a key contributor; earlier reviews, such as those by Zhang et al and Liu et al,16,17 were unable to incorporate the findings of more recent RCTs, which were included in the later, more comprehensive analysis by Deng et al.22 Furthermore, variations in methodological quality, reflected by AMSTAR scores spanning from 6 to 9, likely influenced the results. Meta-analyses with lower scores may have employed less rigorous inclusion criteria or statistical methods, leading to less precise or potentially biased effect estimates.24,25 As our detailed examination in the introduction revealed, these methodological differences manifested as conflicting conclusions on key outcomes like amputation rates and ulcer depth reduction.17,20,22,23
From a clinical standpoint, these findings carry significant weight. The confirmation that NPWT accelerates healing and reduces amputations provides a strong evidence-based rationale for its integration into DFU treatment algorithms.3,22 A more rapid formation of healthy granulation tissue facilitates earlier consideration of definitive wound closure procedures, such as skin grafting, which may in turn reduce the length of hospital stay and lower overall healthcare costs.1,3,6,22 The demonstrated reduction in amputation risk is paramount, as limb preservation is a primary objective of DFU care, with profound implications for patient mobility, quality of life, and survival.2,3,6 The robust safety profile of NPWT should provide clinicians with confidence in its application, assuming appropriate patient selection and monitoring protocols are followed.
While our analysis confirms the efficacy of NPWT as a crucial advanced therapy, it is important to contextualize this finding within the rapidly evolving field of wound care materials science.7,9 Recent advancements in biofabrication, such as the development of electrospun Janus nanofibers, offer novel therapeutic possibilities.7–9,72 As reviewed by Yu et al,72 these multi-functional dressings can be engineered to possess different properties on each side (eg, hydrophobic outer layer for protection and hydrophilic inner layer for exudate management), allowing for a combination of effects such as simultaneous antibacterial action and promotion of cell growth. This goes beyond the primarily mechanical function of NPWT. Therefore, the future of DFU management may involve not just the optimization of existing methods like NPWT, but also the integration or combination of these therapies with such advanced, multi-functional biomaterials to achieve synergistic healing effects.
Furthermore, the future of wound dressing development is increasingly focused on sustainability and “green” approaches, as highlighted in a recent comprehensive review by Verma et al.10 This involves a shift towards utilizing natural biopolymers such as cellulose, chitosan, and alginates, which offer advantages like biocompatibility, biodegradability, and derivation from renewable resources.10 This trend towards “green” biomaterials complements the development of advanced mechanical therapies like NPWT. Future research may therefore explore hybrid systems that combine the proven mechanical benefits of NPWT with bioactive, sustainable biopolymer dressings to optimize healing outcomes in a more environmentally conscious manner.
This study, however, is subject to certain limitations. First, and most fundamentally, while our method’s principal value lies in providing a clear, high-level directive, this comes at the cost of the granular detail found in primary studies. Nuances regarding specific patient subgroups, wound characteristics, or variations in NPWT application protocols are inevitably lost in a cross-sectional analysis of meta-analyses. Second, our approach means our findings are based on aggregate data from previously published studies rather than a de novo analysis of primary trial data, and the validity of our conclusion is therefore contingent upon the quality of the source reviews. If all existing meta-analyses are flawed, our conclusion, though representing the best available evidence, will still inherit those limitations. Third, the potential for publication bias in the primary literature remains a concern, as studies with null or negative findings may be underrepresented, which could skew the results of the meta-analyses we evaluated. Finally, this cross-sectional analysis is inherently retrospective; new primary trials may have been published after the search cutoff dates of the included meta-analyses, representing a potential evidence lag.
Conclusion
In summary, this critical appraisal identified the highest-quality evidence, which demonstrates that NPWT is a safe and effective intervention for DFUs, significantly enhancing wound healing rates, accelerating granulation tissue formation, and reducing the incidence of amputations compared to CT. The primary innovation of this study lies in its methodological approach, which was predicated on the premise that a systematic, quality-based appraisal of overlapping meta-analyses could resolve the clinical uncertainty arising from a landscape of conflicting reports. Our final conclusion, derived from the most robust available evidence, aligns with prior meta-analyses that reported a benefit for NPWT, while providing a methodological explanation for the discordance with those that found no significant effect. By harmonizing these findings, this study provides a clear and compelling rationale for the routine consideration of NPWT as an effective adjunct to standard multidisciplinary care for DFUs. Future research should now focus on direct head-to-head comparisons between NPWT and other advanced wound therapies and evaluate long-term, patient-centered outcomes such as quality of life and treatment burden.
