Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Dupilumab Can Be Effective for Immune-Related Adverse Event Dermatitis: A Case Report and Review of the Literature
Authors Mima Y ![]() , Yamamoto M, Chiba K, Iozumi K
, Yamamoto M, Chiba K, Iozumi K
Received 22 February 2026
Accepted for publication 5 May 2026
Published 16 May 2026 Volume 2026:19 604678
DOI https://doi.org/10.2147/CCID.S604678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Yoshihito Mima,1 Masako Yamamoto,1 Kaoru Chiba,2 Ken Iozumi1
1Department of Dermatology, Tokyo Metropolitan Police Hospital, Tokyo, Japan; 2Department of Respiratory Medicine, Tokyo Metropolitan Police Hospital, Tokyo, Japan
Correspondence: Yoshihito Mima, Department of Dermatology, Tokyo Metropolitan Police Hospital, 4-22-1 Nakano, Nakano-ku, Tokyo, 164-8541, Japan, Tel +81-03-5343-5611, Fax +81-03-5343-5612, Email [email protected]
Abstract: Immune checkpoint inhibitors (ICIs) have significantly improved outcomes in various malignancies but frequently induce immune-related adverse events (irAEs), among which cutaneous irAEs are the most common. Although systemic corticosteroids are the mainstay of treatment, some cases are refractory or difficult to manage due to comorbidities. We report a case of refractory irAE dermatitis successfully treated with dupilumab in a patient with atopic dermatitis (AD) in whom corticosteroid escalation was limited by multiple irAEs. A 79-year-old man with AD, well controlled with lebrikizumab, developed disseminated erythematous eruptions consistent with irAE dermatitis following treatment with carboplatin, etoposide, and atezolizumab for stage IVB small cell lung carcinoma. Although the skin lesions initially improved with systemic corticosteroids, they recurred during tapering. Further escalation of corticosteroids was precluded by the development of ICI-associated pneumonitis, hypothyroidism, and adrenal insufficiency. Given the T helper (Th)2-skewed immune background and the limitations of corticosteroid therapy, dupilumab was initiated. Erythema and pruritus improved rapidly, and near-complete remission was achieved after four doses, enabling discontinuation of systemic corticosteroids. Recent evidence suggests that Th2 cytokines, including IL-4 and IL-13, are involved in ICI-associated dermatitis, supporting the mechanistic rationale for IL-4/IL-13 blockade. This case indicates that dupilumab may represent an effective, steroid-sparing therapeutic option for irAE dermatitis, particularly in patients with an atopic background or in those in whom corticosteroid escalation is limited. Further studies are warranted to clarify its efficacy and clinical positioning.
Keywords: dupilumab, immune checkpoint inhibitor, immune-related adverse events, T helper 2, corticosteroid
Introduction
Immune checkpoints are key mechanisms by which cancer cells evade immune surveillance and escape immune-mediated attack. They function as negative regulators of the immune system, maintaining self-tolerance, suppressing autoimmunity, and protecting tissues from excessive immune responses.1 Tumor cells enhance immune resistance by activating specific checkpoint pathways that inhibit T-cell activation.2 Immune checkpoint inhibitors (ICIs) have demonstrated potent antitumor activity across various malignancies, including urothelial carcinoma, renal cell carcinoma, melanoma, non–small cell lung cancer, colorectal cancer, and Hodgkin lymphoma, and are now widely used in clinical practice.3 By blocking inhibitory signaling pathways that physiologically restrain T-cell responses, ICIs promote the activation and persistence of T-cell effector functions.4 However, disruption of immune homeostasis by ICIs can lead to immune-related adverse events (irAEs).5 Although the precise pathophysiological mechanisms remain incompletely understood, ICIs are thought to induce irAEs by activating both CD4⁺ and CD8⁺ T cells and impairing peripheral immune tolerance, thereby enhancing inflammation and autoimmunity, with features that overlap with other autoimmune diseases.6–9
