Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Effectiveness of Discharge Planning Interventions for Stroke and Heart Conditions: A Systematic Review of Interventional Studies
Authors Ruksakulpiwat S ![]() , Benjasirisan C
, Benjasirisan C ![]() , Phianhasin L
, Phianhasin L ![]() , Koson N, Chei NE, Rounratana T
, Koson N, Chei NE, Rounratana T ![]() , Saenkla P
, Saenkla P ![]() , Thampakkul J
, Thampakkul J
Received 27 August 2025
Accepted for publication 30 October 2025
Published 15 November 2025 Volume 2025:18 Pages 7521—7537
DOI https://doi.org/10.2147/JMDH.S563476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Linda Yoder
Suebsarn Ruksakulpiwat,1 Chitchanok Benjasirisan,1 Lalipat Phianhasin,1 Naruebeth Koson,2 Nway Eint Chei,3 Thanin Rounratana,4 Pennapa Saenkla,1 Jai Thampakkul5
1Faculty of Nursing, Mahidol University, Bangkok, Thailand; 2Department of Adult and Gerontological Nursing, Boromrajonnani College of Nursing, Nakhon Si Thammarat, Faculty of Nursing, Praboromarajchanok Institute, Nakhon Si Thammarat, Thailand; 3Department of Business Management, Faculty of Arts, Science and Business Management, Myanmar Creative College, Yangon, Myanmar; 4Department of Nursing, King Chulalongkorn Memorial Hospital, The Thai Red Cross Society, Bangkok, Thailand; 5Department of Biomedical Engineering, Case Western Reserve University, Cleveland, OH, USA
Correspondence: Suebsarn Ruksakulpiwat, Faculty of Nursing, Mahidol University, Bangkok, 10700, Thailand, Email [email protected]
Objective: To evaluate the effectiveness of discharge planning interventions in improving health outcomes among individuals with stroke and heart conditions, synthesizing evidence from randomized controlled trials and quasi-experimental studies.
Methods: Following PRISMA guidelines, seven electronic databases (PubMed/MEDLINE, Scopus, ScienceDirect, CINAHL Plus with Full Text, Web of Science, Ovid, and ClinicalKey Nursing) were searched for studies published between 2019 and 2024. Eligible studies included adults with stroke or heart conditions who received discharge planning interventions, with outcomes compared to usual care or alternative interventions. Risk of bias was assessed using the Cochrane Risk of Bias 2 tool for randomized controlled trials and ROBINS-I for quasi-experimental studies. Data were extracted with a standardized chart and synthesized using a convergent integrated approach in accordance with the Joanna Briggs Institute methodology.
Results: Sixteen studies (11 randomized controlled trials and 5 quasi-experimental studies) met the inclusion criteria, representing diverse populations across 11 countries. Interventions included structured discharge programs, early supported discharge, interdisciplinary planning, family-based care, nurse-led eHealth rehabilitation, and technology-enhanced approaches such as SMS, telephone, and interactive voice response systems. Six major outcome themes emerged: (1) healthcare utilization and cost outcomes, (2) patient activation and health behavior change, (3) psychological well-being, (4) functional recovery, (5) health-related quality of life, and (6) caregiver outcomes and support. Although mortality and long-term outcomes showed mixed results, most interventions demonstrated positive short-term effects across clinical, behavioral, and psychosocial domains.
Conclusion: Discharge planning interventions improve transitional care and support recovery in stroke and heart disease populations, with particular benefits when multidisciplinary, nurse-led, or digitally supported. This review highlights the value of structured and innovative discharge planning models for clinical practice. Incorporating patient- and caregiver-centered strategies can reduce readmissions, strengthen adherence, and improve long-term health outcomes.
Keywords: discharge planning, transitional care, stroke, heart conditions, readmission, quality of life, systematic review
Background
Stroke and heart conditions are major forms of non-communicable diseases (NCDs) and remain among the leading causes of morbidity and mortality worldwide. In 2021, cardiovascular diseases (CVDs), including both heart disease and stroke, accounted for about 20 million deaths, representing nearly one-third of all global deaths, with more than 80% occurring in low- and middle-income countries (LMICs).1,2 Stroke alone caused approximately 7 million deaths, ranking as the third leading cause of mortality worldwide.1 These statistics highlight the urgent need for coordinated and effective care strategies, especially during high-risk transition periods such as hospital discharge.
Hospitalization for stroke or cardiac events often necessitates comprehensive treatment and rehabilitation plans.3,4 However, the transition from hospital to home remains a vulnerable phase. Ineffective discharge planning can result in fragmented care, miscommunication between providers, unclear roles and responsibilities, and ultimately, poor patient outcomes such as avoidable readmissions or deterioration in functional status.5,6 For instance, a study by Hesselink et al (2014) highlighted that poor discharge processes contribute significantly to unplanned hospital readmissions.7 Similarly, Patel and Bechmann (2020) emphasized that inadequate discharge planning is associated with increased risks of medication errors, patient dissatisfaction, and higher readmission rates.6 These findings underscore the importance of comprehensive discharge planning to ensure continuity of care and improve patient outcomes. Given the fluctuating clinical status and frequent transitions across care settings for these populations, structured and timely discharge planning is essential to support recovery and continuity of care.
In recent years, digital health innovations, such as telemonitoring, electronic care coordination platforms, and mobile health applications, have begun transforming discharge planning.8,9 These tools facilitate remote monitoring, enhance communication between patients and healthcare teams, and ensure timely follow-up after hospital discharge.8,9 Integrating such technologies into transitional care models has demonstrated potential to reduce readmissions and strengthen self-management, particularly for individuals with stroke10,11 and heart conditions.12,13
Discharge planning refers to a structured process that ensures patients and their caregivers are adequately prepared to manage care at home. This includes the provision of follow-up services, patient education, and home-based support interventions tailored to individual needs.6,14,15 For individuals recovering from stroke or managing heart conditions, such planning is particularly crucial to prevent complications, enhance treatment adherence, and promote quality of life.16–18
A multidisciplinary or interdisciplinary approach is often recommended in discharge planning to foster collaboration among healthcare professionals.19–21 By involving diverse team members, nurses, physicians, physiotherapists, case managers, and social workers, this approach enhances care integration, improves communication, and allows for a more comprehensive understanding of the patient’s needs.19–21 Such models are associated with improved patient satisfaction, better self-management, and reduced healthcare utilization. Emerging digital health solutions, including telemonitoring and electronic care coordination platforms, further augment the effectiveness of discharge planning by improving continuity of care and minimizing unnecessary hospital visits.22,23 These innovations are especially beneficial for stroke and heart disease patients, who often require close monitoring and early detection of deterioration after discharge.
Despite these advancements, evidence on how such multidisciplinary and technology-enhanced approaches translate into measurable health outcomes remains limited. Individuals with stroke and heart conditions are among the most vulnerable groups during care transitions due to the complexity of their conditions and the high risk of adverse outcomes after hospital discharge.24–26 Despite the recognized importance of discharge planning, there is a lack of consolidated evidence focused specifically on these populations. Existing studies vary in terms of intervention strategies, care settings, and outcome measures, making it difficult to establish best practices. This systematic review will address this gap by synthesizing high-quality empirical evidence from randomized controlled trials and quasi-experimental studies to determine the effectiveness of discharge planning interventions. The findings aim to inform clinical practice, enhance transitional care strategies, and support health policy development for stroke and heart disease management.
Objective
To systematically evaluate the effectiveness of discharge planning interventions on health-related outcomes among individuals with stroke and heart conditions, based on evidence from randomized controlled trials and quasi-experimental studies.