Abbreviations
AMSTAR, Assessment of Multiple Systematic Reviews; CT, Conventional therapy; DFUs, Diabetic foot ulcers; GRADE, Grading of Recommendations, Assessment, Development and Evaluations; NPWT, Negative pressure wound therapy; RCTs, Randomized clinical trials; VAC, Vacuum-assisted closure.
Data Sharing Statement
Data are available on reasonable request to the corresponding author.
Author Contributions
Ying Du and Tiangang Zhai: Data curation, methodology, investigation, validation, formal analysis, writing—original draft; Zhujun Sheng, Weinan Xie, and Zhiwei Jia: Methodology, investigation, visualization, formal analysis, writing—review and editing; Tianlin Wen, Xiyan Zhao, and Xiaolin Tong: Conceptualization, supervision, writing—review and editing. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
National Natural Science Foundation of China (82205089), Beijing Health Promotion Public Welfare Foundation (320.2745.2024102501), National Key R & D Program of China (2022YFC3502100), Fundamental Research Funds for the Central Public Welfare Research Institutes (ZZ13-YQ-030), Scientific and Technological Innovation Project of China Academy of Chinese Medical Sciences (CI2021A01614), Clinical Research Center Construction Project of Guang’anmen Hospital, CACMS (2022LYJSZX13), High Level Chinese Medical Hospital Promotion Project (HLCMHPP2023009), The Escort Project of Guang’anmen Hospital, China Academy of Chinese Medical Science-Backbone Talent Cultivation Project (9323002).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293(2):217–228. doi:10.1001/jama.293.2.217
2. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–2375. doi:10.1056/NEJMra1615439
3. Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic foot ulcers: a review. JAMA. 2023;330(1):62–75. doi:10.1001/jama.2023.10578
4. Ramsey SD, Newton K, Blough D, et al. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care. 1999;22(3):382–387. doi:10.2337/diacare.22.3.382
5. Jeffcoate WJ, Price P, Harding KG; International Working Group on Wound Healing and Treatments for People with Diabetic Foot Ulcers. Wound healing and treatments for people with diabetic foot ulcers. Diabetes Metab Res Rev. 2004;20 Suppl 1(S1):S78–89. doi:10.1002/dmrr.476
6. Huang C, Leavitt T, Bayer LR, Orgill DP. Effect of negative pressure wound therapy on wound healing. Curr Probl Surg. 2014;51(7):301–331. doi:10.1067/j.cpsurg.2014.04.001
7. Dawi J, Tumanyan K, Tomas K, et al. Diabetic foot ulcers: pathophysiology, immune dysregulation, and emerging therapeutic strategies. Biomedicines. 2025;13(5):1076. doi:10.3390/biomedicines13051076
8. Rehman ZU, Khan J, Noordin S. Diabetic foot ulcers: contemporary assessment and management. J Pak Med Assoc. 2023;73(7):1480–1487. doi:10.47391/JPMA.6634
9. Sidhu AS, Harbuzova V. Emerging technologies for the management of diabetic foot ulceration: a review. Front Clin Diabetes Healthc. 2024;5:1440209. doi:10.3389/fcdhc.2024.1440209
10. Verma D, Okhawilai M, Nangan S, et al. A sustainable and green approach towards the utilization of biopolymers for effective wound dressing applications: a detailed review. Nano-Struct Nano-Objects. 2024;37:101086. doi:10.1016/j.nanoso.2023.101086
