Back to Journals » Infection and Drug Resistance » Volume 19
Development and Internal Validation of a Nomogram Model to Predict Invasive Pulmonary Aspergillosis Occurrence Risk in ICU Patients with Sepsis
Authors Li H, Liang Y ![]() , Xiao W, Zheng Y, Hua T, Yang M
, Xiao W, Zheng Y, Hua T, Yang M
Received 16 February 2026
Accepted for publication 19 May 2026
Published 25 May 2026 Volume 2026:19 603823
DOI https://doi.org/10.2147/IDR.S603823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Hui Li,1,2 Yao Liang,1,2 Wenyan Xiao,1,2 Yao Zheng,1,2 Tianfeng Hua,1,2 Min Yang1,2
1The Second Department of Critical Care Medicine, The Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China; 2The Laboratory of Cardiopulmonary Resuscitation and Critical Care Medicine, the Second Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China
Correspondence: Min Yang, Email [email protected]
Background: Sepsis is characterized by immune dysregulation and increased susceptibility to secondary infections. Invasive pulmonary aspergillosis (IPA) is an important complication in intensive care unit (ICU) patients with sepsis and is associated with poor outcomes. Identifying its predictors and developing a prediction model may facilitate early risk assessment and identification of high-risk patients.
Methods: A single-centre retrospective cohort of 574 adult ICU patients with sepsis (January 2020–December 2024) was randomly divided into a training set (n=459) and a validation set (n=115) in an 8:2 ratio. IPA was diagnosed according to international consensus criteria. In the training set, candidate predictors were screened by least absolute shrinkage and selection operator (LASSO) regression, followed by multivariable logistic regression. A nomogram-based prediction model was developed and internally validated in the validation set. Model discrimination, calibration, and clinical utility were assessed using the area under the receiver operating characteristic curve (ROC), calibration curves, and decision curve analysis (DCA), respectively.
Results: Among 574 ICU patients with sepsis, 86 (14.98%) developed IPA. LASSO followed by multivariable logistic regression showed that smoking history, corticosteroid therapy, coexisting SFTS or COVID-19, duration of mechanical ventilation, NRS 2002 score, and SOFA score were independently associated with IPA. The area under the ROC curve (AUC) for the training set was 0.883 (95% CI 0.842– 0.924), and for the validation set, it was 0.844 (95% CI 0.766– 0.921). The nomogram constructed from these variables suggested good discrimination and calibration in both the training and validation cohorts. DCA indicated a net clinical benefit across clinically relevant threshold probabilities.
Conclusion: We developed and internally validated a nomogram for predicting secondary IPA occurrence risk in ICU patients with sepsis. The inclusion of NRS 2002 suggests that nutritional risk may contribute to IPA occurrence risk. External validation is warranted before broader clinical application.
Keywords: sepsis, IPA, ICU, nomogram, prediction model
Introduction
Sepsis constitutes a major global disease burden and remains one of the leading causes of death in intensive care unit (ICU).1 Older adults account for a substantial proportion of sepsis cases. Given the ongoing population aging worldwide, the incidence of sepsis is expected to rise further, making it an increasingly serious public health challenge.2 As understanding of sepsis pathophysiology has advanced, a dysregulated host response to infection is now recognized as a central mechanism driving disease pathogenesis and progression.3,4 In particular, sepsis-induced immune dysfunction increases susceptibility to life-threatening secondary infections, posing major challenges to clinical management.5–8
Aspergillus species are ubiquitous saprophytic fungi found in soil, decaying vegetation, and indoor/outdoor environments, and their conidia readily aerosolize, resulting in frequent exposure in both community and healthcare settings.9 Whether inhaled conidia lead to outcomes ranging from airway colonization and allergic manifestations to invasive aspergillosis depends largely on the host’s pulmonary and systemic immune status.10 A. fumigatus is the species most commonly implicated in invasive infection, followed by A. flavus, A. niger, and A. terreus. In hospitals, especially ICU setting, indoor air and environmental rervoirs are recognized sources of Aspergillus exposure; Aspergillus colonization of air-conditioning and ventilation systems may further contribute to spore dissemination.11 In addition, some Aspergillus species can produce mycotoxins, which may further underscore the complexity of environmental exposure in healthcare settings.
Against this exposure background, critically ill patients with sepsis may be particularly vulnerable to progression from exposure to infection. Respiratory failure and the need for mechanical ventilation are common in ICU patients with sepsis, and the development of invasive pulmonary aspergillosis (IPA) can substantially complicate management, increases healthcare resource utilization, and worsens clinical outcomes. IPA may also progress rapidly and cause abrupt clinical deterioration; thus, early recognition is critical to improving outcomes.12 However, early manifestations are often nonspecific and can be obscured by underlying conditions. Typical radiologic features and microbiological evidence are frequently unavailable or delayed in ICU practice, and distinguishing airway colonization from invasive infection can be difficult. In addition, the emerging context of viral-associated aspergillosis, such as COVID-19-associated pulmonary aspergillosis (CAPA), may further complicate early recognition. Clinical management is therefore shifting from passive early diagnosis to proactive risk prediction and preemptive intervention.13,14 To date, most existing risk prediction studies for IPA have been conducted in mixed ICU populations or certain subgroups, such as patients with acute exacerbation of chronic obstructive pulmonary disease (COPD).15,16 However, to the best of our knowledge, little attention has been paid to the risk of IPA specifically in ICU patients with sepsis, and no dedicated prediction model has yet been reported for this population. A sepsis-specific approach may be warranted because sepsis-associated immune dysfunction, together with the high burden of organ failure and treatment-related exposures, may shape a distinct susceptibility profile for IPA. Therefore, in this context, we aim to develop and validate a risk prediction model for IPA in ICU patients with sepsis using routinely available clinical data.
To achieve this, we systematically collected clinical, laboratory, radiologic, and microbiological data from ICU patients with sepsis. The least absolute shrinkage and selection operator (LASSO) regression was applied to identify predictors significantly associated with IPA, and a nomogram-based risk prediction model was subsequently developed and internally validated. This model may serve as a decision-support tool for early identification of high-risk patients and facilitate timely implementation of individualized monitoring and preemptive therapeutic interventions.
Methods
Research Patients
This retrospective cohort study included adult patients with sepsis admitted to the ICU of the Second Affiliated Hospital of Anhui Medical University between January 2020 and December 2024. Inclusion criteria were: (1) sepsis diagnosed according to the Sepsis 3.0 international consensus criteria,17 and (2) age ≥18 years. Exclusion criteria were: (1) ICU length of stay <48 hours; (2) age <18 years; (3) diagnosis of IPA prior to ICU admission (proven or probable); (4) Aspergillus colonization; (5) pregnancy; (6) missing key predictor or outcome data; and (7) repeat ICU admissions (for patients with multiple ICU admissions, only the first ICU admission was included) (Figure 1). In this study, Aspergillus colonization refers to isolation of Aspergillus in lower respiratory tract samples without any symptom or new pulmonary infiltrate.
