Back to Journals » Cancer Management and Research » Volume 18

Development and Validation of a Nomogram for Predicting Postoperative Deep Vein Thrombosis Risk in Patients After Laparoscopic Partial Nephrectomy
Authors Wu C, Li Y, Wang X, Pan H, Jiang D
Received 10 April 2025
Accepted for publication 29 August 2025
Published 12 January 2026 Volume 2026:18 533674
DOI https://doi.org/10.2147/CMAR.S533674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Chunyan Wu,1 Yujia Li,2,3 Xianglian Wang,2,3 Hanlin Pan,1 Duoyun Jiang2,3
1School of Nursing, Yongzhou Vocational Technical College, Yongzhou, Hunan, 425100, People’s Republic of China; 2Department of Urinary Surgery, The Central Hospital of Yongzhou, Yongzhou, Hunan, 425000, People’s Republic of China; 3Department of Urinary Surgery, Yongzhou Hospital Affiliated to University of South China, Yongzhou, Hunan, 425000, People’s Republic of China
Correspondence: Duoyun Jiang, Department of Urinary Surgery, The Central Hospital of Yongzhou, 151 Xiaoshui West Road, Lingling District, Yongzhou, Hunan, 425100, People’s Republic of China, Tel +8615807463629, Email [email protected]
Objective: To construct a nomogram model for individualized prediction of risk of deep vein thrombosis (DVT) in renal cell carcinoma (RCC) patients after laparoscopic partial nephrectomy (PN).
Methods: A retrospective study was conducted on 556 RCC patients admitted to our hospital from January 2015 to January 2025. Patients were randomly divided into a modeling group (n=389) and a validation group (n=167) at a ratio of 7:3. The modeling group was further subdivided into DVT and non-DVT groups based on postoperative DVT occurrence. Clinical data were collected. Logistic regression was used to analyze the influencing factors. R software was used to construct the nomogram. ROC curves were generated to evaluate the discrimination ability of the nomogram. Decision curve analysis (DCA) was performed to assess its clinical utility.
Results: Of 556 patients, 100 (17.98%) developed DVT, including 70 (17.99%) in the modeling group. Logistic regression identified age, operation time, time in bed, pneumoperitoneum pressure, duration of indwelling drains, total cholesterol (TC), and D-dimer as significant risk factors (P < 0.05). The area under the curve (AUC) was 0.889 for the modeling group and 0.866 for the validation group. Hosmer-Lemeshow test indicated good calibration (modeling group: χ²=7.120, P=0.714; validation group: χ²=7.058, P=0.724). DCA showed clinical utility for predicted probabilities between 0.08 and 0.96.
Conclusion: Age, operation time, time in bed, pneumoperitoneum pressure, duration of indwelling drains, TC, and D-dimer are risk factors for DVT in patients after laparoscopic PN. The constructed nomogram demonstrates good predictive performance and can be used for individualized risk assessment of postoperative DVT in RCC patients.
