Back to Journals » Journal of Pain Research » Volume 19
Crisugabalin Combined with Acetyl-Levo-Carnitine for Diabetic Peripheral Neuropathic Pain: A Phase 2 Randomized Controlled Trial
Authors Fu L, Xu N, Shang J, Yang Q, Li Y, Huang Q, Li J, Jiang H ![]()
Received 12 December 2025
Accepted for publication 27 March 2026
Published 21 April 2026 Volume 2026:19 588472
DOI https://doi.org/10.2147/JPR.S588472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Liujun Fu,1 Na Xu,2 Junjie Shang,3 Qiuwei Yang,4 Yaming Li,5 Qin Huang,5 Jing Li,5 Hongwei Jiang1
1Endocrinology and Metabolism Center, The First Affiliated Hospital, and College of Clinical Medicine of Henan University of Science and Technology, Luoyang, Henan, People’s Republic of China; 2Department of Endocrinology, Nanyang Central Hospital, Nanyang, Henan, People’s Republic of China; 3Department of Endocrinology, Nanyang Second General Hospital, Nanyang, Henan, People’s Republic of China; 4Department of Endocrinology, Luoyang First People’s Hospital, Luoyang, Henan, People’s Republic of China; 5Haisco Pharmaceutical Group Co., Ltd., Chengdu, Sichuan, People’s Republic of China
Correspondence: Hongwei Jiang, Endocrinology and Metabolism Center, The First Affiliated Hospital, and College of Clinical Medicine of Henan University of Science and Technology, Luoyang, Henan, 471003, People’s Republic of China, Email [email protected]
Purpose: To investigate the efficacy and safety of Crisugabalin combined with Acetyl-Levo-Carnitine (ALC) for treating Diabetic Peripheral Neuropathic Pain (DPNP) in Chinese adults.
Methods: This 16-week, multicenter, randomized, positive-controlled phase 2 trial was conducted from June 21, 2023, through February 22, 2024, employing a non-inferiority design with the non-inferiority limit set at 0.3 for the difference in Average Daily Pain Score (ADPS) change. A total of 137 Chinese adults with DPNP for at least 6 months were randomized to receive Crisugabalin with ALC or Alpha Lipoic Acid (ALA) with ALC. The primary endpoint was the change in ADPS from baseline at week 12. Secondary outcomes included sleep interference and quality of life measures.
Results: The Crisugabalin group showed a statistically significant reduction in ADPS compared to the ALA group (P< 0.0001). Specifically, the least square mean (LSM) change from baseline in the Crisugabalin group was − 4.0 (95% CI: − 4.405, − 3.620), while in the ALA group it was − 2.1 (95% CI: − 2.505, − 1.706). Secondary outcomes also demonstrated significant improvements in the Crisugabalin group. The treatment in the Crisugabalin group was well-tolerated, with adverse events primarily mild to moderate, and no serious related adverse events were reported.
Conclusion: Crisugabalin combined with ALC is a promising therapeutic option for DPNP, offering pain relief, improved sleep, and enhanced quality of life. This combination therapy may be more effective than standard ALA treatment. (Trial registration: ClinicalTrials.gov identifier, NCT06122012).
Keywords: diabetic peripheral neuropathy, Crisugabalin, combination treatment, pain management
Introduction
Diabetes mellitus (DM) is a chronic condition that has become an increasingly severe public health issue. It can lead to serious and progressive macrovascular and microvascular complications, contributing to increased mortality rates and a decrease in the quality of life. Diabetic peripheral neuropathy (DPN) is one of the microvascular complications of diabetes, sharing pathophysiological mechanisms of glucose-mediated vascular damage with other complications. The risk of DPN increases with age, and the lifetime prevalence may be >50%,1 with a significant number of cases going undiagnosed (12.5–61.5%).2,3 Among the symptoms of diabetic sensorimotor polyneuropathy, diabetic peripheral neuropathic pain (DPNP) affects up to 30% of individuals,4 often presenting as symmetrical peripheral neuropathic pain primarily involving the distal extremities, or as mononeuropathy or plexopathy.5–7
Neuropathic pain is often chronic, severe, and challenging to treat and manage. DPNP is a major cause of disability, foot ulcers, and ultimately, amputations. Over 70% of patients with DPNP suffer from moderate to severe persistent pain, leading to sleep disturbances, anxiety, and depression, which in turn reduce the quality of life.1,8
While DPN treatment goals include blood glucose control and addressing pathogenic mechanisms, DPNP primarily requires effective pain management. Current guidelines prioritize calcium channel modulators as first-line treatments for DPNP due to their efficacy in pain relief. Other options like antidepressants, anticonvulsants, and opioids may provide symptomatic relief, but they do not address the underlying neuropathy. Therapies such as alpha lipoic acid (ALA) and B-vitamin supplements are more focused on slowing DPN progression rather than treating DPNP.1,4,5,9 This distinction underscores the need for treatments that not only alleviate pain but also potentially modify the course of neuropathy, highlighting the rationale for exploring combination therapies in clinical trials.
The mechanisms underlying DPNP formation are complex, involving peripheral and central sensitization, the dysfunction of descending inhibitory systems, and changes in ion channel function, with various mechanisms interacting with each other. Calcium ions are crucial in pain signal initiation and modulation. Voltage-gated calcium channels, which include α1, α2δ, and β subunits, regulate calcium influx into neurons. The α2δ subunits are key therapeutic targets.10,11 These subunits may reduce pain by limiting calcium influx, thereby decreasing the release of excitatory neurotransmitters like glutamate and norepinephrine.12 In DPNP, nerve injury can increase α2δ subunit expression, leading to increased calcium influx and neuronal hyperexcitability, which contributes to allodynia and hyperalgesia. Targeting these subunits could provide an effective treatment approach for DPNP.
Crisugabalin capsules (HSK16149) are oral GABA-like agents that bind to the α2δ subunits of calcium ion channels, reducing calcium ion inflow through voltage-dependent calcium channels in the central nervous system, thereby reducing the release of excitatory neurotransmitters such as glutamate, norepinephrine, and substance P, and exhibiting anticonvulsant, analgesic, and anxiolytic activities.13,14 Crisugabalin, identified as a novel third-generation calcium channel modulator, has demonstrated potent bioactivity, with in vitro data indicating it is 23 times more bioactive than pregabalin, and coupled with the advantage of not requiring titration. The efficacy of Crisugabalin monotherapy for the treatment of DPNP was proved in a recently published phase 3 trial.15 Despite the established efficacy of Crisugabalin monotherapy, no clinical evidence currently exists for Crisugabalin-based combination therapy in the treatment of DPNP.
