Back to Journals » International Journal of General Medicine » Volume 15
Development and Evaluation of a Risk Prediction Model for Left Ventricular Aneurysm in Patients with Acute Myocardial Infarction in Northwest China
Authors Xing Y, Wang C, Wu H, Ding Y, Chen S, Yuan Z
Received 9 May 2022
Accepted for publication 30 June 2022
Published 6 July 2022 Volume 2022:15 Pages 6085—6096
DOI https://doi.org/10.2147/IJGM.S372158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuanming Xing,1,2 Chen Wang,1,2 Haoyu Wu,1,2 Yiming Ding,1,2 Siying Chen,3 Zuyi Yuan1,2
1Department of Cardiovascular Medicine, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 2Key Laboratory of Environment and Genes Related to Diseases, Ministry of Education, Xi’an, People’s Republic of China; 3Department of Pharmacy, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China
Correspondence: Zuyi Yuan, Department of Cardiovascular Medicine, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China, Email [email protected]
Purpose: Left ventricular aneurysm (LVA) is a severe and common mechanical comorbidity with acute myocardial infarction (AMI) that can present high mortality and serious adverse outcomes. Accordingly, there is a need for early identification and prevention of patients at risk of LVA. The aim of this study was to develop and validate a risk prediction model for LVA among AMI patients in Northwest China.
Methods: A total of 509 patients with AMI were retrospectively collected between January 2018 and August 2021. All patients were randomly divided into a training group (n=356) and a validation group (n=153). Potential risk factors for LVA were screened for predictive modelling using least absolute shrinkage and selection operator regression, multivariate logistic regression, clinical relevance, and represented by a comprehensive nomogram. Receiver operating characteristic curve, calibration curve, and decision-curve analysis (DCA) were used to assess the discrimination capacity, calibration, and clinical validity, respectively.
Results: Seven predictors were finally identified for the establishment of prediction model, including age, cardiovascular disease history, left ventricular ejection fraction, ST-segment elevation, percutaneous coronary intervention history, mean platelet volume, and aspartate aminotransferase. The prediction model achieved acceptable areas under the curves of 0.901 (95% confidence interval [CI]=0.868– 0.933) and 0.908 (95% CI=0.861– 0.956) in the training and validation groups, respectively, and the calibration curves fit well in our model. The DCA result indicated that this nomogram exhibited a favorable performance in terms of clinical utility.
Conclusion: An accurate prediction model for LVA development established, which can be applied to rapidly assess the risk of LVA in patients with AMI. Our findings will aid clinical decision-making to reduce the incidence of LVA in high-risk patients, and counteract adverse cardiovascular outcomes.
Keywords: cardiovascular disease, acute myocardial infarction, left ventricular aneurysm, risk prediction model, adverse cardiovascular outcomes
Introduction
Acute myocardial infarction (AMI) is a type of acute coronary syndrome (ACS), including ST-segment-elevation myocardial infarction (STEMI) and non-STEMI.1,2 The common clinical complications of AMI include heart failure, cardiogenic shock, arrhythmia, cardiac arrest, and mechanical complications,3 which is of low incidence but high mortality rate.4 Ventricular aneurysm, one of the mechanical complications, is a severe and common comorbidity with AMI, occurring mainly in the left ventricle and apical wall.5
Left ventricular aneurysm (LVA) manifests as partial myocardial degeneration and necrosis induced by pathological factors (such as myocardial infarction and cardiomyopathy), resulting in myocardial thinning, decreased strain capacity, and a decrease or loss of its usual range of motion, gradually forming scar tissue that bulges outward. The appearance of ventricular aneurysm will have a long-term effect on cardiac function and require real-time monitoring or surgical treatment. A previous report indicated that 30–35% of the patients typically experience LVAs after AMI,6,7 but due to the rapid development of myocardial infarction revascularization techniques in recent years, LVA occurs in less than 15% of myocardial infarctions.8 Previous studies have focused on risk factor analysis for LVA formation, noting that common risk factors include being >65 years old, female, smoking, and occlusion of the anterior descending vessel, high N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels, ST-segment changes on the electrocardiogram, and a long blood vessel recanalization time.9,10 However, some risk factors are controversial, while no risk prediction model can accurately predict the formation of LVA in clinical practice.
Recent studies have increasingly focused on patient characteristics and laboratory testing indicators to develop risk models for predicting disease incidence. Considering the severity and outcomes of LVA, as well as the high mortality and heavy medical burden of AMI, this study aims to develop an accurate risk prediction model using routine clinical measures that can perform risk prediction for LVA in patients during early AMI, with the goal of improving adverse cardiovascular outcomes in these patients.
Materials and Methods
Study Population
This study collected patients with AMI aged >18 years who were admitted to the First Affiliated Hospital of Xi’an Jiaotong University from January 2018 to August 2021. This retrospective study was approved by the ethics committee of the First Affiliated Hospital of Xi’an Jiaotong University (No. XJTU1AF2021LSK-343). The requirement for individual informed consent was waived by the ethics committee due to the study’s retrospective nature. The data were maintained with confidentiality to protect privacy of the participants. All the procedures were performed under principles of the local law and the Declaration of Helsinki. A combination of criteria is required to diagnose AMI, namely the detection of an increase and/or decrease in a cardiac biomarker, with at least one value above the 99th percentile of the upper reference limit and at least one of the following: 1) symptoms of myocardial ischaemia; 2) new ischaemic electrocardiogram (ECG) changes; 3) development of pathological Q waves on ECG; 4) imaging evidence of loss of viable myocardium or new regional wall motion abnormality in a pattern consistent with an ischaemic aetiology; 5) intracoronary thrombus detected on angiography or autopsy.11 LVA was diagnosed by two-dimensional transthoracic echocardiography (TTE) according to the coronary artery surgery study (CASS) protocol,12 which is considered as the presence of a demarcated bulge in the contour of the left ventricular cavity during systole and diastole with an akinetic or dyskinetic wall.13 AMI and LVA were diagnosed by skilled clinicians according to the American Heart Association/American College of Cardiology guidelines and included STEMI and non-ST-segment elevation acute coronary syndrome.14,15 The LVAs of patients included were usually diagnosed within 1 month of onset of AMI by TTE. Moreover, patients were excluded if they had incomplete data or missing laboratory test indicators. We retrospectively included 202 patients with LVA, the number of patients without LVA was much higher than that of patients with LVA. We ultimately selected 307 matched patients without LVA (approximately 1.5 times the number of patients with ventricular aneurysm). Finally, 509 patients with AMI were included in this study.
