Back to Journals » Patient Preference and Adherence » Volume 17
Reliability and Validity of the Amharic Version of the Hill-Bone Adherence to High Blood Pressure Therapy Scale Among Ethiopian Hypertensive Patients
Authors Yirba TY, Gebremariam GT ![]() , Tadesse TA
, Tadesse TA ![]() , Degu A
, Degu A ![]() , Mekonnen D, Alemkere G
, Mekonnen D, Alemkere G
Received 17 September 2023
Accepted for publication 5 December 2023
Published 8 December 2023 Volume 2023:17 Pages 3207—3217
DOI https://doi.org/10.2147/PPA.S439715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Tsegaab Yoseph Yirba,1,2 Girma Tekle Gebremariam,1 Tamrat Assefa Tadesse,1 Amsalu Degu,3 Desalew Mekonnen,4 Getachew Alemkere1
1Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa Univerisity, Addis Ababa, Ethiopia; 2Department of Pharmacy, College of Health and Medical Science, Dilla Univerisity, Dilla, Ethiopia; 3School of Pharmacy and Health Sciences, United States International University-Africa, Nairobi, Kenya; 4Division of Cardiology, Department of Internal Medicine, School of Medicine, College of Health and Medical Science, Addis Ababa Univerisity, Addis Ababa, Ethiopia
Correspondence: Tamrat Assefa Tadesse, Email [email protected]
Background: Hypertension is the leading cause of death from cardiovascular disease. Non-adherence to treatment and lifestyle modification are the key drivers of suboptimal blood pressure control and cardiovascular events.
Objective: To assess the reliability and validity of the Amharic version of the Hill–Bone Adherence to High Blood Pressure Therapy Scale (HBTS) among Ethiopian hypertensive patients.
Methods: A cross-sectional study was conducted among 294 hypertensive patients at two health facilities from 1st October to 30th December 2021 using the culturally adapted HBTS. Psychometric properties were assessed in terms of acceptability, internal consistency, construct validity, and predictive validity. Statistical Package for Social Sciences version 26 was used to perform statistical tests at a significance level of p-value < 0.05. The Statistical Package for Social Sciences AMOS version 26 was used for the confirmatory factor analysis.
Results: Cronbach of the 14-item HBTS was initially 0.801. After excluding one item from the appointment-keeping subscale, Cronbach of the modified 13-item HBTS was 0.806. The initial principal component analysis revealed four constructs for the 14-item and three for the 12-item with a total explained variance of 58.65% and 55.73%, respectively. The confirmatory factor analysis failed to fit the observed items with the latent subscales. The predictive validity test showed that the modified 12-item Amharic version was correlated (r= 0.118;p< 0.043) with systolic blood pressure.
Conclusion: The modified 13-item Amharic version of the HBTS is a reliable and valid tool with adequate psychometric properties. It can be used to assess adherence to antihypertensive medications in Amharic-speaking patients in Ethiopia.
Keywords: hypertension, reliability, Hill-Bone adherence to high blood pressure therapy scale, validity, Ethiopia
Background
Hypertension (HTN), defined as sustained high blood pressure (BP)1 is the leading preventable risk factor for cardiovascular events, cerebrovascular, renal disease, and other end-organ damage.2 It affects more than 1.13 billion people worldwide and is responsible for more than 10.4 million preventable deaths globally each year.3–5 This high burden is perplexing with unacceptably poor awareness, care, and control worldwide, particularly in low and middle-income countries.6 HTN prevalence in Sub-Saharan Africa is estimated to be 20.95% by 2020.7 Despite underdiagnosis, treatment, and control, there has been a significant increase in urban areas.8–10 In Ethiopia, the prevalence of HTN is estimated to be 19.6%, with a higher rate in the urban population (23.7%) than in the rural population (14.7%).
Effective BP control is essential to reduce mortality and end-organ damage related to HTN.11,12 Despite this, optimal HTN control is rarely achieved, and the primary cause of this failure to achieve adequate BP control is frequently attributed to patients’ failure to adhere to a prescribed treatment regimen.13 Adherence is the extent to which a person’s behaviour of taking medication, following a diet, and/or executing lifestyle changes corresponds with agreed recommendations from a health care provider.14
Non-adherence to antihypertensive medication is linked to several factors, including social and economic factors, healthcare team and system-related factors, condition-related factors, therapy-related factors, and patient-related factors.14 Resolving the massive non-adherence problem demands an appropriate assessment of patients’ medication adherence levels using direct and indirect approaches. Measuring drug concentration (or a metabolite) in body fluids and directly observed therapy are examples of direct approaches.15 In contrast, indirect approaches include evaluating the clinical response, performing pill counts, determining rates of prescription refills, self-reported questionnaires, scales, and electronic medication monitors.16 Although each approach has advantages and disadvantages, self-reported scales have the benefits of being inexpensive, easy to administer, non-intrusive, and able to provide information on attitudes and beliefs and hence are easily adaptable to varied patient populations and settings.7,15,17,18
There are several self-reported tools to measure adherence in hypertensive patients, but the most common one is the Morisky Medication Adherence Scale (MMAS), an eight-item validated tool.19 Even though it is validated in different settings, it has limitations like the inability to measure lifestyle modification-related elements.17 Thus, it is imperative to use another tool that is valid and addresses the above limitations such as Hill–Bone adherence to the high blood pressure therapy scale (HBTS). In addition to measuring medication adherence, HBTS measures lifestyle (salt intake) and appointment-keeping unlike MMAS.20
As simple, reliable, and valid, tools are required for accurate estimation of adherence level and its predictors, psychometric tests of tools used to assess treatment adherence to antihypertensive treatment were hardly studied in Ethiopia. Therefore, our study aimed to assess the reliability and validity of the Amharic version of the Hill-Bone high blood pressure therapy scale (HBTS-Am) in Ethiopian hypertensive patients.
Materials and Methods
Study Design and Setting
A hospital-based cross-sectional study design was conducted among ambulatory hypertensive patients of Tikur Anbessa Specialized Hospital (TASH) and Saint. Paul’s Hospital Millennium Medical College (SPHMMC) from 1st October to 30th December 2021. These two hospitals are among the largest teaching hospitals in the country, educating a large number of undergraduate and graduate students. Furthermore, they offer specialties and sub-specialties not found in other public or private institutions.
