")
Back to Journals » Journal of Inflammation Research » Volume 16
Comparison of the Predicting Value of Neutrophil to high-Density Lipoprotein Cholesterol Ratio and Monocyte to high-Density Lipoprotein Cholesterol Ratio for in-Hospital Prognosis and Severe Coronary Artery Stenosis in Patients with ST-Segment Elevation Acute Myocardial Infarction Following Percutaneous Coronary Intervention: A Retrospective Study
Authors Guo J, Chen M, Hong Y, Huang Y, Zhang H, Zhou Y, Zhou B, Fu M
Received 13 June 2023
Accepted for publication 30 September 2023
Published 16 October 2023 Volume 2023:16 Pages 4541—4557
DOI https://doi.org/10.2147/JIR.S425663
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam D Bachstetter
Jiongchao Guo,1,2 Min Chen,3 Yu Hong,1,2 Yating Huang,1,4 Haiyan Zhang,2 Yuan Zhou,1,2 Bingfeng Zhou,1,5 Minmin Fu1
1Department of Cardiology, The Third Affiliated Hospital of Anhui Medical University (The First People’s Hospital of Hefei), Hefei, Anhui, 230000, People’s Republic of China; 2Graduate School, Anhui Medical University, Hefei, Anhui, 230000, People’s Republic of China; 3Department of Cardiology, the Second People’s Hospital of Hefei, Hefei Hospital Affiliated to Anhui Medical University, Hefei, Anhui, 230000, People’s Republic of China; 4Department of Endocrinology department, the Third Affiliated Hospital of Anhui Medical University (The First People’s Hospital of Hefei), Hefei, Anhui, 230000, People’s Republic of China; 5Department of Cardiology, Hefei BOE Hospital, Hefei, Anhui, 230000, People’s Republic of China
Correspondence: Minmin Fu, Department of Cardiology, the Third Affiliated Hospital of Anhui Medical University (The First People’s Hospital of Hefei), Hefei, Anhui, 230000, People’s Republic of China, Email [email protected] Bingfeng Zhou, Department of Cardiology, The Third Affiliated Hospital of Anhui Medical University (The First People’s Hospital of Hefei), Hefei BOE Hospital, Hefei, Anhui, 230000, People’s Republic of China, Email [email protected]
Background: Neutrophil to high-density lipoprotein cholesterol ratio (NHR) has demonstrated predictive value for coronary artery disease (CAD). However, few research has been conducted on the predictive capacity of NHR for Major Adverse Cardiovascular Events (MACE) following Percutaneous Coronary Intervention (PCI) or the degree of coronary artery stenosis in hospitalized ST-segment elevation myocardial infarction (STEMI) patients.
Methods: The study involved 486 patients diagnosed with STEMI between the years 2020 and 2023. Univariate and multivariate logistic regression analyses were conducted to evaluate the risk factors for MACE after PCI and severe coronary artery stenosis during hospitalization. Receiver operating characteristic (ROC) curves were generated to determine predictive power of NHR and MHR. Spearman correlation analysis was performed to assess the correlation between NHR, MHR and the Gensini score (GS).
Results: Multivariate logistic regression analysis showed that the NHR and MHR were the independent risk factor for MACE during hospitalization in STEMI patients (MHR: the odds ratio (OR)=2.347, 95% confidence interval (CI)=1.082– 5.089, P=0.031) (NHR: OR=1.092, 95% CI=1.025– 1.165, P=0.004). In addition, NHR was also an independent risk factor for high GS (NHR: OR=1.103, 95% CI=1.047– 1.162, P< 0.001), and the MHR was not an independent risk factor. The ROC curve analysis was performed to evaluate the predictive ability of NHR and MHR for in-hospital MACE in STEMI patients after primary PCI. The area under the curve (AUC) for NHR was 0.681. The AUC for MHR was 0.672. Regarding the prediction of high GS, the AUC for NHR was 0.649. The AUC for MHR was 0.587. Spearman correlation analysis showed that NHR exhibited stronger correlation with GS, while MHR was lower (NHR: r=0.291, P< 0.001) (MHR: r=0.156, P< 0.001).
Conclusion: These findings highlight the potential clinical utility of NHR as a predictive indicator in STEMI patients after PCI during hospitalization, both for MACE events and the degree of coronary artery stenosis.
Keywords: neutrophil to high-density lipoprotein cholesterol ratio, monocyte to high-density lipoprotein cholesterol ratio, acute myocardial infarction, coronary artery disease, cardiovascular disease
Introduction
Acute myocardial infarction (AMI), a prominent contributor to morbidity and mortality within the realm of cardiovascular diseases (CVD), holds substantial global significance. In the United States (US), the overall prevalence of AMI among adults aged 20 years and above is estimated to stand at 3.2%, based on NHANES data spanning from 2017 to 2020. In the year 2020 alone, AMI was responsible for approximately 109,199 fatalities in the US.1 The World Bank’s projections indicate an escalating number of AMI cases in China, with estimates reaching 23 million by the year 2030.2 Despite the noteworthy decline in mortality rates attributed to AMI due to the advancements in PCI, the prognosis remains unfavorable. Hence, it holds paramount importance to identify risk factors that can serve as prognostic indicators for patients with AMI, enabling timely intervention.
AMI primarily arises from coronary atherosclerosis, wherein inflammation and abnormal lipid metabolism play pivotal roles in its pathogenesis.3–6 Previous investigations have indicated a strong correlation between the abundance of neutrophils, monocytes, high-density lipoprotein cholesterol (HDL-C), and the occurrence of atherosclerosis and MACE.7–11 Moreover, HDL-C exerts a protective effect against atherosclerosis and MACE by modulating the function of neutrophils and monocytes, inhibiting their activation. Presently, several studies propose that a combination of inflammatory and lipid markers may offer a more comprehensive reflection of CVD prognosis compared to a solitary lipid marker. Notably, MHR and NHR, as novel composite indices, demonstrate predictive value for CAD and MACE.12–14 While the correlation between NHR and STEMI has been explored to a limited extent, no relevant research has been conducted on the prognostic capacity of NHR for MACE following PCI or the degree of coronary artery stenosis in hospitalized STEMI patients, rendering this a relatively novel research avenue.
This study aims to compare the predictive value of NHR and MHR, two indices incorporating inflammation and lipids, in relation to the occurrence of MACE in hospitalized patients with AMI after PCI. Additionally, this study evaluates the predictive value of NHR for extent of coronary artery stenosis assessed by the GS. By doing so, it seeks to further elucidate the significance of NHR and MHR in relation to MACE occurrence in hospitalized patients with AMI after PCI. The results demonstrate that NHR exhibits superior predictive value compared to MHR for MACE. Furthermore, in terms of predicting the degree of coronary artery stenosis as assessed by the GS, NHR shows certain predictive value, while MHR is not a relevant predictor.
Materials and Methods
Study Participants
This retrospective study was conducted at a single center, specifically the Third Affiliated Hospital of Anhui Medical University. The study involved the collection of data from 486 patients diagnosed with STEMI between the years 2020 and 2023 (Figure 1). The inclusion criteria for the study were as follows:1. All patients diagnosed with AMI according to the “2019 Chinese Society of Cardiology guidelines for the diagnosis and management of patients with ST-segment elevation myocardial infarction”. 2. All patients signed an informed consent form and underwent coronary angiography (CAG). 3.Primary PCI was performed to revascularize the culprit vessels, and successful revascularization treatment was anticipated. The following were the exclusion criteria for patient selection: 1. Refuse to undergo CAG or other reasons, the extent of coronary artery lesions is not clear. 2. Patients with severe abnormalities in liver and kidney function, autoimmune diseases, hereditary familial hypercholesterolemia, malignant tumors, or recent severe infections. 3.Patients who had previously undergone PCI or coronary artery bypass grafting for AMI. 4.Cases where primary PCI failed to revascularize the culprit vessels. Following the application of the aforementioned inclusion and exclusion criteria, a total of 486 patients were ultimately enrolled in the study. Among them, the subjects were categorized into two groups: the MACE group (n=148, 30.45%), comprising patients who experienced MACE during hospitalization after PCI, and the Non-MACE group (n=338, 69.55%), comprising patients who did not experience MACE. The study protocol and informed consent procedures were approved by the Ethics Committee of the Third Affiliated Hospital of Anhui Medical University.
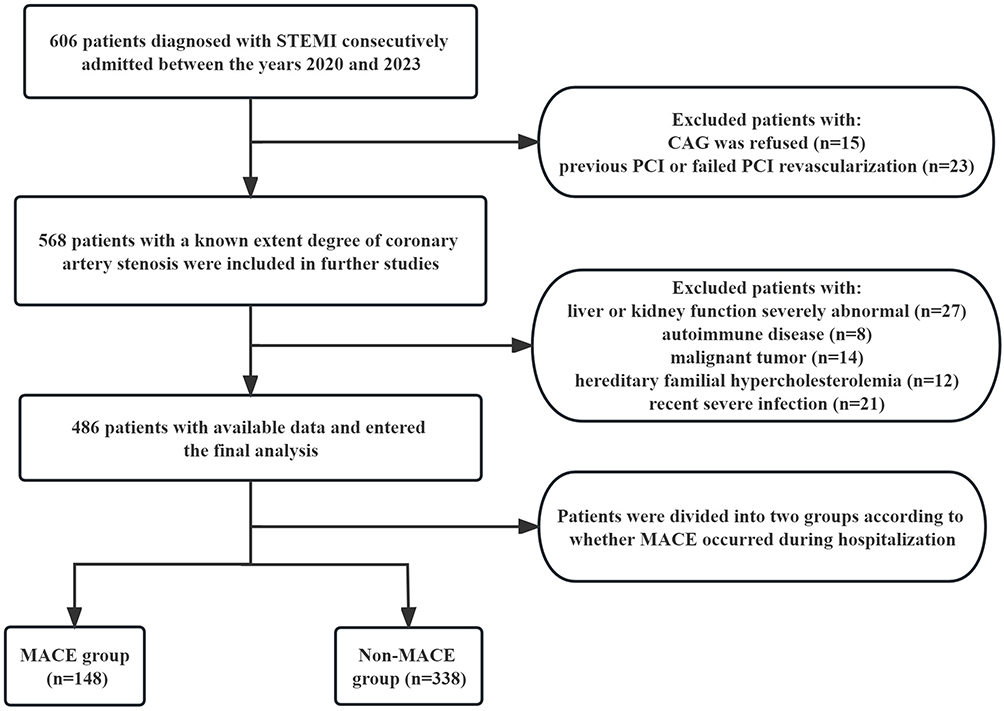 |
Figure 1 Flow chart of the study selection. Abbreviations: MACE, Major adverse cardiovascular event; STEMI St-segment elevation acute myocardial infarction; CAG, coronary arteriography. |
Data Collection and Outcome
The study collected various data from the medical record system, including demographic information of patients (such as gender, age, history of hypertension, diabetes, and stroke), vital sign data (systolic blood pressure, diastolic blood pressure, and heart rate), laboratory data within 24 hours of admission (neutrophils, monocytes, lymphocytes, serum creatinine (sCr), blood urea nitrogen (BUN), uric acid (UA), platelets, albumin (ALB), HDL-C, low-density lipoprotein cholesterol (LDL-C), triglyceride (TG) and fasting plasma glucose (FPG), echocardiography data (left ventricular ejection fraction [LVEF] and left ventricular fractional shortening [LVFS]), as well as data related to CAG (including GS, which reflects the degree of stenosis in coronary artery).
