Back to Journals » Drug Design, Development and Therapy » Volume 20
Effect of Oliceridine on the Acute Postoperative Pain Management After Elective Cesarean Delivery: A Randomized Non-Inferiority Trial
Authors Jiang J, Yuan G, Shi Y, Zhou Z, Wang X, Sang X ![]() , Zhang X
, Zhang X ![]()
Received 13 February 2026
Accepted for publication 8 July 2026
Published 14 July 2026 Volume 2026:20 603352
DOI https://doi.org/10.2147/DDDT.S603352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas Panos
Jing Jiang,1,* Guanghua Yuan,1,* Yuhui Shi,1,* Zhou Zhou,1 Xinxin Wang,1 Xiaoqiao Sang,1 Xiaobao Zhang1,2
1Department of Anesthesiology, The Affiliated Lianyungang Hospital of Xuzhou Medical University, Lianyungang, Jiangsu, People’s Republic of China; 2The First Affiliated Hospital of Kangda College of Nanjing Medical University, Lianyungang, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaobao Zhang, Department of Anesthesiology, The Affiliated Lianyungang Hospital of Xuzhou Medical University, No. 6 Zhenhua East Road, Lianyungang, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: Effective postoperative analgesia following cesarean delivery is crucial for maternal recovery. Sufentanil, commonly administered via patient-controlled intravenous analgesia (PCIA), is associated with dose-dependent adverse effects, particularly gastrointestinal disturbances. Oliceridine, a novel G protein-biased μ-opioid receptor agonist, offers the dual advantage of potent analgesia and a reduced risk of opioid-related adverse events. This study aimed to compare the analgesic efficacy and the incidence of side effects between the G protein-biased μ-opioid receptor agonist oliceridine and the conventional opioid sufentanil.
Patients and Methods: In this single-center, randomized, double-blind, non-inferiority trial, women undergoing elective cesarean delivery under combined spinal-epidural anesthesia (CSEA) were randomly assigned to receive either oliceridine or sufentanil via patient-controlled intravenous analgesia (PCIA) for 48 hours postoperatively. The primary outcome was the sum of pain intensity differences over 48 hours (SPID48), calculated from resting Numerical Rating Scale (NRS) scores (0– 10) assessed at 0, 12, 24, 36, and 48 hours postoperatively. Secondary outcomes included the sum of pain intensity differences at 12 h, 24 h, and 36 h, total PCIA demand, rescue analgesia utilization, time to first lactation, maternal satisfaction, and incidence of adverse events.
Results: 160 participants were included in the final analysis. The primary outcome, SPID48, showed an adjusted mean of 172.50 (95% CI, 163.37– 181.63) in the oliceridine group and 147.90 (95% CI, 137.59– 158.21) in the sufentanil group (mean difference 24.60; 95% CI, 10.83– 38.37). The lower limit of the 95% CI for the difference exceeded the pre-specified non-inferiority margin of − 20, establishing non-inferiority of oliceridine.
Conclusion: Oliceridine provides non-inferior postoperative analgesic efficacy compared with sufentanil in women undergoing cesarean delivery. Exploratory observations suggested a lower incidence of nausea and higher patient satisfaction in the oliceridine group; these findings are hypothesis-generating and require further validation.
Keywords: oliceridine, sufentanil, postoperative analgesia, patient-controlled intravenous analgesia, lactation
Introduction
Cesarean delivery ranks among the most frequently performed surgical procedures globally.1 Effective management of acute postoperative pain extends beyond patient comfort, constituting a critical element of Enhanced Recovery After Surgery (ERAS) protocols.2 Inadequate pain control can impede early ambulation, hinder mother-infant bonding, disrupt the establishment of breastfeeding, and potentially contribute to the development of chronic postsurgical pain.3
Neuraxial opioid analgesia, particularly intrathecal morphine, represents the gold standard for post-cesarean analgesia due to its prolonged duration of action.4 However, their application is often supplemented or replaced by intravenous modalities, especially in settings where neuraxial opioids are unavailable or contraindicated. Sufentanil, a potent μ-opioid receptor agonist, is extensively utilized in PCIA.5,6 While effective, its use, like other traditional opioids, is limited by a well-documented constellation of dose-dependent adverse effects, including nausea, vomiting, pruritus, respiratory depression, and sedation, which collectively diminish patient satisfaction and delay recovery.5,7 The underlying mechanism for these undesirable effects is linked to the non-selective activation of both G protein and β-arrestin-2 signaling pathways by conventional opioids.8,9
Oliceridine is a first-in-class G protein-biased μ-opioid receptor agonist. It was specifically engineered to preferentially activate the G protein signaling pathway, which mediates potent analgesia, while minimizing engagement of the β-arrestin-2 pathway, believed responsible for many typical opioid-related adverse effects, particularly respiratory depression and gastrointestinal dysfunction.9,10 Phase III clinical trials (APOLLO and ATHENA) demonstrated that oliceridine provides rapid and effective analgesia for moderate-to-severe acute pain with a lower incidence of nausea, vomiting, and hypoxia compared to morphine.11 In recent years, multiple clinical studies have confirmed the efficacy and safety of oliceridine in patient-controlled intravenous analgesia (PCIA) after laparoscopic colorectal cancer radical resection, total hysterectomy, and thoracoscopic lung resection, demonstrating analgesic effects comparable to those of morphine or sufentanil, and featuring a more favorable adverse reaction profile.12–14
Despite this promising profile, robust clinical data on oliceridine use in the specific population of postpartum women undergoing cesarean delivery remains scarce. This population presents unique considerations, including implications of opioid use on maternal recovery, breastfeeding initiation, and neonatal well-being.15 Therefore, we conducted this prospective, randomized, double-blind, non-inferiority trial to test the hypothesis that oliceridine is non-inferior to sufentanil for PCIA after cesarean delivery in terms of analgesic efficacy, with a significantly improved safety and tolerability profile.
Materials and Methods
Ethics Statement
This was a single-center, prospective, randomized, double-blind, non-inferiority clinical trial conducted at a tertiary care hospital. The study protocol was approved by the Institutional Review Board of the Affiliated Lianyungang Hospital of Xuzhou Medical University. (Ethic Approval No: [KY-20240801002-02]) and registered with the Chinese Clinical Trials Registry (ChiCTR2500100326). Written informed consent was obtained from all participants prior to any study-related procedures.
Study Design and Randomization
The study flowchart (Figure 1) illustrates the screening, randomization, and analysis procedures. The trial was conducted in the Department of Anesthesiology, The Affiliated Lianyungang Hospital of Xuzhou Medical University, from May 2025 and November 2025. Eligible patients were randomly assigned in a 1:1 ratio to either the oliceridine group or the sufentanil group. A computer-generated block randomization sequence was created by an independent statistician. The allocation sequence was concealed from investigators, anesthesiologists, nursing staff, and patients. Study medications were prepared by staff members not directly involved in the study, opaque PCIA bags containing a total volume of 100 mL, ensuring all parties involved in patient care and data collection remained blinded to group assignment.
