Back to Journals » ImmunoTargets and Therapy » Volume 14
Durable Tumor Control with Multi-Organ Immune-Related Adverse Events Following Immune Checkpoint Inhibitor and Sequential Radiotherapy in Locally Advanced NSCLC: A Case Report
Authors Zhai M, Liu X, Li Y, Pi G, Bi J, Han G ![]()
Received 10 August 2025
Accepted for publication 2 December 2025
Published 10 December 2025 Volume 2025:14 Pages 1411—1417
DOI https://doi.org/10.2147/ITT.S559801
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah Wheeler
Menglan Zhai,1,* Xianwen Liu,2,* Ying Li,1 Guoliang Pi,1 Jianping Bi,1 Guang Han1
1Department of Radiation Oncology, Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Oncology, Zhongxiang Traditional Chinese Medicine Hospital, Jingmen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianping Bi, Department of Radiation Oncology, Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Tel +86-27-8767-1510, Email [email protected] Guang Han, Department of Radiation Oncology, Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Tel +86-27-8767-0023, Email [email protected]
Abstract: Combining radiotherapy (RT) with immune checkpoint inhibitors (ICIs) improves survival in stage III non-small cell lung cancer (NSCLC), though immune-related adverse events (irAEs) require vigilant management. Emerging evidence suggests multi-organ irAEs may correlate with favorable outcomes. We report a case of unresectable stage IIIA NSCLC achieving sustained partial response (PR) with progression-free survival (PFS) exceeding 42 months after one cycle of pembrolizumab-chemotherapy followed by sequential thoracic RT (50 Gy/25 fractions). Severe multi-organ irAEs (muscular, cardiovascular, respiratory, hematologic) developed but were effectively managed with corticosteroid-based therapy. Remarkably, durable tumor control persisted despite suboptimal therapeutic dosing and early systemic treatment discontinuation. This case demonstrates that RT-ICI synergy can induce robust systemic antitumor immunity even with dose-reduced RT, while severe multi-system irAEs may signal favorable prognosis. These findings support optimizing RT parameters (eg, dose de-escalation, target volume refinement) as a viable approach in the immunotherapy era.
Keywords: non-small cell lung cancer, immune checkpoint inhibitor, radiotherapy, immune-related adverse events, long-term survival
Introduction
The management of unresectable, locally advanced non‑small cell lung cancer (NSCLC) has evolved substantially through the incorporation of immune checkpoint inhibitors (ICIs) and concurrent chemoradiotherapy (cCRT). The PACIFIC trial established consolidative durvalumab following chemoradiotherapy as a standard of care, demonstrating significant survival benefits.1,2 This therapeutic synergy arises from a delicate equilibrium between enhanced antitumor immunity and off‑target toxicity. Evidence suggests that the development of multi-organ immune-related adverse events (irAEs) predicts significantly improved progression-free survival (PFS) and overall survival (OS) in patients treated with immune checkpoint inhibitors (ICIs).3,4 Mechanistic insights from single‑cell RNA sequencing studies indicate that patients with severe irAEs exhibit expanded T‑cell receptor clones that cross-react with both tumor neoantigens and healthy tissue epitopes.5 These findings provide a biological rationale linking robust antitumor efficacy to autoimmune manifestations.
This intricate link between immune activation and efficacy, coupled with the integration of ICIs, compels a fundamental reevaluation of conventional radiotherapy (RT) parameters. In the pre-immunotherapy era, the RTOG 0617 trial demonstrated that dose escalation to 74 Gy increased toxicity without improving survival compared to 60 Gy.6 In contrast, within the modern immuno-oncology paradigm, combining ICIs with RT can yield potent synergy, and emerging evidence suggests that lower radiation doses may be sufficient to initiate a robust antitumor immune response while mitigating toxicity,7 thereby directly challenging the traditional “more is better” dogma.
Here, we present a case of unresectable stage IIIA lung squamous cell carcinoma (cT4N1M0) treated with one cycle of pembrolizumab-chemotherapy followed by sequential thoracic RT (50 Gy/25 fractions). Severe sequential irAEs developed but were controlled with corticosteroids. Despite treatment discontinuation, sustained partial response (PR) with > 42-month PFS was achieved (Figure 1). This case not only reflects the interconnection between robust immune activation, multi-organ irAEs, and sustained antitumor efficacy, but also provides clinical support for RT dose optimization in contemporary immuno-oncology practice.
