Back to Journals » Patient Preference and Adherence » Volume 19
Cultural Adaptation and Preliminary Validation of Adherence Questionnaires for Japanese Patients with Breast Cancer: A Pilot Study
Authors Matsuda A, Tozuka K ![]() , Momiyama M, Inoue K, Kobayashi K, Kroep JR
, Momiyama M, Inoue K, Kobayashi K, Kroep JR ![]() , Kaptein AA
, Kaptein AA ![]() , Yamaoka K
, Yamaoka K
Received 11 July 2025
Accepted for publication 27 October 2025
Published 4 November 2025 Volume 2025:19 Pages 3399—3408
DOI https://doi.org/10.2147/PPA.S553154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Ayako Matsuda,1 Katsunori Tozuka,2 Manami Momiyama,2 Kenichi Inoue,2 Kunihiko Kobayashi,3 Judith R Kroep,4 Ad A Kaptein,5 Kazue Yamaoka6
1Center for Health Informatics Policy, National Institute of Public Health, Saitama, Japan; 2Division of Breast Oncology, Saitama Cancer Center, Saitama, Japan; 3Department of Respiratory Medicine, Kumagaya General Hospital, Saitama, Japan; 4Department of Medical Oncology, Leiden University Medical Center, Leiden, the Netherlands; 5Department of Medical Psychology, Leiden University Medical Center, Leiden, the Netherlands; 6Tetsuyu Clinical Research Center, Tetsuyu Institute Medical Corporation, Tokyo, Japan
Correspondence: Ayako Matsuda, National Institute of Public Health, Center for Health Informatics policy, 2-3-6 Minami, Wako-shi, Saitama, 351-0197, Japan, Tel +81-48-458-6206, Email [email protected]
Purpose: This pilot study conducted a cultural adaptation and preliminary validation of the Beliefs about Medicines Questionnaire (BMQ) and the Medication Adherence Rating Scale (MARS) for Japanese patients with breast cancer.
Patients and Methods: The grammatical accuracy of the Japanese translations of the BMQ and MARS, which are originally in English, was assessed by 10 physicians. A pilot survey was conducted with 50 patients with breast cancer in Japan who were starting adjuvant endocrine therapy. Internal consistency was examined using item-total and item-rest correlations and Cronbach’s alpha. Items with low correlations were flagged for revision or removal. Oncology experts further reviewed problematic items for clinical relevance and cultural appropriateness.
Results: Several items showed low relevance, particularly those that were inconsistent with the Japanese healthcare context. In the BMQ, Q6 (“This medicine is a mystery to me”) and Q14 (“Natural remedies are safer than medicines”) had low item-rest correlations (r = 0.079 and 0.075, respectively). In the MARS, four items (Q3–Q5 and Q9) were redundant.
Conclusion: This pilot study demonstrated the significance of culturally adapting the BMQ and MARS. Revising or removing culturally incongruent items improved their relevance and reliability for Japanese patients with breast cancer.
Keywords: adherence, adjuvant endocrine therapy, BMQ, MARS, breast cancer, patient perceptions, validity
Introduction
Breast cancer is the most common cancer among Japanese women.1 Among those prescribed postoperative endocrine therapy, many decide to discontinue taking medication because of side effects and doubts about the efficacy of the treatment.2 With the shift toward patient-centered care, patients are increasingly involved in making informed decisions about their treatment plans. In this context, the perceived efficacy and side effects of medications as well as patients’ illness awareness and psychosocial factors have been shown to influence adherence—that is, patients’ agreement with and engagement in their treatment plans.3–5 However, few investigations have validated such adherence measures in Japan. Therefore, this study was designed as a pilot investigation to validate these measures.
Given the effectiveness of endocrine therapy in protecting against mortality, maintaining adherence is critical. Previous studies have emphasized how patient compliance in cancer treatment directly affects treatment outcomes (recurrence and mortality rates).6–8 Zhao et al9 emphasized that illness perception not only directly affected medication adherence but also indirectly affected medication adherence through beliefs about medicines in patients with breast cancer. These beliefs shape how patients perceive and manage side effects, especially as they return to work and attempt to resume their pre-diagnosis lifestyles. Understanding the rationale for medication, anticipating potential side effects, and preserving an acceptable quality of life can all facilitate adherence. Health care providers play a pivotal role in supporting patients by exploring patients’ cognitive and emotional responses to treatment and by helping them improve their adherence behaviors.
Despite the importance of adherence in optimizing treatment outcomes, few validated tools are available in Japan to measure patients’ beliefs and behaviors regarding medication. The Beliefs about Medicines Questionnaire (BMQ) and the Medication Adherence Rating Scale (MARS) are widely used instruments that assess beliefs and adherence across various populations and disease contexts.10,11 Iihara et al12 described their study as the first to apply factorial invariance analysis to adherence research among Japanese respondents but acknowledged that further studies are needed to confirm item validity and enhance measurement accuracy.
This effort is part of a broader initiative to develop a culturally appropriate, psychometrically sound adherence assessment tool for use in Japanese clinical settings. This tool is being developed in the context of existing cross-cultural work investigating the quality of life and disease awareness among patients with breast cancer across cultures.5 Against this background, we conducted a pilot study to culturally adapt and preliminarily validate the BMQ and MARS for Japanese patients with breast cancer.