Demographic and Clinical Data Collection
All data were accurately extracted from the hospital information system and electronic medical records by two trained researchers and checked by a third experienced physician at the study center. The demographic characteristics included age, sex, smoking history, hypertension, diabetes, cardiovascular diseases (CVDs), and cerebrovascular diseases. The clinical indicators included heart rate, systolic and diastolic blood pressures, hemoglobin, hematocrit, platelet count, platelet distribution width, mean platelet volume (MPV), platelet-larger cell ratio, plateletcrit, blood urea nitrogen, serum creatinine (Scr), serum uric acid (SUA), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), alpha-hydroxybutyrate dehydrogenase (HBDH), creatine kinase (CK), creatine kinase isoenzymes (CK-MB), total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), NT-proBNP, and D-dimer. They also contained cardiac parameters (left ventricular ejection fraction [LVEF] and Killip class), electrocardiographic parameters (ST-segment elevation and Q wave), percutaneous coronary intervention (PCI) history, and various drug treatment histories (β-receptor blocker, calcium-channel blocker, aspirin, clopidogrel, angiotensin-converting-enzyme inhibitor/angiotensin receptor antagonist, and antilipemic agents). The values of LVEF were measured by TTE. Coronary angiography (CAG) was used to evaluate the coronary vessels of the patients. All experiments and methods were performed in accordance with international guidelines and regulations.
Prediction Model Establishment and Validation
The 509 patients with AMI were randomly divided into a training group (n=356) and a validation group (n=153) at a ratio of 7:3.16 For the training group, the least absolute shrinkage and selection operator (LASSO) regression model was used to obtain the best subset of predictors from the primary data, which could minimize the prediction error of a response variable and reduce high-dimensional data.17 The variables selected using LASSO regression were then analyzed using multivariate logistic regression to produce odds ratios (ORs) with 95% confidence intervals (CIs), and the associated P values. After the multivariate analysis, the independent predictors were selected for inclusion in a nomogram. The prediction model for LVA formation was consequently established based on the results of the LASSO regression, multivariate logistic regression, and clinical correlations among patients with AMI.
The established prediction model was validated internally and externally in the training and validation groups, respectively. The receiver operating characteristic curve (ROC) and area under the ROC curve (AUC) were used to determine the discriminative capacity of the model.18 Furthermore, the calibration curves were applied to estimate the strengths of correlations between the actual outcomes and predictions.19 Decision-curve analysis (DCA) was performed to determine the potential clinical effectiveness and benefits of the prediction model.20
Statistical Analysis
Categorical variables were expressed as absolute numbers and percentages, while continuous variables were expressed as the mean±standard deviation values. The differences in demographic and clinical features between the training and validation groups were compared using chi-square, Student’s t, and Wilcoxon tests as appropriate. LASSO regression and multivariate logistic regression were used to screen the significant predictive variables. All statistical analyses were performed using SPSS (version 24.0, SPSS, Chicago, IL, USA) and R software (version 4.1.1, https://www.r-project.org/). All tests were two-tailed, and P<0.05 was considered statistically significant.
Results
Patient Characteristics
The detailed baseline demographics and clinical characteristics of the patients in the two groups are listed in Table 1. The baseline features were similar in the two groups. For the training group, most patients with AMI were >65 years old (59.6%), male (78.9%), had a history of smoking (58.7%), and had hypertension (51.4%), LVEF ≥50% (41.6%), Killip class I (68.5%), and ST-segment elevation (66.3%). The related parameters of myocardial enzyme spectrum, cardiac function, and coagulation function were abnormally elevated in these patients, which mostly included AST, LDH, HBDH, CK, CK-MB, NT-proBNP, and D-dimer. Adversely, these patients had abnormally low HDL-C levels.
