Back to Journals » Journal of Asthma and Allergy » Volume 19
Effectiveness of Mepolizumab in Severe Uncontrolled Asthma Associated or Not with EGPA Based on the Exacto Scale and Separ-Remas Criteria
Authors Leon Lloreda A ![]() , Muñoz-Sánchez B, Echavarria Kashmiri D, Polonio Gonzalez ML, Maestre Sanchez MV, Ferrrer Galvan M, Romero Falcon A, Medina Gallardo JF, Alvarez-Gutierrez FJ
, Muñoz-Sánchez B, Echavarria Kashmiri D, Polonio Gonzalez ML, Maestre Sanchez MV, Ferrrer Galvan M, Romero Falcon A, Medina Gallardo JF, Alvarez-Gutierrez FJ ![]()
Received 5 October 2025
Accepted for publication 16 January 2026
Published 11 February 2026 Volume 2026:19 565740
DOI https://doi.org/10.2147/JAA.S565740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Antonio Leon Lloreda, Belen Muñoz-Sánchez, David Echavarria Kashmiri, Maria Luisa Polonio Gonzalez, Maria Victoria Maestre Sanchez, Marta Ferrrer Galvan, Auxiliadora Romero Falcon, Juan Francisco Medina Gallardo, Francisco Javier Alvarez-Gutierrez
High-Complexity Asthma Unit. Medical–Surgical Unit of Respiratory Diseases, Virgen Del Rocío University Hospital, Seville, Spain
Correspondence: Antonio Leon Lloreda, High-Complexity Asthma Unit. Medical–Surgical Unit of Respiratory Diseases. Virgen del Rocío University Hospital, Avenue Manuel Siurot, S/N, Seville, 41013, Spain, Email [email protected]
Abstract: Eosinophilic Granulomatosis with Polyangiitis (EGPA) is a rare systemic disorder frequently presenting with severe asthma. Mepolizumab, an interleukin-5 inhibitor, is approved for both severe asthma and relapsing or corticosteroid-dependent EGPA, yet treatment response has traditionally been evaluated using systemic-focused scores, such as BVAS, which may underestimate asthma-specific improvements. We conducted a retrospective study of 142 patients with severe uncontrolled asthma (SUA), including 14 with EGPA, all treated with mepolizumab 100 mg every four weeks. Biologic response was assessed using asthma-focused tools, the EXACTO scale and SEPAR-REMAS criteria, which consider exacerbations, asthma control, lung function, and oral corticosteroid (OCS) use. At baseline, EGPA patients exhibited higher prevalence of nasal polyposis and OCS dependence. After one year of treatment, patients with EGPA showed numerically higher rates of good or complete response and clinical remission compared with patients with severe asthma; however, these differences did not reach statistical significance (70% vs 55.7% and 30% vs 18.5%, respectively; p = 0.03). Regarding oral corticosteroid (OCS) use, a higher proportion of EGPA patients remained on OCS after one year (p < 0.001), and the relative reduction in the number of OCS users from baseline was smaller than in the severe asthma group but without statistically significant (p = 0.55). Mean daily OCS dose increased in EGPA (9.8 to 15.3 mg) but decreased in non-EGPA patients (18.4 to 10.3 mg). These findings suggest that patients with SUA and EGPA can achieve asthma-specific improvements with 100 mg mepolizumab, highlighting the value of asthma-focused assessment tools and the need for larger multicenter studies to optimize treatment strategies.
Keywords: asthma control, type 2 inflammation, vasculitis spectrum, biologic therapy, precision medicine
Introduction
Eosinophilic Granulomatosis with Polyangiitis (EGPA) is a systemic disorder characterized by eosinophilic granulomatous inflammation, clinically manifesting as severe asthma often accompanied by eosinophilia, nasal polyposis, or allergic rinitis.1 Systemic corticosteroids remain the mainstay of treatment; however, chronic relapsing disease can result in irreversible organ damage due to both disease activity and glucocorticoid toxicity. Mepolizumab, an interleukin-5 inhibitor, is approved for type 2 high severe asthma at 100 mg every four weeks and for relapsing or corticosteroid-dependent EGPA at 300 mg every four weeks.2,3
Assessment of treatment response in EGPA has traditionally relied on the Birmingham Vasculitis Activity Score (BVAS),4 which primarily evaluates systemic manifestations rather than asthma control. In contrast, the Exacto scale (from the 2022 Severe Asthma Consensus)5 and SEPAR-REMAS criteria (from the 2024 SEPAR-REMAS Consensus)6 provide validated metrics for biologic therapy response in severe uncontrolled asthma (SUA). This study aimed to compare baseline clinical and functional characteristics between SUA patients with and without EGPA and evaluate the effectiveness of mepolizumab using the Exacto scale and SEPAR-REMAS criteria.
