Back to Journals » Cancer Management and Research » Volume 18

Deficient Mismatch Repair Subtypes in Vietnamese Colorectal Cancer: Clinicopathologic Associations, Predictive Modeling, and IHC-PCR Concordance
Authors Trinh HD, Pham QT ![]() , Phong NH, Huong Ly TT, Ho QC, Vu HA, Kha VV, Ngo QD
, Phong NH, Huong Ly TT, Ho QC, Vu HA, Kha VV, Ngo QD
Received 9 December 2025
Accepted for publication 11 March 2026
Published 17 March 2026 Volume 2026:18 587649
DOI https://doi.org/10.2147/CMAR.S587649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Harikrishna Nakshatri
Hoang Duc Trinh,1,2 Quoc Thang Pham,1 Nguyen Hong Phong,2 Tran Thi Huong Ly,3 Quoc Chuong Ho,4 Hoang Anh Vu,1,4 Vo Van Kha,5 Quoc Dat Ngo1
1Department of Histology, Embryology and Pathology, School of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 2Department of Pathology, Faculty of Medicine, Can Tho University of Medicine and Pharmacy, Can Tho, 94000, Vietnam; 3Department of Pathophysiology – Immunity, Can Tho Oncology Hospital, Can Tho, 94000, Vietnam; 4Center for Molecular Biomedicine, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 5Department of Internal Oncology, Can Tho Oncology Hospital, Can Tho, 94000, Vietnam
Correspondence: Quoc Dat Ngo, Department of Histology, Embryology and Pathology, School of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, 217 Hong Bang Street, Cho Lon Ward, Ho Chi Minh City, Vietnam, Tel +84-28-3855-8411, Fax +84-28-3855-2304, Email [email protected]
Background: Microsatellite instability (MSI) caused by deficient mismatch repair (dMMR) influences prognosis and immunotherapy response in colorectal cancer. The dMMR phenotype includes MutL-deficient (dMutL) and MutS-deficient (dMutS) subtypes, which may differ in their clinicopathologic profiles, yet data from Southeast Asian populations remain limited. Our study aimed to investigate the associations between clinicopathological features with MSI/dMMR status and concordance in dMMR identification between immunohistochemistry (IHC) and polymerase-chain reaction (PCR) in Vietnamese patients.
Methods: Two hundred and twelve colorectal cancer patients were included. Tumor tissues underwent hematoxylin and eosin staining, IHC staining (for four MMR proteins: MLH1, PMS2, MSH2, and MSH6), and PCR assay. Clinicopathological characteristics were collected and compared between dMMR tumors and their subtypes (dMutL and dMutS) with proficient MMR (pMMR). Firth’s logistic regression was conducted to construct the model predicting each subtype of dMMR based on clinicopathological characteristics. A PCR assay was performed on selected cases, and the concordance in MMR results between IHC and PCR was examined.
Results: dMMR tumors accounted for 25.5% of total tumors. Compared to pMMR tumors, dMutL tumors showed differences in tumor location, vascular invasion, lymphovascular invasion, histopathologic grade, and pTNM stage, whereas dMutS tumors showed differences in tumor size and pTNM stage. MMR results between IHC and PCR showed high concordance (Kappa = 0.88, 95% CI: 0.78– 0.97), with IHC demonstrating 100% sensitivity, 87.5% specificity, and 88.9% precision relative to PCR. The dMutL predictive model exhibited good discrimination and calibration, but the dMutS model exhibited poor performance.
Conclusion: dMMR status, especially dMutL, might be associated with clinicopathologic characteristics, which might support decision-making in clinical practice. These findings require validation in larger cohorts but may inform clinical screening practices in resource-limited settings.
Keywords: colorectal cancer, microsatellite instability, deficient mismatch repair, clinicopathology, Vietnam
Introduction
Colorectal cancer is the third most commonly diagnosed cancer and the second leading cause of cancer-related deaths globally, with approximately 1.93 million new cases and 904,000 deaths in 2022.1 In Vietnam, colorectal cancer ranked fourth among all cancers in 2022, with 16,835 new cases (9.7% of total cancers), and was the fifth leading cause of cancer death, with 8,454 deaths that year.1 Risk factors for colorectal cancer include genetic factors, diet, and lifestyle factors, which might be different among countries worldwide.2 Despite recent advancements, early diagnosis and treatment for this type of cancer still pose challenges to healthcare systems, especially in developing countries.3,4
The pathogenesis of colorectal cancer is complicated, in which two main molecular pathways have been reported, including the chromosomal instability (CIN) and microsatellite instability (MSI) pathways.5 MSI, defined as alterations in microsatellite length, is commonly observed in colorectal cancer that showed distinct clinicopathologic features and treatment responses compared to microsatellite stability (MSS) tumors.6 MSI is mainly caused by a deficiency of mismatch repair (MMR) proteins, which play an important role in correcting single base mismatches and small insertions or deletions.7 The MMR system relies on two functional heterodimers: MutSα (MutS homolog 2 (MSH2)/MutS homolog 6 (MSH6) proteins), which recognizes DNA mismatches, and MutLα (MutL homolog 1 (MLH1)/Postmeiotic Segregation Increased 2 (PMS2)), which is subsequently recruited to coordinate downstream repair.8,9 In each heterodimer, one protein (MLH1 or MSH2) is the obligate stabilizing partner: loss of MLH1 leads to secondary degradation of PMS2, and loss of MSH2 leads to secondary degradation of MSH6. Therefore, by immunohistochemistry, loss of both MLH1 and PMS2 expression (with intact MSH2/MSH6) indicates a MutL-pathway defect (dMutL), most commonly caused by MLH1 promoter hypermethylation or germline MLH1 mutation. Loss of both MSH2 and MSH6 expression (with intact MLH1/PMS2) indicates a MutS-pathway defect (dMutS), typically associated with germline MSH2 mutations. Isolated loss of PMS2 or MSH6, while less common, points to primary defects in these individual genes.9
Several techniques have been used to detect MSI/dMMR, including immunohistochemistry (IHC) and polymerase chain reaction (PCR) assay.9,10 Detecting MSI/dMMR status is important not only for screening Lynch syndrome but also for predicting treatment effectiveness in patients with colorectal cancer. Although PCR is considered a gold standard for MSI identification, IHC has been considered the feasible and cost-effective alternative approach, especially in developing countries.10
The clinicopathologic characteristics and molecular subtypes of colorectal cancer have been considered to exhibit significant geographic and ethnic heterogeneity.11 Investigating MSI/dMMR status and its relation to clinicopathologic characteristics in a specific population might further provide evidence supporting decision-making in regional clinical practice. In Vietnam and other resource-limited settings in Southeast Asia, access to PCR-based MSI testing is often restricted to tertiary referral centers due to equipment costs and technical requirements. Establishing the reliability of IHC as an alternative is therefore of particular clinical relevance for regional hospitals where MMR testing is increasingly recommended for guiding immunotherapy decisions but PCR infrastructure may be unavailable. To address this, the primary objective of this study was to estimate the MSI/dMMR prevalence and its association with key clinicopathologic features in a cohort of Vietnamese patients with colorectal cancer. In addition, the concordance between IHC and PCR in detecting MSI/dMMR was also examined.
