Back to Journals » Drug Design, Development and Therapy » Volume 19
Dexamethasone, but Not Esketamine, Reduces Rebound Pain After Interscalene Nerve Block: A Randomized Factorial Trial
Authors Yao J ![]() , Wang C, Szmuk P, Xu C
, Wang C, Szmuk P, Xu C ![]() , Pu S, Lu J
, Pu S, Lu J ![]() , Du D
, Du D
Received 21 September 2025
Accepted for publication 14 December 2025
Published 24 December 2025 Volume 2025:19 Pages 11511—11523
DOI https://doi.org/10.2147/DDDT.S569175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Jiahui Yao,1,* Chengyu Wang,2,* Peter Szmuk,3– 5 Cheng Xu,2 Shaofeng Pu,1 Jie Lu,2 Dongping Du1
1Department of Pain Management, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200233, People’s Republic of China; 2Department of Anaesthesiology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 3Department of Anesthesiology and Pain Management, University of Texas Southwestern Medical Center, Dallas, TX, USA; 4Children’s Health of Texas, Dallas, TX, USA; 5Outcomes Research Consortium, Cleveland, OH, USA
*These authors contributed equally to this work
Correspondence: Dongping Du, Department of Pain Management, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200233, People’s Republic of China, Email [email protected]
Background: Rebound pain following peripheral nerve block resolution is a distressing phenomenon that impairs recovery and commonly arises at night when treatment options are limited.
Objective: To evaluate whether intravenous esketamine and/or dexamethasone, as adjuvants to interscalene ropivacaine block, reduce rebound pain after arthroscopic shoulder surgery.
Design: A patient- and outcome assessor–blinded, randomized, controlled, 2× 2 factorial clinical trial.
Setting: A single tertiary-care academic hospital.
Patients: A total of 160 adult patients undergoing arthroscopic shoulder surgery under general anaesthesia with single-shot interscalene brachial plexus block.
Interventions: Patients were randomized to receive intravenous combinations of esketamine–placebo, placebo–dexamethasone, esketamine–dexamethasone, or placebo–placebo, in addition to ropivacaine block after induction of general anaesthesia and before surgical incision.
Main Outcome Measures: Co-primary outcomes were: (1) the increase in pain score from before to after the ISB resolved; and (2) the incidence of severe rebound pain, defined as numerical rating scale (NRS) pain score ≥ 7.
Results: All 160 patients completed the trial. Rebound pain occurred in 32% of patients, with no interaction between esketamine and dexamethasone. The pain score increased by 6.2 ± 2.5 in the placebo–placebo group versus 4.4 ± 2.5 in the esketamine–dexamethasone group (difference – 1.8; 95% CI – 2.9 to – 0.7; P = 0.002). Dexamethasone significantly reduced the pain score increase compared to placebo (– 1.7; 95% CI – 2.8 to – 0.6; P = 0.003), while esketamine alone did not. Severe rebound pain occurred in 22/80 (27%) of patients receiving esketamine versus 26/80 (32%) without (RR 0.84; 95% CI 0.50 to 1.41; P = 0.459), and in 18/80 (22%) of patients receiving dexamethasone versus 29/80 (36%) without (RR 0.62; 95% CI 0.38 to 0.89; P = 0.016).
Conclusion: Intravenous dexamethasone, but not esketamine (low dose), significantly reduced the incidence and severity of rebound pain following interscalene nerve block.
Trial Registration: Chinese Clinical Trial Registry (ChiCTR2300072416).
Keywords: esketamine, dexamethasone, peripheral nerve block, rebound pain, central sensitization, factorial trial
Introduction
Single-injection interscalene blocks (ISB) ameliorates pain following arthroscopic shoulder surgery,1,2 with single-injection blocks (ISB) typically lasting 12–18 hours. However, patients given blocks may experience more pain than those who do not after the block resolves1 —a phenomenon referred to as rebound pain.3,4
Arthroscopic shoulder surgery is typically conducted as an outpatient procedure. Consequently, rebound pain typically occurs at home,5 and often late at night when alternative analgesic options and healthcare support are limited.6 Rebound pain is under-recognized and too often misunderstood.7,8 Causes may include inadequate pre-emptive multimodal analgesia, exaggerated hyperalgesia, or personal inability to cope with pain.7,9 Ameliorating rebound pain would improve satisfaction with regional analgesia including ISB.
Local anesthetic adjuncts for ISB have been extensively explored.10,11 However, most previous studies used duration of sensory block or pain scores at fixed postoperative time points as primary outcomes and did not explicitly address rebound pain as a distinct clinical problem. Rebound pain is now thought to reflect an abrupt transition from dense afferent blockade to restored nociceptive input on a background of postoperative inflammation and NMDA receptor–mediated central sensitization.
Among potential systemic or perineural adjuvants, we focused on esketamine and dexamethasone because their mechanisms of action plausibly target these pathophysiologic components. Esketamine, the S-enantiomer of ketamine, is a potent NMDA receptor antagonist that can attenuate central sensitization and reduce postoperative pain and opioid requirements.12,13 Dexamethasone, in contrast, has well-described anti-inflammatory effects and consistently prolongs the duration of peripheral nerve block–related analgesia and improves postoperative pain control.10,14–16
We therefore chose a 2×2 factorial randomized design to evaluate esketamine and dexamethasone both separately and in combination. This design allows efficient estimation of the main effects of each drug within a single trial, while also permitting formal assessment of any interaction—synergistic or antagonistic—between the two agents on rebound pain, without the need for separate, larger parallel-group trials. Because rebound pain is clinically relevant in both its overall intensity and its extreme manifestations, we prespecified two co-primary outcomes: the mean increase in NRS pain score after block resolution, capturing the overall magnitude of pain escalation, and the incidence of severe rebound pain episodes (NRS ≥7), reflecting clinically important, treatment-demanding pain.
Methods
Our randomized double-blind trial was performed in adherence to the principles outlined in the Declaration of Helsinki, and the study protocol received approval from the Ethical Committee of Shanghai Jiaotong University Affiliated Sixth People’s Hospital [2023–042-(1)]. All participants provided written informed consent. The trial was registered on www.chictr.org.cn (ChiCTR2300072416) before the first patient was enrolled.
Subject Selection
We enrolled patients aged ≥18 years with an American Society of Anesthesiologists (ASA) physical status of I or II who were scheduled for elective arthroscopic shoulder surgery from June 2023 to May 2024.
