Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Oliceridine Combined with Sufentanil on Patient-Controlled Intravenous Analgesia in Elderly Patients After Laparoscopic Radical Resection of Rectal Cancer: A Prospective Randomized Controlled Study
Authors Tian Y, Hu J ![]() , Pan H, Bai G, Zhang Z, Zhang P
, Pan H, Bai G, Zhang Z, Zhang P
Received 1 August 2025
Accepted for publication 25 October 2025
Published 8 November 2025 Volume 2025:19 Pages 10033—10043
DOI https://doi.org/10.2147/DDDT.S553848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Solomon Tadesse Zeleke
Yifu Tian, Jiarui Hu, Haitao Pan, Guang Bai, Zhao Zhang, Peng Zhang
Department of Anesthesiology, Tianjin Cancer Hospital Airport Hospital, National Clinical Research Center for Cancer, Airport Economic Zone, Tianjin, 300308, People’s Repulic of China
Correspondence: Peng Zhang, Department of Anesthesiology, Tianjin Cancer Hospital Airport Hospital, National Clinical Research Center for Cancer, Airport Economic Zone, Tianjin, 300308, People’s Repulic of China, Email [email protected]
Background: Currently, there is no report on the efficacy evaluation of oliceridine in patient - controlled intravenous analgesia (PCIA) for elderly patients after surgery. This study aims to investigate the analgesic effect of oliceridine combined with sufentanil under the PCIA treatment mode.
Methods: A total of 112 patients were randomly assigned to the sufentanil group (Group S), the oliceridine group (Group O), and the oliceridine + sufentanil group (Group Z). Patients in Group S received 2.0 μg/kg sufentanil; those in Group O received 0.35 mg/kg oliceridine; and patients in Group Z received 1.0 μg/kg sufentanil + 0.35 mg/kg oliceridine. The visual analogue scale (VAS) for pain at rest and during activity within 48 hours after surgery were used as the primary outcome indicators. The secondary observation indicators include the Athens Insomnia Scale (AIS) score for postoperative sleep quality, the number of times the analgesia pump is pressed within 48 hours after surgery, the situation of rescue analgesia, and the occurrence of adverse events.
Results: Among the 112 patients analyzed, the combination of oliceridine and sufentanil significantly reduced the VAS scores for pain at rest and during activity within 48 hours after surgery (p < 0.01), and had the lowest incidence rates of postoperative nausea and vomiting (PONV) and respiratory depression (p < 0.05). Meanwhile, this combination regimen significantly decreased the AIS scores (P < 0.001), the times of analgesia pump pressing (p < 0.01), the times of rescue analgesia (p < 0.05), and the rescue analgesia rate (P < 0.001).
Conclusion: In the pain management after laparoscopic radical resection of rectal cancer in elderly patients, oliceridine combined with sufentanil provides the best analgesic effect and has the lowest incidence of adverse reactions associated with opioids.
Keywords: oliceridine, patient-controlled intravenous analgesia, laparoscopic surgery, visual analog scale, elderly patient
Introduction
The International Association for the Study of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.”1 Despite advancements in predicting and managing postoperative pain, many patients continue to endure moderate to severe pain after surgery. Studies from various countries indicate that about 50% of patients experience such pain within the first 24 hours post-surgery.2
Laparoscopic surgery, a minimally invasive type of radical resection of the rectum, involves smaller incisions and less trauma than traditional surgical methods. Despite its advantages, severe postoperative pain may result, frequently due to the abdominal wall and viscera. Furthermore, insufflation of carbon dioxide during the procedure may result in shoulder pain, which can be understood on the basis of muscular traction and stretch effects.3 Postoperative pain may lead to a wide range of complications such as enhanced anxiety, sleep abnormalities, suppression of the immune system, and limitations in early postoperative activity and food and fluid intake. Complications can compromise comfort and patient satisfaction in the perioperative period and prolong hospital stays and medical costs.4 Therefore, it is crucial to effectively manage acute pain.
In the context of enhanced recovery after surgery (ERAS), multimodal analgesia is promoted, employing a combination of pain management techniques to ensure effective relief while minimizing opioid-related side effects.5 Patient-Controlled Intravenous Analgesia(PCIA) is becoming increasingly a field of concern in anesthesiology. Patient-controlled intravenous analgesia remains a widely accepted element of multimodal analgesia for postoperative pain, garnering high satisfaction from both patients and medical staff. Opioids, despite their frequent use due to their efficacy in alleviating even severe pain, continue to be the cornerstone of postoperative pain management.6 Sufentanil, with its high efficacy and rapid onset but short duration, is most frequently utilized in PCIA regimens.7 Nevertheless, it carries notable risks and adverse effects. Activation of μ receptors in the brainstem respiratory center and intestines is linked to postoperative nausea and vomiting (PONV), respiratory depression, and constipation due to their distribution in these areas.8 A study involving elderly patients undergoing hip replacement with preventive PCIA found higher rates of PONV and respiratory depression in the sufentanil group.9 However, its administration in a single form for use as an analgesic is limited, in consideration of its side effects including respiratory depression, nausea, emesis, bradycardia, syncope, hypotension, and constipation.10 Sufentanil is therefore most frequently blended with a mixture of drugs in an effort to maximize its analgesia and minimize its side effects.
G protein-biased agonists at opioid receptors are a new class of drugs increasingly appreciated for selectively acting through G protein-dependent routes. By selectively acting through G proteins, β-arrestin pathway activation is diminished, and effective pain relief with fewer side effects is produced.11 Oliceridine, an innovative G protein-biased agonist, exhibits a distinctive safety profile that differentiates it from traditional opioids, demonstrating potential in clinical trials for its analgesic effectiveness and minimized side effects.12 Neil K. Singla and colleagues’ findings indicated that the 0.35mg oliceridine cohort exhibited superior safety and tolerability regarding adverse gastrointestinal and respiratory responses.13 Sergio D Bergese and co-authors’ research further validated oliceridine’s overall safety and tolerability for managing acute moderate to severe pain.14 Notably, oliceridine does not necessitate dose adjustments in patients with renal impairment, although adjustments for frequency may be necessary in those with mild to moderate hepatic impairment.15
There are no existing studies, domestically or internationally, on the safety and efficacy of oliceridine, either alone or combined with other analgesics, for postoperative PCIA in elderly patients. The diminished physiological functions and high incidence of chronic illnesses in this population, coupled with their reduced pain tolerance, complicate the choice of postoperative analgesia regimens. Although most safety data for oliceridine comes from preclinical studies or trials where adverse reactions were only secondary considerations, there remains a significant gap in clinical evidence regarding its analgesic efficacy and safety.12 Therefore, we explored the analgesic effect of oliceridine combined with sufentanil for PCIA in elderly patients after laparoscopic radical resection of rectal cancer., comparing it with sufentanil to assess its influence on postoperative adverse reactions and to propose a new approach for PCIA.
