Back to Journals » Patient Preference and Adherence » Volume 17
Adherence Behaviors and Related Factors Among Elderly Hypertensive Patients in China: Evidence from the China Health and Retirement Longitudinal Study
Received 20 October 2023
Accepted for publication 18 December 2023
Published 23 December 2023 Volume 2023:17 Pages 3539—3553
DOI https://doi.org/10.2147/PPA.S445789
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Fengyu Liu,1,2,* Huajing Chang,1,* Xiaojun Liu1,3
1School of Public Health, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2School of Public Health, National Key Laboratory of Health Technology Assessment (National Health Commission of the People’s Republic of China), Global Health Institute, Fudan University, Shanghai, People’s Republic of China; 3School of Health Management, Provincial Research Center for Healthcare Reform and Development of Fujian, Health Research Institute, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaojun Liu, School of Health Management, Fujian Medical University, No. 1 Xuefu North Road, University New District, Fuzhou City, Fujian Province, 350122, People’s Republic of China, Tel + 86 591-22869579, Email [email protected]
Background: Non-adherence or partial adherence is the main reason for poor therapeutic effect of hypertension. This paper aims to assess adherence behaviors and related factors among elderly hypertensive patients in China.
Methods: Participants aged ≥ 60 years, with hypertension, and with complete data in 2018 interviews of the China Health and Retirement Longitudinal Study (CHARLS) were included. The adherence behaviors included medication, blood pressure monitoring and the combined adherence behaviors. Referring to the social-ecological theory, correlates of adherence behaviors were divided into three layers, namely demographic characteristics, health behaviors, living environment and retirement. Univariate and multivariable logistic regression models were performed to identify factors of adherence behaviors.
Results: The prevalence of medication adherence (76.58%) was higher than that of blood pressure monitoring adherence (20.08%), and the full adherence rate was 18.53%. Self-rated health status, smoking status, living area, and health education status were detected to be associated with medication adherence and blood pressure monitoring adherence (all p < 0.05). Gender, sleep duration, health examination, and physical exercise were also detected to be associated with blood pressure monitoring adherence (all p < 0.05). Self-rated health status and health education status were detected to be associated with partially and fully adherence, while age, living area, and life satisfaction were detected to be associated with partially adherence, smoking status, sleep duration, health examination, and pension reliance were detected to be associated with fully adherence (all p < 0.05).
Conclusion: Our study reveals the poor adherence behaviors of elderly hypertensive patients in China. This is most evident among those who were male, 60– 69 years old, living in rural areas, self-reported being healthier, those without health examination and health education. Targeting these vulnerable populations, we suggest to strengthen health education, increase the publicity of basic public health services and enhance the self-management ability of hypertensive patients.
Keywords: medication adherence, blood pressure monitoring, hypertension, behavior, elderly
Introduction
Global population aging has become one of the greatest challenges among human beings. China has the largest elderly population in the world. By the end of 2022, the number of people aged 60 and above reached 280 million, accounting for 19.8% of the total population.1 In comparison to other countries, China’s aging is distinguished by a high degree and rapid progress, which brings greater challenges to the construction of Healthy China.2 Among them, the challenges brought by non-communicable diseases are the most serious.3,4 It was estimated that 75.8% of older people had at least one chronic illness, with hypertension being the most common one.5 More than half of the elderly were affected by hypertension, especially for those over 80 years old, the percentage was close to 90%.6 It is widely acknowledged that hypertension is the primary and modifiable risk factor for increased risk of cardiovascular disease and death.7–9 Therefore, proactive prevention and treatment of hypertension can reduce the number of fatalities caused by the disease and its comorbidities, as well as the financial burden it imposes on individuals, families, and society.
Due to medical advances and effective routine management, China has achieved remarkable success in controlling hypertension in recent decades.10,11 However, the management of hypertensive patients is challenging, and the control rate of hypertension remains low owing to the long duration and slow progression of the disease, the generally low health literacy of the population, and the lack of knowledge about hypertension.12–14 A longitudinal study showed that about a quarter of patients in China were diagnosed and treated for hypertension, while only 9% of all hypertensive patients had their blood pressure under control.15
Low adherence is an important patient-related reason for poor blood pressure control.16,17 Previous studies in different countries,15 genders,18 age groups,19 and races20 consistently found poor adherence behavior in patients with hypertension. Although pharmacotherapy can control blood pressure at a low cost and reduce the risk of hypertensive sequelae,21 the fact that hypertension is incurable and patients need to take medication every day or even for life makes insufficient adherence limit the effectiveness of pharmacotherapy. According to a population-based screening study in China, less than one-third of hypertensive patients are taking prescribed antihypertensive medications.19 Medication nonadherence could increase health care costs, comorbid diseases, and even lead to death.22
Accurate blood pressure monitoring is fundamental and vital for assessing blood pressure levels, diagnosing hypertension, improving long-term medication adherence and evaluating the efficacy of therapy.23,24 Compared to traditional measurements in the clinical setting, home blood pressure monitoring (HBPM) is gaining recognition for the effective management of hypertension.25 In China, 64.2% of hypertensive patients only checked their blood pressure when they were uncomfortable,26 and 71.43% of patients ignored the changes in blood pressure.27 Worse still, HBPM protocols specified in the hypertension guidelines were rarely followed in practice, and only 4.4% of patients achieved optimal HBPM regimens.28
In the process of hypertension treatment, it is not enough to take medication regularly or monitor blood pressure only, but rather to coordinate these behaviors with each other. However, although numerous research has concentrated on medication adherence in hypertensive patients, there are limited studies involving blood pressure monitoring and even fewer studies combining the two adherence behaviors. Compared to a single behavior, the co-occurrence of two behaviors can provide a more accurate picture of patients’ overall treatment adherence. Therefore, this study focuses not only on the current status of two single behaviors, medication adherence and blood pressure monitoring adherence, but also on their co-occurrence, ie, the overall adherence of hypertensive patients.
The influencing factors of hypertensive patients’ adherence behaviors have received great attention, and more and more studies paid attention to social determinants based on health views. A literature review revealed that in addition to individual factors, organizational and interpersonal factors also indirectly affect elderly adherence.29 Compared with the traditional cognitive-based model, the social-ecological model provides a wider range of intervention options and has the potential to promote long-term behavioral change.30 Therefore, in order to determine the key factors affecting adherence behaviors and understand their relationship, this study took the social-ecological model as an organizational framework and divided factors related to the adherence behavior of hypertensive patients into three categories: demographic characteristics, health behaviors, living environment and retirement. The first goal of this study was to determine the prevalence of adherence behaviors among elderly hypertensive patients in China. The second objective was to investigate the related factors of adherence and provide reference measures to improve adherence and health outcomes for relevant authorities in the treatment and control of hypertension.