Methods
Identify Relevant Studies
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines27 in this systematic review, presenting a flow diagram of literature identification, screening, exclusion, and inclusion. A systematic search was conducted across seven electronic databases—PubMed/MEDLINE, Scopus, ScienceDirect, CINAHL Plus with Full Text, Web of Science, Ovid, and ClinicalKey Nursing—to identify relevant studies published between 2019 and 2024 that investigated the effectiveness of discharge planning interventions among individuals with stroke and heart conditions. The search strategy combined Medical Subject Headings (MeSH) and free-text terms using Boolean operators (Supplementary Data 1). Additionally, reference lists of included articles were manually reviewed to identify further relevant studies. All references were stored and managed using EndNote X7, and duplicates were removed prior to screening.
Study Selection
Titles and abstracts of all retrieved articles were initially screened to identify potentially relevant studies. Subsequently, the full texts of these articles were reviewed to assess their relevance to the review objectives. Studies were selected based on predefined inclusion criteria to ensure alignment with the scope of this review. Concurrently, exclusion criteria were applied to remove articles that did not meet the eligibility requirements (Table 1).
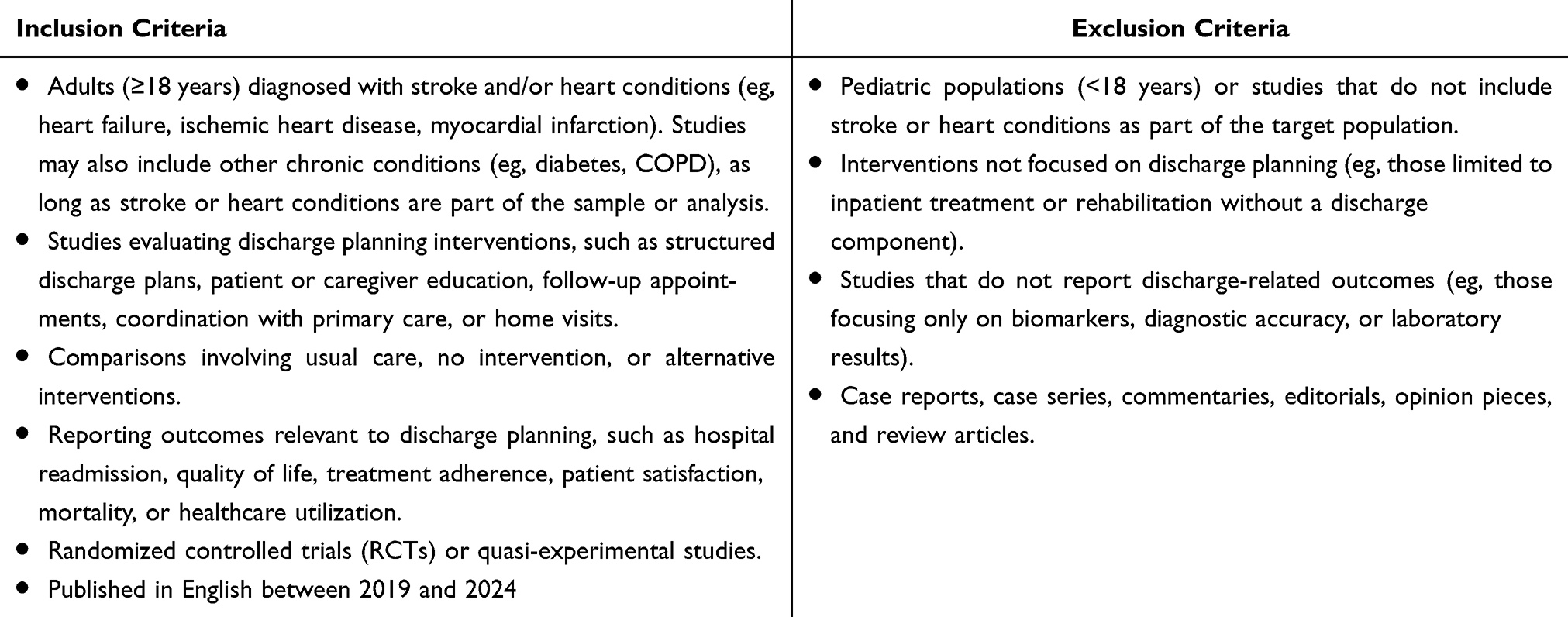 |
Table 1 Inclusion and Exclusion Criteria |
Risk of Bias Assessment
The methodological quality of the included studies was evaluated using two established tools recommended by the Cochrane Collaboration: the Risk of Bias 2 (RoB 2) tool for randomized controlled trials (RCTs) and the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool for quasi-experimental studies. The RoB 2 tool28 examines five critical domains: the randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and the selection of reported results. Each domain was rated as presenting a low risk of bias, some concerns, or a high risk of bias. For studies without randomization, the ROBINS-I tool29 was utilized to assess potential bias across seven domains: confounding, participant selection, intervention classification, deviations from intended interventions, missing data, outcome measurement, and reporting of results. Based on these domains, each study was assigned an overall risk rating of low, moderate, serious, or critical. Two reviewers independently conducted all risk of bias assessments. Any disagreements were resolved through discussion, and when necessary, by consulting a third reviewer to maintain consistency and methodological rigor.
Data Extraction
A standardized chart for data extraction (Supplementary Data 2) was developed to systematically organize and document the characteristics of each included study. All data were extracted independently by two reviewers using the standardized chart, and any disagreements were resolved through discussion or consultation with a third reviewer to ensure accuracy and completeness.
Data Synthesis
Data from the included studies were synthesized using a convergent integrated approach, following the Joanna Briggs Institute (JBI) methodology for systematic reviews.30 The synthesis process was designed to identify key outcome domains improved by discharge planning interventions among individuals with stroke and heart conditions. A thematic analysis framework was applied to systematically examine and categorize the outcomes reported across studies.
At this stage, data are being reviewed to group similar outcome measures into overarching themes. For example, outcomes such as reduced hospital readmission, improved treatment adherence, enhanced patient satisfaction, and better quality of life may be grouped under broader thematic categories such as healthcare utilization, self-management, and patient-centered outcomes. Sub-themes may also emerge to reflect specific intervention effects or contextual differences across studies. This process allows for the integration of findings from both randomized controlled trials and quasi-experimental studies into a structured narrative that highlights the effectiveness of discharge planning across various outcome dimensions.
Results
Following the PRISMA guidelines,31 a total of 2,708 records were initially identified through seven electronic databases, including PubMed and MEDLINE (n = 360), Scopus (n = 33), ScienceDirect (n = 1,159), CINAHL Plus with Full Text (n = 452), Web of Science (n = 212), Ovid (n = 347), and ClinicalKey Nursing (n = 145). After duplicate removal (n = 0), 2,708 records remained for title and abstract screening. During this phase, 2,654 records were excluded based on the predefined inclusion and exclusion criteria. Consequently, 54 full-text articles were retrieved and assessed for eligibility. Of these, 38 studies were excluded for reasons such as publication date or language (n = 6), ineligible study design (n = 9), intervention not related to discharge planning (n = 17), population not meeting criteria (n = 2), only abstract available (n = 3), and article retraction (n = 1). Ultimately, 16 studies were included in the final systematic review32–47 (Figure 1).
