Back to Journals » Journal of Inflammation Research » Volume 18
Kimura Disease: Retrospective Analysis of 53 Cases and Three Mepolizumab-Responsive Cases
Authors Zhu W, Zhang L, Zhang J, Wang W, Xiang Y, He D, Shi J, Liang Y, Shi Y, Ning X, Jin M, Ye L ![]()
Received 7 May 2025
Accepted for publication 26 September 2025
Published 4 October 2025 Volume 2025:18 Pages 13773—13785
DOI https://doi.org/10.2147/JIR.S538560
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Wenjiao Zhu,1,* Lei Zhang,2,* Jing Zhang,3,* Wei Wang,4 Ye Xiang,1 Dingxian He,5 Jing Shi,1 Yiran Liang,1 Yuanping Shi,6 Xianhui Ning,7 Meiling Jin,1 Ling Ye1
1Department of Allergy, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China; 2Department of Pathology, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China; 3Department of Pathology, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200011, People’s Republic of China; 4Department of Neurosurgery, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200011, People’s Republic of China; 5Department of Neurology, Huashan Hospital, Fudan University, Shanghai, 200040, People’s Republic of China; 6Department of Endocrinology and Metabolism, Peking University People’s Hospital, Beijing, 100044, People’s Republic of China; 7Department of Otolaryngology, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Meiling Jin, Email [email protected] Ling Ye, Email [email protected]
Background: Kimura disease (KD) is a rare, chronic lymphoproliferative disorder, which is believed to be driven by a Th2 immune response, though its exact pathogenesis remains unclear. Despite various treatment approaches, no standardized therapy has been established. This study investigated the clinical features of 53 KD patients and evaluated the therapeutic potential of mepolizumab in three cases.
Methods: A retrospective age-stratified analysis was performed on 53 patients diagnosed with KD at two tertiary medical centers in China, covering the period from January 2014 to December 2024. We also provided an in-depth case series of three patients who received mepolizumab treatment.
Results: This study included 53 KD patients, predominantly male (88.7%) with a mean age of 41 years. The median time from symptom onset to diagnosis was 24 months, and the median lesion diameter was 3.0 cm. Pruritus was present in 52.8% of patients, with frequency increasing with age (P=0.015). Coexisting conditions included IgG4-related disease (11.3%), asthma (9.4%), and thrombotic events (9.4%). Lesions were bilateral in 66.0% and primarily located in the head and neck region (83.0%). Average eosinophil count was 2.09 × 109/L, and mean serum IgE level was 1069 IU/mL. Surgical excision (62.3%) is the most common initial treatment approach, followed by corticosteroids (15.1%). The overall recurrence rate is 60.4%. In the case series, three patients treated with different doses of mepolizumab showed favorable responses, including lymph nodes shrink, symptom control and eosinophil reduction.
Conclusion: This study provided a comprehensive summary and age-stratified analysis of the clinical characteristics of KD, providing valuable insights into its pathophysiology and potential overlapping mechanisms. Additionally, the study presents clinical cases of three patients treated with mepolizumab, highlighting its potential as a promising therapeutic option for the management of KD.
Keywords: Kimura disease, eosinophilia, type 2 inflammation, mepolizumab
Introduction
Kimura disease (KD) is a rare chronic lymphoproliferative disorder of unidentified cause, predominantly seen in Asian males aged 20 to 40 years.1 Clinically, KD is characterized by painless subcutaneous soft tissue masses or lymphadenopathy, typically localized to the head and neck region. It is often associated with peripheral eosinophilia and elevated serum immunoglobulin E (IgE) levels. Histopathological examination remains the gold standard for diagnosis, revealing follicular hyperplasia, prominent eosinophilic infiltration in both the interfollicular regions and germinal centers, and occasionally eosinophilic microabscesses. The clinical heterogeneity and rarity of KD contribute to diagnostic challenges and limited recognition.
The exact etiology of KD remains unclear; however, it is hypothesized that T helper (Th) 2 cells and their associated cytokines, including interleukin (IL)-4, IL-5, and IL-13, play a crucial role in the pathogenesis of the disease.2 IL-4 drives the immunoglobulin class switching to IgE, and, in conjunction with IL-13, enhances the production of chemotactic factors, thereby increasing eosinophil chemotaxis to tissues. IL-5 is a critical biological mediator responsible for the differentiation, growth, activation, survival, and recruitment of eosinophil. The elevated Th2 response and cytokine-driven immune response in KD may explain the characteristic tissue and peripheral eosinophilia, as well as the increased serum IgE levels observed in these patients. IgE-mediated mast cell recruitment and activation further contribute to common symptoms, including skin rashes and pruritus.
Despite various treatment modalities, such as surgical resection, corticosteroids, radiotherapy, and immunosuppressive agents, there is no consensus on the optimal therapeutic approach. The long-term prognosis remains suboptimal, with an overall reported recurrence rate as high as 60%.2 In recent years, four biologic therapies have been reported in case reports/series for the treatment of KD with promising clinical efficacy KD.3–5 These biologics all block type 2 inflammatory pathways, either by targeting IgE (omalizumab), the IL-5 pathway (mepolizumab, benralizumab), or the IL-4/13 pathway (dupilumab). Omalizumab, which binds to free IgE and prevents its interaction with the FceRI receptor on basophils and mast cells, inhibits the release of inflammatory mediators such as histamine and leukotrienes, thereby suppressing IgE-mediated allergic reactions. Dupilumab, by targeting the interleukin-4 receptor alpha (IL-4Rα), inhibits the signaling of both IL-4 and IL-13, which are key contributors to eosinophilic inflammation and IgE overproduction. Mepolizumab, a humanized IgG1-κ monoclonal antibody, binds to IL-5, preventing its interaction with the IL-5 receptor and inhibiting the crucial role of IL-5 in eosinophilopoiesis, activation and degranulation. Targeted therapies against Th2-mediated inflammation have the potential to be more effective than traditional treatments. However, due to the rarity of KD and the delayed availability of biologic agents, the evidence for these therapies is primarily derived from case reports, resulting in a lack of consensus regarding their use in clinical practice.