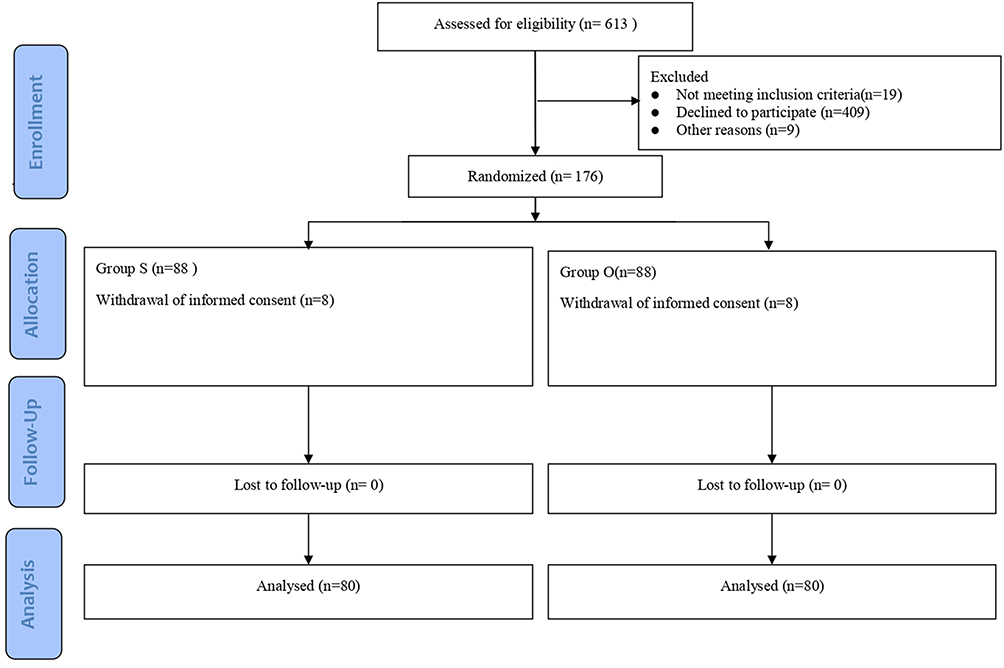 |
Figure 1 The CONSORT flow chart for the recruitment of patients. |
Inclusion and Exclusion Criteria
Inclusion Criteria Comprised
(1) Age 20–45 years; (2) Preoperative American Society of Anesthesiologists (ASA) Grade II to III; (3) Patients undergoing elective cesarean delivery under combined spinal-epidural anesthesia; (4) Subjects voluntarily participated in this study and signed informed consent.
Exclusion Criteria Included
(1) Known allergy to any medication used in the study protocol; (2) History of chronic pain or chronic use of sedative or analgesic medications; (3) History of psychiatric disorders or long-term use of psychotropic medications; (4) Presence of significant hepatic or renal dysfunction; (5) Severe obstetric complications, such as preeclampsia, placenta accreta spectrum, or HELLP syndrome; (6) Inability to comprehend or accurately express Numeric Rating Scale (NRS) pain scores; (7) Participation in any other clinical trial within the 3 months preceding this study.
Sample Size Calculation
Sample size calculation was based on SPID48 data from previous literature. Assuming a non-inferiority margin (δ) of −20, standard deviation of 45, 80% power, and one-sided alpha of 0.025, a minimum of 80 patients per group was required. Accounting for a potential 10% dropout rate, 176 patients were needed.
The non-inferiority margin (δ) of −20 for the primary endpoint SPID48 was determined based on both clinical and statistical considerations. Clinically, preserving at least 80% of the analgesic effect of the active control (sufentanil) was considered the minimum acceptable standard for postoperative pain management after cesarean delivery. Statistically, a previous study reported a mean SPID48 of 105 for sufentanil via PCIA.16 Retaining 80% of this effect yields a value of 84, corresponding to a permissible mean difference of −21 (84−105 = −21). For practical convenience and to adopt a conservative integer threshold, the margin was rounded to −20. This rounded value actually requires preserving approximately 81% of the sufentanil effect, which is slightly more stringent than the original 80% criterion. This margin was pre-specified in the protocol and used for sample size calculation and non-inferiority testing.
Anesthetic and Analgesic Management
To ensure high controllability of research variables and data comparability, a standardized perioperative anesthesia and analgesia management protocol was implemented for all participants, designed to minimize the impact of intraoperative variations on postoperative pain assessment.
Upon arrival in the operating room, intravenous access was established, followed by routine monitoring. CSEA was performed at the L3–L4 interspace using 2–2.5 mL of 0.5% bupivacaine to achieve a T4–T5 sensory block. The anesthesiologist provided 1.5% lidocaine 3–5 mL through the epidural catheter for women with inadequate sensory block. During the operation, a uterine contraction agent was administered as needed.
After the surgery, the NRS score was performed at 60 ± 5 min intervals. When the patient’s NRS score at rest was ≥4 points, a loading dose of the study medications was administered, with the initiation time of the loading dose recorded as 0 hours. The PCIA infusion was started after the loading dose. PCIA solutions were prepared by an independent pharmacist. Oliceridine group: 25 mg oliceridine diluted to 100 mL with 0.9% normal saline. Parameters: loading dose 1.5 mg (6 mL), bolus dose 0.35 mg (1.4 mL), lockout interval 6 minutes, no background infusion. Sufentanil Group: 100 μg sufentanil diluted to 100 mL with 0.9% normal saline. Parameters: loading dose 6 μg (6 mL), bolus dose 1.4 μg (1.4 mL), lockout interval 6 minutes, no background infusion. The dose selection was determined based on previous clinical studies and pharmacological equivalence analysis. According to the literature, the analgesic potency of oliceridine is approximately four times that of morphine,17 whereas sufentanil is approximately 1000 times as potent as morphine.18 Consequently, sufentanil is estimated to be about 250 times more potent than oliceridine. Based on equianalgesic dose conversion: 25 mg of oliceridine is equivalent to 100 mg of morphine (a 4-fold potency ratio), and the calculated equivalent dose of sufentanil is 100 μg (a 1000-fold potency ratio). Thus, the analgesic strength of 25 mg of oliceridine is comparable to that of 100 μg of sufentanil.