11. Ahmed R, Augustine R, Chaudhry M, et al. Nitric oxide-releasing biomaterials for promoting wound healing in impaired diabetic wounds: state of the art and recent trends. Biomed Pharmacother. 2022;149:112707. doi:10.1016/j.biopha.2022.112707
12. Augustine R, Hasan A, Patan NK, et al. Cerium oxide nanoparticle incorporated electrospun poly(3-hydroxybutyrate-co-3-hydroxyvalerate) membranes for diabetic wound healing applications. ACS Biomater Sci Eng. 2020;6(1):58–70. doi:10.1021/acsbiomaterials.8b01352
13. Augustine R, Hasan A, Patan NK, et al. Titanium nanorods loaded PCL meshes with enhanced blood vessel formation and cell migration for wound dressing applications. Macromol Biosci. 2019;19(7):e1900058. doi:10.1002/mabi.201900058
14. Augustine R, Rehman SRU, Ahmed R, et al. Electrospun chitosan membranes containing bioactive and therapeutic agents for enhanced wound healing. Int J Biol Macromol. 2020;156:153–170. doi:10.1016/j.ijbiomac.2020.03.207
15. Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W. Vacuum-assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg. 1997;38(6):553–562. doi:10.1097/00000637-199706000-00001
16. Zhang J, Hu ZC, Chen D, Guo D, Zhu JY, Tang B. Effectiveness and safety of negative-pressure wound therapy for diabetic foot ulcers: a meta-analysis. Plast Reconstr Surg. 2014;134(1):141–151. doi:10.1097/PRS.0000000000000275
17. Liu S, He CZ, Cai YT, et al. Evaluation of negative-pressure wound therapy for patients with diabetic foot ulcers: systematic review and meta-analysis. Ther Clin Risk Manag. 2017;13:533–544. doi:10.2147/TCRM.S131193
18. Liu Z, Dumville JC, Hinchliffe RJ, et al. Negative pressure wound therapy for treating foot wounds in people with diabetes mellitus. Cochrane Database Syst Rev. 2018;10(10):CD010318. doi:10.1002/14651858.CD010318.pub3
19. Huang Q, Wang JT, Gu HC, Cao G, Cao JC. Comparison of vacuum sealing drainage and traditional therapy for treatment of diabetic foot ulcers: a meta-analysis. J Foot Ankle Surg. 2019;58(5):954–958. doi:10.1053/j.jfas.2018.12.020
20. Chen L, Zhang S, Da J, et al. A systematic review and meta-analysis of efficacy and safety of negative pressure wound therapy in the treatment of diabetic foot ulcer. Article Ann Palliat Med. 2021;10(10):10830–10839. doi:10.21037/apm-21-2476
21. Dalmedico MM, Do Rocio Fedalto A, Martins WA, de Carvalho CKL, Fernandes BL, Ioshii SO. Effectiveness of negative pressure wound therapy in treating diabetic foot ulcers: a systematic review and meta-analysis of randomized controlled trials. Wounds. 2024;36(8):281–289. doi:10.25270/wnds/23140
22. Deng YX, Wang XC, Xia ZY, Wan MY, Jiang DY. Efficacy and safety of negative pressure wound therapy for the treatment of diabetic foot ulcers: a meta-analysis. Article. World J Diabetes. 2025;16(6):103520. doi:10.4239/wjd.v16.i6.103520
23. Angulo AR, Caballero-Alvarado J, Sarmiento-Falen J, Zavaleta-Corvera C. Comparative assessment of negative pressure wound therapy versus standard treatment in diabetic foot ulcers: a systematic review and meta-analysis. J Wound Ostomy Continence Nurs. 2025;52(3):227–238. doi:10.1097/WON.0000000000001164
