Back to Journals » Journal of Pain Research » Volume 15
Effectiveness of Patient-Controlled Intravenous Analgesia (PCIA) with Sufentanil Background Infusion for Post-Cesarean Analgesia: A Randomized Controlled Trial
Authors Nie Z ![]() , Cui X, Zhang R
, Cui X, Zhang R ![]() , Li Z, Lu B, Li S, Cao T, Zhuang P
, Li Z, Lu B, Li S, Cao T, Zhuang P ![]()
Received 23 February 2022
Accepted for publication 29 April 2022
Published 6 May 2022 Volume 2022:15 Pages 1355—1364
DOI https://doi.org/10.2147/JPR.S363743
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Zhongbiao Nie,1 Xianmei Cui,2 Ran Zhang,3 Zhihong Li,1 Bin Lu,4 Suxian Li,1 Tao Cao,2 Ping Zhuang4
1Pharmaceutical Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030012, People’s Republic of China; 2Obstetrics Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030012, People’s Republic of China; 3Nephrology Department, Affiliated Hospital of Shanxi University of Traditional Chinese Medicine, Taiyuan, 030036, People’s Republic of China; 4Anesthesiology Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030012, People’s Republic of China
Correspondence: Ping Zhuang, Anesthesiology Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030012, People’s Republic of China, Tel +86-13700503507, Email [email protected]
Purpose: To investigate the effectiveness of sufentanil patient-controlled intravenous analgesia pump (PCIA) and background infusion in patients of post-cesarean analgesia.
Patients and Methods: This trial compared two groups of women undergoing cesarean section and receiving PCIA: no background infusion group (n=30), 6-min lockout time, and background infusion group (n=30), 2 mL/h infusion, 10-min lockout time. Both groups with 2 μg/kg sufentanil was diluted to 100 mL with normal saline. VAS scores at rest at 36 h was the primary endpoint. The secondary endpoints were the VAS scores at rest at 6, 12, and 24 h, the total amount of sufentanil consumed, the Ramsay sedation score (RSS) assessed at the same time points, postpartum bleeding within 24 h, the injection/attempt (I/A) ratio, BP and HR, PONV, side effects of sufentanil.
Results: Compared with the no background infusion group, the background infusion group showed lower VAS pain scores at 6, 12, and 24 h (P< 0.01), but no differences at 36 h (95% CI = − 0.5– 0.8. P> 0.05). Attempts, injections, and total sufentanil consumption were significantly different between the two groups (P< 0.001), but without difference in I/A. Bleeding was less in the background infusion group at 1 h (P=0.03). The minimal respiration rates were not significantly different between groups.
Conclusion: Background infusion increased the total consumption of sufentanil within 36 h after cesarean section. Although it did not reduce uterine contraction pain and wound pain at 36 h, it significantly reduced the pain at 6, 12, and 24 h after cesarean section. It improved patient satisfaction and reduced the amount of bleeding after 1 h. Importantly, it did not increase the incidence of hypertension, PONV and respiratory depression.
Keywords: background infusion, patient-controlled intravenous analgesia, PCIA, sufentanil
Introduction
Pain after cesarean section is usually ranked moderate to severe.1 Management of pain after birth is important and can impact a woman’s return to normal activities and caring for her baby and shorten lactogenesis.2 Traditionally, intravenous administration of opioids has been successfully used for pain control after cesarean section.3 Patient-controlled intravenous analgesia pump (PCIA) is a commonly used method to relieve postoperative pain in hospitalized patients. The method is to titrate analgesics according to demand. Compared with “on-demand” opioid injections, it usually provides better pain control and improves patient satisfaction.4,5 The PCIA prescription includes the parameters programmed into the PCIA machine, such as bolus dose, lockout interval, dose limits, and background infusion. Each may have some effect on the safety and efficacy of PCIA.
A panel of the American Pain Society recommends against routine background infusion of opioids with PCIA in opioid-naïve adults because a background infusion of opioids is associated with an increased risk of nausea and vomiting, and in some studies with increased risk of respiratory depression in adults.6–10 Still, conflicting results were reported. Indeed, a study showed that adding a background morphine infusion to a standard morphine PCIA improved postoperative analgesia without increasing the side effects.11
Sufentanil, one of the opioids with the strongest analgesic potency, is now widely used for anesthesia of surgery patients, and has also been extensively used in postoperative pain control and labor pain relief.12–14 Furthermore, Grass et al suggested that a small background infusion might be necessary to sustain analgesia with sufentanil.15 Zhen et al16 and Gao et al17 showed that PCIA with background infusion of sufentanil achieved good analgesia without increased adverse effects after abdominal surgery. Similar results were observed for thoracotomy.18
This randomized controlled trial (RCT) aimed to investigate the effectiveness of sufentanil PCIA and background infusion in patients of post-cesarean analgesia.
Materials and Methods
Study Design
This study was a prospective, single-blind, randomized controlled trial with a two-arm parallel-group design in the gynecology and obstetrics department of Shanxi Bethune hospital from June 2020 to March 2021.