A standardized rescue analgesia protocol was established: after initiating PCA treatment, subjects may self-administer PCA pump pressure if experiencing pain. If the patient’s NRS score reaches or exceeds 4 at any time during treatment, rescue analgesia must be administered promptly—ideally within 15 minutes of pain assessment. The recommended rescue medication is acetaminophen, administered orally at a single dose of 500 mg. If the patient experiences severe nausea and vomiting after the operation, palonosetron is selected for rescue antiemesis. All adverse reactions were meticulously recorded.
Data Collection
Patient characteristics and medical history were recorded, including age, body mass index (BMI), gestational age, history of pain, surgical history, nausea/vomiting during pregnancy, surgery duration, supine hypotensive syndrome, and ASA classification. Professional anesthesia assessors conducted follow-up visits for all patients 12, 24, 36, and 48 hours after the analgesic pump was put into use. Their postoperative pain after cesarean delivery was assessed using the NRS scale.
Outcome Measures
The primary outcome was the Sum of Pain Intensity Differences over 48 hours (SPID48), calculated from resting NRS scores (0–10) assessed at 0, 12, 24, 36, and 48 hours postoperatively. Pain intensity difference (PID) at each time point was defined as the baseline NRS score at 0 hours minus the NRS score at the corresponding postoperative time point (ie, PID = NRS0−NRSt). Time-weighted SPID is the cumulative sum of the product of the PID at each time point multiplied by the time difference (the time difference is the current time point minus the previous time point). The following formula is used to calculate SPID: SPIDt = PIDt1*(t1 - 0) + PIDt2*(t2-t1) +…+ PIDtn*(tn - tn-1); SPIDt represents the time-weighted cumulative pain intensity difference of resting pain from the first postoperative medication to time point t, t is 12, 24, 36, 48 h, PIDtn represents the pain intensity difference at rest at the nth time, and tn is the actual time of the NRS measurement of resting pain score. SPID is an outcome that measures treatment effect over a specific time period. Higher values indicate greater pain relief.16
Secondary Outcomes Included
- The sum of pain intensity differences at 12 h, 24 h, and 36 h.
- Total PCIA demands, valid boluses delivered, total opioid consumption over 48 hours.
- Number of patients requiring rescue medication, time to first rescue request, number of rescue doses, total acetaminophen consumption.
- Time to first lactation, overall analgesia satisfaction at 48 h.
- Incidence of adverse events including nausea, vomiting, dizziness, constipation, pruritus, chest tightness, fever.
Statistical Analysis
Statistical analyses were performed using SPSS version 27.0. For continuous data, normality was assessed using the Shapiro–Wilk test, and homogeneity of variances was assessed using Levene’s test. For independent samples, normally distributed continuous data are presented as mean ± standard deviation, with between-group comparisons performed using Student’s t-test; non-normally distributed continuous data are presented as median (interquartile range) and analyzed using the Mann–Whitney U-test (Wilcoxon rank-sum test). For repeated-measures continuous data, repeated-measures analysis of variance (RM-ANOVA) was used if the data met the assumptions of normality, homogeneity of variance, and sphericity (where applicable); generalized estimating equations (GEE) were applied when these assumptions were not satisfied. Categorical data are presented as frequency (percentage), with between-group comparisons performed using the chi-square test or Fisher’s exact test.
The primary analysis was based on the full analysis set (FAS), defined as all randomized subjects who received at least one dose of study drug and provided at least one post-baseline pain Numerical Rating Scale (NRS) assessment. We screened for outliers using boxplots and the Z-score method (|Z|>3 considered an outlier). Missing data for the primary and secondary outcomes were handled using multiple imputation. All available data were retained in the analyses.
The non-inferiority conclusion was based on the full analysis set. For the summed pain intensity difference (SPID) at each time point, generalized estimating equations (GEE) were used, assuming an AR(1) working correlation matrix and adjusting for baseline NRS. Oliceridine was considered non-inferior to sufentanil if the lower limit of the two-sided 95% confidence interval (CI) for the GEE-adjusted mean difference in SPID48 was greater than the pre-specified non-inferiority margin of −20. The one-sided α was set at 0.025, corresponding to a two-sided 95% CI.
For comparisons of NRS at multiple time points among secondary endpoints, exploratory analyses using Bonferroni correction were performed; for the remaining secondary endpoints, only nominal P values are reported without multiplicity adjustment, and all results are considered exploratory.
This study was designed as a non-inferiority trial. If the lower limit of the 95% CI for the primary outcome exceeded the non-inferiority margin (−20) and the entire CI lay above zero, this would suggest a possible superiority signal; however, such an interpretation is hypothesis‑generating only, because the study was not powered for superiority. Any conclusion of superiority must be confirmed in a dedicated superiority trial.
Unless otherwise specified for multiplicity adjustment, a P value <0.05 was considered statistically significant. All tests were two-sided.
Results
Baseline Characteristics of Participants
A total of 613 patients were assessed for eligibility, Among them, 437 were excluded (19 did not meet the inclusion criteria, 409 declined to participate, and 9 were excluded due to other reasons). The remaining 176 patients were randomized at a 1:1 ratio to receive either oliceridine (n = 88) or sufentanil (n = 88). Prior to the initiation of the study intervention, 8 patients in each group withdrew their informed consent and did not receive any study medication. No patients were lost during the follow - up in either group.160 participants were included in the final analysis, with 80 participants in both the oliceridine group and the sufentanil group (Figure 1). The robust standardized mean difference (Robust SMD) was computed using the median and the normalized median absolute deviation (MADN = 1.4826 × MAD), providing a distribution-free effect size estimate suitable for non-normally distributed covariates. Balance was interpreted as follows: Robust SMD < 0.1 indicates excellent balance; 0.1 ≤ Robust SMD < 0.2 indicates acceptable balance; and Robust SMD ≥ 0.2 indicates substantial imbalance.
Baseline characteristics, including age, BMI, ASA classification, gestational age, history of pain, surgical history, supine hypotensive syndrome, and duration of surgery, were well balanced between the two groups (Robust SMD < 0.2 for all variables). Baseline resting pain scores (NRS0) showed no meaningful between-group difference (Robust SMD < 0.2) (Table 1).
