Back to Journals » Cancer Management and Research » Volume 18

Development and Internal Validation of a Nomogram for Predicting Recurrence in Endometrial Cancer Based on Pathological and Histological Indicators
Authors Miao M, Huang B, Jiang Y, Hua Y, Guo F ![]() , Liu Q, Ding L, Zhou H
, Liu Q, Ding L, Zhou H ![]()
Received 5 February 2026
Accepted for publication 26 February 2026
Published 4 March 2026 Volume 2026:18 600578
DOI https://doi.org/10.2147/CMAR.S600578
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Mengdan Miao,1 Bingna Huang,2 Yirou Jiang,2 Yue Hua,3 Feifei Guo,3 Qi Liu,3 Ling Ding,3 Huaijun Zhou1– 3
1Department of Gynecology, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Gynecology, Nanjing Drum Tower Hospital Clinical College of Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China; 3Department of Gynecology, Affiliated Drum Tower Hospital, Medical School, Nanjing University, Nanjing, People’s Republic of China
Correspondence: Huaijun Zhou, Department of Gynecology, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, Nanjing, People’s Republic of China, Email [email protected]
Background: Endometrial cancer (EC) is a common malignant tumor in the female reproductive system. Identifying patients with a high risk of recurrence is beneficial for formulating personalized follow-up and treatment plans. This study aims to develop a prediction model for evaluating the risk of recurrence of EC after treatment.
Methods: This study conducted a retrospective analysis on 486 patients with EC and randomly divided them into a training group (n = 389) and a validation group (n = 97). A nomogram was constructed after identifying predictors. The concordance index (C-index), receiver operating characteristic (ROC) curve, calibration plots, net reclassification index (NRI), integrated discrimination improvement (IDI), decision curve analysis (DCA) and Kaplan-Meier curves were used to evaluate the predictive model for EC recurrence.
Results: A predictive nomogram was constructed based on the six selected predictors. The ROC curve (area under the curve = 0.890) and calibration curve indicate that the model has high discrimination and calibration capabilities. The NRI in the training set was 0.321 (95% CI: 0.031– 0.438), and the IDI was 0.133 (95% CI: 0.052– 0.215), indicating a significant improvement compared to the ESGO-ESTRO-ESP pattern. The DCA curves indicated that this model exhibited excellent discriminative performance and clinical application value.
Conclusion: A nomogram based on pathological factors and immunohistochemical indicators was constructed and validated for predicting the recurrence of EC. Its predictive performance was superior to the ESGO-ESTRO-ESP pattern, and it can be used as a prognostic tool for clinical risk stratification.
Keywords: endometrial cancer, nomogram, predictive model, histological biomarkers, recurrence
Introduction
Endometrial carcinoma (EC) ranks among the top three most prevalent gynecologic malignancies globally, with a steadily increasing incidence.1–3 Its predominant histological types are endometrioid carcinoma (EEC) and the more clinically aggressive non-endometrioid carcinoma (NEEC). Surgical intervention serves as the cornerstone of management for this disease, and approximately 90% of early-stage patients have a favorable prognosis, but some patients still experience postoperative recurrence. According to statistics, the 5-year survival rate for stage I–II EEC can reach 92.7%.4 However, in the context of recurrence, even with chemotherapy, the response rate is only 12% to 42%, and the improvements in progression-free survival and overall survival are usually short-lived.5 For patients with advanced or recurrent disease, currently available effective treatment options are relatively limited.
In traditional prognostic evaluation of EC, age, surgical-pathological stage, histological type and grade, depth of myometrial invasion, and lymphatic and vascular invasion are key clinicopathological factors for assessing the risk of recurrence.6 Utilizing pathological information of postoperative tumors to predict the risk of recurrence can help provide precision medicine for EC.7 With the increasing depth of molecular biology research, immunohistochemical markers have gradually been incorporated into the prognostic evaluation system for malignant tumors,8–10 providing significant molecular basis for predicting patient survival outcomes.
In routine postoperative immunohistochemical markers of EC tumor tissues, the abnormal expression of estrogen receptor (ER) and progesterone receptor (PR) plays a crucial role in the pathogenic mechanism of EC. Moreover, they serve as crucial biomarkers for assessing prognosis and guiding treatment.11,12 Human epidermal growth factor receptor 2 (HER2), a transmembrane tyrosine kinase, plays a critical role in regulating cell proliferation, differentiation, and survival. Patients with HER2-positive EC usually have a poorer prognosis.13 Abnormal expression of the p53 gene promote tumor development14,15 and can predict the prognosis of EC. The Ki-67 protein can serve as a marker for tumor proliferation and invasion16,17 and predict a poor prognosis in EC.18,19 Dysfunction or low expression of mismatch repair system proteins (MMR) can prevent the correction of DNA repair defects, leading to microsatellite instability and mutation accumulation.20,21 Immunohistochemistry enables the direct assessment of MMR protein expression in tumor samples. The four proteins most frequently evaluated for loss of expression in this context are MLH1, MSH2, MSH6, and PMS2.22,23 In recent years, with the advancement of The Cancer Genome Atlas (TCGA) project, molecular classification of EC has been incorporated into the prognosis assessment.24
Although the ESGO-ESTRO-ESP (European Society of Gynecological Oncology, European Society for Radiotherapy and Oncology and European Society of Pathology) risk stratification model has made progress in incorporating molecular classification,25 it still faces limitations such as limited predictive accuracy. Studies showed that this model achieves a c-index of 0.78 in assessing recurrence risk for early-stage EC, with unclear prognostic differentiation in the intermediate-risk group.26 Even after incorporating molecular classification, 26.6% of patients primarily belonging to the intermediate-high-risk group were still misstratified.27 Most p53mut cases occur in NEEC subtypes, but when NEEC subtypes are excluded, the predictive power of this subgroup decreases in EEC patients, suggesting the need for more histology-specific stratification methods.28
In terms of predictive model construction methods, although nomograms are inferior to machine learning in fitting certain complex nonlinear relationships, they are widely adopted due to their good interpretability and clinical usability. Our previous study has attempted to construct a nomogram for EC recurrence, but it did not incorporate the latest molecular biomarkers and lacked independent validation.29 Therefore, based on clinicopathological and immunohistochemical indicators, this study developed and internally validated a nomogram for predicting postoperative recurrence risk, and compared it with the ESGO-ESTRO-ESP pattern, hoping to assist clinicians in conducting more precise risk stratification.