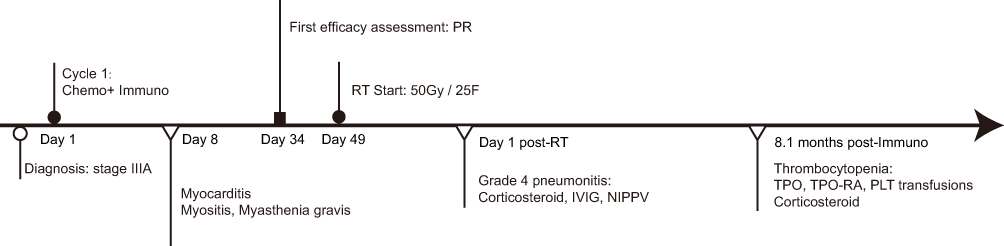 |
Figure 1 Schematic timeline of anti-tumor treatment and its immune-related adverse events. Abbreviations: Chemo, chemotherapy; Immuno, immunotherapy; PR: partial response; RT, radiotherapy; IVIG: intravenous immunoglobulin; NIPPV: non-invasive positive pressure ventilation; TPO, thrombopoietin; TPO-RA, TPO receptor agonists; PLT, platelet. |
Case Presentation
A 52-year-old male with a significant smoking history underwent contrast-enhanced chest computed tomography (CT) for a persistent cough, which demonstrated a large mass in the right upper lobe. Histopathological examination of a bronchoscopic biopsy specimen confirmed the diagnosis of squamous cell carcinoma. Subsequent staging with brain magnetic resonance imaging (MRI) and bone scintigraphy demonstrated an 8.4×6.0 cm primary tumor with direct invasion into the brachiocephalic vein and over 180° of the ascending aortic arch, along with ipsilateral hilar lymph node involvement, without evidence of distant metastasis. The disease was staged as cT4N1M0 (stage IIIA). Following multidisciplinary review, the tumor was deemed unresectable due to extensive vascular invasion. The patient received one cycle of induction therapy (paclitaxel 175 mg/m2, carboplatin AUC 5, pembrolizumab 200 mg, Day 1). Seven days post-treatment, he developed bilateral asymmetric ptosis (right > left) with diplopia, proximal muscle weakness, palpitations, and dyspnea. An urgent orbital MRI was performed, which showed normal anatomical structures without evidence of optic nerve or muscle abnormalities (Figure S1). Biochemical profiling showed profound elevation of muscle injury markers: creatine kinase (CK) peaked at 2006 U/L (ref: 38–174 U/L), CK-MB isoenzyme at 38.63 U/L (ref: 0–5 U/L), accompanied by a dynamic rise in high-sensitivity cardiac troponin I (hs-cTnI) from 0.035 to 0.512 ng/mL (ref: 0–0.04 ng/mL) over 72 hours (Figure 2). After comprehensive evaluation excluded acute myocardial infarction, common infections, and direct chemotherapy toxicity, the condition was attributed to an immune-mediated overlap syndrome (MMM syndrome) encompassing grade 2 myocarditis, grade 3 myositis, and grade 3 myasthenia gravis. The patient was promptly started on pulse methylprednisolone therapy (2 mg/kg/day), which was subsequently tapered to oral prednisone. His symptoms gradually resolved. A restaging CT scan performed in late November 2021 confirmed a partial response per RECIST 1.1 criteria, with a 38.8% reduction in the sum of target lesions (Figure 3).