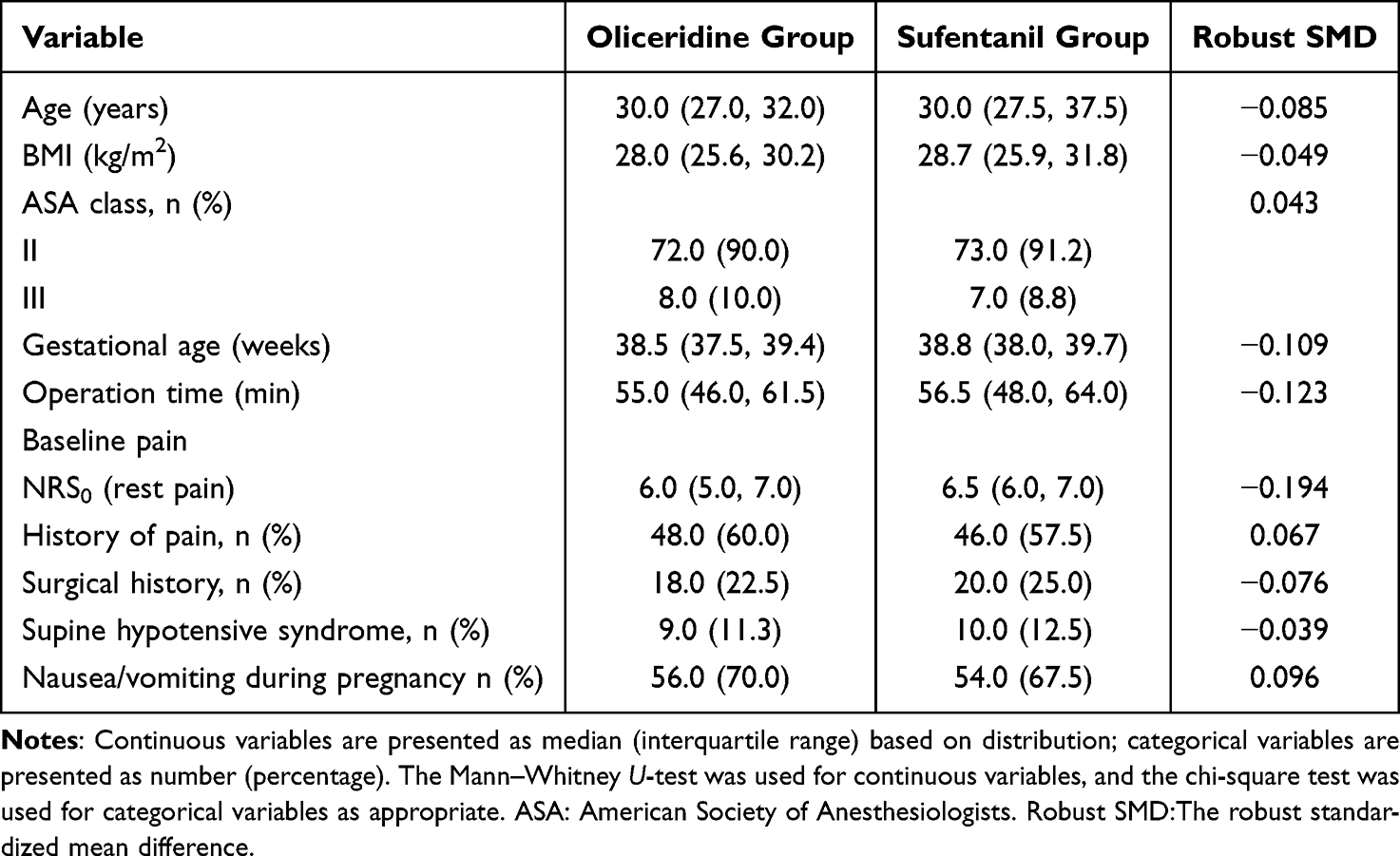 |
Table 1 Comparison of Baseline Characteristics Between the Two Groups |
Primary Outcome
The primary outcome measure was the Sum of Pain Intensity Differences over 48 hours (SPID48). Based on GEE analysis, the adjusted mean SPID48 was 172.50 (95% CI, 163.37–181.63) in the oliceridine group and 147.90 (95% CI, 137.59–158.21) in the sufentanil group, with a mean difference of 24.60 (95% CI, 10.83–38.37). The lower limit of the 95% CI for the difference exceeded the pre-specified non-inferiority margin of −20, confirming the non-inferiority of oliceridine (Table 2).
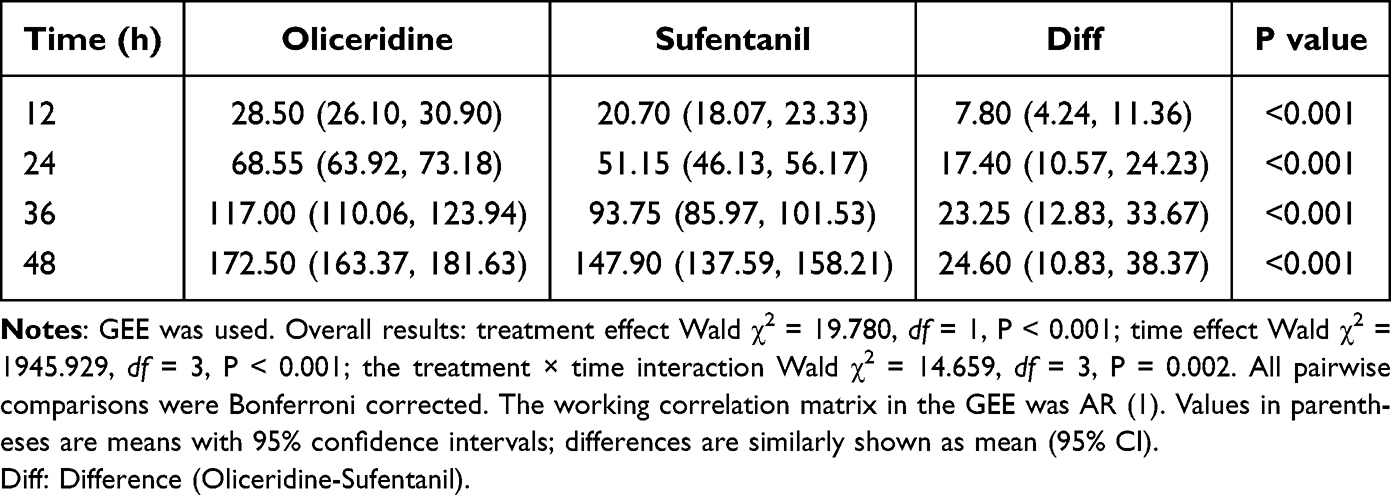 |
Table 2 Comparison of Summed Pain Intensity Difference (SPID) at 12, 24, 36, and 48 Hours Between the Two Groups Using GEE |
For SPID48, the overall treatment effect was significant (Wald χ2 = 19.780, df = 1, P < 0.001), as were the time effect (Wald χ2 = 1945.929, df = 3, P < 0.001) and the treatment × time interaction effect (Wald χ2 = 14.659, df = 3, P = 0.002) (Table 2).