Materials and Methods
Study Design and Patient Enrollment
This study (EC-2024-010A) was approved by the Ethics Committee of Airport Hospital of Tianjin City Cancer Hospital in accordance with the Declaration of Helsinki. Informed consent was obtained from all patients. The study enrolled patients who underwent laparoscopic radical resection for rectal cancer at the hospital from January 2025 to March 2025. The trial is registered with the China Clinical Research Information Center (ChiCTR2400094171).
Participants
The trial’s eligibility criteria included voluntary participation, individuals aged 60–80 years, BMI between 18.5 and 24 kg/m2, and ASA classes I–III. Exclusion criteria encompassed uncontrolled or untreated hypertension, severe cardiovascular and cerebrovascular conditions, significant respiratory and circulatory disorders, neurological, mental, or psychological disorders, history of chronic pain, notable liver and kidney impairment, lung infection, bleeding tendency, and hyperthyroidism. Further exclusion criteria comprised postoperative ICU transfer, intraoperative conversion to laparotomy, postoperative bleeding, reoperation within 48 hours post-surgery, severe perioperative complications such as anaphylactic shock, myocardial infarction, or stroke, as well as non-cooperation or withdrawal during the study.
Randomization and Blinding
A computer-generated randomization sequence assigned patients in a 1:1:1 ratio to three groups: Sufentanil (group S), Oliceridine (group O), and Oliceridine + sufentanil (group Z). Group assignments were concealed using sequentially numbered envelopes sealed in opaque covers. Blinding procedures were applied to surgeons, patients, data collectors, and analysts to maintain confidentiality. It is important to note that the principal anesthesiologist was not blinded throughout the study.Unblinding was allowed only in the event of serious adverse events (eg respiratory depression) requiring clear treatment, after which the patient was withdrawn from the study.
Anesthetic Management
One day before surgery, patients were thoroughly instructed on the use of the analgesic pump and the VAS, until they became proficient. Patients were also advised to mobilize as soon as postoperative pain became tolerable.
Upon entering the operating room, patients underwent monitoring for non-invasive blood pressure, blood oxygen saturation, electrocardiogram, PETCO2, and bispectral index (BIS) until their exit. The process of anesthesia induction involved the administration of Remimazolam at 0.1 mg/kg, alongside sufentanil ranging from 0.3 to 0.5 µg/kg, cisatracurium at 0.15 mg/kg, and etomidate within the range of 0.2 to 0.3 mg/kg. Once the BIS value stabilized between 40 and 50 for one minute, anesthesia was maintained, leading to the initiation of endotracheal intubation and the connection of the patient to the anesthesia machine for volume-controlled ventilation. The parameters for ventilation were modified to include a tidal volume of 6–8 mL/kg, a respiratory rate ranging from 10 to 15 breaths per minute, PEEP set between 4 and 8 mmHg, and an oxygen concentration maintained at 30% to 50%. The parameters were actively regulated to sustain PETCO2 within the range of 35–45 mmHg, keep airway pressure under 30 cmH2O, and ensure SPO2 remained above 90%. Before the surgical procedure, all groups were administered an intravenous dose of sufentanil at 0.1 µg/kg. The administration of total intravenous anesthesia involved the continuous infusion of ciprofol at 3–6 mg/(kg·h) alongside remifentanil at 0.1–0.2 μg/(kg·min). Throughout the procedure, blood pressure was carefully regulated to remain within 20% of baseline values, while the BIS was maintained between 40 and 60. The procedure involved continuous monitoring of body temperature using a nasopharyngeal temperature probe. Thirty minutes prior to the completion of the surgical procedure, sufentanil (0.1 µg/kg) was delivered intravenously to serve as an analgesic intermediary. Postoperatively, 4 mg of tropisetron was administered to prevent nausea, coupled with a combination of neostigmine (0.04 mg/kg) and atropine (0.02 mg/kg) to reverse muscle relaxation. Once BIS exceeded 70, patients were encouraged to stay awake until eye opening was observed. Patients eligible for awake extubation had their endotracheal tubes removed and were transferred to the recovery room.
Interventions and Postoperative Management
Postoperative pain management was conducted using PCIA (ZB100-II, Jiangsu, China) for all subjects. Participants were randomly assigned to three groups: group S received sufentanil 2μg/kg,7 group O received Oliceridine 0.35 mg/kg,16,17 and group Z received Oliceridine 0.35 mg/kg combined with sufentanil 1μg/kg. The PCIA settings consisted of a background infusion of 2mL/h, a lockout interval of 15 minutes, and a self-administered dose of 0.5 mL. Patients were briefed on the PCIA procedure during pre-anesthetic consultations and instructed to activate the system when in pain. PCIA was maintained until discharge, depletion of fluids without requesting additional PCIA, or discontinuation due to adverse reactions. In instances where a VAS score of 3 persisted despite PCIA activation, intravenous tramadoxin 5 mg was administered as a rescue analgesic. Patients with a PONV score of ≥2 received intravenous metoclopramide 10 mg.
Outcome Measures
The main efficacy endpoints comprised Visual Analogue Scale(VAS)scores measured at rest and during movement at intervals of 3, 6, 12, 24, and 48 hours following surgery, aimed at assessing pain levels, with scores spanning from 0 (indicating no pain) to 10 (representing severe intolerable pain).
Secondary endpoints in the study encompassed the total and effective number of analgesic pump activations within 48 hours post-surgery (defined as the maximum permissible presses within a 15-minute lockout period), requirement for rescue analgesia, Athens Insomnia Scale (AIS) scores on postoperative days 1 and 2, and occurrence of adverse events such as PONV, respiratory depression (SPO2 <90%), skin itch and shivering. Sleep quality was assessed using the AIS, ranging from (indicating no sleep disturbances) to 24 (reflecting severe insomnia). Each press of the analgesic pump dispensed 0.5 mL of medication promptly upon activation, with a maximum frequency of 4 presses per hour. Higher rates of effective pump activations signify suboptimal analgesic efficacy and increased demand for pain relief.