Patient Recruitment and Data Collection Procedure
Adult hypertensive patients (18 years and above) who had regular follow-ups at least for six months, those who were taking at least one antihypertensive medication and those with complete medical records were included in the study. The study excluded newly diagnosed hypertensive patients, patients with gestational hypertension, and those who did not give consent to participate.
Sample Size Determination
Even though there is no general agreement about the size of the sample required for factor analysis, some authors recommend a rule of thumb regarding the minimum ratio of participants to variables (2:1) or extracted factors (20:1).21 Based on evidence from the previous study, a subject-item ratio of 20:1 was used to calculate the sample size. Since the Hill–Bone scale contains 14 questions, a minimum sample size of 280 patients was required22 adding 5% contingency, a total of 294 hypertensive patients were included in this study.
Data Collection and Management
A data collection tool was prepared from a review of the literature to capture the sociodemographic and clinical characteristics of the patients. The data collection instrument had four sections (sociodemographic characteristics; patient medical and medication history; 14-item HBTS-Am; and details of the prescribed regimen, clinical outcome parameters, and comorbidities). Data was collected using an interview and medical record review.
Instruments
HBTS Translation and Cultural Adaptation
HBTS assesses patients’ three important behavioral domains of HTN treatment including medication compliance, appointment keeping, and salt intake. The scale consists of 14 items in three subscales. Each was graded according to a four-point Likert scale ranging from 1 (All of the Time) to 4 (None of the Time).
First, permission for translation of the HBTS into the Amharic version was obtained from the original developer of the English version of the HBTS. Then, it was translated into Amharic language and back-translated into English by bilingual speakers of both languages, including expert physicians, clinical pharmacists, and nurses. The changes were made to reflect the local culture. The World Health Organization’s guidelines for linguistic validation and translation were also followed.23
The translation process was based on the five-stage process and proceeded as follows: 1) forward translation into Amharic by two independent translators which include one Expert physician and bilingual personnel; 2) synthesis of translated versions where the two translations were examined by a team including expert physician, expert clinical pharmacist and the principal investigator (target language); 3) backward translation (blind) which includes one physician and expert clinical nurse; 4) synthesis of translated versions (original language) which involves members of the research team; 5) pretest of synthesized translated version: cognitive debriefing and cultural equivalence.24 The changes made to the original HBTS were; 1) “How often do you shake salt on your food before you eat it?” was changed into “How often do you add salt before you eat it?” because “shaking salt” is unusual in Ethiopian culture; 2) “How often do you eat fast food?” was changed in to “How often do you eat fast foods (Chips, fried food, sandwiches)?” because fast food may not be well understood in Ethiopia, hence examples were given.
Statistical Analysis
Data were entered into Epi info 7.1.0.6 and analyzed using Statistical Package for Social Science (SPSS) software version 26.0. Frequency, mean, percentage, median, and standard deviation (SD)) were used to report descriptive data. The psychometric properties of the HBTS-Am were assessed by testing the reliability and validity of the tool as follows:
Acceptability
The acceptability of the HBTS-Am was assessed in terms of difficulty in answering the questions, percentage of missing data, response rate, the time needed to complete the questionnaire, and upsetting nature, confusion, and difficult words in the questionnaire.
Reliability
The reliability of scales was assessed by measuring the internal consistency of HBTS-Am using Cronbach’s α coefficient. Cronbach’s alpha value >0.70 was considered acceptable and item-total correlation was also examined with a value of >0.3 was considered acceptable.25
Construct Validity
Principal component extraction (PCA) was used to assess the construct validity. Factors were extracted based on Eigenvalues greater than 1. Items with loading >0.40 within one factor were retained. The appropriateness of PCA was checked by estimating the Kaiser-Meyer-Olkin (KMO) test and Bartlett’s test of sphericity. Following the identification of a factor solution via PCA, the model construct was further evaluated using confirmatory factor analysis (CFA).
Predictive Validity
The predictive validity of HBTS was assessed by determining the correlation between the original 14-item scale, the modified 13-item Amharic scale, the modified 12-item Amharic scale, the Amharic version medication intake subscale, and blood pressure. All statistical tests were performed using a level of significance of p-value < 0.05.
Ethical Approval
Ethical clearance was obtained from the Ethics Review Committee of the School of Pharmacy, College of Health Sciences, Addis Ababa University (ERB/SOP/258/13/2021). Permission to conduct the study was sought from the renal unit of TASH (PCP/260/13/21) and SPHMMC (PM23/327), and permission to use the HBTS was obtained from Johns Hopkins University. The ethical standards outlined in the Declaration of Helsinki for research involving human participants were followed in this study. Written informed consent was obtained from participants, and confidentiality was maintained through anonymity.
Results
Sociodemographic and Clinical Characteristics of the Participants
A total of 294 hypertensive patients participated in the study with a mean age of 54.5±11.9 years. One hundred fifty-three (52%) were females, 264 (89.8%) were married and 16 (5.4%) were illiterate. More than half (60.2%) of the study participants were on treatment for less than five years. About 89.1% of the patients have one or more comorbid conditions. Most of the participants (66.3%), engaged in regular exercise (Table 1).