Additionally, hyperglycemia is considered a triggering factor for DPNP. Increased oxidative stress caused by free radical formation and the defect of antioxidant defenses associated with hyperglycemia are believed to lead to endoneurial hypoxia and neurodysfunction, resulting in DPN. Preclinical studies have shown that the administration of the antioxidant ALA can reduce neurovascular abnormalities associated with DPN.16 According to data from the Korean National Health Insurance Service-National Sample Cohort, the proportion of drug treatment in DPN ranges from 66.5% to 69.0%, with monotherapy accounting for 91.6% and combination therapy for 8.1%. In monotherapy, ALA is used the most, followed by anticonvulsants and tricyclic antidepressants (TCAs).17 ALA can reduce pain intensity measured by the 11-point numeric rating scale and total symptom scores (TSS) in patients with DPNP.18
Acetyl-Levo-carnitine (ALC), catalyzed by acetyltransferase, promotes cellular energy synthesis. Its mechanism of action includes stimulating aerobic metabolism in the brain, reducing oxidative stress injury, reducing excitotoxic effects, and reducing synaptic glutamate concentration to alleviate allodynia, which is closely related to neurological diseases. ALC treatment has been proven to improve DPN, stimulate nerve regeneration, and provide neuroprotection.19–21 Recent phase 3 clinical trial results show that 6 months of ALC treatment combined with anti-diabetic therapy can effectively reduce the severity of DPN-related symptoms, and patients have good tolerance to a daily dose of 1500 mg of ALC.9
Although monotherapy is commonly used in clinical practice as first-line treatment, the best treatment results usually only achieve at least 50% pain relief in less than half of the patients, often accompanied by dose-limiting side effects.22,23 However, most current international guidelines do not recommend combination therapy due to insufficient evidence, despite its widespread use by clinicians.23 In contrast, the Chinese expert consensus recognizes the potential benefits of combination therapy, emphasizing the synergistic effects of drugs with different mechanisms of action, which may offer superior outcomes compared to monotherapy.24 In clinical practice, the treatment of DPNP patients often involves a combination of analgesic drugs with neurotrophic, antioxidant stress, and aldose reductase inhibitory drugs, which can relieve pain and repair nerve damage. Accordingly, this study employs the combination of ALA and ALC as a positive control group, a treatment regimen that has demonstrated improvements in neurophysiological parameters, pain, and quality of life for patients with DPN in previous research.25 Our objective is to assess the efficacy and safety of a novel drug combination, Crisugabalin with ALC, in the management of DPNP.
Materials and Methods
Study Design
This was a 16-week, multicenter, randomized, open-label, non-blinded, positive-controlled phase 2 clinical trial, aimed at evaluating the efficacy and safety of Crisugabalin capsules combined with ALC tablets in Chinese patients with DPNP. The study adhered to the Declaration of Helsinki and was approved by the Ethics Committee of our hospital (approval no.2023–0141). Additionally, the study has been registered with clinicaltrials.gov (registration no. NCT06122012) (Figure 1a).
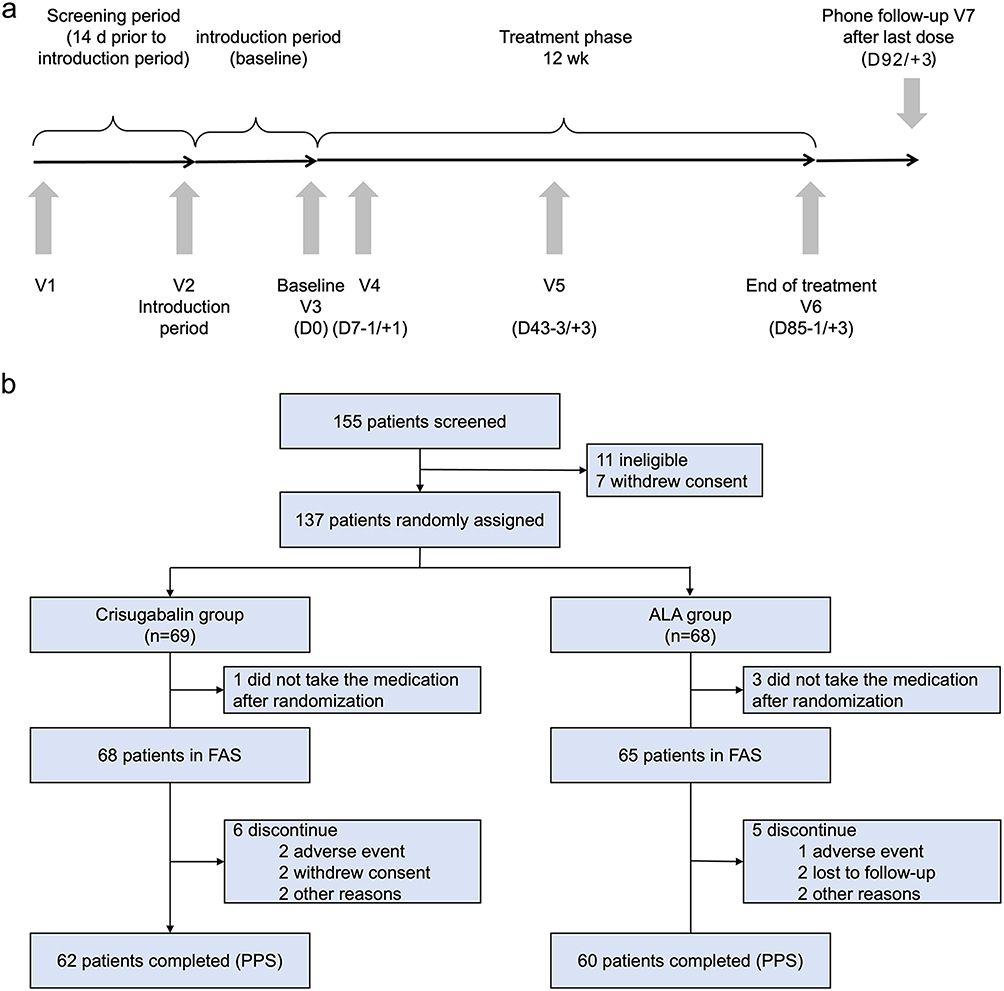 |
Figure 1 (a) Overall study design. D indicates day; wk, week; V, visit. Visit time windows refer to the setting of a visit period, within which the completion of the relevant test operations specified for this visit are all in accordance with the requirements of the study protocol, which contributes to the smooth and scientific conduct of the clinical study. (b) Flow of participants through the trial. Abbreviations: ALA, alpha-lipoic acid; FAS, Full Analysis Set; PPS, Per Protocol Set. |
Participants
The study enrolled participants who were diagnosed with DPNP according to established clinical criteria. Eligibility was determined by a comprehensive set of inclusion and exclusion criteria. Inclusion criteria mandated that participants be adults aged 18 years or older, capable of understanding the study’s implications and voluntarily providing written informed consent. A key inclusion metric was the presence of DPNP, confirmed by clinical diagnosis, and a measurable pain intensity reflected by a visual analog scale (VAS) score between 40 mm and below 90 mm within the 24 hours preceding the screening.
Conversely, exclusion criteria were designed to ensure the safety of participants and the reliability of the study outcomes. Participants were excluded if they presented with a history of peripheral neuropathy or pain not related to DPNP that could confound the study’s assessments, a history of malignancy within the past five years, with exceptions for certain types of cancer. Additionally, participants with severe hepatic or renal impairment, as indicated by specific laboratory values, were not eligible for enrollment. Known allergies to the trial medication components or structurally similar drugs, a history of suicidal ideation or attempts, and pregnancy or breastfeeding status were also criteria for exclusion.
Randomization and Procedures
The clinical trial was meticulously designed, encompassing a 2-week screening period, a 1-week introduction phase including baseline assessment (D0), a 12-week treatment period, and a final 1-week safety follow-up period. After clinical evaluation and confirmation of eligibility, participants provided informed consent and received comprehensive instructions regarding their involvement in the study from trained research personnel.