24. Jadad AR, Cook DJ, Browman GP. A guide to interpreting discordant systematic reviews. CMAJ. 1997;156(10):1411–1416.
25. Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7(1):10. doi:10.1186/1471-2288-7-10
26. Shea BJ, Hamel C, Wells GA, et al. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J Clin Epidemiol. 2009;62(10):1013–1120. doi:10.1016/j.jclinepi.2008.10.009
27. Yin S, Zhang B, Li T, et al. Platelet-rich plasma in arthroscopic repair of full-thickness rotator cuff tears: a cross-sectional analysis of overlapping meta-analyses. Orthop J Sports Med. 2025;13(5):23259671251337481. doi:10.1177/23259671251337481
28. Azzam AY, Ghozy S, Elswedy A, et al. Carotid endarterectomy versus carotid stenting for asymptomatic carotid stenosis: evaluating the overlapping meta-analyses of randomized controlled trials. Eur J Radiol Open. 2023;10:100460. doi:10.1016/j.ejro.2022.100460
29. Liu D, Wen T, Li X, et al. Percutaneous vertebroplasty versus balloon kyphoplasty in the treatment of osteoporotic vertebral compression fractures: evaluating the overlapping meta-analyses. Pain Physician. 2024;27(4):E383–E394. doi:10.36076/ppj.2024.7.E383
30. Yin S, Zhao X, Li T, et al. Intra-articular platelet-rich plasma versus hyaluronic acid in the treatment of Hip osteoarthritis: a cross-sectional analysis of the overlapping systematic reviews. Ther Clin Risk Manag. 2024;20:919–927. doi:10.2147/TCRM.S487948
31. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
32. Wright JG, Swiontkowski MF, Heckman JD. Introducing levels of evidence to the journal. J Bone Joint Surg Am. 2003;85(1):1–3. doi:10.2106/00004623-200301000-00001
33. McCallon SK, Knight CA, Valiulus JP, Cunningham MW, McCulloch JM, Farinas LP. Vacuum-assisted closure versus saline-moistened gauze in the healing of postoperative diabetic foot wounds. Ostomy Wound Manag. 2000;46(8):28–32,34.
34. Eginton MT, Brown KR, Seabrook GR, Towne JB, Cambria RA. A prospective randomized evaluation of negative-pressure wound dressings for diabetic foot wounds. Ann Vasc Surg. 2003;17(6):645–649. doi:10.1007/s10016-003-0065-3
35. Etöz A, Özgenel Y, Özcan M. The use of negative pressure wound therapy on diabetic foot ulcers:: a preliminary controlled trial. Wounds. 2004;16(8):264–269.
36. Armstrong DG, Lavery LA; Diabetic Foot Study Consortium. Negative pressure wound therapy after partial diabetic foot amputation: a multicentre, randomised controlled trial. Lancet. 2005;366(9498):1704–1710. doi:10.1016/S0140-6736(05)67695-7
37. Sun J, Sun J. Vacuum assisted closure technique for repairing diabetic foot ulcers: analysis of variance by using a randomized and doublestage crossover design. J Clin Rehab Tissue Eng Res. 2007;11(44):8908–8911.
38. Akbari A, Moodi H, Ghiasi F, Sagheb HM, Rashidi H. Effects of vacuum-compression therapy on healing of diabetic foot ulcers: randomized controlled trial. J Rehabil Res Dev. 2007;44(5):631–636. doi:10.1682/jrrd.2007.01.0002
39. Etoz A, Kahveci R. Negative pressure wound therapy on diabetic foot ulcer. Wounds. 2007;19(9):250–254.
40. Blume PA, Walters J, Payne W, Ayala J, Lantis J. Comparison of negative pressure wound therapy using vacuum-assisted closure with advanced moist wound therapy in the treatment of diabetic foot ulcers: a multicenter randomized controlled trial. Diabetes Care. 2008;31(4):631–636. doi:10.2337/dc07-2196
41. Mody GN, Nirmal IA, Duraisamy S, Perakath B. A blinded, prospective, randomized controlled trial of topical negative pressure wound closure in India. Ostomy Wound Manag. 2008;54(12):36–46.
42. Sepúlveda G, Espíndola M, Maureira M, et al. Negative-pressure wound therapy versus standard wound dressing in the treatment of diabetic foot amputation. A randomised controlled trial. Cir Esp. 2009;86(3):171–177. doi:10.1016/j.ciresp.2009.03.020
43. Novinščak T, Zvorc M, Trojko S, Jozinovic E, Filipovic M, Grudic R. Comparison of cost-benefit of the three methods of diabetic ulcer treatment: dry, moist and negative pressure. Acta Medica Croatica. 2010;64(Suppl 1):113–115.