Keywords: renal cell carcinoma, partial nephrectomy, deep vein thrombosis, risk factors, nomogram
Introduction
Renal cell carcinoma (RCC) is a common malignancy, originating from the epithelium of the renal tubules and accounting for approximately 80% of malignant tumors of the kidney. It mainly affects middle-aged and elderly patients, and its incidence is increasing annually worldwide, posing a serious threat to patient survival.1,2 Partial nephrectomy (PN) is the main clinical treatment for early-stage RCC. Compared with traditional open surgery, laparoscopic PN offers the advantages of less trauma, greater precision, faster postoperative recovery, and better preservation of surrounding renal tissue. These benefits allow for the effective treatment of localized RCC while maximizing renal function, ultimately improving surgical outcomes and patient prognosis.3,4 The incidence of DVT with conventional surgery may reach 25%, whereas laparoscopic surgery may reduce it to around 10%. However, postoperative complications remain unavoidable. Due to VHL gene mutations, RCC exhibits an inherent hypercoagulable state, leading to HIF-mediated overexpression of procoagulant factors. Combined with surgical stress, this forms a high-risk condition, and some patients still develop deep vein thrombosis (DVT) of the lower extremities after surgery. If a thrombus dislodges, it may cause pulmonary embolism, and in the long term, it may trigger post-thrombotic syndrome, or even lead to death.5 Therefore, identifying the risk factors that influence DVT in clinical practice is particularly important for preventing this complication and improving patient outcomes. Nomogram prediction models can more accurately predict adverse outcomes by transforming a relatively complex regression equation into an easily understandable graphical tool, thereby assisting clinicians in calculating the values of various variables using the figure and determining the incidence of adverse outcomes.6 For instance, a predictive model for postoperative lower extremity DVT in gastric cancer patients demonstrated good predictive value in both the training and validation cohorts.7 While there have been many studies analyzing the risk factors for DVT after PN in patients with RCC, research on a nomogram in this context remains limited. Therefore, this study aimed to develop and validate a nomogram prediction model for the individualized DVT risk in RCC patients after PN.
Materials and Methods
Study Population
A retrospective analysis was conducted on 556 RCC patients admitted to our hospital from January 2015 to January 2025. They were randomly divided into a modeling group (389 cases) and a validation group (167 cases) at a ratio of 7:3. According to whether postoperative DVT occurred, the modeling group was further subdivided into a DVT group and a non-DVT group. The flowchart of case collection is shown in Figure 1. Inclusion criteria: (1) meeting the standards for RCC,8 confirmed by pathology; (2) unilateral RCC, all at early stage; (3) all underwent PN; (4) no preoperative radiotherapy or chemotherapy; (5) complete clinical data. Exclusion criteria: (1) history of DVT; (2) presence of other malignant tumors; (3) diabetic nephropathy; (4) failure of vital organs such as the liver; (5) immunodeficiency; (6) cognitive impairment; (7) hematological diseases; (8) any surgical contraindications. This study was approved by the hospital’s ethics committee.
 |
Figure 1 Case flow collection diagram. |
Methods
Surgical Procedure
Under general anesthesia, the patient was placed in the healthy-side lateral decubitus position. After skin disinfection and draping, a pneumoperitoneum was established with carbon dioxide, maintaining the pressure at 12–15 mmHg. The dorsal and ventral aspects of the kidney were separated along the renal fascia to fully expose the lesion. The renal artery was then clamped with a vascular clip, and the tumor was excised using an ultrasonic scalpel. After suturing the wound surface, the vascular clip was removed, and once renal blood supply was restored, a drainage tube was placed and the incision was closed. Low-molecular-weight heparin prophylaxis was administered according to the patient’s condition.
DVT Determination Criteria
Postoperatively, patients underwent Wells scoring9 and D-dimer tests. Those with moderate/high DVT risk based on the Wells score, together with elevated D-dimer levels, were subjected to lower-extremity deep venous ultrasonography. Ultrasonic imaging revealing solid echo filling in the lower-extremity deep venous lumen was indicative of DVT.10
Clinical Data Collection
Collect data from the patients’ electronic medical record database, mainly including clinical data:age, gender, body mass index(BMI), diabetes, hypertension, smoking history, drinking history, coronary heart disease, side of the tumor, TNM stage, tumor location, tumor diameter, operation time, intraoperative blood loss, bed rest time, surgical approach, pneumoperitoneum pressure, indwelling drainage time, time to recovery of bowel sounds, use of intermittent pneumatic compression devices; Lipid metabolism indicators: total cholesterol(TC),triglycerides(TG),LDL cholesterol (LDL-C), HDL cholesterol (HDL-C); Blood pressure indicators:systolic pressure, diastolic pressure; Complete blood count (CBC) indicators: white blood cell count (WBC), hemoglobin (HGB), platelet count (PLT);Inflammatory markers:total protein (TP), high-sensitivity C-reactive protein (HsCRP), fibrinogen (FIB); Glucose metabolism indicators:fasting blood glucose (FBG);Renal function indicators: urinary microalbumin (UmAlb), β2 microglobulin (β2-MG), urinary retinol-binding protein (RBP), creatinine (Cr), urea nitrogen (BUN), D-dimer;Coagulation function indicators:prothrombin time (PT), and activated partial thromboplastin time (APTT).