Materials and Methods
Development of Adherence Questionnaires
The original English versions of the BMQ and MARS were translated into Japanese using a forward–backward translation process, consistent with established guidelines for cross-cultural adaptation of patient-reported outcome measures.13 First, two bilingual Japanese researchers independently translated the questionnaires from English to Japanese. Next, a native English speaker fluent in Japanese back-translated the combined Japanese version into English. The back-translation was compared with the original by a team of Japanese- and English-speaking experts, and discrepancies were discussed and reconciled. This forward–backward translation sequence was performed twice to ensure linguistic accuracy and conceptual equivalence, in line with ISPOR Task Force principles.13 Subsequently, to investigate content validity, a pilot survey was conducted among 50 patients with breast cancer who had been prescribed adjuvant endocrine therapy. Their feedback was incorporated to refine wording and ensure content validity before administering the patient survey.
Study Design and Participants
We conducted a single-center pilot study at the Saitama Cancer Center in Japan. The study enrolled 50 women with stage I–III breast cancer who were scheduled to initiate adjuvant endocrine therapy (ET). Because HER2-positive breast cancer requires trastuzumab-based chemotherapy in addition to ET, patients with HER2-positive breast cancer were not enrolled. Consequently, all participants in this pilot cohort were HER2-negative. Inclusion criteria required participants to be female patients aged ≥20 years, with Performance Status (ECOG) 0–1, histologically confirmed stage I, II, or III hormone receptor-positive breast cancer, and an adjuvant ET regimen planned. Exclusion criteria included the presence of metastatic disease, any other active cancer within the past 3 years, prior exposure to ET or chemotherapy, or any medical/psychological condition that could interfere with study participation or informed consent as judged by the investigators. All participants provided written informed consent before enrollment.
Participants completed the Japanese BMQ at baseline (before starting ET) and the MARS at 3, 6, and 12 months after the initiation of ET. For the purposes of this preliminary validation analysis, we used the BMQ data collected at baseline and the MARS data collected at 12 months. This approach allowed us to assess BMQ at baseline and MARS after 1 year of therapy.
Assessment Instruments (BMQ and MARS)
Previous studies have reported a Cronbach’s α of approximately 0.60–0.80 for BMQ subscales14,15 and 0.75 for the MARS,16 providing a benchmark for interpreting our results. Although ET is usually prescribed for 5 years, we limited the follow-up period to 12 months in this pilot validation, as adverse effects leading to discontinuation typically appear within the first year.
Beliefs About Medicines Questionnaire (BMQ)
The BMQ is a validated instrument that assesses patients’ beliefs about medications, specifically their perceived necessity for the prescribed medication and concerns about potential adverse effects. The questionnaire consists of 18 items divided into two sections: BMQ-Specific (10 items) and BMQ-General (8 items). The BMQ-Specific section includes a 5-item Necessity subscale (evaluating the patient’s belief in the necessity of their medication) and a 5-item Concerns subscale (evaluating worries about the medication’s adverse effects). The BMQ-General section includes a 4-item General Harm subscale (assessing beliefs about the harmful nature of medicines in general) and a 4-item General Overuse subscale (assessing the belief that medicines are overprescribed by doctors). The development and initial validation of the BMQ were originally reported by Horne et al,14 demonstrating the reliability and validity of the instrument. The BMQ is scored by summing the item scores within each subscale and computing the mean (total score divided by the number of items), with higher scores indicating stronger beliefs in the respective domain file. In this study, we used the Japanese-translated BMQ as adapted above, where higher Necessity scores indicated a stronger perceived need for medication, and higher Concerns scores indicated greater worry about medications.15
Medication Adherence Rating Scale (MARS)
MARS is a self-reported measure of medication-taking behavior and adherence. It contains 10 dichotomous (yes/no) items that address common behaviors related to medication adherence. Each item is phrased as a statement (eg, “I forget to take my medicine”, “I stop taking my medication when I feel better”), to which patients respond “Yes” or “No”. According to the standard scoring criteria, a “No” answer to items 1–6 and 9–10 (or a “Yes” to items 7–8) is considered indicative of a compliant (adherent) behavior file. We calculated each patient’s overall adherence score by counting the number of adherence-indicative responses (range: 0–10), with higher scores denoting better self-reported adherence. The original MARS was developed for use in chronic illness populations, and its validity and internal consistency have been documented in previous studies.16 For this study, we employed the Japanese-translated MARS to assess medication adherence over the 12-month follow-up period.
Sociodemographic and Clinical Variables
Baseline sociodemographic and clinical data were obtained from each patient’s medical records file. Collected variables included age at study entry, breast cancer subtype and stage (I–III), tumor type (eg, invasive ductal carcinoma), hormone receptor status (all participants were estrogen and/or progesterone receptor-positive by inclusion criteria), HER2 receptor status (positive or negative), and details of prior treatments. We recorded whether the patient had received chemotherapy (and if so, whether in the neoadjuvant or adjuvant setting) and prior radiotherapy. In addition, we recorded each patient’s employment status (employed vs not employed) and partner status (having a spouse or partner vs not). These sociodemographic and clinical characteristics were later summarized to describe the study sample.