Materials and Methods
We conducted a retrospective observational cohort study of patients with SUA, defined according to the Spanish Asthma Management Guidelines:7 persistent poor symptom control, frequent or severe exacerbations, and airflow limitation despite high-intensity therapy. Patients were followed at the Severe Asthma Unit of our hospital from January 2017 to December 2024. Patients with EGPA were diagnosed according to European College of Rheumatology criteria:8 primarily exhibiting asthma, nasal polyposis, and blood eosinophilia >500/µL, with limited systemic involvement (five with mononeuritis multiplex, three with dermatologic manifestations). Given the rarity of EGPA, all available patients were included, resulting in a fixed sample size determined by case availability rather than by a priori calculation. Baseline demographic, clinical, functional, and biomarker data were collected. Historical eosinophilia reflected the highest recorded value, and baseline eosinophils were pre-mepolizumab. All patients received mepolizumab 100 mg every four weeks, with adherence monitored by nursing staff and no patients discontinued treatment during follow-up.
Biologic response was assessed during the first treatment year in each patient using the EXACTO scale for good or complete response and the SEPAR-REMAS criteria for clinical remission. EXACTO quantifies exacerbations, ACT score, FEV1 variability and adds points for continuous OCS, while SEPAR-REMAS defines remission as no exacerbations or rescue medication, no OCS, well-controlled asthma (ACT ≥20), and normal or near-normal lung function (with negative broncodilatador test) over 12 months. OCS use was defined as daily or alternate-day administration for ≥3 months (≥5 mg/day prednisone) to maintain disease control. Both the proportion of patients on OCS and the mean dose before and after treatment were analyzed. Statistical analyses included parametric and non-parametric tests, chi-square and Fisher exact tests for categorical variables, and effect size calculations where relevant.
Results
We analyzed 142 patients with SUA (mean age 54 ± 17 years; 59.9% female), including 14 patients (9.9%) with EGPA and 128 without EGPA. At baseline, no significant differences were observed between groups with respect to sex, smoking status, or comorbidities such as allergic rhinitis, COPD, bronchiectasis, atopy, anxiety/depression, immunodeficiency, obstructive sleep apnea, or obesity; however, patients with EGPA showed a significantly higher prevalence of nasal polyposis (64.2% vs 29.6%, p<0.01) and more frequent use of OCS (71.43% vs 29.85%, p<0.02). As shown in Table 1, EGPA patients also exhibited higher significant historical eosinophil counts, fewer severe exacerbations and lower baseline daily OCS doses.