Definitions
In this study, the following definitions were used:
MACE encompassed all-cause mortality, new stroke after AMI, recurrent myocardial infarction, malignant arrhythmia, and new-onset heart failure after AMI.
NHR was defined as the ratio of neutrophils to HDL-C, while MHR represented the ratio of monocytes to HDL-C.
The patients were divided into three groups based on their GS: the low GS group (GS < 44), the medium GS group (GS ≥ 44 and ≤ 80), and the high GS group (GS > 80).
Statistical Analysis
The statistical analysis in this study was performed using IBM SPSS Statistics 26.0 (IBM, New York, NY, USA) and R version 4.2.2 (R Foundation for Statistical Computing, University of Science and Technology of China). Continuous variables were presented as mean ± standard deviation or median (interquartile range). To compare data between two groups, the T test or Mann–Whitney U-test was employed depending on the normality of the data. The non-normally distributed GS data among the three groups were analyzed using the Kruskal–Wallis H-test. Categorical variables were presented as numbers and percentages, and the Chi-square test or Fisher’s exact test was used for statistical analysis. Univariate and multivariate logistic regression analyses were conducted to evaluate the risk factors for MACE after PCI and severe coronary artery stenosis during hospitalization. ROC curves were generated to determine the cut-off values and predictive power of NHR, MHR, and LDL-C/HDL-C. Spearman correlation analysis was performed to assess the correlation between NHR, MHR, LDL-C/HDL-C, and the GS. Except for the LR backward stepwise multivariate logistic regression analysis (where variables with P < 0.05 were included, and variables with P > 0.10 were removed), all statistical tests were two-tailed, and a significance level of P < 0.05 was considered statistically significant.
Result
Baseline Characteristics
In the comparison of baseline characteristics between the in-hospital MACE group and the non-MACE group, the following findings were observed: In the MACE group, the age, neutrophil count, monocyte count, sCr, BUN, UA, HDL-C, FPG, Killip class 2–4, GS, MHR, NHR, and LDL-C/HDL-C were significantly higher compared to the Non-MACE group (P < 0.05) (Table 1) (Figure 2A-D). Systolic blood pressure, diastolic blood pressure, and TG were significantly lower in the MACE group compared to the Non-MACE group (P < 0.05). No significant differences were observed in other indicators between the two groups (P > 0.05) (Table 1).
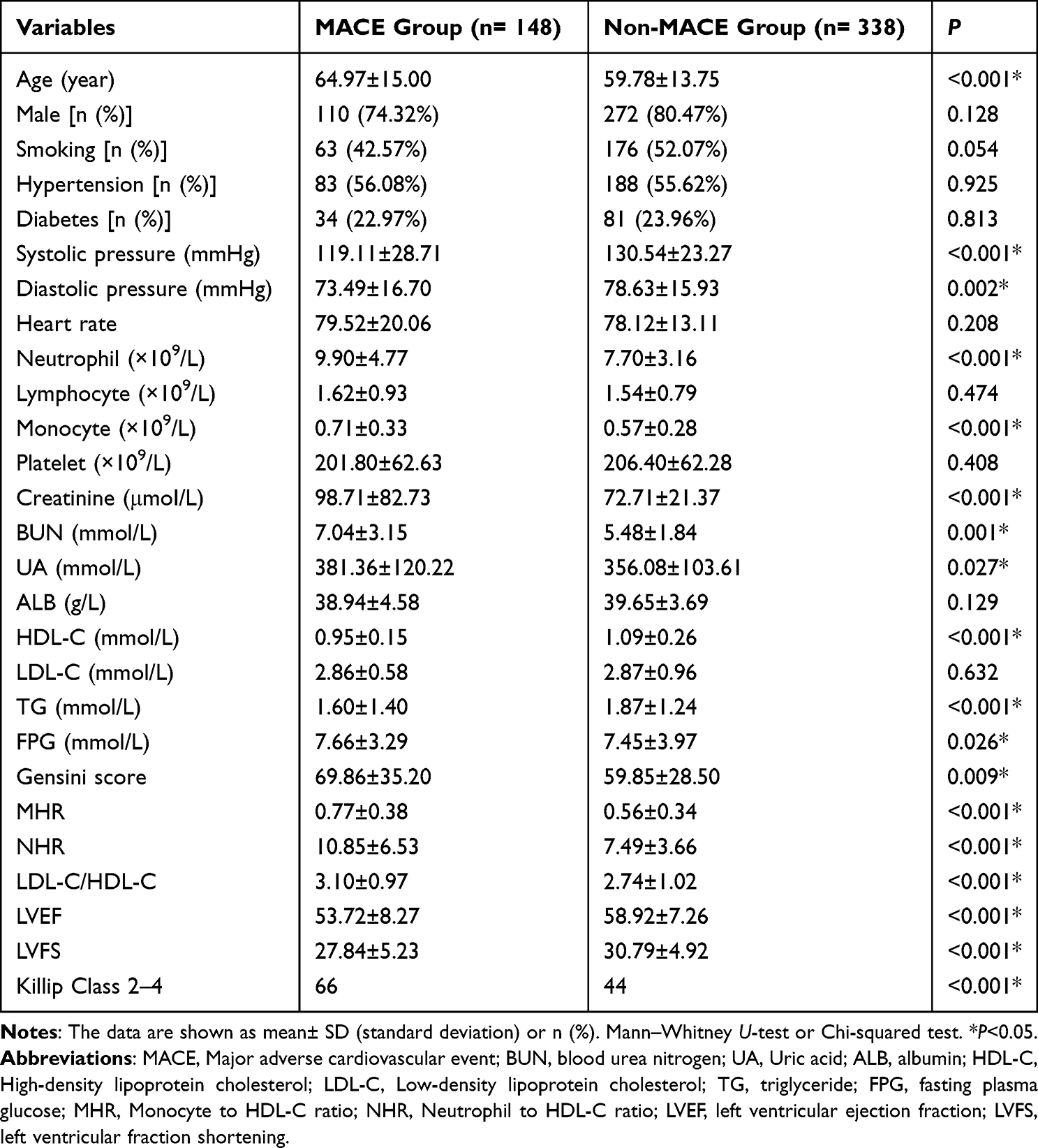 |
Table 1 Baseline Demographic and Clinical Characteristics of the Study Population According to in-Hospital Major Adverse Cardiovascular Events |
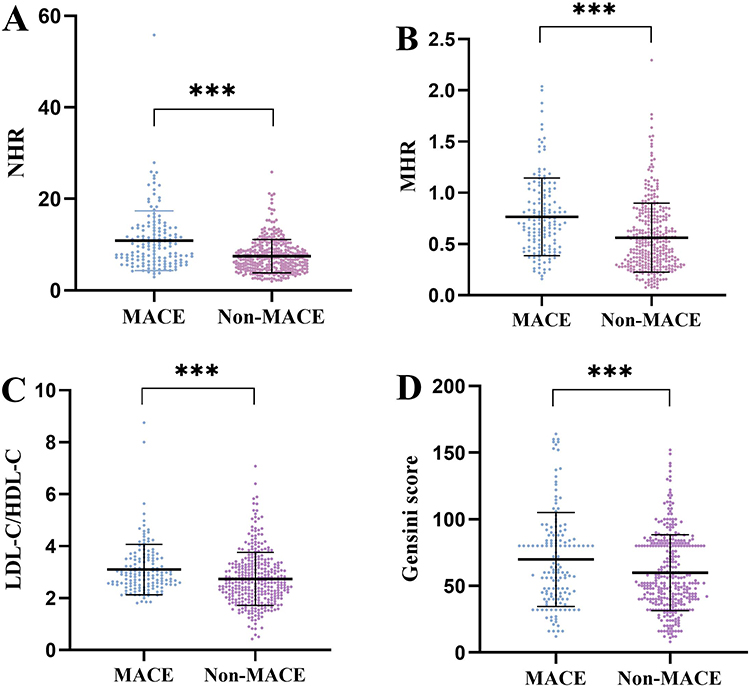 |
Figure 2 (A) Comparison of NHR according to in-hospital major adverse cardiovascular events. (B) Comparison of MHR according to in-hospital major adverse cardiovascular events. (C) Comparison of LDL-C/HDL- according to in-hospital major adverse cardiovascular events. (D) Comparison of Gensini score according to in-hospital major adverse cardiovascular events. ***P<0.001. Abbreviations: NHR, Neutrophil to HDL-C ratio; MHR, Monocyte to HDL-C ratio; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol; MACE, major adverse cardiovascular events. |
Based on the GS, the patients were categorized into three groups: high GS group (GS > 80), medium GS group (44 ≤ GS ≤ 80), and low GS group (GS < 44). The following observations were made: Significant differences were found in age, history of hypertension, heart rate, neutrophils, monocytes, LDL-C, TC, TG, MHR, NHR, and LDL-C/HDL-C (P < 0.05). No significant differences were observed in other indicators (P > 0.05) (Table 2).