Statistical Analysis
Descriptive statistics were used to summarize the sample characteristics and item responses. Internal consistency reliability of the BMQ and MARS subscales was evaluated using item-total correlations, item-rest correlations, and Cronbach’s alpha coefficients. Following standard criteria, a Cronbach’s α value of ≥0.70 was considered acceptable for internal consistency, and item-total or item-rest correlation coefficients ≥0.30 were deemed acceptable for individual items.17 We also examined “Cronbach’s α if item deleted” for each item to determine whether removing any item would substantially improve the scale’s reliability.
Content validity was emphasized as a critical property for these adherence questionnaires, consistent with COSMIN guidelines that identify content validity as one of the most important measurement properties for patient-reported outcomes.18 To assess content validity, we analyzed the expert panel’s ratings of each item’s relevance, clarity, and cultural suitability. Ten oncology experts reviewed each item for relevance and clarity. Following the COSMIN guidelines, we considered an item-level CVI ≥ 0.78 as acceptable The proportion of experts who endorsed each item as appropriate was examined. Any item that received mixed feedback or was deemed problematic by the medical doctors was flagged for potential revision. Items identified as problematic were further reviewed in depth by the research team including oncology specialists to determine whether modifications or exclusions were warranted, focusing on clinical relevance, cultural appropriateness, and practical utility. This content validation process was conducted through iterative feedback from the experts, obtained via meetings, Email correspondence, and online communications.19,20
All statistical tests were two-tailed, with a significance level set at p < 0.05. All analyses were performed using Stata version 19.0 (Stata Corp, College Station, TX, USA).
Results
Participants
