Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
Evaluating the Fragility of Long-Term Outcomes for Neoadjuvant versus Adjuvant Chemotherapy Prescription in Early Breast Cancer: Pooled Data from 10 Randomised Clinical Trials
Received 29 June 2022
Accepted for publication 16 August 2022
Published 17 October 2022 Volume 2022:14 Pages 343—350
DOI https://doi.org/10.2147/BCTT.S379393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Matthew G Davey, Michael J Kerin
Department of Surgery, The Lambe Institute for Translational Research, National University of Ireland, Galway, H91YR71, Ireland
Correspondence: Matthew G Davey, Department of Surgery, The Lambe Institute for Translational Research, National University of Ireland, Galway, H91YR71, Ireland, Tel +35391524411, Email [email protected]
Introduction: Randomised clinical trials (RCTs) report similar outcomes following neoadjuvant (NAC) and adjuvant chemotherapy (AC) in breast cancer. “Fragility Indices” (FI) test significance reversal reported in RCTs.
Aim: To evaluate the FI of findings from RCTs assessing outcomes of NAC and AC.
Methods: A systematic review was performed as per PRISMA guidelines. RCTs of interest were identified and data pooled. Fisher’s exact test was used to calculate FI for reversal of statistical significance for dichotomous outcomes. “Fragility Quotient” (FQ) was calculated by division of the calculated FI by the sample size.
Results: Ten RCTs including 4928 patients. Mean follow-up was 8.2 years. For breast conservation surgery (BCS), the FI was 500 and FQ was 0.10781. For local recurrence (LR), the FI was 42 and FQ was 0.00852. FI and FQ varied for LR at 0– 4 years (FI: 9), 5– 9 years (FI: 2), 10– 14 years (FI: 4), and 15+ years (FI: 3). Regarding distant recurrence (DR), the FI was 13 and FQ was 0.00264. FI and FQ trended downwards over time: 0– 4 years (FI: 56), 5– 9 years (FI: 18), 10– 14 years (FI: 4), and 15+ years (FI: 4). For breast-cancer-specific mortality (BCSM), the overall FI was 51 and FQ was 0.01035. FI and FQ varied for BCSM at 0– 4 years (FI: 5), 5– 9 years (FI: 19), 10– 14 years (FI: 8), and 15+ years (FI: 5). For overall survival (OS), the FI was 17 and FQ was 0.00345. FI and FQ were calculated with respect to OS at 0– 4 years (FI: 19), 5– 9 years (FI: 17), 10– 14 years (FI: 19), and 15+ years (FI: 1).
Conclusion: FIs comparing survival following NAC and AC were of moderate-to-high fragility, indicating weak statistical significance. BCS eligibility following NAC was of low fragility, ratifying the oncological and surgical safety of NAC versus AC.
Level of Evidence: Systematic Review of Level I Randomised Control Trials.
Keywords: Fragility Index, breast cancer, statistics, chemotherapy, patient outcomes
Introduction
Breast Oncology has evolved to recognise the inherent value of treating patients with chemotherapy in the neoadjuvant setting. Advantages of prescribing neoadjuvant chemotherapy (NAC) included tumour downstaging, increasing patient eligibility for breast conservation surgery (BCS), as well as the generation of in-vivo data regarding tumour sensitivity to systemic therapies, which has been illustrated to carry prognostic significance for long-term survival.1–4 In the data generated by the Early Breast Cancer Triallist’s Collaborative Group (EBCTCG) in their meta-analysis of 10 randomised clinical studies, survival outcomes observed following NAC were similar to those treated with adjuvant chemotherapy (AC)5 (15-year breast cancer-specific mortality (BCSM) of 34.4% for NAC vs 33.7% for AC), supporting the oncological safety of NAC in clinical practice. Additionally, these data highlighted that patients undergoing NAC are more likely to achieve BCS (65.0% vs 49.0%), however these findings were offset by increased risk of local recurrence (LR) (NAC: 21.4% vs AC: 15.9%).5 While such findings are important for patient counselling prior to NAC prescription, the EBCTCG concluded that despite the increased LR risk following NAC, distant recurrence (DR), BCSM, and overall survival (OS) outcomes were similar in their study. Nevertheless, the robustness of these findings is yet to face statistical interrogation or appraisal.