Secondary Outcomes
Pain Scores at Each Time Point and Sum of Pain Intensity Differences
EE model analysis showed that after adjusting for baseline NRS, the average resting NRS scores at 12, 24, and 36 hours postoperatively were all significantly lower in the oliceridine group than in the sufentanil group (all P < 0.001) (Table 3). The overall treatment effect was significant (Wald χ2 = 125.694, df = 1, P < 0.001), as were the time effect (Wald χ2 = 616.828, df = 3, P < 0.001) and the treatment × time interaction effect (Wald χ2 = 7.506, df = 3, P = 0.057) (Table 3).
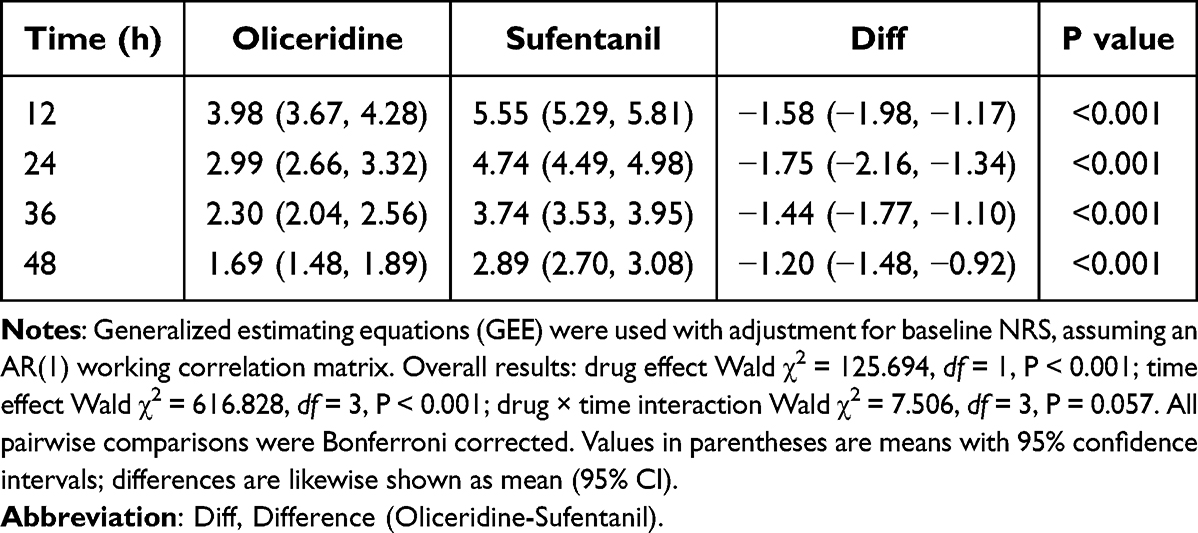 |
Table 3 Comparison of NRS Pain Scores at 12, 24, 36, and 48 Hours Between the Two Groups Using GEE |
The summed pain intensity differences (SPID) at 12, 24, and 36 hours, analyzed by GEE, were all significantly greater in the oliceridine group compared to the sufentanil group (all P < 0.001).
The trends of resting NRS scores over time in both groups are illustrated in Figure 2.
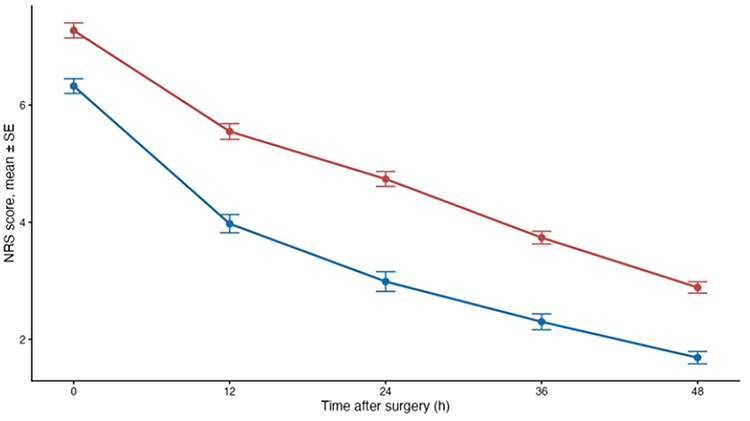 |
Figure 2 Trends in NRS scores within 48 hours postoperatively in the two groups. Note: Data are presented as mean±SE values. The vertical axis represents the pain Numerical Rating Scale (NRS, 0–10), with lower scores indicating less pain. From 0 to 48 h postoperatively, pain scores in both groups showed a continuous downward trend, and the oliceridine group had lower scores than the sufentanil group at all time points. The red line represents sufentanil, and the blue line represents oliceridine. |
PCIA Usage
During the 48-hour postoperative period, the oliceridine group had significantly fewer median total PCIA demands (34.0 vs 56.0, P < 0.001), fewer valid boluses delivered (32.0 vs 44.5, P < 0.001), and a lower total analgesic pump dose (62.5 mL vs 69.0 mL, P = 0.034) compared with the sufentanil group (Table 4).
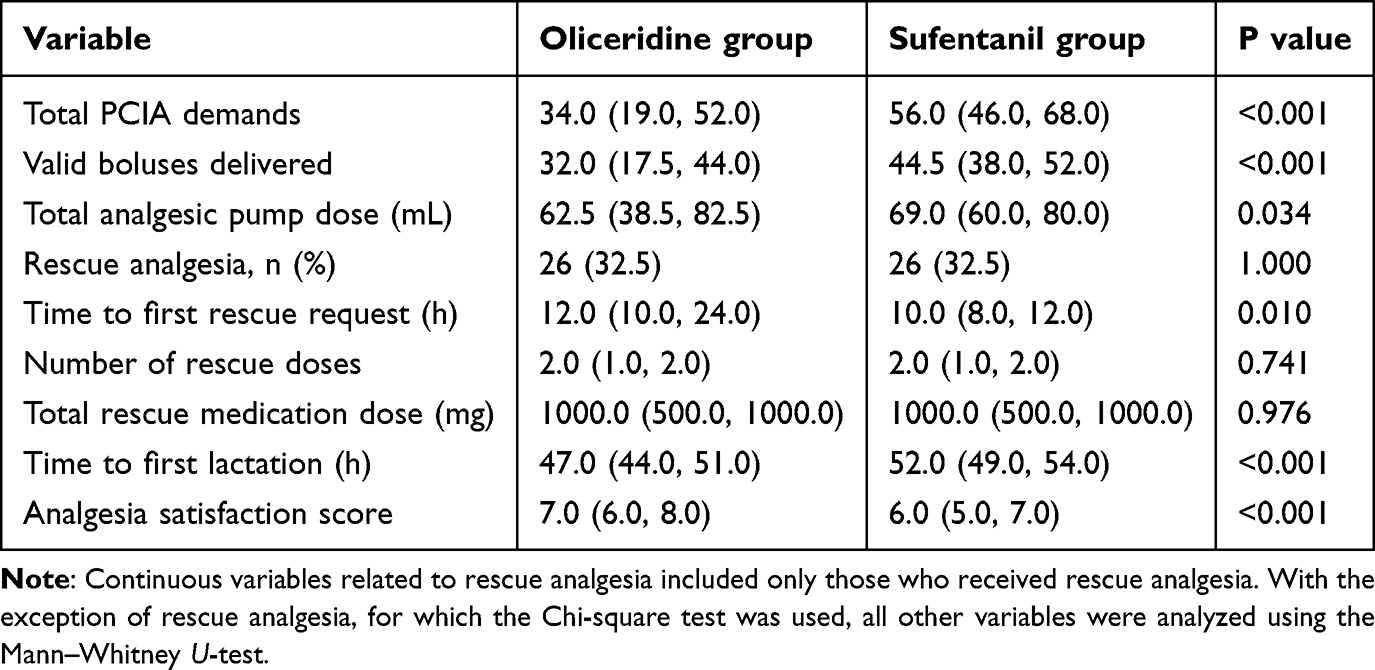 |
Table 4 Comparison of Analgesic Pump Use, Rescue Analgesia, Time to Lactation, and Satisfaction |
Rescue Analgesia
The proportion of patients requiring rescue analgesia was identical in both groups (32.5%). Among those who received rescue analgesia, the median time to first rescue request was significantly longer in the oliceridine group (12.0 hours) than in the sufentanil group (10.0 hours, P = 0.010). No statistically significant differences were found between groups in the number of rescue doses or total rescue medication dose (P > 0.05) (Table 4).