Sample Size Estimation
The study assessed rest pain scores as the primary outcome and categorized participants into three groups. Sample size calculation utilized PASS 15 software (NCSS, Caseville, Utah, USA). Based on preliminary findings, post-treatment mean pain scores for groups S, O, and Z were 0.84±0.66, 1.25±0.72, and 1.54±0.85, respectively. Employing a two-sided α of 0.05 and power of 0.80, the “One-Way Analysis of Variation F-Tests” function in PASS 15 determined a minimum of 35 subjects per group. Accounting for a 10% dropout rate, 128 patients were initially enrolled, with 112 included in the final analysis.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS, Inc., USA). The normality of continuous variables was assessed with the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation (SD) and analyzed using one-way analysis of variance (ANOVA) with Bonferroni post-hoc corrections. Non-normally distributed data were expressed as mean ± SD and compared using the Kruskal–Wallis H-test, with pairwise comparisons adjusted using the Dunn-Bonferroni method. Fisher’s exact test was utilized to compare the incidence of postoperative adverse events.
Results
Comparison of Demographic Information
A total of 128 patients underwent initial assessment for eligibility, with 8 patients subsequently excluded: 5 for failing to meet inclusion criteria and 3 for declining participation. The remaining 120 patients were evenly randomized into three groups (S, O, and Z). During the allocation phase, 3 patients in group S and 3 in group O did not receive the designated intervention due to changes in surgical plans. Throughout the follow-up period, 1 patient in group S was lost due to postoperative bleeding, and 1 patient in group Z was lost due to an extended stay in the ICU. Ultimately, 112 patients were included in the final analysis: 36 in group S, 37 in group O, and 39 in group Z. The progression of patient enrollment, allocation, follow-up, and analysis is delineated in the CONSORT flowchart (Figure 1).
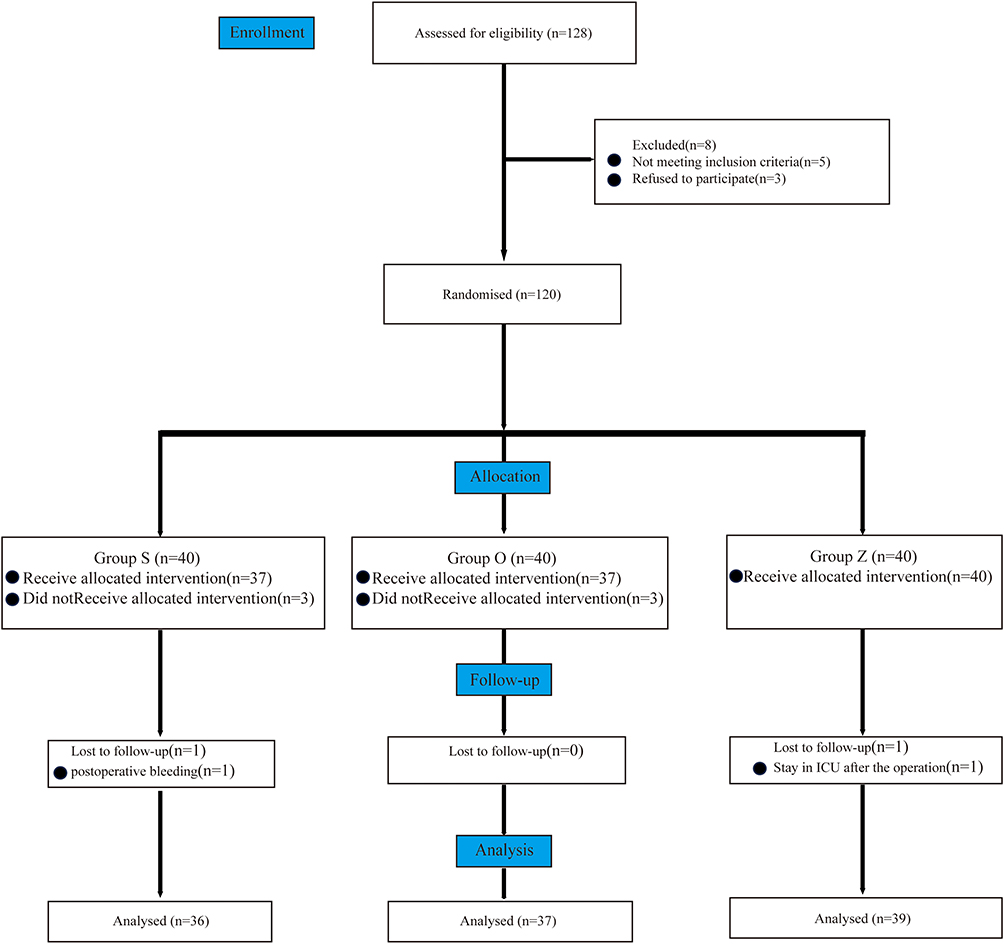 |
Figure 1 CONSORT flow diagram. Abbreviation: CONSORT, Consolidated Standards of Reporting Trials; S group, Sufentanil group; O group-Oliceridine group; Z group, Sufentanil +Oliceridine group. |
The demographic characteristics of the 112 patients distributed in the three treatment groups were similar (Table 1) and no differences were noted between males and females (P =0. 579), age (P=0. 978), BMI (P=0. 847), Surgery Duration (P=0. 869), Sufentanil (P =0. 984), Remifentanil (P =0. 628),and ASA classification (P=0. 760). These data indicate that the baseline differences between the groups were not significant, verifying the appropriateness of further comparisons.