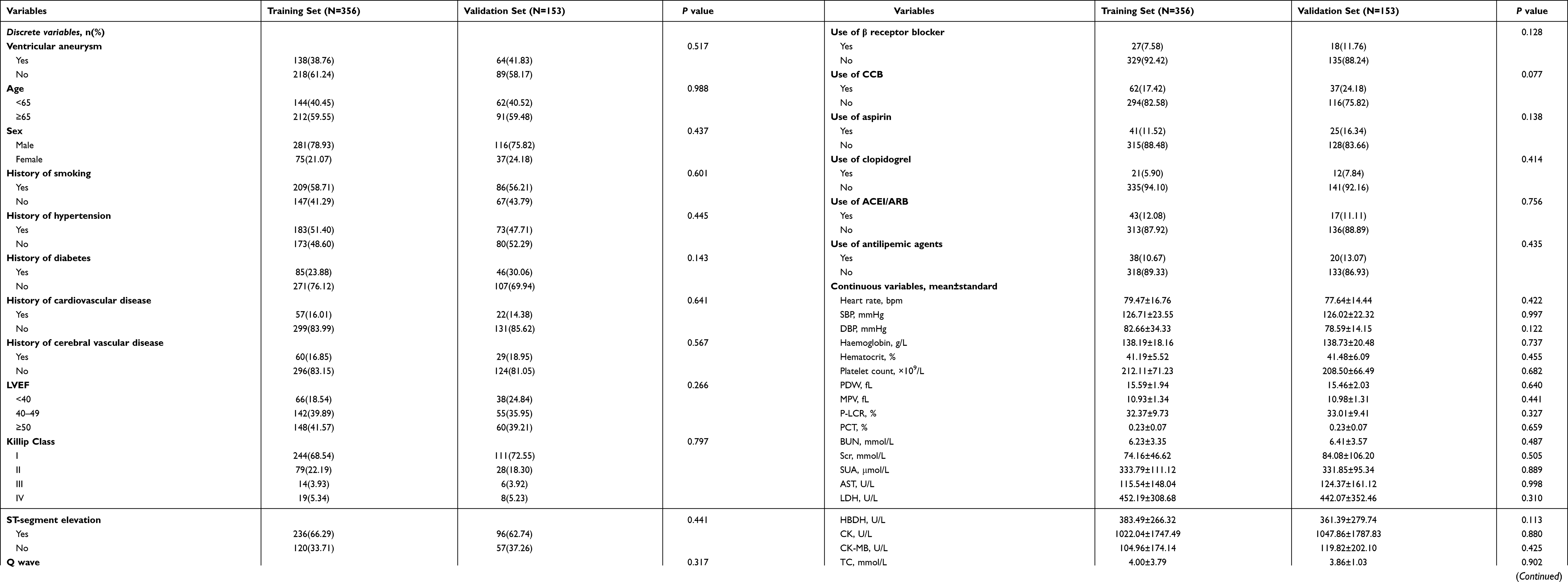 |
Table 1 Baseline Demographics and Clinical Characteristics of Patients in the Training Set and Validation Set |
Additionally, in the LVAs group, the sizes of the LVAs were reported from 200 patients. It was found that the average size of LVA was 31×19 mm, most of the LVAs were small in size with <50 mm diameter (95.5%), and only 9 patients had LVAs with the maximum diameter exceeding 50 mm (4.5%), and the maximum diameter was 70 mm (Table S1). We separately analyzed the differences in coronary vessel lesions from 476 AMI patients recorded for the non-LVAs and LVAs groups, training set and validation set. Patients with right coronary artery (RCA) + left anterior descending artery (LAD) + left circumflex artery (LCx) three-vessel lesions accounted for the largest proportion, followed by LAD one-vessel lesions, and LAD+LCx two-vessel lesions. Comparing the non-LVAs and LVAs groups, there was a statistical difference in patients with one-vessel lesions (Table S2). The characteristics of ECG leads in STEMI patients were also analyzed, which demonstrated that V1-V5 leads, aVL and I leads occurred frequently in patients with LVAs; II, III, aVF leads accounted for the largest proportion in the non-LVAs patients (Table S3).
Feature Selection
Of the demographic characteristics and related clinical parameters, 42 potential variables listed in Table 1 were included in the LASSO regression. After applying LASSO regression to the training group, 42 variables were reduced to the following 18 more-accurate variables with nonzero coefficients: age, CVD history, cerebrovascular disease history, LVEF, Killip class, ST-segment elevation, PCI history, heart rate, use of antilipemic agents, hematocrit, MPV, Scr, SUA, AST, LDH, CK, CK-MB, and LDL-C (Figure 1). These 18 selected variables were then analyzed using multivariate logistic regression. Ultimately, the seven variables of age ≥65 years (OR=8.119, P<0.001), CVD history (OR=5.615, P<0.001), LVEF ≥50% (OR=0.071, P<0.001), ST-segment elevation (OR=3.215, P=0.002), PCI history (OR=0.116, P<0.001), MPV (OR=1.450, P=0.003), and AST (OR=1.004, P<0.001) were statistically significant and hence selected for the development of the prediction model (Table 2). Moreover, most of these seven factors were significantly different between LVAs set and non-LVAs set (Table S4).