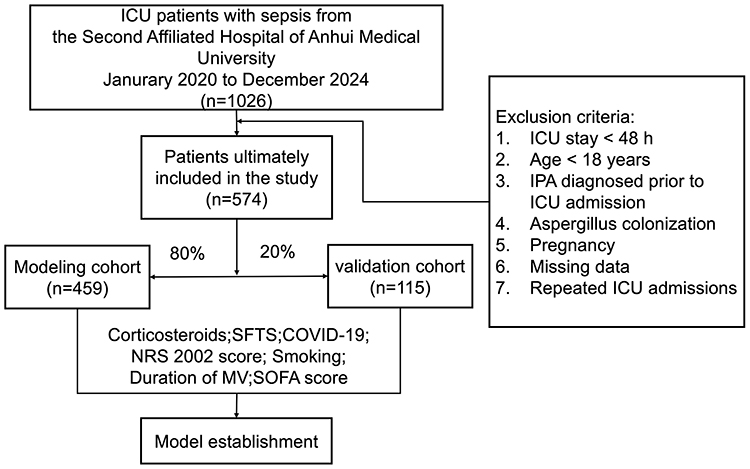 |
Figure 1 Flowchart of patients’ enrollment. |
The outcome of this study was the occurrence of IPA during the ICU stay. IPA was diagnosed and classified primarily according to the 2024 FUNDICU consensus definitions for invasive fungal diseases in critically ill adults, with the 2020 EORTC/MSGERC updated definitions referenced where applicable (particularly for host factors).18,19 Given the limited feasibility of histopathological confirmation in critically ill patients, IPA cases were classified as probable IPA using an integrated criterion set. A case required at least one compatible clinical sign and symptom, one host factor, one clinical criterion, and one mycological criterion, as defined below. (a) Compatible clinical signs and symptoms. Persistent fever (≥3 days) despite appropriate antibacterial therapy, or recurrent fever occurring≥48 hours after defervescence following antibiotic discontinuation without another clear explanation. In addition, at least one of the following respiratory symptoms/signs was required: pleuritic chest pain, pleural friction rub, dyspnea, hemoptysis; or progressive respiratory failure despite appropriate antibacterial therapy and adequate respiratory support. (b) Host factors. An underlying condition or exposure known to be associated with increased IPA risk, including but not limited to: prolonged systemic corticosteroid therapy (typically≥3 weeks; prednisone-equivalent dose≥0.3 mg/kg/day), other immunosuppressive agents (eg., tumor necrosis factor-α antagonists or calcineurin inhibitors), acute respiratory distress syndrome (ARDS), moderate-to-severe COPD, solid-organ or hematopoietic stem cell transplantation, hematologic malignancy, or prolonged neutropenia (absolute neutrophil count<0.5×109/L for>10 days). (c) Clinical criteria. Chest computed tomography (CT) findings compatible with invasive fungal infection, including pulmonary nodules (with or without a halo sign), consolidation, cavitation (after excluding non-infectious causes), or wedge-shaped infarction. Alternatively, tracheobronchial involvement was considered present when bronchoscopy demonstrated suggestive endobronchial lesions (eg., ulceration, pseudomembrane, nodules, plaques, or eschar). (d) Mycological criteria. At least one of the following: serum galactomannan (GM) optical density index>0.5; bronchoalveolar lavage fluid (BALF) GM optical density index≥1.0, positive Aspergillus polymerase chain reaction (PCR) from a qualified respiratory specimen (sputum, BALF, bronchial brushing, or tracheal aspirate); or culture isolation of Aspergillus species from a qualified respiratory specimen. IPA was diagnosed in routine clinical practice by ICU physicians. During data collection, the diagnosis was independently and blindly re-adjudicated by a senior physician with expertise in critical care and infectious diseases; discrepant assessments were resolved by a supervising senior physician. Patients were categorized into an IPA group and a non-IPA group according to whether IPA occurred. In addition, the overall cohort was randomly split into a training set (n = 459) and a validation set (n = 115) at an 8:2 ratio for model development and internal validation.
This study was approved by the institutional review board of The Second Affiliated Hospital of Anhui Medical University (Approval No. YX2025-055). Given the retrospective observational design and the use of de-identified data, the requirement for informed consent was waived by the ethics committee. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Sample Size Calculation
Modeling principles suggest that the sample size should be at least 10–20 times the number of candidate predictors to improve model stability and reduce the risk of overfitting. In this study, 42 variables were considered for model development. The modeling cohort included 574 patients, exceeding the recommended minimum sample size. In addition, dimensionality reduction and variable selection were performed before final model construction to further support statistical power and model robustness.
Data Collection
Clinical data for patients with sepsis admitted to the ICU were reviewed and extracted from the hospital electronic medical record system, including sociodemographic characteristics, comorbidities, laboratory tests, severity scores, supportive care, and length of stay. Two investigators independently collected data using a standardized case report form and performed cross-checking; discrepancies were adjudicated by a third investigator. Based on a review of the literature on risk factors for IPA, the collected variables mainly included as follows. General characteristics and comorbidities: age, sex, smoking history, hospital length of stay (LOS), ICU length of stay, diabetes, hypertension, chronic lung disease, chronic liver disease, Severe Fever with Thrombocytopenia Syndrome (SFTS), and Coronavirus Disease 2019 (COVID-19). Severity and supportive care at ICU admission: Acute Physiology and Chronic Health Evaluation II (APACHE II), Sequential Organ Failure Assessment (SOFA), Nutritional Risk Screening 2002 (NRS 2002), multiple organ dysfunction syndrome (MODS), mechanical ventilation, and renal replacement therapy. Laboratory variables for analysis included blood-related variables (white blood cell count, hemoglobin, platelet count, neutrophil count, lymphocyte count), liver-related variables (alanine aminotransferase, and aspartate aminotransferase, total bilirubin, lactate dehydrogenase), kidney-related variables (creatinine, blood urea nitrogen),coagulation-related variables (prothrombin time, activated partial thromboplastin time, fibrinogen, D-Dimer), inflammatory-related variables (c-reactive protein, procalcitonin, c-reactive protein albumin ratio), electrolyte indicators (iron), and arterial blood gas analysis, including arterial partial pressure of oxygen (PaO2)/fraction of inspired oxygen (FiO2), arterial partial pressure of carbon dioxide (PaCO2) and lactate. A unified data management and quality-control workflow was implemented throughout the study to ensure data accuracy and traceability. Mycological findings, including serum GM, BALF GM, lower respiratory tract culture results and antifungal treatment data, were also collected. Detailed variable definitions are provided in Table S1.
Statistical Analysis
All statistical analyses were performed using R software (version 4.4.1) and SPSS (version 25.0). Normally distributed continuous variables are presented as mean  standard deviation (SD), and between-group comparisons were conducted using the independent-samples t test. Non-normally distributed continuous variables are described as medians with interquartile range (IQR) and were compared using the Mann–Whitney U-test. Categorical variables were presented as frequencies and proportions, the Chi-square (
standard deviation (SD), and between-group comparisons were conducted using the independent-samples t test. Non-normally distributed continuous variables are described as medians with interquartile range (IQR) and were compared using the Mann–Whitney U-test. Categorical variables were presented as frequencies and proportions, the Chi-square ( ) test or Fisher’s exact test were used for analyzing when appropriate. Among the 42 variables assessed, 38 had no missing data. Missingness was observed for three numeric variables: CRP (12/574, 2.09%), PCT (12/574, 2.09%), and LDH (29/574, 5.05%). Given the low proportion of missing data, missing values were imputed using median imputation for each variable. All patients were divided into a training cohort and a validation cohort at an 8:2 ratio using stratified random sampling. Before model development, variable distributions and baseline comparability between the two cohorts were assessed. Model development was performed in three steps. First, in the training cohort, least absolute shrinkage and selection operator (LASSO) regression was used for variable selection. The optimal penalty parameter (λ) was determined by 10-fold cross-validation, and predictors with non-zero coefficients were retained. Second, the retained predictors were entered into a multivariable logistic regression model, and maximum likelihood estimation was used to identify variables independently associated with IPA occurrence risk, from which the final prediction model was established. Third, a nomogram was constructed based on the final model to provide individualized visual risk estimation. Model performance was evaluated in terms of discrimination, calibration, and clinical utility. Discrimination was assessed by the area under the receiver operating characteristic curve (AUC). Calibration was evaluated using calibration plots to examine agreement between predicted probabilities and observed event rates. Clinical utility was assessed by decision curve analysis (DCA), which quantified net benefit across a range of threshold probabilities. A p value <0.05 was considered to indicate statistical significance.