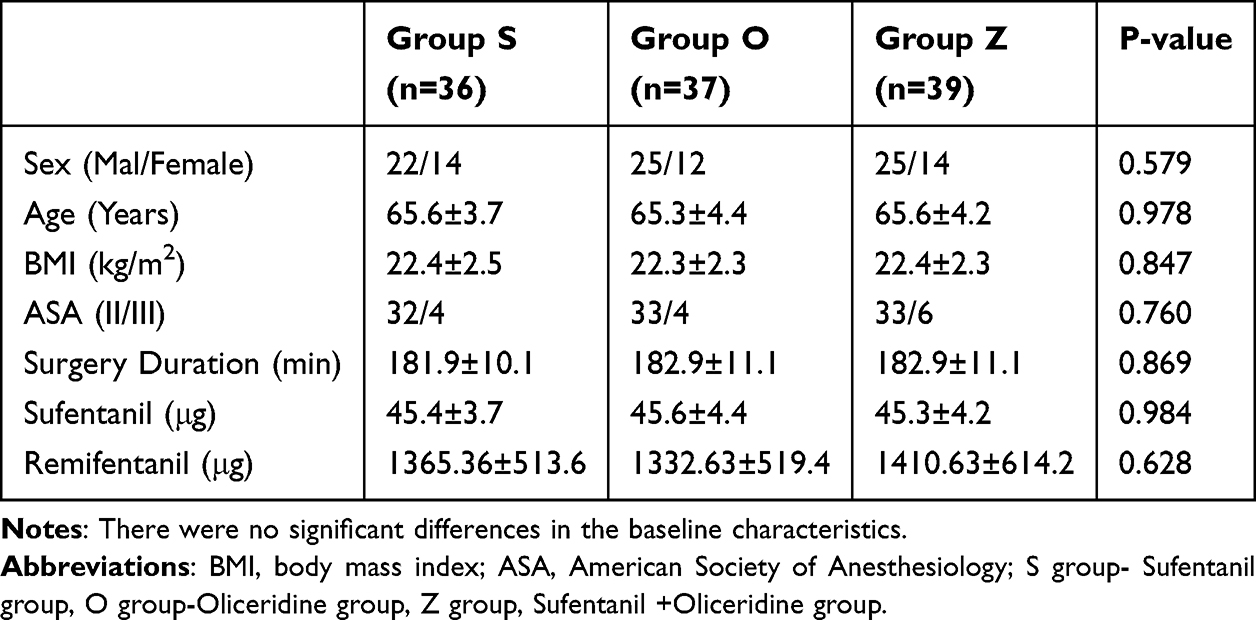 |
Table 1 Basic Characteristics, Surgical Information of the Patients and Total Perioperative Opioid Consumption |
General Condition of Postoperative Recovery
Statistical analysis revealed no significant differences among the three groups concerning extubation time, awakening time, and Post Anesthesia Care Unit.(PACU)duration (P>0.05) (Table 2).
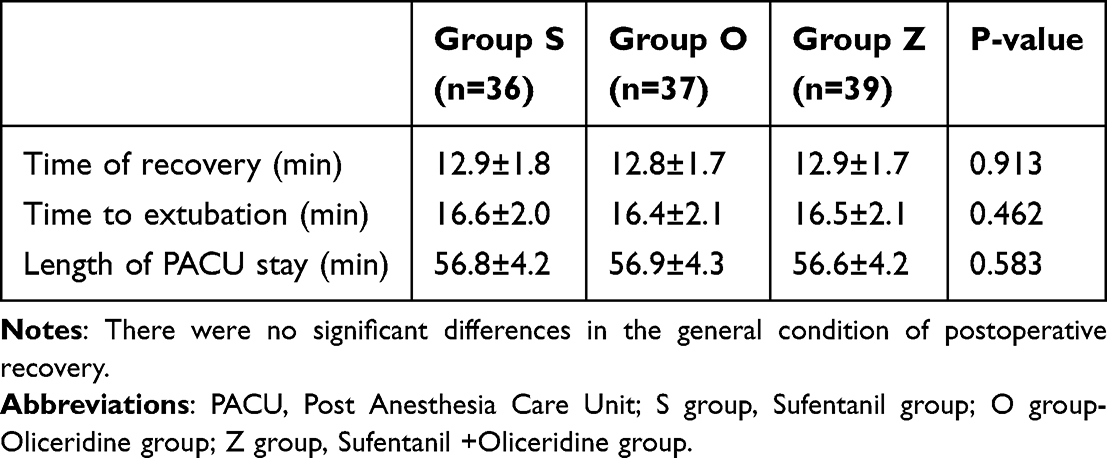 |
Table 2 Postoperative Recovery General Condition |
General Condition of Postoperative Pain
Figure 2 illustrates the comparison of VAS scores at various postoperative time points during rest and activity. The VAS scores for all three patient groups exhibited a decreasing trend from 3 to 48 hours postoperatively. Group Z demonstrated significantly lower VAS scores during both rest and activity at 3, 6, 12, 24, and 48 hours post-surgery compared to Group O (P < 0.001). Moreover, within the initial 48 hours post-surgery, Group Z exhibited a significant reduction in both the total number of presses and effective presses of the analgesia pump compared to Group O (P <0.001). Additionally, Group Z showed a decrease in the frequency of rescue analgesia and the number of required rescue analgesia interventions compared to Group O (P <0.001) (refer to Tables 3 and 4). There were no significant disparities in VAS scores, total number of presses and effective presses of the analgesia pump, and frequency of rescue analgesia between Group S and Group Z within the first 48 hours post-surgery.
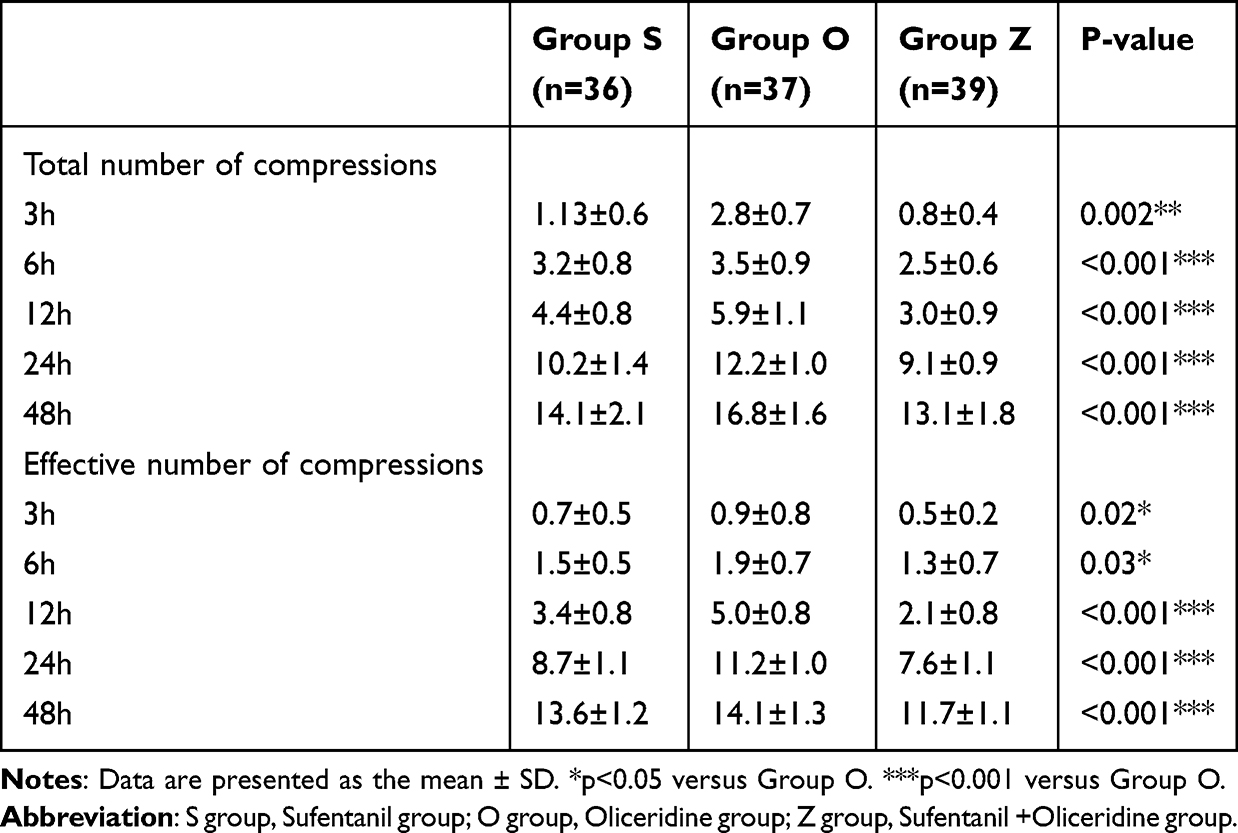 |
Table 3 Comparison of the Total Number of Presses and Effective Number of Presses of the Analgesia Pump at Different Time Points Among the Three Groups of Patients |
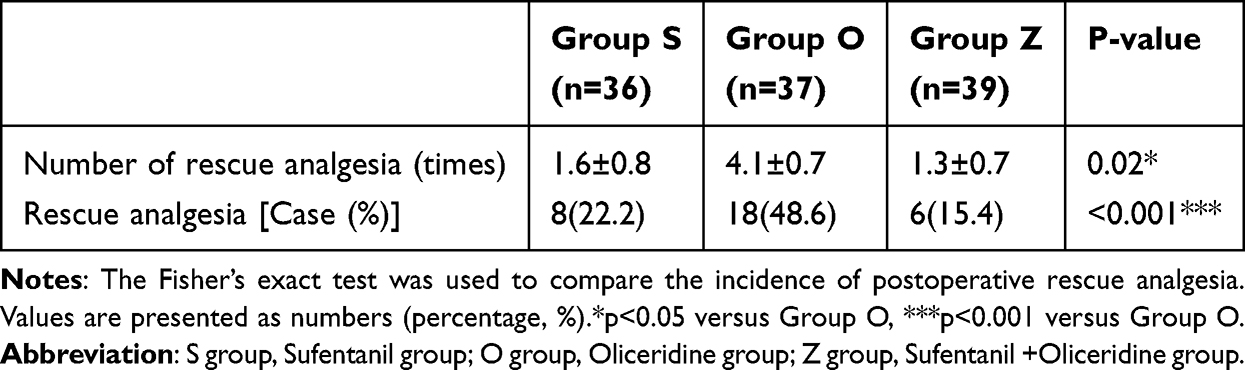 |
Table 4 Comparison of Rescue Analgesia Within 48 Hours After Surgery Among the Three Groups of Patients |
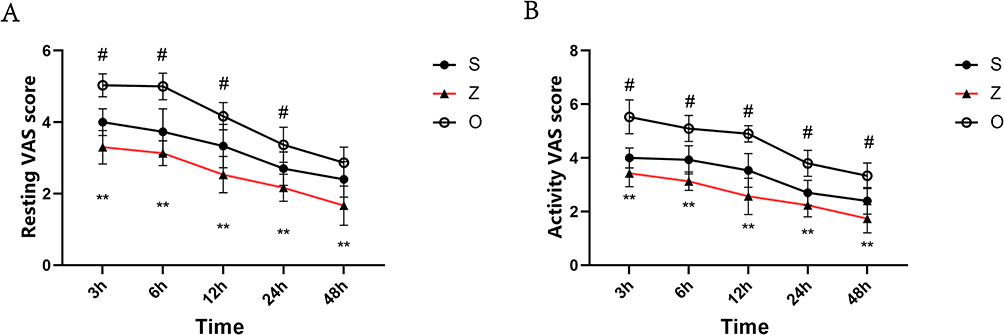 |