IrAEs are organ-specific, with cutaneous irAEs being the most common, followed by gastrointestinal toxicities such as diarrhea and colitis.10 Endocrine irAEs are the third most frequent and include thyroid dysfunction, hypophysitis, and adrenal insufficiency.10 Musculoskeletal adverse events and ocular toxicities are also relatively common.10 Although less frequent, pneumonitis, myocarditis, neurologic disorders, nephritis, and cytopenias can be severe and clinically significant. Despite their high incidence, approximately two-thirds of patients with cutaneous irAEs require systemic corticosteroids for their control, and about 19% discontinue immunotherapy due to irAEs.10 Clinically, mild-to-moderate presentations such as pruritus, maculopapular eruptions, lichenoid dermatitis, psoriasiform eruptions, eczematous dermatitis, vitiligo or alopecia are typical. Severe cutaneous irAEs, including bullous pemphigoid, Stevens–Johnson syndrome, or toxic epidermal necrolysis, have also been reported.11,12
IrAE dermatitis is often refractory, and some patients show inadequate responses to systemic corticosteroids and topical therapy. Although dupilumab is not currently approved for irAE dermatitis, its therapeutic potential has attracted increasing attention because it targets the Th2 cytokines such as interleukin (IL)-4 and IL-13.13,14 Herein, we report a case of irAE dermatitis developing in a patient with a history of atopic dermatitis (AD) in whom the introduction of dupilumab enabled successful disease control and ultimately allowed discontinuation of systemic corticosteroids that had been difficult to taper.
Case Report
A 79-year-old man with AD was treated with lebrikizumab for >1 year. Computed tomography revealed mass lesions in the right lung and bilateral adrenal tumors (Figure 1a and b). A biopsy of the lung mass revealed diffuse proliferation of small round cells with a high nuclear-to-cytoplasmic ratio. Immunohistopathological staining was positive for thyroid transcription factor-1, insulinoma-associated protein 1, chromogranin A, and synaptophysin. The patient was diagnosed with stage IVB small cell lung carcinoma with adrenal metastases. Because skin lesions and pruritus were well-controlled, lebrikizumab was temporarily discontinued. First-line treatment comprising carboplatin, etoposide, and atezolizumab was administered as four cycles. After the third cycle, disseminated erythematous eruptions considered immune-related adverse event (irAE) dermatitis developed. Oral prednisolone (20 mg/day) and topical clobetasol propionate resulted in gradual improvement. Subsequently, prednisolone was tapered and discontinued. After two additional cycles of atezolizumab, recurrent irAE dermatitis and immune checkpoint inhibitor (ICI)-associated drug-induced pneumonitis, hypothyroidism, and adrenal insufficiency developed. Steroid pulse therapy was administered for pneumonitis. Thereafter, prednisolone was gradually tapered to ≤3 mg/day. Endocrine dysfunction was managed with thyroid hormone and adrenal corticosteroid replacement therapies. However, relapsed dermatitis with disseminated pruritic erythema over the trunk and extremities and marked scratching behavior occurred with prednisolone tapering (Figure 1c and d). Histopathological examination from the erythematous lesion revealed scattered lymphocytic and eosinophilic infiltration predominantly around superficial dermal vessels, along with mild vacuolar degeneration associated with lymphocytic infiltration into the epidermis (Figure 1e and f). Cytological atypia and malignant features were not observed. These findings suggested ICI-induced maculopapular drug eruption. Adrenal insufficiency precluded further escalation of systemic corticosteroids. The patient’s history of AD suggested a T helper (Th) 2-mediated component. Because of reports of its efficacy for irAE-associated dermatitis, dupilumab (initial 600 mg dose followed by 300 mg biweekly) was initiated.15,16 Erythema and pruritus improved rapidly. Near-complete resolution of skin lesions and complete disappearance of pruritus were observed after the fourth dose (Figure 1g and h). Dermatitis was successfully controlled without increasing systemic corticosteroids, allowing prednisolone discontinuation.