Statistical Analysis
SPSS 25.0 software was used to perform independent sample t-test and χ^2 test. Logistic regression analysis was conducted to identify the influencing factors of postoperative DVT risk in RCC patients after PN. R software (version 4.5.1) with the rms package was used to construct the nomogram model for predicting postoperative DVT risk. The Receiver Operating Characteristic (ROC) curves were applied to evaluate the discriminatory ability of the nomogram; Calibration curves were used to assess the model’s consistency; and Decision Curve Analysis (DCA) was performed to evaluate the clinical utility of the nomogram model. A p-value < 0.05 was considered statistically significant.
Results
Comparison of Clinical Data Between the Modeling Group and the Validation Group
There were no differences in age, sex, or other clinical data between the modeling group and the validation group (P > 0.05). See Table 1.
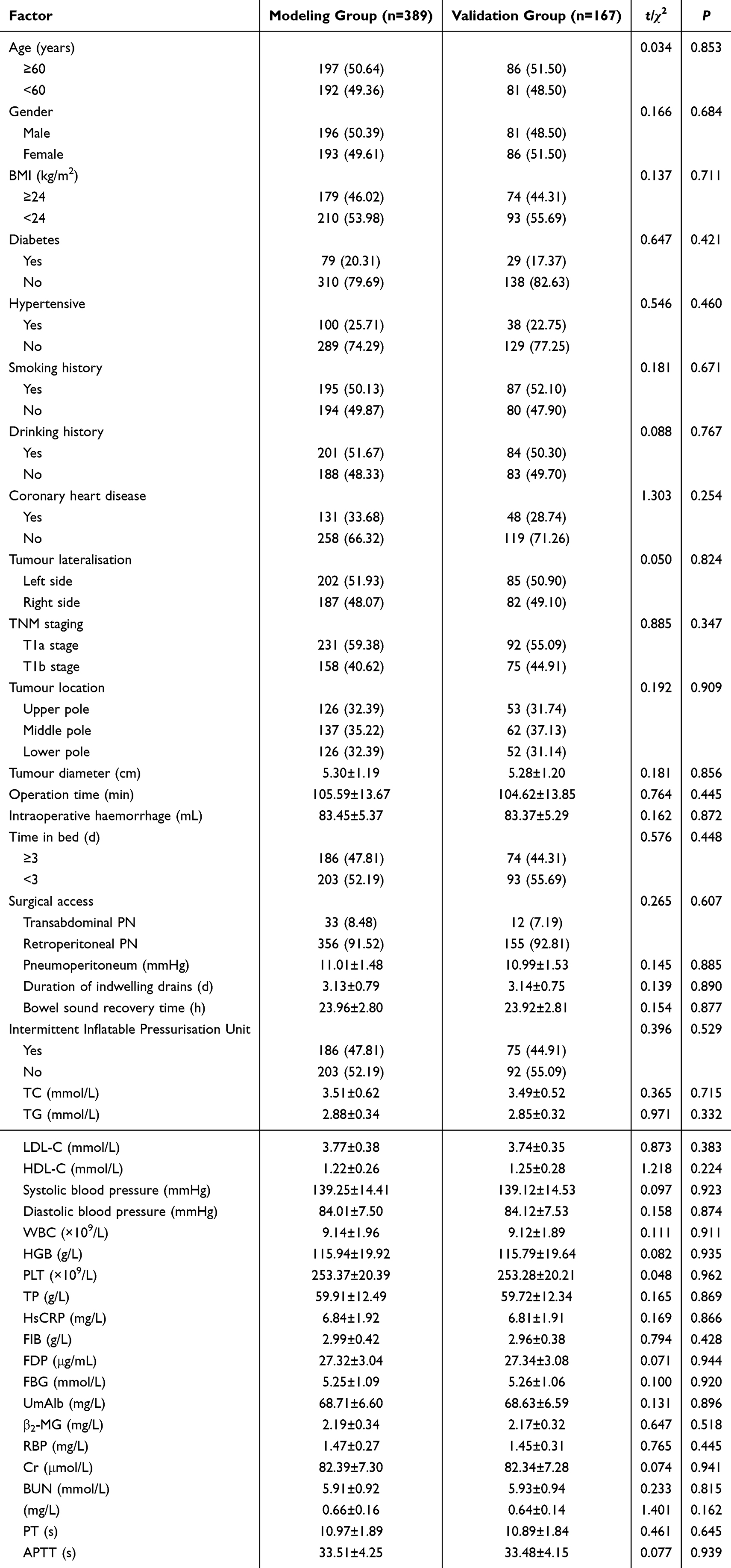 |
Table 1 Comparison of Clinical Data Between the Modeling Group and the Validation Group |
Comparison of Clinical Data Between the DVT Group and the Non-DVT Group
Among the 389 patients in the modeling group, 70 developed DVT, with an incidence rate of 17.99%. The groups showed differences (P < 0.05) in age, operation time, bed rest time, pneumoperitoneum pressure, indwelling drainage time, TC, and D-dimer. There were no significant differences (P > 0.05) in other clinical data between the two groups. Details were shown in Table 2.
 |
Table 2 Comparison of Clinical Data Between DVT and Non-DVT Groups |