Materials and Methods
Study Population
This study is a retrospective cohort study that included 486 EC patients treated at Nanjing Drum Tower Hospital from January 2017 to December 2021. The study was conducted in accordance with the ethical guidelines of the Helsinki Declaration and was approved by the Ethics Committee of Nanjing Drum Tower Hospital (2022–276-03). Due to the retrospective study design, the requirement for informed consent was waived.
We included patients with a diagnosis of EC in the study cohort, which was confirmed by clinical manifestations, auxiliary examinations, and postoperative pathological results. All included patients were surgical cases, thus postoperative pathological results were obtained for analysis. Whether adjuvant therapy was administered postoperatively and the specific treatment regimens were strictly determined based on current clinical guidelines and pathological findings, meaning all enrolled patients received standardized treatment. Recurrence is determined by a multidisciplinary team when the patient meets the following criteria after completing initial radical treatment: confirmed by pathological biopsy or imaging examinations (CT, MRI, or PET-CT) showing new local or distant lesions, along with clinical symptoms associated with recurrence supported by imaging findings.
The postoperative pathological results were clear and definite, and immunohistochemical detection were routinely conducted on the tumor tissues. Essential documented parameters included age, menopausal status, tumor histology, International Federation of Gynecology and Obstetrics (FIGO)stage, grade, lymph node metastasis, vascular invasion, myometrial invasion, and immunohistochemical indicators of tumor tissues (HER2, ER, PR, P53, P16, Ki67, Mismatch Repair Deficiency (dMMR) status). The patient will be followed up every 3 months after the treatment, and then every 6 months after three years. The median follow-up period was 48 months. Individuals lacking regular follow-up were excluded from the analysis.
Immunohistochemical Staining
These immunohistochemical results were obtained from the standardized routine pathological examination for postoperative EC at Nanjing Drum Tower Hospital, provided by the Department of Pathology. The immunohistochemistry was performed using Roche Diagnostics antibodies with 3-3’-diaminobenzidine (DAB) chromogen (Maxin, Jiehao Co., Ltd, Shanghai). Two experienced pathologists, blinded to relevant clinical and pathological data, independently evaluated the results by randomly selecting five high-power fields (400×) under an optical microscope (Carl Zeiss Axio microscope). In the pathological results, HER2 and P16 staining results are presented as staining intensity (-, +, ++, +++); ER and PR staining results are scored based on the product of the percentage of positive cells (0 = 0%, 1 = 1–24%, 2 = 25–49%, 3 = 50–74%, 4 = 75–100%) and staining intensity (0 = no staining, 1 = weak, 2 = moderate, 3 = strong); P53 results indicate staining intensity, wild-type (scattered positive results of varying intensities) or abnormal expression (overexpression or complete absence). The P53 immunohistochemical detection examines the protein expression pattern and serves as an alternative marker for TP53 gene mutations. Ki67 immunohistochemical results are quantified as the percentage of positive cells (positivity rate). The dMMR status is determined by the immunohistochemical results of MLH1, MSH2, PMS2, and MSH6. If the results show complete absence of any one of the four proteins, it is interpreted as dMMR.
Development and Validation of the Nomogram
Among all the patient data, 80% was used as the training group, and the remaining 20% was selected as the validation group. For the training queue, the aim was to screen factors for model construction. Meanwhile, the validation queue verified the results from the training group. The overall proportion of incomplete data was 0.68%, and individual missing items varied between 0.20% and 3.00%. To handle these gaps, after dividing the data into training set and validation set, multiple imputation was carried out in SPSS 26 using the complete conditional specification approach, applying predictive mean matching for scale-type variables. All available variables served as predictors to estimate EC recurrence risk. In the univariate logistic regression, variables with P < 0.10 were included in the multivariate analysis. Those predictors that demonstrated statistical significance (p < 0.05) in the multivariate analysis were retained. To reduce the risk of overfitting, stepwise backward regression was applied to screen variables based on the Akaike Information Criterion (AIC) criterion, and the stability of the model was evaluated through internal validation (random split validation set). The goodness of fit of the model was assessed by the Hosmer-Lemeshow test. The discriminative ability of the model was evaluated using the concordance index (C-index) and the receiver operating characteristic (ROC) curve, while calibration was assessed via calibration plots. To further compare the performance of the nomogram against the ESGO-ESTRO-ESP pattern, the Net Reclassification Index (NRI), Integrated Discrimination Improvement (IDI),30,31 decision curve analysis (DCA) and Kaplan-Meier curves were employed (Supplementary Figure 1).
Statistical Analysis
All statistical analyses in this investigation were performed with RStudio (ver. 4.4.2) and IBM SPSS Statistics (ver. 26). A significance threshold of p < 0.05 (two-tailed) was adopted. Several R packages supported specific analytical steps: “caret” was used to randomly divide the research subjects into a training set and a validation set in a 8:2 ratio, “corrplot” helped visualize variable correlations, “regplot” assisted in developing a nomogram through univariate, multivariate, and stepwise logistic regression, and “pROC” enabled the ROC curve plotting. Model calibration was evaluated using the “rms” package, while clinical usefulness was appraised via DCA from the “rmda” library, which computes net benefit over a range of probability thresholds.32,33 The “survival” and “survminer” packages were used to plot Kaplan-Meier curves. For comparative analyses across groups, continuous measures were examined with t-tests and categorical measures with chi-square tests.