Prospective, randomised clinical trials (RCTs) represent the highest level of evidence for the clinical evaluation of optimal treatment strategies in managing disease and currently serve as the gold standard methodology in medical research.6 The results presented in RCTs are typically reported with reference to achieving statistical significance, typically defined as a P-value with a chosen alpha threshold of less than 0.050.7 Clinicians often rely heavily upon such results in the hope of making the correct treatment decisions for their patients. However, P-values, and with their associated chosen alpha threshold, are often chosen in arbitrary fashion, with little consideration of a variety of factors, including sample size, data spread, as well as the failure to consider the clinical implication of statistically significant differences in results if adopted into routine clinical practice.8,9
Assessing the “Fragility” of reported results was first described by Walsh et al, as a means of testing the robustness of results and aiding the interpretation of statistically significant results reported in RCT data.10 In brief, the “Fragility Index” (or FI) aids in determining whether the statistical significance reported in an RCT may be lost due to the intentional shift of dichotomous events from the experimental arm to the control arm within the trial,11 thus interrogating and testing the reversal of statistical significance. FI investigates this by simply and pragmatically increasing the results of one of the sample sizes by one outcome event and then reassessing the significance of the outcome. The calculated FI for each outcome is the smallest number of additional events required to reverse statistical significance (eg: if the original data were significant with a P-value less than 0.050, outcomes would be added and reassessed one at a time until the P-value became greater than or equal to 0.05). The number of added outcomes required to alter significance refers to the “fragility” of the analysis.
The emergence of FI brings into question the validity of the interpretation of previously reported analyses, which may over- or underestimate the impact of certain treatments on patient outcomes. As previously outlined, the EBCTCG previously highlighted the oncological safety of NAC relative to AC in an analysis of 10 RCTs,5 however no previous analyses have been performed evaluating the fragility of these results. Accordingly, the aim of this study was to evaluate the “Fragility Index” of statistically significant findings reported in RCTs assessing oncological outcomes of NAC and AC in early breast cancer.
Methods
A systematic review was performed in accordance to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist and meta-analysis and systematic reviews of observational studies (MOOSE) guidelines.12,13
Search Strategy
An electronic search was performed of the PubMed, Cochrane and Scopus databases on the 11th May 2022 for relevant studies which would be suitable for inclusion in this study. The search was performed of all fields under the following headings: (neoadjuvant therapies[MeSH Terms]), (adjuvant therapies[MeSH Terms]), (breast cancer[MeSH Terms]), (clinical trial, randomized[MeSH Terms]), which were linked with the Boolean operator “AND”. Ten RCTs included in the EBCTCG were extracted in parallel and included.5 Included studies were limited to those published in the English language. Included studies were not restricted based on year of publication but did have to report robust patient-specific long-term follow-up. Following the removal of duplicate studies, all titles were initially screened, and studies deemed relevant had their abstracts and full texts reviewed. Following this, the pre-determined inclusion criteria was used in assessing the full manuscript of all potentially eligible studies.
Eligibility Criteria
Prior to commencement of the search, the authors agreed on pre-determined inclusion, exclusion criteria, and designed a data collection sheet for use in this study. The inclusion criteria for this study were as follows: (1) patients being treated in the RCT setting with NAC or AC for early-stage breast cancer, (2) long-term survival outcomes (ie: LR, DR, BCSM, or OS, etc.) had to be available, (3) statistical significance reported for at least one dichotomous outcome measure (ie, P<0.050 under a null hypothesis that no difference existed or a 95% confidence interval that excluded a null value), (4) published in the English language, and (5) manuscript published in a peer-reviewed journal. The exclusion criteria included: (1) studies failing to meet the inclusion criteria, (2) non-RCT studies, (3) no statistical significance found for any of the dichotomous outcome measure reported in the study, and (4) conference abstracts.