 |
Figure 2 The dynamic changes in myocardial enzyme profiles following the single cycle of chemotherapy-immunotherapy. CK or CK-MB (A) and hsTnT (B). Abbreviations: CK, Creatine Kinase; CK-MB, Creatine Kinase-MB; hsTNT, high-sensitivity troponin-T. CK are multiplied by 10. |
 |
Figure 3 Representative CT images of the patient at baseline (A and B) after chemotherapy combined with immunotherapy (C and D) and at 5.1 months (E and F), 17.0 months (G and H) 28.2 months (I and J) and 39.5 months (K and L) after radiotherapy. Abbreviation: CT, Computed tomography. |
Following resolution of the initial irAEs to grade 1, the patient commenced thoracic RT. The original plan was to deliver a total dose of 60 Gy in 30 fractions (2 Gy/fraction, 5 fractions/week). Dosimetric analysis indicated acceptable pulmonary tolerance parameters [mean lung dose (MLD) 14 Gy, V20 23.2%, V5 50.3%]. However, during the fifth week of treatment (specifically, at the 24th fraction), the patient began experiencing persistent mild chest tightness. A thoracic CT revealed new bilateral scattered inflammatory infiltrates. Despite initiation of broad-spectrum antibiotics (imipenem-cilastatin), his respiratory symptoms progressed to overt dyspnea. A follow-up CT scan a few days later showed worsening, with coalescence of the bilateral inflammatory lesions. RT was immediately halted after a total delivered dose of 50 Gy, and the patient required admission to the intensive care unit (ICU). Comprehensive microbiological workup (blood cultures, respiratory viral panel, and SARS-CoV-2 RT-PCR) was negative. The pulmonary manifestations were attributed to a severe grade 4 pneumonitis, with contributions from both immune-mediated pneumonitis and radiation pneumonitis (RP) as per CTCAE v5.0 criteria. Management included high-dose methylprednisolone (4 mg/kg/day), intravenous immunoglobulin (IVIG, 20 g daily), continued anti-infective prophylaxis, and non-invasive positive pressure ventilation (NIPPV). His condition improved steadily, allowing for a gradual taper and eventual discontinuation of corticosteroids. Follow-up CT imaging confirmed the resolution of the pulmonary infiltrates (Figures 4 and S2).
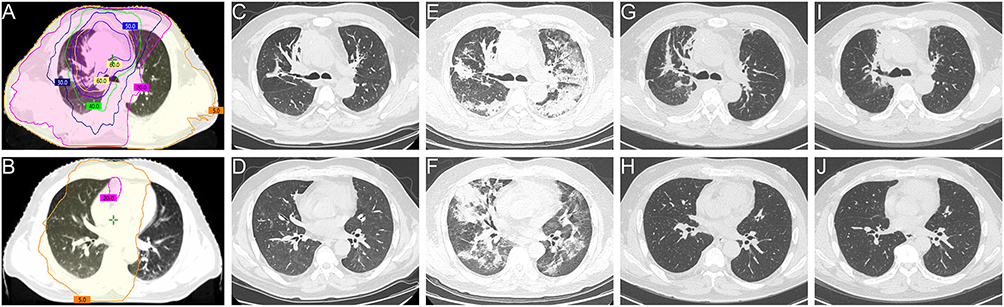 |
Figure 4 Timeline of pneumonitis evolution on CT imaging. Serial chest CT images demonstrate findings at the following time points: RT start (A and B) day 36 (C and D) 1 day post-RT (E and F) 5.1 months post-RT (G and H) and 14 months post-RT (I and J). Color codes indicate volumes enclosed by successive isodose lines, from innermost to outermost: V5, V20, V30, V40, V50, V60, and CTV. Abbreviations: CT, Computed tomography; RT, radiotherapy; CTV, clinical target volume. |
Approximately 8.1 months after immunotherapy, the patient presented with isolated, severe thrombocytopenia (platelet count 30×109/L). This condition was refractory to initial interventions, including thrombopoietin (TPO), TPO receptor agonists (TPO-RA), and repeated platelet transfusions. Comprehensive evaluation ruled out common autoimmune disorders (eg, ITP), coagulopathies, and other secondary causes. Bone marrow aspiration and cytology revealed impaired megakaryocyte maturation in the absence of malignant infiltration. After excluding other potential etiologies such as lingering chemotherapy effects, infection, or pseudothrombocytopenia, a diagnosis of pembrolizumab-induced immune thrombocytopenia was made. Initiation of corticosteroid therapy successfully normalized the platelet count. However, attempts to discontinue steroids led to a recurrence of thrombocytopenia, which again responded to re-initiation of corticosteroids (Figure 5). Notably, despite the permanent discontinuation of all antitumor therapies after the pneumonitis event, subsequent serial imaging assessments consistently demonstrated a sustained partial response. At the last follow-up in April 2025, the patient maintained excellent disease control, with a progression-free survival exceeding 42 months from diagnosis (Figure 3).