Materials and Methods
Data Sources
This research data was obtained from the China Health and Retirement Longitudinal Study (CHARLS), which was a large-scale survey organized by the China Center for Economic Research, National School of Development, Peking University. They conducted the first national baseline survey in 2011, covering 150 county-level units and 450 village-level units across China, and these samples were subsequently followed up every 2–3 years. The latest data publicly available was the 2018 national follow-up survey data, which covered 19,800 people nationwide. The CHARLS survey used a stratified multi-stage probability proportional to size (PPS) whole-group sampling and had a wide range of contents, including demographic background, family structure, health status, health service utilization, work and retirement status, insurance benefits, income and expenditure status, asset status, etc. More details about this cohort were described in other research papers.31 Previous studies have proven that the CHARLS survey can provide long-term follow-up of respondents, obtain a large amount of personal health information, and cover a wide range of topics, which has been widely used.32–34 In this study, we included participants aged 60 years and older with physician-diagnosed and self-reported hypertension. After completing the missing information on adherent behavior, 5175 samples were finally included.
Adherence Behaviors
The adherence behaviors of hypertensive patients were measured by three indicators: medication adherence, blood pressure monitoring adherence, and overall adherence evaluation. (a) Medication adherence: at the time of being interviewed, patients who took traditional Chinese medicine, western medicine, or both for hypertension were defined as having good adherence, otherwise defined as poor medication adherence. (b) Blood pressure monitoring adherence: according to the Guidelines for Education of Hypertensive Patients that advocated monitoring blood pressure at least once a month in patients with hypertension,6 the number of annual blood pressure monitoring was transformed into a binary variable, ie, <12 times/year and ≥12 times/year. With ≥12 times/year defined as good adherence, and otherwise defined as poor adherence. (c) Overall adherence evaluation: if patients had good adherence with both medication and blood pressure monitoring, they were defined as fully adherence; if they had only one good adherence behavior, they were defined as partially adherence; if both behaviors were poor, it was defined as fully non-adherence.
Predictor Variables
Based on the social-ecological model, predictor variables were categorized into three main groups: demographic characteristics, health behaviors, living environment and retirement. Demographic characteristics consisted of gender, age, education level, marital status, and self-rated health. Marital status was reclassified by the options in the questionnaire: the answers “married and live with spouse” and “married but do not living with spouse temporarily for reasons such as work” were defined as married, while the answers “separated, do not live together as a couple anymore”, “divorced”, “widowed” and “never married” were defined as others. Health behaviors were made up of smoking, drinking, sleep duration, health examination, and physical activity. Smoking was defined according to the patient’s history of smoking, ie, “still have” or “quit” was defined as smoking, “never smoked” was defined as non-smoking. Physical activity was the type of activity that was taken consistently for at least ten minutes every week, which was classified into four levels: no activity, mild activity, moderate activity, and vigorous activity. Living environment and retirement variables included living area, life satisfaction, health education, and pension reliance. Pension reliance was according to the question “If you are too old to work, what would be your financial resource?” which was used to classify the respondents into three groups: children, savings or pension, and others.
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) version 26.0 (SPSS Inc., Chicago, IL, USA) was used to analyze the data. The alpha level was set at 0.05 to determine statistical significance. Descriptive analysis was first conducted. The frequency and proportion were used to describe the basic information and the current status of adherence behaviors of elderly hypertensive patients. Univariate logistic regression was then used to determine the difference in adherence by sample characteristics. Finally, to further explore the potential related factors of medication adherence and blood pressure monitoring adherence in elderly hypertensive patients, a stepwise regression method was used to construct the model. Since the overall adherence evaluation was a multi-categorical variable, multivariable logistic regression analysis was used to construct the model. The results obtained from univariate and multivariable logistic regression models were expressed as crude odds ratios (CORs) and adjusted odds ratios (AORs) with 95% confidence interval (CI), and p < 0.05 was used for statistical significance.
Results
Basic Characteristics of the Study Sample
A total of 5175 elderly patients with hypertension were included in this study. There were 2394 (46.26%) males and 2781 (53.74%) females. The largest proportion of patients (28.64%) was in the 65–69 age group, and the mean age was 70.18 (SD = 7.30). We found that more than half of the participants (54.55%) had an education level below elementary school. About 75.44% of the patients were married. Most participants (42.53%) evaluated their health as fair. Other basic information about the participants was shown in Table 1.
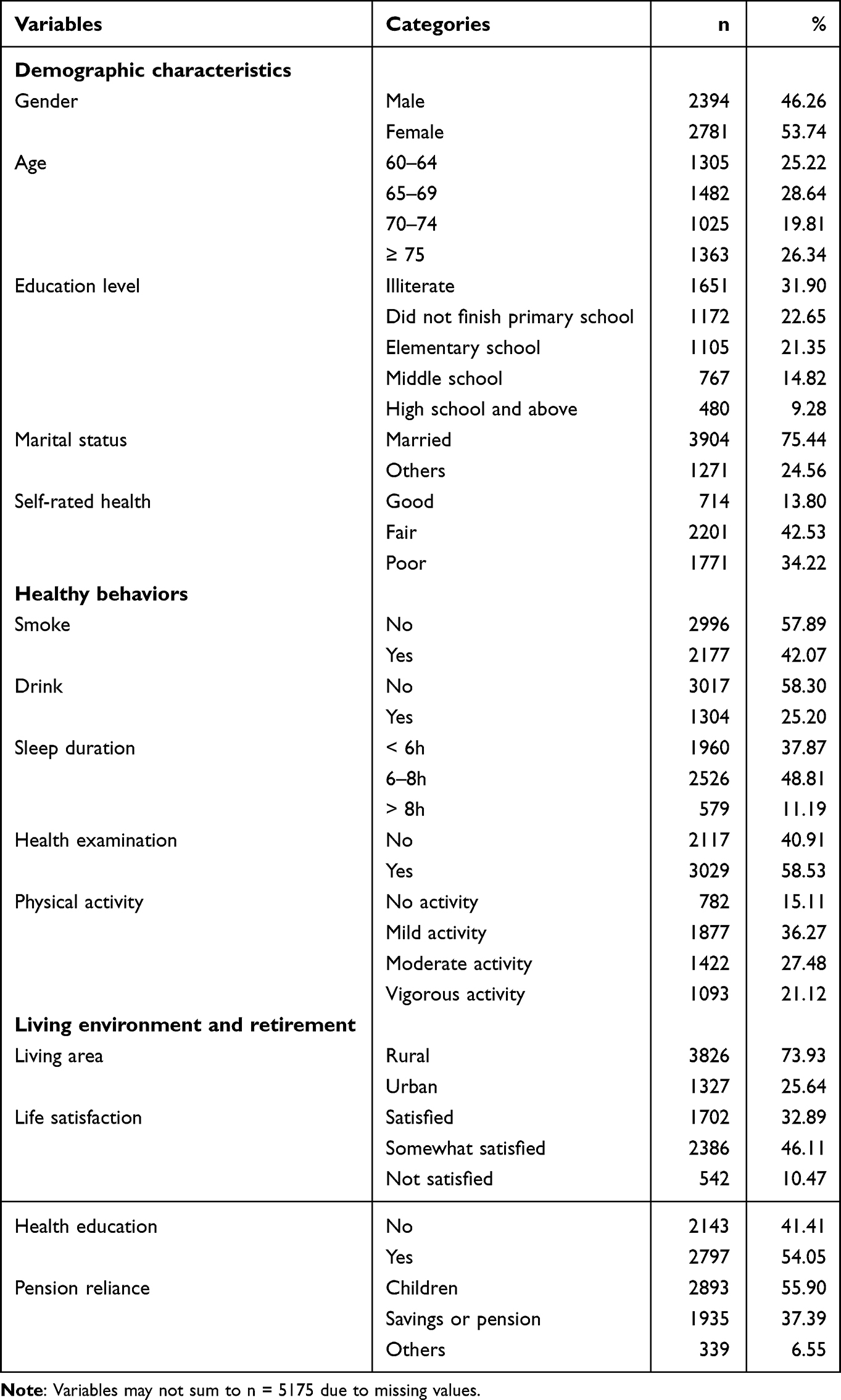 |
Table 1 Basic Information of Study Subjects (n = 5175) |
Regarding the adherence behavior of elderly patients with hypertension, 76.58% of patients had good adherence to medication. Among them, 4.17% of patients only took Chinese traditional medicine, 66.30% of patients only took western modern medicine, and 6.11% of patients took both Chinese traditional medicine and western modern medicine. 20.08% of patients measured their blood pressure 12 times or more during the past year. In the overall adherence evaluation, the fully adherence rate was 18.53%, partial adherence rate was 59.59%, and fully no-adherence rate was 21.87%. Tables 2–4 demonstrated the adherence in different populations.