Data Extraction and Risk Assessment
Using the aforementioned pre-determined data collection sheet, assessment of each of the included manuscripts of the included studies was performed to gather all relevant data for analysis. For each study, data for all dichotomous outcomes of interest were collected and tabulated. Data extracted included: (1) first author name, (2) year of publication, (3) study design, (4) country of origin, (5) number of patients, (6) Follow up, (7) numbers of patients in receipt of NAC, (8) numbers of patients in receipt of AC, (9) BCS eligibility rates, (10) LR rates, (11) DR rates, (12) BCSM rates, and (13) OS rates. In cases where RCT data were unavailable following review of the full-text, cross referencing with the EBCTCG study was performed.5 The trial-level risk of bias was assessed using the Cochrane Collaboration’s Risk of Bias Tool.14
Statistical Analysis with Application of Fragility Index
The Fisher’s Exact (†) test was used as appropriate to determine the association between clinical and surgical outcomes following NAC and AC.15 With reference to the method previously described by Walsh et al,10 the FI for each dichotomous outcome of interest was calculated. This analysis involved manipulating the reported outcome events using Fisher's exact test in a 2×2 contingency table,15 until a potential reversal of significance was calculated, with statistical significance defined as P < 0.050. This involved adding one potential event to the group with a smaller number of events, whilst simultaneously subtracting one potential non-event from the same group in order to maintain the total number of participants constant. This step was repeated with each potential event being added in the aforementioned manner until Fisher's exact test found a reversal of statistical significance. The term “Fragility Index” for each outcome was the smallest number of additional potential events required to reverse statistical significance, ie, the calculated P value became greater than or equal to 0.05. This is further illustrated in Figure 1. The “Fragility Quotient” (FQ) was calculated by division of the calculated FI by the sample size; this aims to standardize the fragility to the sample size of a trial, with smaller FQ suggesting a less robust study outcome. Quantitative statistical analysis was performed using SPSS version 26.0 (IBM Corp. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp.)
 |
Figure 1 Illustration of how the alteration of two events results in alteration of statistical significance, demonstrating the concept of “Fragility”. |
Results
Literature Search
The initial literature search resulted in 1754 studies for systematic evaluation. After the removal of 239 duplicates, the remaining 1515 studies were screened using our exclusion criteria. Thereafter, our inclusion criteria were applied to the full texts of the remaining 18 studies to screen for eligibility. Overall, 10 RCTs were included in this study and had their data pooled for assessment of FI.16–25 Figure 2 illustrates the systematic search process.