Materials and Methods
Participants
In this retrospective cross-sectional study, we recruited patients who had received confirmed diagnosis of colorectal cancer and underwent treatment at Can Tho Oncology Hospital from 01/01/2019 to 31/12/2021. The patients were included in this study if: 1) they were diagnosed with primary colorectal cancer and had undergone colectomy surgery with histopathological examination results being colorectal carcinoma; and 2) they had MMR measurement. The patients were excluded from this study if they had at least one of the following: 1) Recurrent carcinoma; 2) underwent chemotherapy/radiotherapy before; 3) coexisting tumors. The study protocol was approved by the Institute Research Board of the University of Medicine and Pharmacy in Ho Chi Minh City (approval number: 20/HĐĐĐ-ĐHYD on 20/01/2022) and complied with the Declaration of Helsinki. Informed consent was obtained from all participants before enrolling in this study. After applying inclusion and exclusion criteria, 212 eligible patients were identified during the study period and all were enrolled.
Demographic, Clinical, and Preclinical Data Collection
Clinicopathology data, including demographic and tumor characteristics, in this study were obtained from the hospital’s medical records. For demographic data, we collected data on age and sex. For tumor characteristics, the data on tumor size, tumor location, histopathological types, perineural invasion (PNI), vascular invasion, lymphovascular invasion (LVI), histopathological grade, and pathological TNM classification (pTNM) were included. In addition, the presence of MutL homolog 1 (MLH1), Postmeiotic Segregation Increased 2 (PMS2), MutS homolog 2 (MSH2), and MutS homolog 6 (MSH6) proteins was collected to determine whether the tumors are dMMR (dMutL or dMutS) or pMMR. In this study, histopathological tissue classification was based on WHO classification, including non-mucinous adenocarcinoma, mucinous adenocarcinoma, and signet-ring-cell carcinoma.
Tumors were classified as dMutL if IHC showed loss of MLH1 and/or PMS2 with intact MSH2 and MSH6 expression, and as dMutS if IHC showed loss of MSH2 and/or MSH6 with intact MLH1 and PMS2 expression. Cases showing concurrent loss of proteins from both MutL and MutS pathways were classified as dual dMutL-dMutS deficiency (n = 3). These dual-deficiency cases were excluded from the dMutL-pMMR and dMutS-pMMR comparisons due to their small number but were included in the dMutL predictive model, as they technically exhibited MutL pathway loss.
Hematoxylin and Eosin (H&E) Staining
All tissue samples were fixed in 10% neutral buffered formalin for 6–48 hours, at a fixative-to-tissue volume ratio of approximately 20:1, prior to processing and embedded in paraffin. We sectioned the resulting formalin-fixed, paraffin-embedded (FFPE) blocks at 3–5 µm, mounted the sections on positively charged slides, and then baked them at 60°C for 30 minutes to ensure adhesion. A representative slide from each block was stained with Hematoxylin and Eosin (H&E) for routine morphological review.
For staining, the slides first undergo deparaffinization and rehydration. They are then stained with hematoxylin, which imparts a blue-violet color to cell nuclei. This is followed by a brief differentiation step in 0.5% acid alcohol to remove excess stains and a bluing step in 1% ammonium hydroxide to sharpen nuclear detail. Subsequently, the slides are counterstained with eosin, which stains the cytoplasm and extracellular matrix in varying shades of pink and red. Finally, the slides are dehydrated through graded alcohols, cleared, and permanently coverslipped for microscopic examination.12
Immunohistochemical Staining and Interpretation Protocol
We performed immunohistochemistry for the four mismatch repair (MMR) proteins including MLH1, MSH2, MSH6, and PMS2, on a VENTANA BenchMark automated platform. The analysis used the following ready-to-use primary antibodies from VENTANA Medical Systems, Inc., including anti-MLH1 (clone M1; Cat. No. 760–5091), anti-MSH2 (clone G219-1129; Cat. No. 760–5093), anti-MSH6 (clone SP93; Cat. No. 760–5092), and anti-PMS2 (clone A16-4; Cat. No. 760-5094) (more details were provided in their website at: https://diagnostics.roche.com/global/en/products/tests/ventana-mmr-rxdx-panel.html). Protein expression was visualized with a DAB (3,3’-Diaminobenzidine) chromogen, and all slides were counterstained with Hematoxylin.
A pathologist evaluated the nuclear immunoreactivity for each antibody. Expression was considered intact if any distinct brown nuclear staining was observed in tumor cells. According to the manufacturer’s instructions and the FDA approval for the Ventana MMR panel, this test is validated as a qualitative assay and classified into two categories – intact or loss – based on nuclear staining. To ensure reliability, it is recommended that at least ≥50 viable tumor cells should be available for evaluation. We confirmed the validity of each stain by verifying appropriate staining patterns in internal controls, such as lymphocytes and normal epithelial cells, on every slide. Representative examples of intact and lost MMR protein expression are presented in Figure 1.