) test or Fisher’s exact test were used for analyzing when appropriate. Among the 42 variables assessed, 38 had no missing data. Missingness was observed for three numeric variables: CRP (12/574, 2.09%), PCT (12/574, 2.09%), and LDH (29/574, 5.05%). Given the low proportion of missing data, missing values were imputed using median imputation for each variable. All patients were divided into a training cohort and a validation cohort at an 8:2 ratio using stratified random sampling. Before model development, variable distributions and baseline comparability between the two cohorts were assessed. Model development was performed in three steps. First, in the training cohort, least absolute shrinkage and selection operator (LASSO) regression was used for variable selection. The optimal penalty parameter (λ) was determined by 10-fold cross-validation, and predictors with non-zero coefficients were retained. Second, the retained predictors were entered into a multivariable logistic regression model, and maximum likelihood estimation was used to identify variables independently associated with IPA occurrence risk, from which the final prediction model was established. Third, a nomogram was constructed based on the final model to provide individualized visual risk estimation. Model performance was evaluated in terms of discrimination, calibration, and clinical utility. Discrimination was assessed by the area under the receiver operating characteristic curve (AUC). Calibration was evaluated using calibration plots to examine agreement between predicted probabilities and observed event rates. Clinical utility was assessed by decision curve analysis (DCA), which quantified net benefit across a range of threshold probabilities. A p value <0.05 was considered to indicate statistical significance.
Results
Comparison of Clinical Characteristics Between the Training and Validation Cohorts
Among 574 ICU patients with sepsis included in this study, 14.98% (86/574) developed IPA. As shown in Table S2, there were no statistically significant differences in baseline clinical characteristics between the training and validation cohorts (p > 0.05), indicating good comparability between the two groups.
Mycological Findings
Of the IPA patients, 60.47% (52/86) had a positive serum GM, with a median index of 1.07 (IQR, 0.62–3.98) for the positive results. BALF GM testing was performed in 34 patients (39.53%); 33 patients were positive (97.06% of those tested), with a median index among positives of 3.36 (IQR, 1.91–7.92). Among all IPA patients, 44.19% (38/86) had culture positive for Aspergillus species in respiratory specimens. Positive cultures recovered A. fumigatus (n=19), A. flavus (n=17), A. niger (n=4), and A. terreus (n=1). Co-isolation occurred in 3 patients (3.49%): A. fumigatus plus A. niger in 2 patients and A. flavus plus A. niger in 1 patient. Seven patients (8.14%) had concordant positivity for serum GM, BALF GM, and respiratory specimen culture. Twenty patients (23.26%) were positive for both serum GM and culture, nine patients (10.47%) for both BALF GM and culture, and eight patients (9.30%) for both serum GM and BALF GM. Regarding antifungal management, 8 patients (9.30%) received no antifungal therapy, 50 patients (58.14%) received monotherapy, and 28 patients (32.56%) received combination antifungal therapy.
Baseline Comparison Between IPA and Non-IPA Patients in the Training Cohort
In the training cohort, comparison of baseline characteristics between patients with and without IPA showed that patients in the IPA group were older and had longer ICU and overall hospital stays. Regarding comorbidities, the proportions of SFTS, COVID-19, and MODS were higher in the IPA group.
Comparisons of laboratory and physiologic parameters showed that the IPA group had significantly lower white blood cell count, neutrophil count, platelet count, C-reactive protein, procalcitonin, prothrombin time, C-reactive protein-to-albumin ratio (CAR), and oxygenation index, whereas serum iron, lactate dehydrogenase, total bilirubin, and PaCO2 were higher.
In addition, the IPA group had higher APACHE II, SOFA, and NRS 2002 scores than the non-IPA group. With respect to treatment, patients in the IPA group were more likely to receive corticosteroid therapy, mechanical ventilation, and continuous renal replacement therapy (CRRT), and had a longer duration of mechanical ventilation (Table 1).
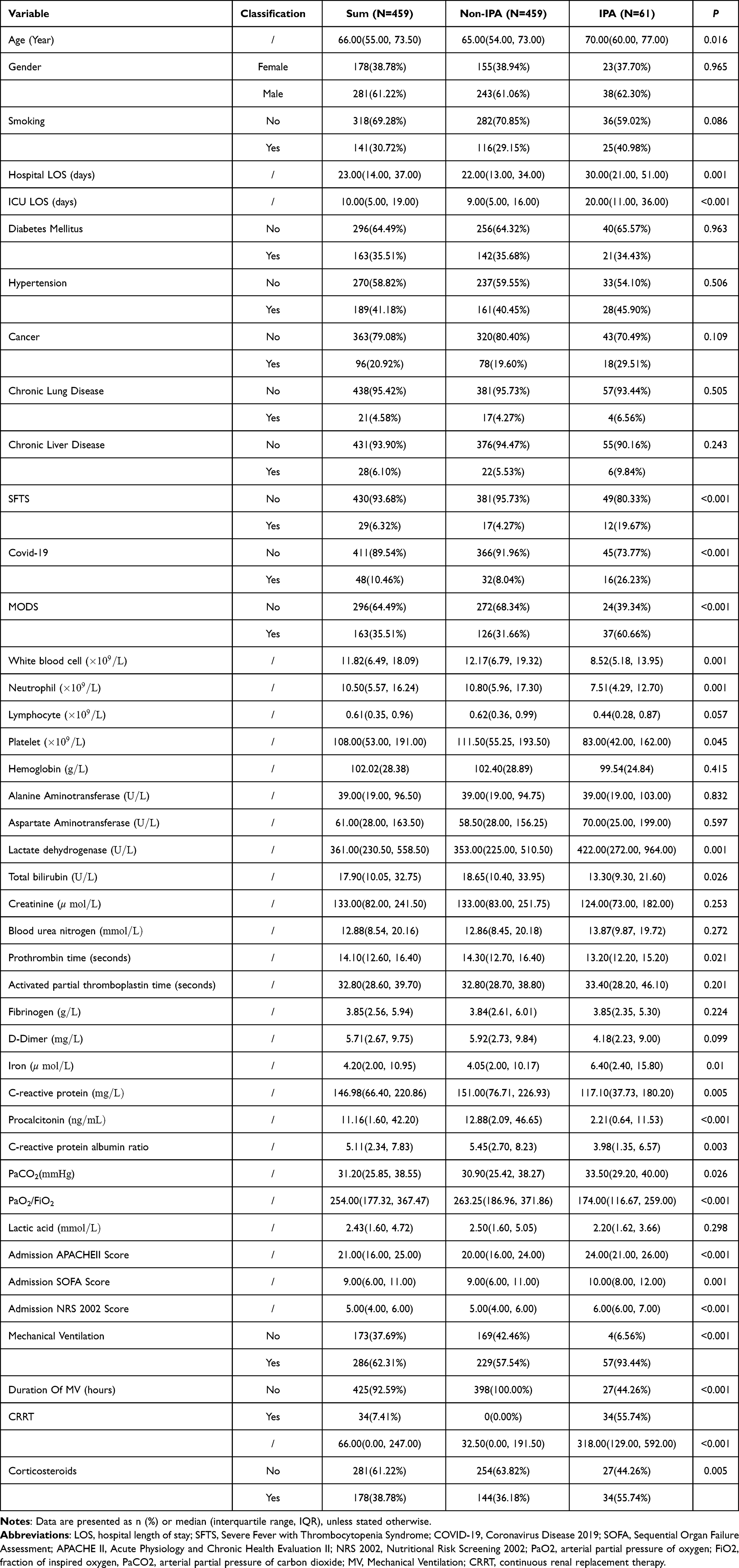 |
Table 1 Baseline Characteristics of Patients with and without IPA in the Training Cohort |
Development of a Nomogram for Predicting IPA Occurrence Risk in ICU Patients with Sepsis
42 candidate predictors were first screened using LASSO regression. At the selected λ, 16 predictors with non-zero coefficients were retained (Figure 2A and B). These predictors were further analyzed using multivariable logistic regression. In multivariable logistic regression, SFTS (OR:27.305; 95% CI:8.782–84.899, p <0.001), COVID-19 (OR: 4.551; 95% CI: 1.854–11.174, p <0.001), NRS-2002 score at ICU admission (OR: 1.698; 95% CI: 1.367–2.111, p=0.001), smoking history (OR: 2.552; 95% CI: 1.264–5.150, p=0.009), duration of mechanical ventilation (OR: 1.002; 95% CI: 1.001–1.003, p<0.001; per 1-hour increase), SOFA score at ICU admission (OR: 1.135; 95% CI: 1.012–1.274, p=0.031), and corticosteroid therapy (OR: 3.278; 95% CI: 1.511–7.107, p=0.003) were independently associated with IPA occurrence risk in ICU patients with sepsis (Table 2). A nomogram was then developed based on these predictors. The model provides an individualized predicted probability for each patient according to their predictor profile, this probability is derived by summing the points assigned to each predictor and transforming the total score through the model (Figure 3).