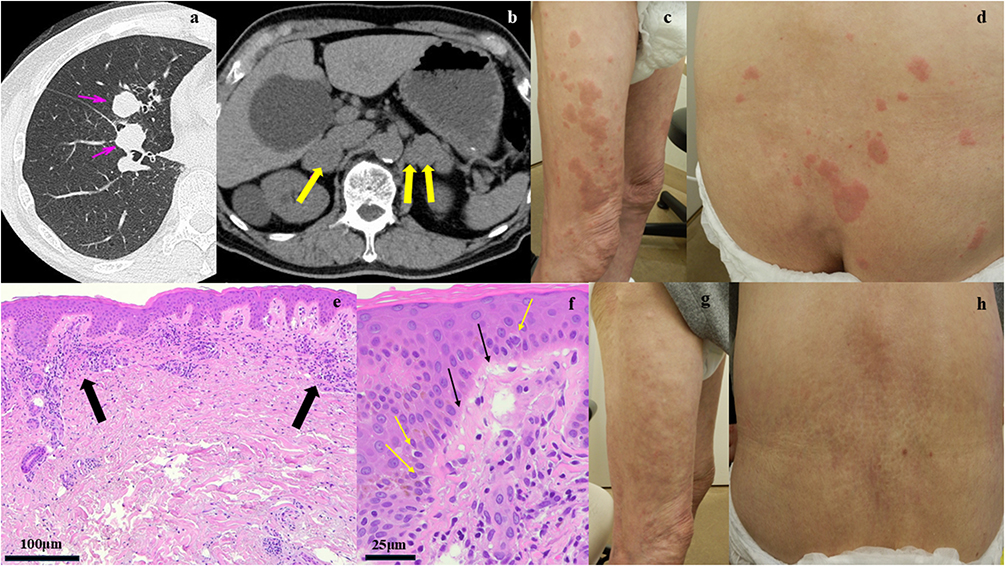 |
Figure 1 Clinical findings and results of radiological imaging. (a and b) Computed tomography demonstrated mass lesions in the right lung ((a) pink arrows) and bilateral adrenal tumors ((b) yellow arrows). (c and d) Recurrent dermatitis presenting as disseminated pruritic erythema over the extremities (c) and trunk (d). (e and f) Histopathological examination of erythematous lesions showed scattered lymphocytic and eosinophilic infiltration predominantly around the superficial dermal vessels ((e) black arrows, hematoxylin and eosin staining, ×40). In addition, vacuolar degeneration of the basal layer (black arrows) and mild lymphocytic infiltration into the epidermis (yellow arrows) were observed ((f) hematoxylin and eosin staining, ×100). (g and h) Near-complete resolution of the lesions on the extremities (g) and trunk (h) was observed after the fourth dose. |
Discussion
Cutaneous adverse events following ICI therapy include not only the well-recognized Th1/Th17-dominant inflammatory reactions but also a spectrum of Th2-mediated inflammatory dermatoses, such as bullous pemphigoid (BP), AD, and prurigo nodularis (PN). Theoretically, Th2 immune responses are regulated in part by the Programmed Death (PD)-1–PD-Ligand 2 axis, and blockade of this pathway by ICIs may lead to excessive Th2 activation, thereby inducing inflammatory reactions in the skin as well as in internal organs.10 Indeed, cytokine analyses of lesional skin in patients with ICI-induced cutaneous symptoms have demonstrated increased expression of Th2 cytokines, including IL-4, IL-5, and IL-13, in many cases presenting with erythema, pruritus, and eczema.15 Furthermore, recent tape-stripping studies analyzing cytokine expression in irAE lesions have shown significant upregulation of Th1-related inflammation along with concurrent elevation of Th2 signals, particularly IL-4, suggesting broad immune dysregulation and distinct immunologic pathway alterations in cutaneous irAEs.16 Consistently, dupilumab, which targets IL-4 signaling, has shown efficacy in more than 80% of patients with ICI-induced cutaneous toxicities in case series and retrospective cohorts, with significant improvements in both skin eruptions and Dermatology Life Quality Index scores, strongly supporting the hypothesis that ICIs can induce Th2 cytokine–related dermatitis.17–19 In addition, dupilumab has enabled control of irAE dermatitis with discontinuation or low-dose maintenance of prednisolone and, in some cases, allowed resumption of ICI therapy.17–19 A systematic review of dupilumab for irAE-related dermatitis reported that the treated phenotypes were predominantly eczematous (35%), bullous pemphigoid (30.7%), maculopapular eruptions (15.7%), and lichenoid eruptions (8.6%), with complete response achieved in over 90% of patients. Regarding safety, only mild adverse events such as psoriasiform eruptions, conjunctivitis, and injection-site reactions were observed, with no serious adverse events reported.20 Moreover, retrospective studies in patients with malignancy have indicated that dupilumab does not adversely affect mortality, and its favorable safety profile suggests that it may be a feasible therapeutic option even in patients with active cancer.21,22