In this study, we performed a retrospective age-stratified analysis of 53 KD patients from two medical centers in China, with a particular focus on three patients who were treated with mepolizumab. The objective of this study is to characterize the disease features of KD in a larger cohort and to explore the potential of mepolizumab as a therapeutic option for this rare and challenging disorder.
Methods
Study Design and Participants
We conducted a retrospective review of medical records for 53 patients with histopathologically confirmed KD, initially diagnosed at Zhongshan Hospital, Fudan University, or Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, between January 2014 and December 2024.
Data Collection and Outcomes
Patient data for these 53 consecutive cases were retrieved from the electronic medical record systems, including demographics, clinical features, comorbidities, laboratory parameters, imaging findings, histopathology, treatment modalities and outcomes. All patients met the pathological criteria for KD, which includes prominent eosinophilia or eosinophilic microabscesses, florid follicular hyperplasia, and proliferation of small blood vessels with postcapillary venule expansion. Additionally, the diagnosis of IgG4-related disease (IgG4-RD) was made based on the criteria established in 2012.6 Fulfilment of two major histopathological features with tissue IgG4/IgG+ plasma cells (PC) ratio >40% and IgG4+PC >50/high-power field (HPF) or fulfilment of one major histopathological feature with tissue IgG4/IgG+ PC ratio >90% and IgG4+PC >200/HPF are required for diagnosis.
Following the approval of mepolizumab in China, three consecutive cases of KD were recommended for treatment with mepolizumab 300 mg every four weeks subcutaneously, after obtaining informed consent. However, due to economic constraints, Cases 1 and Cases 2 were administered 100 mg and 200 mg of mepolizumab, respectively. The specific duration of follow-up and evaluation was individualized according to each patient’s treatment and monitoring schedule. Asthma control was assessed using the Five-Item Asthma Control Questionnaire (ACQ-5).7 Skin pruritus severity was evaluated using the Visual Analog Scale (VAS). Furthermore, pulmonary function parameters, including forced expiratory volume in one second (FEV1, as a percentage of predicted values), and fractional exhaled nitric oxide (FeNO) levels were recorded.
Statistical Analysis
Variables with a normal distribution are represented by the mean± standard deviation (SD), whereas nonparametric data are shown as the median (interquartile range [IQR]). The reporting of categorical variables is done using absolute numbers and percentages. To compare groups, ANOVA, Kruskal–Wallis test, or Fisher’s exact test were employed. A P-value below 0.05 was considered statistically significant. SPSS version 21 (IBM Corp., Armonk, N.Y., USA) was used for all analyses.
Results
Clinical Characteristics of 53 Patients
Table 1 summarizes the characteristics of patients with a clinical diagnosis of KD by the age group. Among the 53 patients, 47 (88.7%) patients were male, with a mean age at diagnosis of 41 years. The median interval from initial symptom onset to KD diagnosis was 24 months (IQR: 9–68 months), and the median maximal lesion diameter was 3.0 cm (IQR: 2.2–4.6 cm). The symptom of pruritus was noted in 52.8% of the patients, and the frequency of pruritus increased with age (overall, 52.8%; <20; 0.0%; 20–39 years, 52.6%; >40 years, 64.3%; P=0.015). Additional symptoms or complications included coexisting IgG4-RD in 6 patients (11.3%) based on pathological findings (Supplementary Figure 1), asthma in 9.4%, and thrombotic events in 9.4%. Lesions were bilateral in 66.0% and multiple in 79.2% of cases. The head and neck regions were most common locations (83.0%). The average blood eosinophil count (BEC) was 2.09 ×109/L, accounting for 22.3% of total leukocytes. The mean serum IgE level was 1069 IU/mL (range: 220–3508 IU/mL). In all age groups, the initial treatment was most often surgical excision (62.3%) followed by corticosteroids treatment (15.1%). The overall recurrence rate after initial treatment was 60.4%. No significant differences were observed across different age groups regarding gender, diagnostic delay, lesion size or distribution, laboratory parameters, initial treatment or recurrence.
 |
Table 1 Clinical Characteristics of Kimura Disease by Age Group |
Case Series
Case 1
A 45-year-old non-smoking male presented with a 15-year history of recurring submandibular lumps and elevated eosinophil levels. Surgical excision of a left submandibular lymph node was performed in 2010, but recurrence was noted six months later (Figure 1A). His BEC peaked at 2.42 ×109/L, accounting for 21.4% of total white blood cells. He had a long-term history of atopic dermatitis (AD) and allergic rhinitis. Histopathology initially revealed chronic reactive lymphadenitis, and no further treatment was administered. Over the following years, multiple diagnostic procedures were performed. A skin biopsy in 2017 for generalized pruritus (VAS: 10) revealed perivascular lymphocytic infiltration with scattered eosinophils. In 2018, fine-needle aspiration (FNA) of a right inguinal lymph node showed reactive hyperplasia. In 2022, a core needle biopsy of a left cervical lymph node identified a lymphoproliferative lesion with notable eosinophilic infiltration. Bone marrow biopsy in 2023 showed eosinophils accounting for 17% of peripheral leukocytes and 5% of bone marrow cells. Immunophenotyping and karyotype analysis was normal. Serologic tests for parasites, autoimmune markers, and infectious agents were negative. Serum IL-5 was mildly elevated (18 pg/mL; reference range: <3.1 pg/mL), and serum total IgE was markedly elevated at 3680 IU/mL (reference range: <200 IU/mL), with moderate sensitization to mold (class 2). The patient developed new-onset chest tightness and dyspnea and was diagnosed with asthma (ACQ-5:1.6), managed with inhaled budesonide/formoterol.