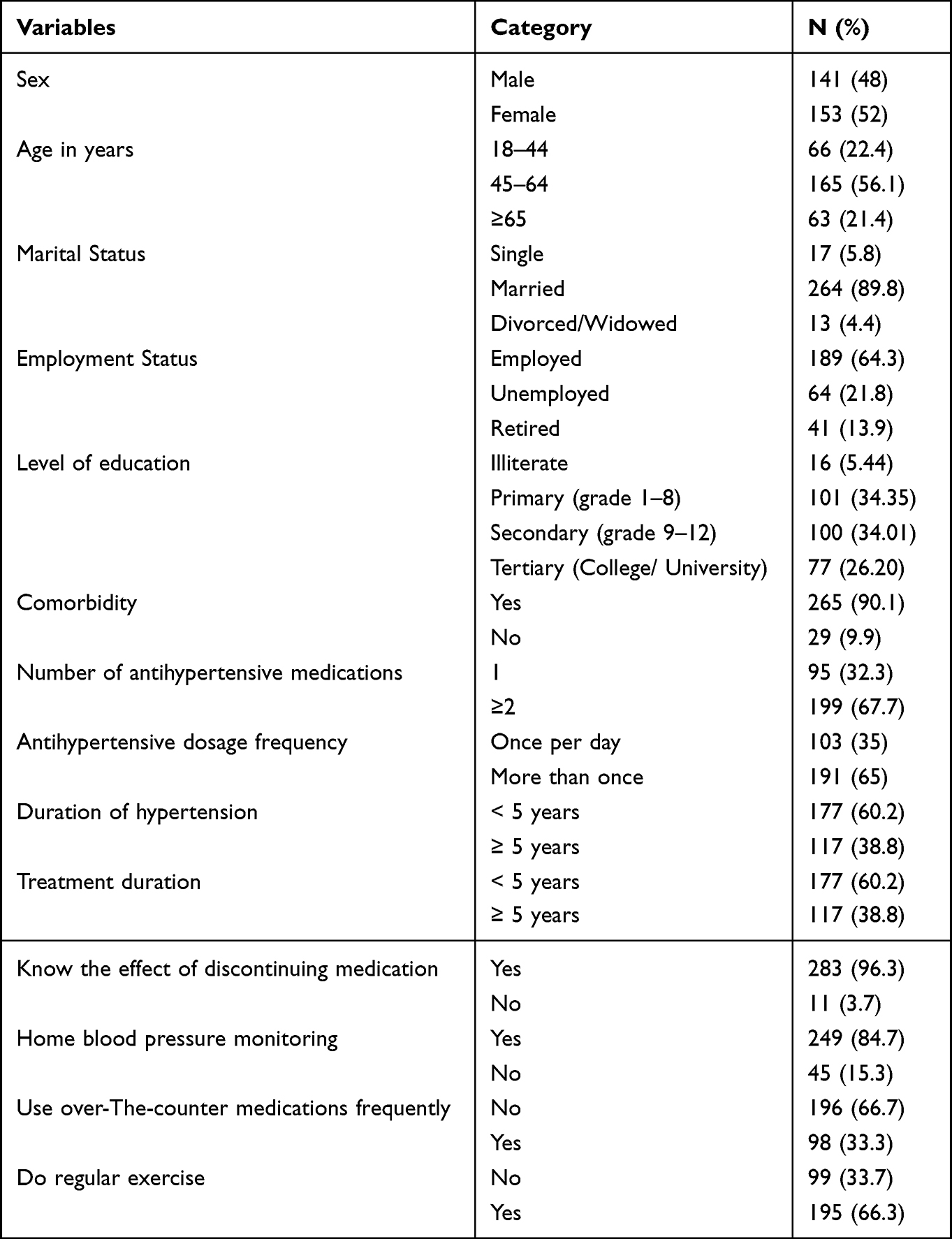 |
Table 1 Sociodemographic and Clinical Characteristics of the Participants (N= 294) |
Psychometric Properties of the HBTS-Am
The mean (n = 294) score for the 13-item was 18.82 ±3.51 (14–52). Mean scores of medicine-taking adherence, reduced salt intake, and appointment keeping were 11.4±4.31, 6.14±1.83, and 2.32±0.67, respectively. Most items had a mean score of < 2 except item 4 (how often do you add salt to your food before you eat it) with a mean score of 2.73. None of the items had a perfect mean score of 1.
Except for items 1, 3, 4, and 6, most of the items had the highest proportion of respondents who answered “none of the time”. Item 1 and Item 3 had the highest number of respondents who answered “some of the time”, ie, (50.7%) and (58.5%) respectively. While item 6 had the highest proportion of respondents who answered “all the time”, (96.6%, item 4 had the highest proportion of respondents who answered “most of the time”, (52%) (Table 2).
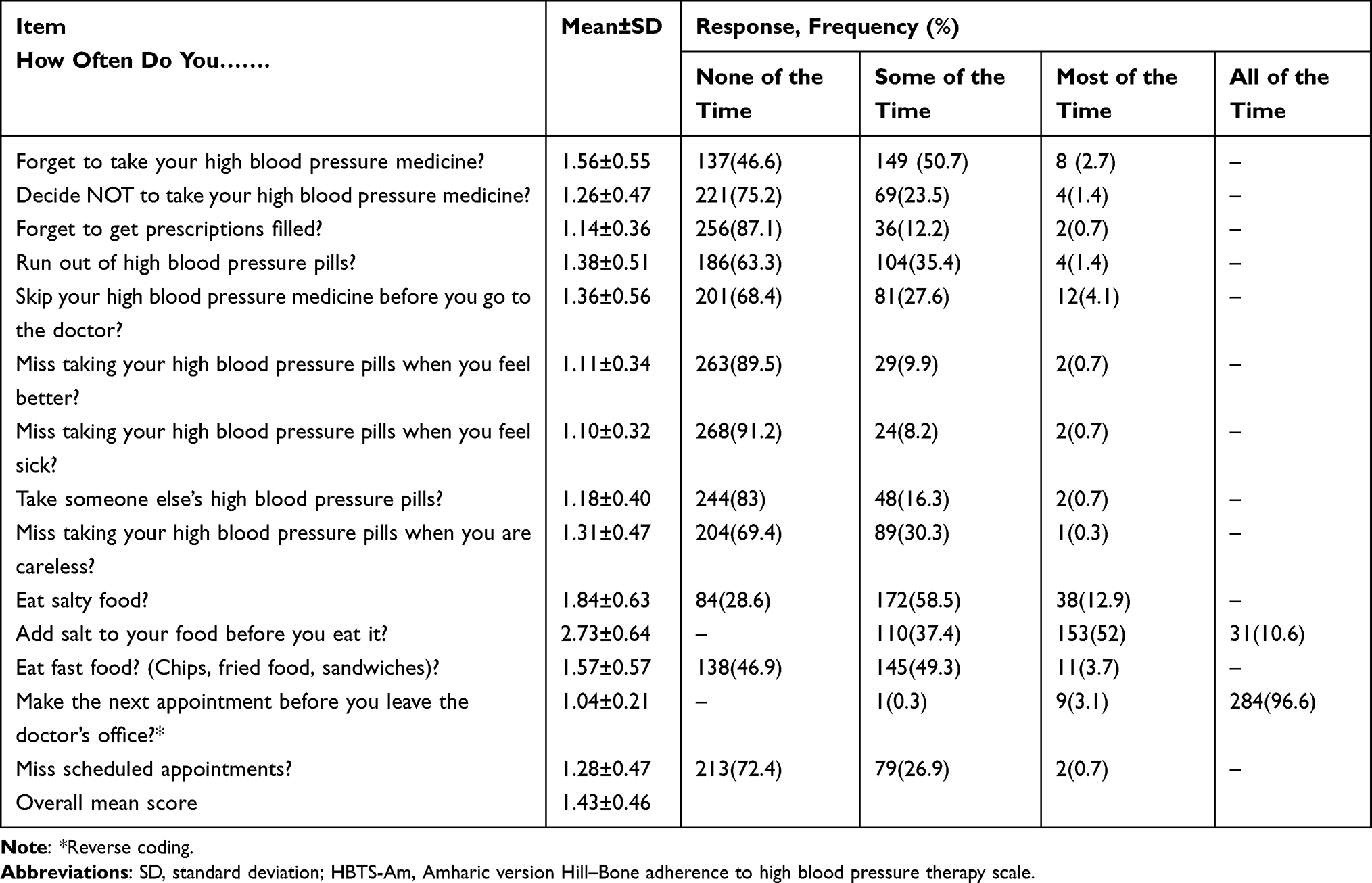 |
Table 2 Frequency of the Responses to the Amharic Version Hill–Bone Adherence to High Blood Pressure Therapy Scale (HBTS-Am) (N=294) |
Reliability
The Cronbach alpha of the 14 items HBTS was 0.801, and it was 0.771 for medication-taking subscales. Cronbach alpha was not calculated for salt intake and appointment-keeping components because they contain only three and two items, respectively. A modified scale consisting of 13 items (after the exclusion of item 6 from the original scale) showed acceptable internal consistency with Cronbach alpha of 0.806 and item-total correlation of all (>0.3). The item-total-correlation coefficients ranged from 0.307 to 0.575 (Mean= 0.440) (Table 3).