Descriptive findings and reliability results are presented below. Descriptive statistics for sociodemographic and clinical variables were calculated (Table 1). All 50 participants completed the study questionnaires with no missing data. The mean age of the participants was 60.5 years (range, 43–76; standard deviation, 10.6). Most patients were diagnosed with stage I or II breast cancer (98.0%) and had invasive ductal carcinoma (87.8%) that was HER2-negative (100%). Approximately 60% of the sample had received radiotherapy. At the time of the survey, about 43% of patients were employed, and 86% reported having a partner.
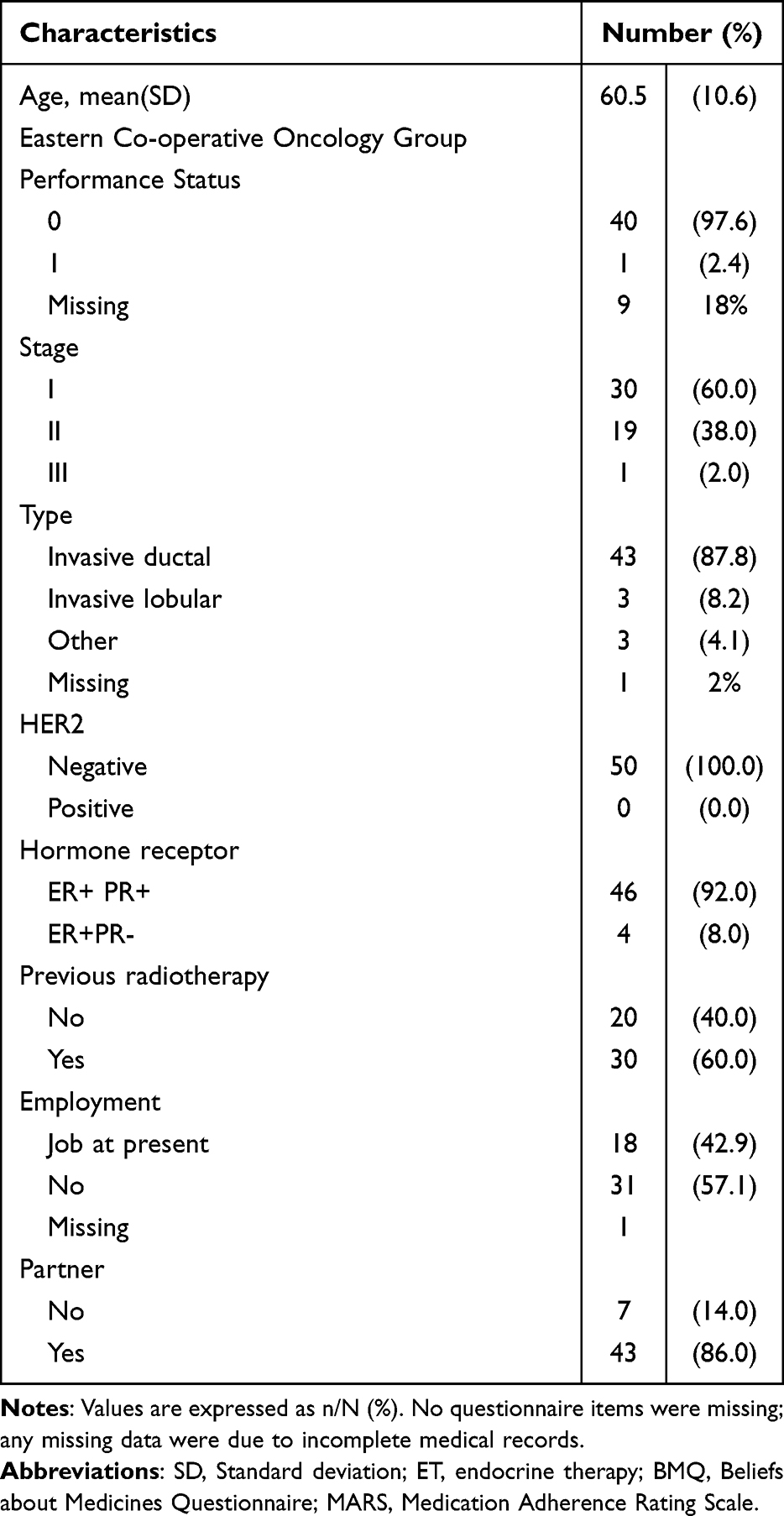 |
Table 1 Sample Characteristics at Baseline (n=50) |
Internal Consistency Reliability
BMQ
Table 2 presents the internal consistency reliability and mean item scores for each BMQ subscale. The BMQ-Specific Necessity subscale showed good reliability (Cronbach’s α = 0.768). However, item Q10 had a low item-rest correlation (r = 0.332), and its removal would improve the internal consistency of the scale. Items Q1, Q3, Q4, and Q7 were retained as core components. The BMQ-Specific Concerns subscale showed weak reliability (α = 0.494). Item Q6 (“This medicine is a mystery to me”) had a very low correlation (r = 0.079) and was recommended for removal. Q8 (“This medicine disrupts my life”) had low correlation (r = 0.120) and was recommended for substantial revision. Q2, Q5, and Q9 showed somewhat low correlations but were retained due to conceptual importance.
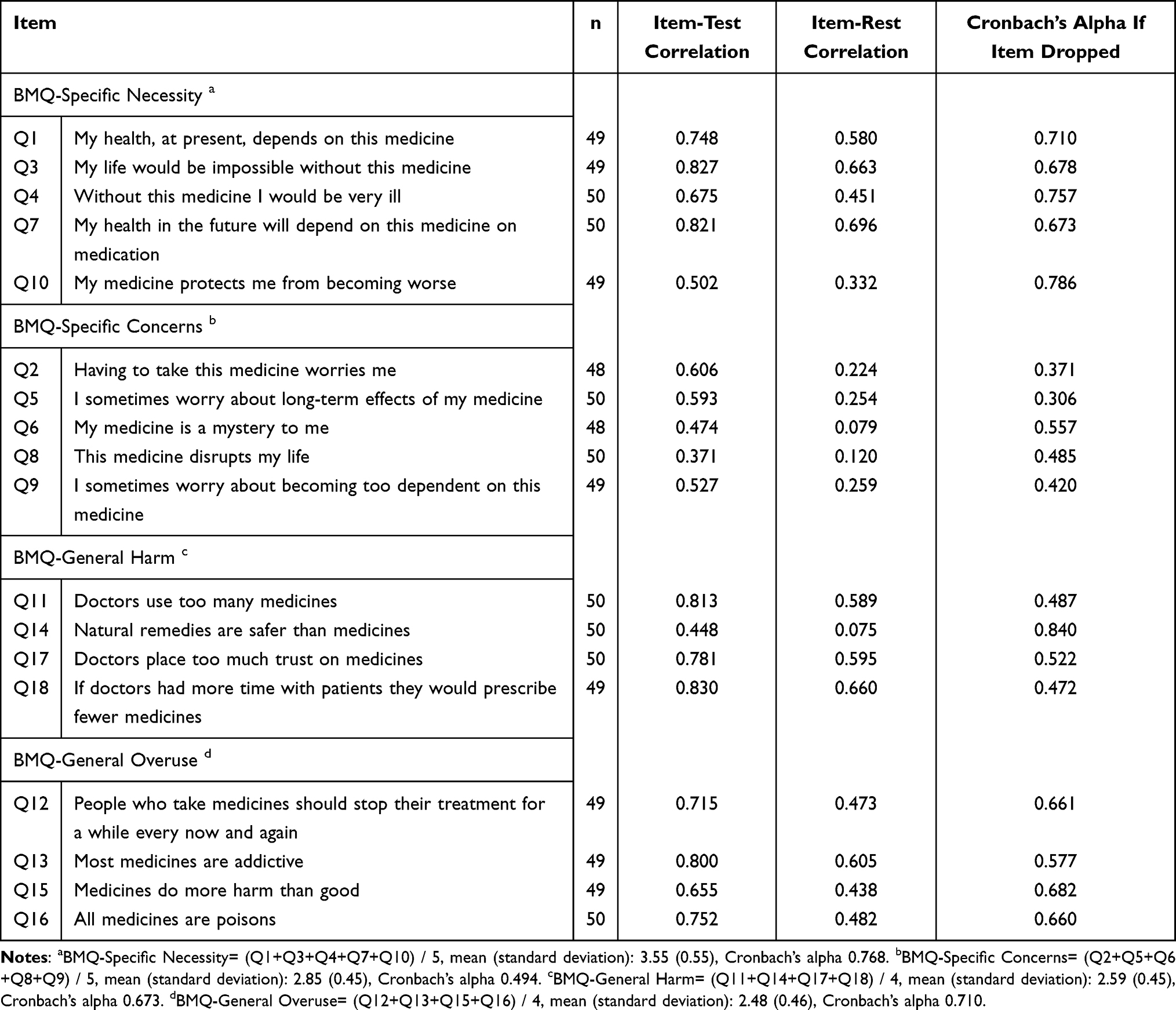 |
Table 2 Internal Consistency Reliability of the BMQ |
The BMQ-General Harm subscale had moderate reliability (α = 0.673). Item Q14 (“Natural remedies are safer than medicines”) showed poor item-total correlation (r = 0.075) and was recommended for removal. Q11, Q17, and Q18 showed acceptable reliability. The BMQ-General Overuse subscale showed satisfactory reliability (α = 0.710), and all items (Q12, Q13, Q15, and Q16) were retained.