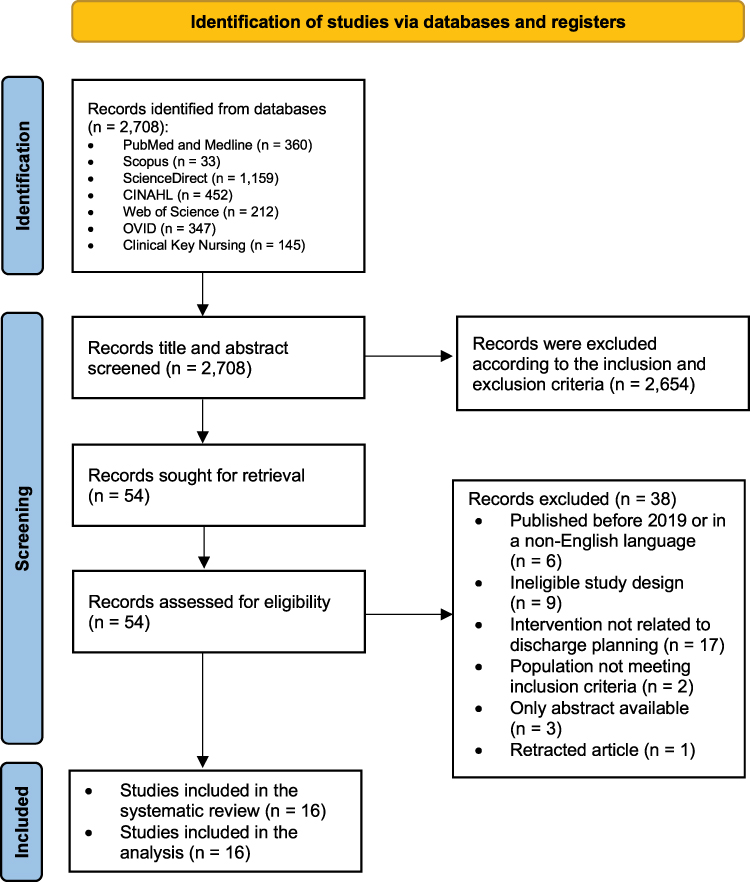 |
Figure 1 PRISMA Flow Chart. Note: Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71.27. |
Description of Included Studies
A total of 16 studies were included in this review, encompassing randomized controlled trials and quasi-experimental designs conducted across various countries, including Iran, Colombia, Switzerland, Thailand, Indonesia, China, France, the Netherlands, Australia, Brazil, and the United States. The target populations consisted of adult and older adult patients diagnosed with stroke, coronary artery disease (CAD), heart failure (HF), chronic heart failure (CHF), diabetes mellitus (DM), and other cardiovascular conditions. Several studies also included family caregivers as part of the intervention dyads. Sample sizes in the intervention groups ranged from 14 to 403 participants, with most studies reporting comparable control group sizes. The mean age of participants varied considerably, ranging from approximately 52.8 to 82.5 years, reflecting a predominance of older adults in post-discharge care studies. Most studies included a relatively balanced gender distribution, although some reported a higher proportion of male participants. Discharge planning interventions included a wide range of approaches, such as interdisciplinary discharge planning, structured discharge programs, early supported discharge (ESD), tailored discharge education, nurse-led eHealth rehabilitation, NIC/NOC frameworks, interactive voice response (IVR) support, family-centered programs, and comprehensive transitional care models like Cardiac Care Bridge. Specific interventions included structured summaries (eg, PC-AH-US, PODS), capacity assessment tools (eg, ICAN), and technology-enhanced methods such as SMS or telephone support. Overall, the interventions aimed to improve outcomes such as readmission rates, treatment adherence, self-care behavior, caregiver competence, patient activation, and quality of life. Many studies reported positive effects on at least one health outcome, though some studies noted no significant differences between groups (Table 2).
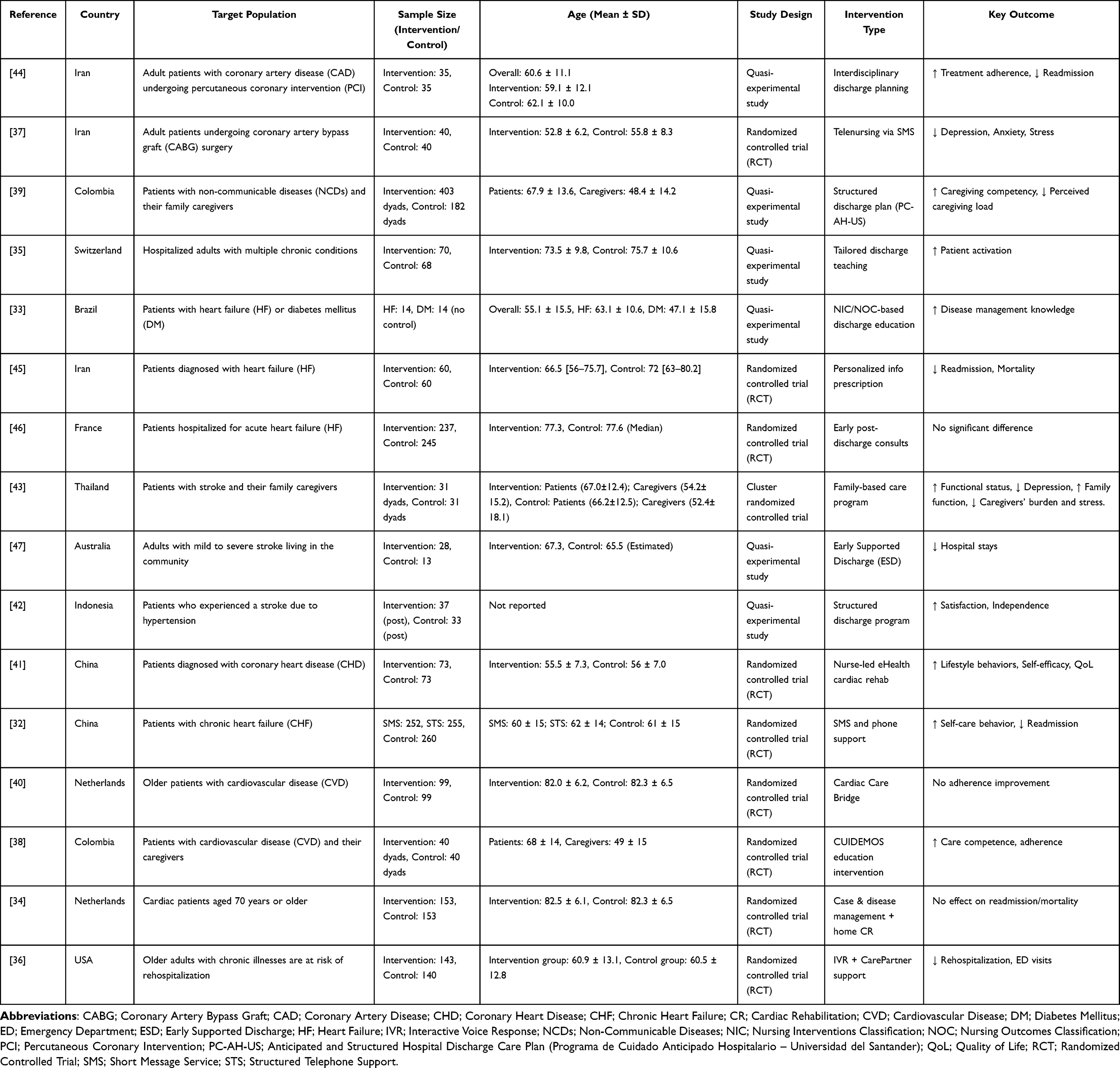 |
Table 2 Description of Included Studies |
Discharge Planning Model or Intervention
The included 16 studies employed diverse discharge planning and transitional care models, highlighting various approaches to support individuals with stroke and heart conditions after hospital discharge (Table 3). While the interventions differed in scope, intensity, and mode of delivery, most emphasized patient education, care continuity, and multidisciplinary collaboration. Several studies utilized interdisciplinary or team-based approaches. Rahpeima et al (2022) implemented a structured discharge model featuring in-person education, printed booklets, and 12-week telephone follow-ups.44 Similarly, Carvajal Carrascal et al (2024) employed the PC-AH-US model, a proactive, patient-family–centered plan initiated before discharge.39 Estrada et al (2024) used the CUIDEMOS program, which combined printed educational materials and structured phone support to enhance post-discharge adherence.38
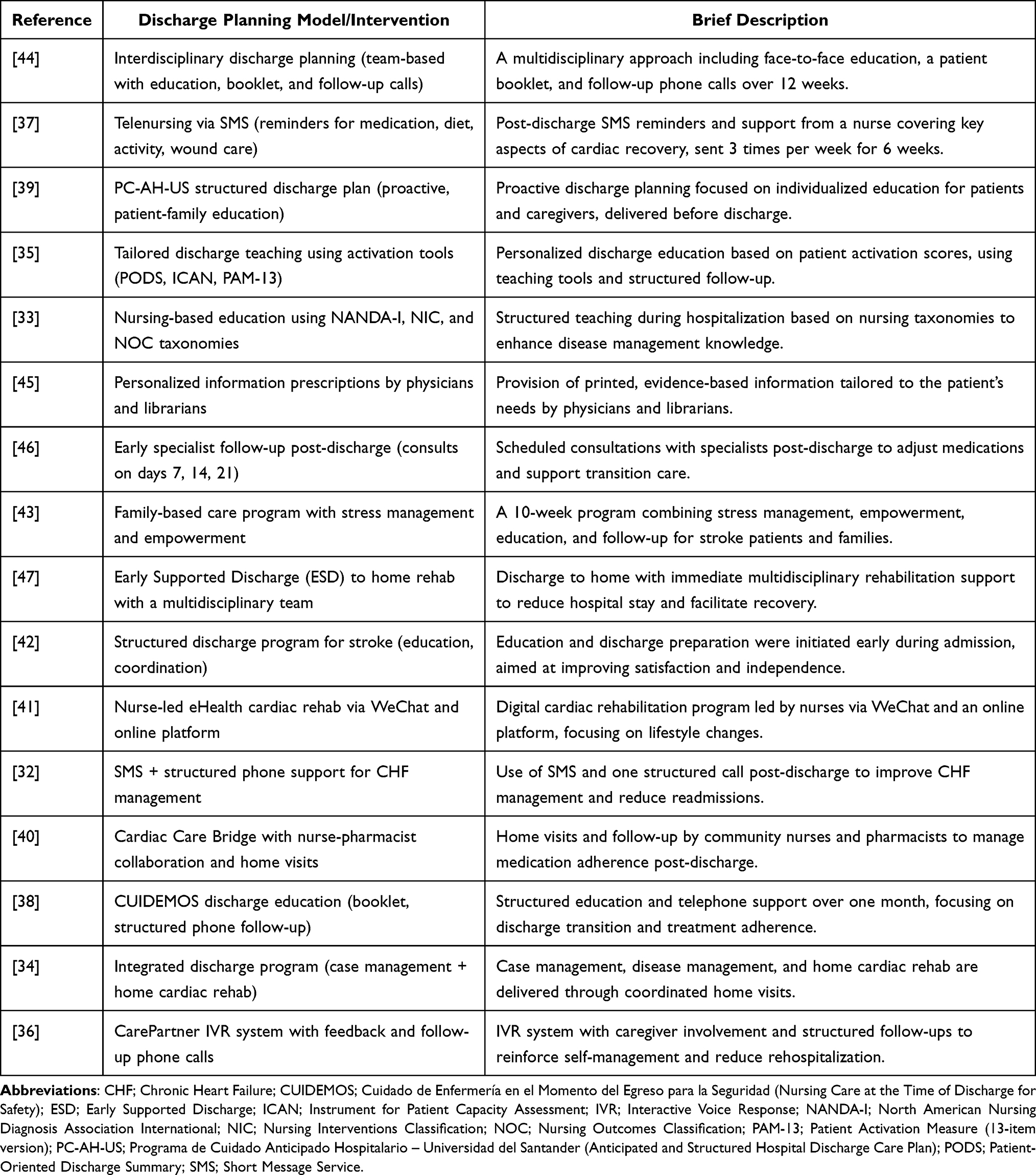 |
Table 3 Discharge Planning Models and Descriptions |
Technology-enhanced strategies were also prominent. Bikmoradi et al (2023) introduced SMS-based telenursing to reinforce medication and lifestyle adherence.37 Piette et al (2021) utilized an IVR-based CarePartner system that involved caregivers and incorporated structured follow-up calls.36 Su and Yu (2021) conducted a nurse-led eHealth cardiac rehabilitation program via WeChat, focusing on education and behavioral support.41 Some models incorporated standardized assessment and teaching tools to personalize care. Pellet et al (2024) tailored discharge teaching using the Patient-Oriented Discharge Summary (PODS), the Instrument for Patient Capacity Assessment (ICAN), and the Patient Activation Measure (PAM-13).48 Lemos et al (2020) structured discharge education using nursing taxonomies—NANDA-I, NIC, and NOC—to enhance disease self-management.33