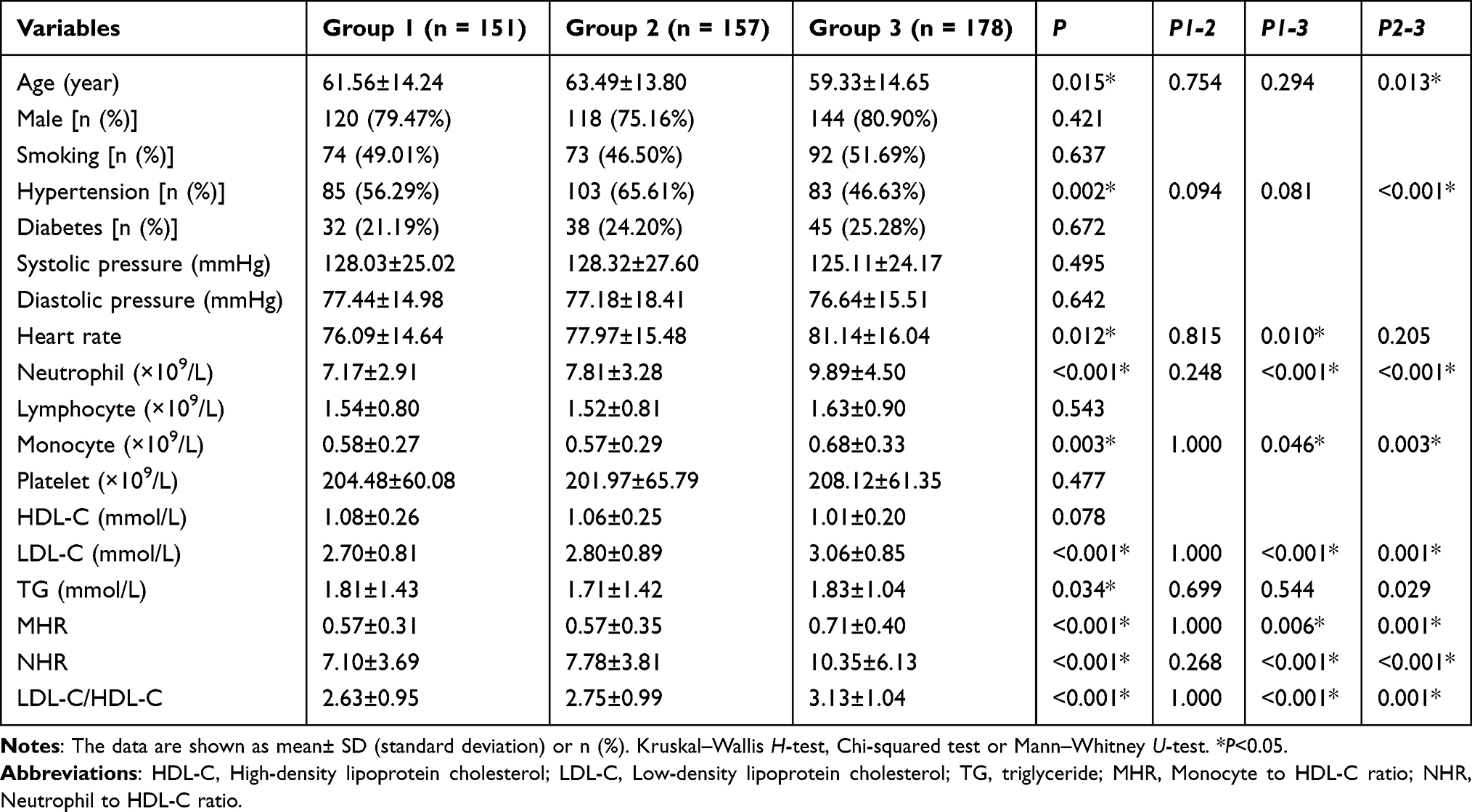 |
Table 2 Comparison of Demographic, Clinical, and Laboratory Characteristics Among the Low Gensini Score Tertile (Group 1: GS<44), Medium Gensini Score Tertile (Group 2: 44≤GS≤80), and High Gensini Score Tertile (Group 3: GS>80) |
After grouping the medium GS group and low GS group as the non-high GS group, a comparison was made between the non-high GS group and the high GS group. The following findings were noted: The high GS group exhibited significantly higher heart rate, neutrophil count, monocyte count, UA, BUN, TG, TC, LDL-C, FPG, NHR, MHR, and LDL-C/HDL-C compared to the non-high GS group (P < 0.05) (Table 3) (Figure 3A-C). The incidence of Anterior MI and Killip class 2–4 was significantly higher in the high GS group than in the non-high GS group (Table 3). No significant differences were observed in other indicators (P > 0.05) (Table 3).
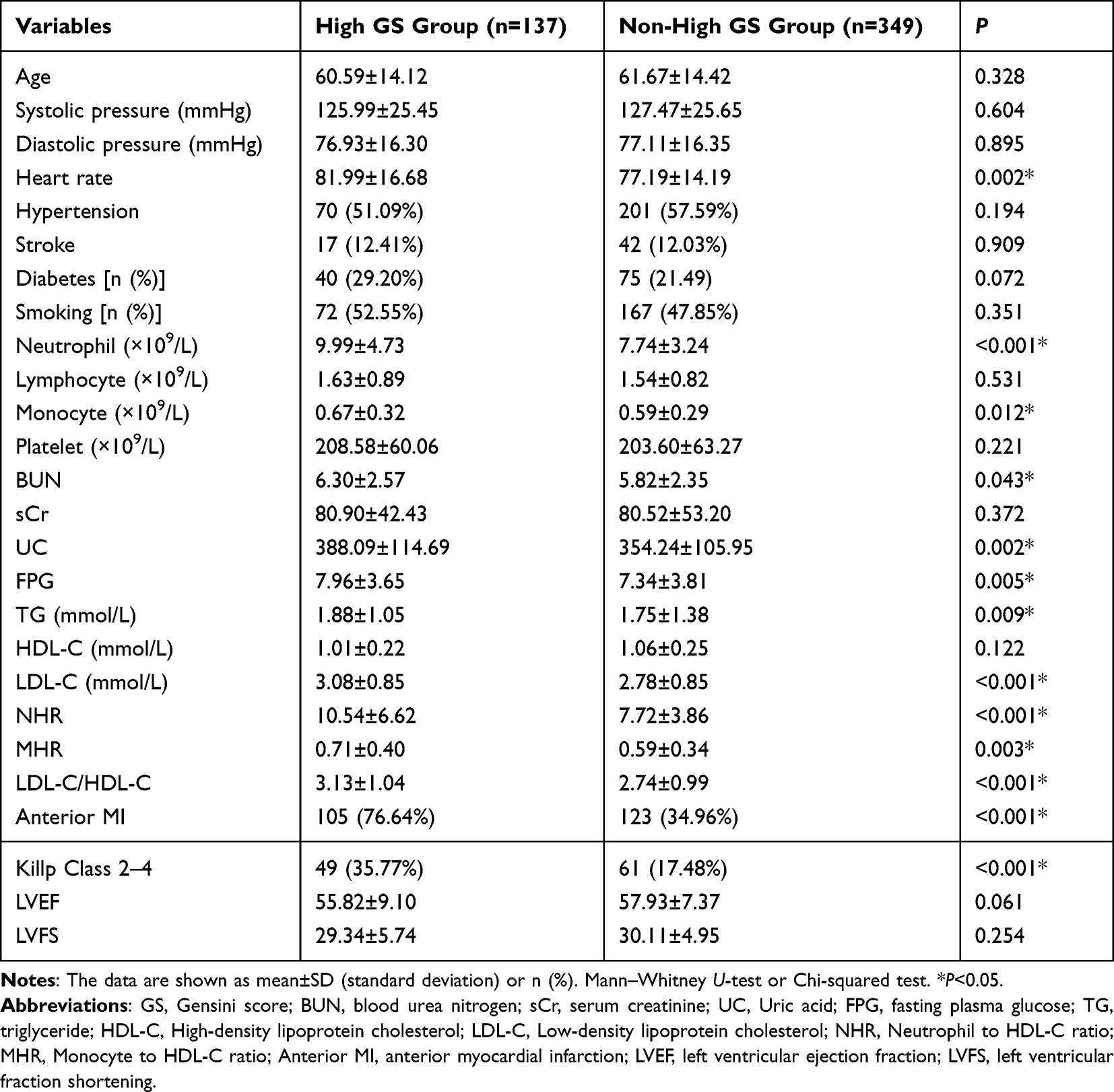 |
Table 3 Comparison of Demographic, Clinical, and Laboratory Characteristics Between the High Gensini Score Group (GS >80 Points) and Non-High Gensini Score Group (GS≤80 Points) |
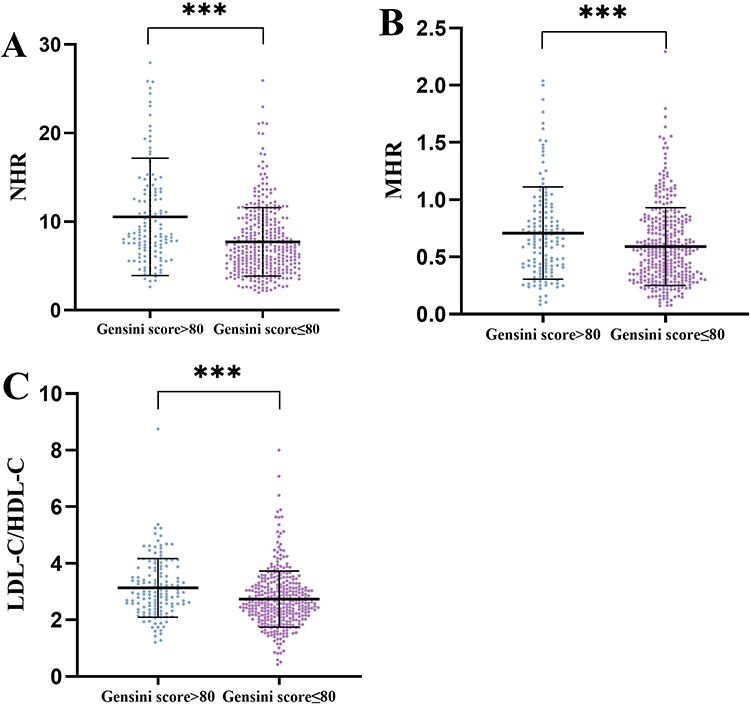 |
Figure 3 (A) Comparison of NHR according to Gensini score>80. (B) Comparison of MHR according to Gensini score>80. (C) Comparison of LDL-C/HDL-C according to Gensini score>80. ***P<0.001. Abbreviations: NHR, Neutrophil to HDL-C ratio; MHR, Monocyte to HDL-C ratio; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol. |
Coronary Angiography and Echocardiography
In the comparison between the MACE group and the Non-MACE group, the following results were observed: The GS of the MACE group was significantly higher compared to the Non-MACE group (P < 0.05). The LVEF and LVFS of the MACE group were significantly lower than those of the Non-MACE group (P < 0.05) (Table 1) (Figure 2D).