Time to First Lactation and Satisfaction
The median time to first lactation was 47.0 hours in the oliceridine group, which was significantly earlier than the 52.0 hours in the sufentanil group (P < 0.001). The median overall analgesia satisfaction score at 48 hours was higher in the oliceridine group (7.0 vs 6.0, P < 0.001) (Table 4).
Safety and Adverse Events
The overall incidence of adverse events was 18.8% (15/80) in the oliceridine group, which was significantly lower than the 36.2% (29/80) in the sufentanil group (P = 0.013). Regarding specific adverse events, the incidence of nausea was significantly lower in the oliceridine group (7.5% vs 20.0%, P = 0.022). For nausea, the absolute risk reduction was 12.5% (95% CI: 2.0% to 23.0%), and the relative risk was 0.38 (95% CI: 0.15 to 0.91). No statistically significant differences were found between the groups in the incidences of vomiting, dizziness, constipation, pruritus, chest tightness, or fever (P > 0.05) (Table 5).
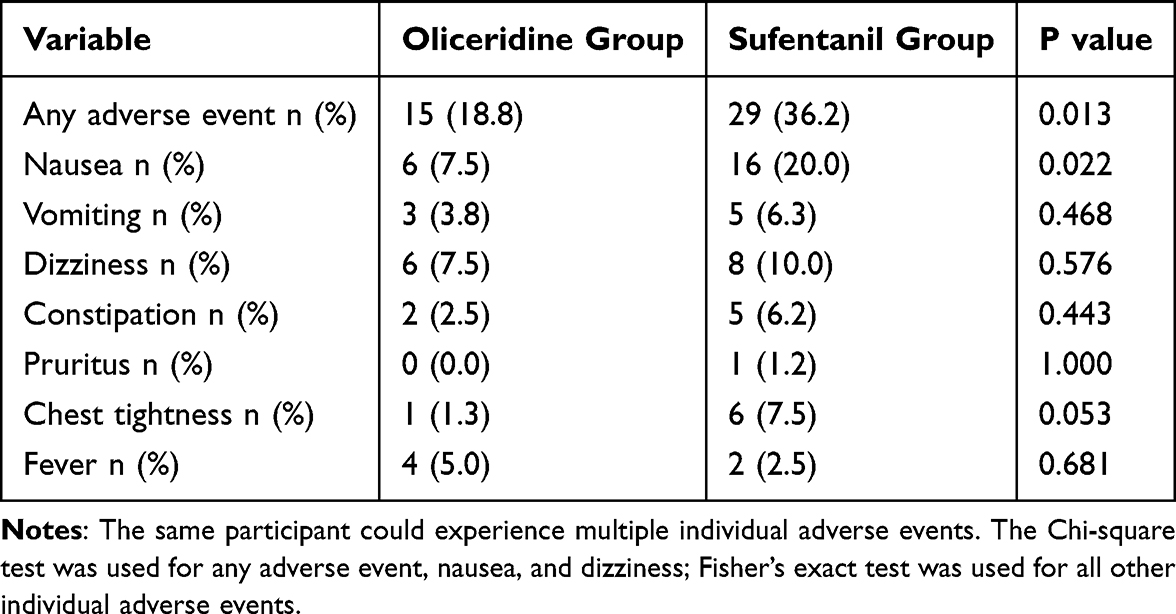 |
Table 5 Comparison of the Incidence of Adverse Events Between the Two Groups |
Discussion
Our study results showed that oliceridine provided comparable postoperative analgesic effects to sufentanil within 48 hours. These results indicate that this method has potential application prospects in the clinical environment. Several clinical studies have explored the analgesic potential of oliceridine in various surgical environments, demonstrating its effectiveness.19–22 Another multicenter study showed that in patients with moderate to severe postoperative pain after abdominal surgery, the response rate to oliceridine within 24 hours after the loading dose was not different from that to traditional opioids, suggesting that oliceridine can provide comparable analgesic effects to traditional opioids in this comprehensive analgesic regimen.23
The early postoperative analgesic response rate of oliceridine was higher, indicating that oliceridine takes effect faster, which may be related to its pharmacokinetic characteristics. According to a pharmacokinetic review, oliceridine has a fast onset of analgesia (1–2 minutes) and reaches peak effect within 6–12 minutes after intravenous administration. Furthermore, oliceridine has a short elimination half-life (approximately 1.3–3 hours), allowing for rapid offset of its analgesic effect. This pharmacokinetic profile not only facilitates prompt postoperative pain control but also enables clinicians to titrate the dose dynamically in response to changes in the patient’s pain intensity.24
The VOLITION prospective cohort study sought to assess the efficacy of oliceridine for managing postoperative pain and to analyze its opioid-related adverse effects. Utilizing a self-administered analgesic system containing oliceridine, the research involved 204 patients aged 18 or older who had received general anesthesia for major non-cardiac surgeries. Findings revealed that over the 48-hour postoperative period, patients experienced both improved pain scores and enhanced Myles Quality of Recovery outcomes.25 This is consistent with our research findings.
