Back to Journals » Patient Preference and Adherence » Volume 16
Determinants of Adherence to Antihypertensives Among Elderly: A Multifactorial Concern
Authors Sheilini M ![]() , Hande HM, Devi ES, Kamath A, Nayak BS, Morisky DE, George A
, Hande HM, Devi ES, Kamath A, Nayak BS, Morisky DE, George A ![]()
Received 19 September 2022
Accepted for publication 9 November 2022
Published 7 December 2022 Volume 2022:16 Pages 3185—3193
DOI https://doi.org/10.2147/PPA.S389437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Melita Sheilini,1 H Manjunatha Hande,2 Elsa Sanatombi Devi,1 Asha Kamath,3 Baby S Nayak,4 Donald E Morisky,5 Anice George4
1Department of Medical Surgical Nursing, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, Karnataka, India; 2Department of Medicine, Kasturba Hospital, Manipal Academy of Higher Education, Manipal, Karnataka, India; 3Department of Data Science, Prasanna School of Public Health, Manipal Academy of Higher Education, Manipal, Karnataka, India; 4Department of Child Health Nursing, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, Karnataka, India; 5Department of Community Health Sciences, UCLA Fielding School of Public Health, Los Angeles, CA, USA
Correspondence: Anice George, Department of Child Health Nursing, Manipal College of Nursing, Manipal Academy of Higher Education, Udupi District, Manipal, Karnataka, India, 576104, Tel +919632094766, Fax +0091-08202922572, Email [email protected]
Purpose: The aim of the study was to assess the predictors of adherence among elderly on antihypertensives and to examine the difference in adherence among males and females.
Patients and Methods: Cross-sectional survey design was adopted for the study. The data were collected from 800 patients of age 60 years and above using demographic proforma, clinical proforma and Morisky Medication Adherence Scale (MMAS-8) with due approval from the institutional ethical clearance committee and written informed consent from the participants.
Results: The findings revealed no significant difference in the non-adherence rates among males and females. Number of medications was identified as the major predictor of adherence.
Conclusion: Awareness of factors influencing medication adherence is crucial for health professionals to provide appropriate advice for patients to maintain quality health. The findings of the study highlight the importance of nurses’ role towards imparting knowledge on hypertension and emphasizing on the importance of adherence to antihypertensives among elderly.
Keywords: hypertension, aged, adherence, medication, gender, medication nonadherence, drug adherence, elderly, antihypertensive agents
Introduction
Hypertension (HTN) contributes significantly to the global disease burden of cardiovascular and cerebrovascular diseases.1 It is the leading cause of death accounting for 7.1 million deaths annually, and 13% globally. Geriatric phase is a crucial stage in every individual’s life that demands utmost care. The main factor for inadequate BP control among the geriatric population is poor medication adherence.2,3 As age advances, the risk of cardiovascular diseases (CVDs) increases among older adults. Gender plays a vital role, with women being at increased risk of CVDs.4
According to the data released by the Ministry of Health and Family Welfare (MOHFW) on January 6, 2020, approximately 23% of the elderly individuals (aged ≥60 years) exhibit multi-morbidities. CVDs prevail among 37% of the individuals aged more than 75 years, whereas HTN is reported among 28% of the individuals aged 60–64 years and 35% of those aged 70–74 years.5 The chronicity of condition and being placed on long-term prescription regimens; nonadherence to antihypertensive medications requires an increasing attention among elderly. In a descriptive, cross-sectional, clinical study conducted in West Bengal, India, only 44.63% of a total of 186 geriatric patients were reported to adhere to antihypertensives.6
According to the World Health Organization statistics (2011), 83 million people in India are aged ≥60 years, accounting for approximately 7% of the nation’s total population. Nonadherence to medications is estimated to result in 8% of hospital admissions in this population. The reasons for nonadherence include cost of medicines, inadequate instruction, switching over to an alternative treatment, and medication side effects. Given that both medication use and the incidence of drug-related problems increase with advancing age, ensuring appropriate intake of medicines in the elderly population holds utmost importance.7
Numerous studies have been conducted to assess nonadherence to medication among patients with HTN. However, in India, limited studies have assessed adherence to antihypertensives among the elderly population. Such studies in India, particularly in coastal areas of Karnataka, are over a decade old, with the most recent one conducted in Udupi district and published in 20168 and another one conducted by Navaneetha.9 Moreover, these studies included patients aged more than 18 years and were not centered on the elderly population. The present study aimed to assess the predictors for adherence among elderly individuals on antihypertensives and examine the difference in adherence between male and female patients.
Materials and Methods
Design
A cross-sectional survey design was used to identify patients who are nonadherent to antihypertensives. The data collection was done from July 2013 to July 2015 from 800 patients aged ≥60 years attending the outpatient clinics of Medicine in a tertiary referral hospital in Karnataka. The hospital caters to a large number of patients from southern states of India such as Karnataka, Kerala, and Goa.
Participants
Hypertensive individuals aged ≥60 years capable of managing medications and able to understand English/Kannada were included from the study. Patients with chronic kidney disease, acute cerebrovascular disease, acute coronary syndrome, and major mental disorders were excluded from the study.
Data Collection
To identify patients meeting the inclusion criteria, the patients’ record was reviewed. Demographic details were obtained using a demographic proforma and the clinical details were obtained from the case records.
Medication adherence was assessed using the Morisky Medication Adherence Scale (MMAS-8), which is a standardized scale authorized for utilization with set norms. MMAS-8 has eight items with “Yes” and “No” options Based on the total score, individuals were categorized as having low adherence (scores from 0 to <6), medium adherence (from 6 to <8), and high adherence (score = 8).10–12 Standardized Kannada version of MMAS-8 with permission from the original author was used.