Upon successful completion of the screening phase, participants entered the introduction period where baseline assessments were conducted. During this time, participants did not receive any specific treatments for DPNP, except in cases of intolerable pain where nonsteroidal anti-inflammatory drugs (NSAIDs) were administered at the discretion of the study physician. Following the introduction period, eligible participants were randomized in a 1:1 ratio to either the Crisugabalin + ALC group (Crisugabalin group) or the ALA + ALC group (ALA group). The Crisugabalin group was prescribed Crisugabalin capsules (20mg, BID) along with ALC tablets (0.5g, TID) for the 12-week treatment duration. In contrast, the ALA group initially received ALA injections (0.6g, once daily) for the first week, followed by ALA tablets (0.6g, QD) combined with the same regimen of ALC tablets for the remaining 11 weeks. Follow-up visits were scheduled on Day 43 (week 6) and Day 85 (week 12) to assess the study endpoints. Throughout the study, participants had the right to withdraw consent at any time without prejudice to their future medical care. The study protocol provided clear guidelines for early withdrawal due to intolerable adverse events, participant refusal to continue, significant deviations from the study protocol, pregnancy, or loss to follow-up, ensuring the ethical conduct of the research and participant safety.
Post-treatment, participants engaged in a 1-week safety follow-up, which included a telephone assessment seven days after the final dose of medication. This assessment was vital for monitoring any potential late-emerging adverse events. For participants unable to complete the full treatment course, an early termination visit was arranged to ensure their safety and to collect necessary follow-up data.
Outcomes
The primary outcome was the change in Average Daily Pain Score (ADPS) from baseline at week 12 between two treatment groups. Secondary outcomes included changes in ADPS at week 8, Short-Form McGill Pain Questionnaire (SF-MPQ) scores, Average Daily Sleep Interference Score (ADSIS), and EuroQol-5D-5L (EQ-5D-5L) scores at week 12.
Safety
It included the documentation and evaluation of all adverse events (AEs) that emerged during the trial, along with extensive laboratory tests to identify any abnormalities in blood, urine, and other physiological parameters. The safety assessment of the study involved a detailed evaluation of treatment-emergent adverse events (TEAEs) and serious adverse events (SAEs). Electrocardiograms (ECGs) were utilized to monitor cardiac safety, while vital signs and physical examinations were systematically conducted to ensure that any changes in participants’ health were promptly detected and addressed.
Statistical Analysis
The sample size for this study was calculated based on a statistical non-inferiority design, assuming a difference in the ADPS of −0.6 between the experimental group receiving Crisugabalin capsules combined with ALC and the control group after 12 weeks of treatment. The non-inferiority limit was set at 0.3, with a standard deviation estimated at 1.7. The study aimed for 80% power to detect a difference at a one-sided significance level α of 0.025. Accounting for a 15% dropout rate, the calculated sample size required 136 participants, with 68 participants per group.
The primary endpoint analysis employed an Analysis of Covariance (ANCOVA) model, using the change in ADPS from baseline at week 12 as the dependent variable. To address missing ADPS scores at week 12, a multiple imputation method was utilized. The adjusted least squares means (LSM) and their standard errors for the change in ADPS were reported, along with the 95% confidence interval for the difference in mean changes between the experimental and control groups. The experimental group’s treatment was considered non-inferior if the upper limit of the 95% confidence interval for the adjusted mean difference was less than 0.3. When comparing the experiment group to the control group, the upper limit of the 95% confidence interval for the adjusted mean difference was less than 0, indicating a statistically significant and superior efficacy outcome for the experiment group. For participants with missing data at 12 weeks due to dropout or other reasons, the analysis was conducted after imputing the missing values using the multiple imputation method. Missing values for secondary efficacy endpoints were not imputed; instead, the adjusted least squares means and their standard errors were reported, along with the 95% confidence intervals for the differences in mean changes from baseline between the groups. For the primary endpoint analysis, we conducted post hoc analyses to assess the proportion of subjects who achieved a reduction of ≥30 or 50% in ADPS from baseline at week 12 or who had an ADPS score of 3 or lower at week 12. We also conducted sensitivity analyses based on the FAS and PPS. For subjects who discontinued and those with missing week 12 ADPS data, we used the multiple imputation method to impute missing week 12 data. Subsequently, we constructed an ANCOVA model with the complete data after imputation, taking the change from baseline at week 12 ADPS as the dependent variable and the study center, treatment group, and baseline ADPS value as explanatory variables. All analyses were performed using SAS software, version 8.3.
Results
The study enrolled a total of 137 participants, who were randomly assigned to either the Crisugabalin group with 69 cases or the ALA group with 68 cases. A total of 15 participants (10.9%) prematurely withdrew from the trial. Out of the randomly enrolled participants, 133 received the study treatment (68 in the Crisugabalin group and 65 in the ALA group), who exhibited consistent demographic and baseline characteristics, with similar drug exposure profiles. The average age of the participants was 58.0 years. In terms of gender distribution, 42.6% of the Crisugabalin group and 47.7% of the ALA group were females. The ADPS, indicating the baseline pain intensity, was 5.769 for the Crisugabalin group and 5.883 for the ALA group. The baseline demographic characteristics were well-balanced between the two groups (Table 1).
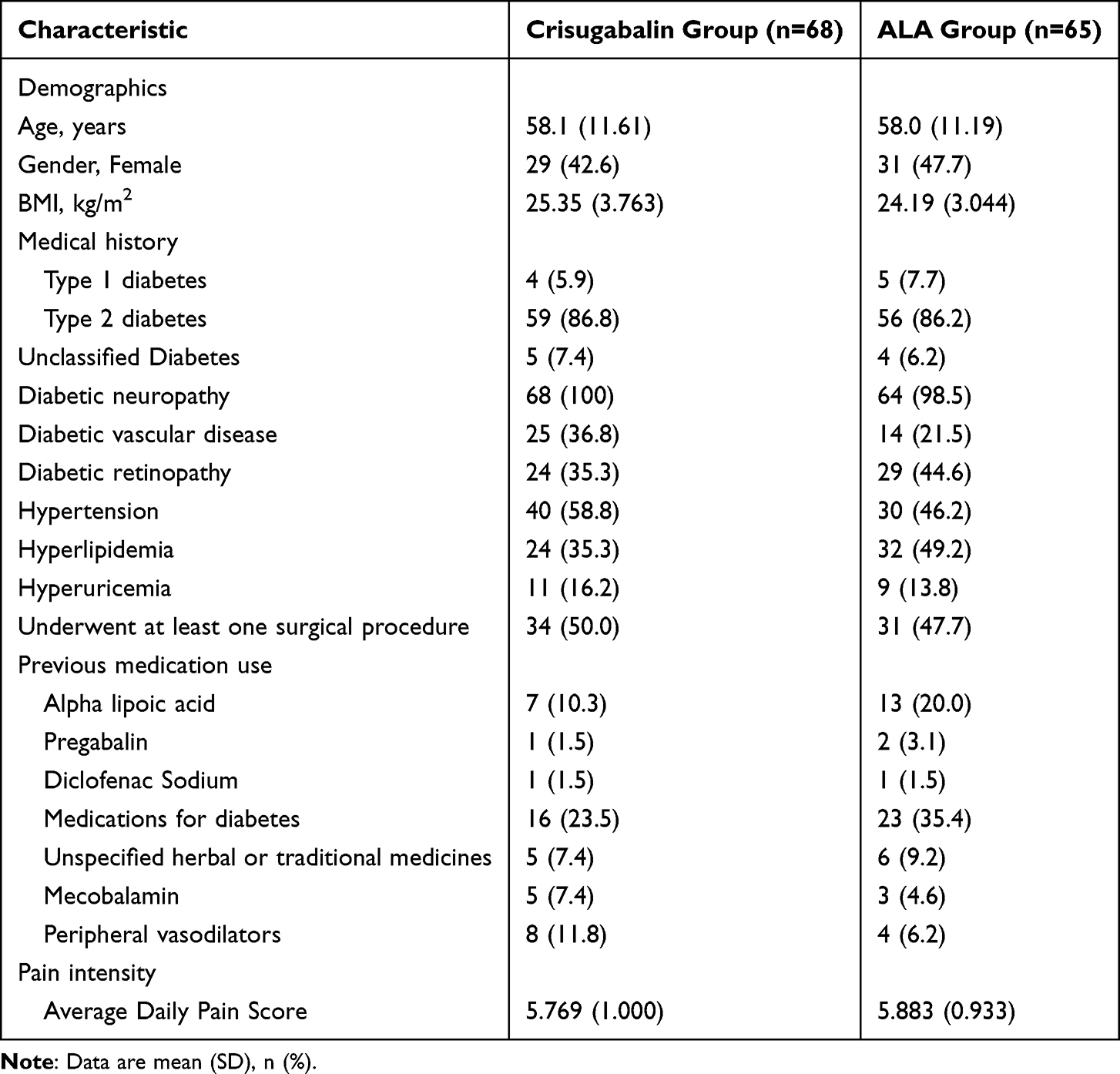 |
Table 1 Baseline Demographic, Diabetes, Previous Medication Uses, and Pain Intensity Characteristics of Participants |
All 133 were included in the Full Analysis Set (FAS) and Safety Set (SS). A total of 122 participants completed the study (62 in the Crisugabalin group and 60 in the ALA group) and were included in the Per Protocol Set (PPS). The primary study results were based on analyses of the FAS and PPS, with the FAS serving as the primary analysis set and the PPS as the supportive analysis set (Figure 1b).