Comprehensive transitional care models were evident in other studies. Daliri et al (2022) described a nurse–pharmacist collaborative model known as the Cardiac Care Bridge, integrating hospital discharge, home visits, and medication monitoring.40 Jepma et al (2021) implemented an integrated discharge program combining case management and home-based cardiac rehabilitation.34 Deepradit et al (2023) offered a family-based care program incorporating stress management and empowerment strategies for stroke survivors and their families.43 Additional approaches included early specialist outpatient follow-ups (Logeart et al, 2022),46 a structured stroke discharge coordination model (Sedia et al, 2019),42 and discharge planning supported by personalized information prescriptions (Kazemi Majd et al, 2021).45 Chen et al (2019) evaluated a hybrid intervention comprising SMS and structured phone support for patients with chronic heart failure (CHF).32
Neale et al (2020) described the Early Supported Discharge (ESD) model, transitioning patients directly to home-based multidisciplinary rehabilitation to reduce hospital stay duration.47 Overall, these discharge planning models collectively aimed to enhance patient readiness for discharge, improve health outcomes, reduce rehospitalization, and support self-management through coordinated, individualized, and often technology-facilitated strategies.
The Quality Appraisal of the Included Studies
A total of 11 randomized controlled trials (RCTs) were assessed using the RoB 2 tool, and five non-randomized studies of interventions (NRSIs) were evaluated using the ROBINS-I tool (Figure 2a and c). Among the RCTs, the majority were rated as having a low risk of bias across most domains. However, several studies, such as Su & Yu (2021), Chen et al (2019), Daliri et al (2022), and Estrada et al (2024) were judged to have some concerns primarily in the domains of deviations from intended interventions and measurement of outcomes. None of the RCTs were rated as having a high overall risk of bias, suggesting a generally robust methodological quality.
 |
Figure 2 Quality Assessment Assessed and Risk Bias. |
In contrast, the five quasi-experimental studies assessed using ROBINS-I showed more variability in methodological rigor. Three studies, Carvajal Carrascal et al (2023), Pellet et al (2023), and Neale et al (2020), were rated as having an overall moderate risk of bias, while Lemos et al (2020) and Sedia et al (2019) were judged to have a serious risk of bias. These ratings were largely influenced by issues related to confounding, participant selection, and measurement of outcomes, particularly in studies lacking randomization or blinded outcome assessment.
Bar charts and risk-of-bias visualizations (Figure 2b and d) further summarize domain-specific ratings for both RCTs and NRSIs. As shown, RCTs displayed higher methodological consistency, while NRSIs exhibited a broader range of risk, particularly in domains such as confounding control. All visualizations were produced using the robvis tool,49 an open-access R-based application that supports transparent reporting in evidence synthesis. We acknowledge the developers for facilitating reproducible and standardized quality assessment reporting.