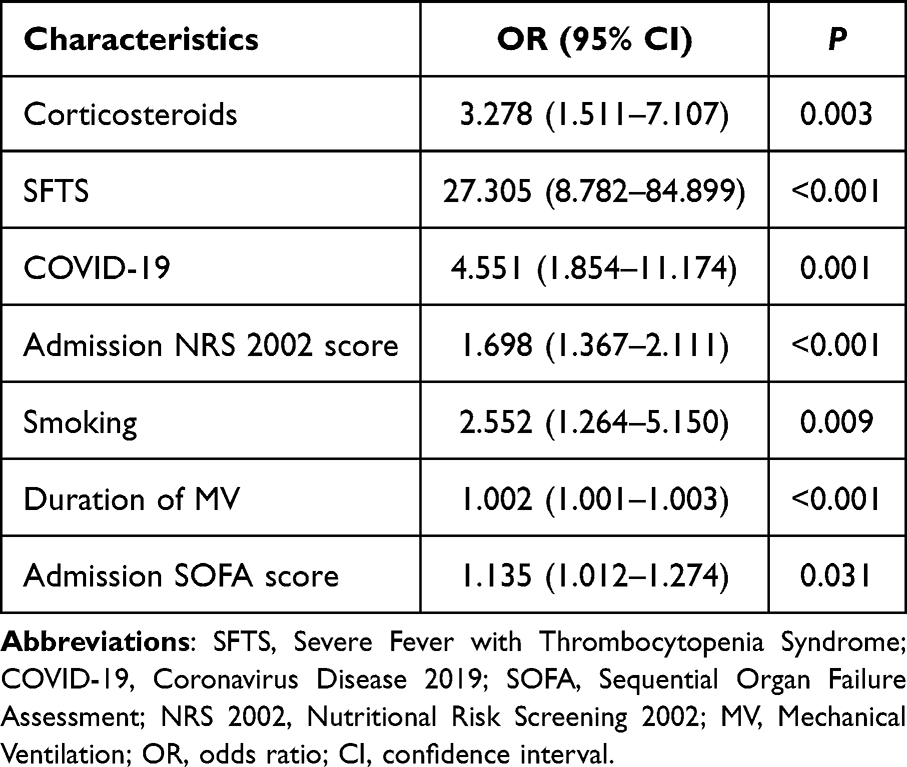 |
Table 2 Multivariable Logistic Regression Analysis of Factors Independently Associated with IPA Occurrence Risk in Patients with Sepsis |
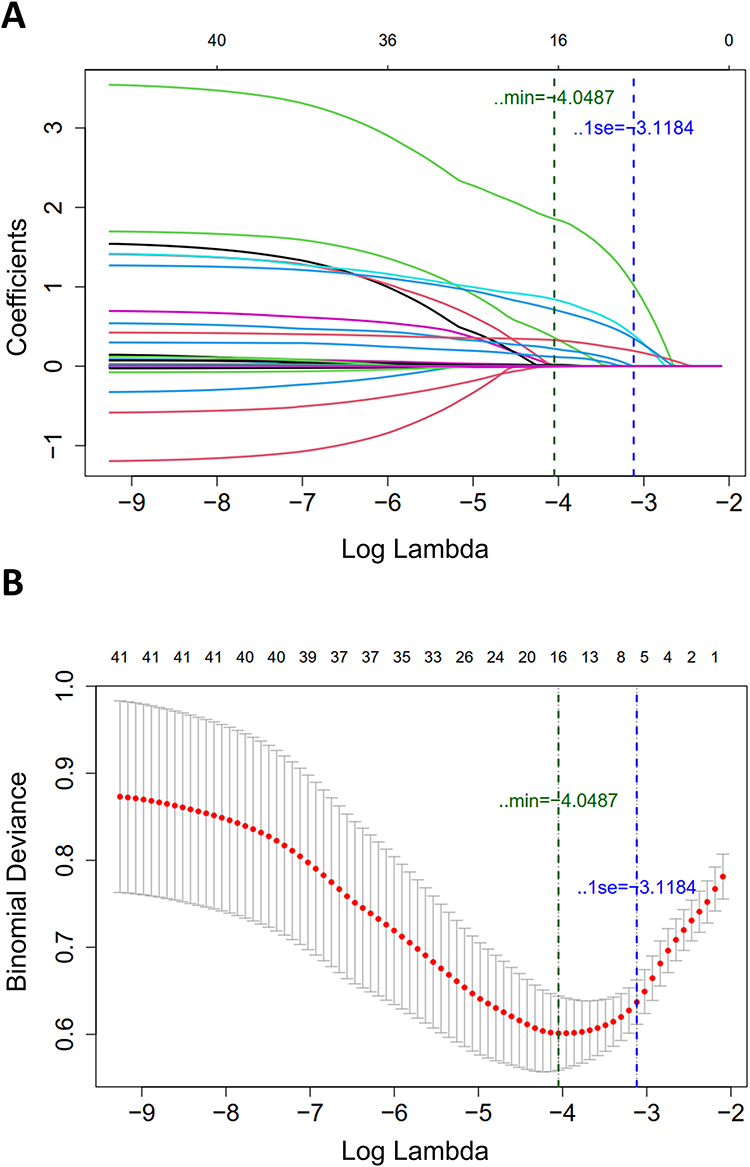 |
Figure 2 Identification of The Predictors of IPA by LASSO Regression. (A) LASSO coefficient profiles of the candidate predictors. Each colored curve represents the coefficient trajectory of one candidate predictor as the penalty parameter λ changes. (B) Cross-validation curve for LASSO regression. The red dots represent the mean cross-validated binomial deviance, and the gray vertical bars indicate the corresponding standard errors. The two vertical dashed lines indicate the values of λ at λmin and λ1se, respectively. Abbreviations: IPA, Invasive pulmonary aspergillosis; LASSO, least absolute shrinkage and selection operator. |
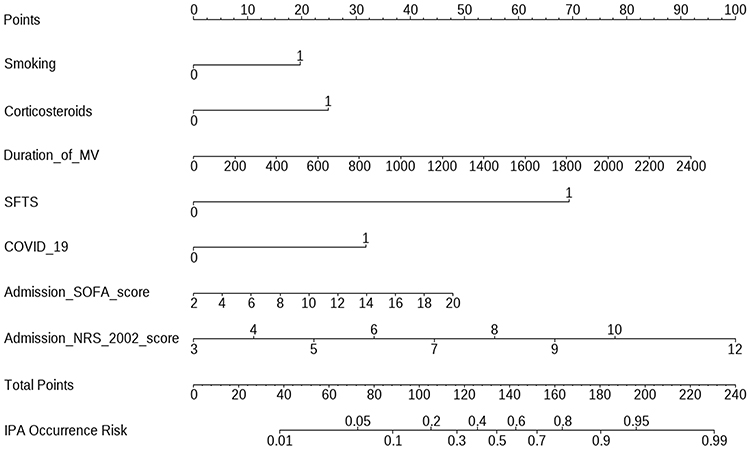 |
Figure 3 Nomogram for predicting IPA occurrence risk in ICU patients with sepsis. Abbreviations: IPA, Invasive pulmonary aspergillosis; ICU, intensive care unit. |
Model discrimination was evaluated using receiver operating characteristic (ROC) curves and the AUC (Figure 4A and B). The AUCs in the training and validation cohorts were 0.883 and 0.844, respectively (95% CI: 0.842–0.924, 0.766–0.921). Model calibration was assessed by calibration curves in both cohorts, comparing predicted probabilities with observed event rates. The model showed good calibration, with close agreement between predicted risk and observed outcomes (Figure 5A and B). The Hosmer-Lemeshow goodness-of-fit test revealed no statistically significant difference between the model’s predictions and actual outcomes in the training group (P=0.138). Clinical utility was further evaluated by DCA. The higher clinical utility can be obtained when the probability is 0.01–0.90 (Figure 6A and B).