Analysis of Influencing Factors for DVT in Patients with RCC After PN
DVT occurrence after PN in RCC patients was used as the dependent variable (yes = 1, no = 0), with independent variables and their coding shown in Table 3. Collinearity diagnostics were performed on seven influencing factors, revealing variance inflation factors (VIF) all less than 10, indicating no multicollinearity or interaction among the variables. Logistic regression (stepwise forward method) indicated that age, operation time, bed rest time, pneumoperitoneum pressure, indwelling drainage time, TC, and D-dimer were risk factors (P < 0.05). Details were shown in Table 4.
 |
Table 3 Assignment Methods of Argument Variables |
 |
Table 4 Multifactorial Analysis of Factors Influencing DVT After PN in RCC Patients |
Construction of a Nomogram Model for DVT in RCC Patients After PN
The nomogram model was constructed using the following equation: P=ex/(1+ex), x=−34.898+0.219×age+0.089×operation time+1.838×bed rest time+0.406×pneumoperitoneum pressure+0.501×indwelling drainage time+1.567×TC+1.177×D-dimer. In this model, the most important influencing factors is TC, followed in order by operation time, D-dimer, pneumoperitoneum pressure, indwelling drainage time, age, and bed rest time. Each indicator corresponds to a specific score, and the total score is the sum of the scores for all indicators. A higher total score indicates a greater probability of developing DVT; for example, when the total score ranges from 220 to 230, the probability of occurrence is 71% to 83%. Details were shown in Figure 2.