MARS
As shown in Table 3, the MARS demonstrated satisfactory internal consistency (Cronbach’s α = 0.738). Items Q2, Q6, and Q10 were considered appropriate for retention. In contrast, items Q1 (r = 0.195), Q7 (r = 0.199), and Q8 (r = 0.274) showed weak associations and were flagged for potential revision. Four items—Q3, Q4, Q5, and Q9—had identical and high inter-item correlations (r = 0.768), suggesting redundancy. These may be considered for consolidation into a single item in future versions.
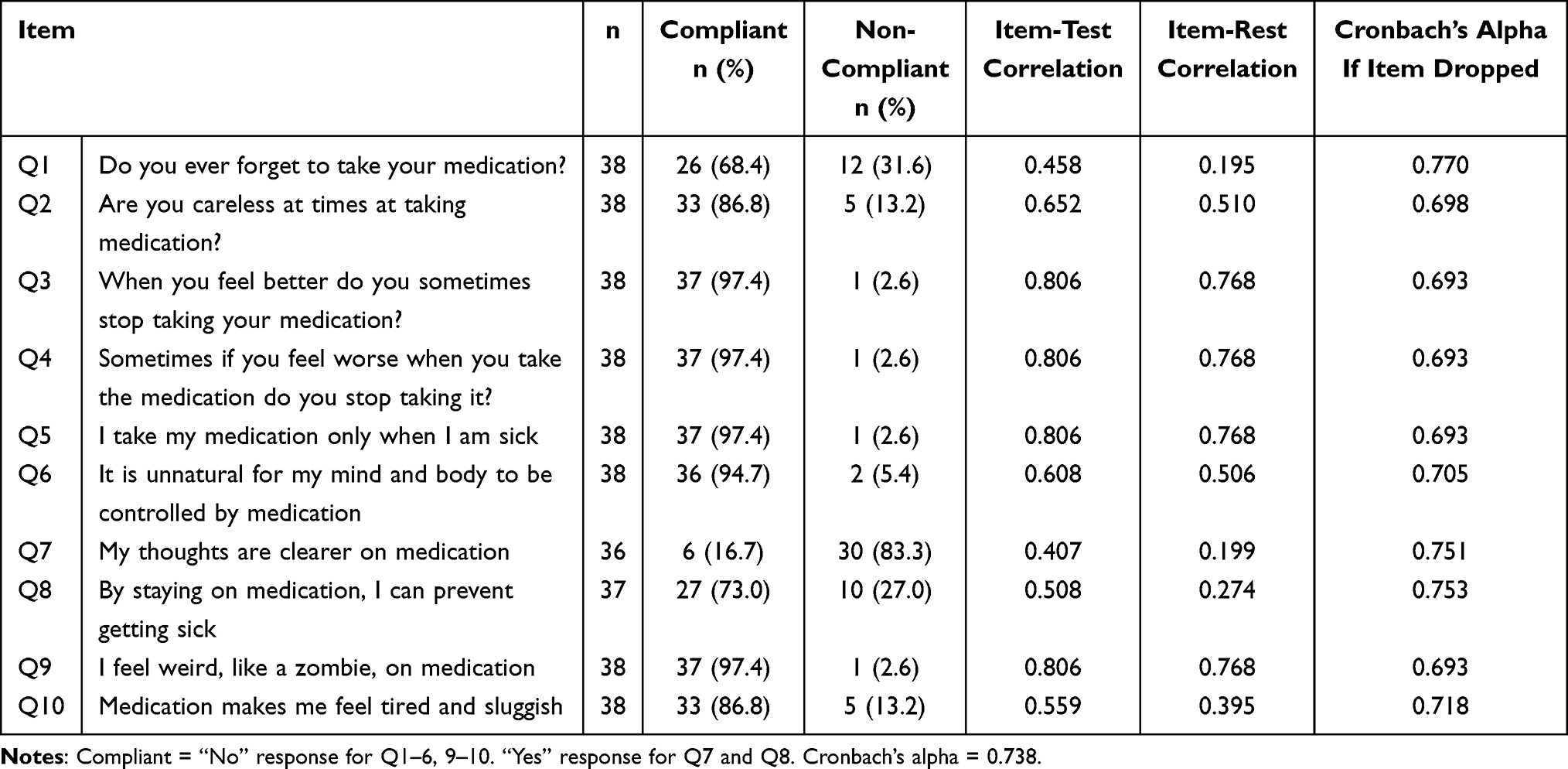 |
Table 3 Internal Consistency Reliability of the MARS |
Content Validation
BMQ
The findings of the expert review were summarized and four items—Q10, Q6, Q8, and Q14—were eliminated following expert consensus due to low relevance, ambiguous interpretation, and cultural inappropriateness. For example, item Q6 (“This medicine is a mystery to me”) differed from the others, and the translation “mystery” was not suitable for Japanese patients. Q14 (“Natural remedies are safer than medicines”) was considered contextually irrelevant because the sample did not include patients using alternative medicine.