Figure 2 Comparison of VAS scores at rest and activity at 3h, 6h, 12h, 24h and 48h after operation among three groups. (A) Comparison of VAS scores at rest at different time points after operation among three groups; (B) Comparison of VAS pain scores during activity at different time points after surgery among the three groups of patients; **: P<0.01 versus Group O; #: P<0.05 versus Group S. Abbreviations: VAS, Visual Analogue Scale; S group, Sufentanil group; O group, Oliceridine group; Z group, Sufentanil +Oliceridine group. |
Sleep Quality
The detailed information regarding the postoperative AIS scores is presented in Figure 3. There was no statistically significant difference in the AIS scores among the three groups of patients in the first month (P > 0.05). The AIS scores of all three groups of patients increased significantly on the first day after surgery, with a remarkable increase in the O group (P < 0.001). The AIS scores of all three groups of patients showed a downward trend on the second day after surgery compared to the first day before surgery. The AIS scores of the S and Z groups decreased significantly on the second day after surgery compared with the O group (P < 0.001).
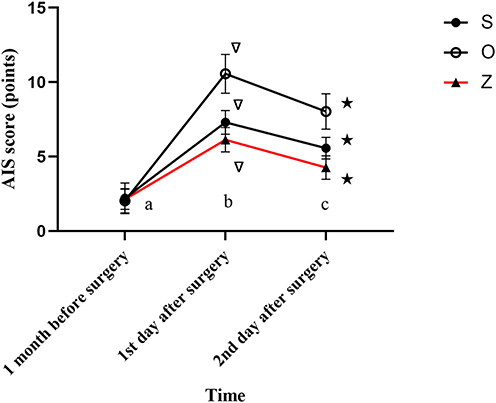 |
Figure 3 The Arthritis Impact Measurement Scales (AIS) scores were compared across three patient groups at different time points. Comparison of AIS scores at three different time points. aP = 0.756, bP < 0.001, cP < 0.001, compared with Group O; ▽P < 0.001, compared with 1 month before surgery; ★P < 0.001, compared with 1 day before surgery. Abbreviations: AIS, Athens Insomnia Scale; S group, Sufentanil group; O group, Oliceridine group; Z group, Sufentanil +Oliceridine group. |
Adverse Reactions
The information related to adverse events within 48 hours after surgery in the three groups of patients is detailed in (Table 5). The incidence of postoperative PONV in the S group was significantly higher than that in the O group and the Z group (P < 0.05). The incidence of postoperative shivering in the O group was significantly higher than that in the S group and the Z group (P < 0.01). However, there were no significant differences in the incidences of respiratory depression, skin itch, and dizziness among the three groups.