Exclusion criteria included coagulation disorders, neuropathic disorders, diaphragmatic paralysis, allergy to local anesthetics, severe cardiopulmonary disease, systemic steroid use, presence of any chronic pain, chronic opioid use, stomach ulcer, uncontrolled diabetes, psychiatric disorders, pregnancy, severe obesity (body mass index >35 kg/m2), previous shoulder surgery, inability to understand pain scoring or instructions for intravenous patient-controlled analgesia (PCA), and a history of failed ISB.
Preoperative Assessment
The day before surgery, we quantified preoperative pain at rest, movement, and night at the surgical site using a numeric rating scale (NRS) ranging 0 to 10 (where 0 represents no pain and 10 indicates the worst possible pain). We documented routine medications and comorbidities. Participants also completed the Central Sensitization Inventory (CSI), a self-report questionnaire consisting of two parts.17 The Chinese version of CSI was used. A score of more than 40 indicates the presence of central sensitisation.18
The Pain Catastrophizing Scale (PCS) was used to assess negative thinking associated with pain, including rumination, magnification, and helplessness.19 A total PCS score of 30 represents clinically meaningful degree of catastrophizing.20 The presence of a neuropathic pain at the operative site was evaluated using the Chinese Version of the Douleur Neuropathique 4 (DN4) questionnaire.21 The scores are added and a score of 4 or more out of 10 is suggestive of neuropathic pain.22
Randomization and Trial Intervention
Randomization 1:1:1:1 was computer-generated and assigned patients to placebo-placebo, esketamine-placebo, dexamethasone-placebo, and esketamine-dexamethasone. Allocation was concealed with sealed opaque envelopes that were opened and prescribed by a researcher not associated with the study before patients entered the OR. After anesthetic induction and before surgical incision, patients randomized to esketamine were given 0.15 mg/kg of the drug intravenously whereas those assigned to dexamethasone were given 5 mg dexamethasone intravenously. In both cases, the placebo had a comparable volume of saline. All adjuvants were prepared and administered by a researcher who was not involved in any other study procedures, to ensure that patients, attending anesthesiologists, outcome assessors, and surgeons remained blinded to the treatment allocation.
Intraoperative and Postoperative Treatments
All patients were given 2 mg intravenous midazolam before block insertion to relax patients and to mask psychomimetic side-effects of esketamine. Under ultrasound guidance, all patients had a standardized single injection interscalene brachial plexus block (ISB) administered by one of two anesthesiologists. Patients were positioned supine with their head turned away from the side to be blocked. A high-frequency linear array transducer (13–6 MHz) was used to identify the brachial plexus in the short-axis view over the interscalene region. Using sterile techniques, a 50-mm-long 22-gauge facet tip needle was advanced towards the point between the C5 and C6 roots or the lateral border of the superior trunk, following the in-plane method. After confirmation of correct placement and negative aspiration, 15 mL of 0.3% ropivacaine was injected around the C5 and C6 roots or the superior trunk. Patients who did not experience a loss of cold sensation in the C5 and C6 sensory dermatome or reported significant shoulder pain (numerical rating scale (NRS) score ≥3) in the recovery room were classified as failed blocks.
General anesthesia was induced with sufentanil 0.2 μg kg−1, propofol 1–3 mg kg−1, and rocuronium 0.6 mg kg−1. The trachea was intubated and anesthesia was maintained with sevoflurane at 1.4–2 vol% end-tidal concentration. All surgery was performed by one of three senior doctors. During the surgery, intravenous sufentanil 5–10 μg was given when blood pressure or heart rate exceeded 20% of the preoperative baseline value. Heart rates <50 bpm were treated with 0.25 to 0.5 mg of atropine. At the end of surgery, patients were given 4 mg of ondansetron for nausea prophylaxis. The trachea was extubated in the operating room after reversal of any residual muscle relaxation.
Upon arrival in the recovery room, patients were given intravenous patient-controlled analgesia (PCA), consisting of a solution with 150 μg of sufentanil diluted to 150 mL (administered as a 2 mL bolus with a 15-minute lockout time interval, with a maximum limit of 8 mL per hour and no baseline infusion). Additionally, and per routine, patients were given 50 mg of intravenous flurbiprofen ester every 12 hours for analgesia. When additional analgesia was needed, patients were given 30 mg intravenous ketorolac (up to a maximum of 90 mg/day) and 100 mg of tramadol (up to a maximum of 300 mg/day). After hospital discharge, patients continued to manage pain with a COX-2 inhibitor and the tramadol/acetaminophen combination.
Outcome Measurements
Our first co-primary endpoint was the mean increase in surgical-site numerical rating scale (NRS) pain score from before to after ISB resolution. For each patient, the increase in pain score was defined as the highest postoperative NRS pain score documented within the initial 24 hours after ISB resolution minus the lowest postoperative pain score recorded before ISB resolution.4 The second co-primary endpoint was the incidence of severe rebound pain at the surgical site, defined as NRS ≥7/10 at rest after block resolution. The time of ISB resolution was defined by the first analgesic request; if analgesics were not required, ISB resolution was considered to occur when the patient no longer experienced numbness or heaviness in the ISB area. Secondary outcomes were block duration, pain scores after block resolution, the duration of rebound pain, and sleep disturbances attributed to shoulder pain. The duration of rebound pain was defined as the time interval from the first recorded NRS ≥7 after block resolution until the first subsequent assessment with NRS <4 that was not followed by any further NRS ≥7 values within the first 24 hours after block resolution.
Our first co-primary endpoint was the increase in surgical site mean pain scores increase from before to after the ISB resolved. The second was the incidence of severe rebound pain at the surgical site, defined by pain scores ≥7/10 at the surgical site after block resolution. Pain score differences were defined as the lowest postoperative pain score recorded before ISB resolution subtracted from the highest pain score documented within the initial 24 hours after ISB resolution.4 The time of ISB resolution was defined by the first analgesic request. If analgesics were not required, ISB resolution was considered to have taken place when the patient no longer experienced numbness or heaviness in the ISB area. Secondary outcomes were block duration, pain scores after block resolution, the duration of rebound pain, and sleep disturbances attributed to shoulder pain.
Secondary outcomes were block duration, pain scores after block resolution, the duration of rebound pain, and sleep disturbances attributed to shoulder pain. The duration of rebound pain was defined as the time interval from the first recorded NRS ≥7 after block resolution until the first subsequent assessment with NRS <4 that was not followed by any further NRS ≥7 values within the first 24 hours after block resolution.