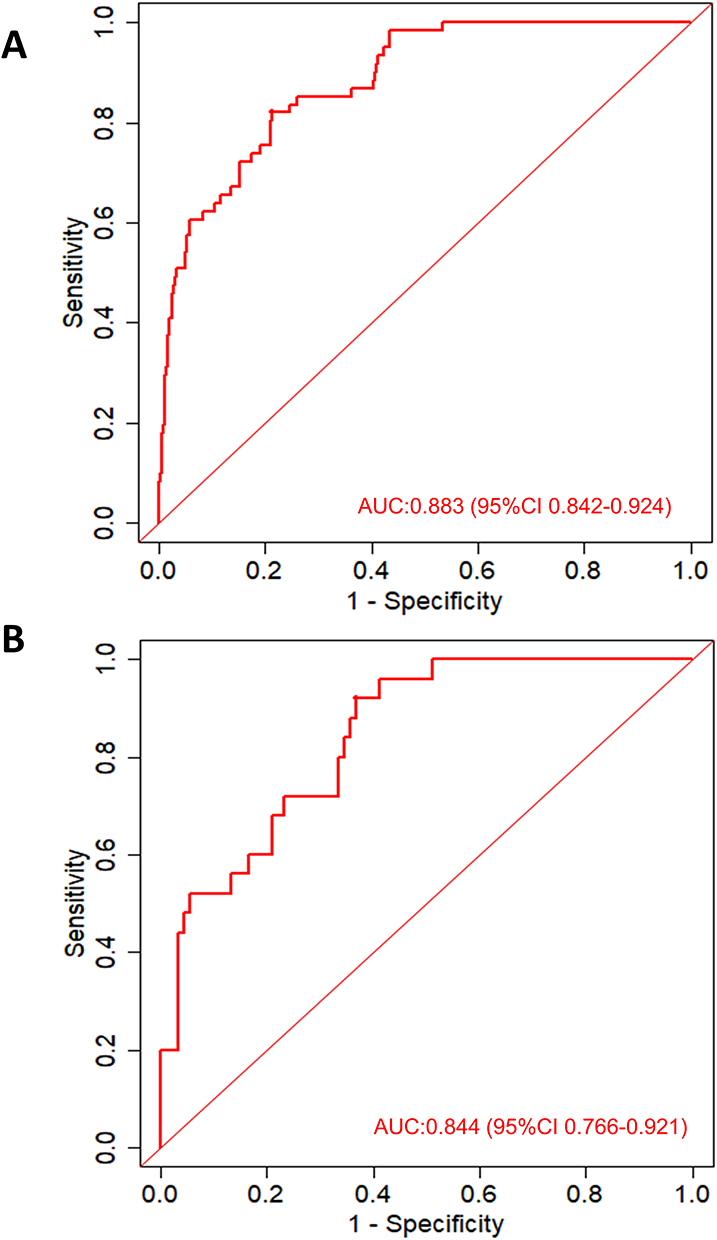 |
Figure 4 ROC Curves The ROC curves of the nomogram in the training cohort (A) and the validation cohort (B). Abbreviations: ROC, receiver operating characteristic curve; AUC, area under the receiver operating characteristic curve. |
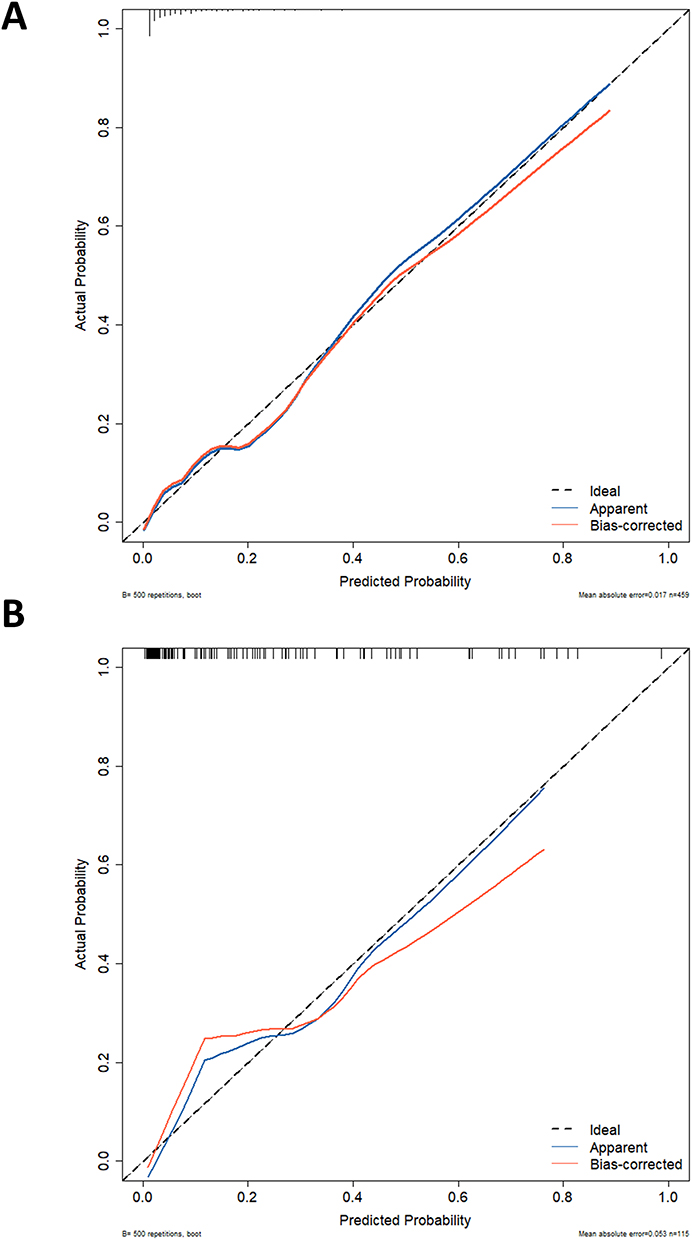 |
Figure 5 Calibration plots of the nomogram in the training cohort (A) and the validation cohort (B). |
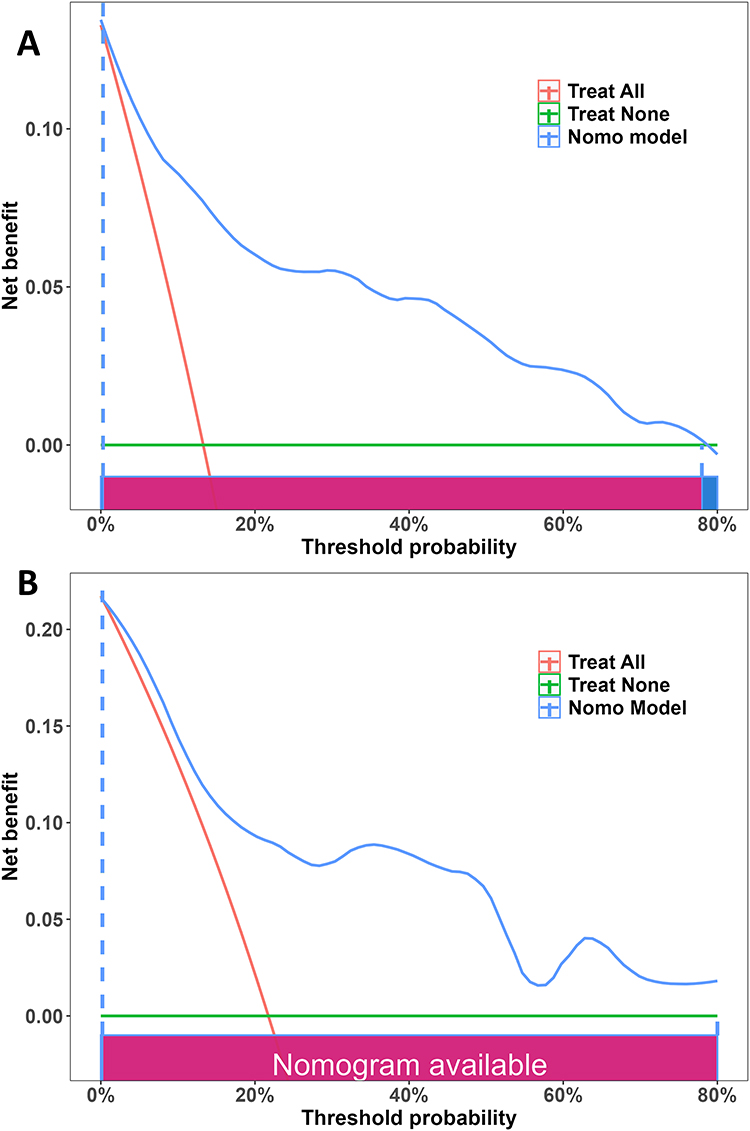 |
Figure 6 The DCA curves of the nomogram in the training cohort (A) and validation cohort (B). Abbreviation: DCA, decision curve analysis. |
Discussion
Early recognition of IPA in the ICU remains challenging. Autopsy data suggest substantial underdiagnosis, with a proportion of cases not recognized before death.20 Radiologic findings in ICU patients are often non-specific, the accuracy of non-culture diagnostics (eg., galactomannan assays and PCR) may be lower, and invasive biopsy is frequently not feasible because of hemodynamic instability, mechanical ventilation, or coagulopathy.21,22 In addition, distinguishing airway colonization from invasive infection is often difficult when Aspergillus is recovered from respiratory specimens. Clinical presentation may be further confounded in patients with concomitant viral pneumonia (eg., COVID-19 or influenza), where overlapping features can obscure recognition of viral-associated aspergillosis such asCAPA.23 Collectively, these challenges support the need for early risk assessment tools in ICU populations, especially in ICU patients with sepsis, in whom sepsis-associated immune dysfunction and a high burden of organ failure and treatment exposures can obscure early signals of IPA and increase clinical uncertainty.