Ethical Considerations
The clearance was obtained from the institutional ethical committee (IEC no. KH IEC 253/2012) of Manipal University, Manipal, and the study was conducted in accordance with the Declaration of Helsinki, with prior CTRI registration (CTRI/2017/04/008405). Before enrolling the participants in the study, written informed consent was ensured and they were briefed regarding the study objectives and provided a subject information sheet.
Data Analysis
The data obtained using MMAS-8 were coded as per the coding instructions given in the standardized scale. The final coded data of demographic proforma, clinical proforma, and the MMAS-8 scale were entered in SPSS (version 20.0) for the statistical analysis. Descriptive and inferential statistics (logistic regression and chi square test) were used to address the study objectives.
Validity, Reliability, and Rigor
The demographic proforma and clinical proforma were given to nine experts from the fields of medicine and nursing for validation. The validated tools were translated to Kannada and retranslated back to English. Both the original and the translated English versions of the tool were given to a language expert to check for any deviation from the original due to translation. The reliability of MMAS-8 has been established (r = 0.83).
Results
Among 800 participants, 417 were men and 383 were women. Of the 383 female participants, 301 (78.6%) were aged ≥60–70 years, 355 (92.7%) were unemployed, 255 (66.6%) were having the annual income of <12, 000–1,00,000 INR, and 352 (91.9%) were dependent on their children and spouse for treatment expenses. Of the 417 male participants, 177 (42.4%) had the educational qualification of >7th standard-Pre University Course (PUC), 397 (95.2%) were living with their spouse, 367 (88%) belonged to a nuclear family, and 283 (67.9%) had insurance facility (Table 1).
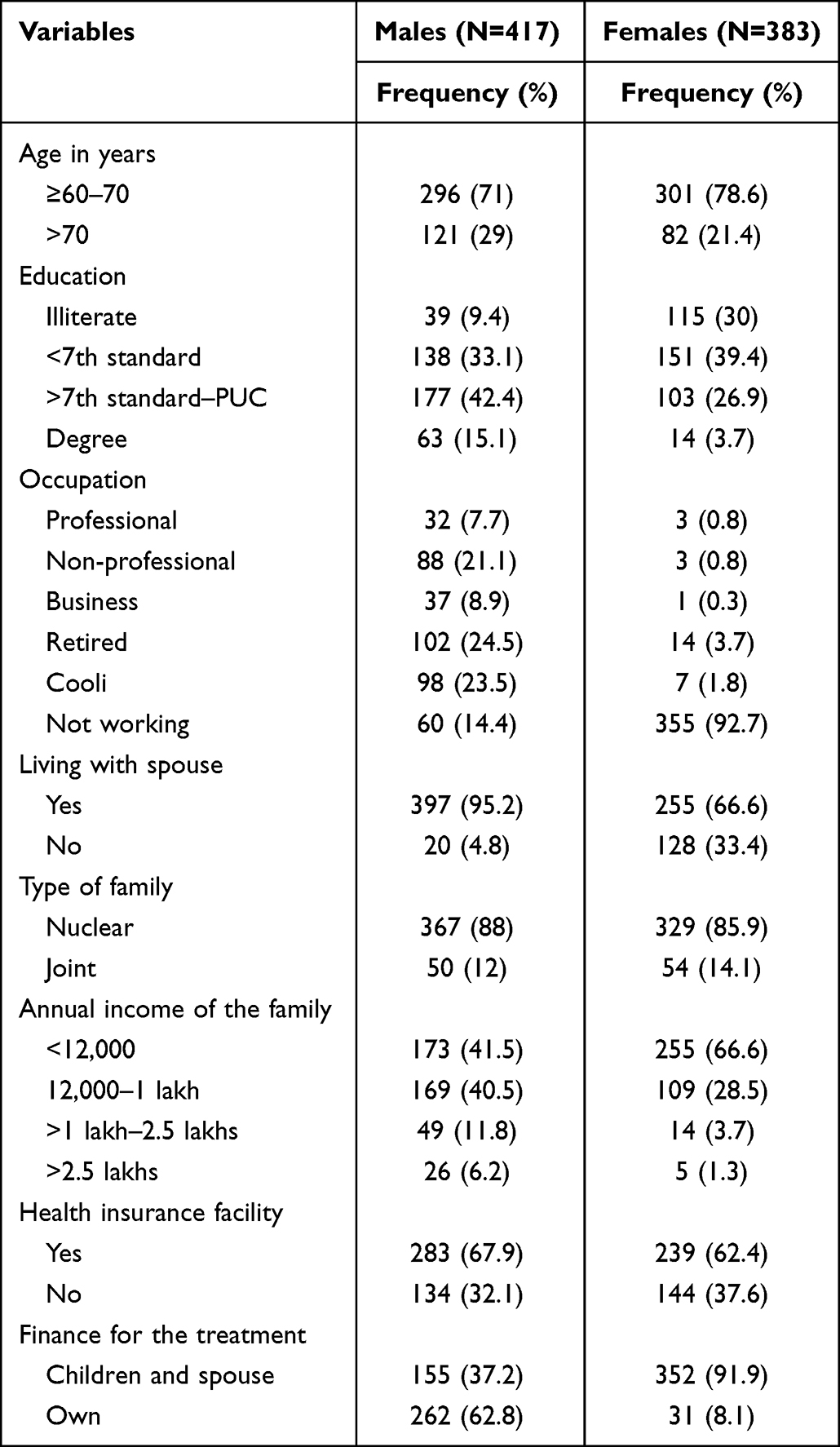 |
Table 1 Gender Wise Socio Demographic Characteristics of Sample in Frequency and Percentage (N=800) |
A larger proportion of the male patients 293 (70.3%) were being treated for HTN for over a year, and 279 (66.9%) had comorbidities. Of the total male patients, 323 (77.5%) were taking an average of 1–4 medications including antihypertensives daily (Table 2).