Results
Characteristics of Patients
In this retrospective study, we included 486 patients diagnosed and treated for EC from January 2017 to December 2021. The median follow-up period was 48 months. During the follow-up period, 65 patients experienced recurrence, and 421 patients had a favorable prognosis, accounting for 86.63%. Table 1 displays the basic information of the patients. There were no significant differences in the clinical pathological characteristics and the immunohistochemical markers data between the training set and the validation set. Table 1 summarizes the clinical characteristics of these EC patients. The mean age of patients in the training set was 58.01 years; 68.64% of the patients were postmenopausal at diagnosis; 91.52% were patients with type I endometrioid adenocarcinoma; 8.23% of the patients had lymph node metastasis at initial treatment, 18.77% had vascular invasion, and 19.02% exhibited myometrial invasion >1/2.
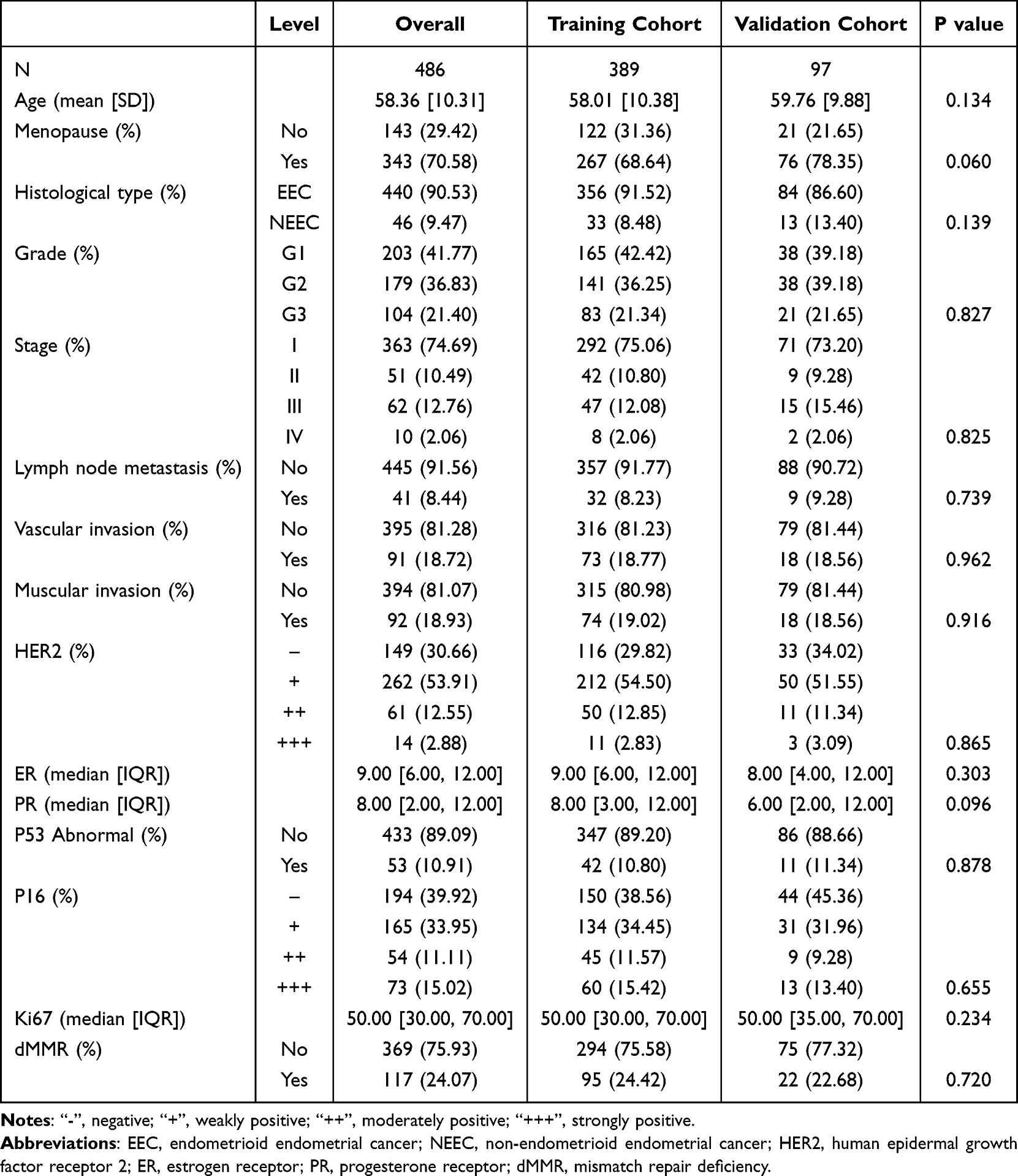 |
Table 1 Clinical Characteristics of Endometrial Cancer Patients |
Screening for Prognostic Variables
Correlation analysis revealed that among the pathological immunohistochemical indicators, there was a positive correlation between ER expression and PR expression, and both were negatively correlated with the expressions of Ki67, HER2, P53, and P16 (Supplementary Figure 2). In the univariate regression analysis, factors with P < 0.1 included age, menopause, histological type, grade, stage, vascular invasion, muscular invasion, expression of HER2, ER, PR, P53, P16, Ki67 and the presence of dMMR. These factors were included in the multivariate logistic regression analysis. Muscular invasion, expression of HER2, ER, P53, P16, and the presence of dMMR were factors with P < 0.05 in the multivariate logistic regression analysis (Table 2, Supplementary Figure 3). The stepwise regression analysis results showed that the AIC values for lymphatic invasion, vascular invasion, muscular invasion, expression of HER2, ER, P53, P16, and the presence of dMMR were the smallest, at 169.39. Therefore, six variables including muscular invasion, expression of HER2, ER, P53, P16, and the presence of dMMR were incorporated into the nomogram prediction model for EC recurrence.
 |
Table 2 Univariate and Multivariate Logistic Regression Analyses on Variables for the Prediction of Recurrence of Endometrial Cancer Patients |
Construction and Validation of a Predicted Nomogram
Based on univariate, multivariate and stepwise logistic regression, a nomogram model was constructed using the six selected variables to estimate the risk of EC recurrence (Figure 1). In the nomogram model shown in Figure 1, after mapping the patient’s values for each variable to the corresponding scale and obtaining individual scores, all the scores are added together to calculate the patient’s total score. Then the corresponding position on the total score axis at the bottom is found, and then map it downward to obtain the individual recurrence risk probability. ROC curve analysis showed that the AUC value of this predictive model was 0.890 (95% confidence interval (CI) = 0.816–0.963) (Figure 2A), indicating that the model has good discriminative power and predictive accuracy.