In the comparison between the non-high GS group and the high GS group, the following findings were noted: There was no significant difference in LVEF and LVFS between the two groups (P > 0.05) (Table 3).
Univariate and Multivariate Logistic Regression Analysis
Univariate logistic regression analysis was conducted to assess the risk factors of MACE during hospitalization, considering various factors including age, systolic blood pressure, diastolic blood pressure, BUN, sCr, UA, FPG, NHR, MHR, LDL-C/HDL-C, GS, LVEF, and LVFS. The results revealed the following: Age, sCr, BUN, UA, GS, MHR, NHR, LDL/HDL, Killip 2–4, and LVEF were identified as risk factors for MACE in AMI patients during hospitalization after PCI (P < 0.05). Systolic blood pressure, diastolic blood pressure, and TG were identified as protective factors for MACE in STEMI patients during hospitalization after PCI, while FPG did not show statistical significance (P > 0.05) (Table 4).
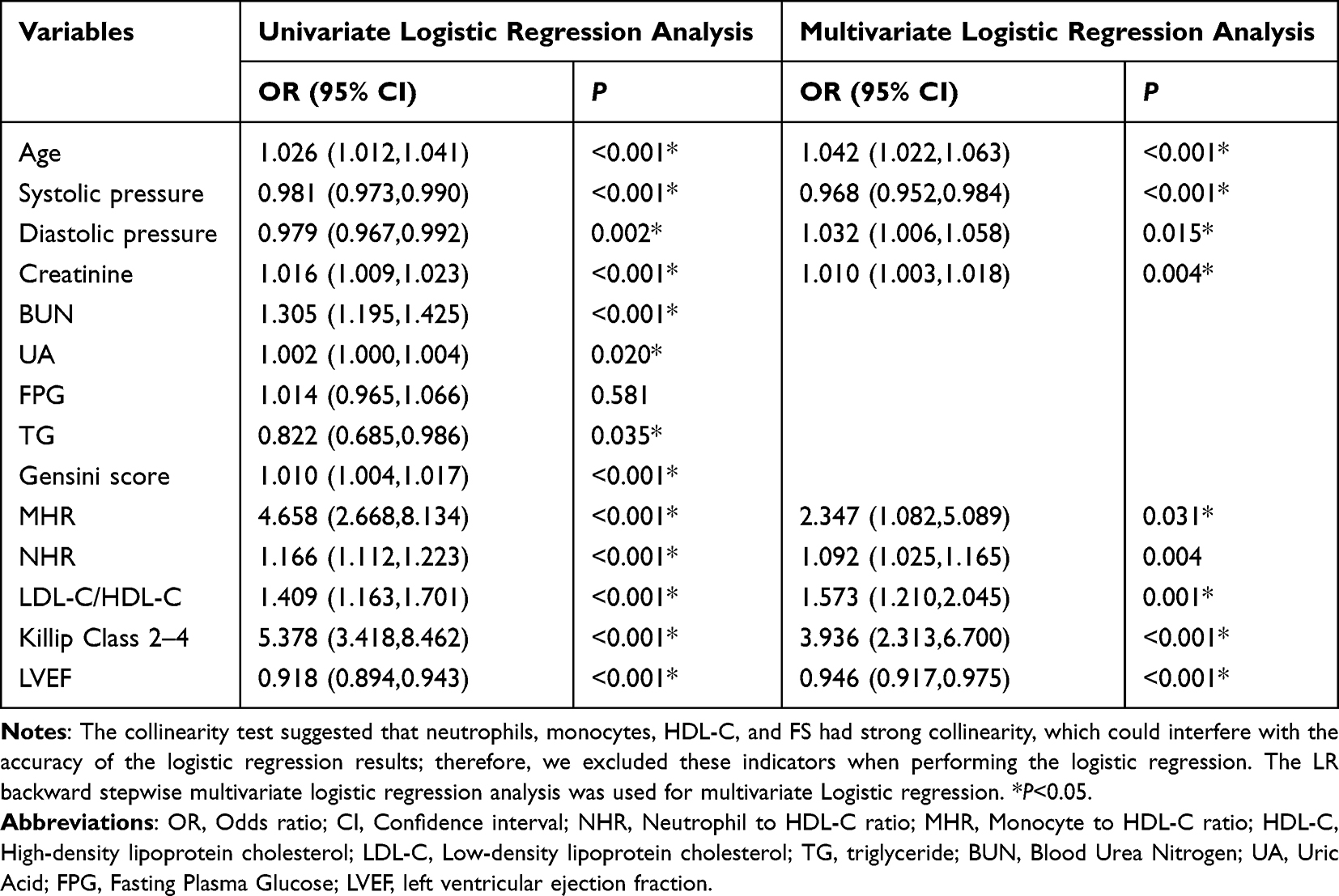 |
Table 4 Univariate Logistic Regression Analysis and Multivariate Logistic Regression Analysis of Selected Variables on in-Hospital Major Adverse Cardiovascular Events |
The significant variables from the univariate regression were included in the LR backward stepwise multivariate regression analysis. After adjusting for factors such as BUN and UA, the multivariate logistic regression analysis revealed that sCr, MHR, NHR, LDL-C/HDL-C, Killip 2–4, and diastolic blood pressure remained as independent risk factors for MACE after primary PCI in patients with STEMI during hospitalization (MHR OR: 2.347, 95% CI: 1.082–5.089, P=0.031) (NHR OR: 1.092, 95% CI: 1.025–1.165, P=0.004) (P < 0.05) (Table 4). Additionally, systolic blood pressure and LVEF were identified as protective factors (P < 0.05) (Table 4). To demonstrate the association of NHR with high GS group, all patients were divided into four groups according to the quartile values of NHR (Q1: NHR ≤ 5.29, Q2: NHR 5.29–7.48, Q3: NHR 7.48–10.49, Q4: NHR > 10.49). The OR value of MACE in the highest quartile compared with the lowest quartile was 6.17 (95% CI: 3.34–11.39, p < 0.001) (Table 5). After adjusting for gender, age, Killip Class 2–4, systolic pressure, diastolic blood pressure, heart rate, smoking, stroke, diabetes, hypertension, Gensini score, platelet counts, FPG, BUN, sCr, UC, ALB, TG, LDL-C, LVEF and LVFS, the risk of MACE remained significantly higher in the highest quartile than in the lowest quartile (OR: 8.15, 95% CI: 3.63–18.29, p <0.001) (Table 5). Finally, after further adjusting for the above confounding factors, the results of a trend analysis suggest that the trend of an increasing probability of MACE occurrence with rising NHR holds statistical significance (OR: 1.79, 95% CI: 1.40–2.30, P < 0.001) (Table 5).
 |
Table 5 Multivariate Logistic Analysis to Determine Associations Between NHR Subgroup Levels and MACE |
Univariate logistic regression analyses were performed for the high GS score group (GS > 80). The results indicated that heart rate, uric acid, TG, NHR, MHR, LDL-C/HDL-C, Killip 2–4, and Anterior MI were risk factors for complex coronary artery lesions. The significant indicators from the univariate regression were included in the backward LR backward multivariate regression analysis. After adjusting for factors such as heart rate, MHR and UA, LDL-C/HDL-C, NHR, Killp2-4 and Anterior MI were identified as independent risk factors for complex coronary artery lesions (NHR: OR:1.103, 95% CI:1.047–1.162, P<0.001) (P < 0.05) (Table 6).