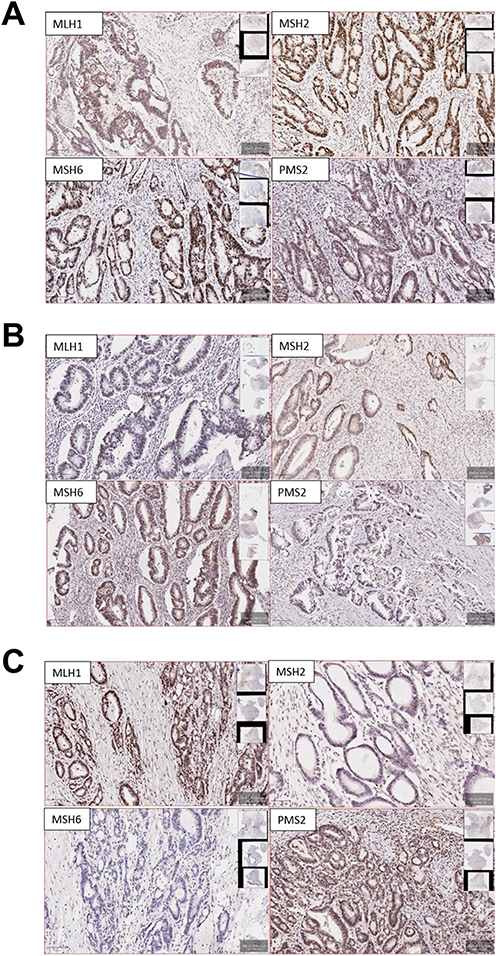 |
Figure 1 Representative immunohistochemical staining for mismatch repair (MMR) proteins. (A) Proficient mismatch repair (pMMR) case showing retained nuclear expression of all four MMR proteins (MLH1, PMS2, MSH2, and MSH6). (B) Deficient MutL complex (dMutL) case showing loss of MLH1 and PMS2 expression with retained expression of MSH2 and MSH6. (C) Deficient MutS complex (dMutS) case showing loss of MSH2 and MSH6 expression with retained expression of MLH1 and PMS2. All images were acquired at ×100 magnification. |
Analysis of MSI by Digital Droplet PCR
In this study, 96 cases of 212 cases, including all 54 IHC-identified dMMR cases and 42 randomly selected pMMR cases, were selected to perform analysis of MSI by digital droplet PCR.13 This enriched sampling design ensures adequate representation of both dMMR and pMMR groups while accounting for practical constraints of digital droplet PCR costs and tissue availability. We acknowledge that this enriched design does not reflect the true prevalence in the study population, and concordance metrics should be interpreted accordingly. DNA was extracted from formalin-fixed, paraffin-embedded (FFPE) specimens using the ReliaPrep™ FFPE gDNA Miniprep Kit (Promega) according to the manufacturer’s protocol.
The digital droplet PCR analysis was performed on the QX200™ System (Bio-Rad) using the Supermix for Probes. Each sample was partitioned into approximately 10,000 droplets using an automated droplet generator (Bio-Rad). The PCR reaction was conducted on a C1000 Touch Thermal Cycler under the following conditions: initial denaturation at 95°C for 10 minutes; 40 cycles of 94°C for 30 seconds and 55°C for 1 minute; followed by a final step at 98°C for 10 minutes. A temperature ramp rate of 2°C/second was applied to all steps.
Following amplification, fluorescence signals were acquired using the QX200 Droplet Reader, and the data were analyzed with QX Manager Software (version 2.1.0.10 Premium Edition). The MSI10_FFPE.apfpack kit was utilized for the assessment of 10 microsatellite loci. The analytical threshold was established using positive and negative control samples.
Tumors were classified as MSI-High (MSI-H) if two or more (≥2) loci exhibited an instability of ≥40%. Cases were classified as Microsatellite Stable (MSS) if one or fewer (≤1) loci were unstable or if the instability percentage was ≤20%.
Statistical Analysis
Continuous variables are summarized as mean (standard deviation), and categorical variables as frequency (percentage). Group differences in demographics and clinicopathological features were compared between each deficient group (dMutL, dMutS) and the mismatch-repair–proficient group (pMMR) using independent-samples t tests for continuous variables and Pearson’s χ2-tests for categorical variables. Variables showing nominal significance in these univariable comparisons were treated as candidate associated factors. To evaluate whether clinicopathological variables could predict dMutL or dMutS status, separate Firth’s bias-reduced logistic regression models were fitted for each outcome, with the candidate variables entered as predictors. Optimal decision thresholds for classification were chosen by maximizing the Youden J statistic and by the Neyman–Pearson paradigm on the ROC curve. Model performance was assessed using the areas under the ROC and precision–recall curves (ROC-AUC, PR-AUC), sensitivity, specificity, F1-score, and calibration. A p-value < 0.05 was considered significant. JASP software was used for statistical analysis. JASP software version 0.95.1.0 and R were used for data analysis.
Results
Participants’ Characteristics
Age and gender showed no significant differences between the dMMR and pMMR groups. However, tumor locations, vascular invasion, lymphovascular invasion, tumor grade, and pTNM stage, were significantly different between the two groups (p < 0.05, Table S1).
In this study, dMMR accounted for approximately 25.5% of total samples, in which MutL deficiency was about 66.7% of dMMR cases (17% of total samples) and MutS deficiency was about 27.8% of dMMR cases (7.1% of total samples). Three cases (5.6% of dMMR cases; 1.4% of total samples) expressed dual MutL-MutS deficiency. Representative IHC staining patterns for pMMR, dMutL, and dMutS are shown in Figure 1.
Associations Between MMR Status and Clinicopathological Characteristics
We compared clinicopathological characteristics between patients with dMutL/dMutS and those with pMMR to find associated factors of either dMutL or dMutS status. In this analysis, we excluded the dual dMutL-dMutS cases because the case number was small for analyses. We found significant differences in tumor location, vascular invasion, LVI, histopathological grade and pTNM stage between the dMutL group and the pMMR group (Table 1). In addition, the dMutS group showed significant differences in tumor size and pTNM stage distributions compared to the pMMR group (Table 1).