Participants in the study were contacted by a research nurse via phone calls on postoperative days 1, 4, 7, 15, and 30. Pain intensity was assessed using the numerical rating scale (NRS), with participants reporting their daily average and maximal pain levels on a scale from 0 to 10. On Day 30 after surgery, participants completed the short form of the Brief Pain Inventory (BPI) to evaluate the impact of pain on various aspects of their daily quality of life, including sleep quality, mood, and analgesic intake.23
Statistical Analyses
The Shapiro–Wilk test was employed to evaluate normalcy. Data are presented as means ± SDs, medians (interquartile range [IQR]), or counts (%). Using a factorial design, a two-way analysis of variance (ANOVA) was conducted with pain score before and after ISB resolution as the dependent variable to evaluate the presence of an interaction between the two therapies. Per routine for factorial trials, in the absence of a significant interaction, treatment effect estimates were to be summarized by comparing results in all patients given esketamine to all patients who were not given esketamine, whether or not given dexamethasone. We similarly would compare results in all patients given dexamethasone to those in all patients who were not given dexamethasone, irrespective of esketamine administration. Should the interaction be substantial, the impact of each intervention would be evaluated within the context of the alternate intervention levels.
Data were analyzed using unpaired t, Mann–Whitney rank-sum, χ2, or Fisher exact tests to evaluate the main effects, as applicable. Differences across groups were additionally expressed as the mean or median differences along with the 95% confidence interval (CI). With a total significance level of 0.05, the significance criterion for the primary outcome in the two comparisons was set at 0.025 for each interventional effect (0.05/2, Bonferroni correction).
Secondary outcomes were not corrected for multiple testing. Predefined exploratory analyses were performed across four factorial groups (representing each combination of esketamine and regional analgesia) via one-way ANOVA, the Kruskal–Wallis test, or the χ2 test, as applicable. In addition, to assess the robustness of the treatment effects and account for prognostically important baseline variables, we performed a multivariable logistic regression analysis with rebound pain as the dependent variable. The model included treatment group (placebo–placebo, dexamethasone alone, esketamine alone, and esketamine plus dexamethasone) and baseline covariates such as female sex, number of inserted anchors, preoperative maximal and night pain, Central Sensitization Inventory (CSI) score, Pain Catastrophizing Scale (PCS) categories, postoperative shoulder outcome index (PSOI) score, and DN4 score.
Primary analyses were performed on all randomized patients with accessible outcome data, without imputation. Data were analyzed utilizing GraphPad Prism software (version 9.0.0; GraphPad, Boston, MA, USA), R version 4.2.2 and Python version 3.7.
In a previous study (N=30), we observed a difference of 5.5±2.0 in the increase in pain score after ISB resolution with the use of ropivacaine alone.19 We anticipated that esketamine and dexamethasone would each reduce the increase in pain scores by approximately 30%, an amount we considered clinically meaningful. A total of 32 patients per level of each intervention were required for α=0.05 and power=90%; we therefore enrolled 40 patients in each of the four groups to account for a 20% dropout rate, for a total of 160 patients. The sample size calculation was thus based on detecting the main effects of each intervention on the first co-primary outcome, assuming no interaction between esketamine and dexamethasone. The trial was not specifically powered to detect a statistically significant interaction effect.