 |
Figure 2 PRISMA flowchart illustrating of the systematic search process. |
Study Characteristics and Risk of Bias Assessments
Of the 10 included RCTs, 7 of these were performed in European translation research facilities.16,18–23 The publication dates of the included studies ranged from 1991 to 2009. In these 10 RCTs, data from 4928 patients were collated with a mean follow-up of 8.2 years. Of these, 45.7% of patients underwent NAC (2254/4928) and 54.3% underwent AC (2674/4928). In total, 30.0%, 50.0%, and 20.0% of these included RCTs had low-, some, and high-risk of biases, respectively. Basic study characteristics are outlined in detail in Table 1.
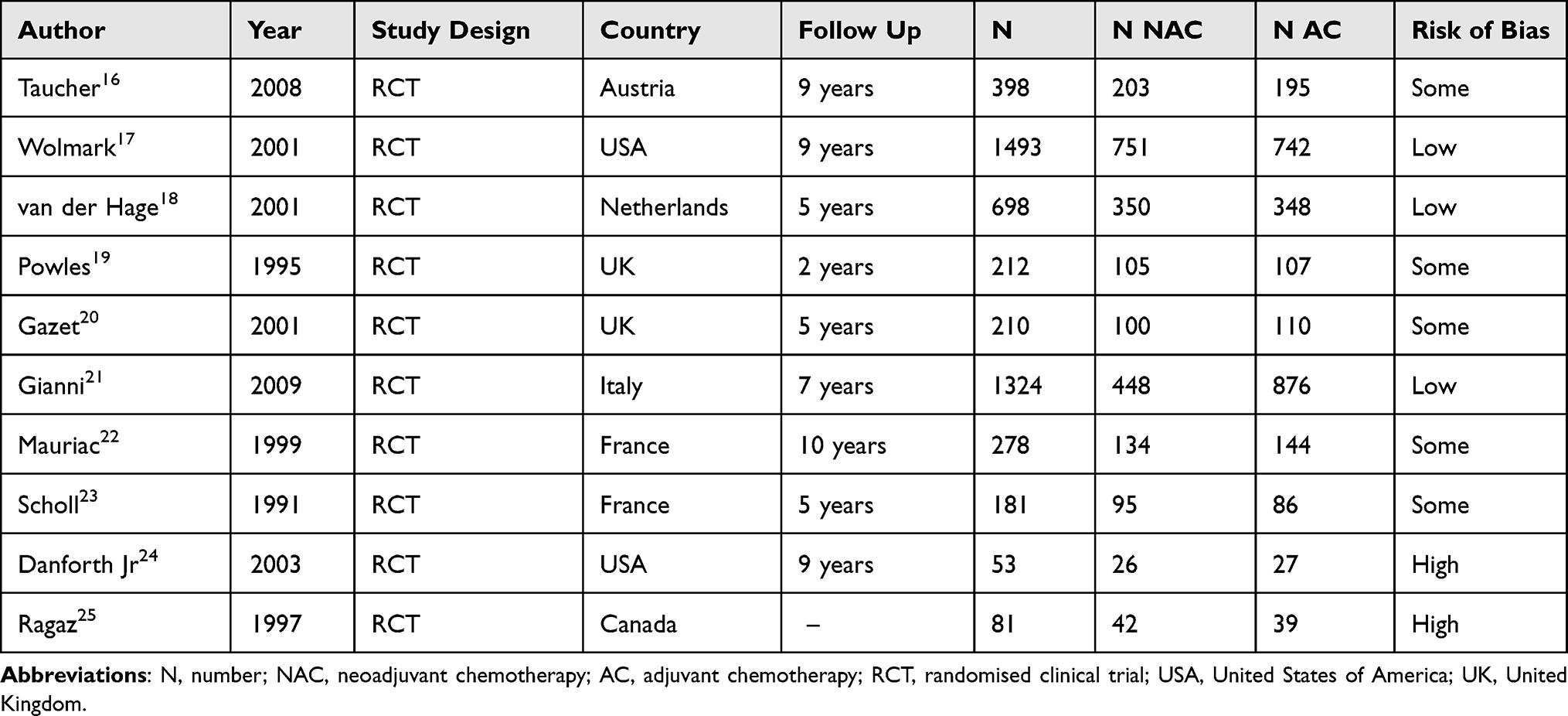 |
Table 1 Data from the 10 Included Prospective Randomised Clinical Trials |
Breast Conservation Surgery
In total, 50.4% of patients included in this study underwent BCS (2485/4928). Of those undergoing NAC, 59.5% successfully underwent BCS (1316/2254) compared to 43.7% of those in receipt of AC (1169/2674) (P<0.001, †). With respect to BCS, the FI was 500 and the associated FQ was 0.10781. Surgical and survival data are outlined in Table 2.
 |
Table 2 Surgical, Oncological, and Survival Data from the 10 Included Prospective Randomised Clinical Trials |
Local Recurrence
Overall, 12.6% of patients suffered LR (623/4928). Of those in receipt of NAC, 15.3% suffered LR (345/2254) compared to 10.4% of those who received AC (278/2674) (P<0.001, †). The FI for LR was 42 and the associated FQ was 0.00852. FI and FQ were calculated with respect to LR at 0–4 years (FI: 9, FQ: 0.00047), 5–9 years (FI: 2, FQ: 0.00018), 10–14 years (FI: 4, FQ: 0.00072), and 15+ years (FI: 3, FQ: 0.00195), respectively.
Distant Recurrence
Overall, 33.2% of patients suffered DR (1638/4928). Of those in receipt of NAC, 35.1% suffered DR (791/2254) while 31.7% of those who received AC (847/2674) (P=0.012, †). The overall FI for DR was 13 and the associated FQ was 0.00264. FI and FQ were calculated with respect to DR at 0–4 years (FI: 56, FQ: 0.00283), 5–9 years (FI: 18, FQ: 0.00144), 10–14 years (FI: 4, FQ: 0.00006), and 15+ years (FI: 4, FQ: 0.00208), respectively.
Breast Cancer Specific Mortality
Overall, 25.7% of patients suffered BCSM (1266/4928). Of those in receipt of NAC, 28.6% suffered BCSM (644/2254) while 23.3% of those who received AC (622/2674) (P<0.001, †). The overall FI for BCSM was 51 and the associated FQ was 0.01035. FI and FQ were calculated with respect to BCSM at 0–4 years (FI: 5, FQ: 0.00024), 5–9 years (FI: 19, FQ: 0.00014), 10–14 years (FI: 8, FQ: 0.00112), and 15+ years (FI: 5, FQ: 0.00242), respectively.
Overall Survival
Overall, 33.3% of patients died in this study (1640/4928). Of those in receipt of NAC, 35.5% died (801/2254), as did 31.4% of those who received AC (839/2674) (P = 0.002, †). The overall FI for OS was 17 and the associated FQ was 0.00345. FI and FQ were calculated with respect to OS at 0–4 years (FI: 19, FQ: 0.00091), 5–9 years (FI: 17, FQ: 0.00125), 10–14 years (FI: 19, FQ: 0.00180), and 15+ years (FI: 1, FQ: 0.00049), respectively.