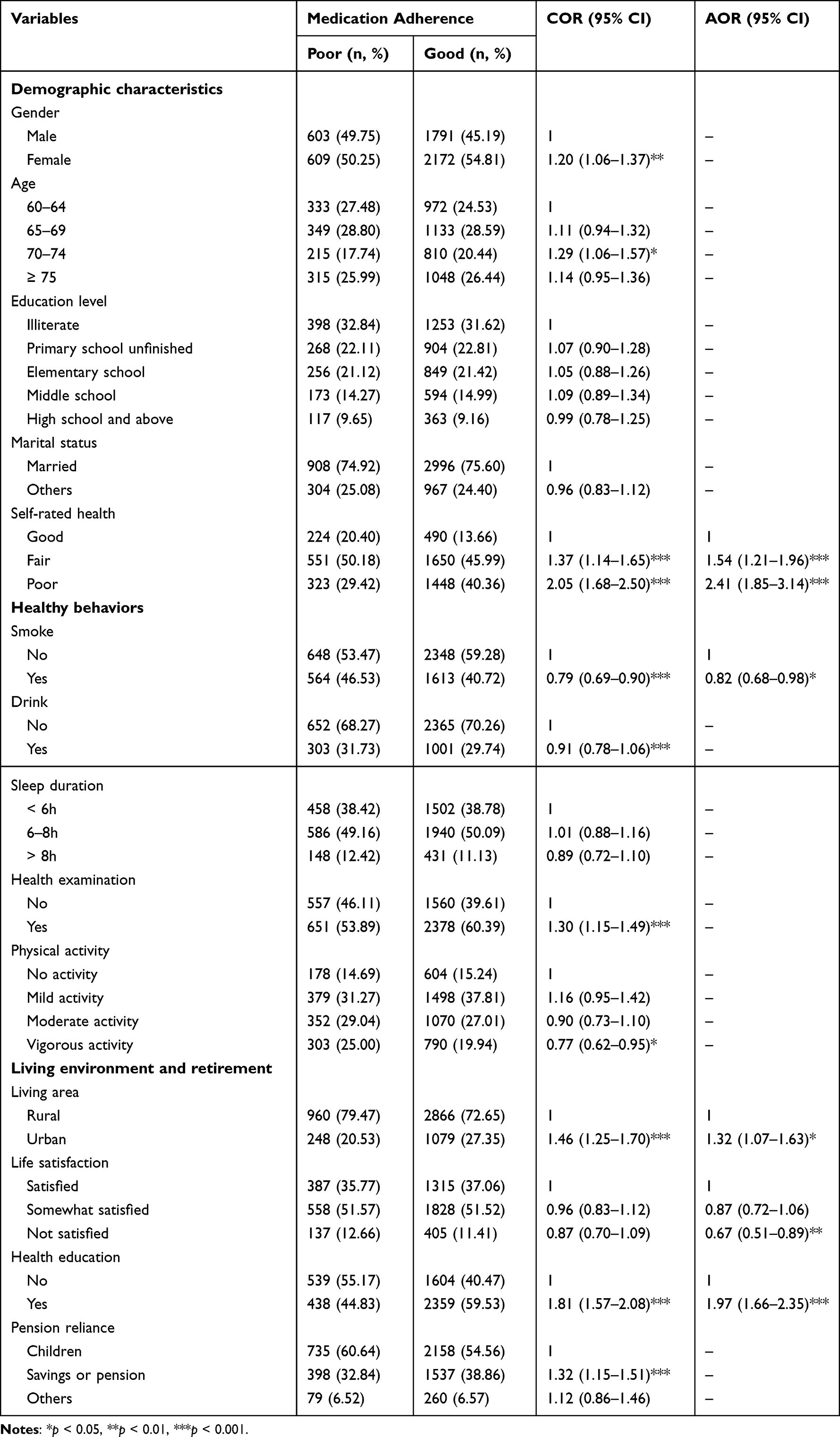 |
Table 2 Logistic Regression Analysis of Factors Associated with Medication Adherence (n = 5175) |
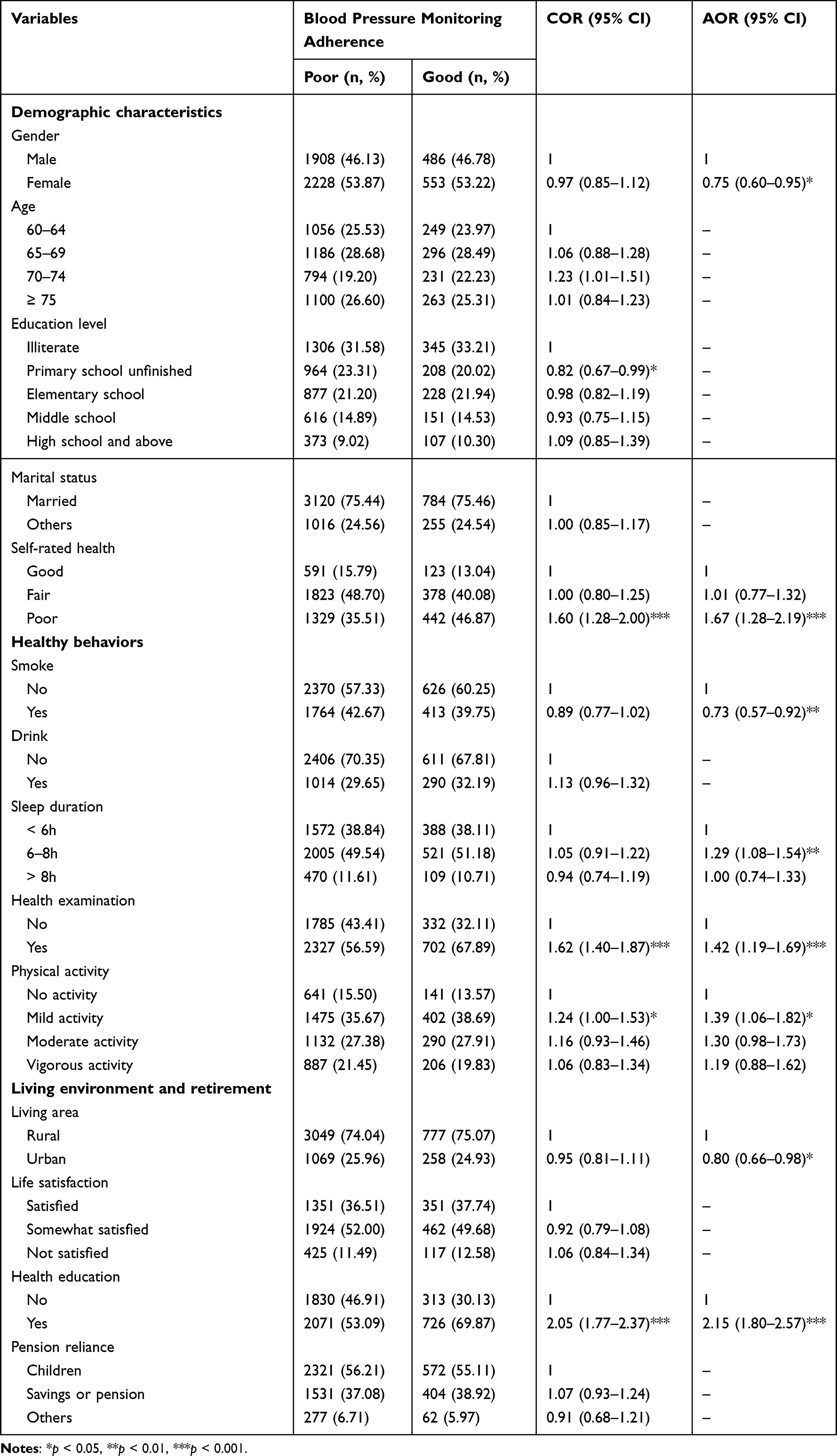 |
Table 3 Logistic Regression Analysis of Factors Associated with Blood Pressure Monitoring Adherence (n = 5175) |
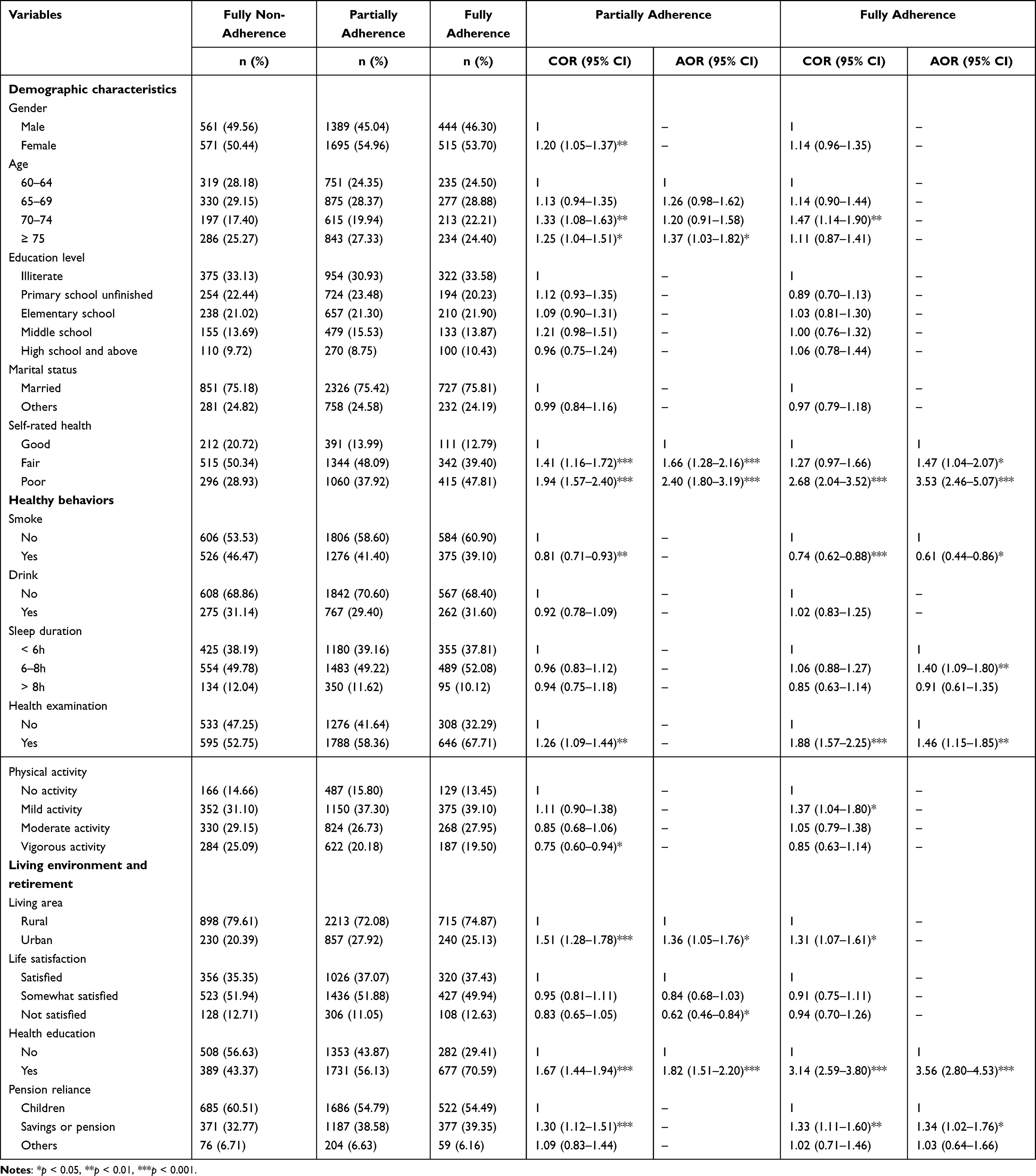 |
Table 4 Logistic Regression Analysis of Factors Associated with Overall Adherence Evaluation (n = 5175) |
Univariate Logistic Analysis of Adherence
The results of univariate analysis in Table 2 showed that the associations of gender, age, self-rated health, smoking, drinking, health examination, physical activity, living area, health education, and pension reliance with medication adherence in elderly hypertensive patients were statistically significant (all p < 0.05). As shown in Table 3, significant differences were observed between good blood pressure monitoring adherence group and poor blood pressure monitoring adherence group in educational level, self-rated health, health examination, physical activity, and health education (all p < 0.05). In the overall adherence evaluation in Table 4, partially adherence significantly differed in patients with different gender, age, self-rated health, smoking, health examination, physical activity, living area, health education, and pension reliance (all p < 0.05). The association of age, self-rated health, smoking, health examination, physical activity, living area, health education, and pension reliance with fully adherence in patients was statistically significant (all p < 0.05).