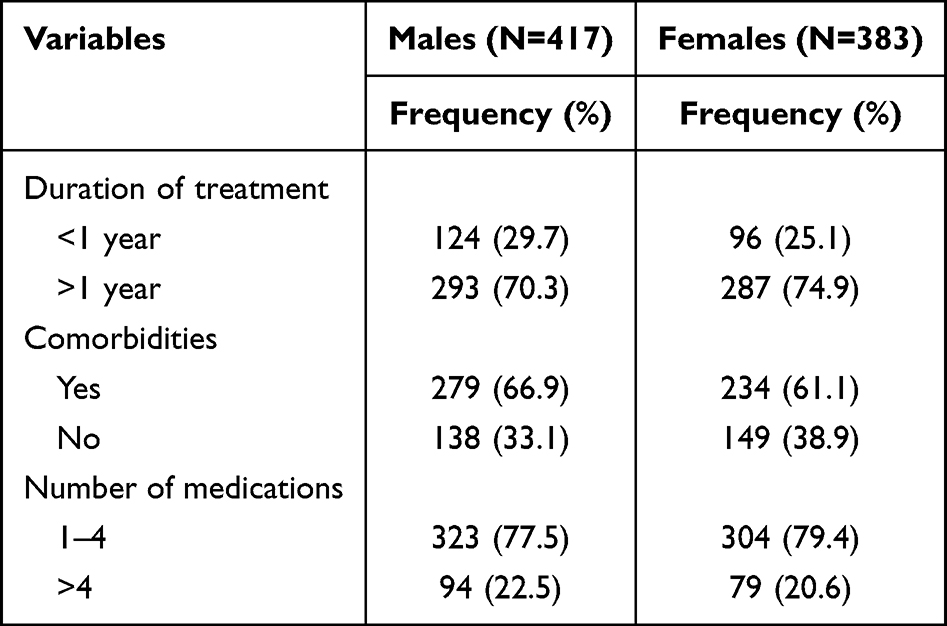 |
Table 2 Gender Wise Clinical Variables of Sample in Frequency and Percentage (N=800) |
Nonadherence to Antihypertensives Among Elderly and Gender Differences in Adherence
Among the patients identified as nonadherent to antihypertensives, 162 (38.8%) were men and 147 (38.4%) were women (Table 3). The difference in medication adherence between the male and female patients was determined used binary logistic regression. The result indicated that the difference in the nonadherence rate between the male and female patients was nonsignificant (crude OR: 0.980; 95% CI: 0.737–1.304) (Table 4).
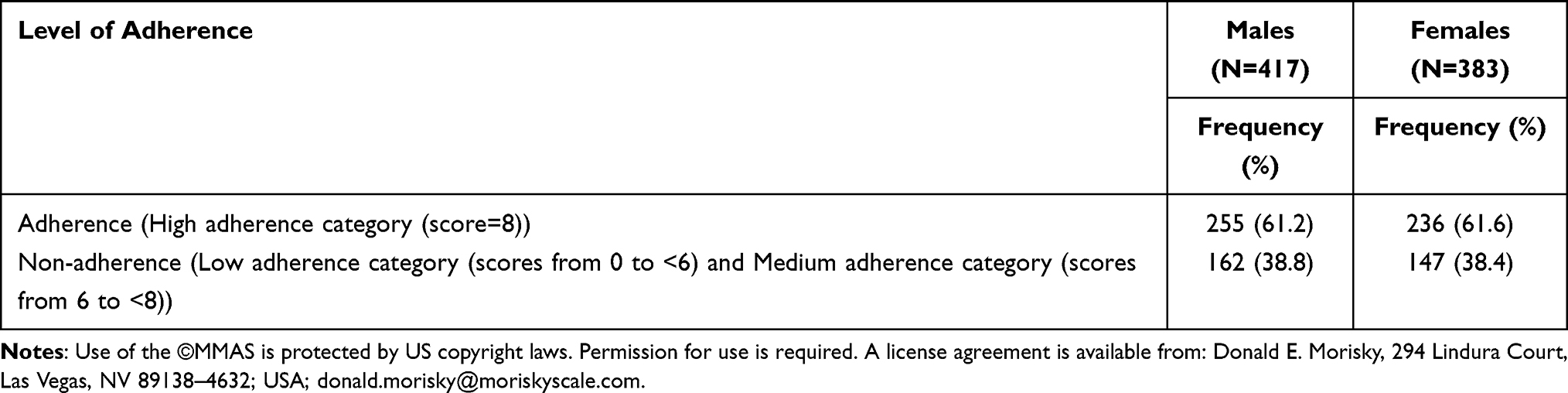 |
Table 3 Gender-Wise Adherence to Antihypertensives in Frequency and Percentage (N=800) |
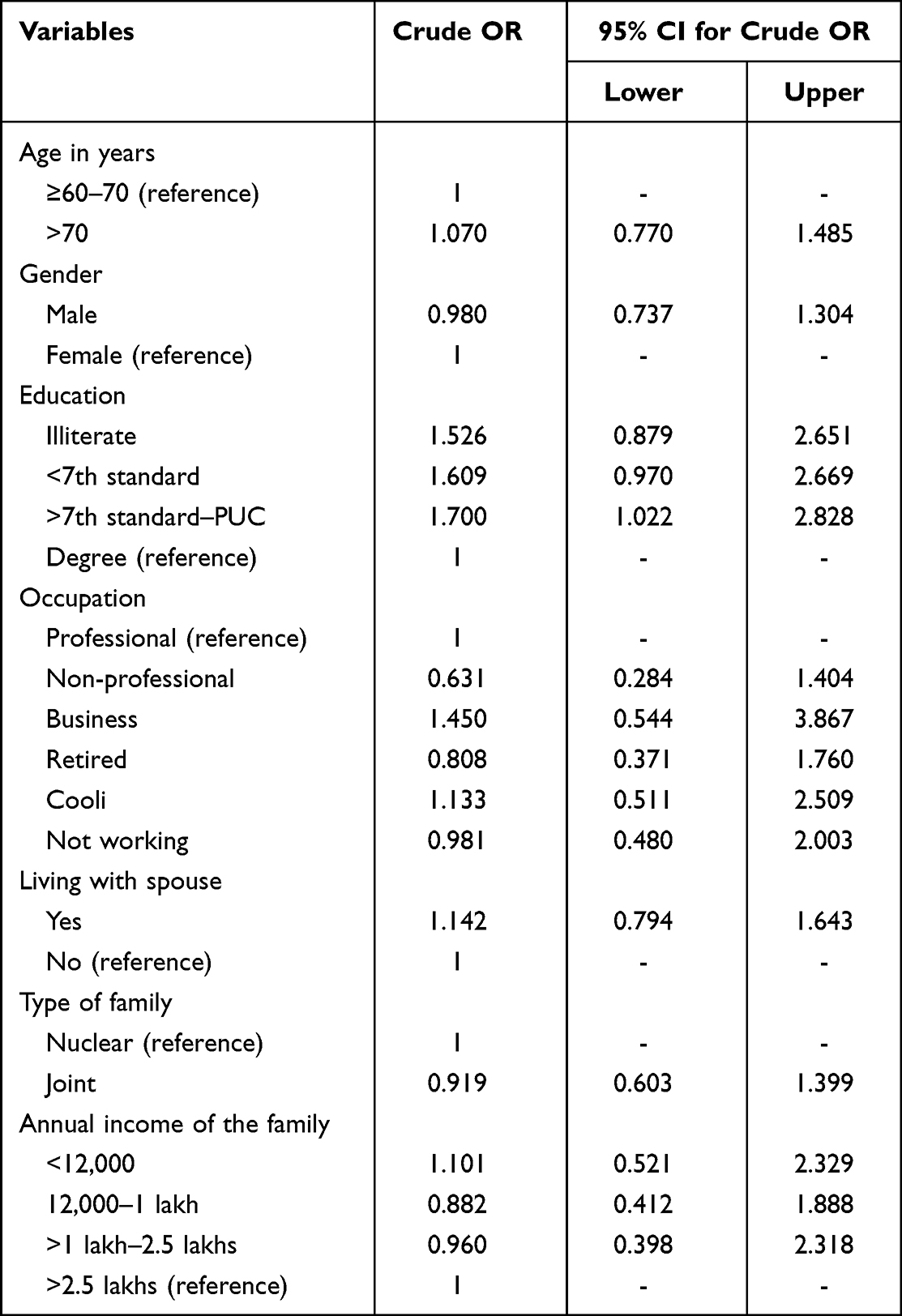 |
Table 4 Logistic Regression Analysis Showing Predictors of Adherence to Antihypertensives Among Elderly (N=800) |
Predictors of Adherence to Antihypertensives Among Elderly individuals
Univariate analysis was performed to determine the association of medication adherence with age, educational level, living with spouse, type of family, annual income of the family, insurance, duration of diagnosis, gender, comorbidities, number of medications, and finance for the treatment. The number of medications and medication adherence was found to be statistically significant (χ2 = 5.114, p = 0.024); however, medication adherence was not found to be associated with the other variables (Tables 5 and 6). Binary logistic regression was done to discover the effects of these variables on the probability of participants’ adherence to the antihypertensive medications. The regression model proved that with an increase in the total number of prescribed medications, the adherence to antihypertensives decreases among elderly individuals (crude OR: 1.511; 95% CI: 1.055–2.163), indicating polypharmacy as a strong predictor for nonadherence. None of the other variables were found to be the statistically significant predictors for adherence to antihypertensives among elderly individuals (Tables 4 and 7).