The inclusion criteria were 1) nulliparous women, 2) aged 18–40 years, 3) planned to undergo a cesarean section, 4) body mass index (BMI) of 18–29 kg/m2, 5) American Society of Anesthesiologists (ASA) grade I to II, and 6) no smoking history. The preoperative exclusion criteria were 1) severe heart, lung, liver, or kidney insufficiency, 2) hypertension during pregnancy, 3) preoperative fetal distress, 4) history of mental or neurological diseases, 5) opioid allergies, 6) opioid tolerance, 7) smoking history, 8) history of motion sickness, or 9) history of postoperative nausea and vomiting (PONV). The postoperative exclusion criteria were 1) re-operation exploration, 2) hemodynamic instability, including systolic blood pressure (SBP) <90 mmHg, severe arrhythmia, or hemorrhage,11 or 3) postoperative confusion.
After approval from the ethics committee of Shanxi Bethune Hospital (#YXLL-SL-2020-017), consenting parturients were included in this prospective randomized study. Written informed consent was obtained from all subjects. The study was registered prior to patient enrollment at the Chinese Clinical Trial Register (Register number: ChiCTR2000037940), participating in the World Health Organization International Clinical Trials Registry Platform. The trial was conducted according to the tenets of the Declaration of Helsinki and the Good Clinical Practice.
Randomization and Blinding
A Microsoft Excel “Random” function-generated randomization sheet was used for randomization. The randomized sheet was kept by the qualified clinical research pharmacist who managed the drugs. The participants were blinded to the intervention.
Intervention
All parturients received 500 mL of intravenous Ringer’s solution before epidural analgesia. All participants received combined spinal and epidural anesthesia (CSEA) at the L3-4 or L2-3 space using the needle-through-needle technique. A 16–18mg of 0.5% ropivacaine injection was given to subarachnoid space. When the effect of subarachnoid block was poor, 3–5mL of 1.5% lidocaine was added to epidural space. If hypotension occurred (SBP <90 mmHg or a reduction >20% of the basal SBP), 50 μg of phenylephrine was administered intravenously, and fluid infusion was sped up. When the SBP was higher than 180 mmHg, the infusion rate was lowered, and 25 mg of urapidil or 0.1 mg of nicardipine was administered intravenously. If the heart rate (HR) was <50 bpm, 0.2 mg of atropine was intravenously injected. The parturients were sent to the post-anesthesia care units (PACU) after surgery. When vital signs were stable and the sensory block was not higher than T8, the PCIA pumps were connected in the PACU, and then the parturients were sent back to their ward. The PCIA pumps were discontinued after 36 h for all participants.
According to body weight, 2 μg/kg sufentanil (Yichang Humanwell Pharmaceutical Jiangxi Province China) was diluted to 100 mL with normal saline. The 60 parturients had a PCIA analgesia protocol initiated consisting of a 0.5-mL bolus and were then randomized to no background infusion, 6-min lockout time (no background infusion Group), or 2 mL/h infusion, 10-min lockout time (background infusion Group). The drugs were delivered in a sealed opaque envelope before surgery, and the envelope was opened in the operating room only by a non-blinded anesthesiologist who was responsible for anesthesia management and setting the PCIA as per the protocol in the operating room. All other investigators who assessed the study endpoints after the operation in the PACU and the ward were blinded to group assignment. All the PCIA devices were applied to parturients with labels with only the patient’s study number so that neither the parturients nor medical care providers and investigators could recognize the PCIA regimen.
The parturients were instructed on using the PCIA pump and told to press the button whenever they felt pain. No other analgesic drug was allowed, but parturients were allowed to receive an intramuscular injection of 100 mg of tramadol when they complained of pain >7 on the VAS; if necessary, the injection could be repeated. Still, analgesia failure had to be excluded. Intravenous metoclopramide 10 mg was given as a rescue antiemetic at the parturients’ request. If severe nausea persisted after two consecutive rescue antiemetics, PCIA was stopped for 2 h and restarted later when the symptoms subsided.
Endpoints
Visual analog scale (VAS) scores at 36 h were assessed as the primary endpoint measures. VAS scores included wound pain at rest (VAS-R) scores and uterine cramping pain (VAS-U) scores. The intensity of pain was recorded with a 10-cm VAS, which ranged from 0 (no pain) to 10 (the worst pain imaginable). The secondary endpoints were the VAS scores at 6, 12, 24 h, the total amount of sufentanil consumed, the Ramsay sedation score (RSS)19 assessed at the same time points, postpartum bleeding within 24 h, the injection/attempt (I/A) ratio, PONV, side effects of sufentanil. The I/A ratio compares the number of actual analgesic doses delivered with the number of requests for analgesic (attempts). Ideally, I/A ratios should be close to 1, indicating that each patient injection corresponds to one attempt for analgesic administration. PONV was rated on a four-point verbal scale (none = no nausea, mild = nausea but no vomiting, moderate = vomiting one attack, severe = vomiting > one attack). All side effects related to sufentanil, including dizziness, pruritus, headache, and constipation, were examined. Respiratory depression was defined by a respiratory rate <10 per min or oxygen saturation <90% for >1 min.20 The participants were asked about their satisfaction with PCIA during the previous 36 h, using a scale with 0 meaning not satisfied to 5 meaning very satisfied. The participants were assessed by a trained nurse who was blinded to group assignment. HR and blood pressure (BP) were recorded postoperatively at 6, 12, 24, and 36 h.
Baseline demographic data were recorded, including age, height, weight, BMI, operation time, gestation, in-hospital days, and ASA classification.