In a previous study (N=30), we observed a difference of 5.5±2.0 in the increase in pain score after ISB resolution with the use of ropivacaine alone.24 We anticipated that esketamine and dexamethasone would each reduce pain scores by 30%, an amount we considered clinically meaningful. A total of 32 patients per group were required for α=0.05 and power=90%; we therefore enrolled 40 patients in each of 4 groups to account for a 20% dropout rate, for a total of 160 patients. The sample size calculation was thus based on detecting the main effects of each intervention on the first co-primary outcome, assuming no interaction between esketamine and dexamethasone. The trial was not specifically powered to detect a statistically significant interaction effect.
Results
A total of 180 patients were assessed for eligibility, of whom 20 were excluded (8 surgery cancelled and 12 declined to participate). The remaining 160 patients were randomised equally into four groups (n = 40 per group): placebo–placebo, placebo–dexamethasone, esketamine–placebo, and esketamine–dexamethasone. All participants received the allocated intervention. No patients were lost to follow-up or excluded after randomisation, and all 160 patients were included in the final analysis (Figure 1).
 |
Figure 1 The Consolidated Standards of Reporting Trials statement. |
Patients Characteristics
Baseline demographic and clinical characteristics were well balanced across the four groups (Table 1). Age, sex distribution, ASA physical status, BMI, and education level were comparable. The prevalence of comorbidities, types of surgery, and number of anchors inserted did not differ substantially between groups. Preoperative pain intensity, psychological measures (PCS, CSI, PSQI), and neuropathic pain scores (DN4) were also similar across groups.
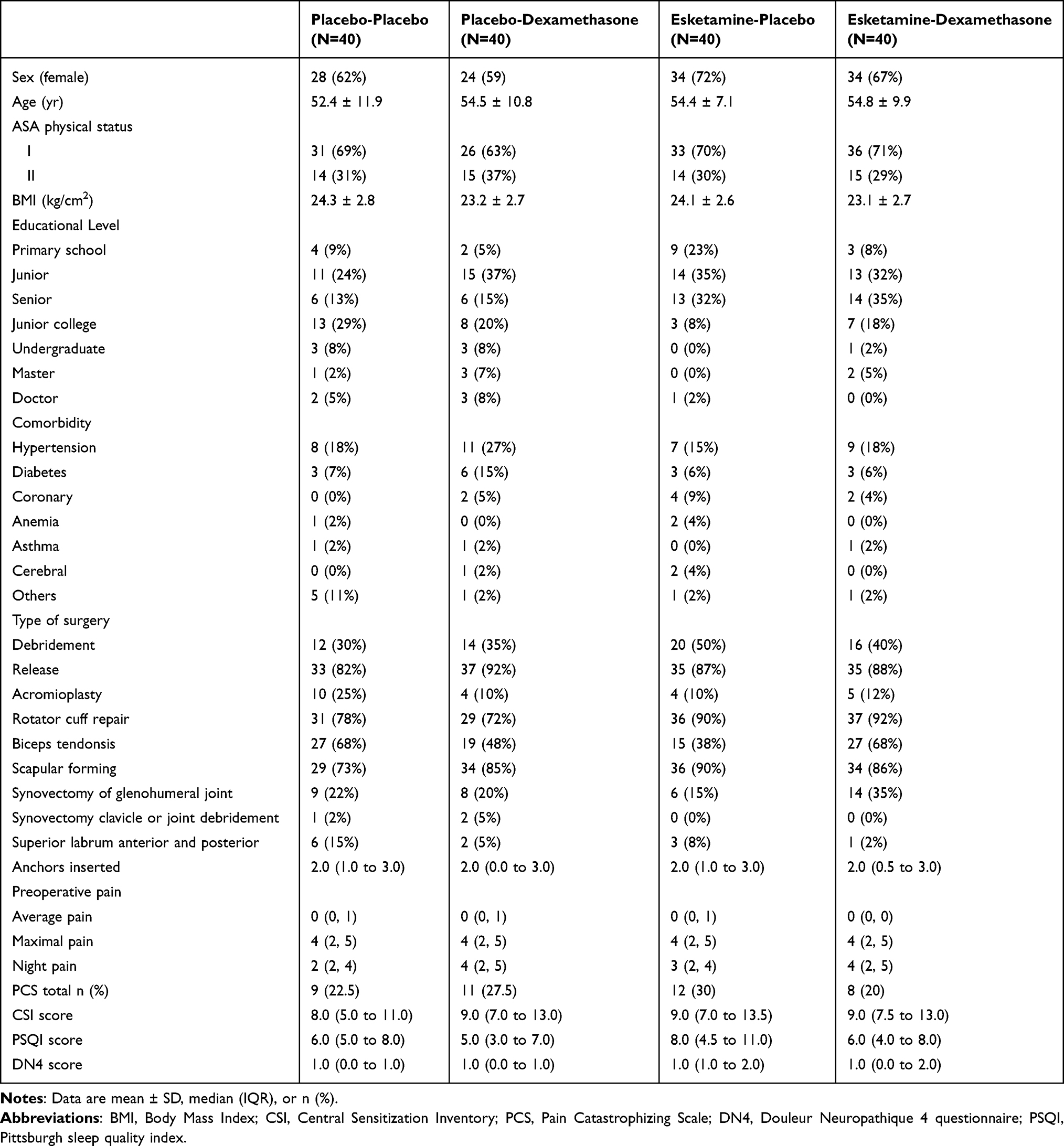 |
Table 1 Patient Characteristics |
Primary Outcomes
No significant interaction was observed between esketamine and dexamethasone for the difference in increase in pain score after ISB resolution (P = 0.4055) or for the incidence of rebound pain (P=0.3793). Consequently, the outcomes of the two primary effects were evaluated across all patients given each drug (Table 2).
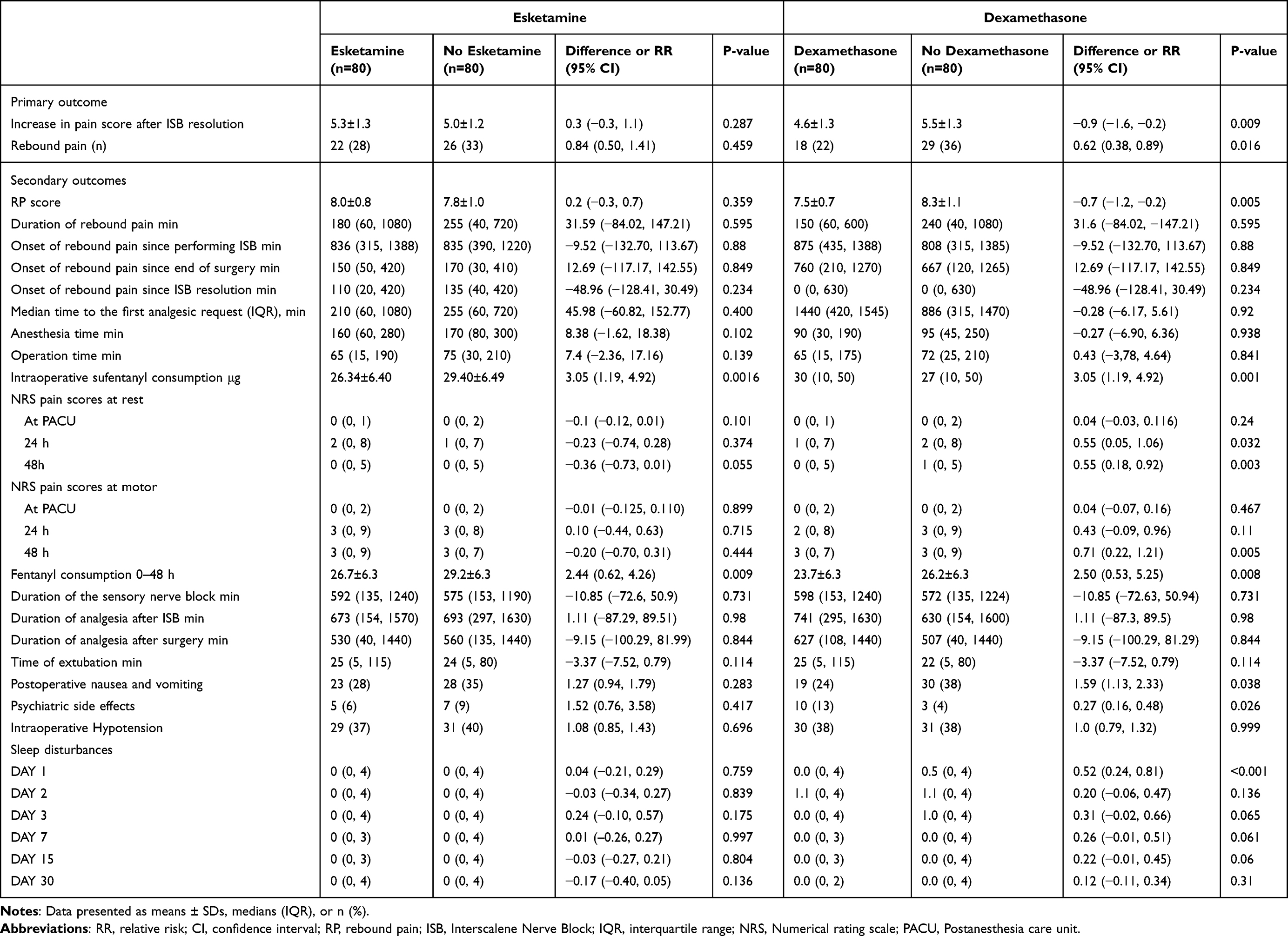 |
Table 2 Primary and Secondary Outcomes |
Increase in pain score after ISB resolution were 4.6±1.3 in patients given dexamethasone (N=80) which was lower than scores of 5.5±1.3 reported by patients who did not receive dexamethasone (N=80, difference 0.9, 95% CI: −1.6, −0.2; P = 0.009, Figure 2). Increase in pain score after ISB resolution were 5.3±1.3 for patients given esketamine (N=80) compared with 5.0±1.2 in those who did not receive esketamine (N=80, difference 0.3, 95% CI: −0.3, 1.1; P=0.287, not statistically significant; Table 2). For esketamine vs no Esketamine, the between-group difference of the treatment effect did not reach the minimal clinically important difference) of 1.0. For dexamethasone vs no dexamethasone, although the difference did not achieve minimal clinically important difference, the pain scores in the dexamethasone group were significantly lower than those in the dexamethasone placebo group (P=0.009) (Figure 2).
