Back to Journals » International Journal of General Medicine » Volume 18
Correlation Between Serum Creatinine-to-Cystatin C Ratio and Prognosis of Patients with Hip Fracture
Authors Lu W ![]() , Rao M, Jia F, Chen W, Li B, Bian J, Wang J
, Rao M, Jia F, Chen W, Li B, Bian J, Wang J
Received 1 April 2025
Accepted for publication 19 July 2025
Published 30 July 2025 Volume 2025:18 Pages 4147—4156
DOI https://doi.org/10.2147/IJGM.S531669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Wenbin Lu,* Miaomiao Rao,* Fan Jia,* Wubin Chen, Bin Li, Jinjun Bian, Jiafeng Wang
Faculty of Anesthesiology, Changhai Hospital, Naval Military Medical University, Shanghai, 200433, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinjun Bian; Faculty of Anesthesiology, Changhai Hospital, Naval Military Medical University, 168, Changhai Road, Shanghai, 200433, People’s Republic of China, Tel/Fax +86-021-31161841, Email [email protected] Jiafeng Wang, Faculty of Anesthesiology, Changhai Hospital, Naval Military Medical University, 168, Changhai Road, Shanghai, 200433, People’s Republic of China, Tel/Fax +86-021-31161886, Email [email protected]
Objective: This study aimed to investigate the association between the serum creatinine-to-cystatin C ratio (CCR) and the prognosis of patients with hip fracture.
Methods: This retrospective cohort study included patients who underwent hip fracture surgery at a tertiary hospital in China between January 2018 and December 2023. CCR was calculated from the preoperative serum creatinine and cystatin C levels. The primary outcome was 1-year mortality after surgery in patients with hip fracture and the secondary outcome was 6-month mortality. The associations between preoperative CCR and prognosis of patients were assessed using Kaplan-Meier curves, Cox regression models, interactions, and stratified analyses.
Results: A total of 1914 patients who underwent surgery for hip fracture were included. The mean age of the participants was 73.4 ± 14.0 years and the median CCR was 7.3 (6.3– 8.5). The prevalence of 1-year mortality flowing hip fracture surgery was 7.3%. Multivariate Cox regression analysis indicated that a high CCR was independently associated with reduced 6-month mortality [hazard ratio (HR) = 0.51; 95% confidence interval (CI) = 0.31– 0.84] and 1-year mortality (HR = 0.61; 95% CI = 0.42– 0.90) after adjusting for covariates. In addition, Kaplan-Meier curve analyses indicated that the low CCR group had higher 6-month and 1-year mortality rates (all P< 0.0001). Subgroup analyses showed that a high CCR was independently associated with reduced 1-year mortality after hip surgery in patients with diabetes (HR = 0.39; 95% CI = 0.17– 0.89), males (HR = 0.48; 95% CI = 0.26– 0.86) and those without hypertension (HR = 0.55; 95% CI = 0.32– 0.97) or cardiovascular disease (HR = 0.54; 95% CI = 0.34– 0.84).
Conclusion: Our study found that a low CCR was associated with poor prognosis in patients undergoing hip fracture surgery. Further research is needed to clarify the mechanism linking low CCR to poor prognosis in hip fracture patients.
Keywords: creatinine-to-cystatin C ratio, mortality, hip fracture, surgery
Introduction
Hip fractures represent a major public health concern in aging populations, with profound implications on morbidity, mortality, and global healthcare resource utilization.1,2 Previous studies have reported a 1-year mortality rate of 10–30% following hip fracture surgery, underscoring its life-threatening nature.3–5 As demographic shifts towards older age groups accelerate, projections indicate an increase in both the incidence of hip fractures and the number of all-cause deaths after hip fracture surgery,6,7 further straining healthcare systems. Therefore, early identification of risk factors associated with mortality is crucial to enable risk stratification, guide targeted interventions, and improve prognosis.