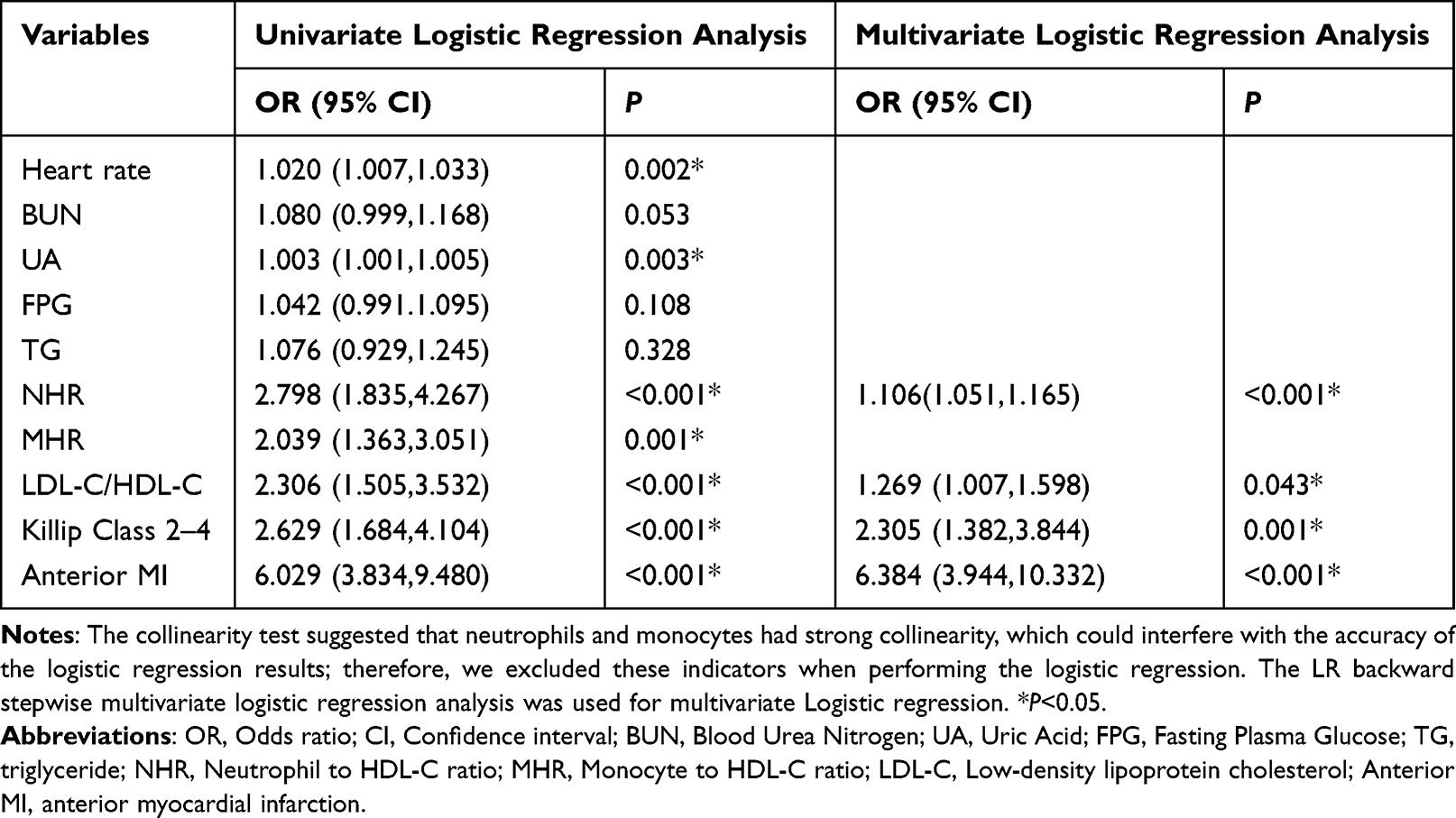 |
Table 6 Univariate and Multivariate Logistic Regression Analysis of Selected Variables on a High Gensini Score (>80 Points) |
To demonstrate the association of NHR with high GS, all patients were divided into four groups according to the quartile values of NHR (Q1: NHR ≤ 5.29, Q2: NHR 5.29–7.48, Q3: NHR 7.48–10.49, Q4: NHR > 10.49, Table 4). The OR value of high GS in the highest quartile compared with the lowest quartile was 4.15 (95% CI: 2.24–7.69, P < 0.001) (Table 7). After adjusting for gender, age, Killip Class 2–4, systolic pressure, diastolic blood pressure, heart rate, smoking, stroke, diabetes, hypertension, platelet counts, FPG, BUN, sCr, UC, ALB, TG, HDL-C, LDL-C, LVEF and LVFS, the risk of high GS remained significantly higher in the highest quartile than in the lowest quartile (OR:3.29, 95% CI: 1.52–7.13, p =0.0025) (Table 7). After further adjusting for the above confounding factors, the results of a trend analysis suggest that the trend of an increasing probability of high GS occurrence with rising NHR holds statistical significance (OR: 1.47, 95% CI: 1.16–1.88, P = 0.0016) (Table 7).
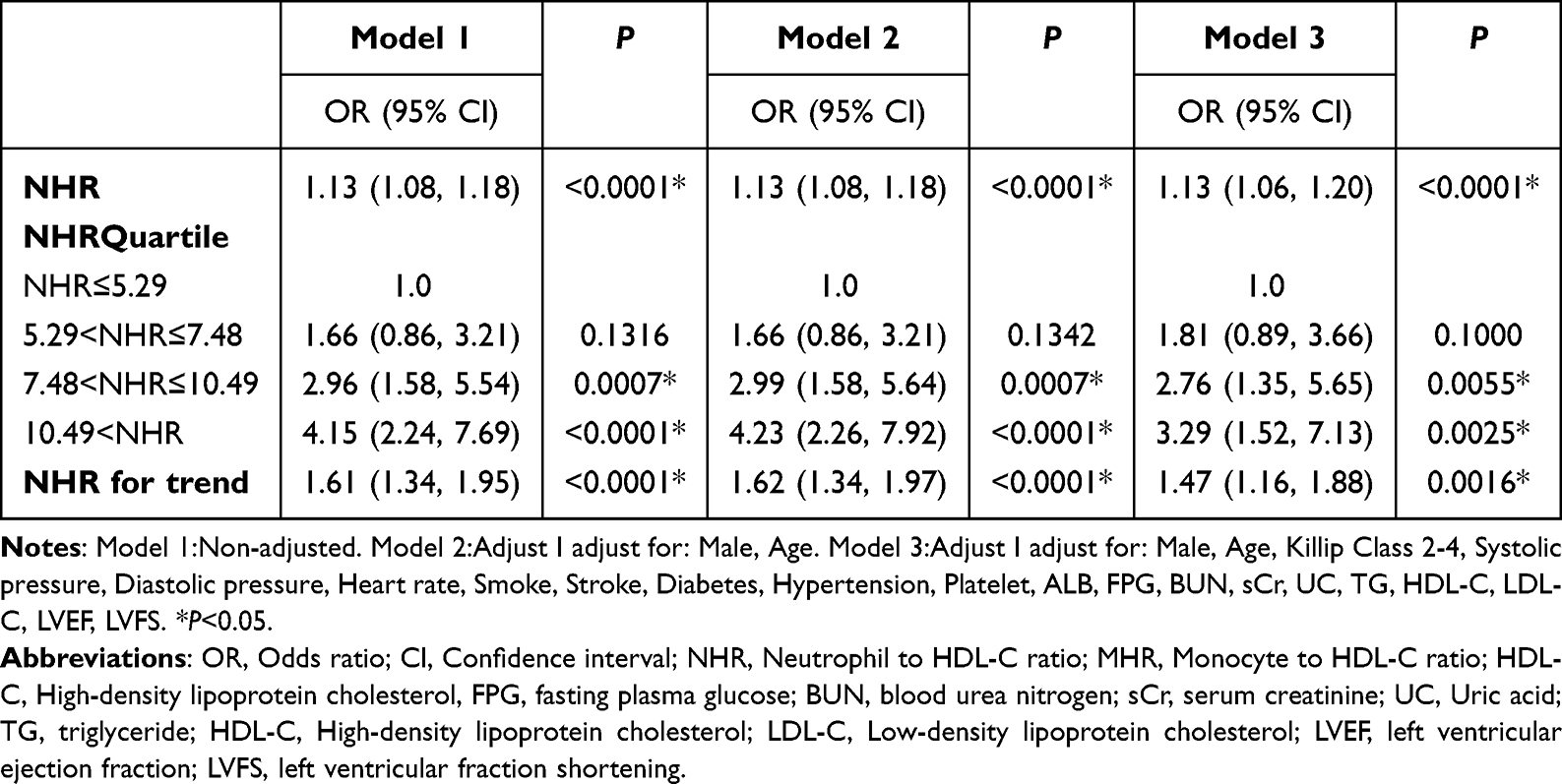 |
Table 7 Multivariate Logistic Analysis to Determine Associations Between NHR Subgroup Levels and High Gensini Score (>80 Points) |
Subgroup Analyses
Herein, subgroup analysis displayed that the tests for the interaction of age (≤ 60 vs > 60), sex (female vs male), systolic blood pressure (≤140vs>140), smoking, stroke, diabetes, hypertension, Gensini score>80, Killip Class 2–4, FPG levels (≤5.6 vs >5.6), HDL-C levels (≤1.1 vs >1.1) and LDL-C (≤2.51 vs 2.51) on the related effects of NHR and MACE were non-significant statistically (all P for interaction > 0.05) (Figure 4). The results showed that the various stratification factors in the model unaffected the correlation between NHR and MACE (Figure 4).
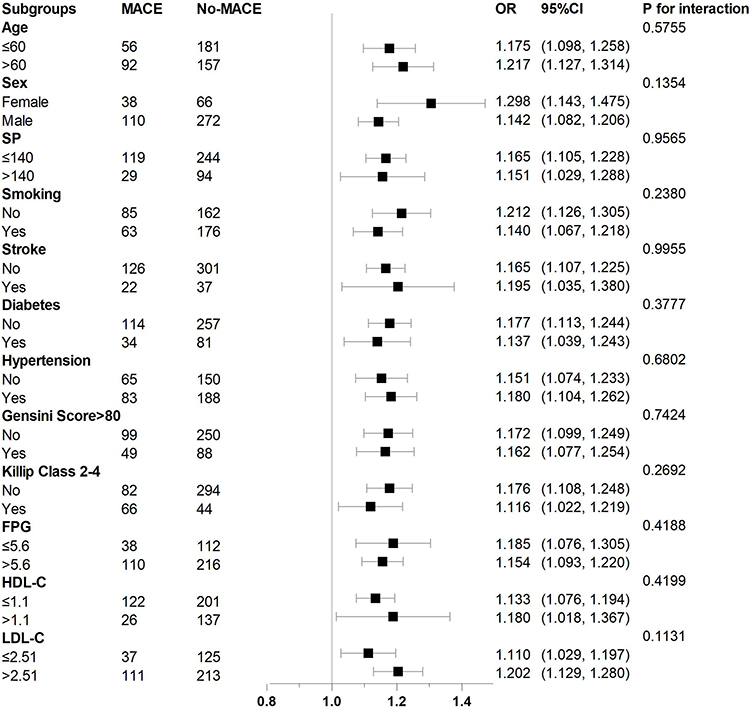 |
Figure 4 Stratified logistic regression analysis model to explore variables affecting the correlation between NHR and MACE. Above model adjusted for age (≤ 60 vs > 60), sex (female vs male), systolic blood pressure (≤140vs>140), smoking, stroke, diabetes, hypertension, Gensini score>80, Killip Class 2–4, FPG levels (≤5.6 vs >5.6), HDL-C levels (≤1.1 vs >1.1) and LDL-C (≤2.51 vs 2.51). Abbreviations: NHR, Neutrophil to HDL-C ratio; MACE, major adverse cardiovascular events; FPG, fasting plasma glucose; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol. |
Another subgroup analysis displayed that the tests for the interaction of age (≤ 60 vs > 60), sex (female vs male), systolic blood pressure (≤140vs >140), smoking, stroke, diabetes, hypertension, Killip Class 2–4, on the related effects of NHR and GS>80 were non-significant statistically (all P for interaction > 0.05) (Figure 5). The results showed that the various stratification factors in the model unaffected the correlation between NHR and GS>80 (Figure 5).