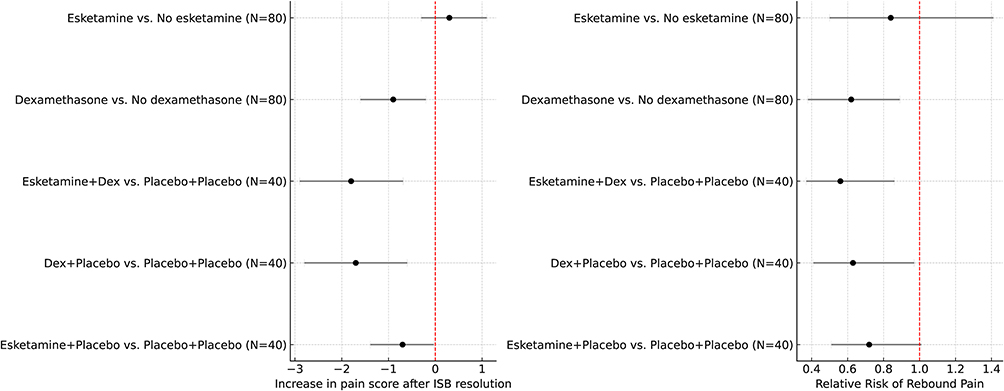 |
Figure 2 Forest plot of treatment effects across groups. This forest plot illustrates the effect sizes and 95% confidence intervals for primary and secondary outcomes comparing different combinations of esketamine and dexamethasone interventions. Point estimates and CIs are presented for each group comparison, with values to the left or right of the vertical line indicating a benefit favouring one intervention over another. The plot demonstrates the differential impact of esketamine, dexamethasone, and their combination on the measured outcomes. Statistically significant differences (i.e. those not crossing the line of no effect) are marked accordingly. |
The incidence of rebound pain was 22 (27%) for patients administered esketamine (N=80), compared to the 26 (32%) observed in those given no esketamine (N=80, relative risk (RR) 0.84, 95% CI: 0.50, 1.41; P=0.459, Table 2). The incidence of rebound pain was 18 (22%) in patients given dexamethasone (N=80), which was lower than 29 (36%) of the patients given no dexamethasone (N=80, RR = 0.62, 95% CI, 0.38, 0.89; P = 0.016, Table 2). Using Placebo-Placebo as the reference category, increase in pain score after ISB resolution were significantly different compared to Placebo-Dexamethasone (N=40, difference = −1.7, 95% CI, −2.8, −0.6, P=0.003) and Esketamine-Dexamethasone (N=40, difference = −1.8, 95% CI, −2.9, −0.69, P=0.002)(Table 3 and Figure 3).
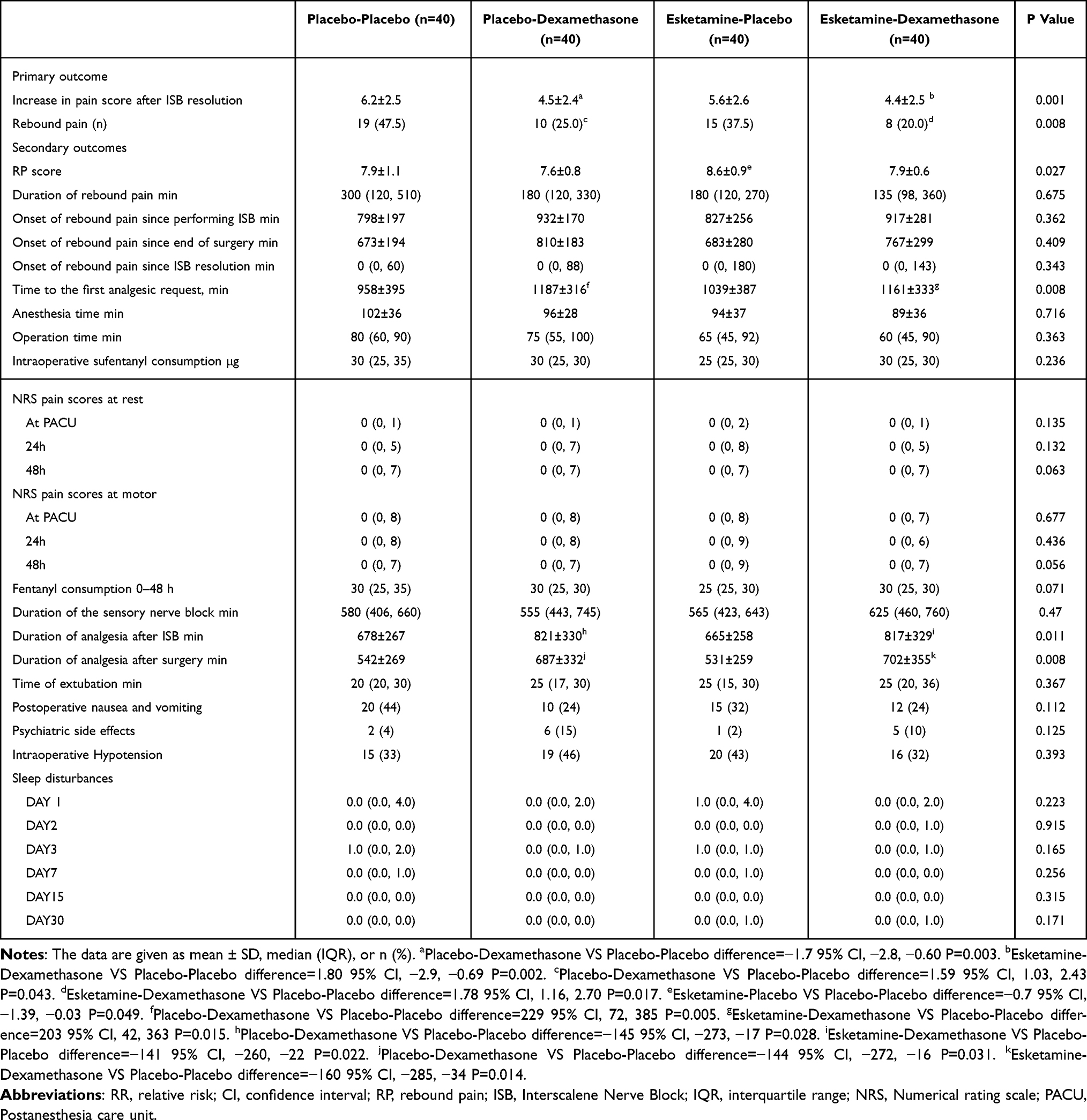 |
Table 3 Exploratory Analyses of Outcomes Across Four Groups |
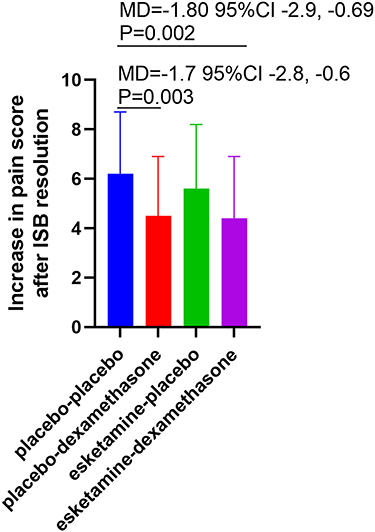 |
Figure 3 Group comparisons of intervention effects. Bar plots show the mean values (with standard error bars) of the primary outcome across the four treatment groups: placebo–placebo, placebo–dexamethasone, esketamine–placebo, and esketamine–dexamethasone. Placebo–dexamethasone reduced the outcome compared to placebo–placebo, with the greatest reduction observed in the combination group. Abbreviations: MD, mean difference; CI, Confidence Interval. |
In a multivariable logistic regression model adjusting for female sex, number of inserted anchors, preoperative maximal and night pain, CSI and PCS categories, PSOI score, and DN4 score, the dexamethasone-containing groups remained independently associated with a lower risk of rebound pain, whereas the estimates for esketamine remained non-significant. The adjusted odds ratios and 95% confidence intervals are presented in Supplementary Table 1, and were consistent in magnitude and direction with the primary unadjusted analyses.