Multivariable Logistic Analysis of Adherence
Medication Adherence
The results of the multivariable analysis in Table 2 revealed that patients with fair self-rated health (AOR = 1.54, 95% CI = 1.21–1.96) and poor self-rated health (AOR = 2.41, 95% CI = 1.85–3.14) had better medication adherence compared to those with good self-rated health. Patients who smoked (AOR = 0.82, 95% CI = 0.68–0.98) were less adherent to medication compared with those who did not smoke. Patients who lived in urban areas (AOR = 1.32, 95% CI = 1.07–1.63) had better medication adherence than those who lived in rural areas. Patients who were dissatisfied with their lives (AOR = 0.67, 95% CI = 0.51–0.89) had poorer medication adherence. In addition, patients who had received health education (AOR = 1.97, 95% CI = 1.66–2.35) were more likely to be compliant with medication.
Blood Pressure Monitoring Adherence
The multivariable logistic regression model in Table 3 indicated adherence to blood pressure monitoring was poorer in females (AOR = 0.75, 95% CI = 0.60–0.95) compared to males. Patients with poor self-rated health (AOR = 1.67, 95% CI = 1.28–2.19) were more likely to have better blood pressure monitoring adherence than those with good self-rated health. Patients who smoked (AOR = 0.73, 95% CI = 0.57–0.92) had poorer blood pressure monitoring adherence compared with patients who did not smoke. Patients with 6–8 hours of sleep (AOR = 1.29, 95% CI = 1.08–1.54) had better blood pressure monitoring adherence compared to patients who sleep less than 6 hours. Patients who exercised lightly (AOR = 1.39, 95% CI = 1.06–1.82) had better adherence to blood pressure monitoring compared to patients who did not do exercise. Patients who had health examinations (AOR = 1.42, 95% CI = 1.19–1.69) and received health education (AOR = 2.15, 95% CI = 1.80–2.57) were more likely to be adherent to blood pressure monitoring. Patients who lived in urban areas (AOR = 0.80, 95% CI = 0.66–0.98) were less likely to be adherent to blood pressure monitoring.
Overall Adherence Evaluation
As the results shown in Table 4, with fully non-adherence as the reference, the results revealed that the associations of age, self-rated health, living area, life satisfaction, and health education with partially adherence were statistically significant (all p < 0.05). Patients who were ≥75 years old (AOR = 1.37, 95% CI = 1.03–1.82), had fair self-rated health (AOR = 1.66, 95% CI = 1.28–2.16), had poor self-rated health (AOR = 2.40, 95% CI = 1.80–3.19), lived in an urban area (AOR = 1.36, 95% CI = 1.05–1.76), and had received health education (AOR = 1.82, 95% CI = 1.51–2.20) were more likely to be partially adherence. Those who were dissatisfied with their lives (AOR = 0.62, 95% CI = 0.46–0.84) were less likely to be partially adherence.
The associations of self-rated health, smoking, sleep duration, health examination, health education, and pension reliance with fully adherence were statistically significant (all p < 0.05). Patients who had fair self-rated health (AOR = 1.47, 95% CI = 1.04–2.07), had poor self-rated health (AOR = 3.53, 95% CI = 2.46–5.07), slept for 6–8 hours (AOR = 1.40, 95% CI = 1.09–1.80), attended health examinations (AOR = 1.46, 95% CI = 1.15–1.85), received health education (AOR = 3.56, 95% CI = 2.80–4.53), and relied on savings or pension to live out the life in retirement (AOR = 1.34, 95% CI = 1.02–1.76) were more likely to be fully adherence. Those who smoked (AOR = 0.61, 95% CI = 0.44–0.86) were less likely to be fully adherence.
Discussion
Many researchers at home and abroad investigated the prevalence of medication adherence in different populations, and the results are quite different. The prevalence of medication adherence in our sample of Chinese elderly hypertensive patients was 76.58%, which is comparable to 74.50% from China’s sixth health service survey.35 A study from India found that the medication adherence rate was 61.2% for males and 61.6% for females,17 and data from the China Health and Nutrition Survey (CHNS) revealed a prevalence of medication adherence of 46.5%, which are lower than our study.36 But there was still a gap when compared to the Korean medication adherence rate of 81.7%.37 The discrepancy may depend upon the method of measurement and definition of adherence. Additionally, we did not precisely ask the patients about their daily medication intake, so this study may overstate the prevalence of medication adherence.
The benefits of blood pressure monitoring have been mentioned in the literature all over the world, including better medication adherence and prognosis.27 This study indicated that only 20.08% of elderly hypertensive patients had good blood pressure monitoring adherence. A similar result was reached in Pakistan, showing that less than 25% of hypertensive individuals monitored their blood pressure regularly.25 A survey in Shanghai found that 41.0% of individuals used HBPM more than once a month,38 but it was carried out in a relatively developed area and could not indicate the overall status of HBPM use in China. We suggest healthcare providers give specific advice and training to patients about how to choose appropriate blood pressure monitoring methods and encourage patients to regularly report their blood pressure readings to their physicians.
In the overall adherence evaluation, 18.53% of patients were fully adherence, 59.59% of patients were partially adherence, and 21.87% of patients were fully non-adherence. Most patients in this study only had one adherence behavior, indicating that elderly hypertensive patients in China did not aware the importance of cooperation between medication taking and blood pressure monitoring. A study included 140 outpatients with hypertension and found the prevalence of partial adherence (ie, only taking medication, not measuring blood pressure) was 19.14%.27 Inadequate patient adherence has become a major obstacle to the advancement of hypertension control strategies. This implies that it is critical for our clinicians and primary care providers to increase health education and improve their health literacy and compliance for patients with hypertension.
Unlike other studies,36,39 we discovered that females had poorer blood pressure adherence than males. Females are economically and educationally disadvantaged, especially among the old generation.40 On the one hand, females may have limited access to blood pressure monitoring devices; on the other hand, due to the lack of relevant knowledge, females may disregard or confuse the signs of high blood pressure, such as mistaking dizziness and back discomfort for exhaustion. In contrast, males’ health status receives more attention because they are the primary economic contributor and labor force of the family. Studies regarding the effect of age on patient adherence were undefined. A study revealed a negative connection between age and adherence to therapy.41 It may be due to neglect, forgetfulness, and even a waning desire to live.25 Forgetting to take medicines is a common cause of nonadherence, which accounts for 30% of all nonadherence.42 Previous studies found that older age was associated with higher rates of hypertension treatment and control.36,43,44 Our study also found patients over the age of 75 had better overall adherence evaluation than patients aged 60–64, which may be related to more severe disease, more fear of the comorbidities, and greater worry for their health in older patients.45 Patients with fair or poor self-rated health had significantly better adherence. With the extended duration of the disease and the aggravation of the disease, patients may become more eager to improve their health and increase their faith in medical advice.43
In terms of health behaviors, nonsmokers were better at both adherence behaviors than smokers, which is consistent with previous studies.46 Our study also demonstrated that patients who slept 6–8 hours and had health examinations had better blood pressure monitoring adherence. No smoking history, longer sleep, health examinations and exercise are health-promoting behaviors, which supports the conclusion that health-promoting behaviors have a positive impact on adherence.47 Patients who maintain healthy lifestyles have higher expectations for their health and stronger feelings of health responsibility and self-regulation, which makes them more attentive to changes in blood pressure.48 Graffigna et al investigated patient adherence from the perspective of patient activation.49 Patient activation was regarded as the most reliable indicator of a patient’s capacity to manage health. More highly activated people are more likely to practice healthy behaviors like exercising regularly and avoid health-damaging behaviors like smoking. Similar to our conclusion, patients’ activation significantly affects their adherence.