In this study, we developed and internally validated a nomogram to predict the occurrence risk of secondary IPA in ICU patients with sepsis. The results showed that smoking history, corticosteroid therapy, coexisting SFTS or COVID-19, duration of mechanical ventilation, NRS 2002 score, and SOFA score were significantly associated with IPA occurrence risk. The model showed good discrimination and calibration in both the training and validation cohorts, suggesting it may assist early risk assessment and identification of high-risk patients.
The results of our study suggest that the development of IPA in ICU patients with sepsis is not determined by a single factor, but associated with combined effects of multiple risk domains, including baseline host status, disease severity, and treatment-related exposures.
Host status appears to be a fundamental determinant of IPA occurrence risk. Sepsis itself can induce a dysregulated immune response and lead to immune dysfunction.6,24 An increased SOFA score reflects a greater burden of organ dysfunction and may also indicate more severe systemic inflammation and immune dysregulation.25–28 In such situation, host clearance of inhaled Aspergillus conidia may be impaired, with a consequent increase in the risk of secondary invasive infection. Smoking history is another important host-related factor. Previous studies suggest that smoking can damage the airway epithelial barrier, impair mucociliary clearance, and alter pulmonary innate immune defenses, thereby reducing the efficiency of respiratory clearance of inhaled pathogens.29–33 These pathophysiological considerations are consistent with our study that smoking history was retained in the final model.
Nutritional risk was an important clinical factor associated with IPA in this study. NRS 2002 is a widely used and pragmatic screening tool in critical care.34 Higher scores generally indicate reduced nutritional reserve and a hypercatabolic state. The inclusion of NRS 2002 in the final model suggests that impaired nutritional status may contribute to the development of secondary IPA in ICU patients with sepsis. Notably, direct evidence specifically linking NRS 2002 to IPA remains limited. Existing studies suggest that nutritional risk may indirectly increase susceptibility to opportunistic infections through impaired immune defense and reduced tissue repair capacity.35 Nutritional derangements are common in critically ill patients, and poor nutritional status has been associated with a higher risk of pulmonary infections, including ventilator-associated pneumonia.36 As an emerging biomarker, CAR is indicative of the metabolic and immune status of the body.37 In our study, the between-group difference in CAR in univariable analysis further supports the possibility that inflammatory burden and nutritional status jointly influence IPA occurrence risk. Previous critical care studies have shown that NRS 2002 has good prognostic performance.38 Our study further suggests that, beyond estimating the risk of adverse outcomes, NRS 2002 may provide additional predictive value for secondary IPA occurrence risk assessment in ICU patients with sepsis. Given its simplicity, bedside availability, and suitability for serial reassessment, incorporating NRS 2002 into infection risk assessment workflows in this population appears clinically feasible.
Treatment-related exposures were also important correlates of IPA occurrence. Corticosteroid therapy was associated with an increased risk of IPA, consistent with previous reports.33 Corticosteroids may impair neutrophil and macrophage function and suppress cell-mediated antifungal immunity, thereby reducing host antifungal defense.39–41 In addition, corticosteroid use is more common among patients with greater disease severity. It may reflect a higher inflammatory burden and organ dysfunction, both of which are associated with increased susceptibility to invasive Aspergillus infection. A longer duration of mechanical ventilation was also associated with higher IPA occurrence risk. This variable may reflect prolonged artificial airway exposure leading to impaired respiratory barrier function, and might also partially indicate persistent critical illness.42 Therefore, it should not be oversimplified as an isolated causal factor, but rather as a clinical risk indicator. For patients requiring prolonged mechanical ventilation, especially those with higher SOFA or NRS 2002 scores, early mycological testing and closer serial chest imaging should be considered to improve timely identification of IPA.
Coexisting SFTS or COVID-19 was associated with an increased risk of IPA, suggesting that viral infection-related background may be relevant to risk assessment. Previous studies indicate that both conditions can be accompanied by lung injury and immune dysregulation, which are often more pronounced in critically ill patients and may increase susceptibility to IPA.43–47When these abnormalities coexist with sepsis-associated immune dysfunction, susceptibility to opportunistic infection may increase further.48,49 Early in the COVID-19 pandemic, European centers reported a high incidence of CAPA, which has subsequently been recognized as an important complication of severe COVID-19 in ICU settings, particularly among patients requiring invasive mechanical ventilation.23,50 Although A. fumigatus remains the predominant species reported in CAPA, non-A. fumigatus species, including A. flavus, A. niger, A. nidulans, A. versicolor, and A. calidoustus, as well as mixed-species infections, have also been described. Similarly, our cohort data showed that A. fumigatus was the most frequently identified species. However, non-A. fumigatus species were also identified in a substantial proportion of isolates, most commonly A. flavus, with occasional isolation of A. niger and A. terreus; mixed-species isolation was observed in a small number of cases. Variation in host characteristics, local epidemiology, and diagnostic sampling strategies may contribute to differences in reported species distributions across studies. Therefore, we cautiously suggest that viral infection related clinical background should be carefully considered when assessing IPA occurrence risk in ICU patients with sepsis, to improve the identification of high-risk patient.
From a clinical standpoint, this model may have potential practical utility. All predictors included in the model are routinely collected clinical variables, readily available, and feasible to apply in ICU practice. Compared with a single indicator, this multivariable model may provide a more comprehensive assessment of IPA occurrence risk.
This study has several limitations. First, as a single-center retrospective study, it is susceptible to selection bias and information bias. Second, external validation was limited; therefore, the model’s stability and generalizability require further evaluation in additional independent cohorts. Third, this was a static model based on baseline variables and did not incorporate dynamic predictors. Fourth, although species-level mycological identification was available, the number of cases for individual Aspergillus species was limited; thus, we did not perform species-specific risk prediction modeling to avoid unstable estimates. Future prospective, multicenter studies with dynamic modeling are needed to further improve model performance, evaluate species-specific risk patterns, and clarify clinical utility.