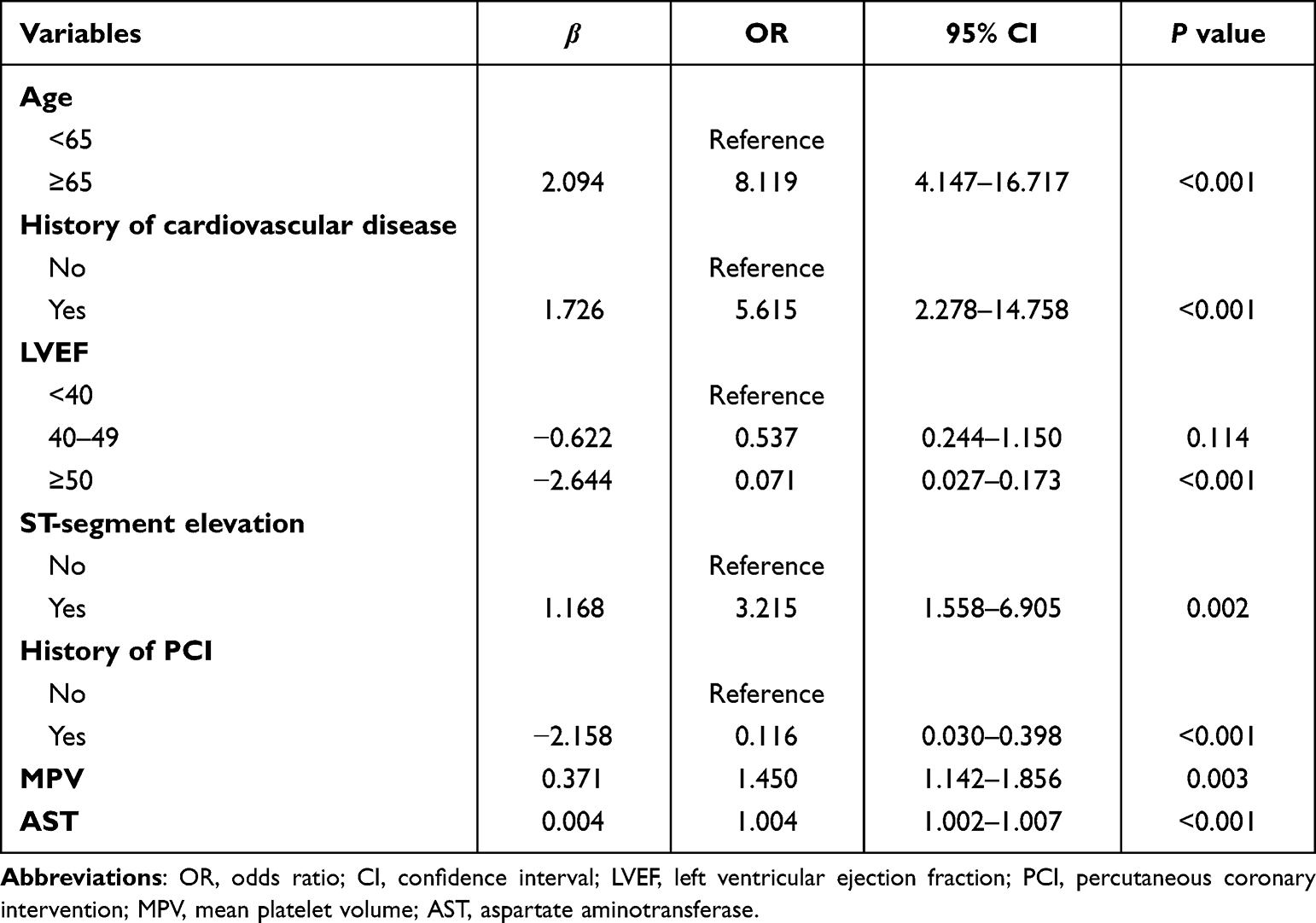 |
Table 2 Multivariate Logistic Regression Analysis for Risk Factors of Ventricular Aneurysm |
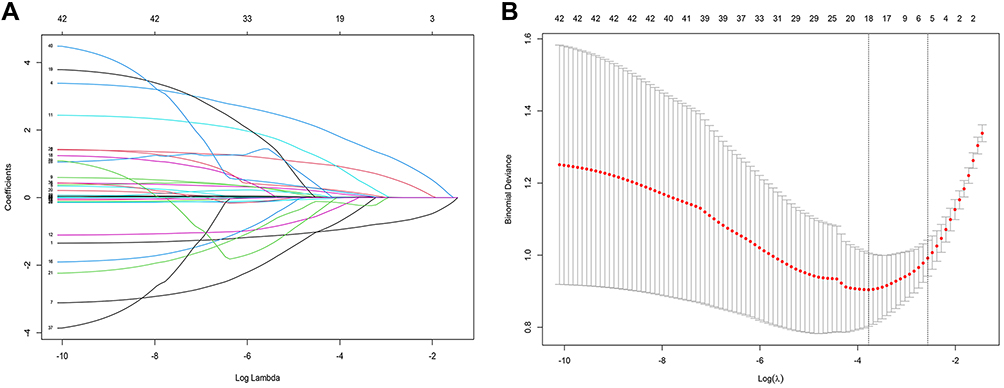 |
Figure 1 Demographic and clinical feature selection using the LASSO regression model. (A) Optimization parameters (lambda) of the LASSO model were obtained via 10-fold cross-validation. (B) The LASSO coefficient profiles of the 42 variables. Abbreviation: LASSO, the least absolute shrinkage and selection operator. |
Development of an Individualized Prediction Model
Based on the LASSO regression and multivariate logistic regression analysis, and clinical correlation results, seven predictors from the training group were included in the LVA risk prediction model and presented as a nomogram (Figure 2A). The nomogram illustrated that each predictor corresponded to a specific score ranging from 0 to 100. The total score is determined by adding the scores of each predictor and is located on the “Total Points” axis. The probability of LVA corresponds to the bottom “Risk of VA” axis of each patient. A higher score for a related factor in the nomogram indicates a higher risk of developing LVA. For instance, this nomogram suggests that a patient with AMI aged ≥65 years and with a CVD history, LVEF of 40–49%, ST-segment elevation, no PCI history, MPV level of 9.3 fL, and AST level of 38 U/L has an estimated LVA probability of 85.1% (Figure 2B).
 |
Figure 2 A nomogram for predicting the risk of LVA in AMI patients. (A) The LVA risk model was developed using the predictors, including ST-segment elevation, history of cardiovascular disease, age, history of PCI, LVEF, MPV and AST. (B) Dynamic nomogram used as an example, **P<0.01, ***P<0.001. This nomogram represents the predicted information of a patient: points shows the predicted risk point for each factor, and total points suggests that the predicted total points of this patient is 389, which corresponding predicted LVA risk is 0.851. Abbreviations: ST, ST-segment elevation; HCAVD, history of cardiovascular disease; PCI, history of percutaneous coronary intervention; LVEF, left ventricular ejection fraction; MPV, mean platelet volume; AST, aspartate aminotransferase. |
Calibration and Validation of the Prediction Model
The prediction model exhibited good accuracy and discrimination in estimating LVA formation in patients with AMI. The AUCs were 0.901 (95% CI=0.868–0.933) and 0.908 (95% CI=0.861–0.956) in the training and validation groups, respectively (Figure 3A and B). Furthermore, the calibration curve demonstrated an agreement between actual observations and predictions of the nomogram in both the training and validation groups (Figure 4A and B). A bias-corrected estimate of the calibration curve (mean absolute error=0.019) was obtained using bootstrapping with 1000 repetitions.