 |
Figure 5 Stratified logistic regression analysis model to explore variables affecting the correlation between NHR and high Gensini score (GS>80). Above model adjusted for age (≤ 60 vs > 60), sex (female vs male), systolic blood pressure (≤140vs > 140), smoking, stroke, diabetes, hypertension, Killip Class 2–4. Abbreviations: NHR, Neutrophil to HDL-C ratio; HDL-C, High-density lipoprotein cholesterol. |
ROC Curve Analysis
The ROC curve analysis was performed to evaluate the predictive ability of NHR, MHR, and LDL-C/HDL-C for in-hospital MACE in AMI patients after primary PCI. The results are as follows: NHR: The AUC for NHR was 0.681 with a 95% CI of (0.629, 0.732) (the specificity was 75.4%, the sensitivity was 52.7%, and the cut-off value was 9.17) (Table 8) (Figure 6A). MHR: The AUC for MHR was 0.672 with a 95% CI of (0.622, 0.722) (the specificity was 68.3%, the sensitivity was 60.1%, and the cut-off value was 0.64) (Table 8) (Figure 6A). LDL-C/HDL-C: The AUC for LDL-C/HDL-C was 0.618 with a 95% CI of (0.568, 0.668) (the specificity was 79.1%, the sensitivity was 45.0%, and the cut-off value was 2.46) (P < 0.05) (Table 8) (Figure 6A).
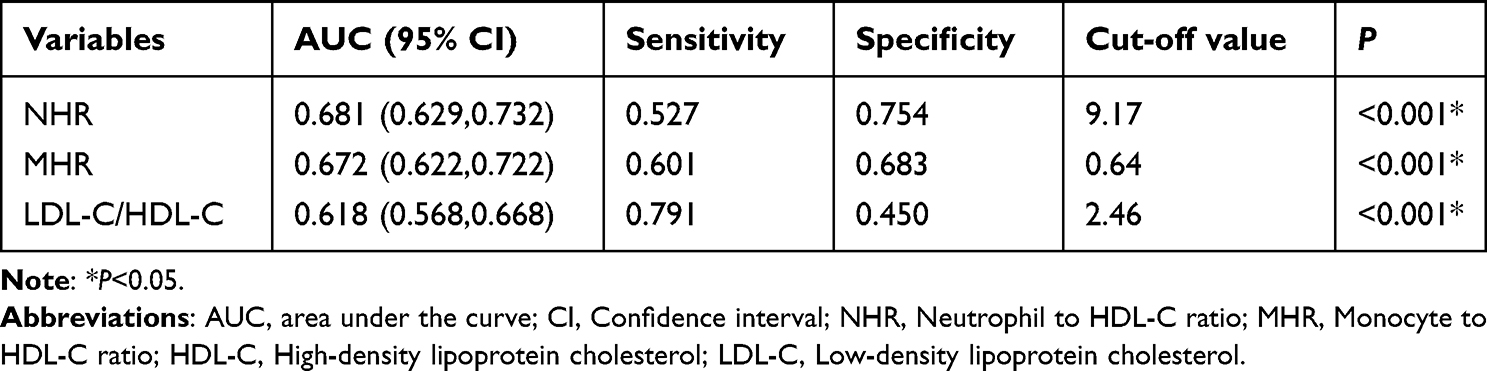 |
Table 8 ROC Curve of NHR, MHR and LDL-C/HDL-C Predicting for MACE After Percutaneous Coronary Intervention PCI in ST-Segment Elevation Acute Myocardial Infarction Patients |
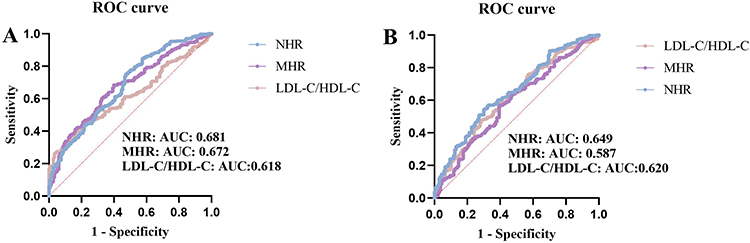 |
Figure 6 (A) ROC curve of NHR, MHR and LDL-C/HDL-C predicting the risk of MACE events during hospitalization in STEMI patients. (B) ROC curve of NHR, MHR and LDL-C/HDL-C predicting the risk of Gensini score>80. Abbreviations: ROC curve, receiver operator characteristic curve; AUC, area under the curve; NHR, Neutrophil to HDL-C ratio; MHR, Monocyte to HDL-C ratio; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol; GS, Gensini score; MACE, major adverse cardiovascular events; STEMI, St-segment Elevation Myocardial Infarction. |
Regarding the prediction of high GS, the ROC curve analysis of NHR, MHR, and LDL-C/HDL-C yielded the following results: NHR: The AUC for NHR was 0.649 with a 95% CI of (0.595, 0.703) (the specificity was 54.4%, the sensitivity was 70.1%, and the cut-off value was 7.24) (Table 9) (Figure 6B). MHR: The AUC for MHR was 0.587 with a 95% CI of (0.531, 0.643) (the specificity was 57.0%, the sensitivity was 60.6%, and the cut-off value was 0.58) (Table 9) (Figure 6B). LDL-C/HDL-C: The AUC for LDL-C/HDL-C was 0.620 with a 95% CI of (0.565, 0.676) (the specificity was 71.5%, the sensitivity was 47.9%, and the cut-off value was 2.57) (P < 0.05) (Table 9) (Figure 6B).
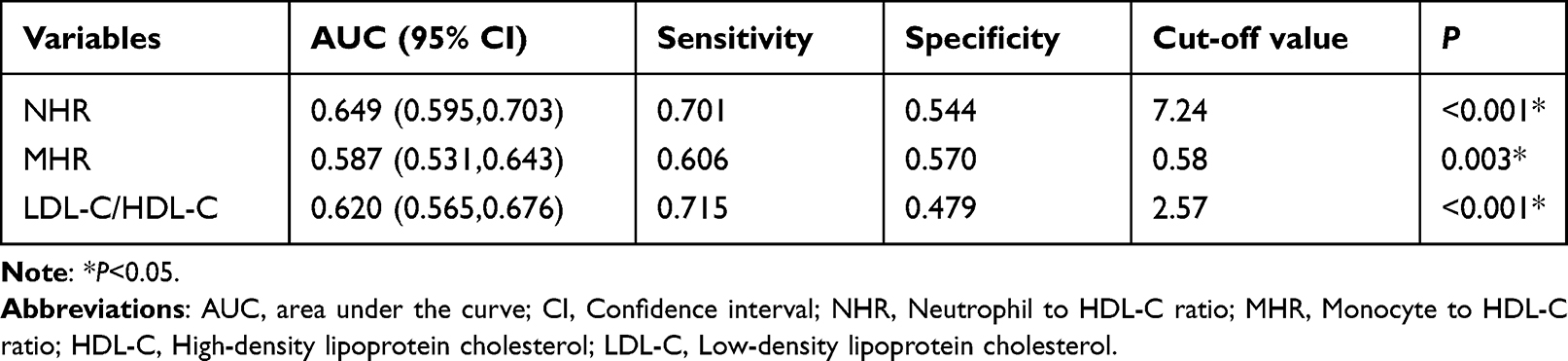 |
Table 9 ROC Curve of NHR, MHR and LDL-C/HDL-C Predicting for ST-Segment Elevation Acute Myocardial Infarction Patients with Gensini Score >80 |
These results indicated that NHR, MHR, and LDL-C/HDL-C have moderate predictive value for in-hospital MACE after primary PCI and NHR have moderate predictive value for high GS in STEMI patients.
Correlation of MHR, NHR, LDL-C/HDL-C and GS
The Spearman correlation analysis was conducted to examine the correlation between NHR, MHR, LDL-C/HDL-C, and GS. The results are as follows: NHR showed a significant correlation with GS (r=0.291, P<0.05) (Table 10) (Figure 7A). This indicates a moderate positive correlation between MHR and the severity of coronary artery lesions. MHR exhibited a lower correlation with GS compared to NHR (r=0.156, P<0.05) (Table 10) (Figure 7B). This suggests a weaker positive correlation between NHR and the severity of coronary artery lesions. LDL-C/HDL-C demonstrated a moderate positive correlation with GS (r=0.217, P<0.05) (Table 10) (Figure 7C). This implies that higher LDL-C/HDL-C are associated with increased severity of coronary artery lesions.