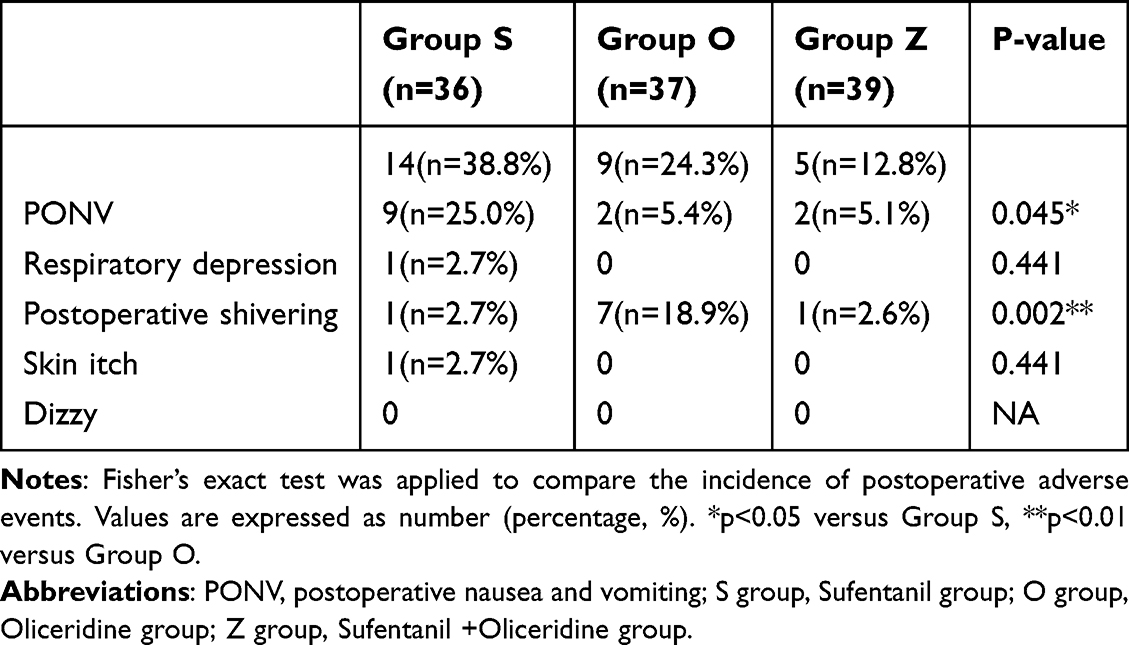 |
Table 5 Comparison of Adverse Reactions Within 48 Hours After Operation Among Three Groups |
Discussion
The results demonstrated that the combination of 1.0 µg/kg sufentanil with 0.35 mg/kg oliceridine for postoperative analgesia after laparoscopic rectal cancer resection yielded superior analgesic effects compared to the use of either sufentanil or oliceridine alone. VAS scores at rest and during activity at 3, 6, 12, 24, and 48 hours post-surgery were significantly lower, AIS scores were significantly decreased, the total number and effective presses of the analgesic pump within 48 hours post-surgery were significantly reduced, and both the number of rescue analgesia interventions and the incidence of postoperative adverse reactions were significantly decreased.
In current the enhanced recovery after surgery (ERAS) clinical practice, multimodal analgesia management is an important aspect of ERAS,18 which can significantly reduce postoperative complications and promote functional recovery. Recent international studies have compared oliceridine with traditional opioids such as morphine,13,19 However, currently, sufentanil is mainly used as the core drug for clinical postoperative pain management. Therefore, this study focused on observing the analgesic effect of oliceridine combined with sufentanil. The study by Manman Yao et al17 found that that sufentanil might be associated with an increased occurrence of respiratory depression, skin itch, and PONV, potentially impeding swift postoperative recovery.20 Our observations correspond with these reports, revealing a heightened occurrence of postoperative complications, including PONV and skin itch, in the sufentanil-alone cohort within 48 hours following surgery. Oliceridine demonstrates enhanced pain relief while minimizing side effects through the selective activation of G-protein signaling pathways and the reduction of β-arrestin activation,11 as reported by Markham A et al. In alignment with the observations made by Singla et al21 our research indicates that oliceridine, whether administered alone or in conjunction with sufentanil, markedly reduces the occurrence of adverse reactions within the 48-hour postoperative period. Additionally, oliceridine has demonstrated good tolerance and safety in elderly patients and those with comorbidities, significantly lowering the risk of respiratory depression in high-risk groups.
Effective management of postoperative pain is crucial within the first 48 hours after surgery. Due to the scheduling requirements of postoperative follow - up, patients who needed to be evaluated late at night or early in the morning were excluded. Notably, within 48 hours after surgery, compared with the S group, the O group had significantly higher VAS scores at rest and during movement, a significantly increased AIS score on the first postoperative day, an increased total number of analgesic pump presses, an increased rate of postoperative rescue analgesia, and a significantly increased incidence of postoperative shivering. Currently, multiple hypotheses have been proposed to explain the occurrence of post - anesthesia shivering. These hypotheses include perioperative hypothermia, postoperative pain, etc.22–24 Notably, numerous studies have confirmed that μ receptor agonists can inhibit post - anesthesia shivering, and in the postoperative stage, the threshold temperature of post - anesthesia shivering is linearly correlated with the plasma sufentanil concentration.25 However, the incidence of adverse reactions such as postoperative respiratory depression and PONV was significantly reduced. This indicates that although the sole use of oliceridine may reduce the occurrence of adverse reactions associated with opioids, it may not provide effective analgesia. In contrast, in the Z group, the postoperative VAS scores, AIS scores, number of analgesic pump presses, number of rescue analgesia events, and incidence of postoperative shivering were significantly reduced. This suggests that the combined use of oliceridine and sufentanil can improve the insufficient analgesic effect of oliceridine used alone, without a significant increase in adverse reactions.Timothy et al26 found that by selectively targeting the G-protein pathway following activation of μ-opioid receptors, these drugs could reduce many adverse reactions associated with traditional opioids like morphine and fentanyl. This finding aligns with international research, which suggests that oliceridine, especially at lower doses, can enhance the safety of opioid drugs by targeting the G-protein pathway. However, this selectivity may diminish at higher doses.27 Oliceridine can also cause side effects such as headache, which are dose-dependent.28 No significant occurrence of these adverse events was observed in our study.