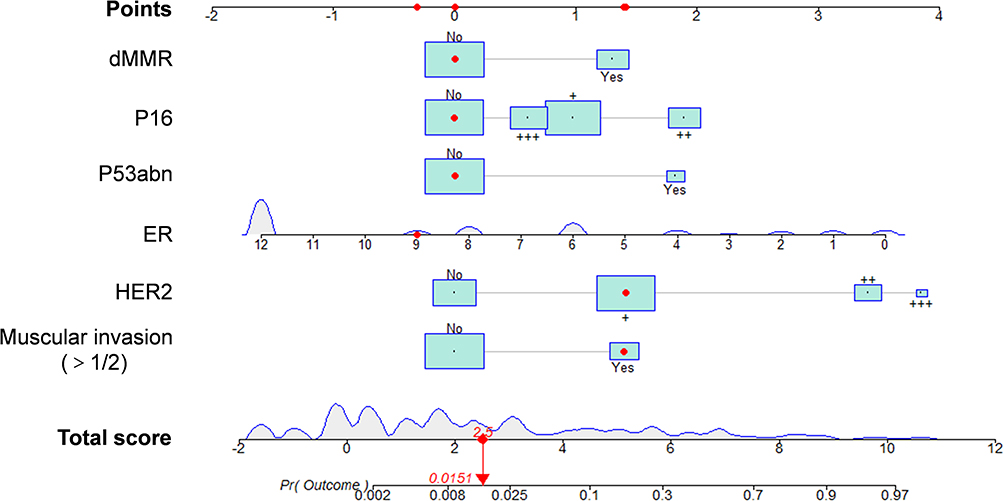 |
Figure 1 A nomogram to predict the recurrence of endometrial cancer. Abbreviations: HER2, human epidermal growth factor receptor 2; ER, estrogen receptor; P53abn, P53 abnormal; dMMR, mismatch repair deficiency. Notes: Read the individual scores for each variable on the corresponding axes. Add up these scores to obtain the total score, and then read the corresponding individualized recurrence probability on the bottom risk axis. The red dot in the figure illustrates an application example, where the total score of 2.50 obtained by summing up the scores of each variable corresponds to a recurrence probability of 0.015. “-”, negative; “+”, weakly positive; “++”, moderately positive; “+++”, strongly positive. |
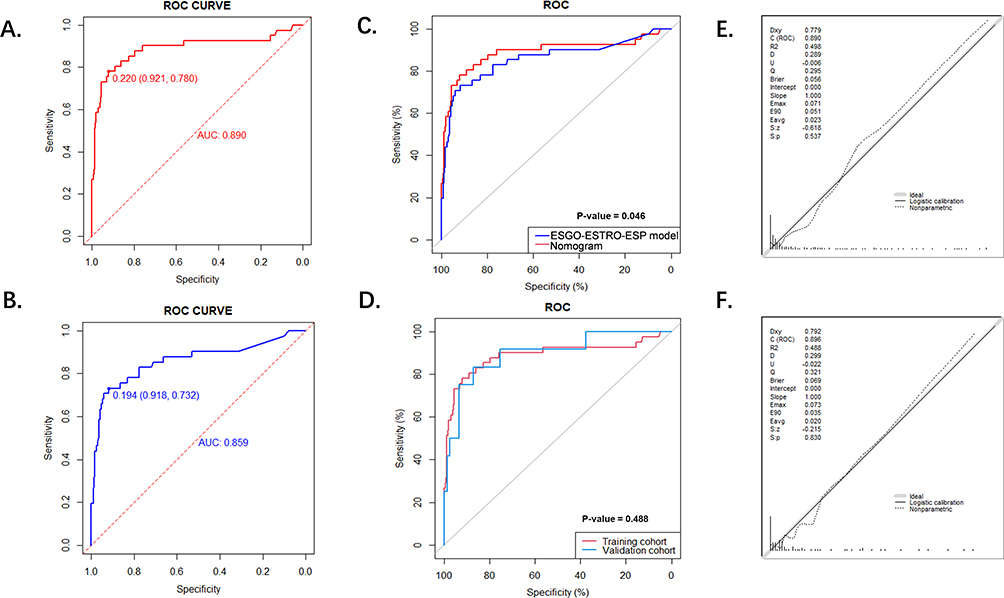 |
Figure 2 Performance evaluation of the model for predicting recurrence in endometrial cancer patients. (A) The ROC curve of the predictive nomogram constructed with the six variables selected in the training cohort. (B) The ROC curve of the ESGO-ESTRO-ESP pattern for the recurrence prediction of EC in the training cohort. (C) Comparison of ROC curves between the six-variable nomogram and the ESGO-ESTRO-ESP pattern in the training cohort. (D) Comparison of the ROC curves between the training and validation cohorts for the predictive nomogram. (E) Calibration plot of the predictive nomogram for EC recurrence in the training cohort. (F) Calibration plot of the predictive nomogram for EC recurrence in the validation cohort. Abbreviations: ROC, receiver operating characteristic; EC, endometrial cancer. |
Subsequently, a predictive model was constructed based on the updated ESGO-ESTRO-ESP guidelines for the management of EC patients in 2025. These guidelines incorporate molecular classification into the treatment decisions.25 ROC curve analysis revealed that the AUC value of the ESGO-ESTRO-ESP pattern was 0.859 (95% CI = 0.782–0.937) (Figure 2B). This indicated that the combination of clinicopathological factors with immunohistochemical results could effectively predict the recurrence of EC, and its predictive ability is superior to the ESGO-ESTRO-ESP model. (P value = 0.046) (Figure 2C). The C-index of the validation cohort was 0.896 (95% CI = 0.829–0.955), and there was no significant difference in the statistical power compared to the training set model (P value = 0.488) (Figure 2D).