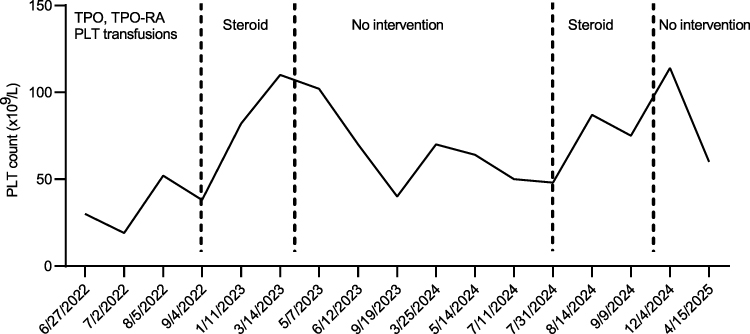 |
Figure 5 Dynamic changes in PLT counts following the single cycle of chemotherapy-immunotherapy. Abbreviations: PLT, platelet; TPO, thrombopoietin; TPO-RA, thrombopoietin receptor agonist. |
Discussion
While ICIs have revolutionized unresectable stage III NSCLC treatment, their application can be constrained by irAEs, particularly multi-organ involvement.1,2 Paradoxically, multi-organ irAEs may predict favorable outcomes.3 Herein, we document a patient with unresectable stage III lung squamous cell carcinoma who developed severe, sequential multi-organ irAEs after one cycle of pembrolizumab-chemotherapy and sequential thoracic RT. Despite suboptimal dosing and early ICI cessation, timely corticosteroids controlled irAEs while maintaining durable PR and PFS > 42 months. This outcome suggests the establishment of a potent and self-sustaining antitumor immune response.
The observed overlap syndrome of MMM represents a rare, life-threatening irAE (40–60% mortality),8–10 typically emerging within 1–2 cycles of ICI initiation.11 Diagnosis requires comprehensive evaluation of ICI exposure, clinical presentation, and laboratory findings. This patient met criteria for ICI-related myocarditis (palpitations, dyspnea, markedly elevated hs-cTnI/CK/CK-MB, exclusion of alternatives) and myositis (muscle weakness, elevated CK).12,13 Characteristic bilateral ptosis and diplopia supported concurrent myasthenia gravis despite negative anti-AChR antibodies.9 Symptoms resolved after 35 days of corticosteroid therapy.
In our previous research, we found that sequential thoracic RT post-immunotherapy significantly elevates RP risk, with V20 and MLD as key predictors.14,15 Prior irAEs further increase susceptibility (grade ≥ 2: 61%; grade ≥ 3: 15%).16 Here, multi-organ irAEs preceded thoracic RT, culminating in grade 4 treatment-related pneumonia including immune-mediated pneumonitis or/and RP. This clinical course underscores the necessity for rigorous pneumonitis risk assessment and intensive monitoring during combined immunotherapy and thoracic RT. Successful management employed high-dose corticosteroids and IVIG, necessitating permanent ICI discontinuation per guidelines.17,18
Subsequent severe thrombocytopenia proved refractory to TPO, TPO-RA, and transfusions but responded to corticosteroids. Bone marrow revealed megakaryocyte maturation arrest, confirming immune-mediated pathogenesis. ICI-associated thrombocytopenia is rare (~2.8% incidence), typically occurring 1–84 weeks post-ICI initiation (median 10 weeks).19 In this case, it emerged at ~35 weeks. Prolonged steroid therapy may have masked pre-existing thrombocytopenia. Steroid-induced remission exhibited dependency and recurrence upon withdrawal, suggesting progressive immune dysregulation: persistent ICI effects may expand autoreactive lymphocytes targeting platelets/megakaryocytes, while corticosteroids spare pathogenic memory cells enabling relapse.20
The exceptional tumor control observed in this patient can be contextualized by two key concepts. First, there is a potential association between multi-organ irAEs and survival benefit. Meta-analyses confirm irAEs independently associate with improved PFS, OS, and objective response rate (ORR) across tumor/ICI types.21 Multi-organ irAEs confer superior outcomes versus single-organ or no irAEs (ORR: 42% vs 23% vs 12%, p < 0.0001; mPFS: 7.2 vs 4.2 vs 2.7 months; mOS: NR vs 20.1 vs 10.3 months; both p < 0.001).4 While some data suggest that the type