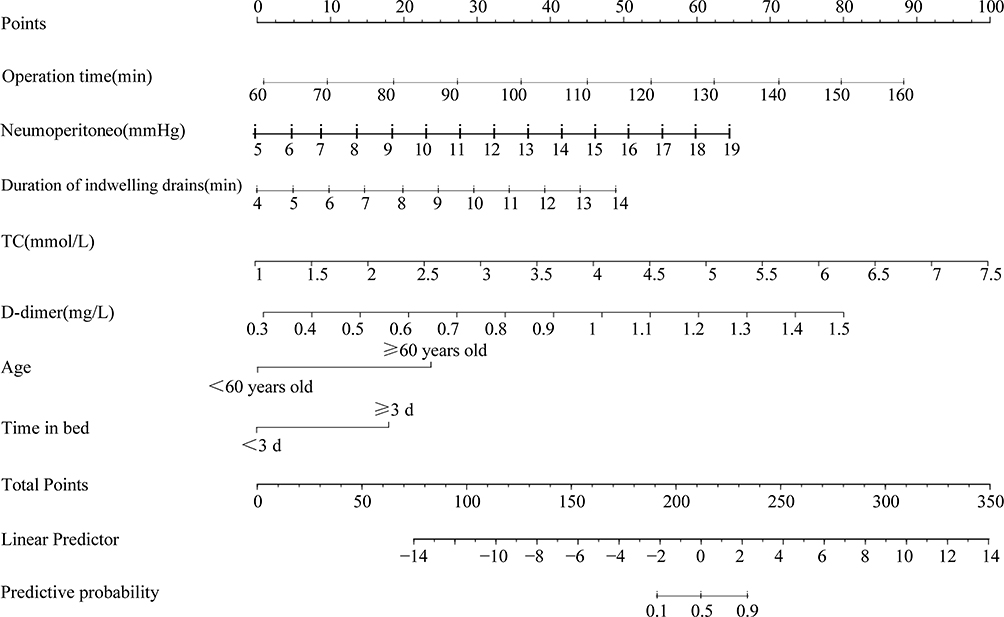 |
Figure 2 The nomogram model for DVT after PN in RCC patients. |
Validation of the Nomogram Model for DVT in RCC Patients After PN
An ROC curve was plotted. The area under the curve (AUC) was 0.889 (95% CI = 0.851–0.927) for the modeling group, and 0.866 (95% CI = 0.801–0.931) for the validation group. Details were shown in Figure 3. The Hosmer-Lemeshow (H-L) test result for the modeling group was χ2 = 7.120 (P = 0.714), and the result for the validation group was χ2 = 7.058 (P = 0.724). Details were shown in Figure 4.
 |
Figure 3 ROC curve (A) ROC curve of modeling group; (B) ROC curve of validation group. |
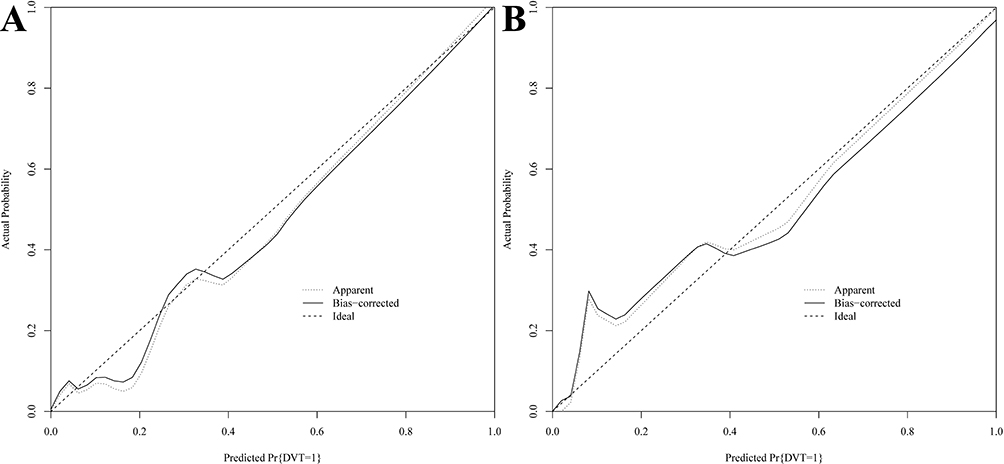 |
Figure 4 Calibration curve (A) Calibration curve of modeling group; (B) Calibration curve of modeling group. |
Curve of the Nomogram Model
According to the DCA curve, when the probability is between 0.08 and 0.96, the nomogram model has a relatively high clinical value in assessing DVT in RCC patients after PN. Details were shown in Figure 5.