This study has several limitations. First, it is a single - center study with a relatively small sample size, including only elderly patients from one hospital. This limitation may affect the generalizability of our study results. Whether oliceridine combined with sufentanil can ensure the same analgesic effect and lower adverse reactions in other special groups such as the obese needs to be further verified in multi - center studies. Second, the assessment of pain intensity and sleep quality is subjective, relying on the perceptions of patients and medical staff, which may introduce bias. In addition, the optimal dose of oliceridine has not been determined and requires further research. The observation period is limited to 48 hours, which restricts the understanding of the long - term clinical significance of the study results. Currently, few clinical studies have explored the analgesic effect of oliceridine or oliceridine combined with other analgesics for PCIA in postoperative patients. Most existing studies are narrative evaluations or are based on retrospective and post hoc analyses conducted in specific surgical settings like abdominoplasty and bunionectomy, often treating adverse reactions as secondary outcomes.29–31 Comprehensive investigations employing larger sample sizes and varied methodologies are essential to confirm the efficacy and safety of oliceridine in the context of postoperative pain management.
Conclusion
Compared with the use of oliceridine or sufentanil alone, the combination of oliceridine and sufentanil for PCIA after laparoscopic radical resection of rectal cancer in elderly patients shows significant efficacy. Meanwhile, it can minimize the risks of postoperative PONV, postoperative shivering, and respiratory depression.
Abbreviations
PCIA, Patient-Controlled Intravenous Analgesia; VAS, Visual Analogue Scale; AIS, Athens Insomnia Scale; BIS, Bispectral Index; BMI, Body Mass Index; ICU, Intensive Care Unit; ASA, American Society of Anesthesiologists; PACU, Post Anesthesia Care Unit; ERAS, enhanced recovery after surgery.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Author Contributions
All authors have made substantial contributions to the reported research work, whether in the aspects of conceptualization, study design, implementation, data collection, analysis and interpretation, or in all of these areas; participated in the drafting, revision or rigorous review of the article; given final approval to the version to be published; agreed to submit the article to this journal; and agreed to be accountable for all aspects of the research work.
Funding
This research was supported by the Bethune Foundation (TJM2024-007).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Kummer I, Lüthi A, Klingler G, et al. Adjuvant analgesics in acute pain – evaluation of efficacy. Curr Pain Headache Rep. 2024;28(9):843–852. doi:10.1007/s11916-024-01276-w
2. Motamed C. Clinical update on patient-controlled analgesia for acute postoperative pain. Pharmacy. 2022;10(1):22. doi:10.3390/pharmacy10010022
3. Gin E, Lowen D, Tacey M, Hodgson R. Reduced laparoscopic intra-abdominal pressure during laparoscopic cholecystectomy and its effect on post-operative pain: a double-blinded randomised control trial. J Gastrointestinal Surg. 2021;25(11):2806–2813. doi:10.1007/s11605-021-04919-0
4. Sánchez-Iglesias JL, Gómez-Hidalgo NR, Pérez-Benavente A, et al. Importance of enhanced recovery after surgery (ERAS) protocol compliance for length of stay in ovarian cancer surgery. Ann Surg Oncol. 2021;28(13):8979–8986. doi:10.1245/s10434-021-10228-2
5. Duan G, Bao X, Yang G, et al. Patient-controlled intravenous tramadol versus patient-controlled intravenous hydromorphone for analgesia after secondary cesarean delivery: a randomized controlled trial to compare analgesic, anti-anxiety and anti-depression effects. J Pain Res. 2018;12:49–59. doi:10.2147/JPR.S184782
6. Li X, Liu M, Chen G, Yan C. Comparison of different hydromorphone bolus doses in patient-controlled intravenous analgesia for post-laparoscopic surgery: a randomized controlled trial. BMC Anesthesiol. 2025;25(1). doi:10.1186/s12871-025-03287-5
7. Nie Z, Cui X, Zhang R, et al. Effectiveness of patient-controlled intravenous analgesia (PCIA) with sufentanil background infusion for post-cesarean analgesia: a randomized controlled trial. J Pain Res. 2022;15:1355–1364. doi:10.2147/JPR.S363743
8. Feng Y, Jia J-M, Cheng Y-X, et al. Effects of remimazolam-propofol with flumazenil reversal on the emergence time and hemodynamics of patients undergoing laparoscopic partial hepatectomy: a prospective randomized controlled trial. Drug Des Devel Ther. 2025;19:6777–6787. doi:10.2147/DDDT.S531034
9. Buvanendran A, Kroin JS. Multimodal analgesia for controlling acute postoperative pain. Curr Opin Anaesthesiol. 2009;22(5):588–593. doi:10.1097/ACO.0b013e328330373a
10. Wang L, Wang Y, Ma Y, et al. Sufentanil combined with nalbuphine via patient-controlled intravenous analgesia after cesarean section: a retrospective evaluation. Drug Des Devel Ther. 2022;16:3711–3721. doi:10.2147/DDDT.S380292
11. Markham A. Oliceridine: first Approval. Drugs. 2020;80(16):1739–1744. doi:10.1007/s40265-020-01414-9
12. Tan HS, Habib AS. Oliceridine: a novel drug for the management of moderate to severe acute pain – a review of current evidence. J Pain Res. 2021;14:969–979. doi:10.2147/JPR.S278279
13. Singla NK, Skobieranda F, Soergel DG, et al. APOLLO‐2: a randomized, placebo and active‐controlled Phase III study investigating oliceridine (TRV130), a G protein–biased ligand at the μ‐opioid receptor, for management of moderate to severe acute pain following abdominoplasty. Pain Pract. 2019;19(7):715–731. doi:10.1111/papr.12801
14. Ok HG, Kim SY, Lee SJ, Kim TK, Huh BK, Kim KH. Can oliceridine (TRV130), an ideal novel ? Receptor G protein pathway selective (?-GPS) modulator, provide analgesia without opioid-related adverse reactions? Korean J Pain. 2018;31(2):73–79. doi:10.3344/kjp.2018.31.2.73
15. Nafziger AN, Arscott KA, Cochrane K, Skobieranda F, Burt DA, Fossler MJ. The influence of renal or hepatic impairment on the pharmacokinetics, safety, and tolerability of oliceridine. Clin Pharmacol Drug Dev. 2019;9(5):639–650. doi:10.1002/cpdd.750
16. Viscusi ER, Skobieranda F, Soergel DG, Cook E, Burt DA, Singla N. APOLLO-1: a randomized placebo and active-controlled phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the µ-opioid receptor, for management of moderate-to-severe acute pain following bunionectomy. J Pain Res. 2019;Volume 12:927–943. doi:10.2147/JPR.S171013
17. Yao M, Fang B, Yang J, Chen P, Chen F. Esketamine combined with sufentanil versus sufentanil in patient-controlled intravenous analgesia: a meta-analysis. Front Pharmacol. 2024;15:1247646.
