Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 18
Diagnostic Performance of the Multi-Biomarker Disease Activity (MBDA) Score for Rheumatoid Arthritis in Patients with New-Onset Joint Symptoms: An Age-Stratified Retrospective Study
Authors Hiura K ![]() , Ito M, Shimizu Y, Takeda T, Iwaki-Egawa S
, Ito M, Shimizu Y, Takeda T, Iwaki-Egawa S
Received 27 October 2025
Accepted for publication 2 February 2026
Published 16 February 2026 Volume 2026:18 576941
DOI https://doi.org/10.2147/OARRR.S576941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Kazuya Hiura,1 Moeko Ito,1 Yuka Shimizu,2 Tsuyoshi Takeda,3 Sachiko Iwaki-Egawa1
1Faculty of Pharmaceutical Sciences, Hokkaido University of Science, Sapporo, Japan; 2Department of Gastroenterology, Obihiro Kosei General Hospital, Obihiro, Japan; 3Department of Internal Medicine, Hokkaido Spinal Cord Injury Center, Bibai, Japan
Correspondence: Kazuya Hiura, Faculty of Pharmaceutical Sciences, Hokkaido University of Science, 7-15-4-1 Maeda, Teine, Sapporo, Hokkaido, 006-8590, Japan, Tel +81 11 676 8574, Fax +81 11 676 8666, Email [email protected]
Purpose: Anti-citrullinated protein antibodies (ACPA) positivity decreases in elderly-onset rheumatoid arthritis (EORA), likely due to immunosenescence and clinical heterogeneity. This study aimed to evaluate the multi-biomarker disease activity (MBDA) score as an alternative diagnostic marker for rheumatoid arthritis (RA) in patients with new-onset joint symptoms, focusing on ACPA–negative cases stratified into young-onset RA (YORA) and EORA.
Patients and Methods: This retrospective study was conducted at two institutions in Hokkaido, Japan (2018– 2022). Patients with new-onset joint symptoms who had not received prior RA therapy were included. Baseline serum samples were analyzed for MBDA and high-sensitivity C-reactive protein (hsCRP). Diagnostic performance for RA was evaluated using sensitivity, specificity, accuracy, area under the curve, and logistic regression.
Results: Among 257 patients, 90 were < 60 years (RA, n = 42) and 167 were ≥ 60 years (RA, n = 84). In YORA, ACPA was the strongest predictor (odds ratio [OR]: 170.48, P < 0.01). In ACPA-negative YORA, both MBDA (OR: 6.51, P = 0.03) and hsCRP (OR: 15.56, P = 0.02) were significant, and their combination improved accuracy to 86.9% (OR: 18.00, P < 0.01). In EORA, ACPA showed lower accuracy (70.1%), whereas MBDA was higher (74.9%). In ACPA-negative EORA, the combination of MBDA and hsCRP provided the highest predictive ability (accuracy: 72.8%; OR: 43.52, P < 0.01).
Conclusion: MBDA, particularly when combined with hsCRP, provides clinically meaningful diagnostic value for RA in patients with new-onset joint symptoms, particularly in ACPA-negative YORA and EORA.
Trial Registration: This study was retrospectively registered in the University Hospital Medical Information Network (UMIN000057829).
Keywords: Biomarkers, Early Diagnosis, Anti-Citrullinated Protein antibodies, Aged
Introduction
Rheumatoid arthritis (RA) requires early diagnosis and treatment initiation to improve prognosis.1–9 In the 2010 classification criteria established by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR),10 the anti-citrullinated protein antibodies (ACPA) play a central role. ACPA has a high specificity of 90–98%; however, its sensitivity remains limited at 70–80%.11–13 Furthermore, the ACPA positivity rate is significantly lower in elderly-onset RA (EORA) than in young-onset RA (YORA).12 This difference may be related to age-associated changes in immune function, known as immunosenescence, which is thought to contribute to the unique clinical features and treatment responses observed in EORA.13 These findings suggest that EORA and YORA have partly distinct immunological characteristics. In addition, patients with ACPA-negative RA often fail to reach the threshold score of 6 in the classification criteria,14 highlighting the need for novel biomarkers to support early diagnosis.
The multi-biomarker disease activity (MBDA) score is an objective index derived from 12 serum biomarkers.15–18 It correlates strongly with conventional disease activity measures, including the Disease Activity Score in 28 joints, the Simplified Disease Activity Index, and the Clinical Disease Activity Index, including in patients with early RA.19,20 Previous studies have also reported that the MBDA score is informative for assessing disease activity and the risk of radiographic joint damage progression irrespective of serological status, including rheumatoid factor and ACPA positivity.21 Furthermore, the MBDA score predicts treatment response, remission, and radiographic progression21–23 and serves as a prognostic indicator. Beyond disease activity assessment, MBDA integrates biomarkers reflecting multiple inflammatory pathways involved in RA pathogenesis, including cytokine signaling, matrix turnover, and acute-phase responses. This integrated profile may capture subclinical inflammatory processes preceding overt clinical progression, providing a rationale for evaluating the MBDA score as a diagnostic adjunct and a potential tool for predicting RA development when conventional serological markers are insufficient. While MBDA has been validated for assessing disease activity and predicting outcomes in established RA, its utility in the early diagnostic phase of patients presenting with new-onset joint symptoms, particularly in ACPA-negative patients and across different age groups, remains unclear.
In this study, we analyzed serum samples collected at the initial visit to evaluate the diagnostic utility of the MBDA score, focusing on ACPA-negative patients and EORA, in whom diagnosis is particularly challenging. ACPA-negative patients often fail to meet the 2010 ACR/EULAR classification criteria, and EORA frequently presents with nonspecific early clinical features. Moreover, aging may influence inflammatory biomarker profiles, making age-stratified evaluation clinically relevant. We considered that the MBDA score, either alone or in combination with other biomarkers, might improve the diagnostic accuracy for RA in patients with new-onset joint symptoms, particularly among ACPA-negative and elderly individuals. Therefore, in this study, we aimed to clarify the value of the MBDA score as a novel diagnostic adjunct to address the limitations of conventional biomarkers.
Materials and Methods
Study Design and Setting
This retrospective diagnostic cohort study was conducted at two institutions in Hokkaido, Japan: the Hokkaido Spinal Cord Injury Center and Obihiro Kosei General Hospital, between September 2018 and December 2022. These two centers were selected because they provide regional rheumatology care in Hokkaido and have systems in place for storing serum samples collected at the initial visit and for the systematic accumulation of clinical data available for research use.
Target Patients
Eligible patients presented with new-onset joint symptoms (pain and/or swelling) within 6 months of symptom onset and had not received disease-modifying antirheumatic drugs or glucocorticoids at the initial visit. Symptom onset was defined as the time of joint pain and/or swelling as reported by the patient. Exclusion criteria included cases with missing essential baseline clinical data (eg, joint findings or laboratory results) or the absence of stored serum samples required for biomarker analysis. Patients aged <60 years were classified as having YORA, whereas those aged ≥60 years were classified as having EORA.24 The age cutoff of 60 years for defining EORA was selected because it is widely used in the literature and is considered to reflect the onset of immunosenescence, allowing consistency with prior studies. Rheumatologists diagnosed RA based on the 2010 ACR/EULAR classification criteria.10 Final diagnoses were established at the initial visit or during the follow-up period and confirmed within 1 year.