MARS
Expert evaluation and redundancy analysis also identified Q3, Q4, Q5, and Q9 as overlapping in content. These four items are candidates for reduction or rephrasing. Their consolidation into a single representative item should be considered in future revisions to improve scale efficiency and discriminative capacity.
Discussion
In the present study, the content validity of the Japanese version of BMQ and MARS was evaluated to develop an adherence assessment tool specifically for Japanese patients with breast cancer.
Cultural Inappropriateness of Items in BMQ
The findings regarding the Japanese version of BMQ items suggest that item Q6 (“My medicine is a mystery to me”) and item Q14 (“Natural remedies are safer than medicines”) should be deleted or substantially revised for Japanese patients with breast cancer. Although the BMQ has been validated across various populations and disease profiles, differences may arise from sociocultural practices and disease-specific beliefs, which in turn influence medication adherence.21
Item Q6 (“My medicine is a mystery to me”) was identified as culturally incongruent by both experts and patients, as the concept of a “mystery” may not resonate as intended. This semantic mismatch may explain the observed low item-rest correlation (r = 0.079), indicating poor alignment with other items. Consistent with the findings of the BMQ-AET validation conducted by a UK study with women receiving adjuvant ET, our results confirm that the “mystery” item showed very low factor loading and thus may not function well in this clinical context.22
For item Q14 (“Natural remedies are safer than medicines”), nondisclosure or patients’ perceived irrelevance of complementary and alternative medicine (CAM) use may have contributed to the poor performance of the item in the Japanese sample. In our study, participants were not systematically asked about CAM use; therefore, underreporting cannot be excluded although such therapies were not reported in our cohort. Similarly, a validation study in Singapore found that item Q14 did not align with the original factor structure and tended to load differently, indicating cultural and contextual effects on its interpretation.23
These converging findings indicate that the problems observed in our Japanese sample are not unique but rather reflect broader cross-cultural issues. In future work, Q6 might be rephrased more neutrally (eg, “I do not fully understand this medicine”), while Q14 could be modified to include specific examples of natural remedies, such as herbal medicine or supplements, thereby reducing ambiguity and improving semantic clarity.
Furthermore, previous studies have shown that Asian patients report poorer overall communication than White patients in the United States,24,25 and relatively low levels of patient-centered communication have been observed in Japan.26 These broader communication patterns may further explain the challenges of adapting items such as Q6 and Q14 to the Japanese clinical context.
These findings are consistent with those of previous international validations,22,23 reinforcing the importance of cross-cultural adaptation when adherence measures are applied in oncology.
Applicability of MARS to Breast Cancer Patients
According to our results for MARS items, the internal consistency of MARS was moderate (α = 0.74), which was similar to the value obtained by Thompson et al (α = 0.75)16 when the scale was first developed. However, Q3, Q4, Q5, and Q9 lacked differentiation and were considered candidate items for factor analysis. Fialko et al27 described that a principal components factor analysis produced a three-factor solution (Factor 1 [Q1-Q4], Factor 2 [Q5-Q8], and Factor 3 [Q9-10]), and further demonstrations are recommended to validate the MARS. Although the MARS scale was developed in a psychiatric population,28 it also has the advantage of recognizing the complexity of adherence behavior.27 This 5-item measure in MARS-5, which is a shorter form of the MARS, asks patients to score adherence behaviors, such as “I alter the dose of my hormonal therapy”.29 Walsh et al demonstrated that concurrent factors were associated with adherence to adjuvant ET among women with non-metastatic breast cancer using the MARS-5 instrument.30 They described that they created an error-free measurement model, including four of the five measure questions, to address this because the reliability of MARS-5 was poor.24 MARS was originally developed to assess adherence in psychiatric populations, particularly among patients with psychotic disorders.16 Although its application has since broadened to include various chronic conditions such as diabetes and cancer, its item content may not fully align with the behavioral and motivational dynamics of oncology populations. In this study, four items (Q3, Q4, Q5, and Q9) demonstrated near-identical response patterns and high inter-item correlations, suggesting redundancy. These items, which focus on general discontinuation behaviors (eg, stopping medication when feeling better or worse), may be less discriminative in patients with breast cancer undergoing structured, long-term ET. Therefore, in this context, adapting or consolidating these items could improve the scale’s relevance and measurement efficiency.
Limitations
This study has some limitations. First, the small sample size (n = 50) limited the ability to perform factor analyses, which are essential/instrumental for evaluating construct validity. Although exploratory factor analysis was considered, the sample was insufficient for meaningful results. Future studies should include larger samples to allow for robust confirmatory factor analysis.
Second, the expert panel consisted of 10 oncology professionals, which may not adequately capture the diversity of perspectives across disciplines such as nursing, psychology, pharmacology or patients.