Evaluation of the Clinical Value of the Nomogram
The accuracy of the prediction model constructed with the six variables selected by univariate, multivariate logistic analysis and stepwise regression was compared with the model based on the ESGO-ESTRO-ESP pattern using the C-index, NRI, and IDI. The NRI was 0.321 (95% CI = 0.031 −0.438), while the IDI was 0.133 (95% CI = 0.052–0.215, P= 0.002) (Table 3), indicating that the nomogram had significantly improved predictive accuracy compared with the ESGO-ESTRO-ESP pattern. As shown in Figure 2E and F, the calibration curve indicates a good agreement between the predicted probabilities of the model and the actual risk of recurrence in both the training set and the validation set. The Hosmer-Lemeshow test also indicated the calibration effect of the nomogram (p = 0.866). To further evaluate its clinical value, a DCA analysis was conducted. The results showed that the nomogram model demonstrated a favorable positive net benefit (Figure 3A). Figure 3B and C demonstrates that the prediction model incorporating six variables—muscular invasion, expression of HER2, ER, P53, P16, and dMMR—exhibits better predictive accuracy to the prediction model based on the ESGO-ESTRO-ESP pattern. Simultaneously, the DCA curve of the validation set confirms this nomogram’s good clinical applicability in predicting recurrence in EC patients (Figure 3D).
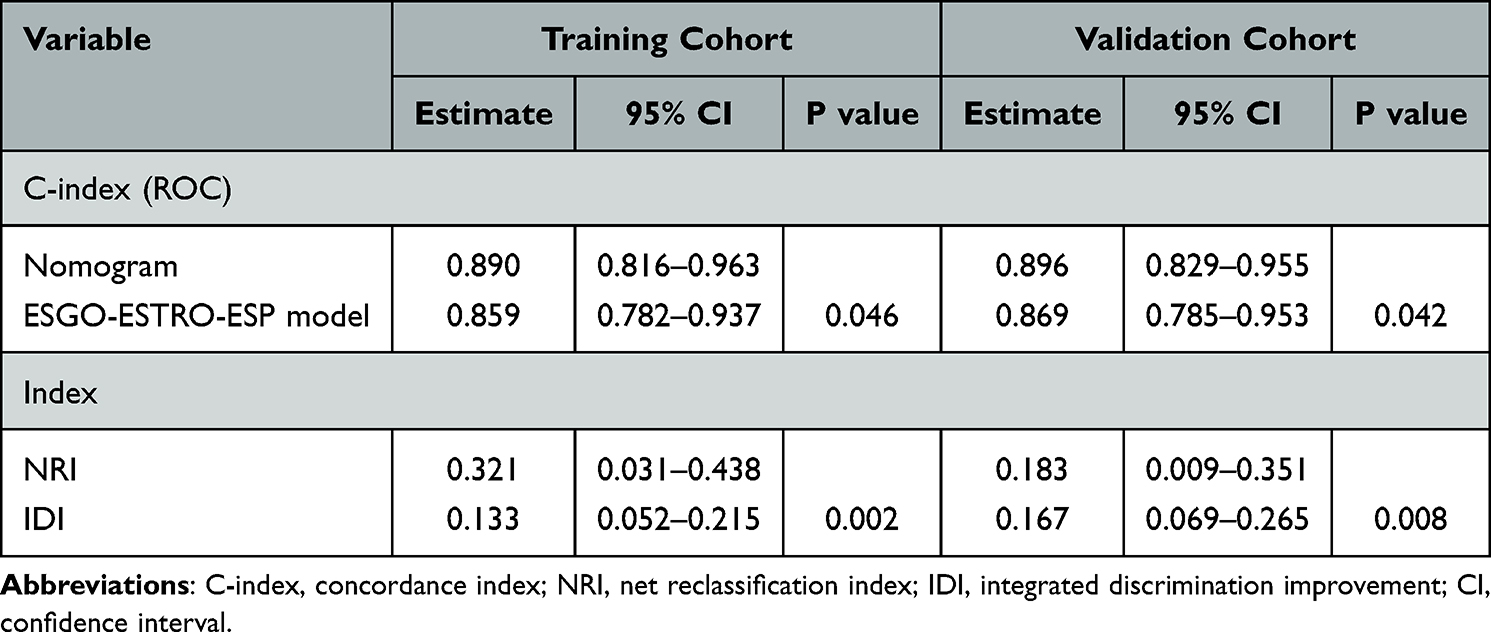 |
Table 3 C-Index, NRI and IDI of the Nomogram in Predicting the Recurrence of Endometrial Cancer Patients |
 |
Figure 3 Clinical applicability analysis of the nomogram for predicting recurrence in endometrial cancer patients. (A) DCA curve of the six-variable nomogram for EC recurrence prediction in the training cohort. (B) DCA curve of the ESGO-ESTRO-ESP pattern in the training cohort. (C) Comparison of DCA curves between the nomogram and the ESGO-ESTRO-ESP pattern in the training cohort. (D) Comparison of the DCA curves between the training and validation cohorts for the predictive nomogram. (E) Kaplan-Meier RFS curves based on the predicted risk levels, with 0.5 as the dividing point. (F) Kaplan-Meier RFS curves based on the classification of the predicted risk levels into four groups, with 0.25, 0.5, and 0.75 as quartile points. Abbreviations: DCA, Decision curve analysis; EC, endometrial cancer; RFS, recurrence-free survival. |
Patients were risk-stratified based on the recurrence probability calculated from the nomogram. When divided into two groups (low-risk group (probability <0.5) and high-risk group (probability ≥0.5)) or four groups (low-risk group (probability <0.25), mediate-risk group (0.25≤probability <0.5), mediate-high-risk group (0.5≤probability <0.75), and high-risk group (probability ≥0.75)), the Kaplan-Meier recurrence-free survival (RFS) curves consistently demonstrated significant differences between risk categories (P < 0.001), indicating that the nomogram has good discriminative ability (Figure 3E and F).