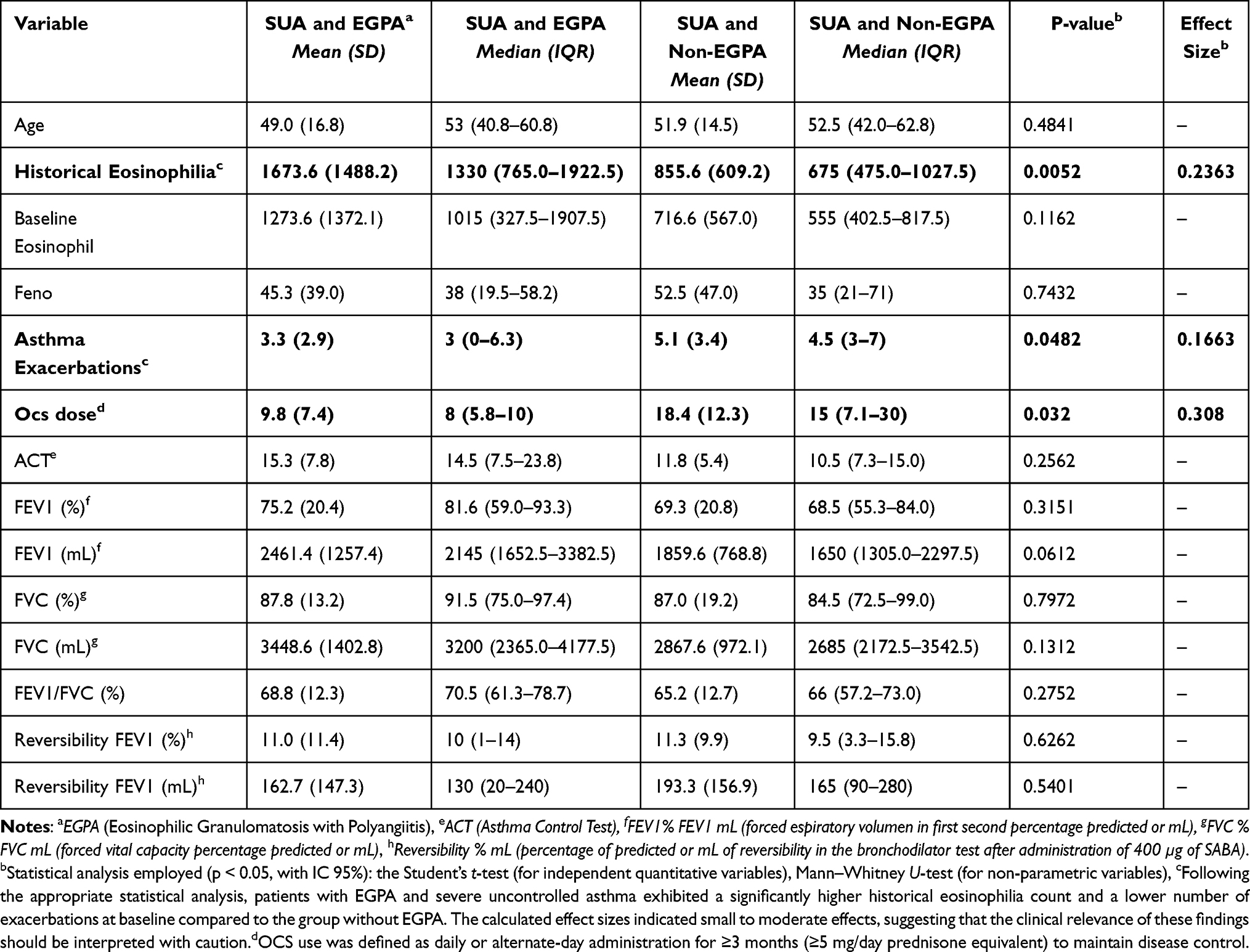 |
Table 1 Comparison Analysis of Clinical, Functional and Inflammatory Parameters at Baseline Visit in the Group of Patients with Severe Uncontrolled Asthma with Our without EGPA |
After one year of treatment (Figure 1), rates of good or complete response and clinical remission were higher in patients with EGPA than in patients without EGPA, although the differences were not statistically significant (p = 0.30). The proportion of patients receiving oral corticosteroids (OCS) was significantly higher in the EGPA group compared with the non-EGPA group (p < 0.001). Compared with baseline, the reduction in the proportion of patients using OCS was smaller in the EGPA group, with no statistically significant difference between groups (p = 0.55). Mean daily OCS dose increased in EGPA patients from 9.8 (7.4) to 15.3 (11) mg, whereas it decreased in non-EGPA patients from 18.4 (12.3) to 10.3 (12.8) mg.