Sample Size
In order to determine the appropriate dose of sufentanil in PCIA after surgery, the primary endpoint pain level assessed by VAS was analyzed. The expected standard deviation of the means in the general patient population was 6.9 mm,16,21,22 and the standard deviation of the participants was 20 mm.23 The significance level was set at 0.05 and the power at 0.8. Sample size assumption was made through the PASS 11 software (NCSS, LLC, Kaysville, Utah, USA). The calculated sample size was 29 in each group. Finally, 30 patients were included in each group.
Statistical Analysis
Statistical analyses were performed using SPSS 20 (IBM, Armonk, NY, USA). The per-protocol (PP) set was used for analysis in this study. Continuous data were shown as means ± standard deviations or mean differences with 95% confidence interval (95% CI). Categorical data were presented as cases and frequency. The Kolmogorov–Smirnov test was performed to test whether the data conformed to a normal distribution. Differences between the two groups were compared using analysis of repeated-measures ANOVA and independent sample t-test. P-values <0.05 were considered statistically significant.
Results
Characteristics of the Participants
A total of 73 patients were assessed for eligibility, and seven were excluded for noncompliance with the study protocol. Thus, 66 patients were randomized: 34 in the no background infusion group and 32 in the background infusion group. Four operations were converted to open hysterectomy, and two patients discontinued IV-PCA due to pump malfunction. Finally, 60 parturients were included in the analysis, with 30 in each group (Figure 1). Table 1 shows the baseline demographic and obstetric data. The values of hemodynamic data remained within the normal range throughout the study period.
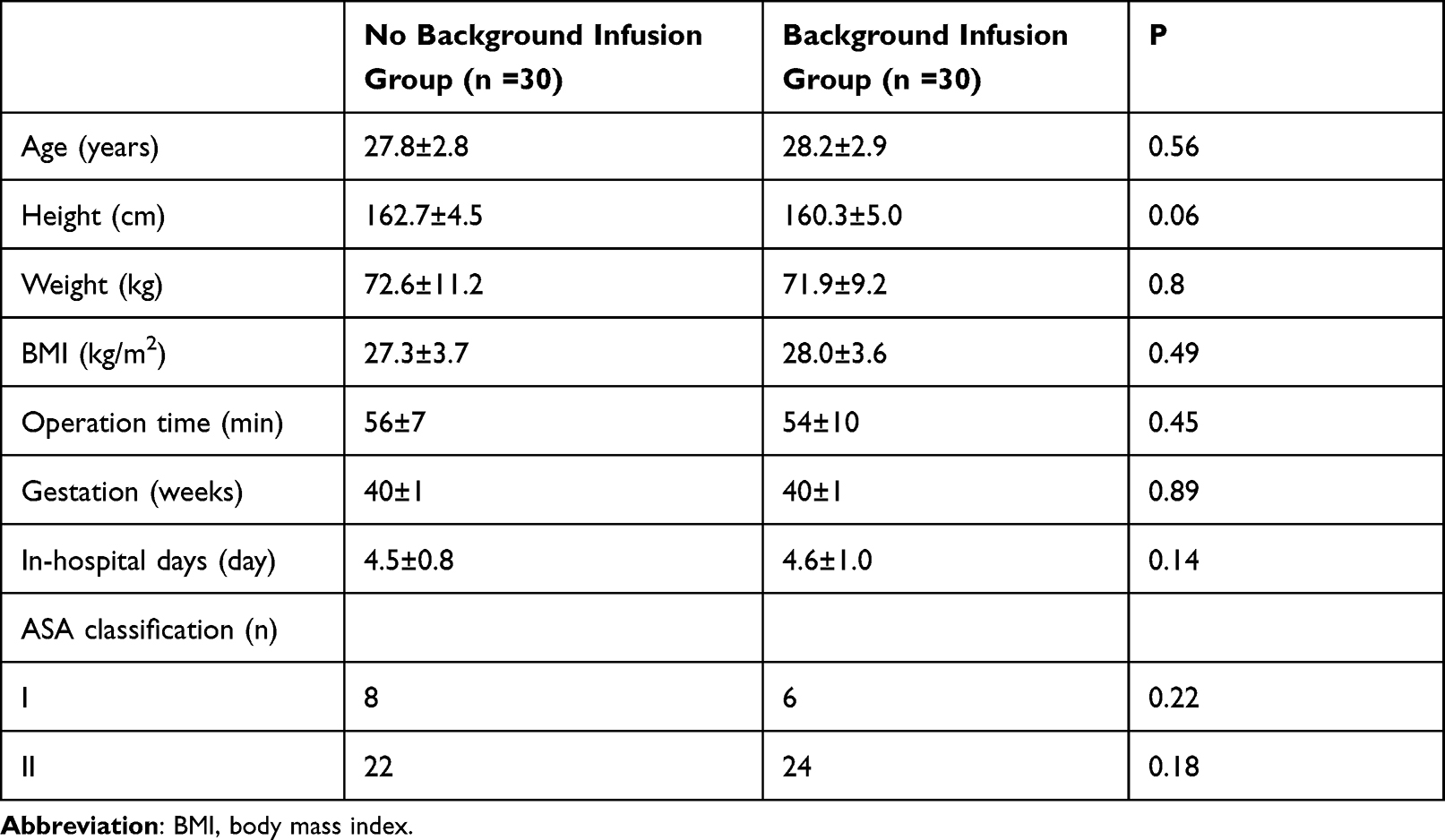 |
Table 1 Baseline Demographic and Obstetric Data |
 |
Figure 1 Study CONSORT flow diagram. |
Primary Outcome
The comparisons of VAS-R and VAS-U at 36 h are presented in Table 2. There were no significant differences in VAS-R and VAS-U at 36 h between the no background infusion and background infusion groups.