In addition, the predictive model was also used to evaluate the recurrence risk after grouping by EC stage (early and advanced) and pathological type (EEC and NEEC), verifying the performance of the model in subgroups. The model demonstrated great performance across different subgroups (Supplementary Figure 4).
Discussion
This study aims to construct a nomogram model for predicting the risk of EC recurrence, achieving effective prediction with as few variables as possible, while balancing statistical power and clinical utility. We collected clinical data from relevant patients and employed multivariate logistic regression analysis. Based on the minimum AIC criterion, predictive variables were selected through stepwise regression method. Ultimately, six variables were identified and integrated into the nomogram design. During the model training phase, 80% of the case data was randomly sampled to establish the prediction model, and then the remaining 20% of the patients were used to form a validation cohort to evaluate the stability of the model. The predictive explanatory power and efficacy of the nomogram performed well by incorporating multiple influencing factors, with a C-index of 0.890. Multiple metrics, including the C-index, NRI, IDI, and DCA curves, indicate that the nomogram exhibits excellent discriminative ability and outperforms the ESGO-ESTRO-ESP pattern.
All the samples included in this study were patients who received surgical treatment. The postoperative pathological and immunohistochemical indicators were mainly used as factors to construct the predictive model, and the variables related to postoperative adjuvant therapy (such as chemotherapy and radiotherapy) were excluded. This is because whether the patients in this institution receive adjuvant therapy and the specific treatment plan are strictly based on the current clinical guidelines and determined according to the postoperative pathological results (including high-risk factors such as stage, grade, and depth of myometrial invasion). Therefore, adjuvant therapy is prescribed based on pathological features. If it is included in the model together with pathological factors, it may lead to collinearity problems, thereby affecting the predictive value of pathological and immunohistochemical indicators. Secondly, the indicators selected in this study are all tumor biomarkers that already exist in pathology and immunohistochemistry, which enhances the stability and clinical applicability of the model. By analyzing these pathological features related to recurrence risk, the interference of different treatment strategies can be reduced, making the model more robust and clinically interpretable, and further guiding treatment.
The clinicopathological factors of interest in this study, such as age, histopathological type, FIGO stage, tumor grade, myometrial invasion, lymph node metastasis, and vascular invasion, are all closely associated risk factors for EC recurrence.6,34,35 Additionally, the immunohistochemical markers can also indicate the prognosis of EC.36 ER can predict EC prognosis, and its prognostic significance varies across different clinicopathological risk groups and molecular subtypes of EC.37 In high-grade EC, the expression level of HER2 is higher,38 and HER2 positivity often indicates a worse prognosis for EC.5,39 P16, a key regulator of the cell cycle functioning, demonstrates upregulated levels in EC and serves as a critical biomarker for its clinical diagnosis.40 P53 immunohistochemistry has evolved into an accurate surrogate marker reflecting the potential TP53 mutation status.41 Most p53abn EC have a higher grade and involve other tissue types, and are consistently associated with poor clinical prognosis.42 Immunohistochemical testing for MMR proteins (including MLH1, MSH2, MSH6, and PMS2) serves as a highly accurate alternative to molecular testing for microsatellite instability in EC.43,44 The dMMR molecular profile is most frequently observed in endometrial and colorectal carcinomas. It is closely related to specific pathogenic mechanisms, pathological features and prognosis.45
Unlike previous prognostic tools that mainly relied on clinical pathological parameters, this model integrates immunohistochemical markers such as p53 and MMR. The theoretical basis lies in the fact that these markers not only reflect the biological behavior of tumors but are also closely related to prognosis in the TCGA molecular classification. This model demonstrates good discrimination and calibration in predicting the recurrence of EC, with predictive performance superior to the ESGO-ESTRO-ESP pattern. However, this study has certain limitations. Firstly, as a single-center retrospective study, the sample size is limited and lacks external validation, so its clinical applicability still needs further verification. Secondly, the actual impact of the model on clinical decision-making has not been fully verified. For example, whether high-risk patients truly benefit from treatment adjustments still requires further prospective research to verify. Thirdly, this model does not include POLE mutation detection, and the integration with the complete TCGA molecular classification requires further exploration. In summary, this study provides a promising tool for predicting the recurrence risk of EC, but its application in clinical practice still requires support of prospective, multicenter, and external validation studies.
Conclusion
Our research established a nomogram model by screening key clinical pathological factors and immunohistochemical indicators and found that the combined evaluation of muscular invasion, expression of HER2, ER, P53, P16, and the presence of dMMR can predict the recurrence of EC. Our nomogram demonstrated the potential for risk stratification of EC recurrence. However, this study was a single-center retrospective design and lacked external validation, requiring further prospective and multicenter validation before clinical application.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The authors state that they have obtained appropriate institutional review board approval (Ethics Committee of Nanjing Drum Tower Hospital, Approval number: 2022-276-03) and have followed the ethical principles of the Declaration of Helsinki. Patient’s data had been anonymized and de-identified before analysis. In accordance with national regulations for retrospective observational studies using fully anonymized data, the requirement for informed consent was formally waived.