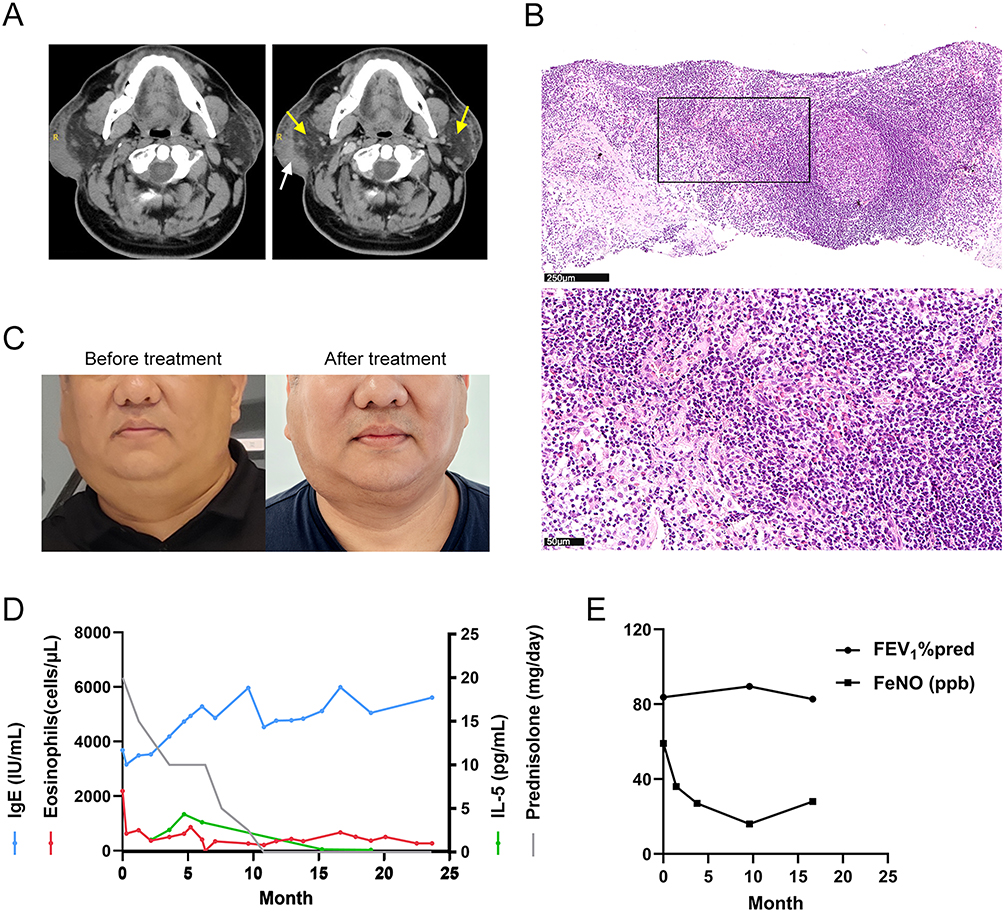 |
Figure 1 Clinical and laboratory parameters of case 1. (A) Axial contrast-enhanced computed tomography (CT) images obtained prior to mepolizumab treatment, showing mild enhancement of the right subcutaneous thickening (white arrow) and enlarged bilateral parotid-region lymph nodes (yellow arrows). (B) Hematoxylin and eosin (HE) staining of a left cervical lymph node biopsy showing scattered eosinophilic infiltration, with both low and high magnifications. (C) Clinical photographs of the submandibular region before and after 10 months of mepolizumab treatment. (D) Longitudinal trends in peripheral eosinophil count (reference range: 20–520 cells/μL), serum immunoglobulin E (IgE, reference range: <220 IU/mL), interleukin-5 (IL-5, reference range: 0.00–3.10 pg/mL) levels, and daily prednisolone dose during mepolizumab therapy. (E) Pulmonary function test results and fractional exhaled nitric oxide (FeNO) levels following the initiation of mepolizumab treatment. |
Reassessment of lymph node pathology at our institution confirmed follicular hyperplasia with eosinophilic infiltration (Figure 1B), consistent with KD. Oral prednisolone (30 mg/day) led to improved control of asthma, pruritus, and lymphadenopathy, with corresponding decreases in eosinophil counts. However, recurrence occurred upon prednisolone tapering to 10 mg/day. After providing written informed consent, mepolizumab (100 mg every four weeks) was introduced as adjunctive therapy for 10 months. After the treatment, the patient achieved sustained symptom control, including reduced lymphadenopathy (Figure 1C), asthma control (ACQ-5:0.4), and successful corticosteroid discontinuation, although mild residual pruritus (VAS: 3) persisted. Eosinophil and IL-5 levels remained low, although serum IgE levels stayed elevated (Figure 1D). Pulmonary function and FeNO levels also improved (Figure 1E). The patient continues receiving mepolizumab 100 mg every four weeks and has been followed up for 24 months without recurrence.
Case 2
A 39-year-old non-smoking male with recurrent urticaria since age 30 was diagnosed with allergic asthma in 2016, despite mild sensitization to dust mites (class 1). He used inhaled budesonide/formoterol for asthma control. His peak BEC was 3.45 × 109/L (31.7% of total leukocytes). Evaluation for secondary causes, including parasitic, autoimmune, and infectious etiologies, was negative. A skin biopsy showed dense eosinophil infiltration in the dermis and subcutaneous tissue, particularly around blood vessels and collagen bundles. Bone marrow examination showed normal morphology, with eosinophils comprising 16.5% of nucleated marrow cells and 45% of peripheral leukocytes. Immunophenotyping, cytogenetics, and molecular testing for BCR/ABL and FIP1L1/PDGFRα/β were unremarkable. Bone marrow histology confirmed eosinophilia (~15%).
Initial treatment included oral prednisolone (15–20 mg/day), budesonide/formoterol, and antihistamines. In 2021, surgical excision was performed because of progressive enlargement of the right axillary lymph nodes (maximum: 35×17 mm) (Figure 2A). Histopathology revealed follicular hyperplasia, interfollicular expansion, and eosinophilic microabscesses (Figure 2B). Serum IgE was significantly elevated at 2880 IU/mL (reference range: <200 IU/mL), while IL-5 was within normal range at 2.5 pg/mL (reference range: <3.1 pg/mL). These findings confirmed the diagnosis of KD.