 |
Table 2 VAS Pain Scores 36 h After Surgery for Two Groups |
Secondary Outcomes
The comparisons of VAS-R and VAS-U at 6, 12, and 24 h are presented in Table 3. VAS-R and VAS-U were different between the two groups, the background infusion group showed lower VAS-R and VAS-U pain scores at 6, 12, and 24 h (P group < 0.01).
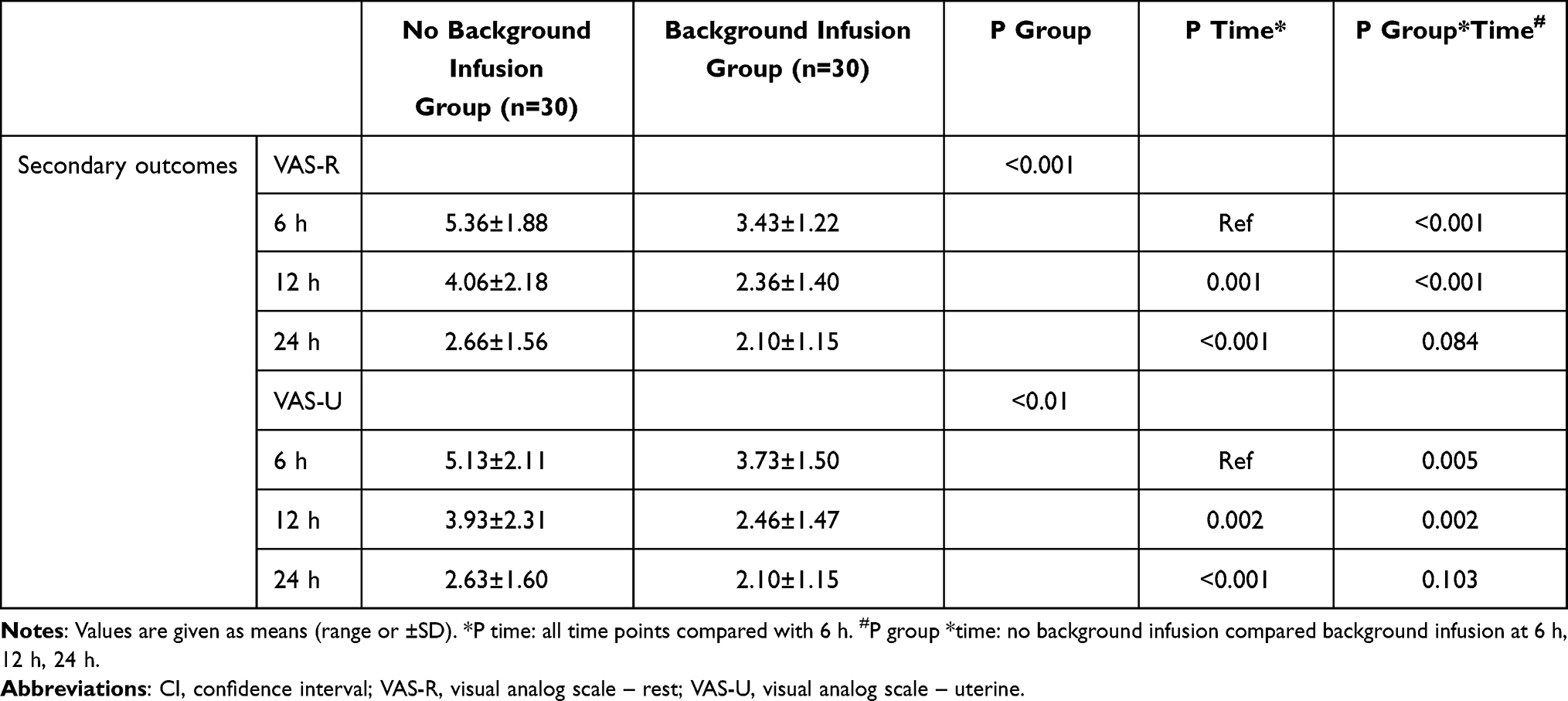 |
Table 3 VAS Pain Scores 6, 12, 24 After Surgery for Two Groups |
The comparisons of attempts, injections, and total sufentanil consumption at 6, 12, 24, and 36 h are presented in Table 4. Attempts, injections, and total sufentanil consumption were different between the two groups. The attempts and injections of background infusion group were significantly lower than those of no background infusion group, and consumption increased significantly (P group < 0.001).
 |
Table 4 Attempts, Injections, and Total Sufentanil Required 6, 12, 24, and 36 h After Surgery for Two Groups |
There were no significant differences in I/A, BP and HR between the two groups at 36 h. The background infusion group showed significantly higher satisfaction than the no background infusion group (P<0.001) (Table 5). Bleeding was smaller in the background infusion group at 1 h (P=0.03), without differences at the other time points (all P>0.05) (Table 6).