Conclusion
In this study, we developed and internally validated a nomogram to estimate the risk of secondary invasive pulmonary aspergillosis (IPA) in ICU patients with sepsis. The results suggested that smoking history, corticosteroid therapy, coexisting SFTS or COVID-19, duration of mechanical ventilation, NRS 2002 score, and SOFA score were associated with IPA occurrence risk in this cohort. Notably, the inclusion of NRS 2002 in the model suggests that nutritional risk may have clinical relevance in IPA occurrence, although this association requires further confirmation. Based on routinely collected clinical data, the prediction model may provide a feasible exploratory tool to support early risk assessment and identification of ICU patients with sepsis who are at higher risk of secondary IPA. Further prospective multicenter studies are needed to validate its external applicability and clinical benefit.
Abbreviations
IPA, invasive pulmonary aspergillosis; ICU, intensive care unit; LASSO, least absolute shrinkage and selection operator; LOS, hospital length of stay; SFTS, Severe Fever with Thrombocytopenia Syndrome; COVID-19, Coronavirus Disease 2019; CAPA, COVID-19–associated pulmonary aspergillosis; ARDS, acute respiratory distress syndrome; COPD, chronic obstructive pulmonary disease; GM, serum galactomannan; BALF, bronchoalveolar lavage fluid; CT, chest computed tomography; PCR, polymerase chain reaction; APACHE II, acute physiology and chronic health evaluation II; SOFA, sequential organ failure assessment; NRS 2002, Nutritional risk screening 2002; MODS, multiple organ dysfunction syndrome; CAR, C-reactive protein-to-albumin ratio; PaO2, arterial partial pressure of oxygen; FiO2, fraction of inspired oxygen; PaCO2, arterial partial pressure of carbon dioxide; MV, Mechanical Ventilation; CRRT, continuous renal replacement therapy; ROC, receiver operating characteristic; AUC, receiver operating characteristic curve; DCA, decision curve analysis; OR, odds ratio; CI, confidence interval; IQR, interquartile range; SD, standard deviation.
Data Sharing Statement
The data sets used during the study are available from the corresponding author on reasonable request.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82072134), the Major Scientific Research Project of the Anhui Provincial Health Commission (No. AHWJ2024Aa40031, AHWJ2024Aa10164), and Anhui Province Natural Science Foundation Project (No.2508085MH208).
Disclosure
All authors report no conflicts of interest in this work.
References
1. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the global burden of disease study. Lancet. 2020;395(10219):200–16. doi:10.1016/s0140-6736(19)32989-7
2. Gray AP, Chung E, Hsu RL. Global. regional, and national sepsis incidence and mortality, 1990-2021: a systematic analysis. Lancet Glob Health. 2025;13(12):e2013–e2026. doi:10.1016/s2214-109x(25)00356-0
3. Pickkers P. Simultaneously mounted pro- and anti-inflammatory host response relates to the development of secondary infections in patients with sepsis. Am J Respir Crit Care Med. 2017;196(4):406–407. doi:10.1164/rccm.201701-0253ED
4. Mankowski RT, Anton SD, Ghita GL, et al. Older adults demonstrate biomarker evidence of the persistent inflammation, immunosuppression, and catabolism syndrome (pics) after sepsis. J Gerontol a Biol Sci Med Sci. 2022;77(1):188–196. doi:10.1093/gerona/glab080
5. Cajander S, Kox M, Scicluna BP, et al. Profiling the dysregulated immune response in sepsis: overcoming challenges to achieve the goal of precision medicine. Lancet Respir Med. 2024;12(4):305–322. doi:10.1016/S2213-2600(23)00330-2
6. Kox M, Bauer M, Bos LDJ, et al. The immunology of sepsis: translating new insights into clinical practice. Nat Rev Nephrol. 2026;22(1):30–49. doi:10.1038/s41581-025-01004-6
7. Darden DB, Kelly LS, Fenner BP, Moldawer LL, Mohr AM, Efron PA. Dysregulated Immunity and Immunotherapy after Sepsis. J Clin Med. 10(8). doi:10.3390/jcm10081742
8. Hotchkiss RS, Monneret G, Payen D. Sepsis-induced immunosuppression: from cellular dysfunctions to immunotherapy. Nat Rev Immunol. 2013;13(12):862–874. doi:10.1038/nri3552
9. Thompson GR 3rd, Young JH. Aspergillus Infections. N Engl J Med. 2021;385(16):1496–1509. doi:10.1056/NEJMra2027424
10. Zelante T, Montagnoli C, Bozza S, et al. Manipulating immunity against Aspergillus fumigatus. Med Mycol.;44(Supplement_1):S237–s243. doi:10.1080/13693780600778668.
11. Latge JP, Chamilos G. Aspergillus fumigatus and Aspergillosis in 2019. Clin Microbiol Rev. 2019;33(1). doi:10.1128/CMR.00140-18
12. Townsend L, Martin-Loeches I. Invasive aspergillosis in the intensive care unit. Diagnostics. 2022;12(11). doi:10.3390/diagnostics12112712
13. Hatzl S, Geiger C, Kriegl L, et al. Performance of diagnostic algorithms in patients with invasive pulmonary aspergillosis. Clin Infect Dis. 2025;80(5):1080–1087. doi:10.1093/cid/ciae633
14. Massart N, Plainfosse E, Benameur Y, et al. Prediction of pulmonary aspergillosis in patients with ventilator-associated pneumonia. Ann Intensive Care. 2023;13(1):109. doi:10.1186/s13613-023-01199-6
15. Gu Y, Ye X, Liu Y, et al. A risk-predictive model for invasive pulmonary aspergillosis in patients with acute exacerbation of chronic obstructive pulmonary disease. Respir Res. 2021;22(1):176. doi:10.1186/s12931-021-01771-3
16. Friol A, Dumas G, Pene F, et al. A multivariable prediction model for invasive pulmonary aspergillosis in immunocompromised patients with acute respiratory failure (IPA-GRRR-OH score). Intensive Care Med. 2025;51(1):72–81. doi:10.1007/s00134-024-07767-z
17. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
18. Bassetti M, Giacobbe DR, Agvald-Ohman C, et al. Invasive Fungal Diseases in Adult Patients in Intensive Care Unit (FUNDICU): 2024 consensus definitions from ESGCIP, EFISG, ESICM, ECMM, MSGERC, ISAC, and ISHAM. Intensive Care Med. 2024;50(4):502–515. doi:10.1007/s00134-024-07341-7
19. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
20. Tejerina EE, Abril E, Padilla R, et al. Invasive aspergillosis in critically ill patients: an autopsy study. Mycoses. 2019;62(8):673–679. doi:10.1111/myc.12927
21. Park SY, Kim SH, Choi SH, et al. Clinical and radiological features of invasive pulmonary aspergillosis in transplant recipients and neutropenic patients. Transpl Infect Dis. 2010;12(4):309–315. doi:10.1111/j.1399-3062.2010.00499.x
22. Boonsarngsuk V, Niyompattama A, Teosirimongkol C, Sriwanichrak K. False-positive serum and bronchoalveolar lavage Aspergillus galactomannan assays caused by different antibiotics. Scand J Infect Dis. 2010;42(6–7):461–468. doi:10.3109/00365541003602064
23. Janssen NAF, Nyga R, Vanderbeke L, et al. Multinational Observational Cohort Study of COVID-19-Associated Pulmonary Aspergillosis(1). Emerg Infect Dis. 2021;27(11):2892–2898. doi:10.3201/eid2711.211174
24. Qing G, Zhang Y, Wang Y, et al. FcγR-targeted tuftsin clusters rejuvenate macrophages in preclinical sepsis-associated secondary infection. Sci Transl Med. 2025;17(830):eadv0313. doi:10.1126/scitranslmed.adv0313