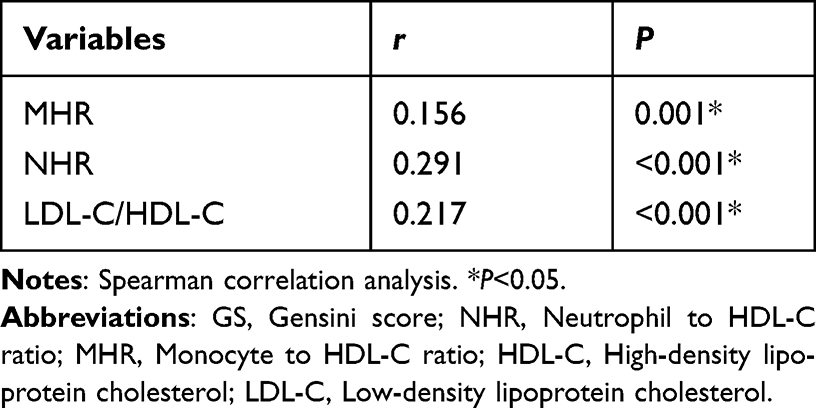 |
Table 10 Correlation of NHR, MHR and LDL-C/HDL-C with GS |
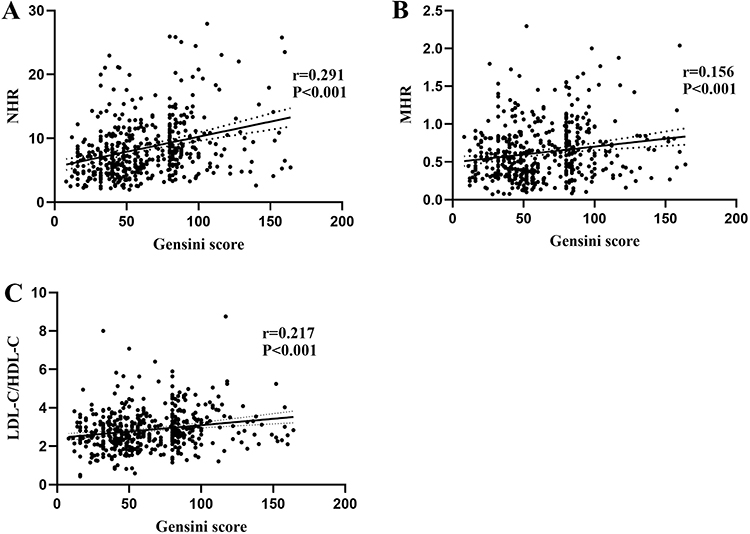 |
Figure 7 (A) Correlation of NHR with Gensini score (Spearman correlation analysis). (B) Correlation of MHR with Gensini score (Spearman correlation analysis). (C) Correlation of LDL-C/HDL-C with Gensini score (Spearman correlation analysis). Abbreviations: NHR, Neutrophil to HDL-C ratio; MHR, Monocyte to HDL-C ratio; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol. |
These findings suggest that MHR, NHR, and LDL-C/HDL-C are correlated with the degree of stenosis reflected by the GS. Among these variables, MHR exhibited the strongest correlation, followed by LDL-C/HDL-C, while NHR had the lowest correlation.
Discussion
The main finding of this study suggests that NHR has a better predictive value for the occurrence of MACE in hospitalized STEMI patients after PCI compared to MHR. Additionally, NHR demonstrates a potential predictive value for the degree of coronary artery stenosis as assessed by the GS. This study is unique in that it explores the predictive value of NHR in relation to MACE occurrence and coronary artery stenosis severity in hospitalized STEMI patients after PCI, an area that has not been extensively studied before.
The development of AMI is primarily attributed to vascular stenosis, myocardial ischemia, hypoxia, and myocardial injury resulting from coronary atherosclerosis.15 Inflammation and dyslipidemia play significant roles in the progression of atherosclerosis.3–6,16 However, relying solely on individual lipid levels or inflammatory markers may not provide sufficient accuracy in predicting the outcomes of AMI patients after PCI. Therefore, this study sought to investigate the association between NHR, MHR, and AMI, taking into consideration both inflammation and dyslipidemia aspects. By examining the combined inflammatory lipid markers, this study aimed to uncover potential relationships between these markers and the occurrence of MACEs as well as the severity of CAD in hospitalized AMI patients after PCI. The findings contribute to a deeper understanding of the complex interplay between inflammation, dyslipidemia, and adverse outcomes in AMI patients undergoing PCI.
STEMI primarily arises from thrombosis as a result of the rupture of coronary atherosclerotic plaques triggered by inflammation and abnormal lipid metabolism.5,17 Atherosclerosis is a complex process in which lipids interplay with immune-inflammatory cells. Research has demonstrated that inflammatory cell-derived substances possess the capability to instigate coagulation system activation, even in the absence of conventional risk factors, emphasizing the pivotal role of inflammatory system dysregulation in pathological thrombosis.18
During the progression of atherosclerosis, there is a substantial increase in the abundance of inflammatory immune cells such as monocytes and neutrophils. Monocytes have the ability to migrate into the vascular endothelium, where they transform into macrophages and express scavenger receptors crucial for the uptake of oxidized low-density lipoprotein cholesterol (OX-LDL-C). Upon the engulfment of oxidized LDL-C and other lipids, monocytes develop into foam cells, depositing within the intima of blood vessels to form atherosclerotic plaques, a significant contributor to the development of coronary atherosclerosis.
Despite being overlooked in cardiovascular research for a long time, the past decade has uncovered the significant regulatory role of neutrophils in cardiovascular inflammation. Neutrophils are implicated in all stages of atherosclerosis and have emerged as a crucial therapeutic target for the development of cardiovascular disease drugs.19 Studies have demonstrated a positive correlation between the extent of hypercholesterolemia-induced neutrophilia and the formation of early atherosclerotic lesions, which can influence atherosclerotic plaques and provoke thrombotic complications associated with atherosclerosis.20 Neutrophils release decondensed nucleosomes known as neutrophil extracellular traps (NETs), which induce platelet activation and initiate coagulation. Moreover, neutrophils secrete various pro-coagulant granzymes, collectively contributing to thrombosis formation and subsequent AMI.21
In AMI, neutrophils are recruited to the infarcted myocardium within the initial hours to initiate localized inflammation and tissue damage. The primary function of recruited neutrophils is to eliminate necrotic tissue from the site of myocardial injury.22 Unfortunately, neutrophils also exacerbate myocardial tissue destruction by releasing myeloperoxidase (MPO) and reactive oxygen species (ROS), which are associated with a poor prognosis in AMI patients.23 Nevertheless, neutrophils possess a dual role in cardiovascular inflammation, as they also play a reparative role.19 In addition, neutrophil-derived mediators regulate the functions of monocytes, macrophages, and dendritic cells, including recruitment, phagocytic capacity, and cytokine release.24,25 Previous investigations have demonstrated a high abundance of neutrophils in ruptured carotid plaques, suggesting a correlation between neutrophil count and the susceptibility to arterial plaque rupture.26 And the thrombosis secondary to plaque rupture represents the primary pathogenesis of STEMI.
In contrast to monocytes and neutrophils, HDL-C is recognized as a protective factor against atherosclerosis and cardiovascular risk.7,8 However, findings from Mendelian randomization studies suggest that HDL-C levels likely serve as a risk marker rather than a causative factor specific to cardiovascular events.27,28 HDL-C exerts its protective effects by facilitating reverse cholesterol transport, thereby reducing intravascular lipid deposition. Additionally, it attenuates atherosclerosis by inhibiting monocyte formation, decreasing monocyte recruitment to the arterial wall, and subsequently suppressing the inflammatory response.29–33
NHR and MHR are novel indicators that reflect the interplay between inflammation and lipid metabolism. MHR represents the ratio of monocytes to HDL-C. Numerous studies have identified MHR as an independent risk factor for all-cause mortality and MACE in patients with STEMI after PCI.13,34,35 Wu TT et al demonstrated that MHR is also predictive of long-term outcomes in patients with AMI after PCI.36 Moreover, a study by E.T. Figueiredo et al indicated that MHR can provide prognostic value in acute coronary syndrome (ACS) patients to a certain extent.12 Similarly, MHR represents the ratio of neutrophils to HDL-C, is also a risk factor for MACE in patients after PCI.14 However, limited research has investigated the correlation between NHR and myocardial infarction, and there is currently a lack of studies examining the predictive value of NHR for both MACE occurrence and the extent of coronary artery stenosis in hospitalized AMI patients after PCI. Therefore, this research direction represents a relatively novel area of investigation.
In clinical practice, despite significant advancements in coronary intervention technology and PCI, the prognosis for patients with AMI remains challenging, with a high incidence of MACE. In this context, the use of NHR as a low-cost and readily available indicator holds promise in predicting the occurrence of MACE. Such prognostic information is invaluable for healthcare professionals, as it enables timely and appropriate interventions to prevent MACE and improve the overall prognosis of AMI patients.
Moreover, it is important to recognize that certain patients may not be suitable candidates for PCI due to factors such as hemodynamic instability, surgical refusal by family members, intervention time constraints, or limited hospital resources. In these situations, NHR can serve as an initial assessment tool for estimating the degree of coronary artery stenosis. This preliminary evaluation aids clinicians in determining appropriate symptomatic treatments for patients who cannot undergo immediate PCI.
This study aimed to compare the predictive value of NHR and MHR in predicting the occurrence of MACE in STEMI patients during hospitalization after PCI. Additionally, the study investigated their predictive value for evaluating the degree of coronary artery stenosis assessed by GS. The findings further support the superiority of NHR compared with MHR in predicting the occurrence of MACE in STEMI patients during hospitalization after PCI. Furthermore, the study suggests that NHR holds value in predicting the degree of coronary artery stenosis assessed by GS, whereas MHR does not appear to be a relevant predictor in this context. Therefore, compared to MHR, NHR may serve as a superior indicator for predicting the occurrence of MACE and the degree of coronary artery stenosis in STEMI patients during hospitalization undergoing PCI.
Limitation
However, it is important to acknowledge several limitations in this study. Firstly, the retrospective nature and single-center design introduce potential biases that may limit the generalizability of the findings. Further studies conducted in multiple centers and with prospective designs are needed to validate the results. Secondly, the sample size in this study was relatively small and restricted to a specific region, which may affect the statistical power and external validity of the findings. Future studies with larger sample sizes and diverse populations are warranted. Thirdly, this study primarily focused on short-term prognosis during hospitalization, and the long-term prognostic value of NHR requires investigation through prospective studies. Furthermore, we have excluded patients who previously underwent PCI, or in cases where primary PCI failed to revascularize the culprit vessels. This decision was prompted by our consideration of the possibility that patients with a history of PCI may have experienced myocardial injury events. In most cases, individuals who have not successfully undergone vascular reconstruction exhibit myocardial injury levels surpassing those who have promptly undergone revascularization. As a result, the likelihood of MACE may experience an increase. Consequently, the correlation analysis involving NHR within these two distinct patient cohorts may yield disparate outcomes, and whether NHR has predictive value for prognosis and the degree of vascular stenosis in patients who primary PCI failed to revascularize the culprit vessels or previous undergo PCI requires further investigation.
Conclusion
The findings confirmed the significance of NHR and MHR in predicting MACE in this patient population, with NHR showing a higher predictive value. Furthermore, the study indicated that NHR holds value in predicting the degree of coronary artery stenosis assessed by GS, while MHR does not possess relevant predictive capability in this regard. These findings highlight the potential clinical utility of NHR as a predictive indicator in STEMI patients after PCI during hospitalization, both for MACE events and the degree of coronary artery stenosis.