Patient Background
The following characteristics were recorded at the initial visit: sex, age, ACPA, rheumatoid factor (RF), MBDA score, and C-reactive protein (CRP). ACPA, RF, and CRP were measured for clinical purposes, with positivity defined according to institutional reference values (ACPA ≥4.5 IU/mL; RF ≥20 IU/mL), consistent with previously reported thresholds.25,26 The MBDA score was calculated using CRP values obtained from standard clinical assays (conventional CRP) in accordance with the original algorithm.15–18 In contrast, high-sensitivity CRP (hsCRP) measured by enzyme-linked immunosorbent assay (ELISA) was used only in the exploratory analysis of biomarker combinations. The methods used to assess MBDA scores and hsCRP levels are described in the following section.
The MBDA Score and hsCRP
Serum samples were collected at the initial visit and stored at −80 °C until analysis. Serum levels of the biomarkers listed below were measured using ELISA kits: chitinase-3-like protein 1 (YKL-40), epidermal growth factor (EGF), leptin, tumor necrosis factor receptor 1 (TNF-R1), soluble vascular cell adhesion molecule-1 (sVCAM-1), and vascular endothelial growth factor A (VEGF-A) were measured using Quantikine ELISA kits (R&D Systems, Minneapolis, MN, USA); interleukin-6 (IL-6) and resistin were measured using Human IL-6 and Human Resistin ELISA kits (BioVendor, Brno, Czech Republic); serum amyloid A (SAA) was assessed using a Human SAA ELISA kit (MyBioSource, San Diego, CA, USA); and matrix metalloproteinase (MMP)-1 and MMP-3 were measured using a Human MMP-1 ELISA kit (Sigma-Aldrich, St. Louis, MO, USA) and the Panaclear MMP-3 ELISA kit (Daiichi Pure Chemicals Co., Ltd., Tokyo, Japan), respectively. hsCRP levels were measured using the CircuLex High-sensitivity CRP ELISA kit (CycLex Co., Ltd., Nagano, Japan). All assays were performed centrally at the Faculty of Pharmaceutical Sciences, Hokkaido University of Science, under standardized laboratory conditions. The cutoff for MBDA positivity was defined as >25, in accordance with previously established criteria (≤25 is considered remission).19 For MMP-3, sex-specific thresholds were applied: >121.0 ng/mL for men and >59.7 ng/mL for women, according to the reference intervals provided by the Panaclear MMP-3 ELISA kit (Daiichi Pure Chemicals Co., Ltd., Tokyo, Japan). hsCRP positivity was defined as >1 μg/mL.19 These thresholds, including those for ACPA and RF, were used to classify patients as biomarker-positive or -negative in diagnostic analyses.
Ethical Considerations
This study was conducted in accordance with the ethical standards of the institutional research committees and the principles of the 1964 Declaration of Helsinki, as revised in later amendments, or with comparable ethical standards. Approval was obtained from the ethics committees of the Hokkaido Spinal Cord Injury Center (approval No. 41, August 30, 2018) and Obihiro Kosei Hospital (approval Nos. 037, September 19, 2018, and 054, August 12, 2020). Written informed consent was obtained from all participants before enrollment.
Study Size
No formal sample size calculation was performed before study initiation. Because analyses were conducted separately for YORA and EORA, post hoc power analyses were performed for each subgroup. In YORA, the study had nearly 100% power (>99.9%) to detect the observed difference in RA progression between MBDA-positive (28/35, 80.0%) and MBDA-negative patients (14/55, 25.5%) at a two-sided α of 0.05. In EORA, the corresponding power was also nearly 100% (>99.9%) for MBDA-positive (78/121, 64.5%) versus MBDA-negative patients (6/46, 13.0%). In addition, post hoc power analyses based on receiver operating characteristic (ROC) curve performance were conducted. The observed area under the curve (AUC) values were 0.79 (95% confidence interval [CI]: 0.69–0.88) in YORA and 0.73 (95% CI: 0.64–0.82) in EORA, each providing approximately 99% power to detect a significant difference from the null value of 0.5 at a two-sided α of 0.05.
Statistical Analysis
Statistical analyses were conducted using JMP Pro 18 software (SAS Institute Inc., Cary, NC, USA). No imputation was applied for missing data; analyses were based on available cases. The Mann–Whitney U-test was used for comparisons between two independent groups, and Fisher’s exact test was applied for categorical variables. Statistical significance was defined at P < 0.05. Sensitivity and specificity were calculated from ROC curve analysis, and the AUC was determined. Logistic regression analyses were performed with progression to RA as the dependent variable. Each biomarker was dichotomized according to predefined cutoff values and entered as an independent variable to estimate the odds ratio (OR), 95% CI, and P values. No multivariable adjustment for potential confounders was performed. This was because key covariates required for adjustment were not consistently available across patients. In addition to evaluating biomarkers individually, we also assessed selected combinations (eg, MBDA with hsCRP, RF, or MMP-3) based on previous reports27 and exploratory considerations to determine whether combined use could enhance diagnostic performance.
Results
Yora
Analysis of Confirmed Diagnoses
We initially enrolled 109 patients aged <60 years (Figure 1). Nineteen patients were excluded due to insufficient medical records or the absence of stored blood samples for biomarker measurement, leaving 90 patients for the final analysis. Malignant tumors were not specified as an exclusion criterion; however, no such cases were included in the analyzed cohort. Based on ACPA results at the initial visit, 29 patients (32.2%) were classified as ACPA-positive and 61 (67.8%) as ACPA-negative. A total of 42 patients were diagnosed with RA and categorized into the YORA group. Of these, 30 patients were diagnosed with RA at the initial visit, while the remaining 12 patients received a diagnosis during the follow-up period, with all final diagnoses determined within 1 year after the initial visit. Among the remaining 48 non-RA patients, diagnoses included osteoarthritis (OA; n = 6), fibromyalgia (FM; n = 2), Sjögren’s syndrome (SS; n = 2), other collagen-related diseases (n = 5), other conditions (n = 28), and patients under observation (n = 5).