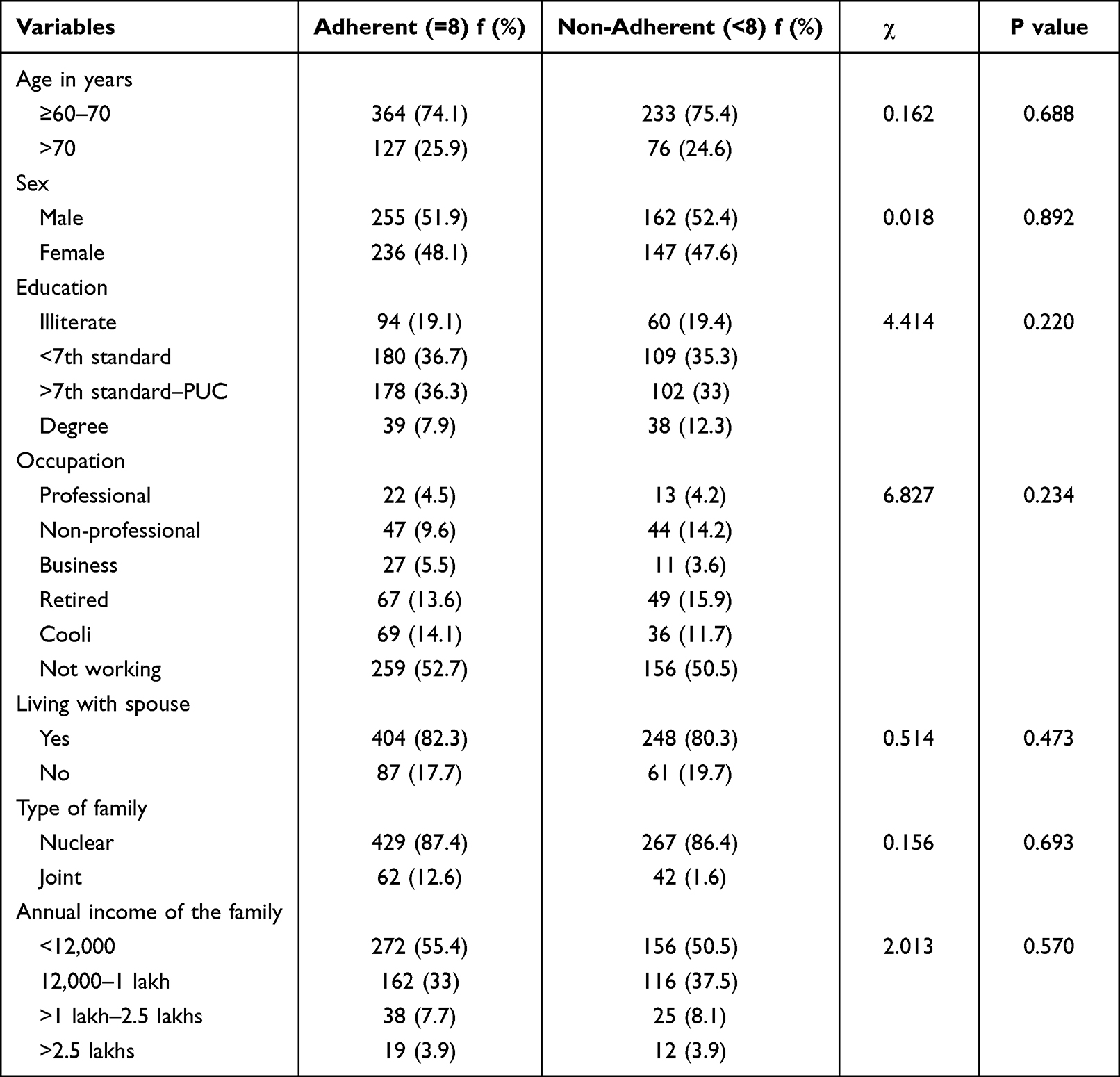 |
Table 5 Chi-Square Test for Exploring the Variables Associated with Adherence to Antihypertensives Among Elderly (N=800) |
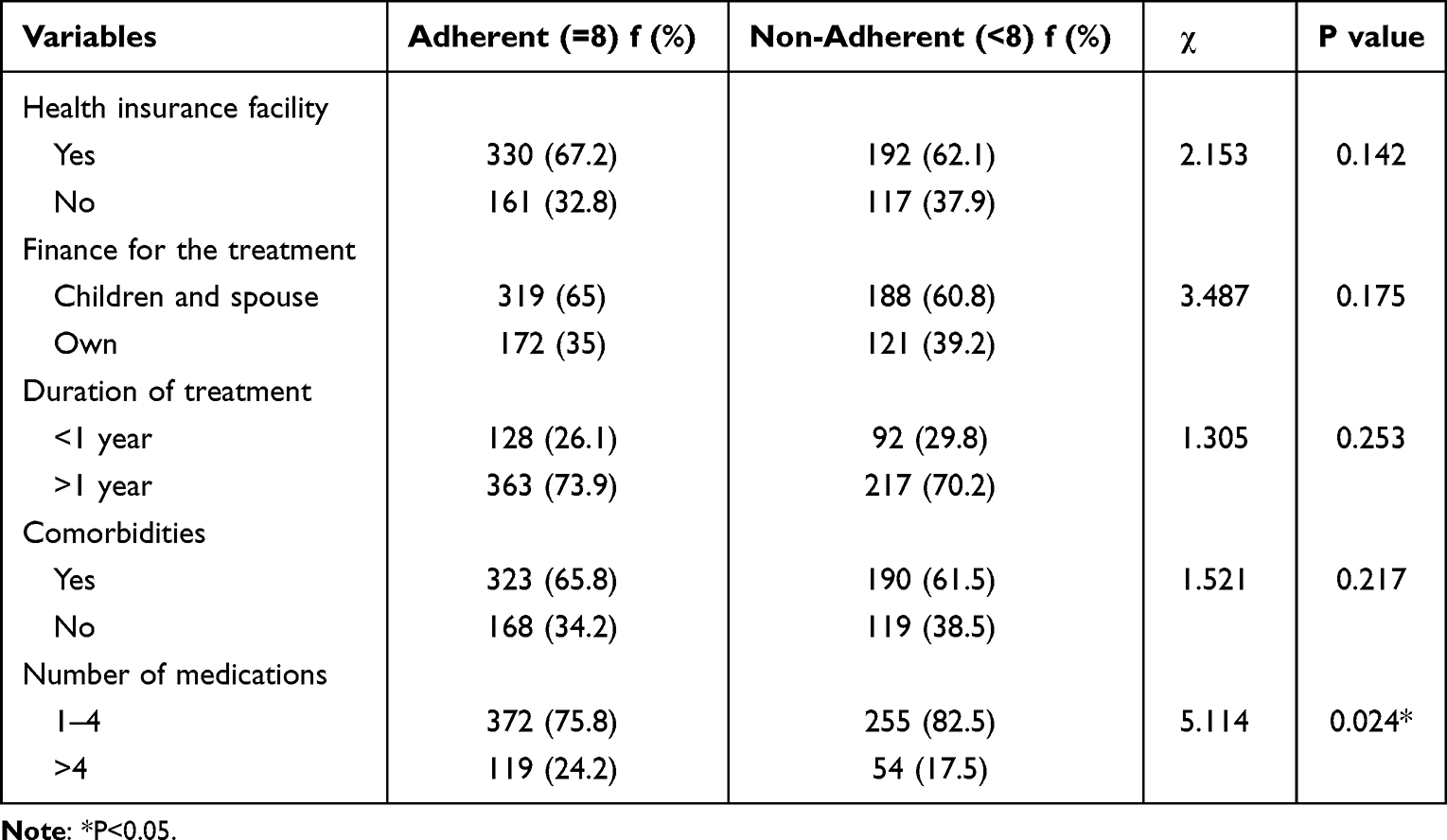 |
Table 6 Chi-Square Test for Exploring the Variables Associated with Adherence to Antihypertensives Among Elderly (N=800) |
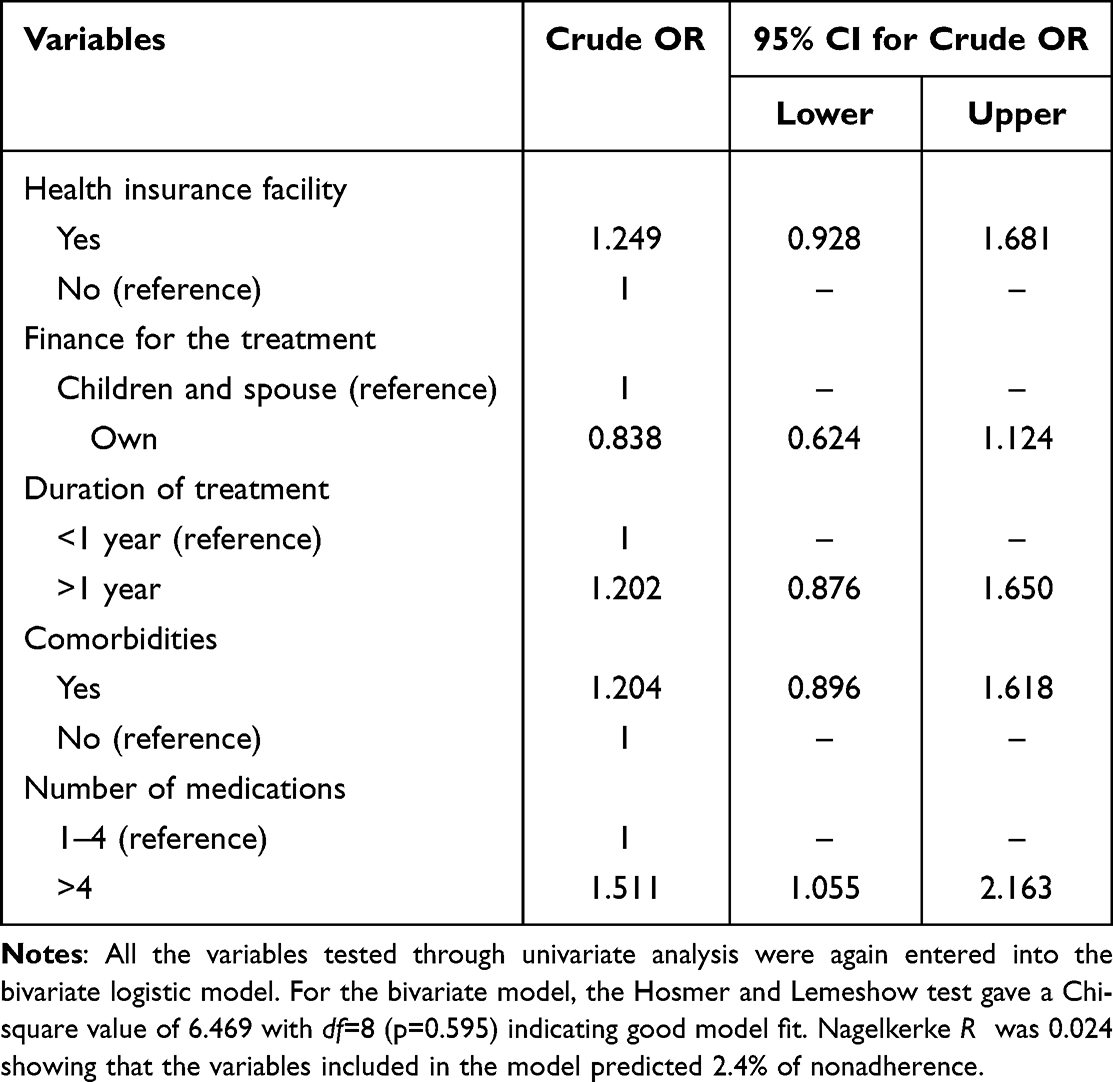 |
Table 7 Logistic Regression Analysis Showing Predictors of Adherence to Antihypertensives Among Elderly (N=800) |
Discussion
The findings of this study indicated that the proportions of nonadherence did not differ significantly between male and female patients. This finding is contrary to those of other studies, which have reported that the adherence rate to the prescribed medications is higher in male patients than in female patients.13,14 Result of a systematic review with meta-analysis conducted on gender differences in the adherence to antihypertensive drugs also revealed that among patients aged ≥65 years, self-reported adherence was lower in women than in men.15
The present study also revealed a statistically significant association between medication adherence to antihypertensives and the number of medications. However, age, educational level, living with spouse, type of family, annual income of the family, insurance, duration of diagnosis, gender, comorbidities, and finance for the treatment were not found to be the significant predictors for adherence to antihypertensives among elderly individuals. This finding is congruent with those of studies conducted at outpatient departments of teaching hospitals in Southern India and Pune, Maharashtra, which have reported nonsignificant associations of the duration since diagnosis, comorbidities, gender, marital status, educational level, and socioeconomic status and a significant association of the number of medications with the adherence to medication. However, these studies have reported divergent observations regarding the association of medication adherence with living in a nuclear family.16–18 Findings of studies piloted in West Bengal, India, and Gweru, an urban area of Zimbabwe, are also inconsistent with those of the present study, which have reported the significant associations of age, educational level, monthly income, and duration of treatment with adherence to antihypertensive medications.6,19