 |
Figure 5 DCA curve for the nomogram. |
Discussion
Currently, the pathogenesis of RCC is not fully understood. Its mechanism is relatively complex. Research has shown that the von Hippel-Lindau (VHL) tumor suppressor gene may be involved during tumor onset. When this gene mutates and its function is lost, it leads to an accumulation of downstream hypoxia-inducible factors, causing excessive expression of vascular endothelial growth factor and other factors. By binding to corresponding receptors, these factors increase vascular permeability, thereby promoting cell proliferation and migration and playing a role in the progression of RCC.11,12 In clinical treatment, compared with open surgery, laparoscopic surgery for early-stage RCC involves less trauma. However, the incidence of postoperative deep vein thrombosis (DVT) remains relatively high, severely impacting patient prognosis. DVT mainly occurs when blood abnormally clots in the deep veins, blocking blood vessels and thus affecting surgical outcomes, prolonging hospital stays, and possibly leading to pulmonary embolism.13 This study revealed that among 389 patients, 70 developed DVT (17.99%), indicating a relatively high incidence. It may be because the selected patients were older and had more severe conditions, leading to a higher incidence. Therefore, early identification of the factors influencing DVT after surgery is crucial for improving patient prognosis.
This study found that age is a risk factor for DVT after PN in RCC patients, mainly because older patients experience vascular endothelial aging, which affects the fibrinolytic function of the endothelium and may lead to DVT. In addition, older patients often have underlying conditions. Inflammatory mediators released by these conditions can activate and induce the coagulation cascade, causing endothelial cell death and increasing DVT risk.14,15 Operation time is a risk factor for DVT after PN in RCC patients, mainly because PN is performed under general anesthesia, during which patients are kept in the same position for a prolonged period, and muscle relaxants slow venous blood flow, thus increasing DVT risk. Additionally, muscle relaxants can raise the incidence of hypercapnia, which affects coagulation and further predisposes patients to DVT.16 Bed rest time is a risk factor for DVT after PN in RCC patients. For patients with prolonged bed rest, reduced physical activity leads to loss of the muscle pump effect. Long-term bed rest can decrease venous return from the lower limbs, promote thrombosis formation, and increase the risk of DVT.17 Pneumoperitoneum pressure is a risk factor for DVT after PN in RCC patients. In laparoscopic surgery, pneumoperitoneum pressure typically ranges from 12 to 15 mmHg, whereas the normal physiological range is 2 to 5 mmHg. Higher pneumoperitoneum pressure exerts force on the inferior vena cava, slowing blood flow. When the body is in a hypercoagulable state, endothelial damage occurs, activating platelets and causing their adhesion and release, thereby increasing the risk of DVT.18,19
Indwelling drainage time is a risk factor for DVT after PN in RCC patients because respiratory movements create negative pressure in the thoracic cavity, promoting venous return from the lower limbs. The presence of an indwelling drainage tube increases the risk of infection, and the tube may affect respiratory mechanics and further raise infection risk, thereby promoting thrombosis formation. Additionally, the drainage tube can cause discomfort and affect normal breathing, and prolonged indwelling time increases the risk of DVT.20 Total cholesterol (TC) is a risk factor for DVT after PN in RCC patients. Elevated TC levels indicate that patients are more likely to have chronic diseases, which may induce a hypercoagulable blood state and predispose them to thrombosis. A study has shown that patients who develop DVT after fracture surgery have higher TC levels, which aligns with our findings.21 D-dimer is a risk factor for DVT after PN in RCC patients. D-dimer is a nonspecific marker of thrombosis. Monitoring it can help assess the coagulation state of the body. Elevated D-dimer suggests a possible thrombotic process in the blood. When clots form, coagulation factors in the blood are activated. D-dimer is also a degradation product of fibrin, so an elevated level indicates an abundance of degradation products in the blood, promoting DVT formation.22
The nomogram model can integrate multiple influencing factors into a single statistical model, allowing for relatively accurate prediction of the patient’s condition and demonstrating high clinical utility. In this study, the constructed nomogram yielded an AUC of 0.889 in the modeling group and 0.866 in the validation group, with a good Hosmer-Lemeshow (H-L) goodness of fit test, indicating satisfactory predictive capability. The decision curve analysis (DCA) showed that when the probability range was 0.08–0.96, the nomogram model for assessing DVT after PN in RCC patients had good clinical applicability, aiding clinicians in targeted interventions.