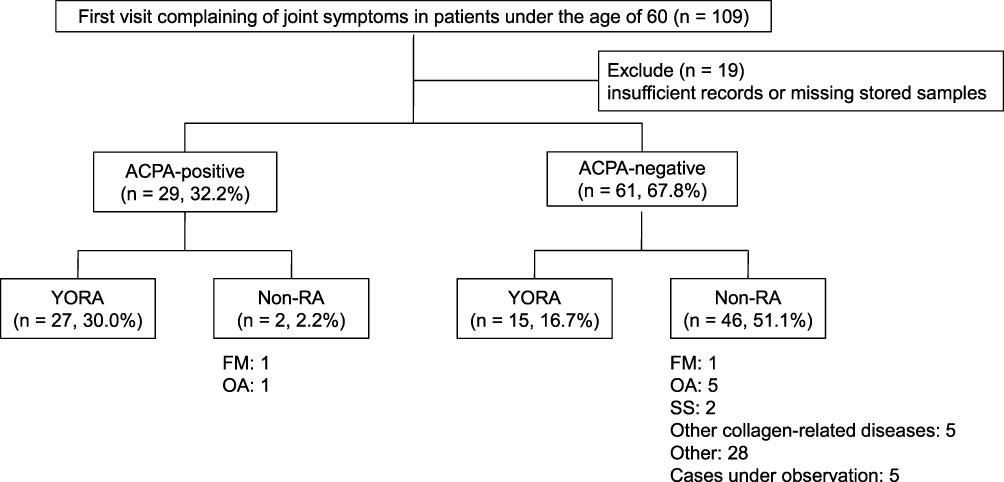 |
Figure 1 Study flow of patients aged <60 years. Abbreviations: YORA, young-onset rheumatoid arthritis; OA, osteoarthritis; FM, fibromyalgia; SS, Sjögren’s syndrome; ACPA, anti-citrullinated protein antibodies; RA, rheumatoid arthritis. Notes: Patients were classified as ACPA-positive or ACPA-negative at the initial visit. Final diagnoses were established during 1-year follow-up and categorized as YORA or non-RA. |
Baseline characteristics and serum biomarker profiles of the YORA group (n = 42) and the non-RA group (n = 48) are summarized in Table 1. Patients in the YORA group were older (P < 0.01), had a higher ACPA positivity rate (P < 0.01), and had significantly higher MBDA scores (P < 0.01) compared with the non-RA group. Among the 12 serum biomarkers comprising the MBDA score, IL-6, TNF-R1, and CRP levels were significantly higher in the YORA group (all P < 0.01).
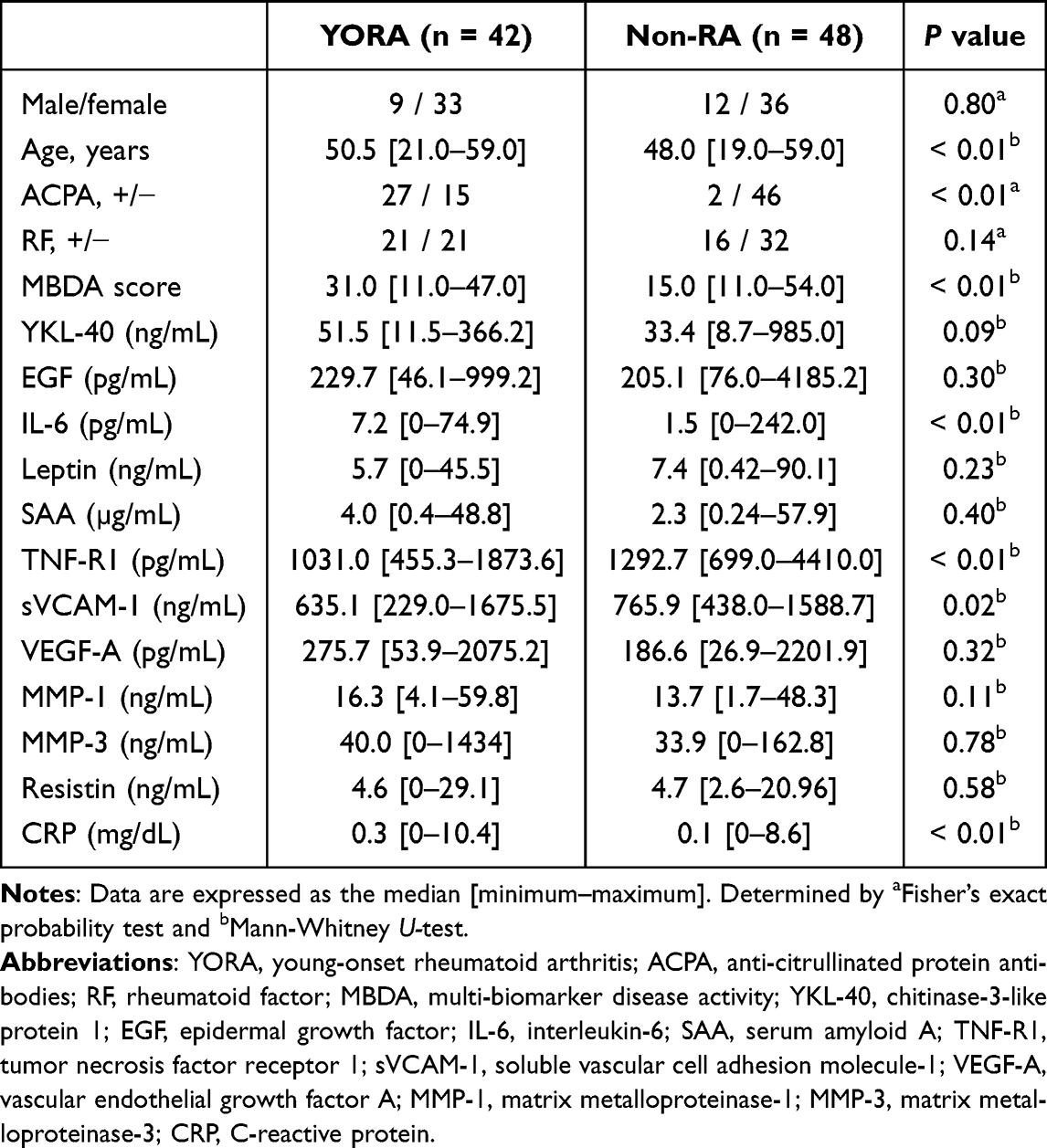 |
Table 1 Baseline Characteristics and Diagnostic Outcomes of Patients Aged <60 years Presenting with New-Onset Joint Symptoms (YORA and Non-RA) |
Table 2 summarizes the diagnostic performance of each serological biomarker for diagnosing RA in the YORA cohort, including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy, and AUC. Of the 90 patients analyzed, 42 were diagnosed with RA. ACPA demonstrated the best diagnostic performance, with a sensitivity of 64.3%, specificity of 95.8%, PPV of 93.1%, NPV of 75.4%, accuracy of 81.1%, and AUC of 0.80. The MBDA score also showed relatively strong diagnostic performance (accuracy: 76.7%; AUC: 0.76), although inferior to ACPA. Among the other biomarkers, hsCRP exhibited the highest sensitivity (76.2%) but relatively low specificity (62.5%). Both RF and MMP-3 showed low sensitivities (50.0% and 28.6%, respectively) and lower accuracies (58.9% each) compared with ACPA and MBDA. Logistic regression analysis, using RA progression as the dependent variable and the five biomarkers as independent variables, revealed that both ACPA (OR: 170.48; 95% CI: 22.19–2730.91; P < 0.01) and MBDA (OR: 8.61; 95% CI: 1.88–47.84; P < 0.01) were significantly associated with RA progression. No significant associations were observed for RF, hsCRP, or MMP-3.
 |
Table 2 Diagnostic Performance of Serological Biomarkers in Patients with YORA (n = 90, YORA = 42) |
Diagnostic Prediction of YORA in ACPA-Negative Cases
We previously analyzed ACPA-negative patients and reported that individual biomarkers had limited predictive value, whereas the combination of MMP-3 and hsCRP was particularly useful.27 However, that analysis did not include age-stratified evaluation. Therefore, in this study, we conducted age-stratified analyses to further investigate the utility of baseline serum biomarkers for predicting progression to RA.