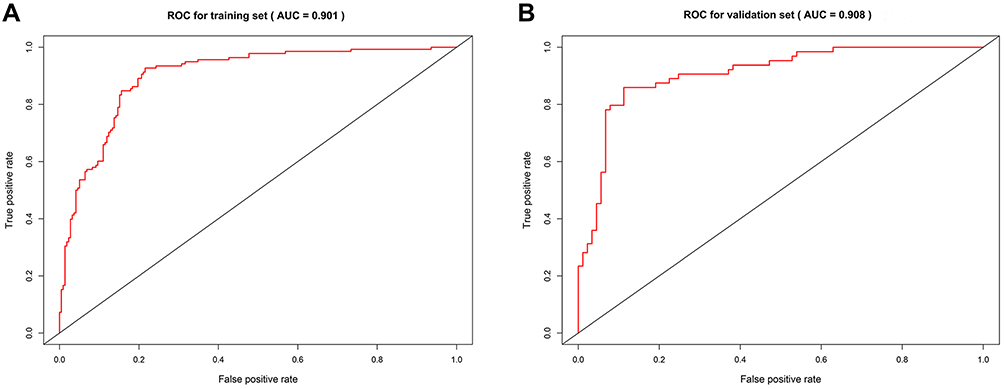 |
Figure 3 ROC curves of the model showing the predictive power for LVA from the training cohort (A) and from the validation cohort (B). Abbreviations: ROC, receiver operating characteristic curve; AUC, area under the ROC curve. |
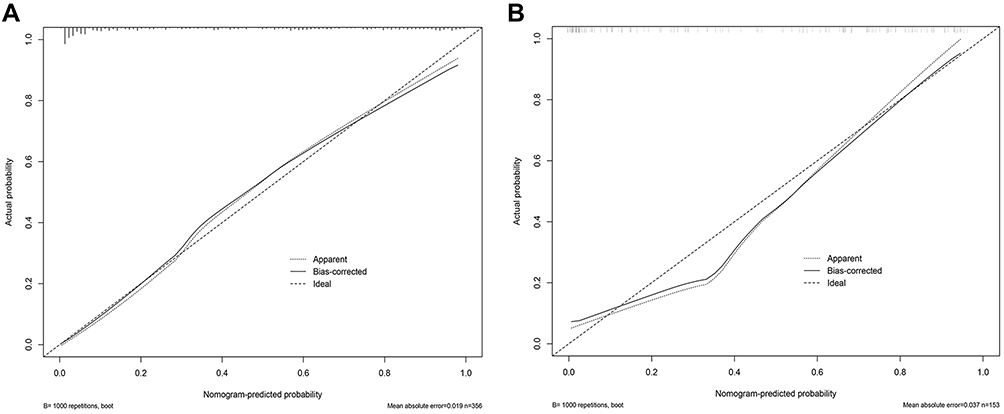 |
Figure 4 The calibration curves of the prediction model for LVA from the training set (A) and from the validation set (B). |
DCA performed to evaluate the potential clinical utility of the prediction model (Figure 5) indicated that the net benefits of the prediction model in both the training and validation groups were significantly higher than those of the two extreme strategies.
 |
Figure 5 Decision curves analysis of the LVA risk from the training set (A) and from the validation set (B). |
Discussion
The clinical mortality rate of AMI remains high, particularly in patients with cardiovascular complications.21 Although the incidence of LVA as a mechanical complication of AMI is relatively low, LVA markedly affects the prognosis of patients with AMI and can even be a serious threat to life.8 Previous studies have mainly reported some risk factors for ventricular aneurysm formation,9,10,22 but an integrated and comprehensive risk model for LVA assessment is still lacking. In the current study, a new prediction model based on a clinical analysis was constructed for LVA risk evaluation in Chinese patients with AMI. A total of seven clinically accessible parameters were included in this prediction model, and the result demonstrated that age ≥65 years, and a history of CVD, LVEF <40%, ST-segment elevation, no history of PCI, and high levels of MPV and AST increased the risk of developing LVA in patients with AMI. Furthermore, the established prediction model allows for more accurate evaluations and predictions of LVA in AMI patients. The model will help clinicians to identify high-risk individuals at an early stage and apply appropriate interventions to improve the prognosis of AMI patients.
Age had a marked effect on the formation of LVA in the included AMI patients, with the majority of AMI patients being older than 65 years (59.6%).23,24 The previous study reported that age in patients with STEMI was related to poor prognosis of cardiovascular disease.25 In addition, the results of this study demonstrated that the risk of developing LVA among patients with AMI was eightfold higher in those >65 years old. Patients with LVA and acute ST-elevation myocardial infarction were reported to be mostly older than those without LVA.10 Although most patients with AMI in the current study had no CVD history (84%), the established risk model confirms for the first time that CVD history is an independent risk factor for LVA formation. Consistently, a previous research has indicated that predictors of AMI include a history of peripheral vascular disease, atrial fibrillation (AF), cardiogenic shock, and cardiac arrest.26 Based on follow-up data, a history of AF was associated with a higher risk of death compared to AMI patients without AF.27 Our result represents evidence that CVD history is a risk factor for a poor prognosis in patients with AMI, and even a risk factor for LVA formation.