25. Vincent JL, de Mendonça A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med. 1998;26(11):1793–1800. doi:10.1097/00003246-199811000-00016
26. Ferreira FL, Bota DP, Bross A, Mélot C, Vincent JL. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA. 2001;286(14):1754–1758. doi:10.1001/jama.286.14.1754
27. Raith EP, Udy AA, Bailey M, et al. Prognostic accuracy of the sofa score, sirs criteria, and qsofa score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA. 2017;317(3):290–300. doi:10.1001/jama.2016.20328
28. Wang L, Ma X, Zhou G, et al. SOFA in sepsis: with or without GCS. Eur J Med Res. 2024;29(1):296. doi:10.1186/s40001-024-01849-w
29. Yang SR, Chida AS, Bauter MR, et al. Cigarette smoke induces proinflammatory cytokine release by activation of NF-kappaB and posttranslational modifications of histone deacetylase in macrophages. Am J Physiol Lung Cell Mol Physiol. 2006;291(1):L46–57. doi:10.1152/ajplung.00241.2005
30. Ghio AJ, Stewart M, Sangani RG, Pavlisko EN, Roggli VL. Cigarette smoking decreases macrophage-dependent clearance to impact the biological effects of occupational and environmental particle exposures. Front Public Health. 2025;13:1558723. doi:10.3389/fpubh.2025.1558723
31. Dai Y, Pu Q, Hu N, et al. The dose-response relationship between smoking and the risk factor for invasive pulmonary aspergillosis in patients with severe fever with thrombocytopenia syndrome. Front Microbiol. 2023;14:1209705. doi:10.3389/fmicb.2023.1209705
32. Xavier RF, Ramos D, Ito JT, et al. Effects of cigarette smoking intensity on the mucociliary clearance of active smokers. Respiration. 2013;86(6):479–485. doi:10.1159/000348398
33. Terrones-Campos C, Gallardo-Pizarro A, Martinez-Urrea A, et al. Invasive pulmonary aspergillosis in the ICU: the corticosteroid link. Pneumonia. 2026;18(1):2. doi:10.1186/s41479-025-00189-5
34. Kondrup J, Allison SP, Elia M, Vellas B, Plauth M. ESPEN guidelines for nutrition screening 2002. Clin Nutr. 2003;22(4):415–421. doi:10.1016/s0261-5614(03)00098-0
35. Wen KL, Cao YX, Du H, Huang WQ, Zhang A. Association between protein and energy intake during acute phase and sepsis outcomes: a retrospective cohort study. Sci Rep. 2025;15(1):27771. doi:10.1038/s41598-025-13738-1
36. Scislo L, Walewska E, Bodys-Cupak I, Gniadek A, Kozka M. Nutritional status disorders and selected risk factors of ventilator-associated pneumonia (vap) in patients treated in the intensive care ward-a retrospective study. Int J Environ Res Public Health. 19(1). doi:10.3390/ijerph19010602
37. Lin J, Yang X, Wu Z, Lu J, Zhang M. C-reactive protein-to-albumin ratio is associated with increased depression: an exploratory cross-sectional analysis. J Affect Disord. 2025;382:131–138. doi:10.1016/j.jad.2025.04.084
38. Arzu YA, Pelin BK, Sevgi A, Guldem T. Association of mNUTRIC and NRS 2002 Scores with mortality in intensive care unit patients. Pak J Med Sci. 2025;41(7):2030–2035. doi:10.12669/pjms.41.7.12087
39. Bernal-Martínez L, Gonçalves SM, de Andres B, et al. TREM1 regulates antifungal immune responses in invasive pulmonary aspergillosis. Virulence. 2021;12(1):570–583. doi:10.1080/21505594.2021.1879471
40. Balloy V, Huerre M, Latgé JP, Chignard M. Differences in patterns of infection and inflammation for corticosteroid treatment and chemotherapy in experimental invasive pulmonary aspergillosis. Infect Immun. 2005;73(1):494–503. doi:10.1128/iai.73.1.494-503.2005
41. Gohir W, McTaggart L, Kus JV, et al. Evaluating the Role of STAT3 in CD4(+) T Cells in Susceptibility to Invasive Aspergillosis. Infect Immun. 2021;89(5). doi:10.1128/iai.00035-21
42. Stello BB, Cattani A, Milanez DSJ, Razzera EL, Lima J, Silva FM. Prognostic value of different cut-off points of the NRS-2002 tool to identify nutritional risk in critically ill patients: a longitudinal study. Br J Nutr. 2023;130(8):1357–1365. doi:10.1017/S0007114523000363
43. Calderón-Parra J, Mills-Sanchez P, Moreno-Torres V, et al. COVID-19-associated pulmonary aspergillosis (CAPA): risk factors and development of a predictive score for critically ill COVID-19 patients. Mycoses. 2022;65(5):541–550. doi:10.1111/myc.13434
44. Feys S, Carvalho A, Clancy CJ, et al. Influenza-associated and COVID-19-associated pulmonary aspergillosis in critically ill patients. Lancet Respir Med. 2024;12(9):728–742. doi:10.1016/s2213-2600(24)00151-6
45. Koehler P, Bassetti M, Kochanek M, Shimabukuro-Vornhagen A, Cornely OA. Intensive care management of influenza-associated pulmonary aspergillosis. Clin Microbiol Infect. 2019;25(12):1501–1509. doi:10.1016/j.cmi.2019.04.031
46. Xu Y, Shao M, Liu N, Tang J, Gu Q, Dong D. Invasive pulmonary aspergillosis is a frequent complication in patients with severe fever with thrombocytopenia syndrome: a retrospective study. Int J Infect Dis. 2021;105:646–652. doi:10.1016/j.ijid.2021.02.088
47. Yao L, Shi Y, Fu J, et al. Risk factors for invasive pulmonary aspergillosis in patients with severe fever with thrombocytopenia syndrome: a multicenter retrospective study. J Med Virol. 2024;96(5):e29647. doi:10.1002/jmv.29647
48. Schauwvlieghe A, Rijnders BJA, Philips N, et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med. 2018;6(10):782–792. doi:10.1016/s2213-2600(18)30274-1
49. Dewi IM, Janssen NA, Rosati D, et al. Invasive pulmonary aspergillosis associated with viral pneumonitis. Curr Opin Microbiol. 2021;62:21–27. doi:10.1016/j.mib.2021.04.006
50. Verweij PE, Bruggemann RJM, Azoulay E, et al. Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med. 2021;47(8):819–834. doi:10.1007/s00134-021-06449-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Role of Procalcitonin in Predicting Mortality and Organ Dysfunction at Intensive Care Admission
Suranadi IW, Sinardja CD, Suryadi IA
International Journal of General Medicine 2022, 15:4917-4923
Published Date: 12 May 2022
Development and Validation of a Predictive Nomogram with Age and Laboratory Findings for Severe COVID-19 in Hunan Province, China
Jiang J, Zhong W, Huang W, Gao Y, He Y, Li X, Liu Z, Zhou H, Fu Y, Liu R, Zhang W
Therapeutics and Clinical Risk Management 2022, 18:579-591
Published Date: 17 May 2022
A Visualized Mortality Prediction Score Model in Hematological Malignancies Patients with Carbapenem-Resistant Organisms Bloodstream Infection
Qian C, Wu Q, Ruan Z, Liu F, Li W, Shi W, Ma L, Peng D, Yin H, Yao L, Li Z, Hong M, Xia L
Infection and Drug Resistance 2023, 16:201-215
Published Date: 7 January 2023
LASSO-Based Identification of Risk Factors and Development of a Prediction Model for Sepsis Patients
Hong C, Xiong Y, Xia J, Huang W, Xia A, Xu S, Chen Y, Xu Z, Chen H, Zhang Z
Therapeutics and Clinical Risk Management 2024, 20:47-58
Published Date: 7 February 2024
A Practical Nomogram Based on RDW-CV for Predicting Clinical Outcome in Elderly Septic Patients
Hong C, Liu Z, Nan C, Xie Y, Xia J, Jiang Y, Liu X, Xu Z, Hui K, Xiong Y, Wang W, Chen H
Infection and Drug Resistance 2025, 18:4799-4809
Published Date: 9 September 2025