In total, 61 ACPA-negative patients were included, of whom 15 progressed to RA and were classified as YORA. In the analysis of individual biomarkers, MBDA (OR: 6.51, P = 0.03) and hsCRP (OR: 15.56, P = 0.02) were identified as significant predictors of RA progression, whereas RF and MMP-3 showed no significant associations (Table 3A).
 |
Table 3 Diagnostic Performance of Serological Biomarkers in ACPA-Negative Patients with YORA (n = 61, YORA = 15) |
When evaluating biomarker combinations, MMP-3 with hsCRP demonstrated reproducible diagnostic performance, with a sensitivity of 40.0%, specificity of 97.8%, and accuracy of 83.6%, consistent with our previous findings. However, no statistically significant association was observed. In contrast, the newly evaluated combination of MBDA and hsCRP showed superior diagnostic performance, with a sensitivity of 73.3%, specificity of 91.3%, accuracy of 86.9%, and AUC of 0.82, and was identified as a significant predictor (OR: 18.00; 95% CI: 2.22–190.43, P < 0.01) (Table 3B). Notably, 11 of the 15 patients with YORA who progressed to RA (73.3%) were positive for both MBDA and hsCRP, compared with only four of the 46 non-progressors (8.7%).
Eora
Analysis of Confirmed Diagnoses
A total of 184 patients aged ≥60 years were initially enrolled. Of these, 17 were excluded due to incomplete medical records or unavailable stored serum samples for biomarker analysis. Consequently, 167 patients were included in the final analysis (Figure 2). Similar to the YORA cohort, no cases with malignant tumors were ultimately included, although this was not a predefined exclusion criterion. Among the eligible patients, 84 patients were diagnosed with RA and categorized into the EORA group. Of these, 48 patients were diagnosed with RA at the initial visit, while the remaining 36 patients received a diagnosis during the follow-up period, with all final diagnoses determined within 1 year after the initial visit. The remaining 83 were diagnosed with non-RA conditions, including polymyalgia rheumatica (PMR; n = 23), OA (n = 24), remitting seronegative symmetrical synovitis with pitting edema (RS3PE; n = 9), FM (n = 2), SS (n = 3), other collagen-related diseases (n = 8), other conditions (n = 13), and one case under observation (n = 1). The baseline characteristics and serum biomarker profiles of the EORA (n = 84) and non-RA (n = 83) groups are presented in Table 4. Compared with the non-RA group, patients in the EORA group had significantly higher positivity rates for ACPA and RF (both P < 0.01) and significantly higher MBDA scores (P < 0.01). Among MBDA score components, YKL-40 and CRP levels were significantly elevated in the EORA group (both P < 0.01).
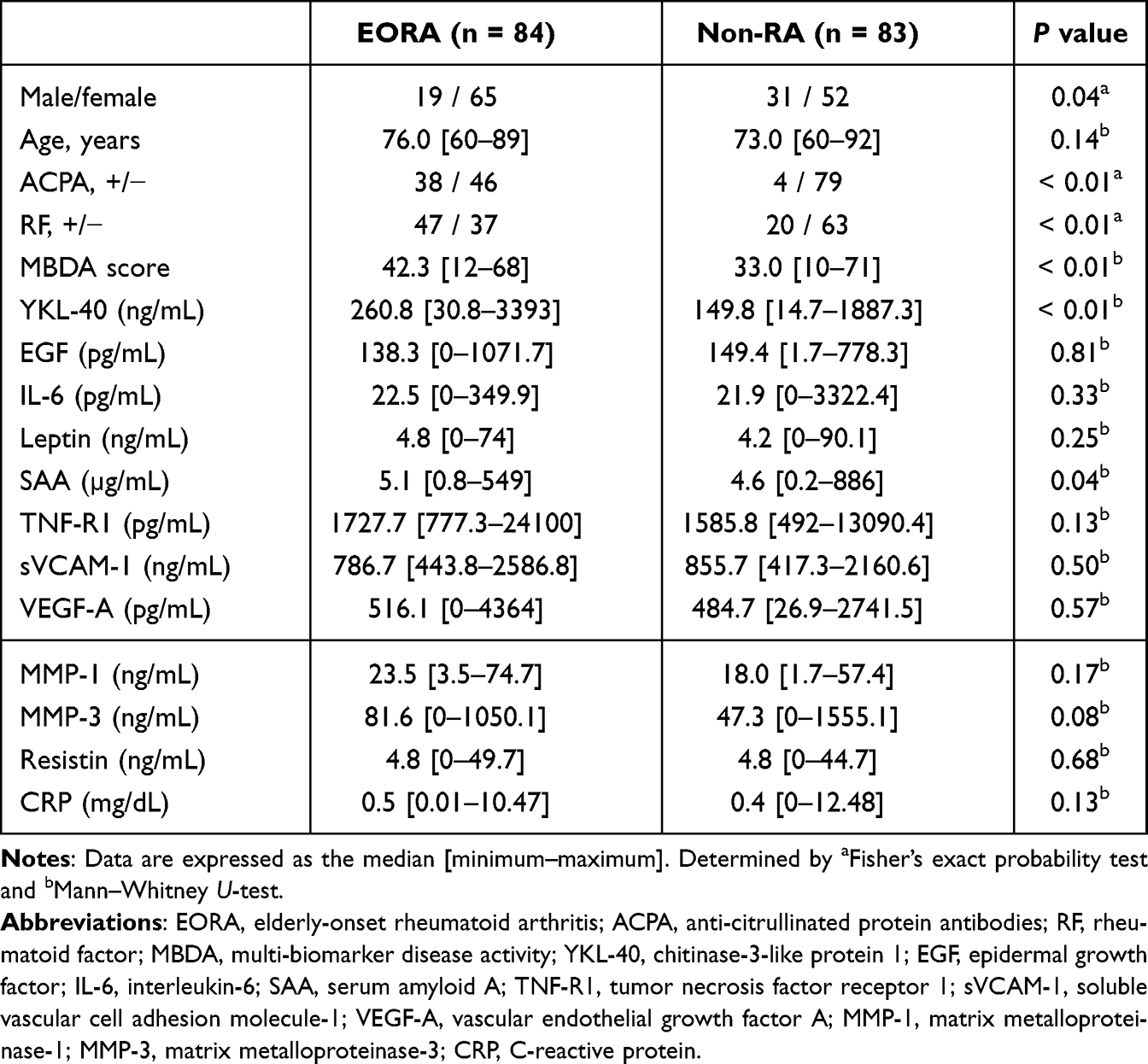 |
Table 4 Baseline Characteristics and Diagnostic Outcomes of Patients Aged ≥60 years Presenting with New-Onset Joint Symptoms (EORA and Non-RA) |
 |
Figure 2 Study flow of patients aged ≥60 years. Abbreviations: EORA, elderly-onset rheumatoid arthritis; PMR, polymyalgia rheumatica; OA, osteoarthritis; FM, fibromyalgia; RS3PE, remitting seronegative symmetrical synovitis with pitting edema; SS, Sjögren’s syndrome; ACPA, anti-citrullinated protein antibodies; RA, rheumatoid arthritis. Notes: Patients were classified as ACPA-positive or ACPA-negative at the initial visit. Final diagnoses were established during 1-year follow-up and categorized as EORA or non-RA. |
Table 5 summarizes the diagnostic performance of each serological biomarker for identifying EORA, including sensitivity, specificity, PPV, NPV, accuracy, and AUC. Among the 167 patients analyzed, 84 were diagnosed with RA. ACPA demonstrated high specificity (95.2%) but low sensitivity (45.2%), yielding an accuracy of 70.1% and an AUC of 0.70. In contrast, the MBDA score showed the highest sensitivity (92.9%) but lower specificity (56.6%), resulting in an accuracy of 74.9% and an AUC of 0.75, thereby outperforming the other biomarkers. Logistic regression analysis was performed with RA progression as the dependent variable and biomarkers as independent variables. Both ACPA (OR: 66.03; 95% CI: 10.24–1385.48, P < 0.01) and MBDA (OR: 83.59; 95% CI: 14.39–1672.69, P < 0.01) were significantly associated with RA progression, whereas RF, hsCRP, and MMP-3 were not.