Primary Efficacy Endpoint Analysis
ADPS, showed a significant reduction from baseline at week 12 in both groups, with the Crisugabalin group achieving a more pronounced decrease. The LSM change from baseline for the Crisugabalin group was −4.0 (95% CI: −4.405, −3.620) versus −2.1 (95% CI: −2.505, −1.706) for the ALA group. The LSM difference between the groups was −1.9 (95% CI: −2.458, −1.357), with the upper limit of the 95% CI being less than 0, indicating the superiority of the Crisugabalin group over the ALA group based on FAS analysis (Table 2 and Figure 2a). Figure 2b illustrates the pain reduction trajectory for both the Crisugabalin group and ALA group over the 12-week study period. From the outset, specifically during the first week, there was a substantial decrease in ADPS from baseline in both groups, indicating an early therapeutic effect. However, commencing from week 3 and continuing through to week 12, the Crisugabalin group consistently showed a significantly greater reduction in ADPS compared to ALA group at each assessed time point. The results based on PPS revealed that LSM for ADPS in the Crisugabalin group was −4.1, compared to −2.2 in ALA group. The LSM difference was −2.0 (95% CI: −2.522, −1.401), with a P-value of less than 0.0001. PPS results were consistent with the findings from the FAS, further validating the efficacy of Crisugabalin in reducing pain scores in patients with DPNP.
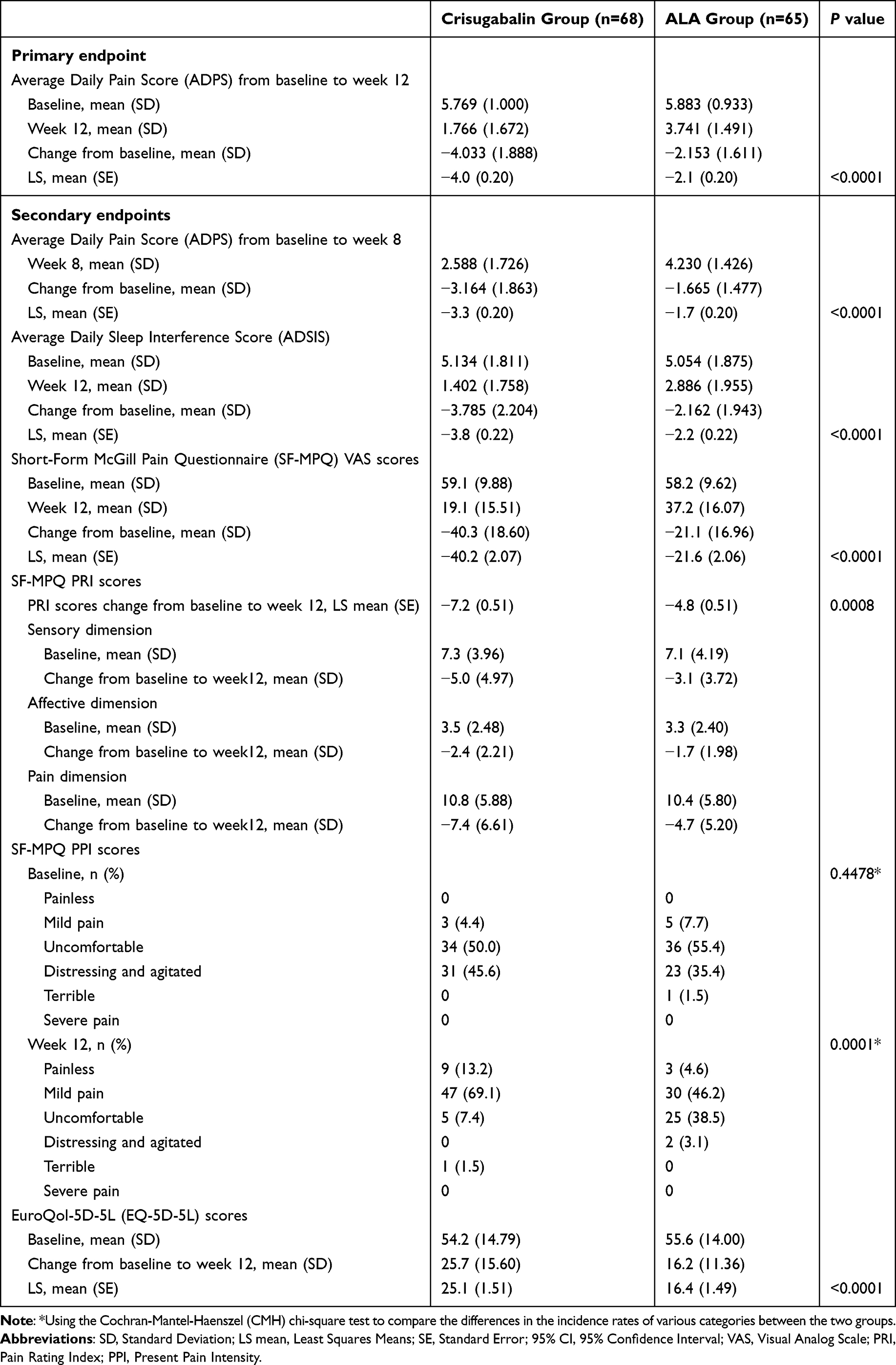 |
Table 2 Average Daily Pain Score, Short-Form McGill Pain Questionnaire (SF-MPQ) Scores, Average Daily Sleep Interference Score (ADSIS), and EuroQol-5D-5L (EQ-5D-5L) Scores, FAS |
 |
Figure 2 (a) The LSM difference of ADPS from baseline at week 12. (b) Change of ADPS from baseline to week 12. LSM: Least Squares mean, ADPS: Average Daily Pain Score (* P< 0.1; ** P< 0.001; *** P< 0.0001). (c) Comparison of ADPS reduction from baseline at week 12. (d) Proportion of patients achieving ADPS score of 3 or lower at week 12 between crisugabalin and ALA groups. |
The results of the sensitivity analysis for the primary efficacy measure were consistent with the FAS analysis. The least squares mean (SE) for the Crisugabalin group’s ADPS was −4.0 (0.20), and for the ALA group, it was −2.0 (0.20). The least squares mean difference (LSMD) in ADPS between the Crisugabalin group and the ALA group, along with its 95% confidence interval (CI), was −1.9 (−2.510, −1.388), with a P-value of less than 0.0001, and the upper limit of the 95% CI was below 0.