Secondary Outcomes
Esketamine showed similar rebound pain score (RP score) with those given no esketamine (N=80, difference = 0.2, 95% CI, −0.3, 0.7), while dexamethasone reduced the RP score (N=80, difference = −0.7, 95% CI, −1.2, −0.2) (Table 2).
Numerical rating scale pain scores at rest were similar in both the esketamine and no esketamine groups. Dexamethasone reduced NRS pain at rest 24 hours (N=80, difference = 0.55, 95% CI, 0.18, 0.92) and during movement 48 hours postoperatively, compared with no dexamethasone (N=80, difference = 0.71, 95% CI, 0.22, 1.21). Intraoperative sufentanil use was reduced in the esketamine groups (N=80, difference = 3.05, 95% CI, 1.19, 4.92), as well as between dexamethasone and no dexamethasone groups (N=80, difference =3.05, 95% CI, 1.19, 4.92). Similarly, postoperative fentanyl use decreased in both the esketamine and no esketamine groups (N=80, difference = 2.44, 95% CI, 0.62, 4.26), and between dexamethasone and no dexamethasone groups (N=80, difference = 2.50, 95% CI, 0.53, 5.25). Sleep disturbances were similar in the esketamine and no esketamine groups, while dexamethasone improved sleep on Day 1 postoperatively (N=80, difference = 0.52, 95% CI, 0.24, 0.81). No serious adverse events occurred (Table 2).
Exploratory Analysis
In the pre-specified exploratory analysis of outcomes across all four groups, significant differences were found in increase in pain score after ISB resolution, rebound pain score, median time to first analgesic request (IQR), duration of analgesia after ISB, and duration of analgesia after surgery (P<0.05) (Table 3).
Placebo-Placebo was associated with a higher incidence of rebound pain than Placebo-Dexamethasone (N=40, RR = 1.59, 95% CI, 1.03, 2.43) and Esketamine-Dexamethasone (N=40, RR = 1.78, 95% CI, 1.16, 2.70). Compared to Placebo-Placebo, Esketamine-Placebo showed a slightly lower difference in rebound pain score (N=40, difference = −0.7, 95% CI, −1.39, −0.03). Placebo-Placebo was associated with shorter duration of analgesia after ISB and surgery than Placebo-Dexamethasone (N=40, difference = −145, 95% CI, −273, −17; N=40,difference = −144, 95% CI, −272, −16) and Esketamine-Dexamethasone (N=40, difference = −141, 95% CI, −260, −22; N=40, difference = −160, 95% CI, −285, −34) (Table 3).
Kaplan-Meier survival analysis revealed a significant difference in time to first analgesic request among the groups (Log rank test, P<0.001), with Placebo-Dexamethasone and Esketamine-Dexamethasone showing longer times compared to Placebo-Placebo (N=40, difference = 229, 95% CI, 72, 385; difference = 203, 95% CI, 42, 363, respectively) (Supplementary Figure 1 and Table 3).
Discussion
In this 2×2 randomized factorial trial targeting patients with postoperative rebound pain after arthroscopic shoulder surgery, the intravenous dexamethasone, administered as a single injection in combination with ISB using ropivacaine reduced pain scores, although the difference did not reach the minimal clinically important difference. This finding suggests that, at the level of average pain intensity, the effect of dexamethasone on rebound pain is modest and should not be interpreted as a large, patient-perceivable improvement in all cases. We therefore consider the reduction in pain escalation to be of uncertain clinical importance when viewed in isolation and have tempered our conclusions accordingly. Moreover, we found that the combination of intravenous dexamethasone and ISB with ropivacaine not only prolonged analgesia but also decreased the incidence of rebound pain. In contrast, a single dose of esketamine did not affect rebound pain incidence or intensity.
Prior research has indicated that, in contrast to general anesthesia, a single-shot brachial plexus block may be linked to severe rebound pain. Rebound pain is not well-defined, The essential characteristic of rebound pain is acute postoperative pain that occurs after the effect of peripheral nerve block resolves, which is clinically significant.9 Therefore, we assessed rebound pain from the time of interscalene block resolution, considering that rebound pain occurred when the NRS score was ≥7/10 at the surgical site after ISB resolution.
Rebound pain incoorating with dexamethasone into ISB is a straightforward and widely recognized method to prolong its analgesic duration. In a randomized controlled trial involving patients undergoing arthroscopic rotator cuff repair, intravenous dexamethasone was more effective than placebo in reducing the increase in pain and the incidence of rebound pain after the resolution of interscalene brachial plexus block (ISB).24 In a subsequent study, Jae Hee Woo et al suggested that dexamethasone may reduce the occurrence of rebound pain by prolonging the duration of nerve blockade and modulating the perioperative inflammatory response.25 In our study, rebound pain was evident at 12 hours after ISB in the control group and at 18 hours after ISB in the dexamethasone group, aligning with the prolonged analgesic duration provided by ISB. Since both groups experienced the onset of rebound pain within 2 days after surgery, during the period when the inflammatory response remained active, it is plausible to attribute the reduction in rebound pain to the aforementioned factors, thus suggesting the effectiveness of intravenous dexamethasone.