LVEF is a critical indicator of clinical concern in AMI patients that reveals myocardial contractility, and has also been used as a reference index for the classification of heart failure after myocardial infarction.28 Some studies indicated a prognostic value of ejection fraction score in patients with STEMI-related cardiogenic shock and in-hospital mortality.25,29,30 The majority of AMI cases had LVEF values >40% in the current data, but in the subsequent analysis, it is interesting to note that AMI patients with LVEF <40% have a considerably higher risk of developing LVA, especially when compared with patients with LVEF ≥50%. Meanwhile, LVEF was also a risk factor that greatly contributed to the comprehensive model for LVA formation. In a previous study, a lower LVEF was similarly observed to be an independent predictor of LVA formation.22 Related research on right ventricular aneurysms also indicated that LVEF <52% was a predictor for the risk of death after AMI.31 Additionally, animal models have demonstrated that LVEF markedly decreases after LVA formation, leading to compromised global systolic function.32
Most of the patients in the training group with myocardial infarction had the characteristics of ST-segment elevation (66.3%). Our established model indicated that the ventricular aneurysm risk in patients with AMI was 3.215-fold higher in those with ST-segment elevation than in those with non-ST-segment elevation. A previous study have also reported that left ventricular pseudoaneurysm with ventricular septal rupture was caused by anterior STEMI.33 LVAs were more commonly observed with anterior ST-segment-elevation AMI (31%) than in inferior (12.3%) and other (7.9%) types of ST-segment-elevation AMI.34 V1-V5 leads, aVL and I leads were noticed to occur frequently in patients with LVAs, which further proved that the anterior leads have the highest frequency of ST-segment elevation after the anterior descending artery was easily injured. Persistent ST-segment elevation was found to be associated with LVA formation after primary PCI in 30% of the cases.35 ST-segment elevation occurs mostly in patients with myocardial infarction complicated by ventricular aneurysm.36,37 A recent study suggested that persistent ST-segment elevation (OR=1.89, P=0.03) was an independent predictor of LVA formation.22
PCI has long been widely considered as the gold standard therapy for improving blood supply to the ischemic tissue after AMI, reversing myocardial necrosis as much as possible, and reducing the risk of death in the acute phase and improving the long-term prognoses of patients.38 Strategies of prompt reperfusion and complete revascularization may be helpful in preventing LVA formation and improving clinical outcomes.22 Early patency of infarct-related artery is the determinant of AMI prognoses, which could prevent acute ventricular remodeling and reverse LVA process.39 In the current study, most of AMI patients, especially those with ST-segment elevation, prompt received CAG and PCI after admission. However, not all included patients received coronary angiography and PCI, thus the time of PCI treatment could not be specifically divided. Considering the long-term impact of vascular lesions for the risk of ventricular aneurysm formation, we mainly investigated the previous history of PCI, but the proportion of such cases was relatively small. These patients essentially had a history of coronary atherosclerotic heart disease with cardiovascular obstructive lesions. However, the risk of LVA after AMI was indicated to be significantly reduced in patients who had been previously treated with PCI, which may be closely associated with the timely dredging of blood vessels. Assessment of the blood vessels by CAG identified that the left anterior descending artery was more likely to be involved. According to the relationship between anatomy and the blood supply of the coronary artery, it was possible that the anterior wall was prone to ischemia and caused LVA when the anterior descending artery was injured.
As an important mediator in initiating thrombosis, platelets play a vital role in the occurrence and development of AMI.40 MPV is the most commonly used measure of platelet size and effectively reflects platelet activation.41 Large-volume platelets contain abundant secretory granules with enhanced metabolism and enzyme activity, associated with a high probability of adhesion and aggregation, leading to acute vascular events.42 In this study, the multivariate logistic regression analysis demonstrated that higher level of MPV represented a higher LVA risk in AMI patients. And the baseline data also showed that the MPV value of AMI patients with LVA was higher than that of non-LVA patients. Elevated MPV value was reported to be associated with AMI, mortality following myocardial infarction, and restenosis following coronary angioplasty.43 Concordantly, AST, an early biomarker for assessing myocardial injury,28 was significantly higher than the normal range in AMI cases, and increased the risk of LVA formation. Comparing with the non-LVAs group, the LVAs patients had high level of AST. These findings suggest that MPV and AST are valuable prognostic biomarkers in patients with CVD.
Several limitations should be addressed. This study retrospectively collected data for modeling, which may have resulted in some missing data, such as cardiac troponin T, characteristics of coronary vessel lesions and information on the transformation of postinfarction scars to aneurysms. Future prospective studies incorporating more comprehensive data for analysis are warranted. This is a single-center study with a model built to collect patients only in northwest China, and external data are needed to further validate the accuracy. Inclusion of additional data, especially multicenter validation studies, including other regions and different ethnic groups, is necessary to validate the performance of the LVA risk model.
Conclusions
The present results highlight several valuable risk factors for LVA after AMI, including age, ST-segment elevation, CVD history, LVEF, PCI, MPV, and AST. An accurate and favorable model was developed based on the risk factors identified in the current study. The application of this model will help identify individuals at high risk for LVA and assist in clinical decision-making to prevent mechanical complications of AMI and counteract adverse cardiovascular outcomes.