 |
Table 5 I/A and Satisfaction 36 h After Surgery for Two Groups |
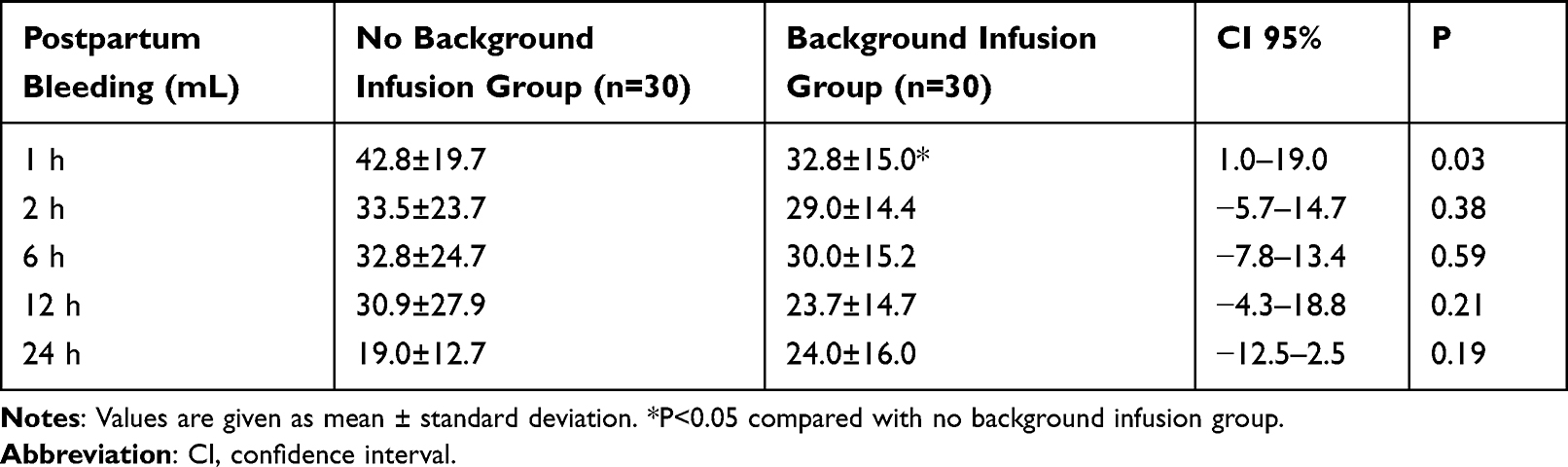 |
Table 6 Postpartum Bleeding Within 24 h |
The minimal respiration rates were not significantly different between the two groups. No patient showed ventilatory depression. The side effects related to sufentanil, including PONV, dizziness, pruritus, headache, and constipation, were not observed in the two groups. All patients had the same Ramsay sedation score.
Discussion
This study aimed to investigate the benefit of sufentanil PCIA and background infusion in patients of post-cesarean analgesia. The results suggest that background infusion increased the total consumption of sufentanil within 36 h after cesarean section. Although it did not reduce uterine contraction pain and wound pain at 36 h, it significantly reduced the pain at 6, 12, and 24 h after cesarean section. It improved patient satisfaction and reduced the amount of bleeding after 1 h. Importantly, it did not increase the incidence of PONV and respiratory depression. According to the American Pain Society postoperative guidelines,7 the use of background infusion is not required because of the aggravation of PONV. Still, one of the conclusions of this study is that the use of background infusion did not increase the incidence of PONV after obstetric surgery. However, a comparative study of the postoperative incidence of PONV requires a sufficient number of samples, and the sample size of this study was very small, and future randomized studies with sufficient sample size are needed.
Opioids are useful and potent analgesics for relieving moderate-to-severe postoperative pain. Morphine, fentanyl, and sufentanil are commonly used opioids for PCIA.15,24–26 Morphine has been regarded as the first choice for PCIA and is the most used and studied drug for PCIA.15 Still, the usefulness of morphine is sometimes compromised by its active metabolite (morphine-6-glucuronide) that produces respiratory depression, especially in patients with renal insufficiency because the metabolite is mainly excreted by the kidney.27 Sufentanil, a selective μ-receptor agonist, is commonly used for PCIA because of its rapid peak, potent analgesic activity, and short half-life.28,29 Like fentanyl, sufentanil has no active metabolites, and it is 5–10 times more potent than its parent drug, fentanyl.30,31 Sufentanil displays a lower incidence of respiratory depression than other opioids.24,32 Sufentanil has a relatively rapid equilibration half-life (t½ of 6.2 minutes) between plasma and brain, compared to 2.8 h for morphine,33,34 and a relatively shorter duration of action than morphine and fentanyl.35 Sufentanil transfer into milk has not been reported. Still, its safety profile is likely similar to fentanyl, and it is unlikely to cause any appreciable effects by its low levels in breast milk.36 Based on these properties, sufentanil can be appropriate and suited for PCIA. It is the most commonly used opioid for PCIA in China,25,37 is now widely used for surgery patients during anesthesia, and has also been extensively used in postoperative pain control and labor pain relief.38–40
A study showed that the dose of 2.5 μg/kg of sufentanil with background infusion is preferred because of better pain alleviation without an increase of adverse effects up to 48 h after surgery.16 Combined with our work experience, the dose of sufentanil was set at 2.0 μg/kg in the present trial. Still, improved pain control was observed for the first 24 h when using background infusion. It was also observed in abdominal and thoracic surgeries.17,18 Uterine contraction pain is defined as the intermittent cramping pain associated with uterine contraction. Wound pain is defined as the constant and evoked pain over the wound and adjacent region. Postcesarean pain, unlike most postoperative pain, consists of a nociceptive barrage from the incisional wound and uterine contraction.41 In this study, both types of pain were scored together. Because the pain of uterine contractions is enough to cover the wound pain, it was found in the study that many patients could not distinguish between the pain of the two, resulting in the same pain score. This study showed that the VAS at 6 h after surgery was higher in the two groups, which may be related to the inability to effectively reduce the pain of uterine contraction by using sufentanil alone. Hsu et al41 reported that 20 mg tenoxicam significantly potentiated morphine PCIA by reducing uterine cramping pain. Uterine contractions can reduce postpartum bleeding, and postpartum hemorrhage is one of the serious complications of cesarean section, and massive hemorrhage is the direct cause of hysterectomy and maternal death.42 This study found that the background infusion group had significantly reduced pain from uterine contractions but also reduced the amount of bleeding 1 h after surgery, directly reducing the adverse reactions of postpartum bleeding.