18. Forster C, Gonzalez M. Enhanced recovery after surgery (ERAS): philosophy, theory and practice. J Thoracic Dis. 2022;14(10):3684–3687. doi:10.21037/jtd-2022-13
19. Bergese SD, Brzezinski M, Hammer GB, et al. ATHENA: a Phase 3, open-label study of the safety and effectiveness of oliceridine (TRV130), A G-protein selective agonist at the μ-opioid receptor, in patients with moderate to severe acute pain requiring parenteral opioid therapy. J Pain Res. 2019;12:3113–3126. doi:10.2147/JPR.S217563
20. Hutchings C, Yadav K, Cheung WJ, Young T, Sikora L, Eagles D. A systematic review of sufentanil for the management of adults with acute pain in the emergency department and pre-hospital setting. Am J Emergency Med. 2023;70:10–18. doi:10.1016/j.ajem.2023.04.020
21. Singla N, Minkowitz H, Soergel D, et al. A randomized, Phase IIb study investigating oliceridine (TRV130), a novel µ-receptor G-protein pathway selective (µ-GPS) modulator, for the management of moderate to severe acute pain following abdominoplasty. J Pain Res. 2017;10:2413–2424. doi:10.2147/JPR.S137952
22. Wang Y, Zhao K, Wu N, et al. Effect of different doses of butorphanol on postoperative shivering in elderly patients: a randomized, double-blind, placebo-controlled trial. Drug Des Devel Ther. 2023;17:839–849. doi:10.2147/DDDT.S396309
23. Koo JM, Chung Y-J, Lee M, Moon YE. Efficacy of dexmedetomidine vs. remifentanil for postoperative analgesia and opioid-related side effects after gynecological laparoscopy: a prospective randomized controlled trial. J Clin Med. 2023;12(1):350. doi:10.3390/jcm12010350
24. Jin W, Wang J, Cao H, Shen X, Yang Y, Lv L. Effects of sufentanil on immune response, pain mediators and brain-sparing effect in patients with breast cancer undergoing radical mastectomy. BMC Surg. 2025;25(1). doi:10.1186/s12893-025-02814-y
25. Alfonsi P, Hongnat JM, Lebrault C, Chauvin M. The effects of pethidine, fentanyl and lignocaine on postanaesthetic shivering. Anaesthesia. 2007;50(3):214–217. doi:10.1111/j.1365-2044.1995.tb04559.x
26. Beard TL, Michalsky C, Candiotti KA, et al. Oliceridine is associated with reduced risk of vomiting and need for rescue antiemetics compared to morphine: exploratory analysis from two Phase 3 randomized placebo and active controlled trials. Pain Ther. 2020;10(1):401–413. doi:10.1007/s40122-020-00216-x
27. Ayad S, Demitrack MA, Burt DA, et al. Evaluating the incidence of opioid-induced respiratory depression associated with oliceridine and morphine as measured by the frequency and average cumulative duration of dosing interruption in patients treated for acute postoperative pain. Clin Drug Invest. 2020;40(8):755–764. doi:10.1007/s40261-020-00936-0
28. Mafi A, Kim S-K, Goddard WA. Mechanism of β-arrestin recruitment by the μ-opioid G protein-coupled receptor. Proc Natl Acad Sci. 2020;117(28):16346–16355. doi:10.1073/pnas.1918264117
29. Tan HS, Habib AS. Safety evaluation of oliceridine for the management of postoperative moderate-to-severe acute pain. Expert Opin Drug Saf. 2021;20(11):1291–1298. doi:10.1080/14740338.2021.1965989
30. Ji K, Gong X, Luan T, Gao X, Zang B. Pain management of nalbuphine and sufentanil in patients admitted intensive care unit of different ages. BMC Emerg Med. 2022;22(1). doi:10.1186/s12873-022-00592-x
31. Viscusi ER. A critical review of oliceridine injection as an IV opioid analgesic for the management of severe acute pain. Expert Rev Neurotherapeutics. 2022;22(6):419–426. doi:10.1080/14737175.2022.2072731
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Patient-Controlled Intravenous Analgesia (PCIA) with Sufentanil Background Infusion for Post-Cesarean Analgesia: A Randomized Controlled Trial
Nie Z, Cui X, Zhang R, Li Z, Lu B, Li S, Cao T, Zhuang P
Journal of Pain Research 2022, 15:1355-1364
Published Date: 6 May 2022
Sufentanil Combined with Nalbuphine via Patient-Controlled Intravenous Analgesia After Cesarean Section: A Retrospective Evaluation
Wang L, Wang Y, Ma Y, Mu X, Zhang Z, Wang H, Zheng Z, Nie H
Drug Design, Development and Therapy 2022, 16:3711-3721
Published Date: 21 October 2022
A Comparative Evaluation of the Safety and Efficacy of Oliceridine and Sufentanil in Gastrointestinal Endoscopy: A Single-Center, Randomized Controlled Trial
Ma B, Li Y, Leng C, Ji A, Zhang N, Tao X, Cao Q, Wang S
Drug Design, Development and Therapy 2025, 19:5111-5121
Published Date: 17 June 2025
Sufentanil-Dezocine Combination in Patient-Controlled Intravenous Analgesia for Postoperative Pain After Pancreatic Cancer Surgery: A Retrospective Propensity Score-Matched Study
Huang Z, Li J, Xia Y, Li Q, Song X, Xu X, Luo Y
Journal of Pain Research 2025, 18:5523-5531
Published Date: 21 October 2025
Effect of Oliceridine on the Acute Postoperative Pain Management After Elective Cesarean Delivery: A Randomized Non-Inferiority Trial
Jiang J, Yuan G, Shi Y, Zhou Z, Wang X, Sang X, Zhang X
Drug Design, Development and Therapy 2026, 20:603352
Published Date: 14 July 2026