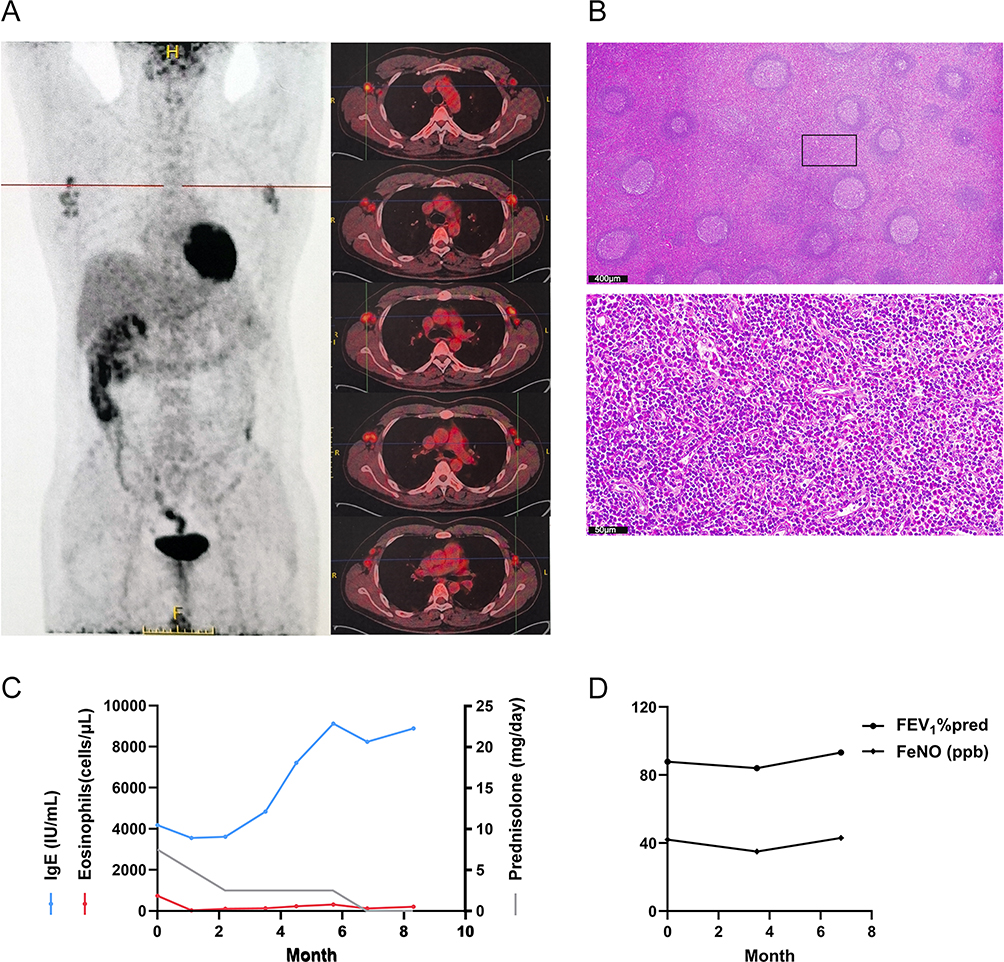 |
Figure 2 Clinical and laboratory parameters of case 2. (A) Positron-emission tomography-computed tomography (PET-CT) showing multiple enlarged lymph nodes in the bilateral axillary regions with increased fluorodeoxyglucose uptake (SUVmax ~4.7). (B) HE staining (low and high magnification) of surgical specimen showing a large number of eosinophils infiltrating the interfollicular areas. (C) Longitudinal trends in peripheral eosinophil count (reference range: 20–520 cells/μL), serum IgE concentration (reference range: <220 IU/mL), and daily prednisolone dosage during therapy. (D) Pulmonary function tests and FeNO levels during mepolizumab treatment. |
The patient continued low-dose prednisolone (7.5 mg/day) and antihistamines but experienced poor asthma control (ACQ-5: 2.8) and severe pruritus (VAS: 8 scores) when he presented to our center in November 2024. Following informed consent, mepolizumab (200 mg every four weeks) was initiated as adjunctive therapy for 8 months. After the treatment, eosinophilia improved over time, but serum IgE levels remained high (Figure 2C). Significant improvement in asthma control (ACQ-5:0), pulmonary function and FeNO (Figure 2D), and pruritus (VAS: 2) was observed and corticosteroids use was successfully tapered off after 6 months of treatment. The patient continues on mepolizumab therapy with regular follow-up.
Case 3
A 43-year-old woman with a longstanding atopic background, including childhood asthma and more than 20 years of allergic rhinitis, was first diagnosed with recurrent urticaria in 2020. In July 2024, she developed unexplained chest tightness and dyspnea. Pulmonary function testing revealed isolated small airway dysfunction (forced expiratory flow rate at 25–75%: 52.97%), and she was diagnosed with allergic asthma despite negative serum-specific IgE testing. Respiratory symptoms were stabilized with low-dose inhaled corticosteroid and long-acting β2-agonist therapy.
At presentation, her peak BEC was 2.83 × 109/L (31.5% of leukocytes), although serum total IgE (10 IU/mL, reference range: <220 IU/mL) and IL-5 (3.28 pg/mL, reference <3.1 pg/mL) remained within normal limits. Asthma control was stable (ACQ-5: 0.6), but the patient had generalized pruritus (VAS: 5). Comprehensive evaluation for secondary causes of eosinophilia, including parasitic infections, autoimmune disorders, and other infectious etiologies, was negative. Bone marrow morphology was unremarkable, showing 10% eosinophils, and cytogenetic and molecular studies for clonal eosinophilic disorders were negative. Ultrasonography revealed left inguinal lymph nodes (maximum: 46×18 mm), and FNA confirmed prominent eosinophilic infiltration and florid vascular proliferation within the interfollicular areas (Figure 3A).