Apfel et al43 showed that patients with a history of motion sickness or PONV. Therefore, such patients were excluded. Although the American Pain Society suggests that background infusion of opioids is associated with an increased risk of nausea and vomiting, the present showed that PONV was not observed in the two groups. Regarding patients who use opioids after cesarean section, the reason for the extremely low incidence of PONV deserves further study. This may be the reason why the sample size of this study is very small. There have been attempts to create a score that could be used to rate the severity of nausea, vomiting, and retching in patients undergoing chemotherapy.44,45 Still, no score or index has been validated to define clinically important PONV. Techniques used in the past to measure PONV have included absolute counts or incidence rates, Likert scales, VASs, and treatment response. Wengritzky et al45 proposed the VAS as a screening tool in the clinical setting for rapid assessment or audit tool, and the VAS was selected in this study.
A lower I/A indicates a higher number of patient attempts occurring for each injection. It may indicate inadequate pain control. Besides, Sinatra et al46 suggest that lower I/A ratios may reflect a delay in obtaining the peak analgesic effect. In the present study, there was no difference in the I/A ratio between the two groups.
This study has limitations. It was performed at only one center, possibly introducing bias due to local practices and limiting the generalizability of the results. Comparisons with other analgesics or doses of sufentanil were not performed.
Conclusion
Compared with no background infusion, the total consumption of sufentanil at 36 h postoperative was greater in the background infusion group. Although uterine contraction pain and wound pain at 36 h were not reduced, background infusion significantly reduced the pain at 6, 12, and 24 h after cesarean section. It improved patient satisfaction and reduced the amount of bleeding after 1 h. Importantly, it did not increase the incidence of PONV and respiratory depression.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
After approval from the ethics committee of Shanxi Bethune Hospital (#YXLL-SL-2020-017), consenting parturients were included in this prospective randomized study. Written informed consent was obtained from all subjects.
Clinical Trials
The study was registered prior to patient enrollment at the Chinese Clinical Trial Register (Register number: ChiCTR2000037940), participating in the World Health Organization International Clinical Trials Registry Platform.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kerai S, Saxena KN, Taneja B. Post-caesarean analgesia: what is new? Indian J Anaesth. 2017;61(3):200–214. doi:10.4103/ija.IJA_313_16
2. Evans KC, Evans RG, Royal R, Esterman AJ, James SL. Effect of caesarean section on breast milk transfer to the normal term newborn over the first week of life. Arch Dis Child Fetal Neonatal Ed. 2003;88(5):F380–F382. doi:10.1136/fn.88.5.F380
3. Bonnet MP, Mignon A, Mazoit JX, Ozier Y, Marret E. Analgesic efficacy and adverse effects of epidural morphine compared to parenteral opioids after elective caesarean section: a systematic review. Eur J Pain. 2010;14(9):
4. Pastino A, Lakra A. Patient controlled analgesia. In: StatPearls. StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC; 2021.