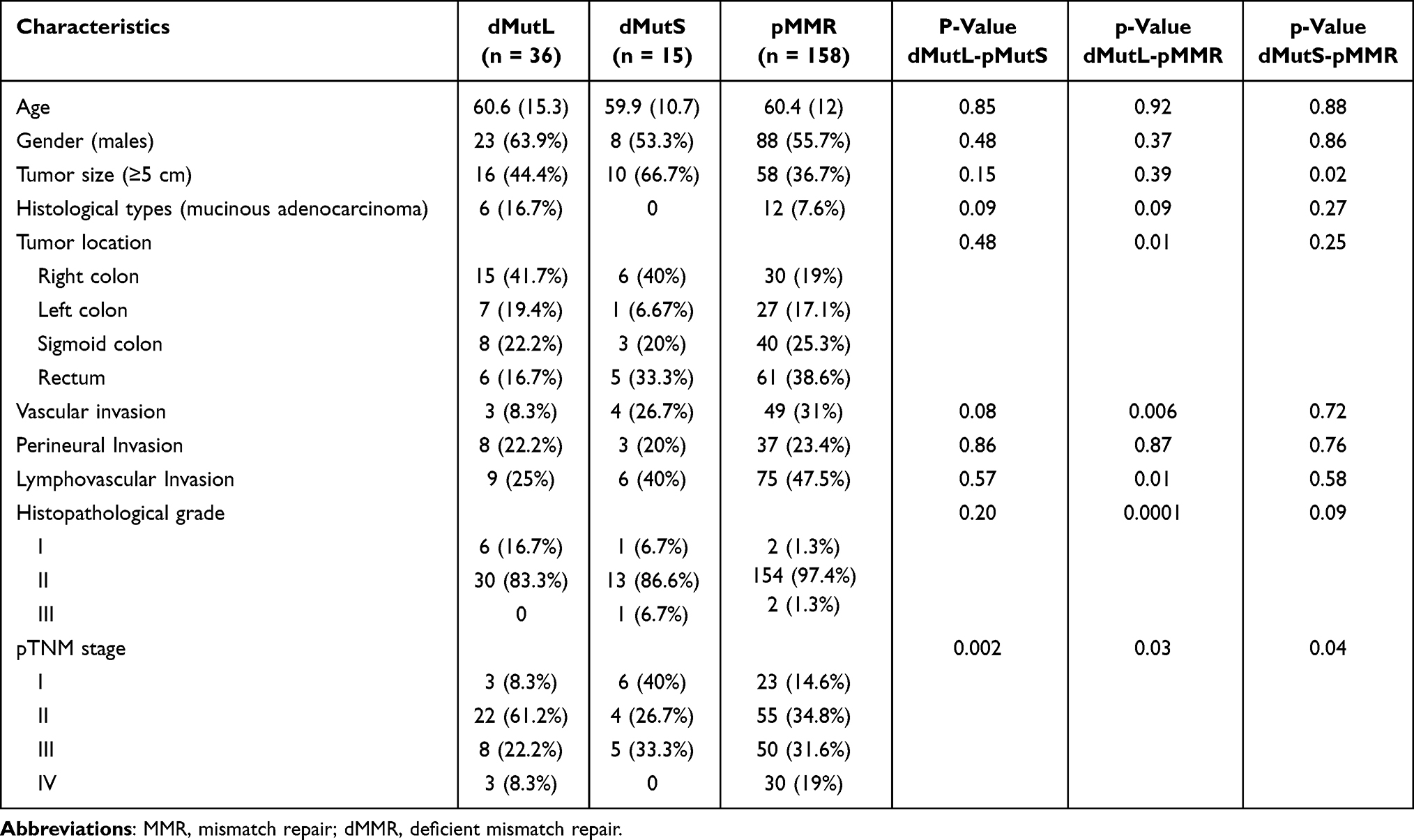 |
Table 1 Associations Between MMR Status with Demographic and Pathological Characteristics |
When directly comparing the characteristics between the dMutL and dMutS groups, only the pTNM stage was significantly different between the two groups (p = 0.002) (Table 1). However, given the small sample size of the dMutS group (n = 15), these comparisons were underpowered to detect moderate effect sizes.
Predicting dMutL and dMutS Using Clinicopathological Characteristics
Given that the dMutL status was associated with several factors, including tumor location, vascular invasion, lymphovascular invasion, histopathological grade, and pTNM stage, those factors were used as independent variables to construct the Firth’s logistic regression model predicting dMutL status. Because dual dMutL-dMutS cases technically had MutL loss, we included the three cases of dual dMutL-dMutS in this analysis. The fitted model was statistically significant (p = 1.7×10−10), with tumor locations (rectum), histopathological grade (II or III), and pTNM (II) being significant predictors in the model (Table 2). The threshold selected by maximizing the Youden J statistic on the ROC curve was 0.142, with sensitivity, specificity, precision, and F1-score being 0.897, 0.572, 0.321, and 0.473, respectively. The threshold selected by the Neyman–Pearson paradigm ROC curve was 0.307, with sensitivity, specificity, precision, and F1-score being 0.564, 0.827, 0.423, and 0.484, respectively. The PR-AUC of the model was 0.505. In addition, the calibration plot showed the good fit of the model, with the calibration slope/intercept being 1.12/0.03 (Figure 2).