Ethics Approval and Informed Consent
This study was approved by the ethics committee of the First Affiliated Hospital of Xi’an Jiaotong University (No. XJTU1AF2021LSK-343). The requirement for individual informed consent was waived by the ethics committee due to the study’s retrospective nature. The data were maintained with confidentiality to protect privacy of the participants. All the procedures were performed under principles of the local law and the Declaration of Helsinki.
Disclosure
The authors declare no conflict of interest.
References
1. Disease, G B D, I Injury and C Prevalence. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
2. Zhao D, Liu J, Wang M, et al. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. 2019;16(4):203–212. doi:10.1038/s41569-018-0119-4
3. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Glob Heart. 2018;13(4):305–338. doi:10.1016/j.gheart.2018.08.004
4. Damluji AA, Forman DE, van Diepen S, et al. Older adults in the cardiac intensive care unit: factoring geriatric syndromes in the management, prognosis, and process of care: a scientific statement from the American Heart Association. Circulation. 2020;141(2):e6–e32. doi:10.1161/CIR.0000000000000741
5. Damluji AA, van Diepen S, Katz JN, et al. Mechanical complications of acute myocardial infarction: a scientific statement from the American Heart Association. Circulation. 2021;144(2):e16–e35. doi:10.1161/CIR.0000000000000985
6. Albuquerque KS, Indiani JMC, Martin MF, et al. Asymptomatic apical aneurysm of the left ventricle with intracavitary thrombus: a diagnosis missed by echocardiography. Radiol Bras. 2018;51(4):275–276. doi:10.1590/0100-3984.2016.0199
7. Achenbach S, Ropers D, Daniel WG. Calcified left ventricular aneurysm. N Engl J Med. 2003;348(24):
8. Lucas LA, Somerville C. Images in clinical medicine. Left ventricular aneurysm. N Engl J Med. 2014;370(3):e5. doi:10.1056/NEJMicm1307241
9. Celebi S, Celebi OO, Cetin S, et al. The usefulness of admission plasma NT-pro BNP level to predict left ventricular aneurysm formation after acute ST-segment elevation myocardial infarction. Arq Bras Cardiol. 2019;113(6):1129–1137. doi:10.5935/abc.20190226
10. Zhang Z, Guo J. Predictive risk factors of early onset left ventricular aneurysm formation in patients with acute ST-elevation myocardial infarction. Heart Lung. 2020;49(1):80–85. doi:10.1016/j.hrtlng.2019.09.005
11. Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–1367. doi:10.1093/eurheartj/ehaa575
12. Bourassa MG, Fisher LD, Campeau L, et al. Long-term fate of bypass grafts: the Coronary Artery Surgery Study (CASS) and Montreal Heart Institute experiences. Circulation. 1985;72(6 Pt 2):V71–78.
13. Visser CA, Kan G, David GK, et al. Echocardiographic-cineangiographic correlation in detecting left ventricular aneurysm: a prospective study of 422 patients. Am J Cardiol. 1982;50(2):337–341. doi:10.1016/0002-9149(82)90185-0
14. O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):485–510. doi:10.1016/j.jacc.2012.11.018
15. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with Non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139–e228. doi:10.1016/j.jacc.2014.09.017
16. Collins GS, Reitsma JB, Altman DG, et al. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350:g7594. doi:10.1136/bmj.g7594
17. Pavlou M, Ambler G, Seaman S, et al. Review and evaluation of penalised regression methods for risk prediction in low-dimensional data with few events. Stat Med. 2016;35(7):1159–1177. doi:10.1002/sim.6782
18. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143(1):29–36. doi:10.1148/radiology.143.1.7063747
19. Huang Y, Li W, Macheret F, et al. A tutorial on calibration measurements and calibration models for clinical prediction models. J Am Med Inform Assoc. 2020;27(4):621–633. doi:10.1093/jamia/ocz228