5. Ocay DD, Otis A, Teles AR, Ferland CE. Safety of patient-controlled analgesia after surgery in children and adolescents: concerns and potential solutions. Front Pediatr. 2018;6:336. doi:10.3389/fped.2018.00336
6. Cheung CW, Ying CL, Lee LH, Tsang SF, Tsui SL, Irwin MG. An audit of postoperative intravenous patient-controlled analgesia with morphine: evolution over the last decade. Eur J Pain. 2009;13(5):464–471. doi:10.1016/j.ejpain.2008.05.013
7. Chou R, Gordon DB, de Leon-casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–157. doi:10.1016/j.jpain.2015.12.008
8. Etches RC. Respiratory depression associated with patient-controlled analgesia: a review of eight cases. Can J Anaesth. 1994;41(2):125–132. doi:10.1007/BF03009805
9. Looi-Lyons LC, Chung FF, Chan VW, McQuestion M. Respiratory depression: an adverse outcome during patient controlled analgesia therapy. J Clin Anesth. 1996;8(2):151–156. doi:10.1016/0952-8180(95)00202-2
10. Macintyre PE. Safety and efficacy of patient-controlled analgesia. Br J Anaesth. 2001;87(1):36–46. doi:10.1093/bja/87.1.36
11. Guler T, Unlugenc H, Gundogan Z, Ozalevli M, Balcioglu O, Topcuoglu MS. A background infusion of morphine enhances patient-controlled analgesia after cardiac surgery. Can J Anaesth. 2004;51(7):718–722. doi:10.1007/BF03018432
12. Zhi M, Diao Y, Liu S, et al. Sufentanil versus fentanyl for pain relief in labor involving combined spinal-epidural analgesia: a systematic review and meta-analysis of randomized controlled trials. Eur J Clin Pharmacol. 2020;76(4):501–506. doi:10.1007/s00228-019-02806-x
13. Nie Y, Tu W, Shen X, et al. Dexmedetomidine added to sufentanil patient-controlled intravenous analgesia relieves the postoperative pain after cesarean delivery: a prospective randomized controlled multicenter study. Sci Rep. 2018;8(1):9952. doi:10.1038/s41598-018-27619-3
14. Hu J, Zhang C, Yan J, Wang R, Wang Y, Xu M. Sufentanil and bupivacaine combination versus bupivacaine alone for spinal anesthesia during cesarean delivery: a meta-analysis of randomized trials. PLoS One. 2016;11(3):e0152605. doi:10.1371/journal.pone.0152605
15. Grass JA. Patient-controlled analgesia. Anesth Analg. 2005;101(5 Suppl):S44–S61. doi:10.1213/01.ANE.0000177102.11682.20
16. Zhen L, Li X, Gao X, Wei H, Lei X. Dose determination of sufentanil for intravenous patient-controlled analgesia with background infusion in abdominal surgeries: a random study. PLoS One. 2018;13(10):e0205959. doi:10.1371/journal.pone.0205959
17. Gao Y, Deng X, Yuan H, et al. Patient-controlled intravenous analgesia with combination of dexmedetomidine and sufentanil on patients after abdominal operation: a Prospective, Randomized, Controlled, Blinded, Multicenter Clinical Study. Clin J Pain. 2018;34(2):155–161. doi:10.1097/AJP.0000000000000527
18. Lin CS, Lu G, Ruan LY, Gu MN. [Patient-controlled intravenous analgesia with sufentanil and fentanyl after thoracotomy: a comparative study]. Nan Fang Yi Ke Da Xue Xue Bao. 2006;26(2):240–241. Chinese
19. Dawson R, von Fintel N, Nairn S. Sedation assessment using the Ramsay scale. Emerg Nurse. 2010;18(3):18–20. doi:10.7748/en2010.06.18.3.18.c7825
20. Tsui SL, Irwin MG, Wong CM, et al. An audit of the safety of an acute pain service. Anaesthesia. 1997;52(11):1042–1047. doi:10.1111/j.1365-2044.1997.232-az0371.x
21. Gerbershagen HJ, Aduckathil S, van Wijck AJ, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118(4):934–944. doi:10.1097/ALN.0b013e31828866b3
22. Brogly N, Schiraldi R, Vazquez B, Perez J, Guasch E, Gilsanz F. A randomized control trial of patient-controlled epidural analgesia (PCEA) with and without a background infusion using levobupivacaine and fentanyl. Minerva Anestesiol. 2011;77(12):1149–1154.
23. Oberhofer D, Skok J, Nesek-Adam V, et al. Intravenous ketoprofen in postoperative pain treatment after major abdominal surgery. World J Surg. 2005;29(4):446–449. doi:10.1007/s00268-004-7612-0
24. Palmer PP, Miller RD. Current and developing methods of patient-controlled analgesia. Anesthesiol Clin. 2010;28(4):587–599. doi:10.1016/j.anclin.2010.08.010
25. Zhang Y, Duan G, Guo S, et al. To predict sufentanil requirement for postoperative pain control using a real-time method: a prospective observational cohort study. Medicine. 2016;95(25):e3915. doi:10.1097/MD.0000000000003915
26. Kim KM. Analysis of the current state of postoperative patient-controlled analgesia in Korea. Anesth Pain Med. 2016;11(1):28–35. doi:10.17085/apm.2016.11.1.28
27. Osborne RJ, Joel SP, Slevin ML. Morphine intoxication in renal failure: the role of morphine-6-glucuronide. Br Med J. 1986;292(6535):1548–1549. doi:10.1136/bmj.292.6535.1548
28. Sedighinejad A, Haghighi M, Naderi Nabi B, et al. Magnesium sulfate and sufentanil for patient-controlled analgesia in orthopedic surgery. Anesth Pain Med. 2014;4(1):e11334. doi:10.5812/aapm.11334
29. Savoia G, Loreto M, Gravino E. Sufentanil: an overview of its use for acute pain management. Minerva Anestesiol. 2001;67(9 Suppl 1):206–216.