At week 12, a notable proportion of patients in the Crisugabalin group achieved a reduction in ADPS of ≥30% and ≥50% from baseline, specifically 83.8% and 77.9%, respectively, which were significantly higher than those observed in the ALA group, with corresponding P-values of 0.0002 and less than 0.0001 (Figure 2c) The percentage of patients with an ADPS score of 3 or lower was also higher in the Crisugabalin group (75.0% vs. 32.3%, P<0.0001) (Figure 2d).
We had integrated the analysis results based on individual patient data, as depicted in Figure 3, which visualized the improvement and maintenance of patients’ ADPS. The Crisugabalin group demonstrated a more rapid improvement in ADPS scores by week 6 (34.8% vs. 9.7%). By week 12, 73.8% of patients in the Crisugabalin group had achieved a state of painless to mild pain, compared to only 19.7% in the ALA group. Throughout the treatment period, the Crisugabalin group maintained a higher proportion of patients with painless to mild pain, indicative of sustained therapeutic efficacy.
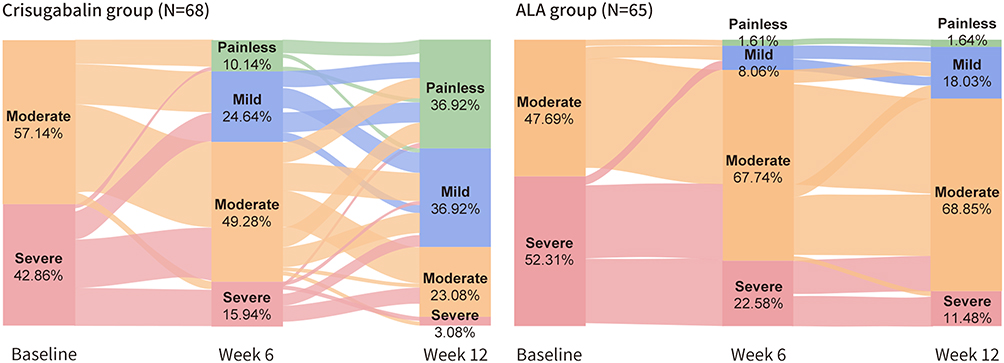 |
Figure 3 Patient Progression: Average Daily Pain Scores (ADPS) Changes from Baseline at weeks 6 and week 12. Pain is categorized as mild (ADPS≤3), moderate (3<ADPS<7), and severe (ADPS ≥7), with a score of 0 indicating no pain. At baseline, all patients were experiencing moderate to severe pain. |
Secondary Efficacy Endpoints Analysis
The Crisugabalin group demonstrated greater improvements compared to the ALA group at week 12, with significant LSM difference for ADSIS (−1.6, 95% CI: −2.217, −1.016) (Figure 4a). ADSIS in the Crisugabalin group also exhibited a significant drop after week 4 (Figure 4b). SF-MPQ Visual Analog Scale (VAS) (−18.6, 95% CI: −24.323, −12.869, P < 0.0001), and SF-MPQ Pain Rating Index (PRI) (−2.5, 95% CI: −3.892, −1.050, P = 0.0008) (Figure 4c and d). The proportion of participants reporting less pain on the SF-MPQ Present Pain Intensity (PPI) was significantly higher in the Crisugabalin group (P = 0.0001) (Table 2).
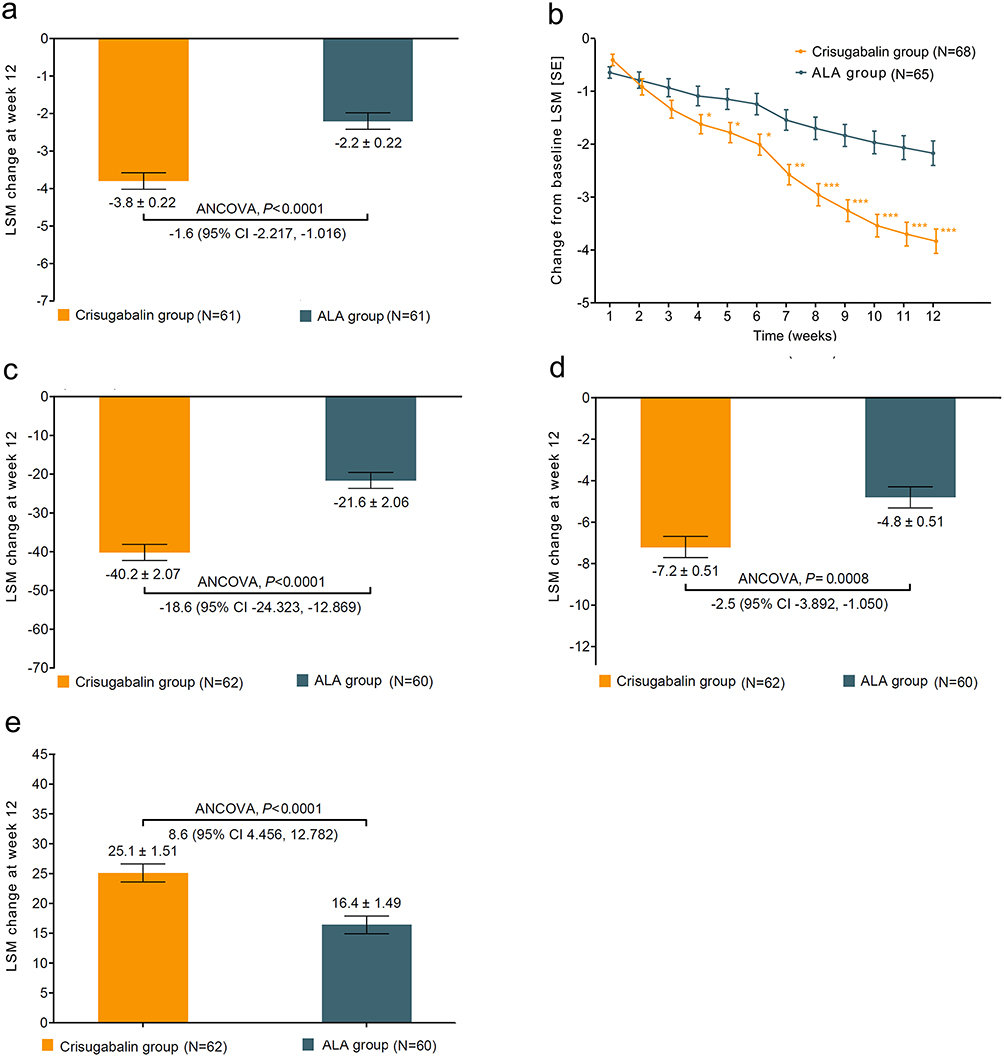 |
Figure 4 (a) Difference in ADSIS from baseline at week 12. (b) Change of ADSIS from baseline to week 12 (* P< 0.05; ** P< 0.001; *** P< 0.0001). (c) Difference in Short-Form McGill Pain Questionnaire (SF-MPQ) VAS scores from baseline at week 12. (d) Difference in SF-MPQ PRI scores from baseline at week 12. (e) Difference in EuroQol-5D-5L (EQ-5D-5L) scores from baseline at week 12. |
The EQ-5D-5L (EQ-VAS) score at week 12 showed a mean change from baseline of 25.1 (SE 1.51) in the Crisugabalin group and 16.4 (SE 1.49) in the ALA group, with a statistically significant difference between the groups (P < 0.0001) (Table 2 and Figure 4e).