of irAE influences prognosis (eg, respiratory and neurologic being less favorable).3 Our case demonstrates that even with severe involvement of muscular, cardiovascular, respiratory, and hematological systems, a profound and durable survival benefit can be realized. Importantly, while high-dose corticosteroids (≥ 2 mg/kg peak) associate with impaired OS [HR 1.66 (95% CI: 1.17–2.37)],22 our patient maintained PFS > 42 months despite methylprednisolone 4 mg/kg, suggesting that the underlying robust immune activation signaled by severe, multi-organ irAEs may outweigh the immunosuppressive effects of corticosteroids in certain scenarios. Second, the role of RT in modulating the immune response is crucial. There is growing evidence that combining RT, even at lower doses, with ICIs can potentiate systemic antitumor immunity.23 In the MATCH study,7 which evaluated first-line treatment for extensive-stage small cell lung cancer, LDRT (15 Gy/5 fractions) was administered concurrently during the first cycle alongside standard chemoimmunotherapy (IMpower133 regimen). Preliminary results demonstrated a 12-month PFS rate of 27.7% and a 12-month OS rate of 71.9%, outcomes surpassing historical chemoimmunotherapy-alone benchmarks,24,25 with favorable toxicity. Similarly, a subgroup analysis from the GEMSTONE-301 trial suggested that consolidation immunotherapy yielded longer median PFS in patients who had received lower doses of prior RT (< 60 Gy) compared to those who received higher doses (≥ 60 Gy) (10.51 vs 8.44 months).26 The durable response achieved in our case with a subtherapeutic radiation dose of 50 Gy following a single ICI cycle aligns with this concept. It supports the hypothesis that the abscopal effect and immunogenic cell death induced by RT can synergize with ICIs to initiate a powerful, systemic immune response that does not necessarily require full-dose radiation or prolonged ICI therapy. This lends strong support to ongoing research into optimizing RT parameters, such as dose de-escalation, hypofractionation, and clinical target volume (CTV) reduction to maximize efficacy and minimize toxicity in the immunotherapy era.27
Conclusion
This case demonstrates exceptional long-term control (PFS > 42 months) in stage IIIA NSCLC after one immunochemotherapy cycle and subtherapeutic thoracic RT, despite severe multi-organ irAEs. It underscores that (1) multi-organ irAEs may be a significant clinical biomarker predicting a favorable prognosis, and their effective management is paramount to unlocking this potential benefit.; and (2) RT-ICI synergy can catalyze a robust and durable systemic antitumor immune response, which may be effective even with attenuated radiation doses, challenging traditional radiotherapeutic paradigms. Therefore, proactive toxicity management and RT parameter optimization are critical to maximizing therapeutic benefit.
Data Sharing Statement
The data used during the current study are available from the corresponding author (Jianping Bi) on reasonable request.
Ethics Approval and Informed Consent
This study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Hubei Cancer Hospital of Huazhong University of Science and Technology (Approval No: LLHBCH2025YN-065). The approval also encompasses permission for the publication of anonymized case details. Written informed consent was obtained from the patient.
Consent for Publication
Written informed consent was obtained from the participant for the publication of this case report (including all data and images).