Previous study has shown that postoperative neutrophil-to-lymphocyte ratio and aggregate inflammatory systemic index markers were highly associated with the surgical invasiveness during humeral shaft fracture osteosynthesis in a younger population.8 In addition, a retrospective cohort study reported the postoperative systemic immune-inflammation index was correlated with surgical trauma sustained by an older population with hip fracture.9 Therefore, the inflammatory markers in peripheral blood are associated with the prognosis of hip fractures.
Emerging evidence suggests that the creatinine-to-cystatin C ratio (CCR), a biomarker that integrates renal function and muscle metabolism, may offer prognostic insight beyond conventional renal indices.10 CCR correlates with skeletal muscle mass, systemic inflammation, and oxidative stress,11–13 both of which are closely associated with the prognosis of patients with hip fractures. Observational studies have further associated low serum CCR with adverse outcomes in critical illnesses, cardiometabolic diseases, and malignancies.14–16 Nevertheless, its utility in predicting the 1-year mortality after hip fracture surgery remains unclear.
Therefore, we conducted a retrospective cohort study to explore the association between serum CCR levels and prognosis of patients undergoing hip fracture surgery. This study provides a novel method of using CCR as a tool for the early identification of patients at elevated mortality risk following hip fracture surgery.
Materials and Methods
Study Design and Participants
In this retrospective cohort study, we recorded the data of patients with hip fracture including femoral neck and intertrochanteric fractures, at Changhai hospital from January 2018 to December 2023. This retrospective study was approved by the ethics committee of Changhai hospital (CHEC2024-257). The ethics committee waived the requirement for informed consent due to the retrospective collection of de-identified clinical data from patients. This study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines and conformed to the principles of the Declaration of Helsinki.
To screen participants for this study, patients undergoing hip surgery who met the following criteria were included: patients with a diagnosis of femoral neck fractures and intertrochanteric fractures by X-ray examination at admission; aged≥18 years. Patients with renal function impairment according to an estimated glomerular filtration rate < 60 mL / (min × 1.73 m2) using the Chinese-based equation,17 with multiple fractures, dementia, and missing data on creatinine or cystatin C were excluded.
Variables
Based on existing literature and clinical practice, we collected the following variables. The demographic characteristics included age, gender, American Society of Anesthesiologists (ASA) physical status, body mass index (BMI), alcohol history, and smoking history. The medical history evaluation included hypertension, diabetes, cardiovascular disease (coronary heart disease, arrhythmia, and chronic heart failure), cerebrovascular disease (cerebral infarction and cerebral hemorrhage), lung disease (chronic bronchitis, bronchial asthma, and chronic obstructive pulmonary disease), and cancer.
We also calculated Charlson comorbidity index to perform overall assessment of comorbidities.18 Laboratory results included serum creatinine, cystatin C, albumin, urea nitrogen, glucose, D-dimer, activated partial thromboplastin time (APTT), hemoglobin, lymphocyte count, monocyte count, neutrophil count, leucocyte count, and platelet count. We also recorded the type of anesthesia, surgical procedure, time to admission (time from injury to admission) and time to surgery (time from admission to surgery). Time to admission and time to surgery were derived from medical records.
The most recent preoperative laboratory results were used in this study. The CCR was calculated as creatinine (mg/L) / cystatin C (mg/dL). We used multiple imputations to deal with missing data in continuous variables whose missing values were less than 10%.
Outcomes
The primary endpoint was all-cause mortality within one year of hip fracture surgery. The secondary endpoint was 6-month mortality after surgery. We collected the data on mortality by telephone follow-up.
Statistical Analysis
Participants were divided into two groups based on their CCR values. Continuous variables with normally distributed data were described as mean ± SD and compared using Student’s t-test. The Mann–Whitney U-test was used to compare continuous variables with non-normally distributed data, described as medians (IQR). Categorical variables are presented as frequencies (%) and analyzed using the chi-square test.