In summary, age, operation time, bed rest time, pneumoperitoneum pressure, indwelling drainage time, TC, and D-dimer are factors influencing DVT after PN in patients with RCC. The nomogram model constructed based on this can effectively predict the risk of postoperative DVT in patients and assist clinicians in implementing targeted prevention based on relevant factors. This study is a retrospective single-center investigation with selection bias, a small sample size, and a lack of independent external validation. Additionally, there is heterogeneity among the patient population, limiting the generalizability of the results. Subsequent multicenter prospective studies with expanded samples will be conducted for further validation.
Data Sharing Statement
The original contributions presented in the study are included in the article.
Ethics Approval
This study involving human participants was in accordance with the ethical standards of the Medical Ethics Committee of The Central Hospital of Yongzhou (No.2025032501) and with the 1964 Helsinki Declaration. The need for informed consent was waived by the Medical Ethics Committee of The Central Hospital of Yongzhou.
Funding
Guiding Science and Technology Plan Projects in Yongzhou City in 2023 (2023YZ030).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Motzer RJ, Jonasch E, Agarwal N, et al. Kidney cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2022;20(1):71–12. doi:10.6004/jnccn.2022.0001
2. Dahman L, Gauthier V, Camier A, et al. Air pollution and kidney cancer risk: a systematic review and meta-analysis. J Nephrol. 2024;37(7):1779–1790. doi:10.1007/s40620-024-01984-x
3. Okhawere KE, Milky G, Razdan S, et al. One-year healthcare costs after robotic-assisted and laparoscopic partial and radical nephrectomy: a cohort study. BMC Health Serv Res. 2023;23(1):1099. doi:10.1186/s12913-023-10111-8
4. Simforoosh N, Simforoosh F, Dadpour M, et al. Oncologic outcomes following positive surgical margins in patients who underwent open versus laparoscopic partial nephrectomy. Urol J. 2022;20(1):17–21. doi:10.22037/uj.v18i.6858
5. Chen Y, Zhao J, Zhang Z, et al. Construction and validation of a nomogram for predicting the risk of deep vein thrombosis in hepatocellular carcinoma patients after laparoscopic hepatectomy: a retrospective study. J Hepatocell Carcinoma. 2021;8:783–794. doi:10.2147/JHC.S311970
6. Wu L, Cheng B. A nomogram to predict postoperative deep vein thrombosis in patients with femoral fracture: a retrospective study. J Orthop Surg Res. 2023;18(1):463. doi:10.1186/s13018-023-03931-1
7. Zhou H, Jin Y, Chen G, et al. Predictive modeling of lower extreme deep vein thrombosis following radical gastrectomy for gastric cancer: based on multiple machine learning methods. Sci Rep. 2024;14(1):15711. doi:10.1038/s41598-024-66754-y
8. Ljungberg B, Albiges L, Abu-Ghanem Y, et al. European association of urology guidelines on renal cell carcinoma: the 2022 update. Eur Urol. 2022;82(4):399–410. doi:10.1016/j.eururo.2022.03.006
9. Sartori M, Gabrielli F, Favaretto E, et al. Proximal and isolated distal deep vein thrombosis and wells score accuracy in hospitalized patients. Intern Emerg Med. 2019;14(6):941–947. doi:10.1007/s11739-019-02066-8