In addition to common ICI-induced erythema and eczematous eruptions, dupilumab has increasingly been reported as a treatment for ICI-associated bullous pemphigoid (BP).20 BP is an autoimmune blistering disorder that predominantly affects older individuals, with incidence rising in parallel with population aging.23 Systemic corticosteroids remain the first-line therapy for severe disease.24 The pathogenesis of BP involves autoantibody-producing B cells, Th2-skewed T-cell responses, eosinophils, mast cells, and the complement system.25,26 Notably, Th2 cytokines such as IL-4 and IL-13 play key roles in eosinophil recruitment and anti-BP180 antibody production,27,28 and similar upregulation has been observed in lesional skin of ICI-associated BP.29 Dupilumab is thought to exert therapeutic effects by inhibiting IL-4/IL-13 signaling and modulating T cell–B cell interactions, thereby attenuating downstream inflammatory pathways.29,30 Consistent with this mechanism, multiple reports have demonstrated its efficacy in ICI-associated BP, including steroid-refractory cases and those in whom immunosuppressive therapy is limited by comorbidities.31–34 Importantly, dupilumab has enabled control of cutaneous irAEs while avoiding escalation of systemic corticosteroids and, in some cases, has allowed continuation or resumption of ICI therapy.31–35 In a case series of 17 patients with ICI-associated BP, complete remission was achieved in 12 patients, including 10 who responded to dupilumab monotherapy.36 Collectively, these findings support the potential utility of dupilumab as a therapeutic option for refractory ICI-associated BP.
Furthermore, dupilumab has shown efficacy in other ICI-associated dermatologic conditions, including acquired reactive perforating collagenosis (ARPC).37 Its effectiveness has also been reported in ICI-related lichenoid dermatitis that was refractory to systemic corticosteroids and methotrexate,38 as well as in ICI-associated lichen planus pemphigoides.39 Immunohistochemical analyses of ARPC lesions have suggested overexpression of Th2-related cytokines, particularly IL-4 and IL-13, supporting a mechanistic rationale for the efficacy of dupilumab.40 Similarly, increased expression of IL-4 and IL-13 has been observed in lichenoid lesions, providing further biological plausibility for dupilumab responsiveness.41 Beyond dermatologic manifestations, dupilumab has also been reported to be effective in eosinophilic reactive airway disease occurring after ICI therapy, suggesting its potential role in managing Th2-dominant irAEs.42
In the present case, dupilumab enabled effective control of erythema and pruritus in irAE dermatitis developing a patient with a history of AD, without the need for escalation of systemic prednisolone. In clinical settings where systemic corticosteroid escalation is limited by comorbidities such as adrenal insufficiency or diabetes, dupilumab may represent a valuable therapeutic option for irAE dermatitis. Importantly, irAE dermatitis is a clinically significant complication not only for dermatologists but also for oncologists, as inadequate response to systemic corticosteroids and difficulty in tapering may necessitate interruption of anticancer therapy.17–20 In this context, dupilumab, with its favorable safety profile and accumulating evidence of use in patients with malignancy, may be a reasonable treatment option in selected cases.21,22 However, this report has several limitations. It is based on a single case and lacks a control group; the use of dupilumab for irAE dermatitis alone is off-label; and the potential impact of dupilumab-induced cytokine modulation on antitumor immunity cannot be fully excluded. Furthermore, given the limited specificity of irAE dermatitis histopathological findings, distinguishing irAE dermatitis from a flare of underlying AD remains challenging and represents a limitation of this study. Further accumulation of cases and prospective clinical studies are warranted to clarify the efficacy and clinical positioning of dupilumab in the management of irAE dermatitis.