Abbreviations
NHR, neutrophil to high-density lipoprotein cholesterol ratio; MHR, monocyte to high-density lipoprotein cholesterol ratio; CAD, coronary artery disease; MACE, major adverse cardiovascular events; STEMI, ST-segment elevation acute myocardial infarction; PCI, percutaneous coronary intervention; CVD, cardiovascular diseases; US, the United States; AMI, acute myocardial infarction; HDL-C, high-density lipoprotein cholesterol; GS, Gensini score; CAG, coronary angiography; sCr, serum creatinine; BUN, blood urea nitrogen; UA, uric acid; ALB, albumin; LDL-C, low-density lipoprotein cholesterol; TG, triglyceride; FPG, fasting plasma glucose; LVEF, left ventricular ejection fraction; LVFS, left ventricular fractional shortening; CI, confidence interval; OX-LDL-C, oxidized low-density lipoprotein cholesterol; NETs, neutrophil extracellular traps; MPO, myeloperoxidase; ROS, reactive oxygen species; ACS, acute coronary syndrome; ROC curves, Receiver operating characteristic curves; OR, the odds ratio.
Ethics Approval and Consent to Participate
The study protocol and informed consent procedures were approved by the Ethics Committee of the Third Affiliated Hospital of Anhui Medical University. All methods were performed following the Declaration of Helsinki. Informed written consent for publication without direct personal identification details (such as name and address) was obtained from all the participants.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding authors, Minmin Fu and Bingfeng Zhou, upon a reasonable request. The data are not publicly available due to their containing information that could compromise the privacy of patients.
Acknowledgments
The authors would like to extend their sincere thanks to YT H, HY Z and YZ for their contribution to data collection. We also extend our gratitude to JC G, MC, YH, BF Z and MM F for their contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Natural Science Project of Anhui Medical University in 2022 (2022xkj242).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics-2023 Update: a Report From the American Heart Association. Circulation. 2023;147(8):e93–e621. doi:10.1161/CIR.0000000000001123
2. bank Tw. Toward a Healthy and Harmonious Life in China: Stemming the Rising Tide of Non-Communicable Diseases. World Bank Report; 2014.
3. Libby P. Inflammation in Atherosclerosis. Arterioscler Thromb Vasc Biol. 2012;32(9):2045–2051. doi:10.1161/atvbaha.108.179705
4. Schaftenaar F, Frodermann V, Kuiper J, Lutgens E. Atherosclerosis: the interplay between lipids and immune cells. Curr Opin Lipidol. 2016;27(3):209–215. doi:10.1097/MOL.0000000000000302
5. Libby P, Theroux P. Pathophysiology of coronary artery disease. Circulation. 2005;111(25):3481–3488. doi:10.1161/CIRCULATIONAHA.105.537878
6. Pepine CJ, Nichols WW. The pathophysiology of chronic ischemic heart disease. Clin Cardiol Feb. 2007;30(2 Suppl 1):I4–9. doi:10.1002/clc.20048
7. Silbernagel G, Schottker B, Appelbaum S, et al. High-density lipoprotein cholesterol, coronary artery disease, and cardiovascular mortality. Eur Heart J. 2013;34(46):3563–3571. doi:10.1093/eurheartj/eht343
8. Gordon DJ, Probstfield JL, Garrison RJ, et al. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation. 1989;79(1):8–15. doi:10.1161/01.cir.79.1.8
9. Weber C, Noels H. Atherosclerosis: current pathogenesis and therapeutic options. Nat Med. 2011;17(11):1410–1422. doi:10.1038/nm.2538
10. Matthias Nahrendorf FKS. Immunology. Neutrophil-macrophage communication in inflammation and atherosclerosis. Science. 2015;349(6245):237. doi:10.1126/science.aac7801
11. Woollard KJ, Geissmann F. Monocytes in atherosclerosis: subsets and functions. Nat Rev Cardiol. 2010;7(2):77–86. doi:10.1038/nrcardio.2009.228
12. Figueiredo ET, Miranda CH. Is the variation in monocyte to high-density lipoprotein cholesterol ratio a predictor of major cardiovascular events after acute coronary syndrome? Braz J Med Biol Res. 2023;55:e12410. doi:10.1590/1414-431X2022e12410
13. Villanueva DLE, Tiongson MD, Ramos JD, Llanes EJ. Monocyte to High-Density Lipoprotein Ratio (MHR) as a predictor of mortality and Major Adverse Cardiovascular Events (MACE) among ST Elevation Myocardial Infarction (STEMI) patients undergoing primary percutaneous coronary intervention: a meta-analysis. Lipids Health Dis. 2020;19(1):55. doi:10.1186/s12944-020-01242-6
14. Chen Y, Jiang D, Tao H, Ge P, Duan Q. Neutrophils to high-density lipoprotein cholesterol ratio as a new prognostic marker in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: a retrospective study. BMC Cardiovasc Disord. 2022;22(1):434. doi:10.1186/s12872-022-02870-9
15. Boateng S, Sanborn T. Acute myocardial infarction. Dis Mon. 2013;59(3):83–96. doi:10.1016/j.disamonth.2012.12.004
16. Stein R, Ferrari F, Scolari F. Genetics, Dyslipidemia, and Cardiovascular Disease: new Insights. Curr Cardiol Rep. 2019;21(8):67.
17. Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and rupture. Circ Res. 2014;114(12):1852–1866. doi:10.1161/CIRCRESAHA.114.302721
18. Swystun LL, Liaw PC. The role of leukocytes in thrombosis. Blood. 2016;128(6):753–762. doi:10.1182/blood-2016-05-718114
19. Silvestre-Roig C, Braster Q, Ortega-Gomez A, Soehnlein O. Neutrophils as regulators of cardiovascular inflammation. Nat Rev Cardiol. 2020;17(6):327–340. doi:10.1038/s41569-019-0326-7
20. Drechsler M, Megens RT, van Zandvoort M, Weber C, Soehnlein O. Hyperlipidemia-triggered neutrophilia promotes early atherosclerosis. Circulation. 2010;122(18):1837–1845. doi:10.1161/CIRCULATIONAHA.110.961714
21. Pircher J, Czermak T, Ehrlich A, et al. Cathelicidins prime platelets to mediate arterial thrombosis and tissue inflammation. Nat Commun. 2018;9(1):1523. doi:10.1038/s41467-018-03925-2
22. Yonggang Ma AY, Merry L. Neutrophil roles in left ventricular remodeling following myocardial infarction. Fibrogenesis Tissue Repair. 2013;6:11. doi:10.1186/1755-1536-6-11
23. Daseke MJ, Valerio FM, Kalusche WJ, Ma Y, DeLeon-Pennell KY, Lindsey ML. Neutrophil proteome shifts over the myocardial infarction time continuum. Basic Res Cardiol. 2019;114(5):678.
24. Soehnlein O, Weber C, Lindbom L. Neutrophil granule proteins tune monocytic cell function. Trends Immunol. 2009;30(11):538–546. doi:10.1016/j.it.2009.06.006
25. Soehnlein O, Zernecke A, Eriksson EE, et al. Neutrophil secretion products pave the way for inflammatory monocytes. Blood. 2008;112(4):1461–1471. doi:10.1182/blood-2008-02-139634
26. Ionita MG, van den Borne P, Catanzariti LM, et al. High neutrophil numbers in human carotid atherosclerotic plaques are associated with characteristics of rupture-prone lesions. Arterioscler Thromb Vasc Biol. 2010;30(9):1842–1848. doi:10.1161/ATVBAHA.110.209296
27. Hassan M, Philip P. CANHEART: is HDL cholesterol a cardiovascular specific risk factor? Glob Cardiol Sci Pract. 2016;2016(4):e201634. doi:10.21542/gcsp.2016.34
28. Voight BF, Peloso GM, Orho-Melander M, et al. Plasma HDL cholesterol and risk of myocardial infarction: a Mendelian randomisation study. Lancet. 2012;380(9841):572–580. doi:10.1016/s0140-6736(12)60312-2
29. Rosenson RS, Brewer HB Jr, Ansell BJ, et al. Dysfunctional HDL and atherosclerotic cardiovascular disease. Nat Rev Cardiol. 2016;13(1):48–60. doi:10.1038/nrcardio.2015.124
30. Maiolino G, Rossitto G, Caielli P, Bisogni V, Rossi GP, Calo LA. The role of oxidized low-density lipoproteins in atherosclerosis: the myths and the facts. Mediators Inflamm. 2013;2013:714653. doi:10.1155/2013/714653
31. Parthasarathy JB S, Fong LG. High-density lipoprotein inhibits the oxidative modification of low-density lipoprotein. Biochim Biophys Acta. 1990.
32. Murphy AJ, Woollard KJ, Hoang A, et al. High-density lipoprotein reduces the human monocyte inflammatory response. Arterioscler Thromb Vasc Biol. 2008;28(11):2071–2077. doi:10.1161/ATVBAHA.108.168690
33. Yvan-Charvet L, Pagler T, Gautier EL, et al. ATP-binding cassette transporters and HDL suppress hematopoietic stem cell proliferation. Science. 2010;328(5986):1689–1693. doi:10.1126/science.1189731
34. Acikgoz SK, Acikgoz E, Sensoy B, Topal S, Aydogdu S. Monocyte to high-density lipoprotein cholesterol ratio is predictive of in-hospital and five-year mortality in ST-segment elevation myocardial infarction. Cardiol J. 2016;23(5):505–512. doi:10.5603/CJ.a2016.0026
35. Karatas MB, Canga Y, Ozcan KS, et al. Monocyte to high-density lipoprotein ratio as a new prognostic marker in patients with STEMI undergoing primary percutaneous coronary intervention. Am J Emerg Med. 2016;34(2):240–244. doi:10.1016/j.ajem.2015.10.049
36. Wu TT, Zheng YY, Chen Y, Yu ZX, Ma YT, Xie X. Monocyte to high-density lipoprotein cholesterol ratio as long-term prognostic marker in patients with coronary artery disease undergoing percutaneous coronary intervention. Lipids Health Dis. 2019;18(1):180. doi:10.1186/s12944-019-1116-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.