10. Zhang S, Chu W, Wang H, et al. Evaluation of stability of deep venous thrombosis of the lower extremities using doppler ultrasound. J Int Med Res. 2020;48(8):300060520942098. doi:10.1177/0300060520942098
11. Sekar H, Krishnamoorthy S, Kumaresan N, et al. Clinicopathological comparison of VHL expression as a prognostic tumor marker in renal cell carcinoma: a single center experience. Niger J Clin Pract. 2021;24(4):614–620. doi:10.4103/njcp.njcp_57_20
12. Liu F, Wen T, Tang Q, et al. Impact of vascular endothelial growth factor gene polymorphisms and their interactions with environmental factors on susceptibility to renal cell carcinoma. Nephron. 2020;144(5):255–260. doi:10.1159/000505817
13. Xiang L, Jin S, Yu Y, et al. Risk of venous thromboembolism in patients undergoing gastric cancer surgery: a systematic review and meta-analysis. BMC Cancer. 2023;23(1):933. doi:10.1186/s12885-023-11424-x
14. Tang G, Qi L, Sun Z, et al. Evaluation and analysis of incidence and risk factors of lower extremity venous thrombosis after urologic surgeries: a prospective two-center cohort study using LASSO-logistic regression. Int J Surg. 2021;89:105948. doi:10.1016/j.ijsu.2021.105948
15. Wei Q, Wei Z-Q, Jing C-Q, et al. Incidence, prevention, risk factors, and prediction of venous thromboembolism in Chinese patients after colorectal cancer surgery: a prospective, multicenter cohort study. Int J Surg. 2023;109(10):3003–3012. doi:10.1097/JS9.0000000000000553
16. Amaral FC, Baptista-Silva JC, Nakano LC, et al. Pharmacological interventions for preventing venous thromboembolism in people undergoing bariatric surgery. Cochrane Database Syst Rev. 2022;11(11):CD013683. doi:10.1002/14651858.CD013683.pub2
17. Bhatt M, Braun C, Patel P, et al. Diagnosis of deep vein thrombosis of the lower extremity: a systematic review and meta-analysis of test accuracy. Blood Adv. 2020;4(7):1250–1264. doi:10.1182/bloodadvances.2019000960
18. Tian Q, Li M. Risk factors of deep vein thrombosis of lower extremity in patients undergone gynecological laparoscopic surgery: what should we care. BMC Womens Health. 2021;21(1):130. doi:10.1186/s12905-021-01276-7
19. Liu C, Han Z, Zhang N, et al. Laparoscopic sleeve gastrectomy affects coagulation system of obese patients. Obes Surg. 2020;30(10):3989–3996. doi:10.1007/s11695-020-04769-w
20. Kermansaravi M, Kassir R, Valizadeh R, et al. Management of leaks following one-anastomosis gastric bypass: an updated systematic review and meta-analysis of 44 318 patients. Int J Surg. 2023;109(5):1497–1508. doi:10.1097/JS9.0000000000000346
21. Zixuan L, Chen W, Li Y, et al. Incidence of deep venous thrombosis (DVT) of the lower extremity in patients undergoing surgeries for ankle fractures. J Orthop Surg Res. 2020;15(1):294. doi:10.1186/s13018-020-01809-0
22. Chai Y-N, Luo M, Liang W-J, et al. The safety and effectiveness of salvianolate in preventing perioperative venous thromboembolism in China: a PRISMA-compliant meta-analysis based on RCTs. Medicine. 2021;100(18):e25639. doi:10.1097/MD.0000000000025639
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Development of Risk Prediction Model for Muscular Calf Vein Thrombosis with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Hu X, Li X, Xu H, Zheng W, Wang J, Wang W, Li S, Zhang N, Wang Y, Han K
International Journal of General Medicine 2022, 15:6549-6560
Published Date: 10 August 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023