Conclusion
IrAE dermatitis represents a clinically significant and sometimes refractory complication of ICI therapy, often requiring systemic corticosteroids that may be difficult to escalate due to comorbidities. Emerging evidence suggests that Th2-related immune dysregulation, including upregulation of IL-4 and IL-13, plays an important role in the pathogenesis of ICI-associated cutaneous toxicities. Accumulating reports indicate that dupilumab can effectively control various Th2-dominant irAEs, including eczematous dermatitis and bullous pemphigoid, while enabling steroid tapering and, in some cases, continuation of ICI therapy. Therefore, dupilumab may serve as a safe and steroid-sparing therapeutic option for refractory irAE dermatitis, although further prospective studies are needed to establish its efficacy and optimal clinical positioning.
Data Sharing Statement
Additional data concerning this article may be requested from the corresponding author for reasonable reasons.
Informed Consent Statement
Although the use of dupilumab for immune-related adverse events was off-label, some symptoms such as pruritus were considered potentially associated with the patient’s pre-existing atopic dermatitis. Therefore, prior consultation was conducted with the Institutional Ethics Committee of Tokyo Metropolitan Police Hospital, which determined that no additional ethical approval was required for the administration of dupilumab in this case. Thus, the institutional approval for the publication of this case was not needed. After providing a thorough explanation, written informed consent was obtained from the patient for the publication of this case report, including the clinical history, photographs, and radiological images.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang J, Yang T, Xu J. Therapeutic development of immune checkpoint inhibitors. Adv Exp Med Biol. 2020;1248:619–6.
2. Lim S, Phillips JB, Madeira da Silva L, et al. Interplay between immune checkpoint proteins and cellular metabolism. Cancer Res. 2017;77:1245–1249. doi:10.1158/0008-5472.CAN-16-1647
3. Rocha M, Correia de Sousa J, Salgado M, et al. Management of gastrointestinal toxicity from immune checkpoint inhibitor. GE Port J Gastroenterol. 2019;26:268–274. doi:10.1159/000494569
4. Hargadon KM, Johnson CE, Williams CJ. Immune checkpoint blockade therapy for cancer: an overview of FDA-approved immune checkpoint inhibitors. Int Immunopharmacol. 2018;62:29–39. doi:10.1016/j.intimp.2018.06.001
5. de Miguel M, Calvo E. Clinical challenges of immune checkpoint inhibitors. Cancer Cell. 2020;38:326–333. doi:10.1016/j.ccell.2020.07.004
6. Wang Y, Zhou S, Yang F, et al. Treatment-related adverse events of PD-1 and PD-L1 inhibitors in clinical trials: a systematic review and meta-analysis. JAMA Oncol. 2019;5:1008–1019. doi:10.1001/jamaoncol.2019.0393
7. Lee DJ, Lee HJ, Farmer JR, et al. Mechanisms driving immune-related adverse events in cancer patients treated with immune checkpoint inhibitors. Curr Cardiol Rep. 2021;23:98. doi:10.1007/s11886-021-01530-2
8. Johnson DB, Balko JM, Compton ML, et al. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. 2016;375:1749–1755. doi:10.1056/NEJMoa1609214
9. Esfahani K, Elkrief A, Calabrese C, et al. Moving towards personalized treatments of immune-related adverse events. Nat Rev Clin Oncol. 2020;17:504–515. doi:10.1038/s41571-020-0352-8
10. Okiyama N, Tanaka R. Immune-related adverse events in various organs caused by immune checkpoint inhibitors. Allergol Int. 2022;71:169–178. doi:10.1016/j.alit.2022.01.001