Our study demonstrated that a single antihyperalgesic dose of esketamine did not lead to a difference in the incidence or intensity of rebound pain among the groups. These finds can be explained through the following mechanisms: firstly, the application of multimodal analgesia may have masked the potential benefits of esketamine. Previous studies investigating low doses of ketamine (0.2–1.0 mg/kg) as an adjunct to locoregional anesthesia were predominantly conducted under general anesthesia.26,27 Although these studies confirmed its opioid-sparing effect postoperatively, the improvement in pain scores remained controversial. A study on patients undergoing cesarean delivery under spinal anesthesia found that even with the administration of 10 mg of intravenous ketamine combined with a perioperative multimodal analgesic regimen,28 the incidence of breakthrough pain within 24 hours was still as high as 75% in the ketamine group and 74% in the placebo group, suggesting that simply increasing ketamine may not overcome the “ceiling effect” of multimodal analgesia.28 Secondly, the ineffectiveness of ketamine may reflect a limited involvement of central sensitization in the occurrence of rebound pain. Although this study assessed the pro-nociceptive system using the Central Sensitization Inventory (CSI), there was no significant difference in the preoperative CSI positive rate (>40) between the groups. Lastly, a comprehensive retrospective study found that intraoperative administration of ketamine had no significant effect on the incidence of breakthrough pain (40%), which is consistent with the conclusion of this study.8
However, rebound pain is clinically relevant not only in terms of average pain intensity but also through the occurrence of severe, treatment-demanding episodes. In this context, dexamethasone was associated with a meaningful reduction in the incidence of severe rebound pain, which we prespecified as a co-primary outcome because it better reflects those episodes that most disturb sleep, prompt unplanned health-care contact, or drive rescue analgesic use. Given the low cost and favorable risk profile of intravenous dexamethasone, even a sub-MCID reduction in the mean increase in pain score, when combined with fewer severe rebound pain episodes, may still represent a worthwhile benefit as part of a multimodal analgesic strategy after shoulder surgery.
Limitations of the Study
Rebound pain in this study was defined based on the Numeric Rating Scale (NRS) reported by patients when the interscalene brachial plexus block (ISB) wore off. Various definitions of rebound pain exist, including one that suggests using the highest pain score within the first 24 hours instead of “recall pain” (pain experienced when the ISB wears off). In this study, recall pain was compared with the NRS reported by patients on Day 1, and both the intensity and incidence of severe pain (NRS >7/10) were strongly correlated. Thus, the rebound pain definition used may be considered acceptable.
The follow-up period was limited to 30 days, not assessing the potential long-term impact of rebound pain on chronic postsurgical pain. The low, single dose of esketamine used may have influenced the anti-hyperalgesic effect observed. Additionally, the psychophysical tests for central sensitization may not be fully reliable in an acute postoperative setting, and the DN4 questionnaire may also have limitations in this context. Our esketamine regimen consisted of a single 0.15 mg/kg intravenous bolus without a maintenance infusion, which is at the lower end of the range used in previous low-dose esketamine trials. Although we chose this subanesthetic dose to balance potential antihyperalgesic effects against the risk of psychotomimetic and hemodynamic adverse events in ambulatory patients, it remains possible that higher or repeated dosing might have produced a larger effect on rebound pain. Our results should therefore be interpreted as showing a lack of meaningful benefit with this specific low-dose regimen rather than excluding any potential effect of esketamine at all possible doses.
Finally, since the study did not include a non-ISB group, we could not determine if the rebound pain observed offset the early benefits of the ISB procedure itself.
Conclusion
Intravenous dexamethasone, but not esketamine, reduced the incidence of severe rebound pain after interscalene brachial plexus block for arthroscopic shoulder surgery and produced a modest, sub-MCID attenuation of the increase in pain intensity after block resolution. These findings support dexamethasone as a useful, low-cost component of multimodal analgesia in this setting, while expectations regarding average pain relief should remain conservative.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
The author(s) declare that no generative AI or AI-assisted technologies were used in the writing process of this manuscript.
Acknowledgments
We would like to thank Daniel I. Sessler for revising the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (82271250).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abdallah FW, Halpern SH, Aoyama K, Brull R. Will the real benefits of single-shot interscalene block please stand up? A systematic review and meta-analysis. Anesthesia Analg. 2015;120(5):1114–1129. doi:10.1213/ANE.0000000000000688
2. Toma O, Persoons B, Pogatzki-Zahn E, Van de Velde M, Joshi GP. PROSPECT guideline for rotator cuff repair surgery: systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2019;74(10):1320–1331. doi:10.1111/anae.14796
3. Salinas FV, Joseph RS. Peripheral nerve blocks for ambulatory surgery. Anesthesiol Clin. 2014;32(2):341–355. doi:10.1016/j.anclin.2014.02.005
4. Lavand’homme P. Rebound pain after regional anesthesia in the ambulatory patient. Current Opin Anaesthesiol. 2018;31(6):679–684. doi:10.1097/ACO.0000000000000651
5. Hade AD, Okano S, Pelecanos A, Chin A. Factors associated with low levels of patient satisfaction following peripheral nerve block. Anaesth Intensive Care. 2021;49(2):125–132. doi:10.1177/0310057X20972404
6. Sunderland S, Yarnold CH, Head SJ, et al. Regional versus general anesthesia and the incidence of unplanned health care resource utilization for postoperative pain after wrist fracture surgery: results from a retrospective quality improvement project. Reg Anesth Pain Med. 2016;41(1):22–27. doi:10.1097/AAP.0000000000000325