The most clinically significant finding was the comparison of adverse reactions. Compared with sufentanil, oliceridine showed a lower incidence of postoperative nausea, vomiting, dizziness, chest tightness, and itching, demonstrating better safety, consistent with previous study results. Another retrospective study showed that compared with traditional opioids, the use of oliceridine in PCIA was associated with a lower incidence of opioid-related adverse reactions.14 These findings suggest that oliceridine may be a safer alternative for postoperative pain treatment. This benefit may be attributed to its unique pharmacological properties as a G protein-biased μ-opioid receptor agonist. The analgesic effects and adverse reactions of traditional opioids are mediated by the μ-opioid receptor (MOR). Upon activation, the MOR primarily couples to inhibitory G proteins (Gαi/o), leading to inhibition of adenylyl cyclase, activation of G protein-coupled inwardly rectifying potassium (GIRK) channels, and reduced opening of voltage-gated calcium channels. These events result in neuronal hyperpolarization, suppression of pain signal transmission, and consequently, analgesia. However, conventional opioids such as morphine and fentanyl also potently recruit β-arrestin-2, a pathway closely associated with opioid-related adverse events, including respiratory depression and constipation.24,26,27 Oliceridine is a novel G protein-biased μ-opioid receptor agonist that, upon binding to the MOR, preferentially activates G protein signaling while exhibiting markedly reduced efficacy in recruiting β-arrestin-2 (approximately 14% of that of morphine).24–26 Therefore, oliceridine provides analgesic efficacy comparable to that of sufentanil while being associated with fewer opioid-related adverse events.24,26
Breast milk, as the ideal natural food for newborns, provides essential immune components that support healthy growth and also promotes postpartum uterine contraction, thereby reducing the risk of bleeding.28 Delayed or impaired milk secretion can lead to breast engorgement and milk stasis, which adversely affect both maternal health and successful breastfeeding.29 In this study, time to first lactation in the oliceridine group was shorter than in the sufentanil group. However, this result is exploratory, and future research should consider it as the primary outcome for further validation.
Limitations
This study has limitations. Its single-center design may affect generalizability. The sample size, while adequate for primary efficacy, was underpowered for rare adverse events. The 48-hour observation period precluded assessment of long-term outcomes like persistent pain or breastfeeding continuation. Finally, the absence of breast milk oliceridine concentration data necessitates future pharmacokinetic studies to fully establish neonatal safety during breastfeeding.
Conclusion
In conclusion, oliceridine exhibited non-inferior analgesic efficacy relative to sufentanil when applied for PCIA after cesarean delivery, and provided effective postoperative pain relief for parturients. Oliceridine can be recommended as a viable alternative for postoperative analgesia in patients undergoing cesarean delivery.
Statement on AI-Assisted Writing
During the preparation of this work, we used Deep Seek for language polishing and sentence refinement. After using this tool, we reviewed and edited the content as needed and take full responsibility for the content of the published article.
Data Sharing Statement
Deidentified individual participant data will be shared. Specifically, data regarding primary and secondary outcomes, baseline characteristics, adverse events, and PCIA usage will be made accessible. The study protocol and statistical analysis plan will also be provided. Data can be accessed by contacting the corresponding author (Xiaobao Zhang, email: [email protected]) when a reasonable request is made. The data will be available starting 6 months after publication and will remain accessible for a period of 5 years.
Ethical Adherence
All patients provided informed consent. All study procedures were performed in accordance with the Declaration of Helsinki and relevant requirements of the clinical research ethics committee.
Acknowledgments
The authors would like to extend their sincere gratitude to Dr. Fangming Shen for his scientific guidance. We also acknowledge the Big Data Center of the Affiliated Lianyungang Hospital of Xuzhou Medical University for providing data support services. Additionally, we extend special thanks to the Department of Anesthesiology for their assistance and support.
Funding
This research was supported by WU JIEPING MEDICAL FOUNDATION, WJPMF (Grant No.320.6750.2024-15-110).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wells JC, Wibaek R, Poullas M. Global epidemiology of use of and disparities in caesarean sections. Lancet. 2019;394(10192):24–11. doi:10.1016/S0140-6736(19)30715-9
2. Lauretta A, Frkovic V, Saporito A. Integrating regional blocks into enhanced recovery after surgery protocols for cesarean delivery: optimizing postoperative recovery. Curr Opinion Anaesthesiol. 2025;38(3):179–185. doi:10.1097/ACO.0000000000001459
3. Borges NC, Pereira LV, de Moura LA, Silva TC, Pedroso CF. Predictors for moderate to severe acute postoperative pain after cesarean section. Pain Res Manag. 2016;2016:5783817. doi:10.1155/2016/5783817
4. Rawal N. Intrathecal opioids for the management of post-operative pain. Best Pract Res Clin Anaesth. 2023;37(2):123–132. doi:10.1016/j.bpa.2023.01.001
5. Pei Q, Xuan H, Peng Z. Impact of oxycodone for the treatment of acute postoperative pain in cesarean section: a review. Medicine. 2025;104(8):e41645. doi:10.1097/MD.0000000000041645
6. Wang L, Wang Y, Ma Y, et al. Sufentanil combined with nalbuphine via patient-controlled intravenous analgesia after cesarean section: a retrospective evaluation. Drug Des Devel Ther. 2022;16:3711–3721. doi:10.2147/DDDT.S380292
7. O’Connor M, Martin A. Device therapy in ccTGA: friend or Foe? Int J Cardiol. 2026;447:134112. doi:10.1016/j.ijcard.2025.134112
8. Tassou A, Richebe P, Rivat C. Mechanisms of chronic postsurgical pain. Reg Anesth Pain Med. 2025;50(2):77–85. doi:10.1136/rapm-2024-105964