11. Kaunitz GJ, Loss M, Rizvi H, et al. Cutaneous eruptions in patients receiving immune checkpoint blockade: clinicopathologic analysis of the nonlichenoid histologic pattern. Am J Surg Pathol. 2017;41:1381–1389. doi:10.1097/PAS.0000000000000900
12. Mima Y, Ohtsuka T, Ebato I, et al. A case of bullous pemphigoid with significant infiltration of CD4-Positive T cells during treatment with pembrolizumab, accompanied by pembrolizumab-induced multi-organ dysfunction. Diagnostics. 2024;14:1958. doi:10.3390/diagnostics14171958
13. Mital R, Otto TS, Savu A, et al. Detection of novel therapies using a multi-national, multi-institutional registry of cutaneous immune-related adverse events and management. Int J Dermatol. 2023;62:1020–1025. doi:10.1111/ijd.16714
14. Gooderham MJ, Hong HC, Eshtiaghi P, et al. Dupilumab: a review of its use in the treatment of atopic dermatitis. J Am Acad Dermatol. 2018;78:S28–S36. doi:10.1016/j.jaad.2017.12.022
15. Lacouture ME, Goleva E, Shah N, et al. Immunologic profiling of immune-related cutaneous adverse events with checkpoint inhibitors reveals polarized actionable pathways. Clin Cancer Res. 2024;30:2822–2834. doi:10.1158/1078-0432.CCR-23-3431
16. Powers CM, Kim M, Chang A, et al. Tape strip profiling of checkpoint inhibitor-associated dermatitis highlights Pan-T-Cell activation: a pilot study. JID Innov. 2025;5:100375. doi:10.1016/j.xjidi.2025.100375
17. Kuo AM, Gu S, Stoll J, et al. Management of immune-related cutaneous adverse events with dupilumab. J Immunother Cancer. 2023;11:e007324. doi:10.1136/jitc-2023-007324
18. Giacchero D, Sibaud V, Gerard E, et al. Dupilumab for immune checkpoint inhibitors-induced pruritic dermatoses: a retrospective, multicentric study. J Eur Acad Dermatol Venereol. 2025. doi:10.1111/jdv.70122
19. Fournier C, Hirsch I, Spreafico A, et al. Dupilumab as a treatment for cutaneous immune-related adverse events induced by immune checkpoint inhibitors: a case series and review of the literature. SAGE Open Med Case Rep. 2023;11:2050313X231195462. doi:10.1177/2050313X231195462
20. Koumprentziotis IA, Niforou A, Tsimpidakis A, et al. Dupilumab for the treatment of cutaneous immune-related adverse events: a systematic review. Int J Dermatol. 2025;64:1825–1832. doi:10.1111/ijd.17850
21. Khattab S, Wan G, Xu S, et al. Long-term mortality outcomes among immunotherapy recipients treated with dupilumab for the management of cutaneous immune-related adverse events. J Immunother Cancer. 2025;13:e010638. doi:10.1136/jitc-2024-010638
22. Li J, Jiang G. Dupilumab for atopic dermatitis in patients with malignancies: a case report and literature review on efficacy, safety and potential mechanisms. Clin Exp Dermatol. 2025;50:1315–1321. doi:10.1093/ced/llaf117
23. Bax CE, Werth VP. The incidence of bullous pemphigoid continues to increase in England. Br J Dermatol. 2021;184:5–6. doi:10.1111/bjd.19207
24. Borradori L, Van Beek N, Feliciani C, et al. Updated S2 K guidelines for the management of bullous pemphigoid initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol. 2022;36:1689–1704. doi:10.1111/jdv.18220
25. Cole C, Vinay K, Borradori L, et al. Insights into the pathogenesis of bullous pemphigoid: the role of complement-independent mechanisms. Front Immunol. 2022;13:912876. doi:10.3389/fimmu.2022.912876
26. Muramatsu K, Ujiie H, Kobayashi I, et al. Regulatory T-cell dysfunction induces autoantibodies to bullous pemphigoid antigens in mice and human subjects. J Allergy Clin Immunol. 2018;142:1818–1830.e6. doi:10.1016/j.jaci.2018.03.014