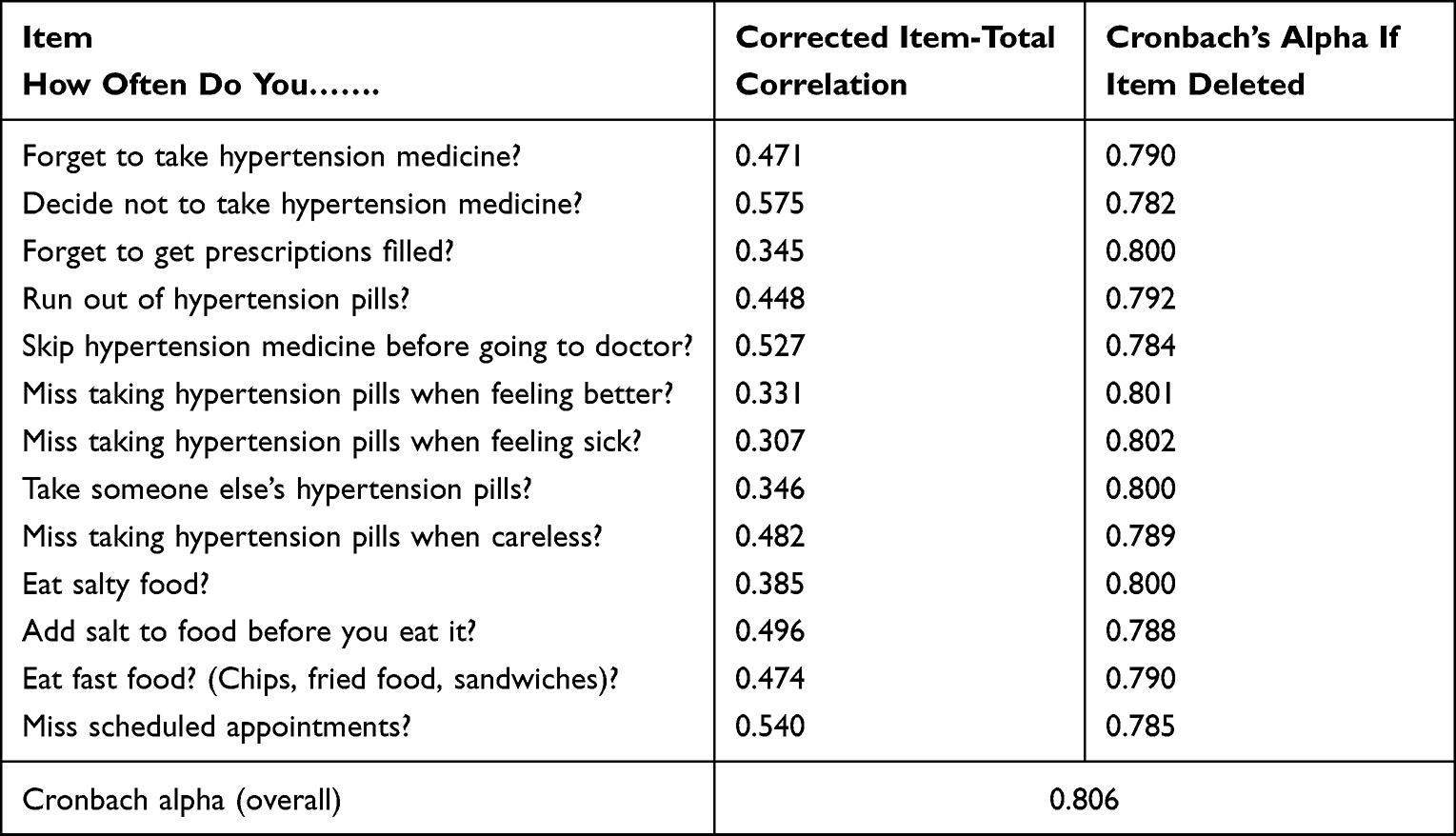 |
Table 3 Reliability Analysis of Amharic Version Hill–Bone Adherence to High Blood Pressure Therapy Scale (HBTS-Am) |
Construct Validity
Construct validity was assessed by PCA with Varimax rotation and Kaiser Normalization. First, Bartlett’s test of sphericity was used to determine if the sample size was appropriate for factor analysis and to determine if the data came from a sample of the normally distributed population. This test showed a statistical significance measure of sampling (χ2 = 1044.429, df = 91, P < 0.001), showing that the variance was different for various components of questionnaires and correlations between items were sufficiently large for PCA.