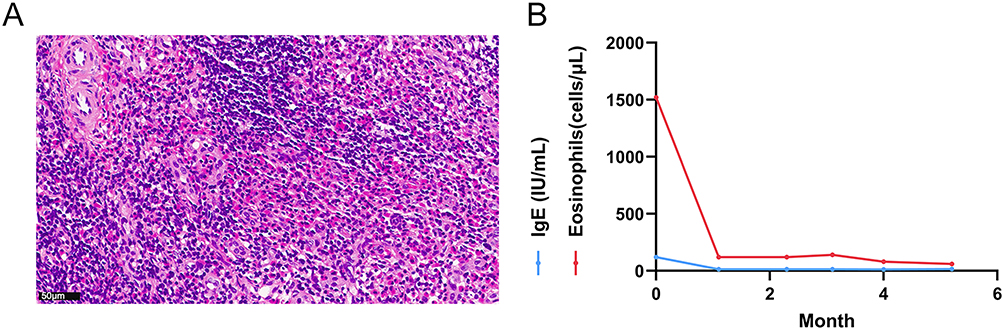 |
Figure 3 Clinical and laboratory parameters of case 3. (A) HE staining of the biopsy specimen a large number of eosinophils infiltrating the interfollicular areas. (B) Longitudinal changes in peripheral eosinophil count (reference range: 20–520 cells/μL) and serum IgE levels (reference range: <220 IU/mL) during mepolizumab treatment. |
The diagnosis of KD was made based on the clinical presentation, blood eosinophilia, characteristic lymph node histopathology, and exclusion of alternative diagnoses. Following informed consent, mepolizumab 300 mg was administered subcutaneously every four weeks for 5 months. After the treatment, a slight reduction of the target lymph node was observed (44 × 15 mm), and the patient reported marked improvement in pruritus (VAS: 0). Peripheral blood eosinophil counts declined steadily over the treatment period, with persistently low IgE levels (Figure 3B). The patient continues on maintenance mepolizumab with regular monitoring.
Discussion
This study provided a comprehensive analysis of 53 KD patients, emphasizing the potential therapeutic role of mepolizumab. A significant finding of this study is the age-stratified analysis, which corroborates previous reports regarding the male predominance of KD and its gradual onset with age. Kakehi et al8 reported a marked increase in pruritus and diagnostic delays in older patients. Our study similarly found an age-related increase in pruritus but did not observe significant differences in the time to diagnosis across different age groups. This discrepancy may be attributed to variations in clinical practice and patient characteristics across different regions. Moreover, our study found that six patients had coexisting IgG4-RD, supporting the notion that KD may overlap with other immune-mediated diseases. This finding aligns with the work of Wang et al,9 who noted that 20–30% of KD patients met the histopathological criteria for IgG4-RD. Both KD and IgG4-RD are thought to be driven by Th2 immune responses.10 In particular, IL-4 and IL-13 secreted by Th2 cells play crucial roles in promoting class switching to IgE and IgG4, leading to eosinophilic inflammation and fibrosis in both diseases. Furthermore, IL-5 supports eosinophil activation, which is a hallmark of both KD and IgG4-RD. Anti-IL-5 therapy, such as mepolizumab, not only alleviates eosinophilic inflammation but also results in a reduction in IgG4-producing plasma cells in situ, as demonstrated in KD from previous study.5 By reducing eosinophil activation and eosinophil-related cytokines, IL-5 inhibition may also impact the IgG4-driven processes, where IL-4 and IL-13 contribute to IgG4 class switching.11 The differences in the type of fibrosis (patternless in KD versus storiform in IgG4-RD) and the involvement of specific organs (KD being more localized to the head and neck region, whereas IgG4-RD can affect multiple organs) may help differentiate the two diseases. Further research into the molecular pathways driving both diseases is necessary to better understand their relationship and refine diagnostic criteria.
The pathogenesis of KD remains unclear but is thought to involve an abnormal immune response, predominantly driven by a Th2 immune response, with elevated levels of IL-4, IL-5, and IgE, which promote eosinophilic inflammation and IgE-mediated immune responses.12–14 Notably, serum IgE levels are not always elevated and may not be essential for KD diagnosis,15,16 as type 2 inflammatory cytokines can stimulate other inflammatory mediators, and eosinophils can independently promote tissue inflammation.17 IL-5 plays a central role in eosinophil recruitment, activation, and survival, contributing tissue damage through the release of cytotoxic granules, reactive oxygen species (ROS), and pro-inflammatory cytokines. These toxic molecules are released independently of IgE. This may explain why the IgE levels in 25% (8/32) of the cohort as well as Case 3 remained low. The persistence of eosinophilic infiltration, especially in lymph nodes and subcutaneous tissues, is one of the defining features of KD. Furthermore, a recent study suggested that the Erk/MAPK signaling pathway, promoted by S100P, is over-activated in eosinophils from KD patients.18 This pathway is associated with eosinophil migration, differentiation, and the production of pro-inflammatory cytokines like IL-4 and IL-13. Moreover, while most KD cases occur in young males from East Asia, increasing reports non-Asian populations suggest that genetic, environmental, or infectious factors may contribute to the disease onset. Infectious agents,19 including human polyomavirus 6, tuberculosis, and parasitic infections, have been implicated in triggering or exacerbating KD, although the exact relationship remains unclear. Genetic studies have not yet identified definitive mutations linked to KD, but autoimmune or hypersensitivity reactions may serve as potential triggers.20
Despite the variety of therapeutic strategies available, including surgical excision, steroids, immunosuppressants, and radiation therapy, the treatment of KD remains challenging, particularly due to high recurrence rates and side effects. Surgical excision is often considered the first-line treatment for localized KD lesions, especially when the disease is confined to well-circumscribed nodules. The histopathologic confirmation of KD following excision offers the greatest diagnostic accuracy. However, surgery alone often fails to prevent recurrence, with reported relapse rates ranging from 25% to 60%.21,22 Furthermore, cosmetic concerns due to excision in the head and neck region make surgery a suboptimal long-term solution for some patients. Corticosteroids have long been the cornerstone of KD treatment due to their potent anti-inflammatory effects. However, prolonged steroids use can result in significant side effects, including osteoporosis, hypertension, and diabetes mellitus. Moreover, recurrence is common once steroids are tapered or discontinued, suggesting that steroids may only provide temporary relief rather than a long-term solution. Immunosuppressive agents, including cyclosporine, azathioprine, and methotrexate, have been explored as alternatives or adjuncts to corticosteroids.23 However, these therapies often result in suboptimal responses and are limited by side effects and the need for prolonged treatment. Radiotherapy has been proposed as an adjunct treatment for recurrent or inoperable KD lesions, particularly in cases where surgery is difficult or contraindicated.24 While studies have shown that radiotherapy can reduce lesion size and prevent recurrence, it is not without risks, including radiation-induced toxicity and potential malignancy. The lack of standardized dosing regimens and uncertainty about the relationship between radiation dose, lesion size, and long-term outcomes limit its widespread application.