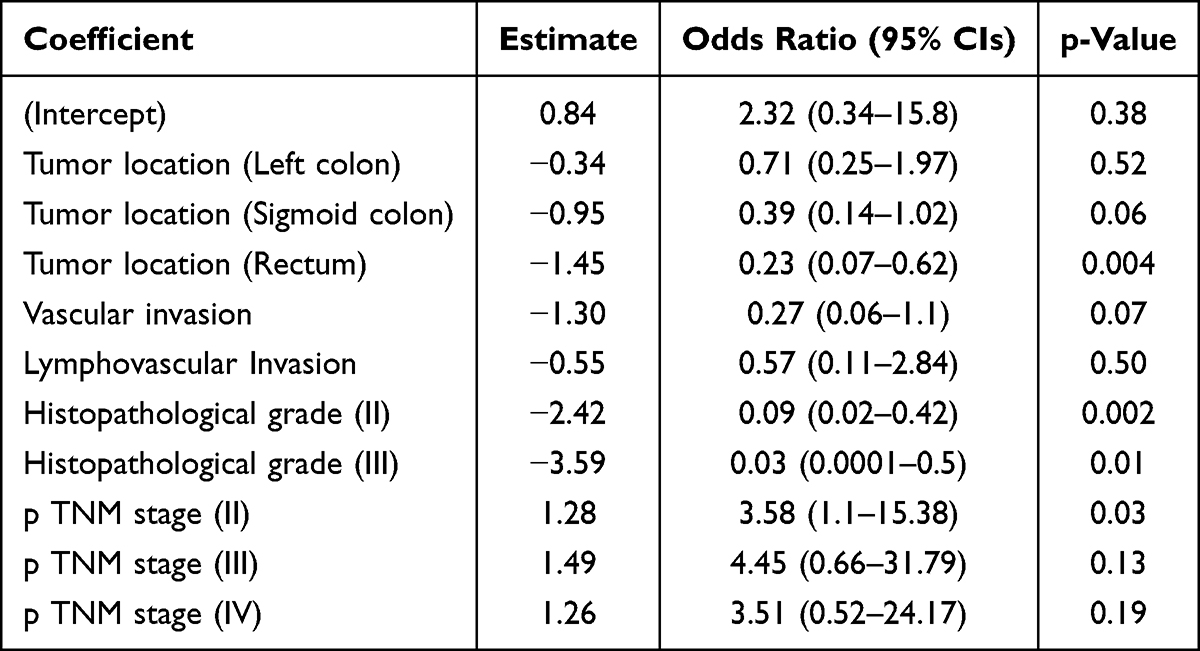 |
Table 2 The Fitted Model of Predicting dMutL Using Histopathological Characteristics |
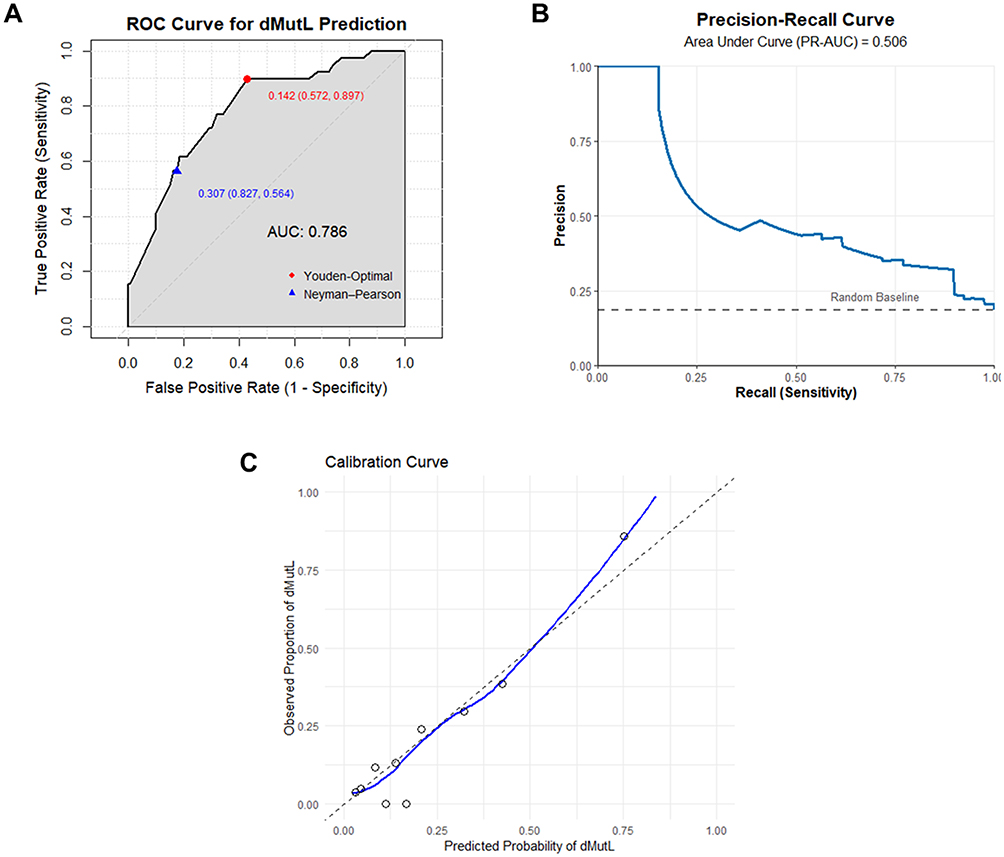 |
Figure 2 Performances of the model predicting dMutL. (A) The Receiver Operating Characteristic (ROC) curve with the area under the curve (AUC) of the model. (B) The precision-recall curve with the area under the curve (PR-AUC) of the model. (C) The calibration plot of the model. |
The Firth’s logistic regression model predicting dMutS status was also performed for reference only because the dMutS case number was too small. The fitted model was statistically significant (p = 2.22×10−16), with tumor size and pTNM (IV) being significant predictors in the model (Table S2). The threshold selected by maximizing the Youden J statistic on the ROC curve was 0.09, with sensitivity, specificity, poor precision, and poor F1-score being 0.833, 0.603, 0.163, and 0.273, respectively. The threshold selected by the Neyman–Pearson paradigm ROC curve was 0.232 with poor sensitivity, specificity, poor precision, and a poor F1-score of 0.167, 0.938, 0.2, and 0.182, respectively. The PR-AUC of the model was 0.174 (Figure S1).
Agreement Between IHC-Based MMR Status and PCR results
To investigate the concordance between MMR status detected by IHC and PCR assays, we performed PCR analysis in the 96 selected cases of 212 cases. Six disagreed cases were shown, in which IHC detected dMMR, whereas PCR analysis detected MSS/MSI-L. The Kappa index was 0.88 (95% CI: 0.78–0.97) (Table 3). The IHC-PCR discordance cases included three cases of isolated MSH6 loss and three cases of isolated PMS2 loss (Table S3).
 |
Table 3 Agreement in MMR Status Detection Between IHC and PCR |
Discussion
A microsatellite instability (MSI) status, resulting from mismatch repair deficiency (dMMR), plays an important role in prognosis and treatment of colorectal cancer.14 Our study investigated clinicopathological characteristics of MSI/dMMR status in Vietnamese patients with colorectal cancers, as well as concordance between the results of IHC and PCR, the two most common methods for detecting MSI/dMMR status. We found that 1) the distribution of tumor locations, vascular invasion, lymphovascular invasion, histopathological grade, and pTNM stage in the dMutL group were different compared to the pMMR group; the model predicting dMutL status that was constructed from those factors exhibited high discrimination and calibration. 2) Differences in tumor size and pTNM stage between the dMutS group and pMMR were also observed. 3) There was high agreement between IHC and PCR results when detecting the MSI/dMMR status. Our findings emphasized the association between histopathological characteristics and MSI/dMMR status, suggesting that we might predict MSI/dMMR status of the cancer based on the histopathological characteristics, thereby supporting the decision-making during the waiting time for IHC or PCR assays. While the clinicopathologic associations observed in our study are broadly consistent with prior reports from other populations, our study added the systematic characterization of dMMR subtypes and IHC-PCR concordance in a Vietnamese cohort. Given the documented geographic and ethnic heterogeneity in colorectal cancer molecular profiles, population-specific validation of these associations is necessary to inform regional clinical practice.