Discussion
The pooled data from the ten randomised clinical trials included in this analysis coherently illustrated the oncological safety of NAC relative to AC for patients treated with curative intent for early breast cancer. While these results are widely accepted in global practice, the robustness of these pooled findings had previously not been interrogated for “fragility”. This FI analysis illustrated that results in relation to LR, DR, BCSM, and OS outcomes following NAC and AC demonstrated moderate “fragility” overall. Therefore, this FI analysis adds further meaning to these previously reported results and may aid the clinician when counselling the patient indicated to undergo standard-of-care chemotherapy by using “fragility”, as opposed to simple interpretation of P-values in isolation. Furthermore, these data demonstrated little “fragility” with respect to the use of NAC to increase patient eligibility for BCS, therefore fortifying the increase in NAC prescription which has come into vogue in recent times, due to the advantages of this strategy in substraifiying cancer subtypes.4,26 Notwithstanding, judicious application of FI is warranted, as “fragility” analyses alone are not robust enough to revoke multidisciplinary decisions regarding systemic therapies when treating patients with early breast cancer.
The EBCTCG comprehensively illustrated the oncological safety of NAC relative to AC,5 with the exception of the increased propensity to develop LR following NAC (LR: 21.4% vs 15.9% following AC). These are important findings, which have revolutionised the management of early stage disease, despite demonstrating moderate-to-high “fragility”: Overall LR had an FI of 42 (with an associated FQ of 0.00852), which had the tendency to increase in the “fragility” of results as time elapsed from 0 to 15 years, as the number of patients and events analysed decreasing during this time. These findings are of the utmost importance as the exponential increase in “fragility” observed over time highlights the non-inferiority of using NAC in attempt to establish locoregional control post-treatment treatment. Thus, the high “fragility” observed with respect to LR should be interpreted to exemplify the oncological safety of NAC relative to AC, and support NAC prescription in the setting of early disease, where feasible.
Interestingly, the results illustrating the increased risk of LR following NAC may be offset by the incredibly low “fragility” associated with successfully achieving breast conservation following NAC. The FI for BCS eligibility following NAC was remarkably high at 500 (with an associated FQ of 0.10781), which is unquestionably the least “fragile” result reported in this analysis. This is an incredibly important finding on account of the management paradigm for early breast cancer now supporting robust NAC prescription where possible for all patient with stage I–III cancers which are substratified into the HER2-positive or triple negative (TNBC) molecular subgroups (with exceptions limited to T1a-1b/N0 disease). Therefore, this “fragility” analysis emphasises the pragmatic use of NAC to increase patient eligibility for BCS, by further interrogating the results without hinging all reliance on P-values in isolation. While the tendency for evidence-based clinical decisions in surgery has developed through reliance solely on P-values, this result clearly highlights the importance of FI assessment to extenuate the robustness of findings beyond statistical significance as reported by P-values (and their selected alpha threshold). For example, this study reported P<0.001 for both BCS eligibility and LR following NAC, yet the FI for LR is more than 10 times more “fragile” than that reported for BCS, despite both results being represented by the same P-value. The provision of high-quality, evidence-based clinical decisions in clinical practice may incorporate robust FI analyses into the paradigm as a means of further optimising clinical outcomes for our prospective patients.
Interestingly, the FI associated with long-term survival outcomes illustrated moderate-to-high fragility, further emphasising the similar oncological safety anticipated with NAC and AC prescription. Overall, the FI associated with BCSM was 51 (with associated FQ of 0.01035) compared to 17 for OS (with associated FQ of 0.00345). These findings suggest that despite differences in survival outcomes following NAC and AC, these differences should be subject to scrutiny, as there is little difference in patient outcomes observed in this pooled analysis, as exemplified by the moderate-to-high “fragility” of the results.