Acknowledgments
We thank all the participants involved in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (NSFC 82172819) to H Zhou, and the Natural Science Foundation of Jiangsu Province (BK20220187) to F Guo.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huvila J, Pors J, Thompson EF, Gilks CB. Endometrial carcinoma: molecular subtypes, precursors and the role of pathology in early diagnosis. J Pathol. 2021;253(4):355–12. doi:10.1002/path.5608
2. Concin N, Matias-Guiu X, Vergote I, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12–39. doi:10.1136/ijgc-2020-002230
3. Crosbie EJ, Kitson SJ, McAlpine JN, et al. Endometrial cancer. Lancet. 2022;399(10333):1412–1428. doi:10.1016/s0140-6736(22)00323-3
4. Ferriss JS, Erickson BK, Shih I-M, Fader AN. Uterine serous carcinoma: key advances and novel treatment approaches. Int J Gynecol Cancer. 2021;31(8):1165–1174. doi:10.1136/ijgc-2021-002753
5. Bruce SF, Wu S, Ribeiro JR, et al. HER2+ endometrioid endometrial cancer possesses distinct molecular and immunologic features associated with a more active immune microenvironment and worse prognosis. Gynecol Oncol. 2023;172:98–105. doi:10.1016/j.ygyno.2023.03.008
6. Oaknin A, Bosse TJ, Creutzberg CL, et al. Endometrial cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(9):860–877. doi:10.1016/j.annonc.2022.05.009
7. Volinsky-Fremond S, Horeweg N, Andani S, et al. Prediction of recurrence risk in endometrial cancer with multimodal deep learning. Nat Med. 2024;30(7):1962–1973. doi:10.1038/s41591-024-02993-w
8. Inoue C, Tamatsuki D, Miki Y, et al. Prognostic significance of combining immunohistochemical markers for cancer-associated fibroblasts in lung adenocarcinoma tissue. Virchows Arch. 2019;475(2):181–189. doi:10.1007/s00428-019-02587-9
9. Wang B, Su A, Li M, et al. Construction of a prognostic model for radical esophagectomy based on immunohistochemical prognostic markers combined with clinicopathological factors. Medicine. 2023;102(9):e32889. doi:10.1097/md.0000000000032889
10. Chelariu-Raicu A, Holley E, Mayr D, et al. A combination of immunohistochemical markers, MUC1, MUC5AC, PAX8 and growth pattern for characterization of mucinous neoplasm of the ovary. Int J Gynecol Cancer. 2022;32(5):662–668. doi:10.1136/ijgc-2021-003104
11. Jamieson A, Huvila J, Chiu D, et al. Grade and estrogen receptor expression identify a subset of no specific molecular profile endometrial carcinomas at a very low risk of disease-specific death. Mod Pathol. 2023;36(4):100085. doi:10.1016/j.modpat.2022.100085
12. Przewoźny S, Rogaliński J, de Mezer M, et al. Estrogen receptor (ER) and progesterone receptor (PgR) expression in endometrial cancer-an immunohistochemical assessment. Diagnostics. 2024;14(3). doi:10.3390/diagnostics14030322
13. Hacker KE, AF K, Gupta M, Pothuri B. HER2 expression in an endometrial cancer cohort. Gynecol Oncol. 2025;201:1–6. doi:10.1016/j.ygyno.2025.07.024
14. Vermij L, Léon-Castillo A, Singh N, et al. p53 immunohistochemistry in endometrial cancer: clinical and molecular correlates in the PORTEC-3 trial. Mod Pathol. 2022;35(10):1475–1483. doi:10.1038/s41379-022-01102-x
15. Jia M, Jiang P, Huang Z, et al. The combined ratio of estrogen, progesterone, Ki-67, and P53 to predict the recurrence of endometrial cancer. J Surg Oncol. 2020;122(8):1808–1814. doi:10.1002/jso.26212
16. Menon SS, Guruvayoorappan C, Sakthivel KM, Rasmi RR. Ki-67 protein as a tumour proliferation marker. Clin Chim Acta. 2019;491:39–45. doi:10.1016/j.cca.2019.01.011
17. Qin L. Application value of Ki67 and serum CA125 in the deep myometrial invasion of endometrial adenocarcinoma. BMC Cancer. 2023;23(1):240. doi:10.1186/s12885-023-10711-x
18. Huang Y, Jiang P, Kong W, et al. Comprehensive assessment of ERα, PR, Ki67, P53 to predict the risk of lymph node metastasis in low-risk endometrial cancer. J Invest Surg. 2023;36(1):2152508. doi:10.1080/08941939.2022.2152508
19. Jia M, Pi J, Zou J, et al. The potential value of Ki-67 in prognostic classification in early low-risk endometrial cancer. Cancer Control. 2023;30:10732748231206929. doi:10.1177/10732748231206929
20. Ryan NAJ, Glaire MA, Blake D, et al. The proportion of endometrial cancers associated with Lynch syndrome: a systematic review of the literature and meta-analysis. Genet Med. 2019;21(10):2167–2180. doi:10.1038/s41436-019-0536-8
21. Puliga E, Corso S, Pietrantonio F, Giordano S. Microsatellite instability in Gastric Cancer: between lights and shadows. Cancer Treat Rev. 2021;95:102175. doi:10.1016/j.ctrv.2021.102175
22. Bateman AC. DNA mismatch repair proteins: scientific update and practical guide. J Clin Pathol. 2021;74(4):264–268. doi:10.1136/jclinpath-2020-207281
23. Dedeurwaerdere F, Claes KB, Van Dorpe J, et al. Comparison of microsatellite instability detection by immunohistochemistry and molecular techniques in colorectal and endometrial cancer. Sci Rep. 2021;11(1):12880. doi:10.1038/s41598-021-91974-x
24. Berek JS, Matias-Guiu X, Creutzberg C, et al. FIGO staging of endometrial cancer: 2023. J Gynecol Oncol. 2023;34(5):e85. doi:10.3802/jgo.2023.34.e85
25. Concin N, Matias-Guiu X, Cibula D, et al. ESGO–ESTRO–ESP guidelines for the management of patients with endometrial carcinoma: update 2025. Lancet Oncol. 2025;26(8):e423–e435. doi:10.1016/s1470-2045(25)00167-6
26. Ramon-Patino JL, Ruz-Caracuel I, Heredia-Soto V, et al. Prognosis stratification tools in early-stage endometrial cancer: could we improve their accuracy? Cancers. 2022;14(4):912. doi:10.3390/cancers14040912