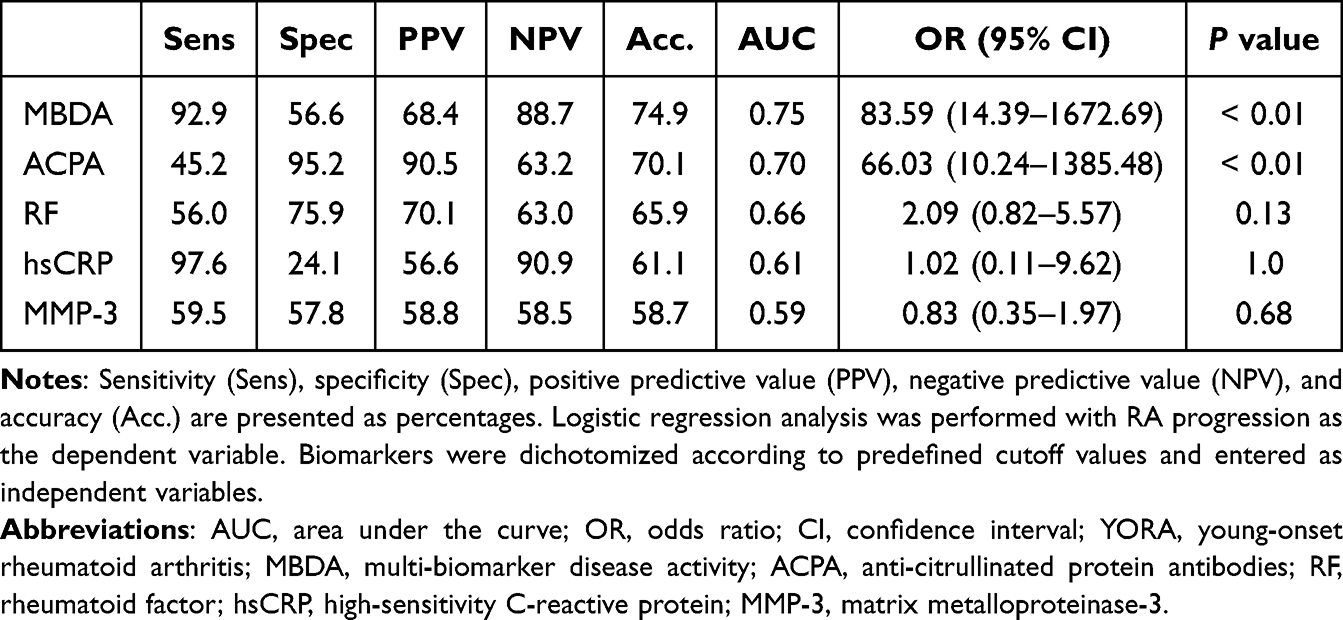 |
Table 5 Diagnostic Performance of Serological Biomarkers in Patients with EORA (n = 167, EORA = 84) |
Diagnostic Prediction of EORA in ACPA-Negative Cases
In this study, 125 ACPA-negative patients were classified into the EORA group, of whom 46 progressed to RA.
In the analysis of individual biomarkers, MBDA demonstrated the highest sensitivity (97.8%) but relatively low specificity (54.4%), yielding an accuracy of 70.4% and an AUC of 0.76. Logistic regression analysis identified MBDA as a significant predictor of RA progression (OR: 46.24; 95% CI: 8.19–398.55, P = 0.0005). RF also showed a significant but weaker association (OR: 3.34; 95% CI: 1.20–10.42, P = 0.03), whereas hsCRP and MMP-3 were not significantly associated (Table 6A).
 |
Table 6 Diagnostic Performance of Serological Biomarkers in ACPA-Negative Patients with EORA (n = 125, EORA = 46) |
When evaluating biomarker combinations, the combination of MBDA and hsCRP demonstrated the best diagnostic performance, with a sensitivity of 95.7%, specificity of 59.5%, accuracy of 72.8%, and an AUC of 0.78. It was also identified as a strong predictor of RA progression (OR: 43.52; 95% CI: 8.09–439.10, P < 0.01). The combination of MMP-3 and hsCRP showed a statistically significant association (OR: 9.23; 95% CI: 1.64–80.74, P = 0.02); however, its diagnostic performance (sensitivity: 78.3%, specificity: 62.0%, accuracy: 68.0%) was inferior to that of MBDA and hsCRP (Table 6B). Among the 46 ACPA-negative patients with EORA who progressed to RA, 44 (95.7%) were positive for both MBDA and hsCRP, compared with 32 of the 79 non-progressors (40.5%).
Discussion
In this study, we evaluated the utility of the MBDA score using serum samples collected at the initial visit from patients with new-onset joint symptoms. Our findings clearly demonstrate that the MBDA score serves as a useful early diagnostic indicator of progression to both YORA and EORA. Notably, in ACPA-negative cases, the combination of the MBDA score and hsCRP improved diagnostic accuracy, suggesting a complementary role beyond conventional biomarkers. These results are consistent with our study objective of evaluating the adjunctive diagnostic role of the MBDA score.