Acknowledgments
We thank Vivek Verma for contributing to the English grammar correction in the revision of the paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by PARP Inhibitor Oncology Research Funding of China Anti-Cancer Association (CACA) [CETSDHRCORP252-4-004], Hubei Provincial Natural Science Foundation Joint Fund Key Project - Hengrui Medical Innovation and Development Joint Fund [2025AFD779], Chinese Society of Clinical Oncology (CSCO) Heathcote-Young Oncology Research Fund Project [Y-Young2022-0325], Hubei Provincial Natural Science Foundation of China [2024AFB931], Talent Project of Hubei Cancer Hospital [2025HBCHQHRC019].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2017;377(20):1919–1929. doi:10.1056/NEJMoa1709937
2. Spigel DR, Faivre-Finn C, Gray JE, et al. Five-year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J Clin Oncol. 2022;40(12):1301–1311. doi:10.1200/JCO.21.01308
3. Wan G, Chen W, Khattab S, et al. Multi-organ immune-related adverse events from immune checkpoint inhibitors and their downstream implications: a retrospective multicohort study. Lancet Oncol. 2024;25(8):1053–1069. doi:10.1016/S1470-2045(24)00278-X
4. Kichenadasse G, Miners JO, Mangoni AA, et al. Multiorgan immune-related adverse events during treatment with atezolizumab. J Natl Compr Canc Netw. 2020;18(9):1191–1199. doi:10.6004/jnccn.2020.7567
5. Khan S, Malladi VS, von Itzstein MS, et al. Innate and adaptive immune features associated with immune-related adverse events. J Immunother Cancer. 2025;13:e012414.
6. Bradley JD, Hu C, Komaki RR, et al. Long-term results of NRG oncology RTOG 0617: standard- versus high-dose chemoradiotherapy with or without cetuximab for unresectable stage III non-small-cell lung cancer. J Clin Oncol. 2020;38(7):706–714. doi:10.1200/JCO.19.01162
7. Wang H, Yao Z, Kang K, et al. Preclinical study and Phase II trial of adapting low-dose radiotherapy to immunotherapy in small cell lung cancer. Med. 2024;5(10):1237–1254.e9. doi:10.1016/j.medj.2024.06.002
8. Lipe DN, Qdaisat A, Krishnamani PP, et al. Myocarditis, myositis, and myasthenia gravis overlap syndrome associated with immune checkpoint inhibitors: a systematic review. Diagnostics. 2024;14(16):1794. doi:10.3390/diagnostics14161794
9. Pathak R, Katel A, Massarelli E, et al. Immune checkpoint inhibitor-induced myocarditis with myositis/myasthenia gravis overlap syndrome: a systematic review of cases. Oncologist. 2021;26(12):1052–1061. doi:10.1002/onco.13931
10. Sánchez-Camacho A, Torres-Zurita A, Gallego-López L, et al. Management of immune-related myocarditis, myositis and myasthenia gravis (MMM) overlap syndrome: a single institution case series and literature review. Front Immunol. 2025;16:1597259. doi:10.3389/fimmu.2025.1597259
11. Johnson DB, Balko JM, Compton ML, et al. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. 2016;375(18):1749–1755. doi:10.1056/NEJMoa1609214
12. Herrmann J, Lenihan D, Armenian S, et al. Defining cardiovascular toxicities of cancer therapies: an International Cardio-Oncology Society (IC-OS) consensus statement. Eur Heart J. 2022;43(4):280–299. doi:10.1093/eurheartj/ehab674
13. Bonaca MP, Olenchock BA, Salem JE, et al. Myocarditis in the setting of cancer therapeutics: proposed case definitions for emerging clinical syndromes in cardio-oncology. Circulation. 2019;140(1):80–91. doi:10.1161/CIRCULATIONAHA.118.034497
14. Bi J, Meng R, Yang D, et al. Dosimetric predictors of radiation pneumonitis in patients with prior immunotherapy exposure: a multi-institutional analysis. Radiother Oncol. 2024;190:110040. doi:10.1016/j.radonc.2023.110040
15. Bi J, Qian J, Yang D, et al. Dosimetric risk factors for acute radiation pneumonitis in patients with prior receipt of immune checkpoint inhibitors. Front Immunol. 2022;12:828858. doi:10.3389/fimmu.2021.828858