Among the living environment and retirement factors, we found that patients living in urban areas had better medication adherence and better overall adherence. The explanation may be the higher level of economic development and more convenient access to medications in urban areas. Interestingly, patients living in rural areas had better adherence to blood pressure monitoring, which may be due to differences in basic public health services between urban and rural areas. A study by Zuo et al found that rural patients were less likely to have blood pressure monitors at home, making it more difficult to conduct HBPM.28 The treatment of hypertension is mainly through primary health care services.50 Compared to urban areas, rural areas have a more centralized lifestyle, and village doctors and patients have a long-term stable relationship. As a result, it promotes unified management and makes it easier for village doctors to perform centralized blood pressure monitoring.51 The study also found that people with higher life satisfaction had better medication adherence because they had a more positive attitude towards health and possessed the confidence to pursue health. In our study, health education was the most important correlate factor of hypertension adherence, and the results showed that the prevalence of medication taking and blood pressure monitoring in patients who received health education was 1.97 times and 2.15 times higher compared to those who did not receive health education, respectively. It is similar to other studies,52,53 suggesting that we can significantly improve the adherence of hypertensive patients through health education. There is always a false belief among hypertensive patients that treatments can be discontinued once blood pressure control has been achieved,54 so in the process of health education, we need to help patients correct such misconceptions. Moreover, patients who relied on savings or pensions tended to be in a better financial situation and were more likely to be fully adherence than those who relied on their children for retirement. Numerous studies have confirmed that financial status and medical expenses are correlated to adherence behavior.41,55,56 Patients in a better financial situation can afford long-term treatment; whereas the elderly who rely on children for retirement may give up treatment out of guilt so as not to place a heavier financial burden on their children.
The limitations of the study also should be considered. First, many important factors related to adherence had been considered in this study, but not all known adherence factors were included (eg, treatment plan, doctor-patient relationship, methods of payment, etc.). Second, cross-sectional studies are difficult to determine the cause-effect relationship between exposure and outcome, and the factors influencing adherence behavior in elderly patients with hypertension need to be demonstrated through rigorously designed longitudinal studies. Third, this study surveyed elderly people aged ≥60 years through self-report, recall bias was thus unavoidable. What’s more, this study is based on the CHARLS data, and there is inevitably the problem of imprecise question formulation in the questionnaire. For example, in the indicator of blood pressure monitoring adherence, it is uncertain whether the act of blood pressure monitoring was done actively by the patient or passively as a result of receiving the service. It is also unclear how often the monitoring is done. Respondents may monitor their blood pressure once a month, or they may concentrate on monitoring their blood pressure several times during the period of severe illness. Furthermore, we did not examine how adherence and blood pressure control differ between hypertensive patients receiving traditional treatments and those receiving western treatments. In further studies, self-administered and more accurate questionnaires should be used to assess the adherence behavior of elderly hypertensive patients.
Conclusions
In this study, medication adherence was better than blood pressure monitoring adherence among Chinese hypertensive elderly. However, the co-occurrence rate of the two behaviors was low. In addition, self-rated health, smoking, living area, life satisfaction, and health education were associated with medication adherence. Gender, self-rated health, smoking, sleep duration, health examination, physical activity, living area, and health education were associated with blood pressure monitoring adherence. Combined with the factors associated with overall adherence evaluation, it was easy to find that self-rated health, health behaviors, living area, and health education were the most important factors associated with adherence in elderly hypertensive patients in this study. Therefore, government departments should give full play to the fundamental role of primary health service institutions in chronic disease management, increase the publicity of hypertension management services and strengthen the intervention of patients’ health behaviors. In particular, patients with poor health status and older age should be evaluated for reasons of nonadherence and difficulties encountered, and targeted health education should be provided to establish awareness of hypertension self-management and improve adherence behaviors.
Data Sharing Statement
The database (CHARLS 2018) used in this study can be found at http://charls.pku.edu.cn.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. The data were obtained by applying to National School of Development, Peking University, and the ethic approval was granted by the Ethical Review Committee of Peking University (IRB00001052-11015). According to the national legislation guidelines in China, the secondary analysis of public data from CHARLS did not require additional ethics approval (details are available at: http://www.nhc.gov.cn/qjjys/s7946/202302/c3374c180dc5489d85f95df5b46afaf5.shtml). The potential participants in this study were fully informed of the content and aim of the research. Only those who were willing to voluntarily participate and signed the informed consent form were considered as final respondents in the survey.
Acknowledgments
The authors would like to express their sincere gratitude to all the participants who wholeheartedly provided invaluable information and their collaboration in this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present study was mainly supported by the National Natural Science Foundation of China (Grant No. 72204047). Meanwhile, this work was also partially supported by the Natural Science Foundation of Fujian Province, China (Grant No. 2022J01234).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ma W. The national economy in 2022 tops the pressure to reach new heights. National Statistics Bureau; 2023. Available from: http://www.gov.cn/xinwen/2023-01/17/content_5737453.htm.
2. Tang S, Xu Y, Li Z, Yang T, Qian D. Does economic support have an impact on the health status of elderly patients with chronic diseases in China? Based on CHARLS (2018) data research. Front Public Health. 2021;9:658830. doi:10.3389/fpubh.2021.658830
3. Jiang CH, Zhu F, Qin TT. Relationships between chronic diseases and depression among middle-aged and elderly people in China: a prospective study from CHARLS. Curr Med Sci. 2020;40(5):858–870. doi:10.1007/s11596-020-2270-5
4. Yang G, Kong L, Zhao W, et al. Emergence of chronic non-communicable diseases in China. Lancet. 2008;372(9650):1697–1705. doi:10.1016/S0140-6736(08)61366-5
5. Liu J, Rozelle S, Xu Q, Yu N, Zhou T. Social engagement and elderly health in China: evidence from the China Health and Retirement Longitudinal Survey (CHARLS). Int J Environ Res Public Health. 2019;16(2):278.