Diagnostic Utility of the MBDA Score in YORA
ACPA remains a standard and reliable marker for the diagnosis of RA due to its consistently high diagnostic performance. In this study, ACPA in the YORA group demonstrated strong diagnostic performance, consistent with previous reports (including those that did not distinguish between YORA and EORA).11,28–30 Boeters et al reported that the ACPA positivity rate in patients with RA declines with age, decreasing by approximately 4% annually after age 50,12 which may influence a subset of older patients with YORA. Nevertheless, ACPA in our cohort maintained high specificity with moderate sensitivity, and logistic regression analysis confirmed it as a significant predictor (OR: 170.48, P < 0.01). In contrast, the MBDA score showed a sensitivity of 66.7%, specificity of 85.4%, and an AUC of 0.76, which is slightly inferior to ACPA; however, it outperformed other biomarkers such as RF, CRP, and MMP-3 in terms of diagnostic performance.
ACPA-negative RA, the focus of this analysis, often present with a higher number of swollen joints and elevated CRP levels at baseline compared with ACPA-positive RA, suggesting greater disease activity at onset.31–33 However, due to the absence of serological markers, these patients may have difficulty meeting the ACR/EULAR classification criteria at the initial visit, as their scoring is limited in the serology domain. We previously reported that the combination of hsCRP and MMP-3 was useful as a diagnostic adjunct for RA in ACPA-negative patients presenting with new-onset joint symptoms, although that study did not stratify patients by age (ie, YORA vs EORA).27 In this age-stratified analysis of ACPA-negative YORA, both MBDA and hsCRP emerged as significant predictors. When combined, they demonstrated the highest diagnostic performance (accuracy: 86.9%; OR: 18.00, P < 0.01). The MBDA score, which integrates 12 inflammation-related biomarkers into a single composite index, provides a more comprehensive and multidimensional assessment of inflammatory activity than any single marker alone. This broader scope may help overcome diagnostic delays and facilitate earlier intervention in ACPA-negative cases. Taken together, our findings suggest that the MBDA score could be clinically useful in YORA, particularly as a supplementary marker in combination with hsCRP, although systematic validation of these exploratory findings is warranted.
Diagnostic Utility of the MBDA Score in EORA
Consistent with previous studies, both the sensitivity and AUC of ACPA in the EORA group were lower than those in the YORA group, reflecting reduced diagnostic performance with advancing age. In contrast, the MBDA score demonstrated superior diagnostic performance in EORA, with a sensitivity of 92.9%, specificity of 56.6%, accuracy of 74.9%, and AUC of 0.75, thereby outperforming ACPA. Furthermore, among ACPA-negative patients with EORA, the combination of MBDA and hsCRP achieved the highest diagnostic performance, with an AUC of 0.78 and a significant association with RA progression (OR 43.52, P < 0.01).
EORA often presents with clinical features distinct from those of YORA. Its onset is frequently acute and accompanied by systemic symptoms such as fever, fatigue, and weight loss. Joint involvement typically favors large joints, particularly the shoulders, and inflammatory markers such as CRP and erythrocyte sedimentation rate are often significantly elevated.34–39 Moreover, patients with EORA commonly present with PMR-like symptoms or features mimicking infection and frequently have age-related comorbidities, including interstitial lung disease and diabetes. These factors can contribute to diagnostic uncertainty and delay treatment initiation.35,40 The findings of this study suggest that the MBDA score may serve as a valuable adjunct for diagnosing RA in patients with EORA, particularly in ACPA-negative cases, thereby facilitating earlier recognition and therapeutic intervention. However, a notable proportion of non-RA patients in the EORA group also exhibited elevated MBDA scores, raising concern for false-positive results (PPV: 68.4%). Previous studies have reported that common comorbid conditions, such as FM, OA, osteoporotic fractures, diabetes mellitus, asthma, and hypertension, do not substantially influence MBDA scores.17,41 Nevertheless, in the present study, false-positive results were more frequently observed in EORA than in YORA (PPV: 80.0%), suggesting that age-related factors specific to older patients may be involved. However, studies evaluating MBDA scores in non-RA diseases or conditions remain limited, making it difficult to fully assess these influences at present. Accordingly, the MBDA score should be interpreted as a supplementary marker, ideally in combination with hsCRP, and further systematic validation of these exploratory findings is warranted.
Clinical Significance of the MBDA Score and Study Limitations
The MBDA score integrates multiple inflammation-related biomarkers, providing a multidimensional assessment of inflammatory status. Previous studies have demonstrated its utility in predicting radiographic progression and treatment response.21–23 Importantly, our findings extend this evidence by demonstrating that the MBDA score has clinically meaningful diagnostic utility as an adjunctive tool during the initial evaluation of patients with new-onset joint symptoms, applicable to both YORA and EORA.
However, this study has some limitations. First, the MBDA score is influenced by factors such as age, sex, and obesity. In particular, elevated scores have been reported in patients with obesity, which may lead to an overestimation of disease activity.42,43 In this study, body mass index and other body size data were missing in many cases and could not be adequately assessed. Therefore, in obese patients presenting with new-onset joint symptoms, elevated MBDA scores may have contributed to an overestimation of RA at the diagnostic stage. Second, this was a retrospective observational study, and potential confounders such as medication history, comorbidities, duration of symptoms, and family history could not be fully accounted for. The absence of prior RA treatment was confirmed; however, the potential influence of medications for comorbid conditions, including nonsteroidal anti-inflammatory drugs, could not be adequately evaluated. Third, as this study was conducted at two institutions in Japan, the generalizability of the findings to populations with different ethnic backgrounds or healthcare delivery systems may be limited, and the results should be interpreted with caution when applied to other clinical settings. Despite these limitations, our study has significant strengths, including the use of baseline serum from patients at the initial visit and age-stratified analysis, which enabled a direct comparison between YORA and EORA. This approach clarified age-related differences in the diagnostic utility of biomarkers. Future large, multicenter prospective studies with more detailed adjustment for medication history and comorbidities are warranted to validate these findings and establish reliable diagnostic algorithms. Accordingly, the combined use of biomarkers in this study should be interpreted as exploratory and hypothesis-generating, given the retrospective design and the lack of adjustment for potential confounders.
Conclusion
This study demonstrates that the MBDA score has diagnostic utility at the stage of new-onset joint symptoms, supporting its additional clinical relevance beyond its previously reported roles in assessing disease activity and predicting prognosis. Diagnostic utility was observed across age groups, with particular value in EORA as a complementary marker to ACPA. These findings extend the diagnostic significance of the MBDA score to the early diagnostic phase and provide new insights through age-stratified analyses of YORA and EORA. By addressing the diagnostic challenges of ACPA-negative and elderly-onset RA highlighted in the Introduction, our findings support the MBDA score as a clinically meaningful diagnostic adjunct at the initial evaluation of patients presenting with new-onset joint symptoms.