CCR levels were categorized as low (<7.3) or high (≥7.3), based on the median. The association between CCR and 6-month, 1-year mortality was constructed using multivariate Cox proportional hazard models when CCR levels were both continuous and binary variables. Variates with a p-value of <0.1 in the comparison of baseline characteristics between the high and low CCR groups, were selected for model adjustment. In Model I, no covariates were adjusted. Model II was adjusted for age, gender, BMI, ASA physical status, time to admission, alcohol history, smoking history, hypertension, diabetes, cardiovascular disease, and lung disease. In model III, covariates including albumin, glucose, D-dimer, APTT, hemoglobin, neutrophil count, and leukocyte count were further adjusted.
We used a smoothed curve fit to assess the association between the CCR and 1-year mortality. Kaplan-Meier curves were generated to compare the probability of survival for the different CCR groups. Stratified and interaction analyses were performed according to age (< 80 or ≥ 80 years), gender (male or female), and ASA physical status (< III or ≥ III), hypertension (yes or no), diabetes (yes or no), and cardiovascular disease (yes or no). Each stratification was adjusted for age, gender, BMI, ASA physical status, time to admission, alcohol history, smoking history, hypertension, diabetes, cardiovascular disease, lung disease, albumin, glucose, D-dimer, APTT, hemoglobin, neutrophil count, and leukocyte count, with exception of the stratification factor itself.
We also performed the propensity score matching and multivariate Cox analyses as sensitivity analyses after excluding patients with younger than 60 years and pathologic fractures due to specific mechanism of hip fracture. This multivariate Cox analysis adjusted for age, gender, BMI, ASA physical status, time to admission, alcohol history, smoking history, hypertension, diabetes, cardiovascular disease, lung disease, albumin, glucose, d-dimer, APTT, hemoglobin, neutrophil count, and leucocyte count. Which were also included in multivariable logistic regression model to conduct propensity score matching analysis. A 1:1 nearest-neighbor matching algorithm with a caliper width of 0.2 was applied and a standardized mean difference (SMD) <0.1 was considered indicative of variable balance between the groups before and after matching.
Free Statistics software version 1.7.1 (Beijing FreeClinical Medical Technology Co., Ltd, Beijing, China), and R 4.2.2 software (http://www.Rproject.org; The R Foundation, Vienna, Austria) were used to conduct all statistical analyses. Statistical significance was set at P < 0.05.
Results
A total of 2,659 patients with hip fracture were identified. After excluding 745 patients with multiple fracture, renal function impairment, dementia, and missing values on creatinine or cystatin C, 1,914 patients with hip fracture were included in the final data analysis as shown in the flow chart (Figure 1).
 |
Figure 1 Flowchart of study population. |
Baseline Characteristics
The baseline information of all the participants is presented in Table 1. The mean age of the patients was 73.4 ± 14.0 years, and females were prevalent (61.9%). The median baseline CCR was 7.3 (6.3–8.5). The 1-year mortality rate of hip fractures was 7.3%. Participants were divided into two groups based on their CCR values. Patients with low CCR had significantly higher 6-month mortality and 1-year mortality (all P < 0.05) than those with high CCR. Comparisons of baseline information between the two groups are shown in Table 1.