27. Bretová P, Ndukwe MI, Laco J, et al. Preoperative risk stratification in endometrial cancer using ESGO/ESTRO/ESP 2021 guidelines: accuracy with and without molecular classification. BMC Cancer. 2025;25(1):1302. doi:10.1186/s12885-025-14741-5
28. Bruno V, Betti M, Mauro J, Buda A, Vizza E. Biomolecular classification in endometrial cancer: onset, evolution, and further perspectives: a critical review. Cancers. 2024;16(17):2959. doi:10.3390/cancers16172959
29. Miao M, Zhu Y, Wang L, et al. A nomogram for predicting recurrence in endometrial cancer patients: a population-based analysis. Front Endocrinol. 2023;14:1156169. doi:10.3389/fendo.2023.1156169
30. Uno H, Tian L, Cai T, Kohane IS, Wei LJ. A unified inference procedure for a class of measures to assess improvement in risk prediction systems with survival data. Stat Med. 2013;32(14):2430–2442. doi:10.1002/sim.5647
31. Pencina MJ, D’Agostino RB Sr, Steyerberg EW. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat Med. 2011;30(1):11–21. doi:10.1002/sim.4085
32. Wu J, Zhang H, Li L, et al. A nomogram for predicting overall survival in patients with low-grade endometrial stromal sarcoma: a population-based analysis. Cancer Commun. 2020;40(7):301–312. doi:10.1002/cac2.12067
33. Van Calster B, Wynants L, Verbeek JFM, et al. Reporting and interpreting decision curve analysis: a guide for investigators. Eur Urol. 2018;74(6):796–804. doi:10.1016/j.eururo.2018.08.038
34. Restaino S, Tortorella L, Dinoi G, et al. Semiquantitative evaluation of lymph-vascular space invasion in patients affected by endometrial cancer: prognostic and clinical implications. Eur J Cancer. 2021;142:29–37. doi:10.1016/j.ejca.2020.10.011
35. Viola L, Londero AP, Bertozzi S, et al. Prognostic role of Krüppel-like factors 5, 9, and 11 in endometrial endometrioid cancer. Pathol Oncol Res. 2020;26(4):2265–2272. doi:10.1007/s12253-020-00817-z
36. Travaglino A, Raffone A, Saccone G, et al. Immunohistochemical predictive markers of response to conservative treatment of endometrial hyperplasia and early endometrial cancer: a systematic review. Acta Obstet Gynecol Scand. 2019;98(9):1086–1099. doi:10.1111/aogs.13587
37. Aro K, Pasanen A, Bützow R, Loukovaara M. The impact of estrogen receptor and L1 cell adhesion molecule expression on endometrial cancer outcome correlates with clinicopathological risk group and molecular subgroup. Gynecol Oncol. 2024;189:9–15. doi:10.1016/j.ygyno.2024.06.016
38. Matoba Y, Devins KM, Milane L, et al. High-grade endometrial cancer: molecular subtypes, current challenges, and treatment options. Reprod Sci. 2024;31(9):2541–2559. doi:10.1007/s43032-024-01544-5
39. Lin G, Chen W, Chen Y, et al. Preoperative prediction of the HER2 status and prognosis of patients with endometrial cancer using multiparametric MRI-based radiomics: a multicenter study. Sci Rep. 2025;15(1):35590. doi:10.1038/s41598-025-12894-8
40. Kalkan HE, Akman L, Serin G, et al. The usefulness of p16 and COX-2 expression on the prediction of progression to endometrial cancer. Histol Histopathol. 2024;39(5):565–571. doi:10.14670/hh-18-650
41. Köbel M, Ronnett BM, Singh N, et al. Interpretation of P53 Immunohistochemistry in endometrial carcinomas: toward increased reproducibility. Int J Gynecol Pathol. 2019;38(1):S123–s131. doi:10.1097/pgp.0000000000000488
42. Jamieson A, Thompson EF, Huvila J, Gilks CB, McAlpine JN. p53abn endometrial cancer: understanding the most aggressive endometrial cancers in the era of molecular classification. Int J Gynecol Cancer. 2021;31(6):907–913. doi:10.1136/ijgc-2020-002256
43. Riedinger CJ, Esnakula A, Haight PJ, et al. Characterization of mismatch-repair/microsatellite instability-discordant endometrial cancers. Cancer. 2024;130(3):385–399. doi:10.1002/cncr.35030
44. Albertí-Valls M, Olave S, Olomí A, Macià A, Eritja N. Advances in immunotherapy for endometrial cancer: insights into MMR status and tumor microenvironment. Cancers. 2024;16(23):3918. doi:10.3390/cancers16233918
45. Ambrosini M, Manca P, Nasca V, et al. Epidemiology, pathogenesis, biology and evolving management of MSI-H/dMMR cancers. Nat Rev Clin Oncol. 2025;22(6):385–407. doi:10.1038/s41571-025-01015-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Predictive Nomogram with Age and Laboratory Findings for Severe COVID-19 in Hunan Province, China
Jiang J, Zhong W, Huang W, Gao Y, He Y, Li X, Liu Z, Zhou H, Fu Y, Liu R, Zhang W
Therapeutics and Clinical Risk Management 2022, 18:579-591
Published Date: 17 May 2022
Development and Validation of a Risk Nomogram Model for Predicting Recurrence in Patients with Atrial Fibrillation After Radiofrequency Catheter Ablation
Zhao Z, Zhang F, Ma R, Bo L, Zhang Z, Zhang C, Wang Z, Li C, Yang Y
Clinical Interventions in Aging 2022, 17:1405-1421
Published Date: 25 September 2022
Nomogram Based on Preoperative Fibrinogen and Systemic Immune-Inflammation Index Predicting Recurrence and Prognosis of Patients with Borrmann Type III Advanced Gastric Cancer
Wang H, Yin X, Ma K, Wang Y, Fang T, Zhang Y, Xue Y
Journal of Inflammation Research 2023, 16:1059-1075
Published Date: 12 March 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023
Nomogram Based on Immune-Inflammatory Score and Classical Clinicopathological Parameters for Predicting the Recurrence of Endometrial Carcinoma: A Large, Multi-Center Retrospective Study
Wang Y, Zheng Y, Tian C, Yu J, Rao K, Zeng N, Jiang P
Journal of Inflammation Research 2024, 17:11437-11449
Published Date: 23 December 2024