Consistent with the findings of the present study, the study conducted in Hong Kong and Nigeria revealed that a high number of prescribed medications was a significant predictor for nonadherence.19,20 Inconsistent with the present study findings, a few studies have reported that the age, educational level, income, comorbidities, co-living, and lack of private health insurance lead to a higher likelihood of patients’ noncompliance to the drug treatment.21–26
Limitations
This study was conducted in a hospital, where patients can be benefited by receiving health information from health profession students and better opportunity to interact with their physicians. Thus, the views expressed by respondents in this study may not reflect those of patients attending other health care settings.
The cross-sectional study design is not the best approach to investigate the predictors of the event of interest since it is affected by several biases. However, this study included only those patients with HTN who were registered at the selected tertiary care hospital. Additionally, the sample was representative of the patients with regard to the inclusion criteria considered in the study. Furthermore, cross-verification of the medications was not possible to assess medication adherence objectively.
Conclusion
The benefits of any medication to patients or individuals depend on the individual’s adherence to the therapeutic regimen. The number of medications prescribed to elderly patients should be considered while providing care as it is one of the key determinants of medication adherence. Special attention must be paid to patients with a relatively high risk, such as older patients, those with low educational level, and individuals recently diagnosed with HTN.
Relevance to Clinical Practice
This study highlights the significance of identifying elderly individuals nonadherent to antihypertensives, which can improve quality of life of the elderly population by facilitating prevention of complications secondary to uncontrolled HTN.
Abbreviations
HTN, hypertension; CVDs, cardiovascular diseases; MMAS-8, Morisky Medication Adherence Scale-8.
Acknowledgment