44. Riaz M, Khan M, Akbar A. Comparison of vacuum assisted closure versus normal saline dressing in healing diabetic wounds. Pak J Med Health Sci. 2010;4:308–313.
45. Paola L, Carone A, Ricci S, Russo A, Ceccacci T, Ninkovic S. Use of vacuum assisted closure therapy in the treatment of diabetic foot wounds. J Diabet Foot Complic. 2010;2:3–44.
46. Karatepe O, Eken I, Acet E, et al. Vacuum assisted closure improves the quality of life in patients with diabetic foot. Acta Chir Belg. 2011;111(5):298–302. doi:10.1080/00015458.2011.11680757
47. Nain PS, Uppal SK, Garg R, Bajaj K, Garg S. Role of negative pressure wound therapy in healing of diabetic foot ulcers. J Surg Tech Case Rep. 2011;3(1):17–22. doi:10.4103/2006-8808.78466
48. Ulusal AE, Sahin MS, Ulusal B, Cakmak G, Tuncay C. Negative pressure wound therapy in patients with diabetic foot. Acta Orthop Traumatol Turc. 2011;45(4):254–260. doi:10.3944/AOTT.2011.2283
49. Ravari H, Modaghegh M, Kazemzadeh G, et al. Comparison of vacuum-assisted closure and moist wound dressing in the treatment of diabetic foot ulcers. J Cutan Aesthet Surg. 2013;6(1):17–20. doi:10.4103/0974-2077.110091
50. Zhu X, Chai Y, Ye J, Han P, Wen G, Chen P. Vacuum sealing drainage technique versus traditional repair in treatment of diabetic foot. Chin JTissue Eng Res. 2014;18(34):5548–5554.
51. Lone AM, Zaroo MI, Laway BA, Pala NA, Bashir SA, Rasool A. Vacuum-assisted closure versus conventional dressings in the management of diabetic foot ulcers: a prospective case-control study. Diabet Foot Ankle. 2014;5(1):23345. doi:10.3402/dfa.v5.23345
52. Vaidhya N, Panchal A, Anchalia MM. A new cost-effective method of NPWT in diabetic foot wound. Indian J Surg. 2015;77(Suppl 2):525–529. doi:10.1007/s12262-013-0907-3
53. Sajid MT, Mustafa Q, Shaheen N, Hussain SM, Shukr I, Ahmed M. Comparison of negative pressure wound therapy using vacuum-assisted closure with advanced moist wound therapy in the treatment of diabetic foot ulcers. J Coll Physicians Surg Pak. 2015;25(11):789–793.
54. Shi F, Ren Q, Yu L. Application of vacuum sealing drainage in treatment and nursing of diabetic foot. Chin J Gen Pract. 2015;13:2057–2059.
55. Yan W, Lei L, Jing-Ling W, Yang G, Jia X, Geratology D. Application of vacuum sealing drainage in the treatment for foot ulcer in elderly patients with diabetes mellitus. Practical Geriatr. 2015;3:239–241.
56. Sun Y, Fan W, Yang W, et al. Effects of intermittent irrigation of insulin solution combined with continuous drainage of vacuum sealing drainage in chronic diabetic lower limb ulcers. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015;29(7):812–817.
57. Galstyan GR, Tokmakova AY, Zaitseva EL, Doronina LP, Voronkova IA, Molchkov RV. Comparative evaluation of the intensity of reparative processes in the lower extremity soft tissues of diabetic patients receiving local negative pressure wound treatment and standard wound care. Ter Arkh. 2016;88(10):19–24. doi:10.17116/terarkh2016881019-24
58. Zaitseva EL, Tokmakova AY, Shestakova MV, Galstyan GR, Doronina LP. The study of influence of different methods of local treatment on wound healing in patients with diabetic foot ulcers. Vestn Ross Akad Med Nauk. 2016;71(6):466–471. doi:10.15690/vramn735
59. Zhang X, Wan L, Yang R, et al. Expression of connective tissue growth factor and periostin of wound tissue in patients with diabetes who had vacuum sealing drainage. Int J Clin Exp Med. 2017;10(8):12942–12950.