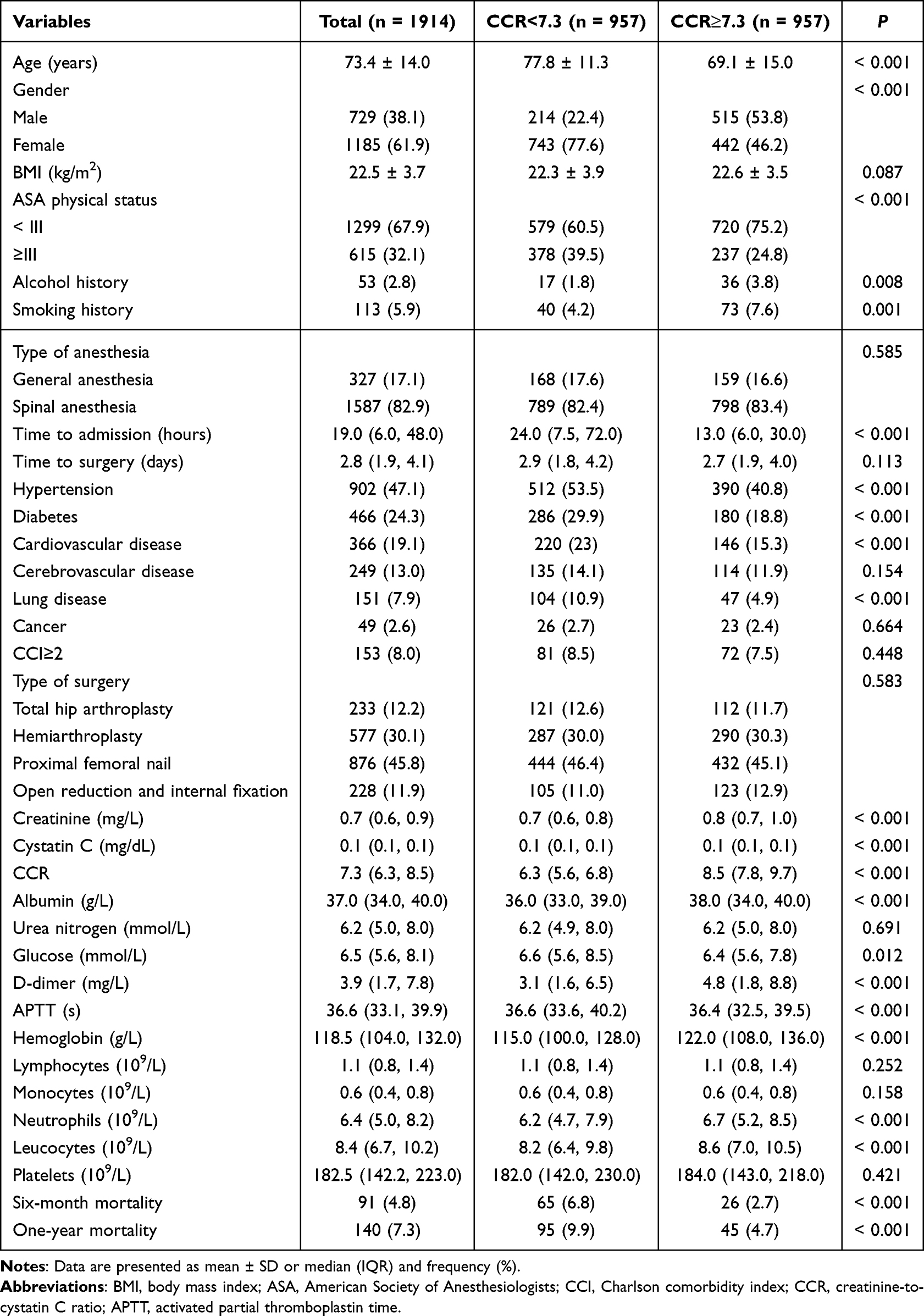 |
Table 1 Demographics and Clinical Characteristics Stratified by CCR |
Association of CCR with Prognosis in Hip Fracture Patients
The linear correlation between the CCR and 1-year mortality after adjusting for confounding variables is shown in Figure 2. Kaplan-Meier curves showed that patients in the high CCR group had a significantly higher 1-year survival rate. A similar result was observed for the 6-month survival curve (Figure 3).