27. Eberle JU, Radtke D, Nimmerjahn F, et al. Eosinophils mediate basophil-dependent allergic skin inflammation in mice. J Invest Dermatol. 2019;139:1957–1965. doi:10.1016/j.jid.2019.03.1129
28. Zhang J, Fang H, Shen S, et al. Identification of immunodominant Th2-cell epitopes in Chinese patients with bullous pemphigoid. J Invest Dermatol. 2018;138:1917–1924. doi:10.1016/j.jid.2018.03.1515
29. Arnold L, Morak M, Kramer N, et al. Interleukin-4 and -13 gene expression profiles in immune-related bullous pemphigoid indicate efficacy of IL-4/IL-13 inhibitors. Cancers. 2025;17:1845. doi:10.3390/cancers17111845
30. Yan T, Xie Y, Liu Y, et al. Dupilumab effectively and rapidly treats bullous pemphigoid by inhibiting the activities of multiple cell types. Front Immunol. 2023;14:1194088. doi:10.3389/fimmu.2023.1194088
31. Khazaeli M, Grover R, Pei S. Concomitant nivolumab-associated Grover disease and bullous pemphigoid in a patient with metastatic renal cell carcinoma. J Cutan Pathol. 2023;50:520–523. doi:10.1111/cup.14383
32. Pop SR, Strock D, Smith RJ. Dupilumab for the treatment of pembrolizumab-induced bullous pemphigoid: a case report. Dermatol Ther. 2022;35:e15623. doi:10.1111/dth.15623
33. Rossi A, Brancorsini D, Gioacchini H, et al. A case of pembrolizumab-induced bullous pemphigoid treated with dupilumab. Skin Health Dis. 2025;5:70–74. doi:10.1093/skinhd/vzae023
34. Grüninger J, Lehr S, Meiss F, Rafei D, Schauer F. Case Report: dupilumab therapy for immune checkpoint inhibitor-induced bullous pemphigoid enables dual immunotherapy initiation in progressive malignant melanoma. Front Oncol. 2025;15:1613552. doi:10.3389/fonc.2025.1613552
35. Florea CM, Parmentier L, Abdou M, Berthod G. Immune checkpoint inhibitor-induced bullous pemphigoid: successful treatment with dupilumab while maintaining immunotherapy. Case Rep Oncol. 2025;18:1171–1177. doi:10.1159/000547431
36. Nykaza I, Moy A, Dusza SW, et al. Immuno-oncologyDupilumab for bullous pemphigoid related to immune checkpoint inhibitors: a retrospective case series. Oncologist. 2025;30:oyaf208. doi:10.1093/oncolo/oyaf208
37. Gold M, Mueller K, Bogner P, et al. Immune checkpoint inhibitor-associated acquired reactive perforating collagenosis treated with dupilumab. JAAD Case Rep. 2025;65:86–88. doi:10.1016/j.jdcr.2025.08.025
38. Park JJ, Park E, Damsky WE, et al. Pembrolizumab-induced lichenoid dermatitis treated with dupilumab. JAAD Case Rep. 2023;37:13–15. doi:10.1016/j.jdcr.2023.05.004
39. Xie X, Chen J, Luo Y, et al. A case report of tislelizumab-induced lichen planus pemphigoides. Clin Cosmet Invest Dermatol. 2025;18:2707–2711. doi:10.2147/CCID.S549402
40. Liu B, Wu Y, Wu X, et al. Dupilumab improve acquired reactive perforating collagenosis characterized by type 2 inflammation. Front Immunol. 2023;14:1240262. doi:10.3389/fimmu.2023.1240262
41. Pousti BT, Jin A, Sklovar L, et al. Dupilumab for the treatment of lichen planus. Cutis. 2021;107:E8–E10. doi:10.12788/cutis.0232
42. Cordial P, Bentley ID, Horowitz JC, et al. Eosinophilic reactive airways disease after immune checkpoint inhibitor treatment. Respirol Case Rep. 2024;12:e70022. doi:10.1002/rcr2.70022
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Durable Tumor Control with Multi-Organ Immune-Related Adverse Events Following Immune Checkpoint Inhibitor and Sequential Radiotherapy in Locally Advanced NSCLC: A Case Report
Zhai M, Liu X, Li Y, Pi G, Bi J, Han G
ImmunoTargets and Therapy 2025, 14:1411-1417
Published Date: 10 December 2025