Safety Outcomes
In the Crisugabalin group, 57.4% of subjects (39 out of 68) experienced a total of 68 TEAEs, with 27.9% of subjects (19 out of 68) having events related to Crisugabalin capsules. A small percentage, 5.9% (4 out of 68), had TEAEs graded as severe (CTCAE grade ≥3), and the same proportion reported SAEs. In contrast, the ALA group showed a slightly lower incidence of TEAEs, with 47.7% of subjects (31 out of 65) affected. TEAEs related to ALA were 15.4% (10 out of 65). 4.6% of participants experienced severe TEAEs and serious SAEs, with three individuals out of 65 affected by both (Table 3 and Supplementary Table 1).
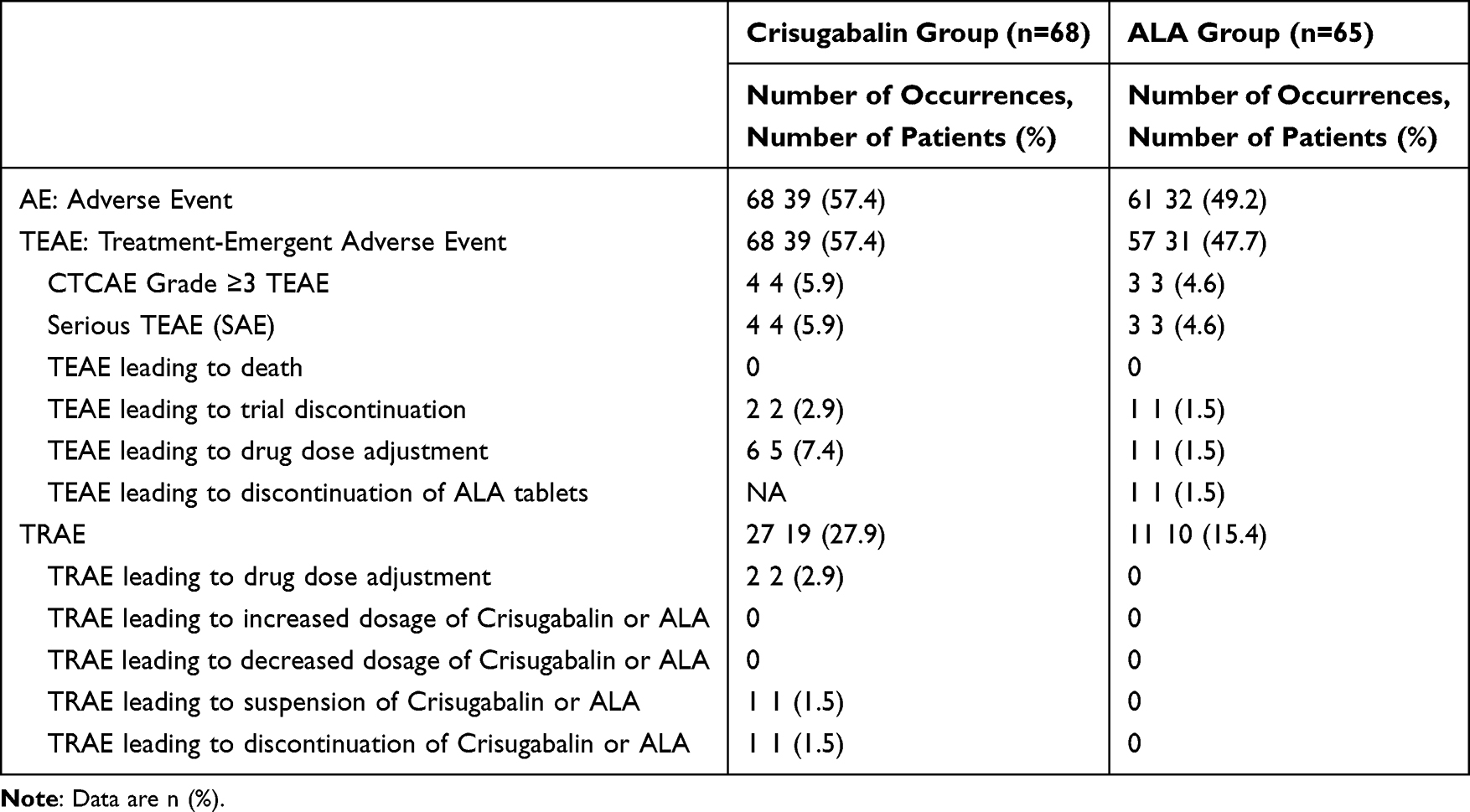 |
Table 3 Adverse Events Summary |
The majority of adverse events in both groups were mild to moderate and self-resolving or responded to minimal intervention. However, a small subset of events required medical treatment for improvement or resolution. The Crisugabalin group predominantly reported dizziness, somnolence, nausea, upper abdominal pain, chronic gastritis, diarrhea, and urinary tract infection as the most common TEAEs (≥1.0%). The ALA group commonly experienced abdominal pain, diarrhea, and urinary tract infection.
Treatment-emergent adverse events leading to study drug discontinuation were low in both groups, with no significant differences between the Crisugabalin and ALA groups. The safety profile of Crisugabalin was consistent with its mechanism of action, and the observed adverse events were manageable, reinforcing the overall safety of the treatment regimen in the context of this study.
Discussion
This phase 2 clinical trial provides evidence supporting the superior efficacy of Crisugabalin capsules combined with ALC over the ALA combination in reducing pain and improving sleep and quality of life in patients with DPNP. The safety profile of the Crisugabalin group was acceptable and manageable, with adverse events being generally mild to moderate.
Crisugabalin is the first calcium channel modulator approved in China for the treatment of DPNP, and it is one of only two medications with this indication in China. Current guidelines consistently recommend calcium channel modulators as first-line treatment for DPNP.3,24 Moreover, Crisugabalin has also been approved for the treatment of postherpetic neuralgia, a different neuropathic pain indication,26 suggesting that future research could explore its potential in a broader range of neuropathic pain conditions.