This manuscript was edited by EditingIndia. Use of the ©MMAS is protected by US copyright laws. Permission for use is required. A license agreement is available from Donald E. Morisky, 294 Lindura Court, Las Vegas, NV 89138-4632; USA; [email protected].
Funding
Self funded.
Disclosure
Donald E. Morisky holds a copyright and trademark for the Morisky Medication Adherence Scale-8, is one of its authors, and collects fees in exchange for licenses to use the scale. This does not alter the authors’ commitment to objectivity in research or adherence to data sharing policies. The authors report no other conflicts of interest in this work.
References
1. Choi HY, Lee JA, Lim J., et al. Factors affecting adherence to antihypertensive medication. Korean J Fam Med. 2018;39(6):325. doi:10.4082/kjfm.17.0041
2. Jhaj R, Gour P, Kumari S, Sharma S. Association between medication adherence and blood pressure control in urban hypertensive patients in central India. Int J Noncommunicable Dis. 2018;3(1):9–14. doi:10.4103/jncd.jncd_29_16
3. Salah M, Ali RES, Talaat A. The effect of counseling on patients’ adherence regarding anti hypertensive therapeutic regimen. Life Sci J. 2014;11(5):314–335.
4. Kundu J, Kundu S. Cardiovascular disease (CVD) and its associated risk factors among older adults in India: evidence from LASI Wave 1. Clin Epidemiol Global Health. 2022;13(2022):1–5. doi:10.1016/j.cegh.2021.100937
5. Devikrishna NB, Rana SG, Mishra LN (2021). Almost 70% senior citizens in India have a chronic illness. Available from: https://www.downtoearth.org.in/author/devikrishna-nb-182295.
6. Sahoo SK, Preeti PS, Biswas D. Adherence to anti-hypertensive drugs: a clinic based study among geriatric hypertensive patients in rural, India. Nat J Commun Med. 2018;9(4):250–254.
7. Evans JM, Kiran PR, Bhattacharyya OK. Activating the knowledge-to-action cycle for geriatric care in India. Health Res Policy Systems. 2011;9(1):1–10. doi:10.1186/1478-4505-9-42
8. Mallya SD, Kumar A, Kamath A, Shetty A, Reddy SK, Mishra S. Assessment of treatment adherence among hypertensive patients in a coastal area of Karnataka,India. International Journal of Community Medicine and Public Health. 2016;3(8):1998–2003. doi:10.18203/2394-6040.ijcmph20162185
9. Navaneetha M, Bairy KL, Udupa N Factors influencing drug compliance among population with chronic diseases in selected areas of udupi distict-A pilot study. Indian J Hosp Pharm. 2008;145:32–34.