 |
Figure 2 Curve fitting of CCR and 1-year mortality in patients with Hip fracture surgery. Data were fit by a Cox proportional hazard regression model based on restricted cubic splines. P-value for non-linearity derived from Likelihood Ratio Test. CCR was entered as continuous variable. Data were adjusted for the factors (age, gender, BMI, ASA physical status, time to admission, alcohol history, smoking history, hypertension, diabetes, cardiovascular disease, lung disease, albumin, glucose, d-dimer, APTT, hemoglobin, neutrophil count, and leucocyte count). The curves line and shaded areas around depict the estimated values and their corresponding 95% confidence intervals. Curves below depict the distribution of the CCR. Abbreviations: CCR, creatinine-to-cystatin C ratio; BMI, body mass index; ASA, American Society of Anesthesiologists; APTT, activated partial thromboplastin time. |
 |
Figure 3 Kaplan–Meier curve of mortality for patients with Hip fracture surgery. (A) Kaplan–Meier curve of 6-month mortality after hip fracture surgery, (B) Kaplan–Meier curve of 1-year mortality after hip fracture surgery. P-value derived from Log Rank Test. Abbreviation: CCR, creatinine-to-cystatin C ratio. |
Multivariate Cox regression models indicated that a high CCR was independently related to reduced 6-month mortality regarding continuous variable (hazard ratio (HR) = 0.82, 95% confidence interval (CI) = 0.71–0.95) or categorical variable (HR = 0.51, 95% CI = 0.31–0.84) in the adjusted model. Moreover, a high CCR was independently related to reduced 1-year mortality with respect to the continuous variable (HR = 0.88, 95% CI = 0.79–0.99) or categorical variable (HR = 0.61, 95% CI = 0.42–0.90) in the adjusted model. The associations between the unadjusted and adjusted models were robust in all three models (all P < 0.05), as shown in Table 2.
 |
Table 2 Univariate and Multivariate Cox Regression Analysis to Assess the Association Between CCR and Prognosis of the Patients with Hip Fracture Surgery |
Additionally, we also performed sensitivity analyses to provide additional robustness to our findings after excluding patients with younger than 60 years and pathologic fractures. The multivariate Cox regression analysis showed that high CCR was associated with low 1-year mortality (HR = 0.58, 95% CI = 0.40–0.85) (Supplementary Table 2). After matching, all covariates were well-balanced (SMD <0.1) (Supplementary Table 1). Moreover, the propensity score matching also indicated that increased CCR was independently related to decreased 1-year mortality (HR = 0.53, 95% CI = 0.35–0.80) (Supplementary Table 2).
Subgroup Analysis
Subgroup analyses showed that a high CCR was independently associated with reduced 1-year mortality after hip surgery in patients with diabetes (HR = 0.39; 95% CI = 0.17–0.89), males (HR = 0.48; 95% CI = 0.26–0.86) and those without hypertension (HR = 0.55; 95% CI = 0.32–0.97) or cardiovascular disease (HR = 0.54; 95% CI = 0.34–0.84) (Figure 4).
 |
Figure 4 Association between CCR and 1-year mortality in subgroups for patients with Hip fracture surgery. Low CCR was the reference for high CCR. Each stratification adjusted for the factors (age, gender, BMI, ASA physical status, time to admission, alcohol history, smoking history, hypertension, diabetes, cardiovascular disease, lung disease, albumin, glucose, d-dimer, APTT, hemoglobin, neutrophil count, and leucocyte count) in the multivariable Cox regression, except for the stratification factor itself. Abbreviations: CCR, creatinine-to-cystatin C ratio; BMI, body mass index; ASA, American Society of Anesthesiologists; APTT, activated partial thromboplastin time; HR, hazard ratio; CI, confidence interval. |
Discussion
This study included 1,914 patients with hip fracture, and the 1-year mortality rate was 7.3%. We found a negative linear relationship between the CCR and 1-year mortality in patients with hip fracture. Meanwhile, we revealed that a high CCR is associated with reduced 6-month and 1-year mortality in patients with hip fractures after adjusting for covariates. In addition, subgroup analysis showed that a high CCR was independently associated with reduced 1-year mortality in patients with diabetes, males, and those without hypertension or cardiovascular disease. Moreover, the sensitivity analyses provided additional robustness to our findings.
Recent studies have shown that 1-year mortality following hip fractures can vary widely across different populations, with estimates in some cohorts ranging from 10% to 30%,3,19–21 higher than the 7.3% observed in our study. This discrepancy may be due to our inclusion criteria (patients aged ≥18 years) and the short median time from injury to hospital admission (only 19 hours). Previous studies have identified factors such as advanced age, comorbidities, and prolonged time from injury to admission as significant risk factors for increased mortality, which is consistent with the results of our study.22–24 In addition, sarcopenia has also been associated with higher mortality rates after hip fracture surgery.25 Moreover, our study found that CCR, as a biomarker of skeletal muscle mass and strength, was related to 6-month and 1-year mortality following hip fracture surgery.