Our study is also the first to report the phase 2 results of Crisugabalin combination therapy, further confirming the efficacy of reducing pain scores and safety of the combined treatment approach. In our study, Crisugabalin combination therapy group achieved a notable outcome, with 75% of patients having ADPS of 3 or lower, which means the patient’s pain level is reduced to mild, and 77.9% of patients having over 50% reduction of ADPS at week 12 (Figure 2d). This finding is particularly advantageous when compared to previous researches in the field of DPNP. In previous phase 3 study, the monotherapy with Crisugabalin demonstrated significant efficacy in reducing pain.15 Specifically, the proportion of responders with at least a 30% or at least a 50% decrease were significantly higher in the Crisugabalin 40-mg/d group (57.3% or 32.0%, respectively) and 80-mg/d group (51.4% or 36.3%, respectively). These figures, while impressive, are lower than the response rates observed in our study with the combination therapy of Crisugabalin and ALC. Previous studies have shown that monotherapy with ALA can reduce patients’ pain intensity by approximately 30%, corresponding to a mean reduction of 1.7 points on the pain scale.18 In the PAIN-CARE trial, the proportion of patients in the ALA and Pregabalin combination therapy group who achieved a reduction of ≥30% in pain from baseline was 51%.27 In our study, the combination of ALA and ALC achieved a 35% reduction in ADPS, corresponding to a mean reduction of 2.1 points. However, the combination therapy with Crisugabalin demonstrated an even more significant reduction of 69% in ADPS, corresponding to a mean reduction of 4.0 points. These findings further highlighting the advantages of a combination treatment strategy. The recently published OPTION-DM study, which employed various treatment strategies including monotherapy and different combination therapies after six weeks, reported proportions of 32–48% for Numerical Rating Scale (NRS) scores of 3 or less at week 16, and 35–48% for those with a reduction in NRS of more than 50%.23
The progression of DPN is typically slow and influenced by factors such as hyperlipidemia, hypertension, obesity, aging, and hyperglycemia. It is unlikely that monotherapy can achieve clinical success in the treatment of DPN; therefore, this study employed a combination therapy with drugs of different mechanisms. As previously mentioned, the therapeutic effects of ALA and ALC in monotherapy have been confirmed in previous studies. A systematic review and meta-analysis suggested that a triple therapy of ALA, epalrestat, and mecobalamin may be more effective than monotherapy or dual therapy, with significant improvements in motor nerve conduction velocity (MNCV), sensory nerve conduction velocity (SNCV), peroneal MNCV, peroneal SNCV, and vibration perception threshold (VPT).28 Our study explored the combined use of Crisugabalin and ALC, aiming to address both pain relief and other sensory symptoms commonly experienced by patients. While ALC is known to ameliorate sensory disturbances such as numbness and tingling, its impact on pain is less pronounced.9,25 The integration of Crisugabalin, which has shown significant pain-reducing effects, with ALC’s neuroprotective properties, is intended to provide a more comprehensive therapeutic approach. This strategy potentially enhances the treatment of DPN by not only alleviating pain but also improving other related symptoms, thus offering a holistic benefit to patients’ overall management and quality of life. This trial was designed to assess symptomatic improvements rather than disease modification. The potential for long-term effects on the progression of DPN could be further explored through real-world evidence studies.
Figure 3’s visual representation of patient progress provides a holistic view of the therapeutic journey, highlighting the immediate and sustained benefits of Crisugabalin combination therapy. This treatment has shown its edge not merely in reducing mean ADPS scores but also in facilitating a swift pain downgrade by week 6 and maintaining a state of mild or no pain by week 12, as evidenced by individual patient data. This mode of presentation provides a novel perspective that can serve as a reference for future pain research, emphasizing the importance of individual patient trajectories in addition to group averages.
Improvements in sleep disturbance and quality of life indicators are also significant outcomes for DPNP patients.4,5 In this study, the results of ADSIS, SF-MPQ (PRI/PPI), and EQ-5D-5L scores showed that both treatment plans could improve patients’ sleep quality and quality of life; moreover, the Crisugabalin group was superior to ALA group, all results showing statistical differences, further proving the efficacy of Crisugabalin capsules from multiple dimensions such as pain relief, sleep improvement, and enhancement of life quality. The OPTION-DM study also confirmed that in different treatment paths, the Patient’s Global Impression of Change (PGIC) questionnaire at the end of treatment showed that 43–49% of patients felt “very much better” or “much better”, and there was still an improvement of 24–43% at the end of the study (week 50).23 The secondary endpoints of the PAIN-CARE study also indicated that combination therapy has more advantages in improving sleep quality and quality of life than monotherapy with ALA.27
When comparing the safety profiles of the two groups, the Crisugabalin group showed an acceptable and manageable safety profile, with the incidence and types of adverse events being consistent with the nature of the treatment and the condition being studied. The overall safety outcomes suggest that both treatments were well-tolerated, with no unexpected safety signals that would compromise the therapeutic potential of Crisugabalin in combination with ALC for the treatment of diabetic peripheral neuropathic pain. Compared with previous studies on ALC9,29,30 and Crisugabalin15 treatment of DPNP we also did not find any new adverse reactions or safety events associated with the combination therapy. The PAIN-CARE study also applied a combination treatment plan27 and did not suggest an increased safety risk.
Our study had some limitations. Pain relief-related studies for DPNP could consider using a placebo-controlled and crossover study design to accurately assess the effects of monotherapy or combination therapy drugs, but such designs would require a longer time to verify the results and would increase the complexity of the study design and the difficulty of patient screening and enrollment. As a phase 2 study, we did not use a complex study design but used a positive control drug for comparison, achieving superior results and providing reliable data for subsequent studies. Due to the limited sample size of the phase 2 study, we did not assess the efficacy rate of pain treatment, the impact of previous treatments, or other subgroup analyses.
Conclusions
In conclusion, this phase 2 trial provides preliminary evidence supporting for the potential use of Crisugabalin capsules combined with ALC as a novel treatment option for DPNP, offering not only pain relief but also improvements in sleep and quality of life for affected patients. Given the exploratory nature of this phase 2 study, these findings should be interpreted with caution and require powered phase 3 trials. The findings position this combination as a candidate for further development and consideration in future clinical guidelines for DPNP treatment.
Data Sharing Statement
The de-identified participant data that support the findings of this study are available upon request from researchers affiliated with academic or scientific organizations. Requests for access to the data should be directed to the corresponding author [Hongwei Jiang, [email protected]] for a period of 2 years following the publication of this manuscript. The data are not publicly available due to privacy restrictions that protect the confidentiality of research participants. Access to the data will be granted by the sponsor [Hongwei Jiang] after review and approval of a research proposal and upon signing a data access agreement.
Ethics Approval and Consent to Participate
This study adhered to the Declaration of Helsinki and was approved by the Ethics Committees of The First Affiliated Hospital of Henan University of Science and Technology (approval No. 2023-0141), Nanyang Central Hospital (approval No. 2023-028-01), Nanyang Second General Hospital (approval No. 2023-01-018-H01), and the Luoyang First People’s Hospital (approval No. EC-2023-188- (1)). Inclusion criteria mandated that participants be adults aged 18 years or older, capable of understanding the study’s implications and voluntarily providing written informed consent.
Acknowledgments
We extend our gratitude to all the participants who contributed to this trial, and to the investigators and staff at the participating sites for their dedication and efforts. The study was sponsored by Haisco Pharmaceutical Group Co., Ltd. which played a role in the study design, data collection, analysis, interpretation, and reporting. Special thanks are due to Meta Clinical Technology Co., Ltd., for their statistical support throughout the study. We also acknowledge the contributions of the nursing and administrative staff, whose work was pivotal to the trial’s smooth operation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Haisco Pharmaceutical Group Co., Ltd. (grant number: HSK16149-206).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jang HN, Oh TJ. Pharmacological and nonpharmacological treatments for painful diabetic peripheral neuropathy. Diabetes Metab J. 2023;47(6):743–14. doi:10.4093/dmj.2023.0018
2. Ziegler D, Landgraf R, Lobmann R, et al. Painful and painless neuropathies are distinct and largely undiagnosed entities in subjects participating in an educational initiative (PROTECT study). Diabet Res Clin Pract. 2018;139:147–154. doi:10.1016/j.diabres.2018.02.043
3. Bril V, England JD, Franklin GM, et al. Evidence-based guideline: treatment of painful diabetic neuropathy--report of the American association of neuromuscular and electrodiagnostic medicine, the American academy of neurology, and the American academy of physical medicine & rehabilitation. Muscle Nerve. 2011;43(6):910–917. doi:10.1002/mus.22092
4. Pop-Busui R, Ang L, Boulton AJM, et al. Diagnosis and treatment of painful diabetic peripheral neuropathy. ADA Clinical Compendia. 2022;2022(1):1–32. doi:10.2337/db2022-01
5. Pain Group of Chinese Society of Pain Medicine, Chinese Medical Association. Expert consensus on the diagnosis and treatment of diabetic peripheral neuropathic pain. Chin J Pain Med. 2018;24(08):561–567.