The Keiser Meyer-Olkin measure (KMO) of sampling adequacy was 0.813, showing that the samples were good enough for factor analysis. PCA with Varimax rotation revealed four underlying constructs among the 14 items (Figure 1). The eigenvalue was 4.029 for factor 1, 2.042 for factor 2, 1.136 for factor 3, and 1.027 for the 4th factor, respectively. Factor 1 explained 28.78% of the variability in the data, while factor 2, factor 3, and factor 4 explained 14.45%, 8.117%, and 7.33%, respectively (Figure 1).
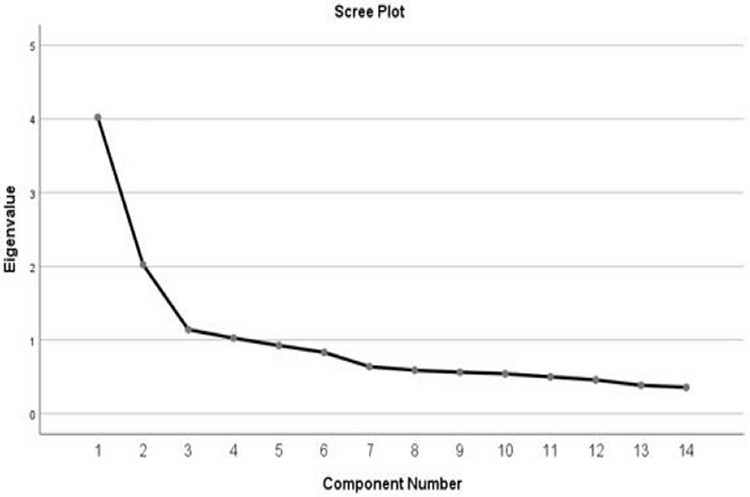 |
Figure 1 The eigenvalue of the fourteen-item Amharic version Hill–Bone adherence to high blood pressure therapy scale (HBTS-Am). |
The total variance explained by these four factors was 58.65%. All of the 14 items loaded above 0.4. All three items of the salt-taking subscale loaded on the first factor. Five of the nine items of the medication-taking subscale loaded on the second factor and four of the nine items of the medication-taking subscale loaded on the third factor. Two of the appointment-keeping items are loaded on the fourth factor (Table 4).
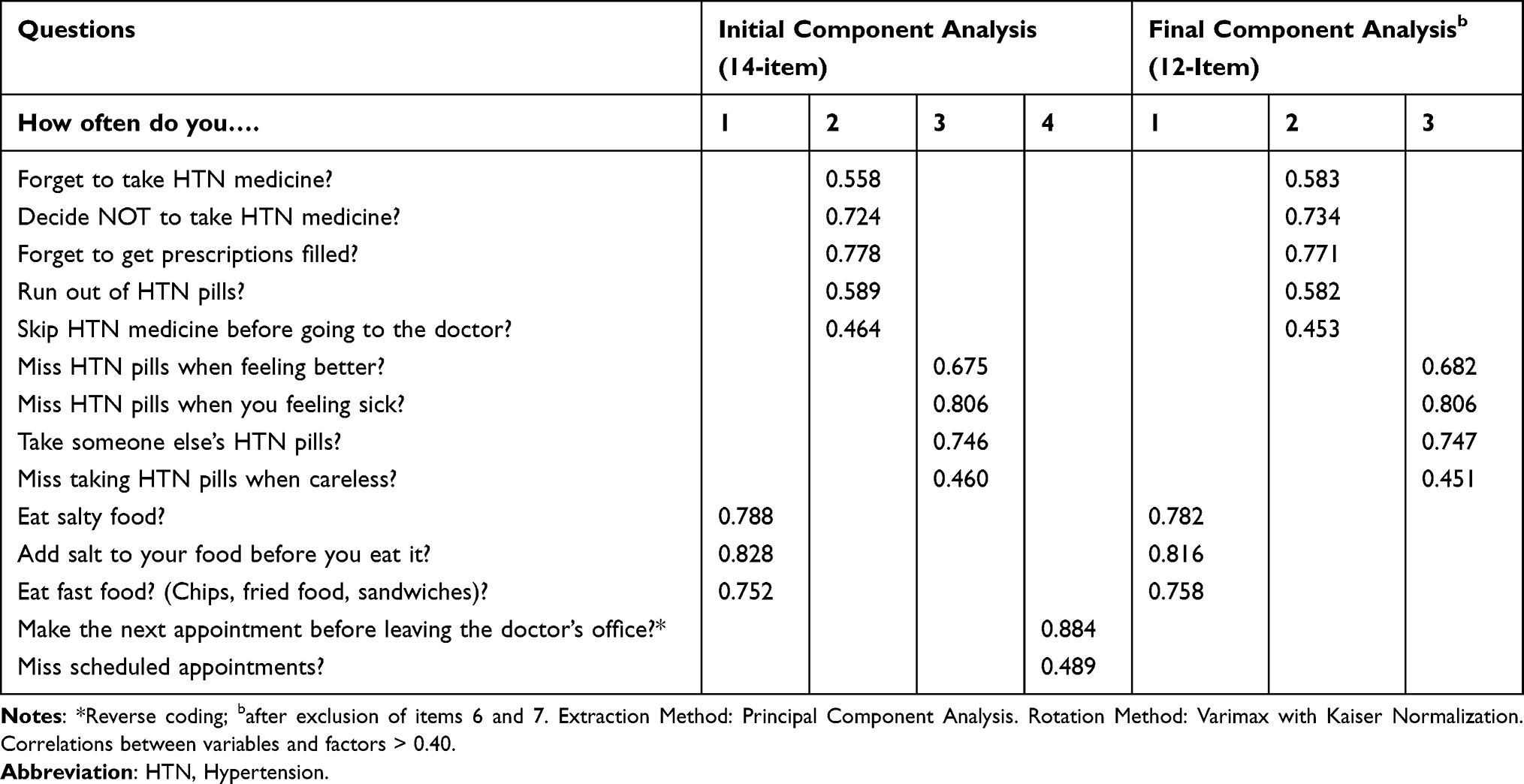 |
Table 4 Construct Validity of Amharic Version Hill–Bone Adherence to High Blood Pressure Therapy Scale (HBTS-Am) |
Following the identification of a four-factor solution via PCA, confirmatory factor analysis (CFA) was used to further test the PCA-derived factor model. The first–order CFA models were used. We assumed that the HBTS-Am was composed of four distinct correlated dimensions. The degree of fit between the data and the results of the hypothesized models was determined using goodness-of-fit indices. The loadings of items and factors were statistically significant at the 0.05 level (t values > 1.96) except for item 6 (t = 0.927, P = 0.354). The χ2-associated P value was below the 0.05 significance level (χ2 = 187.210, d.f. = 71, and P < 0.001). A good model, on the other hand, should have an insignificant P-value. Other fit indices in the model that did not achieve acceptable levels include (AGFI = 0.873, CFI = 0.881, and IFI = 0.883), whereas indices like (χ2/d.f. = 2.637, GFI = 0.914, and RMSEA =0.075) were in the acceptable range (Table 5).