Limitations
The primary limitation of this analysis relates to the fact that FI may only be applied to evaluate dichotomous outcomes, with no analysis of continuous variables. Of course, many oncological and survival outcomes of interest in breast oncology are reported in a dichotomous nature, however several continuous outcome measures will inevitably be missed. Secondly, it is unfortunately beyond the scope of FI to account for confounding factors, such as variance in patient demographics, clinicopathological or biological tumour subtypes, surgical techniques and patient compliance, which inevitably will impact results. Prospective trials of randomised design were pragmatically included in an attempt to overcome this risk of confounding biases, however acknowledgement for this possibility is required. Thirdly, while Walsh et al emphasise the importance of the FI in identifying less robust results, as the time of writing, there are no conventional cut-offs in relation to the “fragility” of results described. Therefore, interpretation of fragility is arbitrary and left open to the interpretation of those conducting the investigation. Finally, within current contemporary breast cancer management, “fragility” analyses are unlikely to refute therapeutic or surgical decisions made by the multidisciplinary team in accordance with expert consensus statements and guidelines. Therefore, the importance of such results may be brought into question and construed to only serve as an “academic” exercise. Nevertheless, in spite of these limitations, the authors wish to emphasise the importance of using metrics such as FI and FQ to facilitate the continuous interrogation of the evidence-base with the ambition of further improving clinical outcomes for our prospective patients.
In conclusion, with the exception of low “fragility” in relation to patient eligibility for BCS following NAC, the “fragility” indices of comparisons between oncological and survival outcomes following NAC and AC are typically of moderate-to-high “fragility” indicating weak statistical significance. Therefore, this analysis further validates the oncological safety of NAC prescription in early breast cancer. Prospective interrogation of RCT “fragility” is imperative to ensure optimisation of oncological and survival outcomes for our prospective patients diagnosed with early stage breast cancer.
Funding
National Breast Cancer Research Institute, Ireland.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cho JH, Park JM, Park HS, Park S, Kim SI, Park BW. Oncologic safety of breast-conserving surgery compared to mastectomy in patients receiving neoadjuvant chemotherapy for locally advanced breast cancer. J Surg Oncol. 2013;108(8):531–536. doi:10.1002/jso.23439
2. Spring LM, Fell G, Arfe A, et al. Pathologic complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: a comprehensive meta-analysis. Clin Cancer Res. 2020;26(12):2838–2848. doi:10.1158/1078-0432.CCR-19-3492
3. Davey MG, Browne F, Miller N, Lowery AJ, Kerin MJ. Pathological complete response as a surrogate to improved survival in human epidermal growth factor receptor-2-positive breast cancer: systematic review and meta-analysis. BJS Open. 2022;6(3):zrac028. doi:10.1093/bjsopen/zrac028
4. Davey MG, Kerin E, O’Flaherty C, et al. Clinicopathological response to neoadjuvant therapies and pathological complete response as a biomarker of survival in human epidermal growth factor receptor-2 enriched breast cancer - a retrospective cohort study. Breast. 2021;59:67–75. doi:10.1016/j.breast.2021.06.005
5. Asselain B, Barlow W, Bartlett J. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018;19(1):27–39. doi:10.1016/S1470-2045(17)30777-5
6. Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg. 2011;128(1):305–310. doi:10.1097/PRS.0b013e318219c171
7. Greenland S, Senn SJ, Rothman KJ, et al. Statistical tests, P values, confidence intervals, and power: a guide to misinterpretations. Eur J Epidemiol. 2016;31(4):337–350. doi:10.1007/s10654-016-0149-3
8. Amrhein V, Greenland S, McShane B. Scientists rise up against statistical significance. Nature. 2019;567(7748):305–307. doi:10.1038/d41586-019-00857-9
9. Solla F, Tran A, Bertoncelli D, Musoff C, Bertoncelli CM. Why a P-value is not enough. Clin Spine Surg. 2018;31(9):385–388. doi:10.1097/BSD.0000000000000695
10. Walsh M, Srinathan SK, McAuley DF, et al. The statistical significance of randomized controlled trial results is frequently fragile: a case for a fragility index. J Clin Epidemiol. 2014;67(6):622–628. doi:10.1016/j.jclinepi.2013.10.019