In our study, colorectal cancer with dMMR status was higher than the dMMR prevalence reported from some previous studies. For instance, studies on the white population showed that MSI/dMMR was exhibited in approximately 15% of colorectal cancer cases.15,16 Another study on the Chinese population showed that 8.9% of colorectal cancer patients were detected with MSI/dMMR status.17 However, a previous study on 202 patients showed that MSI/dMMR accounted for 21.3% of colorectal cancers.18 A previous big cohort study of 14,004 colorectal cancer cases showed that the prevalence of MSI/dMMR might depend on several factors, including tumor location and the onset time, with the highest dMMR prevalence observed in the ascending colon (46%).19 The MSI/dMMR status also accounted for 21% of early-onset cases in this study.19 Another study on early-onset colon cancer also showed MSI/dMMR tumors accounted for 26.2%.20 Prevalence of MSI/dMMR status among colorectal cancer might also depend on age of interest; 30.6% of cases were observed among patients with colorectal cancer younger than 30 years old.21 In sum, the MSI/dMMR prevalence might be varied among studies, which is largely due to differences in demographic and disease characteristics such as study populations, age, or onset-time, as mentioned.
Among colorectal cancers with dMMR, our study showed that colorectal cancer patients with dMutL status exhibited differences in tumor locations. Colorectal tumors with dMutL appear to occur in the right colon more commonly than in the left colon, sigmoid colon, and rectum; they were most common at grade I–II and stage I–II, and had less vascular invasion and LVI than pMMR. Our predictive regression model also showed that the odds of dMutL status in tumors located in the rectum was five-fold lower than tumors located in the right colon. Consistent with our results, a previous study showed that tumors with dMMR tend to occur on the right colon in comparison with the other location.18 Another study showed that dMutL colorectal cancer occurs more frequently in the right colon and less frequently in the rectum when compared to pMMR.22 Evidence suggests that differences in MSI/dMMR status between the right side and left side might be because of different carcinogenesis pathways, which might further impact cancer diagnosis, prognosis, and management.23
From comparison and regression analyses, we found that colorectal cancers with dMMR, especially dMutL, were associated with histopathologic grade and pTNM stage, which were more common in high-grade and early stages. A previous study with 135 patients with colorectal cancer showed that the dMMR status in colorectal cancer was associated with the higher histopathologic grade (grade 3).24 Evidence shows that MSI/dMMR prevalence in stages II, III, and IV was about 20%, 12%, and 4%, respectively, which might suggest the associations between MSI/dMMR status and early-stage colorectal cancer.25 In sum, our study emphasized the characteristics of MSI/dMMR colorectal cancer, which is poor differentiation but is usually observed in the early stages of disease.
Moreover, our study demonstrated that vascular invasion and LVI in dMMR colorectal cancer were less frequent than in pMMR colorectal cancer. A previous study also showed that dMMR colorectal cancer, especially a dMutL type, was had lower rates of LVI than pMMR colorectal cancer.24 Another study showed that the rate of vascular invasion was lower in dMMR tumors compared to pMMR tumors.26 In a study of early-onset colon cancer, vascular invasion and LVI were shown to be lower in dMMR tumors compared to pMMR tumors.20 However, a study also showed that LVI in dMutL tumors might not be different from pMMR tumors,22 which might suggest that the results might be varied among study cohorts. It should be noted that, in our dMutL predictive models, vascular invasion and LVI predictors did not reach the statistically significant threshold, which might be because the inclusions of histopathologic grade and pTNM stage variables in the model control the predictive contribution thresholds of vascular invasion and LVI, making them lower than the statistically significant threshold.
Regarding dMutS colorectal tumors, our study showed that those tumors were likely to be small and in an early stage but not associated with other clinicopathologic features. Evidence showed that dMutS and dMutL tumor profiles might be different.27 For instance, dMutS tumors commonly occur in the left colon instead of the right colon.28 To examine whether the clinicopathologic features identified in the dMutL-pMMR comparison are specific to the dMutL subtype or represent general characteristics of dMMR tumors, we directly compared dMutL and dMutS groups. We found that the only statistically significant difference was in pTNM stage, suggesting that this might represent a subtype-specific feature distinguishing dMutL from dMutS colorectal cancer. In contrast, features such as tumor location, vascular invasion, lymphovascular invasion, and histopathological grade did not differ significantly between the two subtypes, raising the possibility that these characteristics may be shared across dMMR tumors in general rather than being exclusive to the dMutL subtype. Nevertheless, these results should be interpreted with considerable caution. With only 15 patients in the dMutS group, our study was substantially underpowered for this subgroup analysis; for instance, the absolute difference in vascular invasion rates between dMutL (8.3%) and dMutS (26.7%) was clinically notable but did not reach statistical significance. Larger studies with balanced dMMR subtype representation are warranted to definitively distinguish subtype-specific from pan-dMMR clinicopathologic features.
In this study, we have constructed the predictive model for dMMR, which included predictors that are commonly available clinicopathologic characteristics. The model for dMutL prediction exhibited high discrimination and calibration, whereas the model for dMutS showed poor performance. Data limitations may be one of the contributing factors. Further studies might address this issue to improve the models for accurately and effectively predicting dMMR status, which might help enhance immediate decision-making in clinical practice.