6. Tan S, Liu D, Zhang Y, Li S, Zhang K, Zuo H. Trends in blood pressure and hypertension among older adults and oldest-old individuals in China between 2008–2018. Hypertens Res. 2023;46(5):1145–1156. doi:10.1038/s41440-023-01183-4
7. Calas L, Subiros M, Ruello M, et al. Hypertension prevalence, awareness, treatment and control in 2019 in the adult population of Mayotte. Eur J Public Health. 2022;32(3):408–414. doi:10.1093/eurpub/ckac015
8. Yusuf S, Joseph P, Rangarajan S, et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;395(10226):795–808. doi:10.1016/S0140-6736(19)32008-2
9. Chen Y, Hu S, Wu L, Fang X, Xu W, Shen G. Clinical practice guidelines for hypertension in China: a systematic review of the methodological quality. BMJ Open. 2015;5(7):e008099. doi:10.1136/bmjopen-2015-008099
10. Liang X, Zhong H, Xiao L. The effect of community hypertension management on blood pressure control and its determinants in southwest China. Int Health. 2020;12(3):203–212. doi:10.1093/inthealth/ihaa002
11. Liao Y, Gilmour S, Shibuya K, Kokubo Y. Health insurance coverage and hypertension control in China: results from the China Health and Nutrition Survey. PLoS One. 2016;11(3):e0152091. doi:10.1371/journal.pone.0152091
12. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China: results from the China Hypertension Survey, 2012–2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
13. Feng XL, Pang M, Beard J. Health system strengthening and hypertension awareness, treatment and control: data from the China Health and Retirement Longitudinal Study. Bull World Health Organ. 2014;92(1):29–41. doi:10.2471/BLT.13.124495
14. Lu Y, Wang P, Zhou T, et al. Comparison of prevalence, awareness, treatment, and control of cardiovascular risk factors in China and the United States. J Am Heart Assoc. 2018;7(3). doi:10.1161/JAHA.117.007462
15. Mauer N, Geldsetzer P, Manne-Goehler J, et al. Longitudinal evidence on treatment discontinuation, adherence, and loss of hypertension control in four middle-income countries. Sci Transl Med. 2022;14(652):eabi9522. doi:10.1126/scitranslmed.abi9522
16. Feng Y, Guan S, Xu Y, et al. Effects of the two-dimensional structure of trust on patient adherence to medication and non-pharmaceutical treatment: a cross-sectional study of rural patients with essential hypertension in China. Front Public Health. 2022;10:818426. doi:10.3389/fpubh.2022.818426
17. Sheilini M, Hande HM, Devi ES, et al. Determinants of adherence to antihypertensives among elderly: a multifactorial concern. Patient Prefer Adherence. 2022;16:3185–3193. doi:10.2147/PPA.S389437
18. Kim JS, Kim CG. Gender differences in hypertension treatment and control in young adults. J Nurs Res. 2020;28(3):e88. doi:10.1097/JNR.0000000000000359
19. Lu J, Lu Y, Wang X, et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1.7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet. 2017;390(10112):2549–2558. doi:10.1016/S0140-6736(17)32478-9
20. Ferdinand KC, Yadav K, Nasser SA, et al. Disparities in hypertension and cardiovascular disease in blacks: the critical role of medication adherence. J Clin Hypertens. 2017;19(10):1015–1024. doi:10.1111/jch.13089
21. Zhou B, Carrillo-Larco RM, Danaei G, et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–980. doi:10.1016/S0140-6736(21)01330-1
22. Chisholm-Burns MA, Spivey CA. The ‘cost’ of medication nonadherence: consequences we cannot afford to accept. J Am Pharm Assoc. 2012;52(6):823–826. doi:10.1331/JAPhA.2012.11088
23. Fletcher BR, Hartmann-Boyce J, Hinton L, McManus RJ. The effect of self-monitoring of blood pressure on medication adherence and lifestyle factors: a systematic review and meta-analysis. Am J Hypertens. 2015;28(10):1209–1221. doi:10.1093/ajh/hpv008
24. Stergiou GS, Kario K, Kollias A, et al. Home blood pressure monitoring in the 21st century. J Clin Hypertens. 2018;20(7):1116–1121. doi:10.1111/jch.13284
25. Zahid H, Amin A, Amin E, et al. Prevalence and predictors of use of home sphygmomanometers among hypertensive patients. Cureus. 2017;9(4):e1155. doi:10.7759/cureus.1155
26. Peng MD, Gong YC, Ding JL. 南通市社区高血压患者家庭血压计持有及血压自测情况研究[A study of home blood pressure monitor possession and blood pressure self-testing in community hypertensive patients in Nantong city]. Chongqing Med. 2017;46(24):3387–3389. Chinese.
27. Wang YH. 高血压患者自我监测对血压控制率的影响[Effect of self-monitoring on blood pressure control rate in hypertensive patients]. Chin J Pract Neurol Disord. 2010;13(14):74–75. Chinese.
28. Zuo HJ, Ma JX, Wang JW, Chen XR. Assessing the routine-practice gap for home blood pressure monitoring among Chinese adults with hypertension. BMC Public Health. 2020;20(1):1770. doi:10.1186/s12889-020-09901-0
29. Oori MJ, Mohammadi F, Norouzi K, Fallahi-Khoshknab M, Ebadi A. Conceptual model of medication adherence in older adults with high blood pressure-an integrative review of the literature. Curr Hypertens Rev. 2019;15(2):85–92. doi:10.2174/1573402114666181022152313
30. Weiner BJ, Lewis MA, Clauser SB, Stitzenberg KB. In search of synergy: strategies for combining interventions at multiple levels. J Natl Cancer Inst Monogr. 2012;2012(44):34–41. doi:10.1093/jncimonographs/lgs001
31. Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43(1):61–68. doi:10.1093/ije/dys203
32. Wu Y, Wang H, Tong Y, et al. Sarcopenia index based on serum creatinine and cystatin C is associated with mortality in middle-aged and older adults in Chinese: a retrospective cohort study from the China Health and Retirement Longitudinal Study. Front Public Health. 2023;11:1122922. doi:10.3389/fpubh.2023.1122922
33. Hu K, Keenan K, Hale JM, Liu Y, Kulu H, Joshi SK. A longitudinal analysis of PM2.5 exposure and multimorbidity clusters and accumulation among adults aged 45–85 in China. PLOS Glob Public Health. 2022;2(6):e0000520. doi:10.1371/journal.pgph.0000520
34. Pan Y, Pikhart H, Bobak M, Pikhartova J. Labour-market characteristics and self-rated health: evidence from the China Health and Retirement Longitudinal Study. Int J Environ Res Public Health. 2023;20(6):4748. doi:10.3390/ijerph20064748
35. Statistical Information Center of the National Health and Wellness Commission. Report of the Sixth National Health Services Statistical Survey (2018).