11. Tignanelli CJ, Napolitano LM. The fragility index in randomized clinical trials as a means of optimizing patient care. JAMA Surg. 2019;154(1):74–79. doi:10.1001/jamasurg.2018.4318
12. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535
13. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–2012. doi:10.1001/jama.283.15.2008
14. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
15. Kim HY. Statistical notes for clinical researchers: chi-squared test and Fisher’s exact test. Restor Dent Endod. 2017;42(2):152–155. doi:10.5395/rde.2017.42.2.152
16. Taucher S, Steger GG, Jakesz R, et al. The potential risk of neoadjuvant chemotherapy in breast cancer patients—results from a prospective randomized trial of the Austrian Breast and Colorectal Cancer Study Group (ABCSG-07). Breast Cancer Res Treat. 2008;112(2):309–316. doi:10.1007/s10549-007-9844-9
17. Wolmark N, Wang J, Mamounas E, Bryant J, Fisher B. Preoperative chemotherapy in patients with operable breast cancer: nine-year results from national surgical adjuvant breast and bowel project B-18. JNCI Monographs. 2001;2001(30):96–102. doi:10.1093/oxfordjournals.jncimonographs.a003469
18. van der Hage JA, van de Velde CJ, Julien JP, Tubiana-Hulin M, Vandervelden C, Duchateau L. Preoperative chemotherapy in primary operable breast cancer: results from the European Organization for Research and Treatment of Cancer trial 10902. J Clin Oncol. 2001;19(22):4224–4237. doi:10.1200/JCO.2001.19.22.4224
19. Powles TJ, Hickish TF, Makris A, et al. Randomized trial of chemoendocrine therapy started before or after surgery for treatment of primary breast cancer. J Clin Oncol. 1995;13(3):547–552. doi:10.1200/JCO.1995.13.3.547
20. Gazet JC, Ford HT, Gray R, et al. Estrogen-receptor-directed neoadjuvant therapy for breast cancer: results of a randomised trial using formestane and methotrexate, mitozantrone and mitomycin C (MMM) chemotherapy. Ann Oncol. 2001;12(5):685–691. doi:10.1023/A:1011115107615
21. Gianni L, Baselga J, Eiermann W, et al. Phase III trial evaluating the addition of paclitaxel to doxorubicin followed by cyclophosphamide, methotrexate, and fluorouracil, as adjuvant or primary systemic therapy: European cooperative trial in operable breast cancer. J Clin Oncol. 2009;27(15):2474–2481. doi:10.1200/JCO.2008.19.2567
22. Mauriac L, MacGrogan G, Avril A, et al. Neoadjuvant chemotherapy for operable breast carcinoma larger than 3 cm: a unicentre randomized trial with a 124-month median follow-up. Institut Bergonié Bordeaux Groupe Sein (IBBGS). Ann Oncol. 1999;10(1):47–52. doi:10.1023/A:1008337009350
23. Scholl SM, Asselain B, Palangie T, et al. Neoadjuvant chemotherapy in operable breast cancer. Eur J Cancer. 1991;27(12):1668–1671. doi:10.1016/0277-5379(91)90442-G
24. Danforth DN
25. Ragaz JBR, Rebbeck P. Preoperative (neoadjuvant) versus postoperative adjuvant chemotherapy for stage I–II breast cancer. Long-term analysis of British Columbia randomized trial. Proc Am Soc Clin Oncol. 1997;16:142a.
26. Davey MG, Casey MC, McGuire A, et al. Evaluating the role of circulating MicroRNAs to aid therapeutic decision making for neoadjuvant chemotherapy in breast cancer - a prospective, multicenter clinical trial. Ann Surg. 2022;276(5):905–912.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test in Node-Negative Early Breast Cancer
Berdunov V, Millen S, Paramore A, Griffin J, Reynia S, Fryer N, Brown R, Longworth L
ClinicoEconomics and Outcomes Research 2022, 14:619-633
Published Date: 19 September 2022
Advice from One Patient to Another: Qualitative Analysis of Patients’ Perspectives About Chemotherapy Initiation
Malinowski C, Paredes E, Housten AJ, Chavez-MacGregor M
Patient Preference and Adherence 2022, 16:3283-3289
Published Date: 14 December 2022
Dietary Behavior and Its Association with Nutrition Literacy and Dietary Attitude Among Breast Cancer Patients Treated with Chemotherapy: A Multicenter Survey of Hospitals in China
Tang H, Wang R, Yan P, Zhang W, Yang F, Guo S, Li T, Yi L, Bai X, Lin S, Zhang Y, Shang L
Patient Preference and Adherence 2023, 17:1407-1419
Published Date: 9 June 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test from a US Societal Perspective
Berdunov V, Cuyun Carter G, Laws E, Luo R, Russell CA, Campbell S, Abdou Y, Force J
ClinicoEconomics and Outcomes Research 2024, 16:471-482
Published Date: 4 June 2024