 |
Table 5 Model Fit Summary of Amharic Version Hill–Bone Adherence to High Blood Pressure Therapy Scale (HBTS-Am) |
Predictive Validity
To measure the predictive validity, the correlation between the original 14-item scale, the modified 13-item Amharic scale, the Amharic version medication adherence subscale, the modified 12-item Amharic scale, and blood pressure were assessed. A significant correlation was seen only between the modified 12-item Amharic scale, and systolic blood pressure (Table 6).
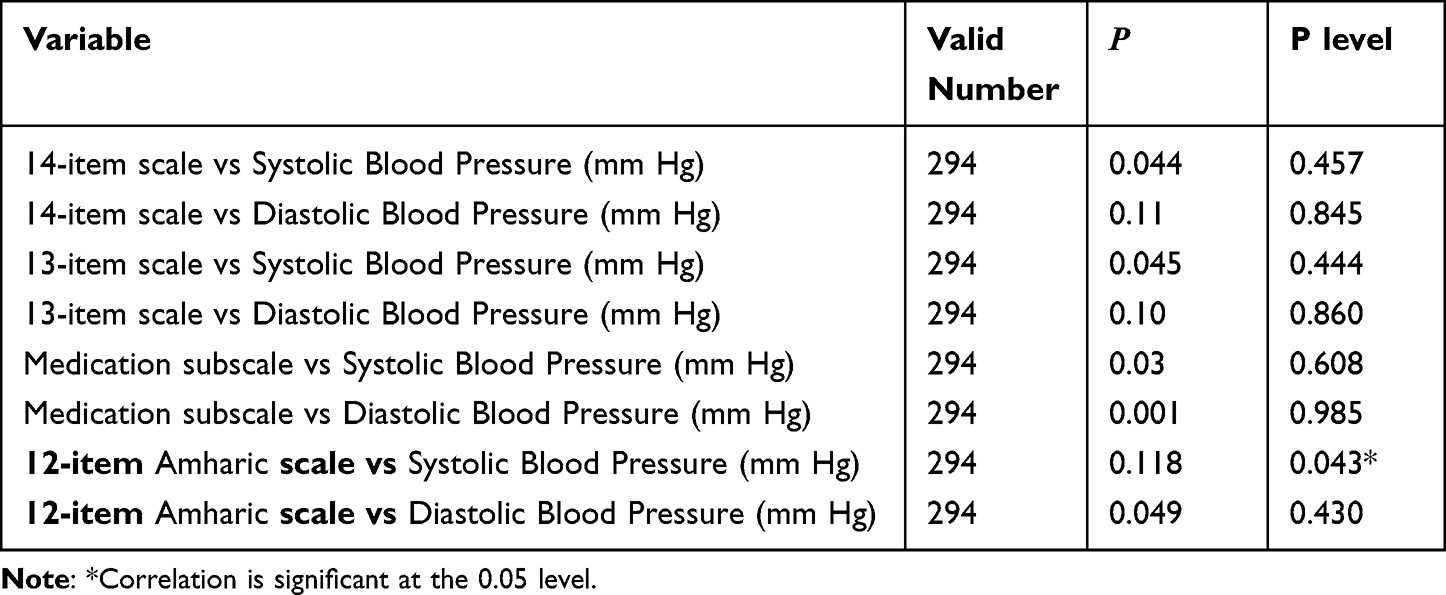 |
Table 6 Predictive Validity of the 14-Item and 13-Item Modified Hill-Bone Scales and Medication Compliance Subscale (Pearson’s Correlation) |
Discussion
The findings of this study confirmed that HBTS-Am has acceptable reliability and validity for the assessment of treatment adherence in Ethiopian hypertensive patients. In addition, this study demonstrated that many behavioral aspects of the fundamental elements of HTN care and control, such as medication taking, appointment keeping, and salt intake reduction are measurable across cultures. Second, we demonstrated that robust psychometric methods can be used effectively in a variety of cultural groups, and the data collected by such a scale can be used for educating patients, behavioral reinforcement, and making treatment decisions.
Our study revealed that the modified 13-item HBTS showed reasonable internal consistency after excluding one of the two items of appointment keeping subscale (Item with reverse coding). This item was deleted because of two reasons. One reason is that it is inappropriate for the local setting, where patients do not make appointments. This is similar to the Malay,26 South African,27 and Nambian28 versions of HBTS where appointments are given by healthcare professionals. The failure to achieve the empirically desired inter-item correlation (<0.3) was the second reason for this item’s deletion. Similarly, this item fails to achieve the desired inter-item correlation in the original scale, however, since the author believed that it was premature to delete the item due to its clinical importance in assessing patient behavior in the setting it was retained and further tested for cross-validation was recommended. However, in our case, we excluded the time since it does not apply to the local setting and has a lower inter-item correlation.
Cronbach alpha of the original scale was determined using two community-based samples of hypertensive adult patients enrolled in clinical trials to improve HTN care and control named Study 1 and Study 2, respectively. Study 1, entitled “Comprehensive high blood pressure care for young black males” was conducted among a sample of 309 men while Study 2 entitled “Urban African American Community-based HBP control program” was a community-based clinical trial with 718 samples of hypertensive patients. Cronbach alpha for the total scale was 0.85 for Study 2 and 0.74 for Study 1. In our case, the Cronbach alpha of the modified 13-item HBTS-Am was 0.806 which is comparable with the 11-item South African version [Cronbach alpha = 0.79],27 the 14-item Polish [Cronbach alpha = 0.80]29 and slightly lower than the 14-item Chinese version [Cronbach alpha = 0.857]17 and Nepalese version [Cronbach alpha = 0.846].30 Some other versions like the 12-item Namibian [Cronbach alpha = 0.695],28 the 14-item Persian [Cronbach alpha = 0.44]31 and 14-item Turkish [Cronbach alpha = 0.72]32 demonstrated lower Cronbach alpha compared to our study. The possible rationale behind these discrepancies might be the difference in the number of items included and the variability of psychometric features of the HBTS from population to population due to the nature of items included in the tool that might have intercultural variability. This implies that a scale that may have excellent reliability with one population may have only marginal reliability in another. This implies the item requires not only linguistic translation and adaptation but also validity and reliability testing before its use across different cultures.