The Effect of Discharge Planning in Individuals with Stroke and Heart Conditions
Six themes emerged from the included studies on the effects of discharge planning in individuals with stroke and heart conditions: (1) healthcare utilization and cost outcomes, (2) patient activation and health behavior change, (3) psychological well-being, (4) functional recovery, (5) health-related quality of life, and (6) caregiver outcomes and support. These themes highlight the broad impact of discharge planning across clinical, behavioral, and psychosocial domains. A summary of outcomes across these six domains is presented in Figure 3.
 |
Figure 3 Effects of Discharge Planning on Individuals with Stroke and Heart Conditions Across Six Outcome Domains. Note: ↑ indicates an increase or improvement in the outcome; ↓ indicates a decrease or reduction in the outcome. |
Although each theme is reported separately for clarity, the outcomes are interrelated and demonstrate synergy across domains. For instance, improvements in functional recovery often enhance health-related quality of life (HRQoL), while greater caregiver support can foster patient activation and adherence. Psychological well-being and self-efficacy also contribute to sustained engagement in health-promoting behaviors. Together, these interactions highlight how discharge planning interventions function synergistically to promote holistic recovery and continuity of care.
Healthcare Utilization and Cost Outcomes
Twelve studies reported healthcare utilization and cost-related outcomes following discharge planning interventions. The most frequently assessed indicators included hospital readmission (n = 8), mortality (n = 4), length of stay (n = 1), healthcare costs (n = 1), and patient satisfaction (n = 1). Approximately half of the studies demonstrated significant or favorable reductions in readmission rates among intervention groups implementing interdisciplinary, evidence-based discharge education and technology-integrated programs.32,36,44,45 Rahpeima et al (2022) reported no readmissions at three months among post-coronary angioplasty patients in the intervention group, compared with an 11.4% rate in controls.44 Kazemi Majd et al (2021) found significantly lower 12-month readmissions in heart failure patients receiving tailored discharge education (RR = 0.61; 95% CI: 0.40–0.93).45 Piette et al (2021) observed reduced 90-day rehospitalizations (20.8% vs 32.2%) and emergency visits using interactive voice response technology,36 and Chen et al (2019) reported lower 180-day readmission rates among patients receiving SMS reminders and structured phone support.32 Other studies implementing personalized education, specialist consultations, or nurse-led e-health rehabilitation found non-significant but favorable trends.34,36,41,46 Mortality outcomes were evaluated in four studies. One study found a lower mortality rate at six months (RR = 0.60, p = 0.46) and at 12 months (RR = 0.47, p = 0.05),45 whereas Logeart et al (2022) and Chen et al (2019) showed no statistically significant changes.32,46 Conversely, Jepma et al (2021) reported a higher 12-month mortality in the intervention group (RR = 1.44, p = 0.028), likely due to a frailer population with multiple comorbidities.34 Neale et al (2020) assessed length of stay and cost among stroke survivors in an Early Supported Discharge (ESD) program. The ESD group had significantly shorter stays in both acute wards (5 vs 6.2 days, p = 0.03) and rehabilitation units (9 vs 15 days, p < 0.001), with lower but non-significant treatment costs (p = 0.99).47 Sedia et al (2019) found significantly improved patient satisfaction following structured discharge planning, with higher scores for room services (p = 0.019) and overall satisfaction within the intervention group, though between-group differences were not statistically significant.42 Overall, these studies indicate that structured, technology-supported discharge planning can reduce healthcare utilization and improve patient experiences, although findings regarding mortality and cost remain mixed.
Patient Activation and Health Behavior Change
Six studies examined outcomes related to patient activation, disease management knowledge, treatment adherence, self-efficacy, and health-promoting lifestyle behaviors.32,33,35,40,41,44 Patient activation, defined as patients’ knowledge, skills, and confidence to manage their own health,35 showed improvement following discharge planning interventions. A quasi-experimental study among patients with multimorbidity reported significantly higher activation scores at 7–10 days post-discharge in the tailored discharge teaching group (p = 0.05).35 Similarly, another quasi-experimental study among patients with heart failure or diabetes found significant gains in disease-specific knowledge for both conditions (p = 0.002 and p < 0.001, respectively).33
Two studies reported on treatment adherence.40,44 In a quasi-experimental study among coronary artery disease patients, interdisciplinary discharge planning significantly improved adherence compared with usual care (p < 0.001).44 Conversely, a single-blind multicenter RCT evaluating the Cardiac Care Bridge intervention found no significant effect on adherence, though post-hoc analysis suggested a modest benefit among participants not using multidose drug dispensing systems (pinteraction = 0.085).40
Self-efficacy outcomes were reported in a single-blind RCT, which found significant improvement at 12 weeks post-intervention compared with controls (p = 0.005).41 Two studies assessed health-promoting lifestyle behaviors.32,41 One RCT among coronary heart disease patients found significant increases in daily steps, weekly activity minutes, and overall lifestyle profile at both 6 and 12 weeks post-intervention (p < 0.05 for all comparisons).41 Another non-blinded RCT among patients with chronic heart failure reported significant improvement in self-care behaviors, including medication compliance (p = 0.011) and water restriction adherence (p = 0.013), in the intervention group receiving educational and reminder messages.32 Collectively, these findings suggest that structured and tailored discharge planning enhances patient activation, knowledge, and self-care behaviors, although results for treatment adherence remain mixed across studies.
Psychological Well-Being
Two included studies reported positive effects on psychological outcomes.37,43 For instance, Bikmoradi et al (2023) examined the effects of a discharge intervention using telenursing combined with SMS follow-up in 40 adult patients diagnosed with coronary artery disease (CAD) who had undergone coronary artery bypass graft (CABG) surgery. The study found that telenursing-based discharge care significantly reduced levels of stress (p < 0.001), anxiety (p = 0.002), and depression (p = 0.04).37 Similarly, Deepradi et al (2023) investigated the effects of a family-based program in 31 stroke patient-caregiver dyads in Thailand. The program was implemented over a 10-week period following hospital discharge. The results demonstrated a reduction in depression levels among participants who received the intervention (p < 0.05).43
Functional Recovery
There are three studies that support the theme of functional recovery.41–43 Outcomes that were discovered for stroke patients include the functional outcome43 and patient independence42 and those for congenital heart disease patients include the number of steps patients take per day.41 All three studies showed improvement of their respective outcomes in each study. Deepradit et al (2023) implemented a family-based discharge program among stroke patients and their families and found statistically significant improvements in the patients’ functional status compared to the control group (p < 0.05).43 Although three patients in the intervention group experienced complications compared to the seven from the control group. Sedia et al (2019) implemented a structured interdisciplinary discharge program among stroke patients due to hypertension and found that patient independence scores significantly increased after the intervention (p < 0.05).42 Su & Yu (2021) implemented a disease management program for CHD patients and found significant improvements in the number of steps patients take per day for the intervention group, at six weeks post-intervention (p = 0.022) and at twelve weeks post-intervention (p = 0.006).41
Health-Related Quality of Life
Health-related quality of life (HRQoL) is one of the health indicators that evaluate the effectiveness of care programs, offering a comprehensive assessment across multiple dimensions, including physical, psychological, and psychosocial well-being. There were two studies that examined the impact of discharge planning on HRQoL.32,41 Su and Yu (2021) reported that a nurse-led e-health cardiac rehabilitation (NeCR) program, combining online education, telemonitoring, and remote support to promote recovery and self-management in post–cardiac surgery patients, significantly improved HRQoL at 84 days post-intervention (p < 0.05).41 In contrast, Chen et al (2019) evaluated a post-discharge short message service (SMS) program for heart failure patients, which provided regular reminders, education, and motivational messages to reinforce self-care behaviors, and found no significant HRQoL differences among groups at the 180-day follow-up, as measured by the Minnesota Living with Heart Failure Questionnaire (MLHFQ).32
Caregiver Outcomes and Support
Three discharge planning programs have been shown to enhance caregiver capacity and reduce caregiver burden.38,39,43 Deepradit et al (2023) developed a discharge model based on a family-based program that simultaneously promoted patient discharge and caregiver support.43 The 10-week intervention resulted in improved family function and a reduction in caregivers’ burden and stress (p < 0.05). These findings are consistent with Carvajal Carrascal et al (2023) study examining the effects of a tailored discharge planning program (PC-AH-US) on caregiving load.39 The results demonstrated an increase in caregiving competencies and a reduction in perceived caregiving burden (p < 0.001 for all dimensions). Similarly, Estrada et al (2024) conducted a study in Colombia among 80 patient–caregiver dyads of individuals with hypertension and/or diabetes mellitus, finding a significant increase in caregiving competence among dyads (p < 0.001).38
Across themes, technology-enhanced discharge planning interventions, including SMS reminders, interactive voice response systems, telemonitoring, and nurse-led digital platforms, emerged as a consistent trend supporting improved continuity of care and patient engagement. These digital approaches demonstrate growing potential to complement traditional multidisciplinary strategies and extend the reach of discharge planning beyond hospital settings.