In recent years, biologic therapies, including omalizumab, dupilumab, mepolizumab, and benralizumab have emerged as potential alternatives, offering more targeted approaches for KD with fewer systemic side effects. Omalizumab has been employed to control KD symptoms, particularly those associated with IgE-mediated allergic responses. However, its effectiveness has been inconsistent, with limited effects observed in corticosteroids tapering.4,25 Dupilumab has shown short-term benefits in cases with concurrent AD-like skin symptoms and high IgE levels,3,12,26–33 although whether IgE-dependence remains debated.32 Concerns have also been raised about dupilumab-induced eosinophilia in AD,34 particularly in diseases like KD, which are already characterized by high eosinophil levels. An anti-IL-5 therapy has garnered attention as a promising therapy for KD,5 particularly due to its ability to target eosinophilic inflammation.
A total of 8 cases has been reported to receive anti-IL-5 therapy, including 3 cases from this study5,16,35–37 (Table 2). Of these, 7 cases were treated with mepolizumab, while one case received benralizumab. Among these eight patients, ages ranged from 21 to 45 years, and the disease duration in some cases extended beyond 15 years. The primary symptoms in these cases included tissue swelling, lymphadenopathy, and pruritus, accompanied by elevated eosinophil and total IgE levels. Asthma was the most common comorbidity, followed by sinusitis, eczema, and urticaria. Six of these patients had received previous treatments, such as surgery and steroid therapy, with limited efficacy.
 |
Table 2 Cases of Kimura Disease Treated with Anti-IL-5 Pathway Antibodies |
The doses of mepolizumab varied in the seven patients treated: 100 mg in two cases, 200 mg in one case, and 300 mg in four cases. The initial evaluation period ranged from 3 to 16 months, and almost all patients showed significant clinical improvements, including symptom resolution and a decrease in eosinophil counts (excluding total IgE levels). Tao et al36 reported that Case 7 showed a greater clinical response to dupilumab after an inadequate response to mepolizumab, as well as the level of serum IgE. This may not be considered a suboptimal therapeutic response given the short treatment duration of only three months. However, a possible explanation for the differing effects on IgE is that dupilumab offers a broader immunomodulatory effect, resulting in more pronounced reductions in IgE levels compared to mepolizumab, whose action is more specifically restricted to eosinophil-mediated pathways, with a less significant impact on IgE production. This phenomenon has been confirmed in previous report5 as well as in our Case 1 and Case 2. Interestingly, Case 5 developed cervical lymphadenopathy after 8 months of mepolizumab 100 mg treatment for eosinophilic sinusitis. After KD diagnosis and lymph node excision, the patient continued mepolizumab therapy with a dose adjustment to 300 mg, in combination with methotrexate, and remained in remission for 16 months without recurrence. However, due to the potential contribution of methotrexate, it is difficult to draw conclusions about the dose-effect relationship of mepolizumab.
Given the similarities between KD and other systemic eosinophilic-associated diseases,38 the dosing regimen of mepolizumab for our three patients was based on the recommended doses for eosinophilic granulomatosis with polyangiitis (EGPA), specifically 300 mg every 4 weeks. However, due to financial constraints, Case 1 and Case 2 received reduced doses of 100 mg and 200 mg, respectively. Despite not achieving complete resolution of pruritus, both patients benefited from mepolizumab therapy, including sustained remission, corticosteroids withdrawal, and a reduction in eosinophil counts. Given the limited number of cases, it is not possible to determine the optimal dosage and treatment duration for mepolizumab. In fact, this issue remains a subject of controversy even in the treatment of EGPA.39 Finally, benralizumab has been shown to be noninferior to mepolizumab in inducing remission in EGPA.40 A case of KD with extensive maculopapular pruritic and ulcerating rashes, reported by Szeto et al37 demonstrated significant improvement in skin lesions after treatment with benralizumab, with no recurrence of the underlying rash, lymphadenopathy, or asthma symptoms. Whether benrelizumab is superior to mepolizumab in the treatment of KD remains to be confirmed by head-to-head clinical trials.
This study has several limitations. Firstly, its retrospective design inherently limits the completeness of the data, comparison with a control group, and the ability to establish causality or control for potential confounding factors. The study also includes a relatively small sample size of 53 patients, with only three receiving mepolizumab, which reduces the generalizability of the findings and makes it challenging to extrapolate the results to the broader KD population. Moreover, variations in dosing regimens and follow-up periods among the patients complicate the interpretation of treatment outcomes and hinder the establishment of optimal therapeutic protocols. All patients in this study were Chinese, which may limit the applicability of the findings to non-Asian populations. Despite these limitations, this study holds significant value for several reasons. First, this study provides valuable insights into the age-stratified characteristics of KD patients. The findings also contribute to the understanding of the potential overlap between KD and IgG4-related disease, suggesting shared immunologic pathways that may influence treatment strategies. Second, this is one of the few studies to explore the use of mepolizumab in KD treatment, offering clinical insights despite the small sample size. Finally, the study paves the way for future research, particularly randomized controlled trials, to assess the long-term safety and efficacy of mepolizumab in KD and establish standardized treatment protocols.