In this study, initial factor analysis generated four components for the 14 items. Following the deletion of one item, three components with one item of appointment-keeping component loading on the salt intake were created, resulting in an unmeaningful construct. When the two items of appointment keeping subscale (Item 6 and 7) were deleted, it resulted in more clustering of items with three components. This suggests that the two items may have a poor correlation with the remaining items. Even though the 12-item construct demonstrates a meaningful construct, we believe it is reasonable to consider the 13-item construct to be valid. The rationale for this is that, first, the 13-item did not show a meaningful construct because a single item cannot be a construct; second, we considered the potential importance of appointment-keeping assessment items as it is one of the critical patient behaviors that affect adherence.
The construct validity of the original HBTS showed three components which include medication adherence, salt intake, and appointment keeping, whereas, our study showed two components for medication adherence and one component for salt intake. This finding is in line with the Persian,31 Malay,26 and South African27 versions, where appointment-keeping was not a distinct factor. Although the study’s factor analysis revealed two components for medication adherence, no meaningful theoretical concept underpinning each concept was identified. This is similar to the findings of the Chinese17 and Malay26 versions of HBTS. However, in contrast to this, the Turkish32 and Korean American33 versions of HBTS found two factors related to the medication adherence scale which were unintentional and intentional medication non-adherence. This may show subtle differences in living habits between cultures can make one item more or less difficult than others in the questionnaire, and such changes can affect the statistical or psychometric properties of an instrument.
The original HBTS studies found a significant correlation between BP control and the total scale at follow-up in both study 1 and study 2. Similar results were seen in the Korean American version,29 where the 8-item HBMA-K demonstrated a positive and significant correlation with systolic BP and diastolic BP, perhaps as a result of Korean Americans’ shared cultural background with the HBTS population. In contrast, the correlation was found only between 12 items of HBTS-Am and DBP in our study. This is in line with the South African version34 where a positive correlation was seen between the 10-item scale and DBP. Furthermore, similar to Persian,31 Malay,26 and Germany35 versions, our study found no statistically significant correlation between BP and the 14-item HBTS-Am, 13-item HBTS-Am, and medication adherence subscale of HBTS-Am. This could be due to differences in participants’ BP control status and interpretation of controlled BP status compared to the original study.
Our study has certain limitations. Self-reported questionnaires may introduce recall bias and generalizing the findings to other settings and populations is also difficult. Furthermore, we did not check the test-retest reliability of the tool which is important for checking its stability over time.
Conclusion
The Amharic version of the Hill-Bone adherence to high blood therapy scale is a valid and reliable scale and can be used to assess adherence to antihypertensive medications in Amharic-speaking patients in Ethiopia.
Abbreviations
BP, Blood Pressure; CFA, Confirmatory Factor Analysis; HBP, High Blood Pressure; HBTS, The Hill–Bone Adherence to High Blood Pressure Therapy Scale; HBTS-Am, Amharic Version Hill–Bone Adherence to High Blood Pressure Therapy Scale; HTN, Hypertension; KMO, Kaiser-Meyer-Olkin; MMAS, Morisky Medication Adherence Scale; PCA, Principal Component Analysis; SPHMMC, Saint Paul’s Hospital Millennium Medical College; SPSS,Statistical Package for Social Sciences, TASH, Tikur Anbessa Specialized Hospital.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Ethics Review Committee of the School of Pharmacy, College of Health Sciences, Addis Ababa University (ERB/SOP/258/13/2021). Permission to conduct the study was sought from the renal unit of TASH (PCP/260/13/21) and SPHMMC (PM23/327), and permission to use the HBTS was obtained from Johns Hopkins University. Written informed consent was obtained from participants, and confidentiality was maintained through anonymity.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was provided by the Addis Ababa University School of Postgraduate Studies.
Disclosure
The authors declare they have no competing interests for this work.
References
1. Lloyd-Jones DM, Morris PB, Ballantyne CM, et al. Focused update of the 2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American college of cardiology task Fo. J Am Coll Cardiol. 2017;70(14):1785–1822. doi:10.1016/j.jacc.2017.07.745
2. Naghavi M, Wang H, Lozano R, et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385(9963):117–171.
3. Unger T, Borghi C, Charchar F, et al. International society of hypertension global hypertension practice guidelines. Hypertension. 2020;75(6):1334–1357. doi:10.1161/HYPERTENSIONAHA.120.15026
4. Barrera L. High Blood Pressure prevention and control: from evidence to action Presión arterial elevada: de la evidencia a la acción. Colombia Medica. 2018;49(2):137–138. doi:10.25100/cm.v49i2.3940
5. Wang X, Hao G, Chen L, et al. Hypertension-mediated organ damage and established cardiovascular disease in patients with hypertension: the China hypertension survey, 2012 – 2015; 2021:1–7.