6. Jensen TS, Baron R, Haanpää M, et al. A new definition of neuropathic pain. Pain. 2011;152(10):2204–2205. doi:10.1016/j.pain.2011.06.017
7. Morales-Vidal S, Morgan C, McCoyd M, Hornik A. Diabetic peripheral neuropathy and the management of diabetic peripheral neuropathic pain. Postgrad Med. 2012;124(4):145–153. doi:10.3810/pgm.2012.07.2576
8. Colloca L, Ludman T, Bouhassira D, et al. Neuropathic pain. Nat Rev Dis Primers. 2017;3(1):17002. doi:10.1038/nrdp.2017.2
9. Guo L, Pan Q, Cheng Z, et al. Acetyllevocarnitine hydrochloride for the treatment of diabetic peripheral neuropathy: a phase 3 randomized clinical trial in China. Diabetes. 2024;73(5):797–805. doi:10.2337/db23-0377
10. Knabl J, Witschi R, Hösl K, et al. Reversal of pathological pain through specific spinal GABAA receptor subtypes. Nature. 2008;451(7176):330–334. doi:10.1038/nature06493
11. Stahl SM, Porreca F, Taylor CP, Cheung R, Thorpe AJ, Clair A. The diverse therapeutic actions of pregabalin: is a single mechanism responsible for several pharmacological activities? Trends Pharmacol Sci. 2013;34(6):332–339. doi:10.1016/j.tips.2013.04.001
12. Catterall WA. Voltage-gated calcium channels. Cold Spring Harb Perspect Biol. 2011;3(8):a003947. doi:10.1101/cshperspect.a003947
13. Bhusal S, Diomampo S, Magrey MN. Clinical utility, safety, and efficacy of pregabalin in the treatment of fibromyalgia. Drug Healthc Patient Saf. 2016;8:13–23. doi:10.2147/dhps.S95535
14. Wu Q, Zhu H, Song R, et al. Effect of a high-fat and high-calorie food on the pharmacokinetics of a novel, potent GABA analog HSK16149 in healthy subjects. Pharmacol Res Perspect. 2023;11(3):e01102. doi:10.1002/prp2.1102
15. Guo X, Zhang T, Yuan G, et al. GABA analogue HSK16149 in Chinese patients with diabetic peripheral neuropathic pain: a phase 3 randomized clinical trial. JAMA Network Open. 2024;7(8):e2425614. doi:10.1001/jamanetworkopen.2024.25614
16. Hounsom L, Horrobin DF, Tritschler H, Corder R, Tomlinson DR. A lipoic acid-gamma linolenic acid conjugate is effective against multiple indices of experimental diabetic neuropathy. Diabetologia. 1998;41(7):839–843. doi:10.1007/s001250050996
17. Moon SS, Kim CH, Kang SM, et al. Status of diabetic neuropathy in korea: a national health insurance service-national sample cohort analysis (2006 to 2015). Diabetes Metab J. 2021;45(1):115–119. doi:10.4093/dmj.2020.0120
18. Won JC, Kwon HS, Moon SS, et al. γ-linolenic acid versus α-lipoic acid for treating painful diabetic neuropathy in adults: a 12-week, double-placebo, randomized, noninferiority trial. Diabetes Metab J. 2020;44(4):542–554. doi:10.4093/dmj.2019.0099
19. Tomassoni D, Di Cesare Mannelli L, Bramanti V, Ghelardini C, Amenta F, Pacini A. Treatment with acetyl-L-carnitine exerts a neuroprotective effect in the sciatic nerve following loose ligation: a functional and microanatomical study. Neural Regen Res. 2018;13(4):692–698. doi:10.4103/1673-5374.230297
20. Wilson AD, Hart A, Wiberg M, Terenghi G. Acetyl-l-carnitine increases nerve regeneration and target organ reinnervation - a morphological study. J Plast Reconstr Aesthet Surg. 2010;63(7):1186–1195. doi:10.1016/j.bjps.2009.05.039
21. Di Stefano G, Di Lionardo A, Galosi E, Truini A, Cruccu G. Acetyl-L-carnitine in painful peripheral neuropathy: a systematic review. J Pain Res. 2019;12:1341–1351. doi:10.2147/jpr.S190231
22. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/s1474-4422(14)70251-0
23. Tesfaye S, Sloan G, Petrie J, et al. Comparison of amitriptyline supplemented with pregabalin, pregabalin supplemented with amitriptyline, and duloxetine supplemented with pregabalin for the treatment of diabetic peripheral neuropathic pain (OPTION-DM): a multicentre, double-blind, randomised crossover trial. Lancet. 2022;400(10353):680–690. doi:10.1016/s0140-6736(22)01472-6
24. Zhu Q, Fan B, Zhang D, Yu SY, Fu ZJ, Lv Y. Chinese expert consensus on the diagnosis and treatment of peripheral neuropathic pain. Chin J Pain Med. 2020;26(5):321–328.
25. Didangelos T, Karlafti E, Kotzakioulafi E, et al. Efficacy and safety of the combination of superoxide dismutase, alpha lipoic acid, vitamin B12, and carnitine for 12 months in patients with diabetic neuropathy. Nutrients. 2020;12(11):3254. doi:10.3390/nu12113254
26. Zhang D, Lei T, Qin L, et al. Efficacy and safety of crisugabalin (HSK16149) in adults with postherpetic neuralgia: a phase 3 randomized clinical trial. JAMA dermatol. 2024;160(11):1182. doi:10.1001/jamadermatol.2024.3410
27. Gilron I, Robb S, Tu D, et al. Randomized, double-blind, controlled trial of a combination of alpha-lipoic acid and pregabalin for neuropathic pain: the PAIN-CARE trial. Pain. 2024;165(2):461–469. doi:10.1097/j.pain.0000000000003038
28. Ran GL, Li YP, Lu LC, Lan SH. Disease-modifying therapies for diabetic peripheral neuropathy: a systematic review and meta-analysis of randomized controlled trials. J Diabetes Complications. 2024;38(2):108691. doi:10.1016/j.jdiacomp.2024.108691
29. Li S, Chen X, Li Q, et al. Effects of acetyl-L-carnitine and methylcobalamin for diabetic peripheral neuropathy: a multicenter, randomized, double-blind, controlled trial. J Diabetes Investig. 2016;7(5):777–785. doi:10.1111/jdi.12493
30. De Grandis D, Minardi C. Acetyl-L-carnitine (levacecarnine) in the treatment of diabetic neuropathy. A long-term, randomised, double-blind, placebo-controlled study. Drugs R D. 2002;3(4):223–231. doi:10.2165/00126839-200203040-00001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Discussion on the Application of Mindfulness Therapy in the Treatment of Diabetic Peripheral Neuropathy: A Narrative Review
Fan Q, Yu S, Sun X, Dong Y, Chen Y, Jia L
Psychology Research and Behavior Management 2025, 18:1729-1747
Published Date: 12 August 2025