Discussion
This systematic review synthesized evidence from 16 studies, including randomized controlled trials and quasi-experimental designs, to evaluate the effectiveness of discharge planning interventions among individuals with stroke and heart conditions. The findings reveal consistent benefits across multiple domains, including healthcare utilization, treatment adherence, psychological well-being, functional recovery, health-related quality of life, and caregiver outcomes. These results underscore the critical role of structured discharge planning as a key component of transitional care for populations at high risk of poor outcomes after hospital discharge. The most consistently reported benefit of discharge planning interventions was the reduction in hospital readmissions. Several studies demonstrated significant improvements, particularly when interventions incorporated structured education, interdisciplinary collaboration, or technology-enabled follow-up. These findings align with previous studies showing that comprehensive discharge planning reduces unplanned readmissions and supports care continuity.50–52 However, not all studies demonstrated statistically significant reductions, suggesting that intervention fidelity, patient characteristics, and health system capacity may influence effectiveness.53,54 Mortality outcomes were mixed; while some studies suggested reductions, others reported no significant change or even increased mortality among frail subgroups, indicating that patient selection and clinical complexity remain critical considerations. Six included studies reported improvements in treatment adherence, disease knowledge, self-care, and patient activation. Tailored education and structured discharge teaching interventions appeared especially effective in empowering patients to engage in self-management behaviors.55,56 The positive outcomes reflect the importance of patient-centered strategies that promote activation and confidence in managing chronic illness. However, the inconsistency observed in some trials suggests that sustained engagement, reinforcement, and integration of digital support tools may be necessary to maintain behavioral improvements over time. Our review found that discharge interventions that incorporated psychosocial support demonstrated significant reductions in depression, anxiety, and stress. These findings highlight the potential of discharge planning not only to address clinical and functional needs but also to support psychological recovery. The integration of family-based approaches and nurse-led follow-up was particularly effective in reducing psychological burden, consistent with evidence that caregiver engagement and emotional support are central to recovery in stroke and cardiac populations.57,58
Several included studies demonstrated improvements in independence, mobility, and functional status following structured or family-based discharge interventions. Early supported discharge models were effective in shortening hospital stays while maintaining or improving functional recovery.59 These results reinforce the value of timely, coordinated transitions that facilitate rehabilitation in the home and community setting. Functional recovery benefits appear especially relevant in stroke patients, where independence and daily living ability are critical to long-term outcomes.
Evidence regarding health-related quality of life (HRQoL) was mixed. While nurse-led eHealth cardiac rehabilitation significantly improved HRQoL, other interventions, such as SMS-based reminders, showed no measurable effect. These differences may reflect variations in intervention intensity, follow-up duration, and outcome measures. Overall, the findings suggest that discharge planning interventions that incorporate ongoing engagement, personalized feedback, and digital monitoring are indeed more effective in improving broader quality-of-life outcomes compared to education alone. These comprehensive approaches address multiple facets of patient care, leading to better preparedness, reduced readmissions, and enhanced overall patient satisfaction and quality of life.60–62
Three included studies highlighted significant improvements in caregiver competence and reductions in burden following structured, family-based, or dyadic discharge interventions. These findings underscore the importance of involving caregivers as active partners in transitional care. Given their critical role in supporting adherence, monitoring symptoms, and providing emotional support, discharge planning should be designed as a dyadic process that addresses the needs of both patients and caregivers. Adopting a multidisciplinary, individualized, and supportive approach can enhance satisfaction, reduce readmissions, and improve overall health outcomes for both patients and caregivers.63,64
Collectively, our findings support the integration of structured, multidisciplinary, and nurse-led discharge planning into standard care pathways for stroke and heart disease patients. The effectiveness of technology-enhanced interventions, such as SMS, interactive voice response, and eHealth platforms, suggests that digital tools can extend the reach of discharge planning, particularly in resource-constrained settings. Policymakers should prioritize investment in discharge planning models that promote continuity of care, caregiver engagement, and patient activation, with adaptations for local health system capacities.
Limitations
This systematic review has a number of limitations that warrant consideration. First, the included studies were heterogeneous in terms of populations, intervention components, delivery platforms, and outcome measures, which limited the ability to conduct a meta-analysis and precluded firm conclusions regarding the relative effectiveness of specific models. Second, although the methodological quality of the randomized controlled trials was generally robust, the quasi-experimental studies demonstrated variable rigor, with several rated as having moderate to serious risk of bias, particularly due to confounding and outcome measurement issues. Third, most included studies were conducted in middle- or high-income countries, which may limit the generalizability of findings to resource-constrained settings where discharge planning practices and health system infrastructures differ significantly. Fourth, the follow-up periods varied considerably, with several interventions evaluated only in the short term, making it difficult to assess the sustainability of benefits over time. Finally, the restriction to English-language publications may have introduced language bias.
Practical Applications and Future Research Directions
The findings of this systematic review highlight several practical applications for healthcare professionals and policymakers. First, implementing structured and multidisciplinary discharge planning as a standard practice can enhance continuity of care and reduce hospital readmissions among individuals with stroke and heart conditions. Integrating digital health technologies, such as telemonitoring, SMS reminders, and electronic care coordination platforms, can further strengthen patient engagement, improve self-management, and support timely clinical follow-up. In addition, involving family caregivers in discharge planning can optimize patient recovery, reduce caregiver burden, and improve long-term outcomes.
Future research should build on these findings by conducting longitudinal studies to assess the sustainability of intervention effects and the long-term impact on mortality, healthcare utilization, and quality of life. Studies examining cost-effectiveness and scalability of digital and nurse-led discharge interventions, particularly in low- and middle-income countries, are also needed. Moreover, comparative effectiveness research across diverse care settings could help identify context-specific strategies that enhance transitional care outcomes.
Conclusion
This systematic review synthesized evidence from 16 randomized controlled trials and quasi-experimental studies evaluating the effectiveness of discharge planning interventions for individuals with stroke and heart conditions. The findings indicate that discharge planning contributes to reduced readmissions and emergency visits, enhanced treatment adherence and self-care, improved psychological well-being and functional recovery, and increased caregiver competence and satisfaction. However, evidence regarding mortality and long-term outcomes remains mixed.
Overall, the review highlights that well-structured and multidisciplinary discharge interventions are effective in facilitating care transitions and improving patient-centered outcomes. Notably, nurse-led approaches, digital health solutions, and family involvement further enhance the impact of these interventions. These results underscore the importance of integrating discharge planning as a standard component of post-acute care for stroke and heart disease patients. Policymakers and healthcare organizations are encouraged to adopt and scale evidence-based discharge models to strengthen continuity of care, reduce healthcare utilization, and improve quality of life. Future research should explore long-term outcomes, cost-effectiveness, and implementation scalability, particularly in low- and middle-income countries.