7. Hamilton DL. Rebound pain: distinct pain phenomenon or nonentity? Br J Anaesth. 2021;126(4):761–763. doi:10.1016/j.bja.2020.12.034
8. Barry GS, Bailey JG, Sardinha J, Brousseau P, Uppal V. Factors associated with rebound pain after peripheral nerve block for ambulatory surgery. Br J Anaesth. 2021;126(4):862–871. doi:10.1016/j.bja.2020.10.035
9. Muñoz-Leyva F, Cubillos J, Chin KJ. Managing rebound pain after regional anesthesia. Kor J Anesthesiol. 2020;73(5):372–383. doi:10.4097/kja.20436
10. Woo JH, Kim YJ, Kim DY, Cho S. Dose-dependency of dexamethasone on the analgesic effect of interscalene block for arthroscopic shoulder surgery using ropivacaine 0.5%: a randomised controlled trial. Eur J Anaesthesiol. 2015;32(9):650–655. doi:10.1097/EJA.0000000000000213
11. Chun EH, Kim YJ, Woo JH. Which is your choice for prolonging the analgesic duration of single-shot interscalene brachial blocks for arthroscopic shoulder surgery? Intravenous dexamethasone 5 mg vs. perineural dexamethasone 5 mg randomized, controlled, clinical trial. Medicine. 2016;95(23):e3828. doi:10.1097/MD.0000000000003828
12. De Kock MF, Lavand’homme PM. The clinical role of NMDA receptor antagonists for the treatment of postoperative pain. Best Pract Res Clin Anaesth. 2007;21(1):85–98. doi:10.1016/j.bpa.2006.12.006
13. Lei Y, Liu H, Xia F, et al. Effects of esketamine on acute and chronic pain after thoracoscopy pulmonary surgery under general anesthesia: a multicenter-prospective, randomized, double-blind, and controlled trial. Front Med. 2021;8:693594. doi:10.3389/fmed.2021.693594
14. Cummings KC 3rd, Napierkowski DE, Parra-Sanchez I, et al. Effect of dexamethasone on the duration of interscalene nerve blocks with ropivacaine or bupivacaine. Br J Anaesth. 2011;107(3):446–453. doi:10.1093/bja/aer159
15. Kawanishi R, Yamamoto K, Tobetto Y, et al. Perineural but not systemic low-dose dexamethasone prolongs the duration of interscalene block with ropivacaine: a prospective randomized trial. Local Reg Anesth. 2014;7:5–9. doi:10.2147/LRA.S59158
16. Sakae TM, Marchioro P, Schuelter-Trevisol F, Trevisol DJ. Dexamethasone as a ropivacaine adjuvant for ultrasound-guided interscalene brachial plexus block: a randomized, double-blinded clinical trial. J Clin Anesth. 2017;38:133–136. doi:10.1016/j.jclinane.2017.02.004
17. Cuesta-Vargas AI, Neblett R, Chiarotto A, et al. Dimensionality and reliability of the central sensitization inventory in a pooled multicountry sample. J Pain. 2018;19(3):317–329. doi:10.1016/j.jpain.2017.11.006
18. Neblett R, Hartzell MM, Cohen H, et al. Ability of the central sensitization inventory to identify central sensitivity syndromes in an outpatient chronic pain sample. Clin J Pain. 2015;31(4):323–332. doi:10.1097/AJP.0000000000000113
19. Osman A, Barrios FX, Kopper BA, Hauptmann W, Jones J, E O. Factor structure, reliability, and validity of the pain catastrophizing scale. J Behav Med. 1997;20(6):589–605. doi:10.1023/A:1025570508954
20. Hayashi K, Ikemoto T, Shiro Y, et al. A systematic review of the variation in pain catastrophizing scale reference scores based on language version and country in patients with chronic primary (non-specific) pain. Pain Ther. 2022;11(3):753–769. doi:10.1007/s40122-022-00390-0
21. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005;114(1–2):29–36. doi:10.1016/j.pain.2004.12.010
22. Bennett MI, Attal N, Backonja MM, et al. Using screening tools to identify neuropathic pain. Pain. 2007;127(3):199–203. doi:10.1016/j.pain.2006.10.034
23. Tan G, Jensen MP, Thornby JI, Shanti BF. Validation of the brief pain inventory for chronic nonmalignant pain. J Pain. 2004;5(2):133–137. doi:10.1016/j.jpain.2003.12.005
24. Woo JH, Lee HJ, Oh HW, Lee JW, Baik HJ, Kim YJ. Perineural dexamethasone reduces rebound pain after ropivacaine single injection interscalene block for arthroscopic shoulder surgery: a randomized controlled trial. Reg Anesth Pain Med. 2021;46(11):965–970. doi:10.1136/rapm-2021-102795
25. Lee HJ, Woo JH, Chae JS, Kim YJ, Shin SJ. Intravenous versus perineural dexamethasone for reducing rebound pain after interscalene brachial plexus block: a randomized controlled trial. J Korean Med Sci. 2023;38(24):e183. doi:10.3346/jkms.2023.38.e183
26. Jouguelet-Lacoste J, La Colla L, Schilling D, Chelly JE. The use of intravenous infusion or single dose of low-dose ketamine for postoperative analgesia: a review of the current literature. Pain Med. 2015;16(2):383–403.
27. Riddell JM, Trummel JM, Onakpoya IJ. Low-dose ketamine in painful orthopaedic surgery: a systematic review and meta-analysis. Br J Anaesth. 2019;123(3):325–334. doi:10.1016/j.bja.2019.05.043
28. Bauchat JR, Higgins N, Wojciechowski KG, McCarthy RJ, Toledo P, Wong CA. Low-dose ketamine with multimodal postcesarean delivery analgesia: a randomized controlled trial. Int J Obstetric Anesth. 2011;20(1):3–9. doi:10.1016/j.ijoa.2010.10.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effects of Intravenous Dexamethasone on Rebound Pain After Nerve Block in Patients with Ankle Fracture: A Randomized Controlled Trial
Gao M, Li Y, Yu J, Li W, Qin S, Zhang Y, Zhu L, Hou Z, Wang Q
Journal of Pain Research 2023, 16:1127-1136
Published Date: 31 March 2023
A Randomized Controlled Trial to Compare the Efficacy of Single versus Triple Injection Technique for Ultrasound-Guided Infraclavicular Block in Upper Limb Surgeries
Vedavyas R, Saravanan R, Mirunalini G, Gayathri B
Local and Regional Anesthesia 2023, 16:51-58
Published Date: 18 May 2023
Current Status and Global Trend of Rebound Pain After Regional Anesthesia: A Bibliometric Analysis
Zhou R, Jiang W, Miao Q, Li X, Xiong L
Local and Regional Anesthesia 2024, 17:67-77
Published Date: 9 May 2024
Preoperative Anxiety’s Impact on the Median Effective Dose of Esketamine for Alleviating Propofol Injection Pain in Patients Undergoing Painless abortion: A Randomized, Double-Blind, Controlled Trial

Shen Y, Yin L, Hu B, Xia Y, Zhang L
Drug Design, Development and Therapy 2024, 18:5863-5872
Published Date: 7 December 2024
Effect of Intravenous Esketamine on Rebound Pain Following Single-Shot Brachial Plexus Block in Patients Undergoing Shoulder Arthroscopic Surgery: A Prospective, Randomized, Placebo-Controlled Study
Chen J, Pan Z, Zheng J
Journal of Pain Research 2025, 18:5235-5248
Published Date: 7 October 2025