In addition to investigating clinicopathologic characteristics of MSI/dMMR in colorectal cancer, we also examined the concordance between IHC and PCR in MSI/dMMR detection. The results suggest the strong agreement between IHC and PCR results. Because the PCR subset was enriched for dMMR cases, it should be noted that prevalence-dependent metrics such as precision and F1-score would be lower if applied to an unselected screening population. Similarly, a previous study showed that sensitivity, specificity, and precision of IHC (compared to PCR) were 87.3%, 96.1%, and 80.7%, respectively.29 Among their 28 dMMR/MSS discordant cases, 11 showed isolated PMS2 loss and 5 showed isolated MSH6 loss, consistent with the discordance pattern observed in our study.29 Several mechanisms might explain this discordance. First, isolated loss of the minor heterodimer partners (MSH6 and PMS2) might produce a milder mismatch repair defect than loss of the obligate partners (MSH2 and MLH1), because MSH2 can alternatively heterodimerize with MSH3 to form MutSβ, and MLH1 can pair with PMS1 or MLH3, which might partially compensate for the lost protein and maintain sufficient repair activity to prevent widespread microsatellite instability. This might result in low-level instability that falls below the ≥2 loci/≥40% threshold used in our ddPCR assay. In addition, MSH6-deficient tumors might show preferential instability at dinucleotide rather than mononucleotide repeats, which might reduce the sensitivity of mononucleotide-based panels for detecting MSH6-related MMR deficiency. Second, technical factors in IHC interpretation should be considered. Heterogeneous or weak staining of MSH6 and PMS2 can be particularly challenging to interpret, and fixation artifacts, suboptimal antigen retrieval, or lymphocyte-rich tumor microenvironments might complicate interpretation, potentially leading to false-positive calls of protein loss. It should be noted that all six discordant cases in our study involved these subjectively challenging isolated loss patterns, which further supports the need for dual-pathologist review in future studies. Third, missense mutations in PMS2 or MSH6 might produce structurally altered proteins that lose immunoreactivity while retaining partial repair function. Moreover, some of these cases might represent true dMMR with only MSI-low status, which would be classified as MSS under the two-locus threshold. From a clinical perspective, these discordant cases might still harbor Lynch syndrome-associated germline mutations in PMS2 or MSH6 and could benefit from genetic counseling, even though the tumor appears microsatellite stable. These findings suggest the importance of reflex germline testing when isolated PMS2 or MSH6 loss is identified by IHC, regardless of PCR results. Despite these discordant cases, the overall high concordance between the two methods suggested that IHC could be used as a practical alternative approach to detect MSI/dMMR status in patients with colorectal cancer, especially in resource-limited settings where PCR infrastructure might be unavailable.
Our study has several limitations. First, our sample size, especially the MSI/dMMR tumor number, was small. The primary focus on dMutL in the analyses and discussion was because of the larger sample size allowing more robust statistical analysis and the greater number of significant univariable associations identified for dMutL, which provided candidate predictors for the regression model. Second, we just focused on the clinicopathologic characteristics when constructing the predictive model for MSI/dMMR status but cannot estimate the predictive contributions of other factors that were not included in the study. In addition, the interpretation of IHC might be subjective because of several factors, including variations in staining patterns, observer inconsistency, specimen quality issues, and the potential for the technique to miss certain types of functional deficiencies. Third, our cross-sectional design does not allow assessment of long-term outcomes such as overall survival or treatment response, which would require prospective follow-up studies. Fourth, as a single-center study at Can Tho Oncology Hospital, the findings might not be generalizable to other Vietnamese populations or clinical settings. Fifth, IHC interpretation was performed by a single pathologist without formal inter-observer agreement assessment, which might introduce subjective interpretation bias. Future studies should incorporate blinded dual-pathologist review to quantify inter-observer variability. Moreover, due to the small number of dMutS cases, we could not perform adequately powered comparisons between dMMR subtypes, therefore could not determine whether the clinicopathologic associations observed for dMutL are truly subtype-specific or shared features of dMMR tumors in general.
In conclusion, in the Vietnamese cohort of colorectal cancer patients, dMutL was the predominant dMMR subtype and was associated with distinct clinicopathologic features, particularly right-sided tumor location, lower rates of vascular and lymphovascular invasion, and earlier pTNM stage. A clinicopathologic-based predictive model for dMutL showed that these features alone are insufficient for reliable clinical prediction. IHC and PCR showed high concordance for MSI/dMMR detection, supporting IHC as a practical alternative in resource-limited settings. However, the small number of dMutS cases limited subtype-specific comparisons, and the features associated with dMutL might partly reflect general dMMR characteristics. Larger, multicenter studies with balanced dMMR subtype representation are needed to validate these findings and assess their clinical utility in Southeast Asian populations.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by the Institute Research Board of the University of Medicine and Pharmacy in Ho Chi Minh City (approval number: 20/HĐĐĐ-ĐHYD on 20/01/2022) and complied with the Declaration of Helsinki. Informed consent was obtained from all participants before enrolling in this study.
Acknowledgment
We express our gratitude to Can Tho University of Medicine and Pharmacy, Can Tho Oncology Hospital, and the University of Medicine and Pharmacy at Ho Chi Minh City for their support in facilitating this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declared no conflict of interest.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–12. doi:10.3322/caac.21834
2. Matsuda T, Fujimoto A, Igarashi Y. Colorectal Cancer: epidemiology, Risk Factors, and Public Health Strategies. Digestion. 2025;106(2):91–99. doi:10.1159/000543921
3. Jackson AT, Megafu O, Abdullahi D, Amajoyi R. Colorectal cancer care continuum: navigating screening, treatment, and outcomes disparities. J Surg Oncol. 2024;130(7):1475–1482. doi:10.1002/jso.27848
4. Tonini V, Zanni M. Why is early detection of colon cancer still not possible in 2023? World J Gastroenterol. 2024;30(3):211–224. doi:10.3748/wjg.v30.i3.211
5. Nguyen LH, Goel A, Chung DC. Pathways of Colorectal Carcinogenesis. Gastroenterology. 2020;158(2):291–302. doi:10.1053/j.gastro.2019.08.059
6. Lo CM, Jiang JK, Lin CC. Detecting microsatellite instability in colorectal cancer using Transformer-based colonoscopy image classification and retrieval. PLoS One. 2024;19(1):e0292277. doi:10.1371/journal.pone.0292277
7. Yang XW, Han XP, Han C, London J, Fishel R, Liu J. MutS functions as a clamp loader by positioning MutL on the DNA during mismatch repair. Nat Commun. 2022;13(1):5808. doi:10.1038/s41467-022-33479-3
8. Qiu R, Sakato M, Sacho EJ, et al. MutL traps MutS at a DNA mismatch. Proc Natl Acad Sci U S A. 2015;112(35):10914–10919. doi:10.1073/pnas.1505655112
9. Wang C, Zhang L, Vakiani E, Shia J. Detecting mismatch repair deficiency in solid neoplasms: immunohistochemistry, microsatellite instability, or both? Mod Pathol. 2022;35(11):1515–1528. doi:10.1038/s41379-022-01109-4
10. Ye M, Ru G, Yuan H, Qian L, He X, Li S. Concordance between microsatellite instability and mismatch repair protein expression in colorectal cancer and their clinicopathological characteristics: a retrospective analysis of 502 cases. Front Oncol. 2023;13:1178772. doi:10.3389/fonc.2023.1178772
11. Diaz-Gay M, Dos Santos W, Moody S, et al. Geographic and age variations in mutational processes in colorectal cancer. Nature. 2025;643(8070):230–240. doi:10.1038/s41586-025-09025-8
12. Fischer AH, Jacobson KA, Rose J, Zeller R. Hematoxylin and eosin staining of tissue and cell sections. CSH Protoc. 2008;2008:prot4986.