9. He G, Liu X. Structure-bias relationship of μ-opioid receptor agonists. Handbook Exp Pharmacol. 2026;290:261–273.
10. Wang C, Liu L, Bai X. Global trends in oliceridine (TRV130) research from 2013 to 2024: a bibliometrics and knowledge graph analysis. Drug Des Devel Ther. 2024;18:4681–4692. doi:10.2147/DDDT.S475205
11. Viscusi ER, Skobieranda F, Soergel DG, Cook E, Burt DA, Singla N. APOLLO-1: a randomized placebo and active-controlled phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the µ-opioid receptor, for management of moderate-to-severe acute pain following bunionectomy. J Pain Res. 2019;12:927–943. doi:10.2147/JPR.S171013
12. Tian Y, Hu J, Pan H, Bai G, Zhang Z, Zhang P. Effect of oliceridine combined with sufentanil on patient-controlled intravenous analgesia in elderly patients after laparoscopic radical resection of rectal cancer: a prospective randomized controlled study. Drug Des Devel Ther. 2025;19:10033–10043. doi:10.2147/DDDT.S553848
13. Duan J, Wang X, Hou C, Yu T, Ju X, Wang S. Comparison of oliceridine and morphine in postoperative analgesia in laparoscopic total hysterectomy, a randomized double-blind controlled trial. Drug Des Devel Ther. 2025;19:6687–6697. doi:10.2147/DDDT.S530296
14. Huang C, Liu B, Xie S, et al. Evaluating the opioid-related adverse events of oliceridine versus conventional opioids in patient-controlled analgesia after thoracoscopic lung resection: a retrospective cohort study. Drug Des Devel Ther. 2025;19:5929–5939. doi:10.2147/DDDT.S532778
15. Hale TW, Krutsch K. Opioid use in breastfeeding mothers and neonatal risks. Clin Pharmacol Ther. 2021;109(3):573–575. doi:10.1002/cpt.2118
16. Ringold FG, Minkowitz HS, Gan TJ, et al. Sufentanil sublingual tablet system for the management of postoperative pain following open abdominal surgery: a randomized, placebo-controlled study. Reg Anesth Pain Med. 2015;40(1):22–30. doi:10.1097/AAP.0000000000000152
17. Liang DY, Li WW, Nwaneshiudu C, Irvine KA, Clark JD. Pharmacological characters of oliceridine, a μ-opioid receptor g-protein-biased ligand in mice. Anesth Analg. 2019;129(5):1414–1421. doi:10.1213/ANE.0000000000003662
18. Meng Y, Yuan S, Zhang H, et al. Comparison of oliceridine and sufentanil in patient - controlled intravenous analgesia for post - thoracoscopic nausea and vomiting: a prospective, double - blind, randomized controlled trial. Front Pharmacol. 2025;16:1576154. doi:10.3389/fphar.2025.1576154
19. Dahan A, van Dam CJ, Niesters M, et al. Benefit and risk evaluation of biased μ-receptor agonist oliceridine versus morphine. Anesthesiology. 2020;133(3):559–568. doi:10.1097/ALN.0000000000003441
20. Singla N, Minkowitz HS, Soergel DG, et al. A randomized, Phase IIb study investigating oliceridine (TRV130), a novel µ-receptor G-protein pathway selective (μ-GPS) modulator, for the management of moderate to severe acute pain following abdominoplasty. J Pain Res. 2017;10:2413–2424. doi:10.2147/JPR.S137952
21. Singla NK, Skobieranda F, Soergel DG, et al. APOLLO-2: a randomized, placebo and active-controlled Phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the μ-opioid receptor, for management of moderate to severe acute pain following abdominoplasty. Pain Prac. 2019;19(7):715–731. doi:10.1111/papr.12801
22. Bergese SD, Brzezinski M, Hammer GB, et al. ATHENA: a Phase 3, open-label study of the safety and effectiveness of oliceridine (TRV130), A G-protein selective agonist at the µ-opioid receptor, in patients with moderate to severe acute pain requiring parenteral opioid therapy. J Pain Res. 2019;12:3113–3126. doi:10.2147/JPR.S217563
23. Gong C, Wen O, Ruping D, et al. Efficacy and safety of oliceridine for treatment of moderate to severe pain after surgery with general anesthesia: a prospective, randomized, double-blinded, multicenter, positive-controlled clinical trial. Chinese J Anesthesiol. 2024;44(2):135–139.
24. Daksla N, Wang A, Jin Z, Gupta A, Bergese SD. Oliceridine for the management of moderate to severe acute postoperative pain: a narrative review. Drug Des Devel Ther. 2023;17:875–886. doi:10.2147/DDDT.S372612
25. Sessler DI, Ayad S, Bakal O, et al. Oliceridine for postoperative pain and opioid-related complications: the intravenous oliceridine and opioid-related complications (VOLITION) prospective cohort study. J Clin Anesth. 2025;105:111870. doi:10.1016/j.jclinane.2025.111870
26. Manglik A, Lin H, Aryal DK, et al. Structure-based discovery of opioid analgesics with reduced side effects. Nature. 2016;537(7619):185–190. doi:10.1038/nature19112
27. Stahl EL, Bohn LM. Low intrinsic efficacy alone cannot explain the improved side effect profiles of new opioid agonists. Biochemistry. 2022;61(18):1923–1935. doi:10.1021/acs.biochem.1c00466
28. Bermejo-Haro MY, Camacho-Pacheco RT, Brito-Pérez Y, Mancilla-Herrera I. The hormonal physiology of immune components in breast milk and their impact on the infant immune response. Mole Cellular Endocrinol. 2023;572:111956. doi:10.1016/j.mce.2023.111956
29. Farah E, Barger MK, Klima C, Rossman B, Hershberger P. Impaired lactation: review of delayed lactogenesis and insufficient lactation. J Midwifery Women’s Health. 2021;66(5):631–640. doi:10.1111/jmwh.13274
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Patient-Controlled Intravenous Analgesia (PCIA) with Sufentanil Background Infusion for Post-Cesarean Analgesia: A Randomized Controlled Trial
Nie Z, Cui X, Zhang R, Li Z, Lu B, Li S, Cao T, Zhuang P
Journal of Pain Research 2022, 15:1355-1364
Published Date: 6 May 2022
Sufentanil Combined with Nalbuphine via Patient-Controlled Intravenous Analgesia After Cesarean Section: A Retrospective Evaluation
Wang L, Wang Y, Ma Y, Mu X, Zhang Z, Wang H, Zheng Z, Nie H
Drug Design, Development and Therapy 2022, 16:3711-3721
Published Date: 21 October 2022
Effect of Oliceridine Combined with Sufentanil on Patient-Controlled Intravenous Analgesia in Elderly Patients After Laparoscopic Radical Resection of Rectal Cancer: A Prospective Randomized Controlled Study
Tian Y, Hu J, Pan H, Bai G, Zhang Z, Zhang P
Drug Design, Development and Therapy 2025, 19:10033-10043
Published Date: 8 November 2025
Comparison of Postoperative Analgesic Efficacy of Oliceridine and Sufentanil in Total Laparoscopy Hysterectomy, a Clinical Double-Blind Controlled Trial
Duan J, Liu N, Lu Q, Gao W, Hou C, Liu H, Lu Y, Xu S
Drug Design, Development and Therapy 2026, 20:582143
Published Date: 27 February 2026
Efficacy and Safety of Oliceridine for Patient-Controlled Intravenous Analgesia in Elderly Patients Undergoing Laparoscopic Radical Resection Surgery for Gastrointestinal Malignant Tumors: A Prospective Randomized Controlled Non-Inferiority Clinical Trial
Wang J, Shang Y, Wang C, Zhang D, Li H, Yu Q, Tao L, Sun L, Gao C
Drug Design, Development and Therapy 2026, 20:593111
Published Date: 8 May 2026