10. Berlowitz DR, Foy CG, Kazis LE. Impact of intensive blood pressure therapy on patient-reported outcomes: outcomes results from the SPRINT Study. N Eng J Med. 2017;377:733–744. doi:10.1056/NEJMoa1611179
11. Morisky DE, Ang A, Krousel-Wood M, Ward H. Predictive validity of a medication adherence measure for hypertension control. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
12. Morisky DE, Hoyle RH, Thorpe CT, Maciejewski ML, Yancy Jr. WS. Improving the measurement of self-reported medication nonadherence: final response. J Clin Epidemiol. 2011;64:258–263. doi:10.1016/j.jclinepi.2010.02.023
13. Chen SL, Lee WL, Liang T. Factors associated with gender differences in medication adherence: a longitudinal study. J Adv Nurs. 2014;70(9):2031–2040. doi:10.1111/jan.12361
14. Manteuffel M, Williams S, Chen W, Verbrugge RR, Pittman DG, Steinkellner A. Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. J Women’s Health. 2014;23:2. doi:10.1089/jwh.2012.3972
15. Biffi A, Rea F, Innaccone T, Filippelli A, Mancia G, Corrao G. Sex differences in the adherence of antihypertensive drugs: a systematic review with meta-analyses. BMJ Open. 2020;10(7):1–17. doi:10.1136/bmjopen-2019-036418
16. Bress AP, Bellows BK, King JB, et al. Cost-effectiveness of intensive versus standard blood-pressure. N Eng J Med. 2017;377(8):744–755. doi:10.1056/NEJMsa1616035
17. Kumaraswamy R, Kauser MM, Jagadeesh MK, Kumar RU, Kumar SV. Study of determinants of nonadherence to anti-hypertensive medications in essential hypertension at a Teaching Hospital in Southern India. J Health Res. 2015;2(1):57–60. doi:10.4103/2348-3334.149348
18. Nagarkar AM, Gadhave SA, Sharma I, Choure A. Factors influencing medication adherence among hypertensive patients in a tertiary care hospital, Pune, Maharashtra. Nat J Commun Med. 2013;4(4):559–563.
19. Li YT, Wang HH, Liu KQ, et al. Medication adherence and blood pressure control among hypertensive patients with coexisting long term conditions in primary care settings. Medicine. 2016;95(20):1–10.
20. Odiase FE, Ogbemudia JE. Predictors of nonadherence to antihypertensive medications among stroke survivors in Benin City Nigeria. Sub-Saharan Af J Med. 2019;6(3):122. doi:10.4103/ssajm.ssajm_18_19
21. Barreto MD, Reiners AA, Marcon SS. Knowledge about hypertension and factors associated with the non-adherence to drug therapy. Rev Latino-Am Enfermagem. 2014;22(3):491–498. doi:10.1590/0104-1169.3447.2442
22. Hamza SA, El Akkad RM, Abdelrahman EE, Abd Elghany SA. Non adherence to Antihypertensive medications among hypertensive elderly patients in outpatient geriatric clinic. Egypt J Geriatrics Gerontol. 2019;6(1):1–7. doi:10.21608/ejgg.2019.30888
23. Hedna K, Hakkarainen KM, Gyllensten H, et al. Adherence to antihypertensive therapy and elevated blood pressure: should we consider the use of multiple medications? PLoS One. 2015;11:1–14.
24. Hussein A, Awad MS, Mahmoud HEM. Patient adherence to antihypertensive medications in upper Egypt: a cross-sectional study. Egyptian Heart J. 2020;72(1):1–8. doi:10.1186/s43044-020-00066-0
25. Lee GK, Wang HH, Liu KQ, Cheung Y, Morisky DE, Wong MC. Determinants of medication adherence to antihypertensive medications among a Chinese population using morisky medication adherence scale. PLoS One. 2013;8(4):1–7.
26. Wan J, Wu Y, Ma Y, Tao X, Wang A. Predictors of poor medication adherence of older people with hypertension. Nursing Open. 2022;9(2):1370–1378. doi:10.1002/nop2.1183
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hypertension and Dyslipidaemia in Argentina: Patient Journey Stages
Sadler AE, Belcastro F, Yarleque CR
International Journal of General Medicine 2022, 15:7799-7808
Published Date: 12 October 2022
Systemic Inflammation Response Index as a Predictor of Stroke Risk in Elderly Patients with Hypertension: A Cohort Study
Cai X, Song S, Hu J, Wang L, Shen D, Zhu Q, Yang W, Luo Q, Hong J, Li N
Journal of Inflammation Research 2023, 16:4821-4832
Published Date: 24 October 2023
Adherence to Lifestyle Modification Practices and Its Associated Factors Among Hypertensive Patients in Bahir Dar City Hospitals, North West Ethiopia
Geremew G, Ambaw F, Bogale EK, Yigzaw ZA
Integrated Blood Pressure Control 2023, 16:111-122
Published Date: 29 November 2023
Reliability and Validity of the Amharic Version of the Hill-Bone Adherence to High Blood Pressure Therapy Scale Among Ethiopian Hypertensive Patients
Yirba TY, Gebremariam GT, Tadesse TA, Degu A, Mekonnen D, Alemkere G
Patient Preference and Adherence 2023, 17:3207-3217
Published Date: 8 December 2023
Adherence Behaviors and Related Factors Among Elderly Hypertensive Patients in China: Evidence from the China Health and Retirement Longitudinal Study
Liu F, Chang H, Liu X
Patient Preference and Adherence 2023, 17:3539-3553
Published Date: 23 December 2023