Data Sharing Statement
The data generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Funding
No funding support was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Di Cesare M, Perel P, Taylor S, et al. The heart of the world. Global Heart. 2024;19(1):11. doi:10.5334/gh.1288
2. Heart G. Circulatory Diseases Factsheet. British Heart Foundation; 2023:1–12.
3. Taylor RS, Dalal HM, McDonagh STJ. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol. 2022;19(3):180–194. doi:10.1038/s41569-021-00611-7
4. Clinic M. Stroke rehabilitation: what to expect as you recover Mayo Clinic; 2024. Available from: https://www.mayoclinic.org/diseases-conditions/stroke/in-depth/stroke-rehabilitation/art-20045172.
5. Omonaiye O, Ward-Stockham K, Darzins P, et al. Hospital discharge processes: insights from patients, caregivers, and staff in an Australian healthcare setting. PLoS One. 2024;19(9):e0308042. doi:10.1371/journal.pone.0308042
6. Patel PR, Bechmann S. Discharge planning; 2020.
7. Hesselink G, Zegers M, Vernooij-Dassen M, et al. Improving patient discharge and reducing hospital readmissions by using intervention mapping. BMC Health Serv Res. 2014;14:1–11. doi:10.1186/1472-6963-14-389
8. Dawes J, Lin AY, Varghese C, Russell MM, Lin AY. Mobile health technology for remote home monitoring after surgery: a meta-analysis. Br J Surg. 2021;108(11):1304–1314. doi:10.1093/bjs/znab323
9. Simon P. Medical home telemonitoring of chronically ill patients. 1) lessons learnt from large international studies. Eur Res Telemed. 2014;3(2):85–93. doi:10.1016/j.eurtel.2014.04.004
10. Kim SK, Jo HS, Park Y, Yim I. Efficacy of transitional care services for patients with stroke: systematic review and meta-analysis. Nurs Res. 2025;74:484–496. doi:10.1097/NNR.0000000000000858
11. Jiang N, Xv Y, Sun X, Feng L, Wang YB, Jiang XL. Study on self-management of real-time and individualized support in stroke patients based on resilience: a protocol for a randomized controlled trial. Trials. 2023;24(1). doi:10.1186/s13063-023-07475-x
12. Saharan P, Rao VS. Evaluating the effectiveness of digital health interventions on reducing hospital readmissions in heart failure patients. J Neonatal Surg. 2025;14(1):345–349. doi:10.52783/jns.v14.1545
13. Qi K, Koike T, Yasuda Y, Tayama S, Wati I. The effects on rehospitalization rate of transitional care using information communication technology in patients with heart failure: a scoping review. Int J Nurs Studies Adv. 2023;5.
14. Haverfield MC, De Leon G, Johnson A, Jackson VL, Basu G, Dodge J. Transforming the discharge conversation through support and structure: a scoping review. Int J Nurs Studies Adv. 2024;6:100203. doi:10.1016/j.ijnsa.2024.100203
15. Lin C-J, Cheng S-J, Shih S-C, Chu C-H, Tjung -J-J. Discharge planning. Int J Gerontol. 2012;6(4):237–240. doi:10.1016/j.ijge.2012.05.001
16. Pourliaka T, Tsiakiri A, Proios H. Exploring discharge preparedness of patients with stroke: a qualitative descriptive study. Creative Nurs. 2025;10784535251320005.
17. Indiartinie AT, Setiyowati E, Septianingrum Y, et al. The importance of discharge planning in stroke patients: literature review. J Nurs Pract. 2023;6(2):130–136. doi:10.30994/jnp.v6i2.301
18. Rusmawati A, Fawzi A, Faizah NH. The effectiveness of discharge planning implementation on the quality of life of post opname patients with heart failure at hospital. J Nurs Practice. 2024;7(2):417–426. doi:10.30994/jnp.v7i2.593
19. Kongkar R, Ruksakulpiwat S, Phianhasin L, et al. The impact of interdisciplinary team-based care on the care and outcomes of chronically ill patients: a systematic review. J Multidiscip Healthcare. 2025;8:445–457. doi:10.2147/JMDH.S497846
20. Brown CL, Tittlemier BJ, Tiwari KK, Loewen H. Interprofessional teams supporting care transitions from hospital to community: a scoping review. Int J Integrat Care. 2024;24(2):1. doi:10.5334/ijic.7623
21. Zanetoni TC, Cucolo DF, Perroca MG. Interprofessional actions in responsible discharge: contributions to transition and continuity of care. Revista da Escola de Enfermagem da U S P. 2023;57:e20220452. doi:10.1590/1980-220X-REEUSP-2022-0452en
22. Po HW, Chu YC, Tsai HC, Lin CL, Chen CY, Ma MH. Efficacy of remote health monitoring in reducing hospital readmissions among high-risk postdischarge patients: prospective cohort study. JMIR Form Res. 2024;8:e53455. doi:10.2196/53455
23. Bennett DJ, Feng J, Goldman S, et al. Reducing readmissions in the safety net through AI and automation. Am J Manag Care. 2025;31(3):142–148. doi:10.37765/ajmc.2025.89697
24. Prevention S. Transition of care for acute stroke and myocardial infarction patients: from hospitalization to rehabilitation. Recovery. 2011.
25. Butler J, Petrie MC, Bains M, et al. Challenges and opportunities for increasing patient involvement in heart failure self-care programs and self-care in the post–hospital discharge period. Res Involve Engage. 2023;9(1):23. doi:10.1186/s40900-023-00412-x
26. Veronese M, Vellone E, Alvaro R, Pucciarelli G. The transitional care from hospital to home for stroke survivors and their caregivers: a systematic review. J Vasc Nurs. 2025;43:86–98. doi:10.1016/j.jvn.2025.03.002
27. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;
28. Higgins JP, Savović J, Page MJ, Elbers RG, Sterne JA. Assessing risk of bias in a randomized trial. Cochrane Handbook Syst Rev Intervent. 2019;205–228.
29. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355.
30. JBI manual for evidence synthesis [Internet]. JBI; 2024. Available from: https://synthesismanual.jbi.global.
31. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. doi:10.1016/j.ijsu.2021.105906
32. Chen C, Li X, Sun L, et al. Post-discharge short message service improves short-term clinical outcome and self-care behaviour in chronic heart failure. ESC Heart Failure. 2019;6(1):164–173. doi:10.1002/ehf2.12380
33. Lemos DMP, Saldanha PF, Vieira LF, Azzolin KO. Nursing taxonomies in hospital discharge planning: a quasi-experimental study. Revista brasileira de enfermagem. 2020;73(5):e20180896. doi:10.1590/0034-7167-2018-0896
34. Jepma P, Verweij L, Buurman BM, et al. The nurse-coordinated cardiac care bridge transitional care programme: a randomised clinical trial. Age Ageing. 2021;50(6):2105–2115. doi:10.1093/ageing/afab146
35. Pellet J, Weiss M, Zúniga F, Mabire C. Improving patient activation with a tailored nursing discharge teaching intervention for multimorbid inpatients: a quasi-experimental study. Patient Educ Couns. 2024;118:108024. doi:10.1016/j.pec.2023.108024
36. Piette JD, Striplin D, Aikens JE, et al. Impacts of post-hospitalization accessible health technology and caregiver support on 90-day acute care use and self-care assistance: a randomized clinical trial. Am J Med Qual. 2021;36(3):145–155. doi:10.1177/1062860620943673
37. Bikmoradi A, Omidvar S, Roshanaei G, Khatiban M, Harorani M. The impact of telenursing on level of depression, stress and anxiety in discharged patients after coronary artery bypass graft surgery: a randomized clinical trial. J Vasc Nurs. 2023;41(3):89–94. doi:10.1016/j.jvn.2023.05.003
38. Estrada YVR, Esteban ANP, Aldana MSC, et al. Efficacy of a hospital discharge transition plan in the care competence of patients with chronic conditions and their family caregivers: a clinical trial. Rev Lat Am Enfermagem. 2024;
39. Carvajal Carrascal G, Fuentes Ramírez A, Pulido Barragán SP, Guevara Lozano M, Sánchez-Herrera B. Effects of the discharge plan on the caregiving load of people with chronic disease: quasi-experimental study. Chronic Illness. 2023;20(4):712–723. doi:10.1177/17423953231192131
40. Daliri S, Kooij MJ, Scholte Op Reimer WJM, et al. Effects of a transitional care programme on medication adherence in an older cardiac population: a randomized clinical trial. Br J Clin Pharmacol. 2022;88(3):965–982. doi:10.1111/bcp.15044
41. Su JJ, Yu DS. Effects of a nurse-led eHealth cardiac rehabilitation programme on health outcomes of patients with coronary heart disease: a randomised controlled trial. Int J Nurs Stud. 2021;122:104040. doi:10.1016/j.ijnurstu.2021.104040
42. Sedia S, Hamid A, Mustikasari M, Besral B. The effectiveness of discharge planning stroke patient due to hypertension to improve patient satisfaction and Independence. Enfermería Clínica. 2019;29(Suppl 2).