 |
Figure 1 Evaluation of treatment effectiveness during the first year of mepolizumab in patients with severe uncontrolled asthma (SUA) with or without EGPA a, b. a Statistical analysis employed (p < 0.05, with IC 95%): the chi-square test.b After one year of treatment (Figure 1), rates of good or complete response and clinical remission were higher in patients with EGPA than in patients without EGPA, although the differences were not statistically significant (p = 0.30). The proportion of patients receiving OCS was significantly higher in the EGPA group compared with the non-EGPA group (p < 0.001). Compared with baseline, the reduction in the proportion of patients using OCS was smaller in the EGPA group, with no statistically significant difference between groups (p = 0.55). |
Discussion
In our cohort, patients with EGPA showed higher rates of good or complete response and clinical remission—according to the EXACTO scale and SEPAR-REMAS criteria—although these differences were not statistically significant. In addition, EGPA patients exhibited a smaller reduction in oral corticosteroid (OCS) use compared with non-EGPA patients, along with an increase in mean daily OCS dose. These findings align with other studies evaluating biologic response in EGPA, although the response definitions differ. Portacci et al defined response based on improvements in ACT (>6 points), FEV1 (>500 mL), absence of exacerbations and OCS use, categorizing 78.1% of patients as “super-responders” if at least two criteria were met.9
Two complementary hypotheses may explain these observations. First, the pathophysiology of EGPA—marked by higher eosinophilic inflammation, nasal polyposis prevalence, and OCS dependence—may confer enhanced sensitivity to IL-5 blockade. Second, EGPA is a systemic disease that is usually diagnosed by internal medicine specialists and subsequently managed through a shared care model involving both internal medicine and pulmonology. Because internal medicine teams often retain primary responsibility for systemic disease control, they may be more likely to maintain or escalate OCS doses to prevent systemic relapse, particularly in patients with long-term OCS exposure. This multidisciplinary management approach may help explain why, despite relative reductions, patients with EGPA remained more OCS-dependent overall.
An additional strength of our study is that clinically meaningful improvements were achieved despite the use of a lower mepolizumab dose (100 mg), which the formulation was initially prescribed for the treatment of SUA in our cohort. Although dose escalation to 300 mg is possible when clinically indicated, but it was not required in our patients. This finding is consistent with previous studies in which the 300 mg dose was frequently used without demonstrating significant differences in efficacy compared with the 100 mg dose.2,3
Additionally, using the EXACTO and SEPAR-REMAS criteria allowed a more precise assessment of biologic response in asthma than systemic EGPA-focused scores such as BVAS, which is particularly appropriate given the limited systemic involvement in our cohort. Finally, the main limitation of our study, and likely the reason why the results did not reach statistical significance regarding biologic response, is the small sample size of the EGPA group, as this is a rare disease (14 patients out of 142 in total). Future studies with larger multicenter cohorts are warranted to confirm these findings and optimize dosing strategies.
Conclusion
In our cohort, patients with SUA and EGPA treated with mepolizumab 100 mg showed higher biologic response rates than patients with SUA alone, although these differences were not statistically significant. These findings suggest that asthma-focused assessment tools, such as the EXACTO scale and SEPAR-REMAS criteria, may be useful for evaluating treatment response in EGPA patients with predominantly asthmatic manifestations and limited systemic involvement.
Abbreviations
EGPA, Eosinophilic Granulomatosis with Polyangiitis; SUA, severe uncontrolled asthma; BVAS, Birmingham Vasculitis Activity Score; OCS, oral corticosteroid; SEPAR, Spanish Society of Pulmonology and Thoracic Surgery.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article and in its tables and figures.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki and was reviewed and approved by the Ethics Committee of the Virgen Macarena Hospital on May 28, 2025 under the sponsor code EREMAG 2025. Regarding the informed consent form and patient information sheet, the committee granted a waiver, as the study was conducted exclusively using pseudonymized clinical data. Appropriate measures were implemented to ensure full compliance with the applicable data protection regulations, guaranteeing that no contact could be established with the individuals involved and that their identities could not be disclosed.
Acknowledgments
Dr. Álvarez Gutiérrez, for his interest and support shown in the development of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Francisco Javier Álvarez-Gutiérrez (FAG) has received consulting fees from AstraZeneca, GSK, and Sanofi/Regeneron; has received speaker honoraria and manuscript support from AstraZeneca, GSK, Bial, Sanofi, Orion Pharma; and has received travel support from AstraZeneca, Chiesi, GSK, and Sanofi/Regeneron. Juan Francisco Medina Gallardo (JFMG), Marta Ferrrer Galván (MFD) and Auxiliadora Romero Falcón (ARF) have, in the last three years, received honoraria for speaking at sponsored meetings from AstraZeneca, GSK, Menarini, and Sanofi; and have received travel support from Gebro, Sanofi, and Chiesi. The remaining authors declare that they have no conflicts of interest that may be considered to directly or indirectly influence the content of the manuscript. This paper has been uploaded to Elsevier as a preprint: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5341950.