Conclusion
Currently, the etiology of KD remains unclear, and its clinical presentation is highly heterogeneous, making diagnosis a significant challenge. Various treatment strategies have not shown substantial efficacy, and recurrence rates remain high. This study provides a comprehensive summary and age-stratified analysis of KD cases from multiple centers in China, revealing an age-dependent increase in pruritus incidence and highlighting the coexistence with IgG4-related disease based on histopathology. These findings offer valuable data for expanding the understanding of KD. Additionally, this study reports three cases of KD treated with mepolizumab, which, despite varying doses and follow-up periods, shows great potential as a new treatment strategy. Prospective trials are needed to define optimal dosing/duration. Our case series provides real-world clinical practice examples of biologic therapy, particularly the limited use of anti-IL-5 treatment, laying a foundation for future larger-scale studies.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding authors upon reasonable request. For data access, please contact either Meiling Jin or Ling Ye.
Ethics Approval
Approval for this research was granted by the ethics committee of Zhongshan Hospital, Fudan University (B2019-020R), and Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (SH9H-2024-T174-2). The institutional approval was waived for publishing the case details since deidentification data involve no potential risk to patients.
Consent for Publication
Informed consent was obtained from all patients or their legal guardians. Written informed consents have been provided by all patients to publish their case details and any accompanying images.
Funding
This research received funding from the National Natural Science Foundation of China (grant numbers: 82202054, 82270028, 82470020) and the Special Fund for Clinical Research, Zhongshan Hospital Affiliated to Fudan University (ZSLCYJ202330).
Disclosure
The authors state that there are no conflicts of interest related to this work.
References
1. Braun J, Mairinger T, Kaschke O, Behrendt K, Ramsbacher J, Karberg K. Bilateral swelling of the salivary glands and sicca symptoms: an unusual differential diagnosis-Kimura’s disease, a rare allergic condition with a high IgE serum level-a case report and review of the literature. RMD Open. 2023;9(2):e003135. doi:10.1136/rmdopen-2023-003135
2. Lagerstrom IT, Danielson DT, Muir JM, Foss RD, Auerbach A, Aguilera NS. A Comprehensive Review of Kimura Disease. Head Neck Pathol. 2025;19(1). doi:10.1007/s12105-025-01812-z
3. Luo SY, Zhou KY, Wang QX, Deng LJ, Fang S. Kimura’s disease treated with dupilumab: A case report and literature review. Int Immunopharmacol. 2024;131:111895. doi:10.1016/j.intimp.2024.111895
4. Ao S, Huang G, Tang X, et al. Anti-immunoglobulin E provides an additional therapy to conventional steroids for Kimura’s disease. J Dermatol. 2024;51(4):602–606. doi:10.1111/1346-8138.17021
5. Kinoshita M, Ogawa Y, Onaka M, Shimada S, Kawamura T. Mepolizumab-responsive Kimura disease. J Allergy Clin Immunol Pract. 2021;9(7):2928–2930. doi:10.1016/j.jaip.2021.02.049
6. Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Modern Patholog. 2012;25(9):1181–1192. doi:10.1038/modpathol.2012.72
7. Juniper EF, Svensson K, Mörk AC, Ståhl E. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med. 2005;99(5):553–558. doi:10.1016/j.rmed.2004.10.008
8. Zhang X, Jiao Y. Kimura’s disease: effects of age on clinical presentation. QJM. 2020;113(5):381–382. doi:10.1093/qjmed/hcaa034
9. Wang X, Ng CS, Yin W. A comparative study of Kimura’s disease and IgG4-related disease: similarities, differences and overlapping features. Histopathology. 2021;79(5):801–809. doi:10.1111/his.14428
10. Munemura R, Maehara T, Murakami Y, et al. Distinct disease-specific Tfh cell populations in 2 different fibrotic diseases: IgG(4)-related disease and Kimura disease. J Allergy Clin Immunol. 2022;150(2):440–455.e17. doi:10.1016/j.jaci.2022.03.034
11. Lee CC, Yu KH, Chan TM. Kimura’s disease: A clinicopathological study of 23 cases. Front Med Lausanne. 2022;9:1069102. doi:10.3389/fmed.2022.1069102
12. Suga K, Kiuchi M, Kageyama T, et al. Single-cell RNA sequencing of peripheral blood mononuclear cells from Kimura disease patient successfully treated with dupilumab. Allergolog inter. 2023;72(4):610–613. doi:10.1016/j.alit.2023.06.002
13. Chen QL, Li CX, Shao B, et al. Expression of the interleukin-21 and phosphorylated extracellular signal regulated kinase 1/2 in Kimura disease. J Clin Pathol. 2017;70(8):684–689. doi:10.1136/jclinpath-2016-204096
14. Ohta N, Fukase S, Suzuki Y, Ito T, Yoshitake H, Aoyagi M. Increase of Th2 and Tc1 cells in patients with Kimura’s disease. Auris Nasus Larynx. 2011;38(1):77–82. doi:10.1016/j.anl.2010.03.011
15. Han Q, Han J, Wang W, et al. Case report: Kimura’s disease with minimal degenerative glomerulopathy without eosinophil infiltration responds to mycophenolate mofetil treatment. Front Med Lausanne. 2022;9:1069553. doi:10.3389/fmed.2022.1069553
16. Ho J, Walter S, Harvey RJ. Eosinophilic chronic rhinosinusitis and concurrent Kimura’s disease treated with mepolizumab. BMJ Case Rep. 2021;14(1):e232627. doi:10.1136/bcr-2019-232627