20. Fitzgerald M, Saville BR, Lewis RJ. Decision curve analysis. JAMA. 2015;313(4):409–410. doi:10.1001/jama.2015.37
21. Mechanic OJ, Gavin M, Grossman SA. Acute Myocardial Infarction. Treasure Island (FL): StatPearls; 2021.
22. You J, Gao L, Shen Y, et al. Predictors and long-term prognosis of left ventricular aneurysm in patients with acute anterior myocardial infarction treated with primary percutaneous coronary intervention in the contemporary era. J Thorac Dis. 2021;13(3):1706–1716. doi:10.21037/jtd-20-3350
23. Saito K, Kondo Y, Takahashi M, et al. Factors that predict ventricular arrhythmias in the late phase after acute myocardial infarction. ESC Heart Fail. 2021;8(5):4152–4160. doi:10.1002/ehf2.13499
24. Kim HR, Kang MG, Kim K, et al. Comparative analysis of three nutrition scores in predicting mortality after acute myocardial infarction. Nutrition. 2021;90:111243. doi:10.1016/j.nut.2021.111243
25. Cinar T, Hayiroglu MI, Seker M, et al. The predictive value of age, creatinine, ejection fraction score for in-hospital mortality in patients with cardiogenic shock. Coron Artery Dis. 2019;30(8):569–574. doi:10.1097/MCA.0000000000000776
26. Tan L, Xu Q, Shi R. A nomogram for predicting hospital mortality in intensive care unit patients with acute myocardial infarction. Int J Gen Med. 2021;14:5863–5877. doi:10.2147/IJGM.S326898
27. Fauchier L, Bisson A, Bodin A, et al. Outcomes in patients with acute myocardial infarction and new atrial fibrillation: a nationwide analysis. Clin Res Cardiol. 2021;110(9):1431–1438. doi:10.1007/s00392-021-01805-2
28. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
29. Hayiroglu MI, Keskin M, Uzun AO, et al. Predictors of in-hospital mortality in patients with ST-segment elevation myocardial infarction complicated with cardiogenic shock. Heart Lung Circ. 2019;28(2):237–244. doi:10.1016/j.hlc.2017.10.023
30. Hayiroglu MI, Canga Y, Yildirimturk O, et al. Clinical characteristics and outcomes of acute coronary syndrome patients with intra-aortic balloon pump inserted in intensive cardiac care unit of a tertiary clinic. Turk Kardiyol Dern Ars. 2018;46(1):10–17. doi:10.5543/tkda.2017.11126
31. Antonelli Incalzi R, Capparella O, Gemma A, et al. Right ventricular aneurysm: a new prognostic indicator after a first acute myocardial infarction. Cardiology. 1991;79(2):120–126. doi:10.1159/000174869
32. Xiao CS, Gao CQ, Li LB, et al. Establishment of a chronic left ventricular aneurysm model in rabbit. J Geriatr Cardiol. 2014;11(2):158–162. doi:10.3969/j.issn.1671-5411.2014.02.009
33. Shimono H, Kajiya T, Inoue H, et al. Left ventricular pseudo-aneurysm with ventricular septal rupture due to anterior ST-segment elevation myocardial infarction. Intern Med. 2019;58(13):1901–1905. doi:10.2169/internalmedicine.2147-18
34. Vallabhajosyula S, Kanwar S, Aung H, et al. Temporal trends and outcomes of left ventricular aneurysm after acute myocardial infarction. Am J Cardiol. 2020;133:32–38. doi:10.1016/j.amjcard.2020.07.043
35. Galiuto L, Barchetta S, Paladini S, et al. Functional and structural correlates of persistent ST elevation after acute myocardial infarction successfully treated by percutaneous coronary intervention. Heart. 2007;93(11):1376–1380. doi:10.1136/hrt.2006.105320
36. Bermudez-Jimenez FJ, Jimenez-Jaimez J, Gonzalez Molina M, et al. Giant biventricular aneurysms: a novel cardiac phenotype in myotubular/centronuclear myopathy. Eur Heart J. 2018;39(48):4289–4290. doi:10.1093/eurheartj/ehy207
37. Khatoon S, Goyfman M, Nabatian S, et al. Inferior wall ST-elevation myocardial infarction complicated by ventricular septal defect and free wall pseudoaneurysm with rupture. Cureus. 2018;10(12):e3805. doi:10.7759/cureus.3805
38. Montone RA, Niccoli G, Crea F, et al. Management of non-culprit coronary plaques in patients with acute coronary syndrome. Eur Heart J. 2020;41(37):3579–3586. doi:10.1093/eurheartj/ehaa481
39. Ling X, Xiang-Hua F, Jun L, et al. Equilibrium radionuclide angiography for evaluating the effect of percutaneous coronary intervention on ventricular aneurysm formation and systolic synchrony in patients with acute myocardial infarction. Int J Cardiovasc Imaging. 2009;25(8):757–763. doi:10.1007/s10554-009-9486-6
40. Davi G, Patrono C. Platelet activation and atherothrombosis. N Engl J Med. 2007;357(24):2482–2494. doi:10.1056/NEJMra071014
41. Ki YJ, Park S, Ha SI, et al. Usefulness of mean platelet volume as a biomarker for long-term clinical outcomes after percutaneous coronary intervention in Korean cohort: a comparable and additive predictive value to high-sensitivity cardiac troponin T and N-terminal pro-B type natriuretic peptide. Platelets. 2014;25(6):427–432. doi:10.3109/09537104.2013.835393
42. Karabacak M, Dogan A, Turkdogan AK, et al. Mean platelet volume is increased in patients with hypertensive crises. Platelets. 2014;25(6):423–426. doi:10.3109/09537104.2013.830181
43. Chu SG, Becker RC, Berger PB, et al. Mean platelet volume as a predictor of cardiovascular risk: a systematic review and meta-analysis. J Thromb Haemost. 2010;8(1):148–156. doi:10.1111/j.1538-7836.2009.03584.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of the Predicting Value of Neutrophil to high-Density Lipoprotein Cholesterol Ratio and Monocyte to high-Density Lipoprotein Cholesterol Ratio for in-Hospital Prognosis and Severe Coronary Artery Stenosis in Patients with ST-Segment Elevation Acute Myocardial Infarction Following Percutaneous Coronary Intervention: A Retrospective Study
Guo J, Chen M, Hong Y, Huang Y, Zhang H, Zhou Y, Zhou B, Fu M
Journal of Inflammation Research 2023, 16:4541-4557
Published Date: 16 October 2023
Construction and Validation of a Predictive Model for Long-Term Major Adverse Cardiovascular Events in Patients with Acute Myocardial Infarction
Yang P, Duan J, Li M, Tan R, Li Y, Zhang Z, Wang Y
Clinical Interventions in Aging 2024, 19:1965-1977
Published Date: 26 November 2024
Risks of Myocardial Infarction and Mortality in Patients with Incident Rheumatoid Arthritis Compared with a Matched General Population: A Danish Nationwide Cohort Study
Løgstrup BB, Ellingsen T, Pedersen AB, Svane HML, Olesen KK, Gyldenkerne C, Hauge EM, Sørensen HT, Bøtker HE, Maeng M
Clinical Epidemiology 2026, 18:568967
Published Date: 24 January 2026