Finally, this manuscript was presented at the ERS Congress in September 2025. It has been published in the ERS Journal: “Comparative study of clinical functional characteristics and treatment effectiveness between patients with severe uncontrolled asthma and EGPA.” Leon Lloreda, A. et al. European Respiratory Journal. 2025; 66(69): PA5669.
References
1. Koike H, Ryoji N, Yagi S, Furukawa S, MIMK YF. A review of anti-il-5 therapies for eosinophilic granulomatosis with polyangiitis. Adv Ther. 2022;40(1):25–6. doi:10.1007/s12325-022-02307-x
2. Wechsler ME, Akuthota P, Jayne D, et al. Mepolizumab or placebo for eosinophilic granulomatosis with polyangiitis. N Engl J Med. 2017;376(20):1921–1932. doi:10.1056/NEJMoa1702079
3. Bettiol A, Urban ML, Dagna L, et al. Mepolizumab for eosinophilic granulomatosis with polyangiitis: a european multicenter observational study. Arthritis Rheumatol. 2022;74(2):295–306. doi:10.1002/art.41943
4. Mukhtyar C, Lee R, Brown D, et al. Modification and validation of the Birmingham vasculitis activity score (version 3). Ann Rheum Dis. 2009;68(12):1827–1832. doi:10.1136/ard.2008.101279
5. Alvarez-Gutiérrez FJ, Blanco-Aparicio M, Casas-Maldonado F, et al. Consensus document for severe asthma in adults. 2022 update. Open Respir Arch. 2022;4(3):100192
6. Álvarez-Gutiérrez FJ, Casas-Maldonado F, Soto-Campos G, et al. Spanish consensus on remission in asthma (REMAS). Arch Bronconeumol. 2024;60(8):503–509. doi:10.1016/j.arbres.2024.04.002
7. Plaza Moral V, Alobid I, Rodríguez C Á, et al. GEMA 5.3. Spanish guideline on the management of asthma. Open Respir Arch. 2023;5(4). doi:10.1016/j.opresp.2023.100277.
8. Grayson PC, Ponte C, Suppiah R, et al. American college of rheumatology/European alliance of associations for rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis. 2022;81(3):309–314. doi:10.1136/annrheumdis-2021-221794
9. Portacci A, Campisi R, Buonamico E, Pelaia C, Crimi N. et al; Real-world characteristics of “super-responders” to mepolizumab and benralizumab in severe eosinophilic asthma and eosinophilic granulomatosis with polyangiitis. ERJ Open Res. 2023;9(5):00419–2023. doi:10.1183/23120541.00419-2023
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023
Kimura Disease: Retrospective Analysis of 53 Cases and Three Mepolizumab-Responsive Cases
Zhu W, Zhang L, Zhang J, Wang W, Xiang Y, He D, Shi J, Liang Y, Shi Y, Ning X, Jin M, Ye L
Journal of Inflammation Research 2025, 18:13773-13785
Published Date: 4 October 2025
Pulmonary Rehabilitation Reduces Airway Inflammation in Asthma Patients with High FeNO Levels
Gloeckl R, Kroll D, Abdulleyev G, Schneeberger T, Jarosch I, Nell C, Koczulla AR
Journal of Asthma and Allergy 2025, 18:1651-1660
Published Date: 22 November 2025
Systemic Immune Dysregulation in Allergic Rhinitis: Mechanisms, Comorbidities, and Implications for Targeted Therapy
Hui D, Shi C, Fan Y, Han M, Wang Y, Sun J, Xue Y, Li E
Journal of Asthma and Allergy 2026, 19:589195
Published Date: 9 March 2026
The Immune Architecture of Eosinophilic Esophagitis: Mechanisms, Therapeutic Targets, and Precision Management
Bertin L, Caldart F, Barchi A, Seregni N, Pasta A, Calabrese F, Marabotto E, Mari A, Farah A, Sirinic E, Sorge A, Ghisa M, Chahuán J, Savarino V, Savarino EV
ImmunoTargets and Therapy 2026, 15:510865
Published Date: 27 May 2026