Abbreviations
Acc, accuracy; ACPA, anti-citrullinated protein antibodies; ACR, American College of Rheumatology; AUC, area under the curve; CI, confidence interval; CRP, C-reactive protein; DMARDs, disease-modifying antirheumatic drugs; EORA, elderly-onset rheumatoid arthritis; EGF, epidermal growth factor; ELISA, enzyme-linked immunosorbent assay; EULAR, European League Against Rheumatism; FM, fibromyalgia; hsCRP, high-sensitivity C-reactive protein; IL-6, interleukin-6; MBDA, multi-biomarker disease activity; MMP, matrix metalloproteinase; NPV, negative predictive value; OA, osteoarthritis; OR, odds ratio; PMR, polymyalgia rheumatica; PPV, positive predictive value; RA, rheumatoid arthritis; RF, rheumatoid factor; ROC, receiver operating characteristic; RS3PE, remitting seronegative symmetrical synovitis with pitting edema; SAA, serum amyloid A; Sens, sensitivity; Spec, specificity; SS, Sjögren’s syndrome; sVCAM-1, soluble vascular cell adhesion molecule-1; TNF-R1, tumor necrosis factor receptor 1; VEGF-A, vascular endothelial growth factor A; YKL-40, chitinase-3-like protein 1; YORA, young-onset rheumatoid arthritis.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient privacy and ethical restrictions, but are available from the corresponding author on reasonable request and with permission of the institutional ethics committees that approved the study.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical standards of the institutional research committees and the principles of the 1964 Declaration of Helsinki, as revised in later amendments, or with comparable ethical standards. Approval was obtained from the ethics committees of the Hokkaido Spinal Cord Injury Center (approval No. 41, August 30, 2018) and Obihiro Kosei Hospital (approval Nos. 037, September 19, 2018, and 054, August 12, 2020). Written informed consent was obtained from all participants before enrollment.
Acknowledgments
We would like to thank Editage (www.editage.jp) for its English language editing services. Artificial intelligence (AI) tools (ChatGPT, OpenAI, San Francisco, CA, USA) were also used to assist in improving the clarity and language of the manuscript. All AI-assisted content was carefully reviewed, verified, and revised by the authors, who take full responsibility for the integrity and accuracy of the final manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have received no specific funding for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fuchs HA, Kaye JJ, Callahan LF, Nance EP, Pincus T. Evidence of significant radiographic damage in rheumatoid arthritis within the first 2 years of disease. J Rheumatol. 1989;16(5):585–13.
2. Möttönen TT. Prediction of erosiveness and rate of development of new erosions in early rheumatoid arthritis. Ann Rheum Dis. 1988;47(8):648–653. doi:10.1136/ard.47.8.648
3. van der Heijde DM, Van leeuwen MA, van Riel PL, et al. Biannual radiographic assessments of hands and feet in a three-year prospective followup of patients with early rheumatoid arthritis. Arthritis Rheum. 1992;35(1):26–34. doi:10.1002/art.1780350105
4. Plant MJ, Saklatvala J, Borg AA, Jones PW, Dawes PT. Measurement and prediction of radiological progression in early rheumatoid arthritis. J Rheumatol. 1994;21(10):1808–1813.
5. Mouterde G, Lukas C, Logeart I, et al. Predictors of radiographic progression in the ESPOIR cohort: the season of first symptoms may influence the short-term outcome in early arthritis. Ann Rheum Dis. 2011;70(7):1251–1256. doi:10.1136/ard.2010.144402
6. Gremese E, Salaffi F, Bosello SL, et al. Very early rheumatoid arthritis as a predictor of remission: a multicentre real life prospective study. Ann Rheum Dis. 2013;72(6):858–862. doi:10.1136/annrheumdis-2012-201456
7. van der Heide A, Jacobs JW, Bijlsma JW, et al. The effectiveness of early treatment with “second-line” antirheumatic drugs. a randomized, controlled trial. Ann Intern Med. 1996;124(8):699–707. doi:10.7326/0003-4819-124-8-199604150-00001
8. van Dongen H, van Aken J, Lard LR, et al. Efficacy of methotrexate treatment in patients with probable rheumatoid arthritis: a double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 2007;56(5):1424–1432. doi:10.1002/art.22525
9. Bukhari MAS, Wiles NJ, Lunt M, et al. Influence of disease-modifying therapy on radiographic outcome in inflammatory polyarthritis at five years: results from a large observational inception study. Arthritis Rheum. 2003;48(1):46–53. doi:10.1002/art.10727
10. Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
11. van Gaalen FA, Linn-Rasker SP, van Venrooij WJ, et al. Autoantibodies to cyclic citrullinated peptides predict progression to rheumatoid arthritis in patients with undifferentiated arthritis: a prospective cohort study. Arthritis Rheum. 2004;50(3):709–715. doi:10.1002/art.20044
12. Boeters DM, Mangnus L, Ajeganova S, et al. The prevalence of ACPA is lower in rheumatoid arthritis patients with an older age of onset but the composition of the ACPA response appears identical. Arthritis Res Ther. 2017;19(1):115. doi:10.1186/s13075-017-1324-y
13. Hammam N, El-Hadidi T, El-Hadidi K, et al. International overview on juvenile-, adult- and elderly-onset rheumatoid arthritis: the age at disease onset as a fundamental determinant of clinical presentation. Clin Rheumatol. 2025;44(3):979–988. doi:10.1007/s10067-025-07356-5
14. Mouterde G, Rincheval N, Lukas C, et al. Outcome of patients with early arthritis without rheumatoid factor and ACPA and predictors of rheumatoid arthritis in the ESPOIR cohort. Arthritis Res Ther. 2019;21(1):140. doi:10.1186/s13075-019-1909-8
15. Curtis JR, van der Helm-van Mil AH, Knevel R, et al. Validation of a novel multibiomarker test to assess rheumatoid arthritis disease activity. Arthritis Care Res. 2012;64(12):1794–1803. doi:10.1002/acr.21767
16. Zhao X, Qureshi F, Eastman PS, et al. Pre-analytical effects of blood sampling and handling in quantitative immunoassays for rheumatoid arthritis. J Immunol Methods. 2012;378(1–2):72–80. doi:10.1016/j.jim.2012.02.007
17. Centola M, Cavet G, Shen Y, et al. Development of a multi-biomarker disease activity test for rheumatoid arthritis. PLoS One. 2013;8(4):e60635. doi:10.1371/journal.pone.0060635
18. Eastman PS, Manning WC, Qureshi F, et al. Characterization of a multiplex, 12-biomarker test for rheumatoid arthritis. J Pharm Biomed Anal. 2012;70:415–424. doi:10.1016/j.jpba.2012.06.003
19. Bakker MF, Cavet G, Jacobs JW, et al. Performance of a multi-biomarker score measuring rheumatoid arthritis disease activity in the CAMERA tight control study. Ann Rheum Dis. 2012;71(10):1692–1697. doi:10.1136/annrheumdis-2011-200963