Third, although the MARS has been applied in various chronic illness populations, its original development for psychiatric patients may limit its sensitivity to oncology-specific adherence behaviors. A modified or cancer-specific version of MARS should be considered to improve relevance and discriminative capacity.
These limitations underscore the need for larger, multicenter validation studies to confirm the psychometric properties and enhance the generalizability of the Japanese versions of the BMQ and MARS. Future studies should also include other healthcare professionals, such as nurses and psychologists, in the expert panel to enhance and clarify content validity.
Conclusion
This pilot study provides preliminary evidence for the content validity and internal consistency of the Japanese versions of the BMQ and MARS in evaluating women with breast cancer undergoing ET. Culturally incongruent or redundant items should be revised or consolidated to improve conceptual clarity and clinical relevance. Further validation, including construct- and criterion-related validity, in larger, multicenter samples is needed to confirm the psychometric properties and facilitate robust factor analyses. Ultimately, the development of a psychometrically robust and culturally appropriate adherence assessment tool will help develop more effective, individualized, and patient-centered care for breast cancer survivors in Japan.
Ethics Approval
All procedures were followed in accordance with the Helsinki Declaration of the World Medical Association, and the protocol was approved by the Institutional Review Board of Saitama Cancer Center (No.1455) and National Institute of Public Health in Japan (NIPH-IBRA#12413).
Acknowledgments
We thank the participants in this trial.
Author Contributions
All authors contributed significantly to the work, including conception, study design, execution, data acquisition, analysis and interpretation, and drafting, revising, or critically reviewing the article. All authors approved the final version to be submitted for publication, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Ministry of Education, Culture, Sports, Science and Technology, Japan, through a Grant-in-Aid for Scientific Research (Grant C) in 2020 (Grant no. 20K07835).
Disclosure
Dr Kunihiko Kobayashi reports speaker fees from Astral Zeneca, Janssen Pharmaceutical K.K., consulting fees from Daiichi Sankyo/UCB Japan, and research grants from Zeria Pharmaceutical Co., outside the submitted work. In addition, Dr Kunihiko Kobayashi has a patent issued (Japanese patent # 7422498). The authors declare that they have no other competing interests in this work.
References
1. Ganjoho. Cancer statistics in Japan 2025. Available from: https://ganjoho.jp/public/qa_links/report/statistics/2025_en.html.
2. Kaptein AA, Schoones JW, van der Meer PB, et al. Psychosocial determinants of adherence with oral anticancer treatment: ‘we don’t need no education’. Acta Oncol. 2021;60(1):87–95. doi:10.1080/0284186X.2020.1843190
3. Moon Z, Moss-Morris R, Hunter MS, Hughes LD. Understanding tamoxifen adherence in women with breast cancer: a qualitative study. Br J Health Psychol. 2017;22(4):978–997. doi:10.1111/bjhp.12266
4. Yeo HY, Wong JHY, Chan SJ, et al. Exploring the important determinants shaping treatment preferences: qualitative insights into breast cancer patient experiences and perspectives in New Zealand. Patient Prefer Adherence. 2023;17:3525–3537. doi:10.2147/PPA.S443217
5. Kaptein AA, Yamaoka K, Snoei L, et al. Illness perceptions and quality of life in Japanese and Dutch women with breast cancer. J Psychosoc Oncol. 2013;31(1):83–102. doi:10.1080/07347332.2012.741092
6. Chen Y, Ng MSN, Wei X, et al. Medication perceptions mediate the association between illness perceptions and adherence to oral anticancer agents among patients with gastrointestinal tract cancer: a cross-sectional study. Eur J Oncol Nurs. 2025;76:102720. doi:10.1016/j.ejon.2024.102720
7. Cazzaniga ME, Huober J, Tamma A, Emde A, Thoele K, O’Shaughnessy J. Oral anticancer therapies: addressing nonadherence in patients with breast cancer. Clin Breast Cancer. 2025;25(4):307–324. doi:10.1016/j.clbc.2024.12.011
8. Shi L, Zhang J, Deng Y. Associations of pretreatment emotional distress with adherence to therapy for patients with locally advanced rectal cancer: a post hoc analysis of the Chinese FOWARC Phase 3 randomized clinical trial. BMC Med. 2025;23(1):293. doi:10.1186/s12916-025-04128-5
9. Zhao M, Zhao J, Chen J, et al. The relationship between medication adherence and illness perception in breast cancer patients with adjuvant endocrine therapy: beliefs about medicines as mediators. Support Care Cancer. 2022;30(12):10009–10017. doi:10.1007/s00520-022-07411-w
10. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
11. Foot H, La Caze A, Gujral G, Cottrell N. The necessity-concerns framework predicts adherence to medication in multiple illness conditions: a meta-analysis. Patient Educ Couns. 2016;99(5):706–717. doi:10.1016/j.pec.2015.11.004
12. Iihara N, Suzuki K, Kurosaki Y, Morita S, Hori K. Factorial invariance of a questionnaire assessing medication beliefs in Japanese non-adherent groups. Pharm World Sci. 2010;32(4):432–439. doi:10.1007/s11096-010-9388-7
13. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. doi:10.1111/j.1524-4733.2005.04054.x
14. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
15. Cinar M, Cinar FI, Acikel C, et al. Reliability and validity of the Turkish translation of the beliefs about medicines questionnaire (BMQ-T) in patients with Behcet’s disease. Clin Exp Rheumatol. 2016;34(6 Suppl 102):S46–S51.
16. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new medication adherence rating scale (MARS) for the psychoses. Schizophr Res. 2000;42(3):241–247. doi:10.1016/S0920-9964(99)00130-9
17. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297–334. doi:10.1007/BF02310555
18. Terwee CB, Prinsen CAC, Chiarotto A, et al. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual Life Res. 2018;27(5):1159–1170. doi:10.1007/s11136-018-1829-0
19. Fredericksen RJ, Yang FM, Gibbons LE, et al. Development and content validation of measures assessing adherence barriers and behaviors for use in clinical care. Res Social Adm Pharm. 2019;15(9):1168–1176. doi:10.1016/j.sapharm.2018.10.001
20. Yusoff MSB. ABC of content validation and content validity index calculation. Educ Med J. 2019;11(2):49–54. doi:10.21315/eimj2019.11.2.6
21. Gatt I, West LM, Calleja N, Briffa C, Cordina M. Psychometric properties of the Belief about medicines questionnaire (BMQ) in the Maltese language. Pharm Pract. 2017;15(1):886. doi:10.18549/PharmPract.2017.01.886
22. Brett J, Hulbert-Williams NJ, Fenlon D, et al. Psychometric properties of the beliefs about medicines questionnaire-adjuvant endocrine therapy (BMQ-AET) for women taking AETs following early-stage breast cancer. Health Psychol Open. 2017;4(2):2055102917740469. doi:10.1177/2055102917740469
23. Tan EH, Wong ALA, Tan CC, et al. Beliefs about medicines and adherence in women with breast cancer on adjuvant endocrine therapy. J Health Psychol. 2022;27(5):1111–1124. doi:10.1177/1359105321990776
24. Cho G, Chang VW. Patient-provider communication quality, 2002-2016: a population-based study of trends and racial differences. Med Care. 2022;60(5):324–331. doi:10.1097/MLR.0000000000001694
25. Palmer NRA, Kent EE, Forsythe LP, et al. Racial and ethnic disparities in patient-provider communication, quality-of care ratings and patient activation among long-term cancer survivors. J Clin Oncol. 2014;32(36):4087–4094. doi:10.1200/JCO.2014.55.5060
26. Okamura M, Fujimori M, Otsuki A, et al. Patients’ perceptions of patient-centered communication with healthcare providers and associated factors in Japan - the INFORM Study 2020. Patient Educ Couns. 2024;122:108170. doi:10.1016/j.pec.2024.108170
27. Fialko L, Garety PA, Kuipers E, et al. A large-scale validation study of the medication adherence rating scale (MARS). Schizophr Res. 2008;100(1–3):53–59. doi:10.1016/j.schres.2007.10.029
28. Urquhart J. The electronic medication event monitor. Clin Pharmacokinet. 1997;32(5):345–356. doi:10.2165/00003088-199732050-00001
29. Chan AHY, Horne R, Hankins M, Chisari C. The medication adherence report scale: a measurement tool for eliciting patients’ reports of nonadherence. Br J Clin Pharmacol. 2020;86(7):1281–1288. doi:10.1111/bcp.14193
30. Walsh EA, Walsh LE, Hernand M, et al. Concurrent factors associated with adherence to adjuvant endocrine therapy among women with non-metastatic breast cancer. J Cancer Surviv. 2024;19(4):1335–1345. doi:10.1007/s11764-024-01556-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Development of Schematics to Illustrate Women’s Experiences with Adjuvant Hormone Therapy in the Treatment of Breast Cancer
AlOmeir O, Patel N, Donyai P
Patient Preference and Adherence 2022, 16:2639-2647
Published Date: 23 September 2022
Palbociclib Adherence and Persistence in Patients with Hormone Receptor Positive/Human Epidermal Growth Factor Receptor 2 Negative (HR+/HER2-) Metastatic Breast Cancer
Engel-Nitz NM, Johnson MG, Johnson MP, Cha-Silva AS, Kurosky SK, Liu X
Patient Preference and Adherence 2023, 17:1049-1062
Published Date: 18 April 2023
Psychometric Properties and Factorial Analysis of the Arabic McGill-QoL Questionnaire in Breast Cancer
Omar MTA, Alnahdi AH
Breast Cancer: Targets and Therapy 2023, 15:813-824
Published Date: 14 November 2023
Reliability and Validity of the Amharic Version of the Hill-Bone Adherence to High Blood Pressure Therapy Scale Among Ethiopian Hypertensive Patients
Yirba TY, Gebremariam GT, Tadesse TA, Degu A, Mekonnen D, Alemkere G
Patient Preference and Adherence 2023, 17:3207-3217
Published Date: 8 December 2023
Predictive Models of Psychological Distress, Quality of Life, and Adherence to Medication in Breast Cancer Patients: A Scoping Review
Pezzolato M, Spada GE, Fragale E, Cutica I, Masiero M, Marzorati C, Pravettoni G
Patient Preference and Adherence 2023, 17:3461-3473
Published Date: 19 December 2023