36. Wei J, Mi Y, Li Y, Xin B, Wang Y. Factors associated with awareness, treatment and control of hypertension among 3579 hypertensive adults in China: data from the China Health and Nutrition Survey. BMC Public Health. 2021;21(1):423. doi:10.1186/s12889-021-10417-4
37. Choi HY, Oh IJ, Lee JA, et al. Factors affecting adherence to antihypertensive medication. Korean J Fam Med. 2018;39(6):325–332. doi:10.4082/kjfm.17.0041
38. Wang Y, Wang Y, Gu H, et al. Use of home blood pressure monitoring among hypertensive adults in primary care: Minhang community survey. Blood Press Monit. 2014;19(3):140–144. doi:10.1097/MBP.0000000000000035
39. Liu X, Gu W, Li Z, Lei H, Li G, Huang W. Hypertension prevalence, awareness, treatment, control, and associated factors in Southwest China: an update. J Hypertens. 2017;35(3):637–644. doi:10.1097/HJH.0000000000001203
40. Backholer K, Peters SAE, Bots SH, Peeters A, Huxley RR, Woodward M. Sex differences in the relationship between socioeconomic status and cardiovascular disease: a systematic review and meta-analysis. J Epidemiol Community Health. 2017;71(6):550–557. doi:10.1136/jech-2016-207890
41. Mamaghani EA, Hasanpoor E, Maghsoodi E, Soleimani F. Barriers to medication adherence among hypertensive patients in deprived rural areas. Ethiop J Health Sci. 2020;30(1):85–94. doi:10.4314/ejhs.v30i1.11
42. Brown MT, Bussell J, Dutta S, Davis K, Strong S, Mathew S. Medication adherence: truth and consequences. Am J Med Sci. 2016;351(4):387–399. doi:10.1016/j.amjms.2016.01.010
43. Uchmanowicz B, Jankowska EA, Uchmanowicz I, Morisky DE. Self-reported medication adherence measured with morisky medication adherence scales and its determinants in hypertensive patients aged ≥60 years: a systematic review and meta-analysis. Front Pharmacol. 2019;10:168. doi:10.3389/fphar.2019.00168
44. Chia YC, Devaraj NK, Ching SM, et al. Relationship of an adherence score with blood pressure control status among patients with hypertension and their determinants: findings from a nationwide blood pressure screening program. J Clin Hypertens. 2021;23(3):638–645. doi:10.1111/jch.14212
45. Chang SM, Lu IC, Chen YC, Hsuan CF, Lin YJ, Chuang HY. Behavioral factors associated with medication nonadherence in patients with hypertension. Int J Environ Res Public Health. 2021;18(18):9614. doi:10.3390/ijerph18189614
46. Trefond J, Hermet L, Lambert C, et al. Home blood pressure monitoring and adherence in patients with hypertension on primary prevention treatment: a survey of 1026 patients in general medicine in the Auvergne region. BMC Prim Care. 2022;23(1):131. doi:10.1186/s12875-022-01725-8
47. Amico KR, Mugavero M, Krousel-Wood MA, Bosworth HB, Merlin JS. Advantages to using social-behavioral models of medication adherence in research and practice. J Gen Intern Med. 2018;33(2):207–215. doi:10.1007/s11606-017-4197-5
48. Shi D, Li J, Wang Y, et al. Association between health literacy and hypertension management in a Chinese community: a retrospective cohort study. Intern Emerg Med. 2017;12(6):765–776. doi:10.1007/s11739-017-1651-7
49. Graffigna G, Barello S, Bonanomi A, Cipresso P. The role of Patient Health Engagement Model (PHE-model) in affecting patient activation and medication adherence: a structural equation model. PLoS One. 2017;12(6):e0179865. doi:10.1371/journal.pone.0179865
50. Xiong S, Jiang W, Meng R, et al. Factors associated with the uptake of national essential public health service package for hypertension and type-2 diabetes management in China’s primary health care system: a mixed-methods study. Lancet Reg Health West Pac. 2023;31:100664. doi:10.1016/j.lanwpc.2022.100664
51. Sun Y, Li Z, Guo X, et al. Rationale and design of a cluster randomized trial of a village doctor-led intervention on hypertension control in China. Am J Hypertens. 2021;34(8):831–839. doi:10.1093/ajh/hpab038
52. Tan JP, Cheng KKF, Siah RC. A systematic review and meta-analysis on the effectiveness of education on medication adherence for patients with hypertension, hyperlipidaemia and diabetes. J Adv Nurs. 2019;75(11):2478–2494. doi:10.1111/jan.14025
53. Bancej CM, Campbell N, McKay DW, Nichol M, Walker RL, Kaczorowski J. Home blood pressure monitoring among Canadian adults with hypertension: results from the 2009 Survey on Living with Chronic Diseases in Canada. Can J Cardiol. 2010;26(5):e152–e157. doi:10.1016/S0828-282X(10)70382-2
54. Sudharsanan N, Ali MK, McConnell M. Hypertension knowledge and treatment initiation, adherence, and discontinuation among adults in Chennai, India: a cross-sectional study. BMJ Open. 2021;11(1):e040252. doi:10.1136/bmjopen-2020-040252
55. Raja W, Ayub T, Jeelani A, Khan SMS. Adherence to antihypertensive therapy and its determinants among patients attending primary care hospitals of Kashmir, India. J Family Med Prim Care. 2021;10(11):4153–4159. doi:10.4103/jfmpc.jfmpc_668_21
56. Teshome DF, Demssie AF, Zeleke BM, Shimosawa T. Determinants of blood pressure control amongst hypertensive patients in Northwest Ethiopia. PLoS One. 2018;13(5):e0196535. doi:10.1371/journal.pone.0196535
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence and Blood Pressure Control Among Hypertensive Outpatients Attending a Tertiary Cardiovascular Hospital in Tanzania: A Cross-Sectional Study
Pallangyo P, Komba M, Mkojera ZS, Kisenge PR, Bhalia S, Mayala H, Kifai E, Richard MK, Khanbhai K, Wibonela S, Millinga J, Yeyeye R, Njau NF, Odemary TK, Janabi M
Integrated Blood Pressure Control 2022, 15:97-112
Published Date: 10 August 2022
A Critical Review of Medication Adherence in Hypertension: Barriers and Facilitators Clinicians Should Consider
Hamrahian SM, Maarouf OH, Fülöp T
Patient Preference and Adherence 2022, 16:2749-2757
Published Date: 7 October 2022
Interventions Incorporating Therapeutic Alliance to Improve Medication Adherence in Black Patients with Diabetes, Hypertension and Kidney Disease: A Systematic Review
Desta R, Blumrosen C, Laferriere HE, Saluja A, Bruce MA, Elasy TA, Griffith DM, Norris KC, Cavanaugh KL, Umeukeje EM
Patient Preference and Adherence 2022, 16:3095-3110
Published Date: 14 November 2022
Patient Pill Organization Strategies and Adherence Measured in a Cross-Sectional Study of Hypertension
Genelin MP, Helmkamp LJ, Steiner JF, Maertens JA, Hanratty R, Vupputuri S, Havranek EP, Dickinson LM, Blair IV, Daugherty SL
Patient Preference and Adherence 2023, 17:817-826
Published Date: 23 March 2023
A Systematic Review of the Hill-Bone Compliance to Blood Pressure Therapy Scale
Commodore-Mensah Y, Delva S, Ogungbe O, Smulcer LA, Rives S, Dennison Himmelfarb CR, Kim MT, Bone L, Levine D, Hill MN
Patient Preference and Adherence 2023, 17:2401-2420
Published Date: 28 September 2023