20. van der Helm-van Mil AHM, Knevel R, Cavet G, Huizinga TWJ, Haney DJ. An evaluation of molecular and clinical remission in rheumatoid arthritis by assessing radiographic progression. Rheumatology. 2013;52(5):839–846. doi:10.1093/rheumatology/kes378
21. Curtis JR, Weinblatt ME, Shadick NA, et al. Validation of the adjusted multi-biomarker disease activity score as a prognostic test for radiographic progression in rheumatoid arthritis: a combined analysis of multiple studies. Arthritis Res Ther. 2021;23(1):1. doi:10.1186/s13075-020-02389-4
22. Boeters DM, Burgers LE, Sasso EH, Huizinga TWJ, van der Helm-van Mil AHM. ACPA-negative RA consists of subgroups: patients with high likelihood of achieving sustained DMARD-free remission can be identified by serological markers at disease presentation. Arthritis Res Ther. 2019;21(1):121. doi:10.1186/s13075-019-1902-2
23. Meznerics FA, Kemény LV, Gunther E, et al. Multibiomarker disease activity score: an objective tool for monitoring rheumatoid arthritis? A systematic review and meta-analysis. Rheumatology. 2023;62(6):2048–2059. doi:10.1093/rheumatology/keac715
24. Pavlov-Dolijanovic S, Bogojevic M, Nozica-Radulovic T, Radunovic G, Mujovic N. Elderly-onset rheumatoid arthritis: characteristics and treatment options. Medicina. 2023;59(10). doi:10.3390/medicina59101878
25. Shiozawa K, Kawasaki Y, Yamane T, et al. Anticitrullinated protein antibody, but not its titer, is a predictor of radiographic progression and disease activity in rheumatoid arthritis. J Rheumatol. 2012;39(4):694–700. doi:10.3899/jrheum.111152
26. Tsuji H, Yano K, Furu M, et al. Time-averaged disease activity fits better joint destruction in rheumatoid arthritis. Sci Rep. 2017;7(1):5856. doi:10.1038/s41598-017-05581-w
27. Hiura K, Iwaki-Egawa S, Kawashima T, et al. The diagnostic utility of matrix metalloproteinase-3 and high-sensitivity C-reactive protein for predicting rheumatoid arthritis in anti-cyclic citrullinated peptide antibody-negative patients with recent-onset undifferentiated arthritis. Rheumatol Int. 2013;33(9):2309–2314. doi:10.1007/s00296-013-2716-1
28. Dubucquoi S, Solau-Gervais E, Lefranc D, et al. Evaluation of anti-citrullinated filaggrin antibodies as hallmarks for the diagnosis of rheumatic diseases. Ann Rheum Dis. 2004;63(4):415–419. doi:10.1136/ard.2003.008623
29. Matsui T, Shimada K, Ozawa N, et al. Diagnostic utility of anti-cyclic citrullinated peptide antibodies for very early rheumatoid arthritis. J Rheumatol. 2006;33(12):2390–2397.
30. van Venrooij WJ, van Beers JJBC, Pruijn GJM. Anti-CCP antibody, a marker for the early detection of rheumatoid arthritis. Ann N Y Acad Sci. 2008;1143:268–285. doi:10.1196/annals.1443.013
31. Chevet B, Cornec D. Clinical presentation and treatment response in ACPA-negative rheumatoid arthritis. Joint Bone Spine. 2025;92(2):105823. doi:10.1016/j.jbspin.2024.105823
32. Weman L, Salo H, Kuusalo L, et al. Initial presentation of early rheumatoid arthritis. PLoS One. 2023;18(7):e0287707. doi:10.1371/journal.pone.0287707
33. Choi S, Lee KH. Clinical management of seronegative and seropositive rheumatoid arthritis: a comparative study. PLoS One. 2018;13(4):e0195550. doi:10.1371/journal.pone.0195550
34. van Schaardenburg D, Breedveld FC. Elderly-onset rheumatoid arthritis. Semin Arthritis Rheum. 1994;23(6):367–378. doi:10.1016/0049-0172(94)90087-6
35. Bajocchi G, La Corte R, Locaputo A, Govoni M, Trotta F. Elderly onset rheumatoid arthritis: clinical aspects. Clin Exp Rheumatol. 2000;18(4 Suppl 20):S49–50.
36. Kobak S, Bes C. An autumn tale: geriatric rheumatoid arthritis. Ther Adv Musculoskelet Dis. 2018;10(1):3–11. doi:10.1177/1759720X17740075
37. Targońska-Stępniak B, Grzechnik K, Kolarz K, Gągoł D, Majdan M. Systemic inflammatory parameters in patients with elderly-onset rheumatoid arthritis (EORA) and young-onset rheumatoid arthritis (YORA)-an observational study. J Clin Med. 2021;10(6):1204. doi:10.3390/jcm10061204
38. Romão VC, Humby F, Kelly S, et al. Treatment-resistant synovitis and radiographic progression are increased in elderly-onset rheumatoid arthritis patients: findings from a prospective observational longitudinal early arthritis cohort study. Semin Arthritis Rheum. 2020;50(4):735–743. doi:10.1016/j.semarthrit.2020.03.018
39. Acuña-Rocha VD, Regalado-Ceballos D, Salcedo-Soto DA, et al. Clinical characteristics of young-onset versus elderly-onset rheumatoid arthritis: a systematic review and meta-analysis. Cureus. 2024;16(11):e74148. doi:10.7759/cureus.74148
40. Ke Y, Dai X, Xu D, et al. Features and outcomes of elderly rheumatoid arthritis: does the age of onset matter? A comparative study from a single center in China. Rheumatol Ther. 2021;8(1):243–254. doi:10.1007/s40744-020-00267-8
41. Johnson TM, Register KA, Schmidt CM, et al. Correlation of the multi-biomarker disease activity score with rheumatoid arthritis disease activity measures: a systematic review and meta-analysis. Arthritis Care Res. 2019;71(11):1459–1472. doi:10.1002/acr.23785
42. Curtis JR, Greenberg JD, Harrold LR, Kremer JM, Palmer JL. Influence of obesity, age, and comorbidities on the multi-biomarker disease activity test in rheumatoid arthritis. Semin Arthritis Rheum. 2018;47(4):472–477. doi:10.1016/j.semarthrit.2017.07.010
43. Baker JF, Curtis JR, Chernoff D, et al. Evaluation of the impact of age and adiposity on a multi-biomarker disease activity score before and after adjustment. Clin Rheumatol. 2021;40(6):2419–2426. doi:10.1007/s10067-020-05508-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
From COPD to Lung Cancer: Mechanisms Linking, Diagnosis, Treatment, and Prognosis

Qi C, Sun SW, Xiong XZ
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2603-2621
Published Date: 17 October 2022
CXCL12 and CXCR4 as Potential Early Biomarkers for Luminal A and Luminal B Subtypes of Breast Cancer
Motyka J, Gacuta E, Kicman A, Kulesza M, Malinowski P, Ławicki S
Cancer Management and Research 2023, 15:573-589
Published Date: 4 July 2023
Retinopathy of Prematurity (ROP): An Overview of Biomarkers in Various Samples for Prediction, Diagnosis, and Prognosis
Huang D, Liu Z, Deng Y
Clinical Ophthalmology 2025, 19:1515-1530
Published Date: 7 May 2025
Proteomic Analysis of Cerebrospinal Fluid: Toward the Identification of Biomarkers for Early Central Nervous System Infection
Ding Y, Wang H, Li K, Zhao S, Li D
Infection and Drug Resistance 2026, 19:570645
Published Date: 2 February 2026