16. Shaverdian N, Beattie J, Thor M, et al. Safety of thoracic radiotherapy in patients with prior immune-related adverse events from immune checkpoint inhibitors. Ann Oncol. 2020;31(12):1719–1724. doi:10.1016/j.annonc.2020.09.016
17. Haanen J, Obeid M, Spain L, et al. Management of toxicities from immunotherapy: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(12):1217–1238. doi:10.1016/j.annonc.2022.10.001
18. Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021;39(36):4073–4126. doi:10.1200/JCO.21.01440
19. Michot JM, Lazarovici J, Tieu A, et al. Haematological immune-related adverse events with immune checkpoint inhibitors, how to manage? Eur J Cancer. 2019;122:72–90. doi:10.1016/j.ejca.2019.07.014
20. Costagliola G, Consolini R. Refractory immune thrombocytopenia: lessons from immune dysregulation disorders. Front Med Lausanne. 2022;9:986260. doi:10.3389/fmed.2022.986260
21. Hussaini S, Chehade R, Boldt RG, et al. Association between immune-related side effects and efficacy and benefit of immune checkpoint inhibitors - A systematic review and meta-analysis. Cancer Treat Rev. 2021;92:102134. doi:10.1016/j.ctrv.2020.102134
22. Verheijden RJ, de Groot JS, Fabriek BO, et al. Corticosteroids for immune-related adverse events and checkpoint inhibitor efficacy: analysis of six clinical trials. J Clin Oncol. 2024;42(31):3713–3724. doi:10.1200/JCO.24.00191
23. Herrera FG, Ronet C, Ochoa de Olza M, et al. Low-dose radiotherapy reverses tumor immune desertification and resistance to immunotherapy. Cancer Discov. 2022;12(1):108–133. doi:10.1158/2159-8290.CD-21-0003
24. Horn L, Mansfield AS, Szczęsna A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. doi:10.1056/NEJMoa1809064
25. Wang J, Zhou C, Yao W, et al. Adebrelimab or placebo plus carboplatin and etoposide as first-line treatment for extensive-stage small-cell lung cancer (CAPSTONE-1): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022;23(6):739–747. doi:10.1016/S1470-2045(22)00224-8
26. Zhou Q, Chen M, Jiang O, et al. Sugemalimab versus placebo after concurrent or sequential chemoradiotherapy in patients with locally advanced, unresectable, stage III non-small-cell lung cancer in China (GEMSTONE-301): interim results of a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2022;23(2):209–219. doi:10.1016/S1470-2045(21)00630-6
27. Zou L, Chu L, Xia F, et al. Is clinical target volume necessary?-a failure pattern analysis in patients with locally advanced non-small cell lung cancer treated with concurrent chemoradiotherapy using intensity-modulated radiotherapy technique. Transl Lung Cancer Res. 2020;9(5):1986–1995. doi:10.21037/tlcr-20-523
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
B Cell Receptor Signaling Pathway Mutation as Prognosis Predictor of Immune Checkpoint Inhibitors in Lung Adenocarcinoma by Bioinformatic Analysis
Lin A, Fang J, Cheng Q, Liu Z, Luo P, Zhang J
Journal of Inflammation Research 2022, 15:5541-5555
Published Date: 23 September 2022
Comparative Efficacy and Safety of Neoadjuvant Immunotherapy with Chemotherapy versus Chemotherapy Alone in Non-Small Cell Lung Cancer: A Propensity Score and Inverse Probability Treatment Weighting Analysis
Zhao J, Hao S, Li Y, Liu X, Liu Z, Zheng C, Han D
ImmunoTargets and Therapy 2023, 12:113-133
Published Date: 11 November 2023
Simultaneous Anti-Tuberculosis and Anti-Tumor Treatment with Immune Checkpoint Inhibitors for Co-Existent Pulmonary Tuberculosis and Advanced Lung Cancer
Wang H, Gao L, Cai X, Li J, Lang Y, Zheng R, Yang S
Infection and Drug Resistance 2025, 18:107-112
Published Date: 6 January 2025
Dupilumab Can Be Effective for Immune-Related Adverse Event Dermatitis: A Case Report and Review of the Literature
Mima Y, Yamamoto M, Chiba K, Iozumi K
Clinical, Cosmetic and Investigational Dermatology 2026, 19:604678
Published Date: 16 May 2026