60. Chiang N, Rodda OA, Sleigh J, Vasudevan T. Effects of topical negative pressure therapy on tissue oxygenation and wound healing in vascular foot wounds. J Vasc Surg. 2017;66(2):564–571. doi:10.1016/j.jvs.2017.02.050
61. Dsouza C, Chirag R, Diaz E, Rao S, Rao S. A randomized controlled trial comparing low cost vacuum assisted dressings and conventional dressing methods in the management of diabetic foot ulcer. Int Surg J. 2017;12(4):3858–3865. doi:10.18203/2349-2902.isj20175142
62. Borys S, Hohendorff J, Koblik T, et al. Negative-pressure wound therapy for management of chronic neuropathic noninfected diabetic foot ulcerations - short-term efficacy and long-term outcomes. Endocrine. 2018;62(3):611–616. doi:10.1007/s12020-018-1707-0
63. Bayoumi A, Al-Sayed A, Al-Mallah A. Negative pressure wound therapy versus conventional dressing in treatment of diabetic foot wound. Egyptian J Hosp Med. 2018;72(3):4054–4059. doi:10.21608/ejhm.2018.9115
64. Hu C, Li D, Pang Z, Li H, Dongye Y, Wu J. Effect of vacuum sealing drainage on expressions of transforming growth factor beta (1) and its receptor in diabetic foot wound. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018;32(8):1061–1065. doi:10.7507/1002-1892.201802024
65. Potula V. Conventional treatment versus vacuum therapy for diabetic foot ulcers treatment. Int Surg J. 2018;5(1):49–53. doi:10.18203/2349-2902.isj20175482
66. Hu X, Lian W, Zhang X, Yang X, Jiang J, Li M. Efficacy of negative pressure wound therapy using vacuum-assisted closure combined with photon therapy for management of diabetic foot ulcers. Ther Clin Risk Manag. 2018;14:2113–2118. doi:10.2147/TCRM.S164161
67. James SMD, Sureshkumar S, Elamurugan TP, Debasis N, Vijayakumar C, Palanivel C. Comparison of vacuum-assisted closure therapy and conventional dressing on wound healing in patients with diabetic foot ulcer: a randomized controlled trial. Niger J Surg. 2019;25(1):14–20. doi:10.4103/njs.NJS_14_18
68. Seidel D, Storck M, Lawall H, et al. Negative pressure wound therapy compared with standard moist wound care on diabetic foot ulcers in real-life clinical practice: results of the German DiaFu-RCT. BMJ Open. 2020;10(3):e026345. doi:10.1136/bmjopen-2018-026345
69. Alamdari N, Mehraneroodi B, Gholizadeh B, Zeinalpour A, Safe P, Besharat S. The efficacy of negative pressure wound therapy compared with conventional dressing in treating infected diabetic foot ulcers: a randomized controlled trial. Int J Diabetes Dev Ctries. 2021;41(4):664–668. doi:10.1007/s13410-021-00941-9
70. Maranna H, Lal P, Mishra A, et al. Negative pressure wound therapy in grade 1 and 2 diabetic foot ulcers: a randomized controlled study. Diabetes Metab Syndr. 2021;15(1):365–371. doi:10.1016/j.dsx.2021.01.014
71. Sheen N, Samar A, Butt M, Ayub Z, Nadeem F. Efficacy of negative pressure wound therapy in early diabetic foot ulcer management compared with advanced moist wound therapy. Pak Armed Forces Med J. 2021;71(6):2087–2090. doi:10.51253/pafmj.v6i6.6231
72. Yu DG, He W, He C, Liu H, Yang H. Versatility of electrospun Janus wound dressings. Nanomedicine. 2025;20(3):271–278. doi:10.1080/17435889.2024.2446139
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Guo Y, Ma Q, Zhou X, Yang J, He K, Shen L, Zhao C, Chen Z, Tan CIC, Chen J
Journal of Pain Research 2022, 15:3509-3521
Published Date: 4 November 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023
Comparison of Balanced Crystalloids versus Normal Saline in Critically Ill Patients: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials
Chen Y, Gao Y
Therapeutics and Clinical Risk Management 2023, 19:783-799
Published Date: 11 October 2023