13. Baudrin LG, Deleuze JF, How-Kit A. Molecular and Computational Methods for the Detection of Microsatellite Instability in Cancer. Front Oncol. 2018;8:621. doi:10.3389/fonc.2018.00621
14. Taieb J, Svrcek M, Cohen R, Basile D, Tougeron D, Phelip JM. Deficient mismatch repair/microsatellite unstable colorectal cancer: diagnosis, prognosis and treatment. Eur J Cancer. 2022;175:136–157. doi:10.1016/j.ejca.2022.07.020
15. Aaltonen LA, Salovaara R, Kristo P, et al. Incidence of hereditary nonpolyposis colorectal cancer and the feasibility of molecular screening for the disease. N Engl J Med. 1998;338(21):1481–1487. doi:10.1056/NEJM199805213382101
16. Hampel H, Frankel WL, Martin E, et al. Screening for the Lynch syndrome (hereditary nonpolyposis colorectal cancer). N Engl J Med. 2005;352(18):1851–1860. doi:10.1056/NEJMoa043146
17. Jiang W, Sui QQ, Li WL, et al. Low prevalence of mismatch repair deficiency in Chinese colorectal cancers: a multicenter study. Gastroenterol Rep. 2020;8(5):399–403. doi:10.1093/gastro/goaa006
18. Lopez-Correa PE, Lino-Silva LS, Gamboa-Dominguez A, Zepeda-Najar C, Salcedo-Hernandez RA. Frequency of Defective Mismatch Repair System in a Series of Consecutive Cases of Colorectal Cancer in a National Cancer Center. J Gastrointest Cancer. 2018;49(3):379–384. doi:10.1007/s12029-018-0132-1
19. Ugai T, Haruki K, Harrison TA, et al. Molecular Characteristics of Early-Onset Colorectal Cancer According to Detailed Anatomical Locations: comparison With Later-Onset Cases. Am J Gastroenterol. 2023;118(4):712–726. doi:10.14309/ajg.0000000000002171
20. Collaborative R, Adamina AAM, Aigner F. Impact of microsatellite status in early-onset colonic cancer. Br J Surg. 2022;109(7):632–636. doi:10.1093/bjs/znac108
21. Gutierrez C, Ogino S, Meyerhardt JA, Iorgulescu JB. The Prevalence and Prognosis of Microsatellite Instability-High/Mismatch Repair-Deficient Colorectal Adenocarcinomas in the United States. JCO Precis Oncol. 2023;7(7):e2200179. doi:10.1200/PO.22.00179
22. Zeng Z, Yan Q, Chen G, et al. Characteristics of colorectal carcinoma patients with PMS2 defects detected by immunohistochemistry. Eur J Cancer Prev. 2021;30(3):251–257. doi:10.1097/CEJ.0000000000000620
23. Baran B, Mert Ozupek N, Yerli Tetik N, Acar E, Bekcioglu O, Baskin Y. Difference Between Left-Sided and Right-Sided Colorectal Cancer: a Focused Review of Literature. Gastroenterol Res. 2018;11(4):264–273. doi:10.14740/gr1062w
24. Hashmi AA, Bukhari U, Rizwan R, et al. Mismatch Repair Deficient (dMMR) Colorectal Carcinoma in a Pakistani Cohort: association With Clinical and Pathological Parameters. Cureus. 2023;15(8):e42781. doi:10.7759/cureus.42781
25. Mulet-Margalef N, Linares J, Badia-Ramentol J, et al. Challenges and Therapeutic Opportunities in the dMMR/MSI-H Colorectal Cancer Landscape. Cancers (Basel). 2023;15(4):1022. doi:10.3390/cancers15041022
26. Ozer L, Senocak Tasci E, Mutlu AU, et al. Intramural Component of Venous, Lymphatic, and Perineural Invasion in Colon Cancer: a Threat or an Illusion? Balkan Med J. 2022;39(6):436–443. doi:10.4274/balkanmedj.galenos.2022.2022-6-94
27. Mao J, He Y, Chu J, et al. Analysis of clinical characteristics of mismatch repair status in colorectal cancer: a multicenter retrospective study. Int J Colorectal Dis. 2024;39(1):100. doi:10.1007/s00384-024-04674-z
28. Li J, Xu Q, Luo C, Chen L, Ying J. Clinicopathologic characteristics of resectable colorectal cancer with mismatch repair protein defects in Chinese population: retrospective case series and literature review. Medicine (Baltimore). 2020;99(24):e20554. doi:10.1097/MD.0000000000020554
29. Chen J, Yan Q, Sun J, et al. Microsatellite Status Detection of Colorectal Cancer: evaluation of Inconsistency between PCR and IHC. J Cancer. 2023;14(7):1132–1140. doi:10.7150/jca.81675
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Mechanisms and Emerging Strategies to Overcome Immunotherapy Resistance in Cold Tumours of Colorectal Cancer
Zhu X, Ge B, Wen L
OncoTargets and Therapy 2026, 19:621109
Published Date: 15 June 2026