17. Ogulur I, Mitamura Y, Yazici D, et al. Type 2 immunity in allergic diseases. Cell Mol Immunol. 2025;22(3):211–242. doi:10.1038/s41423-025-01261-2
18. Wu X, Wang A, Zhang S, et al. Multiomic landscape of immune pathogenesis in Kimura’s disease. Iscience. 2023;26(4):106559. doi:10.1016/j.isci.2023.106559
19. Yorita K, Fujii T, Nagao T, et al. Kimura disease forming a human polyomavirus 6-negative parotid gland nodule with prominent squamous metaplasia in a young female: A case report. Radiol Case Rep. 2023;18(5):1933–1938. doi:10.1016/j.radcr.2023.02.027
20. Xie F, Kou Y, Zhang S, Shi L, Han J, Zhou X. Bilateral posterior auricular masses: A case of Kimura’s disease. Ear Nose Throat J. 2021;100(9):634–637. doi:10.1177/01455613211045549
21. Fan L, Mo S, Wang Y, Clinical ZJ. Pathological, laboratory characteristics, and treatment regimens of Kimura disease and their relationships with tumor size and recurrence. Front Med Lausanne. 2021;8:720144. doi:10.3389/fmed.2021.720144
22. Kim WJ, Kim HK. Current concepts of Kimura disease: pathophysiology and evolution of treatment. Arch Craniofac Surg. 2022;23(6):249–255. doi:10.7181/acfs.2022.01053
23. Ma H. Treatment of Kimura’s disease with oral corticosteroid and methotrexate. An Bras Dermatol. 2020;95(1):115–117. doi:10.1016/j.abd.2019.03.006
24. Muangwong P, Chitapanarux I, Ya-In C, Klibngern H, Kongmebhol P. Natural history and treatment outcome of radiotherapy for Kimura’s disease. Indian J Cancer. 2021. doi:10.4103/ijc.IJC_69_20
25. Nonaka M, Sakitani E, Yoshihara T. Anti-IgE therapy to Kimura’s disease: a pilot study. Auris Nasus Larynx. 2014;41(4):384–388. doi:10.1016/j.anl.2013.12.006
26. Huang HY, Yang CY, Yao WT, et al. Kimura disease of the thigh treated with surgical excision and dupilumab. Ann Plast Surg. 2022;88(1s Suppl 1):S110–S113. doi:10.1097/SAP.0000000000003106
27. Teraki Y, Terao A . Treatment of Kimura Disease With Dupilumab. JAMA Dermatol. 2022;158(3):329–330. doi:10.1001/jamadermatol.2021.5885
28. Bellinato F, Mastrosimini MG, Querzoli G, Gisondi P, Girolomoni G. Dupilumab for recalcitrant Kimura disease. Dermatol Ther. 2022;35(9):e15674. doi:10.1111/dth.15674
29. Cordeil S, Hermine O, Hot A. Diagnostic challenges and updated therapeutic strategies of Kimura’s disease: A case report successfully treated by dupilumab and review. Medicine. 2023;102(47):e34191. doi:10.1097/MD.0000000000034191
30. Shang BS, Hsiao CH, Tsao TF, et al. Clinical effects of dupilumab: A novel treatment for Kimura disease. Immun Inflamm Dis. 2023;11(11):e1084. doi:10.1002/iid3.1084
31. Battesti G, Jachiet M, Lepelletier C, et al. Two cases of dupilumab-responsive Kimura disease. Clin Exp Dermatol. 2024;49(5):502–506. doi:10.1093/ced/llad455
32. Yang B, Yu H, Jia M, et al. Successful treatment of dupilumab in Kimura disease independent of IgE: A case report with literature review. Front Immunol. 2022;13:1084879. doi:10.3389/fimmu.2022.1084879
33. Liu YL, Ran YT, Zhang YF, Peng XT, Xia YM, Yan HL. Efficacy and safety of dupilumab in the treatment of kimura’s disease. QJM. 2024;117(8):575–580. doi:10.1093/qjmed/hcae048
34. Musters AH, van Lookeren FL, van der Gang LF, et al. Real-world reported adverse events related to systemic immunomodulating therapy in patients with atopic dermatitis: Results from the TREAT NL (TREatment of ATopic eczema, the Netherlands) registry. J Euro Acad Dermatol Venereol. 2024;38(3):530–542. doi:10.1111/jdv.19643
35. Al Shammari F, Nasiri A, Alkhathami M, Alawfi F, Alfifi M, Al Otaibi E. Mepolizumab as an effective treatment for Kimura’s disease associated with ulcerative colitis: A case report. J Family Med Prim Care. 2019;8(9):3028–3031. doi:10.4103/jfmpc.jfmpc_373_19
36. Tao M, Gao T, Zhi L, Cao N, Liu H. Rapid improvement of kimura disease with dupilumab in a patient with suboptimal response to mepolizumab: a case report. J Dermatological Treat. 2025;36(1). doi:10.1080/09546634.2025.2486668
37. Szeto VG, Chin-Yee B, Dehghani M, Rizkalla K, Licskai C, Hsia CC. Successful treatment of Kimura disease with benralizumab. Ann Hematol. 2022;101(9):2099–2100. doi:10.1007/s00277-022-04873-0
38. Lombardi C, Berti A, Cottini M. The emerging roles of eosinophils: Implications for the targeted treatment of eosinophilic-associated inflammatory conditions. Curr Res Immunol. 2022;3:42–53. doi:10.1016/j.crimmu.2022.03.002
39. Caminati M, Crisafulli E, Lunardi C, et al. Mepolizumab 100 mg in severe asthmatic patients with EGPA in remission phase. J Allergy Clin Immunol Pract. 2021;9(3):1386–1388. doi:10.1016/j.jaip.2020.09.025
40. Wechsler ME, Nair P, Terrier B, et al. Benralizumab versus Mepolizumab for Eosinophilic Granulomatosis with Polyangiitis. N Engl J Med. 2024;390(10):911–921. doi:10.1056/NEJMoa2311155
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Mepolizumab in Severe Uncontrolled Asthma Associated or Not with EGPA Based on the Exacto Scale and Separ-Remas Criteria
Leon Lloreda A, Muñoz-Sánchez B, Echavarria Kashmiri D, Polonio Gonzalez ML, Maestre Sanchez MV, Ferrrer Galvan M, Romero Falcon A, Medina Gallardo JF, Alvarez-Gutierrez FJ
Journal of Asthma and Allergy 2026, 19:565740
Published Date: 11 February 2026
Systemic Immune Dysregulation in Allergic Rhinitis: Mechanisms, Comorbidities, and Implications for Targeted Therapy
Hui D, Shi C, Fan Y, Han M, Wang Y, Sun J, Xue Y, Li E
Journal of Asthma and Allergy 2026, 19:589195
Published Date: 9 March 2026