43. Deepradit S, Powwattana A, Lagampan S, Thiangtham W. Effectiveness of a family-based program for post-stroke patients and families: a cluster randomized controlled trial. Int J Nurs Sci. 2023;10(4):446–455. doi:10.1016/j.ijnss.2023.09.020
44. Rahpeima E, Bijani M, Karimi S, Alkamel A, Dehghan A. Effect of the implementation of interdisciplinary discharge planning on treatment adherence and readmission in patients undergoing coronary artery angioplasty. Investigación y educación en enfermería. 2022;40(2). doi:10.17533/udea.iee.v40n2e08
45. Kazemi Majd F, Gavgani VZ, Golmohammadi A, Jafari-Khounigh A. Effect of physician prescribed information on hospital readmission and death after discharge among patients with health failure: a randomized controlled trial. Health Informatics J. 2021;27(1):1460458221996409. doi:10.1177/1460458221996409
46. Logeart D, Berthelot E, Bihry N, et al. Early and short-term intensive management after discharge for patients hospitalized with acute heart failure: a randomized study (ECAD-HF). Eur J Heart Fail. 2022;24(1):219–226. doi:10.1002/ejhf.2357
47. Neale S, Leach K, Steinfort S, Hitch D. Costs and length of stay associated with early supported discharge for moderate and severe stroke survivors. J Stroke Cerebrovascular Dis. 2020;29(8):104996. doi:10.1016/j.jstrokecerebrovasdis.2020.104996
48. Pellet J, Weiss M, Zúñiga F, Mabire C. Improving patient activation with a tailored nursing discharge teaching intervention for multimorbid inpatients: a quasi-experimental study. Patient Educ Couns. 2024;118:108024.
49. McGuinness LA, Higgins JPT. Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res Synthesis Methods. 2020;12:55–61. doi:10.1002/jrsm.1411
50. Verhaegh KJ, Buurman BM, Veenboer GC, de Rooij SE, Geerlings SE. The implementation of a comprehensive discharge bundle to improve the discharge process: a quasi-experimental study. Netherlands J Med. 2014;72(6):318–325.
51. Phillips CO, Wright SM, Kern DE, Singa RM, Shepperd S, Rubin HR. Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta-analysis. JAMA. 2004;291(11):1358–1367. doi:10.1001/jama.291.11.1358
52. Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day postdischarge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hospital Med. 2009;4(4):211–218. doi:10.1002/jhm.427
53. Shepperd S, McClaran J, Phillips CO, et al. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2010;(1):CD000313. doi:10.1002/14651858.CD000313.pub3
54. Gonçalves-Bradley DC, Lannin NA, Clemson LM, Cameron ID, Shepperd S. Discharge planning from hospital. Cochrane Database Syst Rev. 2016;2016(1).
55. St JIJ, Englund HM. Improving patient discharge education through daily educational bursts: a pilot study. J Nurses Professional Develop. 2020;36(5):283–287. doi:10.1097/NND.0000000000000627
56. Chen HM, Wang ST, Wu SJ, Lee CS, Fetzer SJ, Tsai LM. Effects of predischarge patient education combined with postdischarge follow-ups on self-care, readmission, sleep, and depression in patients with heart failure. J Nurs Res. 2020;28(5):e112. doi:10.1097/JNR.0000000000000395
57. Verberne DPJ, Kroese MEAL, Staals J, Ponds RWHM, van Heugten CM. Nurse-led stroke aftercare addressing long-term psychosocial outcome: a comparison to care-as-usual. Disability Rehabil. 2022;44(12):2849–2857. doi:10.1080/09638288.2020.1849417
58. Elsheikh MA, Moriyama M, Rahman MM, et al. Effect of a tailored multidimensional intervention on the care burden among family caregivers of stroke survivors: study protocol for a randomised controlled trial. BMJ Open. 2020;10(12):e041637. doi:10.1136/bmjopen-2020-041637
59. Williams S, O’Riordan C, Morrissey AM, Galvin R, Griffin A. Early supported discharge for older adults admitted to hospital after orthopaedic surgery: a systematic review and meta-analysis. BMC Geriatr. 2024;24(1). doi:10.1186/s12877-024-04775-y
60. OuYang J, Li J, Wang B, Wu J, Chen J, Zheng X. The effects of a nurse-led HAPA-based discharge planning on post-operative outcomes in urolithiasis patients with double-J stents: protocol for a randomized controlled trial. Ann Med. 2025;57(1). doi:10.1080/07853890.2025.2519676
61. Keniston A, McBeth L, Pell J, et al. Development and implementation of a multidisciplinary electronic discharge readiness tool: user-centered design approach. JMIR Human Factors. 2021;8(2):e24038. doi:10.2196/24038
62. Fuller TE, Pong DD, Piniella N, et al. Interactive digital health tools to engage patients and caregivers in discharge preparation: implementation study. J Med Internet Res. 2020;22(4):e15573. doi:10.2196/15573
63. Gray J, Lyerly M. Discharge Planning. Stroke for the Advanced Practice Clinician: A Clinically Focused Guide for Acute, Inpatient, and Outpatient Care. Springer Nature; 2024:377–382.
64. Cadel L, Sandercock J, Marcinow M, Guilcher SJT, Kuluski K. A qualitative study exploring hospital-based team dynamics in discharge planning for patients experiencing delayed care transitions in Ontario, Canada. BMC Health Serv Res. 2022;22(1). doi:10.1186/s12913-022-08807-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
Effect of Exercise Interventions on Health-Related Quality of Life in Patients with Fibromyalgia Syndrome: A Systematic Review and Network Meta-Analysis
Zhang KD, Wang LY, Zhang ZH, Zhang DX, Lin XW, Meng T, Qi F
Journal of Pain Research 2022, 15:3639-3656
Published Date: 22 November 2022
The Burden of Sickle Cell Disease in Saudi Arabia: A Single-Institution Large Retrospective Study
Bin Zuair A, Aldossari S, Alhumaidi R, Alrabiah M, Alshabanat A
International Journal of General Medicine 2023, 16:161-171
Published Date: 13 January 2023
The Correlation Between Caregivers Burden and Quality of Life Among Family Caregivers of Stroke Survivors: The Mediating Role of Resilience
Handayani F, Kusumaningrum NSD, Dwidiyanti M
Nursing: Research and Reviews 2024, 14:91-102
Published Date: 19 June 2024
Factor Impacting Quality of Life Among Sepsis Survivors During and After Hospitalization: A Systematic Review of Current Empirical Evidence
Pongsuwun K, Puwarawuttipanit W, Nguantad S, Samart B, Saikaew K, Ruksakulpiwat S
Journal of Multidisciplinary Healthcare 2024, 17:3791-3802
Published Date: 6 August 2024