30. Maciejewski D. Sufentanil in anaesthesiology and intensive therapy. Anaesthesiol Intensive Ther. 2012;44(1):35–41.
31. Kim DK, Yoon SH, Kim JY, Oh CH, Jung JK, Kim J. Comparison of the effects of sufentanil and fentanyl intravenous patient controlled analgesia after lumbar fusion. J Korean Neurosurg Soc. 2017;60(1):54–59. doi:10.3340/jkns.2016.0707.007
32. Bailey PL, Streisand JB, East KA, et al. Differences in magnitude and duration of opioid-induced respiratory depression and analgesia with fentanyl and sufentanil. Anesth Analg. 1990;70(1):8–15. doi:10.1213/00000539-199001000-00003
33. Scott JC, Cooke JE, Stanski DR. Electroencephalographic quantitation of opioid effect: comparative pharmacodynamics of fentanyl and sufentanil. Anesthesiology. 1991;74(1):34–42. doi:10.1097/00000542-199101000-00007
34. Lötsch J, Skarke C, Schmidt H, Grösch S, Geisslinger G. The transfer half-life of morphine-6-glucuronide from plasma to effect site assessed by pupil size measurement in healthy volunteers. Anesthesiology. 2001;95(6):1329–1338. doi:10.1097/00000542-200112000-00009
35. Hughes MA, Glass PS, Jacobs JR. Context-sensitive half-time in multicompartment pharmacokinetic models for intravenous anesthetic drugs. Anesthesiology. 1992;76(3):334–341. doi:10.1097/00000542-199203000-00003
36. Montgomery A, Hale TW. ABM clinical protocol #15: analgesia and anesthesia for the breastfeeding mother, revised 2012. Breastfeed Med. 2012;7(6):547–553. doi:10.1089/bfm.2012.9977
37. Nie Y, Liu Y, Luo Q, Huang S. Effect of dexmedetomidine combined with sufentanil for post-caesarean section intravenous analgesia: a randomised, placebo-controlled study. Eur J Anaesthesiol. 2014;31(4):197–203. doi:10.1097/EJA.0000000000000011
38. Sitsen E, van Poorten F, Jansen G, Kuijpers R, Dahan A, Stienstra R. A comparison of the efficacy of levobupivacaine 0.125%, ropivacaine 0.125% and ropivacaine 0.2%, all combined with sufentanil 0.5 microg/mL, in patient-controlled epidural analgesia after hysterectomy under combined epidural and general anesthesia. Acta Anaesthesiol Belg. 2012;63(4):169–175.
39. Mendola C, Ferrante D, Oldani E, et al. Thoracic epidural analgesia in post-thoracotomy patients: comparison of three different concentrations of levobupivacaine and sufentanil. Br J Anaesth. 2009;102(3):418–423. doi:10.1093/bja/aep004
40. Boselli E, Debon R, Cimino Y, Rimmelé T, Allaouchiche B, Chassard D. Background infusion is not beneficial during labor patient-controlled analgesia with 0.1% ropivacaine plus 0.5 microg/mL sufentanil. Anesthesiology. 2004;100(4):968–972. doi:10.1097/00000542-200404000-00030
41. Hsu HW, Cheng YJ, Chen LK, et al. Differential analgesic effect of tenoxicam on the wound pain and uterine cramping pain after cesarean section. Clin J Pain. 2003;19(1):55–58. doi:10.1097/00002508-200301000-00007
42. Tunçalp O, Souza JP, Gülmezoglu M. New WHO recommendations on prevention and treatment of postpartum hemorrhage.. Int J Gynaecol Obstet. 2013;123(3):254–256. doi:10.1016/j.ijgo.2013.06.024
43. Apfel CC, Läärä E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91(3):693–700. doi:10.1097/00000542-199909000-00022
44. Molassiotis A, Coventry PA, Stricker CT, et al. Validation and psychometric assessment of a short clinical scale to measure chemotherapy-induced nausea and vomiting: the MASCC antiemesis tool. J Pain Symptom Manage. 2007;34(2):148–159. doi:10.1016/j.jpainsymman.2006.10.018
45. Wengritzky R, Mettho T, Myles PS, Burke J, Kakos A. Development and validation of a postoperative nausea and vomiting intensity scale. Br J Anaesth. 2010;104(2):158–166. doi:10.1093/bja/aep370
46. Sinatra RS, Lodge K, Sibert K, et al. A comparison of morphine, meperidine, and oxymorphone as utilized in patient-controlled analgesia following cesarean delivery. Anesthesiology. 1989;70(4):585–590. doi:10.1097/00000542-198904000-00005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sufentanil Combined with Nalbuphine via Patient-Controlled Intravenous Analgesia After Cesarean Section: A Retrospective Evaluation
Wang L, Wang Y, Ma Y, Mu X, Zhang Z, Wang H, Zheng Z, Nie H
Drug Design, Development and Therapy 2022, 16:3711-3721
Published Date: 21 October 2022
Sufentanil-Dezocine Combination in Patient-Controlled Intravenous Analgesia for Postoperative Pain After Pancreatic Cancer Surgery: A Retrospective Propensity Score-Matched Study
Huang Z, Li J, Xia Y, Li Q, Song X, Xu X, Luo Y
Journal of Pain Research 2025, 18:5523-5531
Published Date: 21 October 2025
Effect of Oliceridine Combined with Sufentanil on Patient-Controlled Intravenous Analgesia in Elderly Patients After Laparoscopic Radical Resection of Rectal Cancer: A Prospective Randomized Controlled Study
Tian Y, Hu J, Pan H, Bai G, Zhang Z, Zhang P
Drug Design, Development and Therapy 2025, 19:10033-10043
Published Date: 8 November 2025