6. Zeng Z, Chen J, Xiao C, Chen W. A global view on prevalence of hypertension and human develop index. Ann Glob Health. 2020;86(1):1–6. doi:10.5334/aogh.2591
7. Sorato MM, Davari M, Kebriaeezadeh A, Sarrafzadegan N, Shibru T, Fatemi B. Reasons for poor blood pressure control in Eastern Sub-Saharan Africa: looking into 4P’s (primary care, professional, patient, and public health policy) for improving blood pressure control: a scoping review. BMC Cardiovasc Disord. 2021;21(1):1–15. doi:10.1186/s12872-021-01934-6
8. Bosu WK, Reilly ST, Aheto JMK, Zucchelli E. Hypertension in older adults in Africa: a systematic review and meta-analysis. PLoS One. 2019;14(4):1–25. doi:10.1371/journal.pone.0214934
9. Addo J, Smeeth L, Leon DA. Hypertension in sub-Saharan Africa: a systematic review. Hypertension. 2007;50(6):1012–1018. doi:10.1161/HYPERTENSIONAHA.107.093336
10. Legese N, Tadiwos Y. Epidemiology of hypertension in Ethiopia: a systematic review. Integr Blood Press Control. 2020;13:135–143. doi:10.2147/IBPC.S276089
11. Tola Gemeda A, Regassa LD, Weldesenbet AB, Merga BT, Legesse N, Tusa BS. Adherence to antihypertensive medications and associated factors among hypertensive patients in Ethiopia: systematic review and meta-analysis. SAGE Open Med. 2020;8:205031212098245. doi:10.1177/2050312120982459
12. Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957–967. doi:10.1016/S0140-6736(15)01225-8
13. Nielsen J, Shrestha AD, Neupane D, Kallestrup P. Non-adherence to anti-hypertensive medication in low- and middle-income countries: a systematic review and meta-analysis of 92443 subjects. J Human Hypertens. 2017;31(1):14–21. doi:10.1038/jhh.2016.31
14. Jaa M, Hadi MA, Kheir N, et al. A qualitative exploration of barriers to medication adherence among patients with uncontrolled diabetes in Qatar: integrating perspectives of patients and health care providers. Patient Prefer Adherence. 2018;12:2205–2216. doi:10.2147/PPA.S174652
15. Anghel LA, Farcas AM, Oprean RN. An overview of the common methods used to measure treatment adherence. Med Pharm Rep. 2019;92(2):117–122. doi:10.15386/mpr-1201
16. Kaleva V. Adherence to medication. Pediatriya. 2015;55(2):68–69.
17. Pan J, Hu B, Wu L, Wang H, Lei T, Liu Z. The translation, reliability and validity of the Chinese version of the hill–bone compliance to high blood pressure therapy scale in adults with hypertension. Patient Prefer Adherence. 2020;14:1853–1860. doi:10.2147/PPA.S268031
18. Culig J, Leppée M. From Morisky to Hill-bone; self-reports scales for measuring adherence to medication. Coll Antropol. 2014;38(1):55–62.
19. Sison G. The Morisky Medication adherence scale: an overview. Pillsy; 2018.
20. Kim MT, Hill MN, Bone LR, Levine DM. Development and testing of the Hill-Bone compliance to high blood pressure therapy scale. Prog Cardiovasc Nurs. 2000;15(3):90–96. doi:10.1111/j.1751-7117.2000.tb00211.x
21. Kline P. An Easy Guide to Factor Analysis; 2014.
22. Costello AB, Osborne JW. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10(7).
23. World Health Organization. WHO | Process of translation and adaptation of instruments. WHO; 2017.
24. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. doi:10.1111/j.1524-4733.2005.04054.x
25. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297–334. doi:10.1007/BF02310555
26. Cheong AT, Tong SF, Sazlina SG. Validity and reliability of the Malay version of the hill-bone compliance to high blood pressure therapy scale for use in primary healthcare settings in Malaysia: a cross-sectional study. Malays Fam Physician. 2015;10(2):36–44.
27. Herapy PRT, In SC, Frican a SOA, et al. Cross-cultural validation of the Hill-Bone compliance to high blood pressure therapy scale in a South African, Primary healthcare setting. Ethnicity. 2006;16:286–291.
28. Nashilongo MM, Singu B, Kalemeera F, et al. Assessing adherence to antihypertensive therapy in primary health care in Namibia: findings and implications. Cardiovasc Drugs Ther. 2017;31(5–6):565–578. doi:10.1007/s10557-017-6756-8
29. Uchmanowicz I, Jankowska-Polańska B, Chudiak A, Szymańska-Chabowska A, Mazur G. Psychometric evaluation of the polish adaptation of the Hill-Bone compliance to high blood pressure therapy scale. BMC Cardiovasc Disord. 2016;16(1):1–6. doi:10.1186/s12872-016-0270-y
30. Shakya R, Shrestha R, Shrestha S, et al. Translation, cultural adaptation and validation of the Hill Bone compliance to high blood pressure therapy scale to Nepalese language. Patient Prefer Adherence. 2022;16(February):957–970. doi:10.2147/PPA.S349760
31. Dehghan M, Nayeri N, Iranmanesh S. Validating the Persian version of the Hill-Bone’s Scale of “compliance to high blood pressure therapy. Br J Med Med Res. 2015;5(2):235–246. doi:10.9734/BJMMR/2015/13061
32. Karademir M, Koseoglu IH, Vatansever K, Van Den Akker M. Validity and reliability of the Turkish version of the HillBone compliance to high blood pressure therapy scale for use in primary health care settings. Eur J Gen Pract. 2009;15(4):207–211. doi:10.3109/13814780903452150
33. Kim EY, Han HR, Jeong S, et al. Does knowledge matter? Intentional medication nonadherence among middle-aged Korean Americans with high blood pressure. J Cardiovasc Nurs. 2007;22(5):397–404. doi:10.1097/01.JCN.0000287038.23186.bd
34. Lambert EV MS, PhD, Steyn K MSc, MD, NED, Stender S BSc, Everage N BSc, Fourie JM BA, Martha Hill P. Introduction. Cross-cultural validation of the Hill-Bone compliance to high blood pressure therapy scale in a South African, primary healthcare setting objectives. Ethn Dis. 2006;16:286–291.
35. Koschack J, Marx G, Schnakenberg J, Kochen MM, Himmel W. Comparison of two self-rating instruments for medication adherence assessment in hypertension revealed insufficient psychometric properties. J Clin Epidemiol. 2010;63(3):299–306. doi:10.1016/j.jclinepi.2009.06.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Cross-Cultural Adaptation, Validity, and Reliability Testing of the Tilburg Frailty Indicator (TFI) Amharic Version for Screening Frailty in Community-Dwelling Ethiopian Older People
Kasa AS, Drury P, Chang HCR, Lee SC, Traynor V
Clinical Interventions in Aging 2023, 18:1115-1127
Published Date: 24 July 2023
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023
Adherence to Lifestyle Modification Practices and Its Associated Factors Among Hypertensive Patients in Bahir Dar City Hospitals, North West Ethiopia
Geremew G, Ambaw F, Bogale EK, Yigzaw ZA
Integrated Blood Pressure Control 2023, 16:111-122
Published Date: 29 November 2023