Studies have shown that low CCR is associated with poor renal function assessment and may reflect systemic immune-inflammation status,26–28 which can influence patient outcomes. Additionally, CCR has been increasingly recognized for its potential prognostic value in various clinical contexts including chronic kidney, cardiovascular, and chronic obstructive pulmonary diseases.29–31 Furthermore, an elevated CCR has been linked to improved outcomes after major surgery.32 In line with previous studies, we found that high CCR levels were associated with low mortality rates after hip fracture surgery.
The protective effect of higher CCR against mortality may stem from its dual representation of renal health and muscle integrity. Cystatin C, a sensitive marker of glomerular filtration, reflects renal clearance capacity,33 while creatinine level indirectly indicates muscle mass.34 Therefore, a higher CCR indicates both adequate renal function and preserved muscle mass, which are critical factors for recovery after hip fracture surgery.
However, the definite causes and pathophysiological mechanisms underlying the relationship between CCR and a poor prognosis remain unclear. Patients with low CCR may experience decreased renal function reserve,35 reduced muscle mass,36 and impaired muscle anabolism,37 resulting in decreased postoperative mobility and an increased risk of complications, such as deep vein thrombosis and pneumonia. This exacerbates frailty and susceptibility to adverse outcomes.
This study has several clinical implications and strengths. First, we analyzed data from a large cohort of 1,914 patients with hip fracture to provide an accurate and reliable association between CCR and the prognosis of patients after hip fracture surgery. Second, we performed strict statistical adjustments to investigate the association between CCR and prognosis in patients to minimize potential confounders. And we conducted sensitivity analyses to verify the robustness of our results. Moreover, the CCR is simple, easy to calculate, convenient for clinical use, and is not affected by individual subjectivity. To our knowledge, this is the first study to explore the relationship between CCR and mortality in patients undergoing hip fracture surgery.
However, our study has some limitations. First, the nature of the retrospective study limits its ability to establish causation. Second, this study had limited generalizability to diverse populations because it included only patients with hip fracture. Additionally, although strict statistical adjustments were made to minimize the effects of confounding factors, some potential confounding factors were not determined. Lastly, the mechanisms behind the relationship of CCR with mortality were unclear. Therefore, prospective studies with larger cohorts are needed to validate our findings and to explore the potential mechanisms underlying the relationship between CCR and mortality.
Conclusion
Our study showed a negative linear association between CCR and 1-year mortality in patients who underwent hip fracture surgery. Moreover, our study highlights the prognostic significance of preoperative CCR in patients with hip fracture, with low CCR independently predicting increased 6-month and 1-year mortality.
Data Sharing Statement
Data supporting the findings of this study can be obtained from the corresponding author (Jiafeng Wang) upon reasonable request, and the corresponding author/s can be directly contacted for further inquiry.
Ethics Statement
Studies involving human participants were reviewed and approved by the ethics committee of Changhai Hospital. Due to the nature of the retrospective study, the ethics committee waived the requirement for informed consent.
Acknowledgments
We thank all the investigators and participants of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that the study was conducted without any commercial or financial relationship or potential conflicts of interest.
References
1. Reppas-Rindlisbacher C, Boblitz A, Podolsky S, et al. Language preference, surgical wait time, and outcomes among older adults with hip fracture. JAMA Network Open. 2024;7(11):e2448010. doi:10.1001/jamanetworkopen.2024.48010
2. Viamont-Guerra MR, Guimarães R, Bridges C, Antonioli E, Lenza M. Ultra-early versus early surgery for hip fracture. Cochrane Database Syst Rev. 2024;6(6):Cd015697. doi:10.1002/14651858.CD015697
3. Xi S, Wu Z, Cui J, Yin S, Xi S, Liu C. Association between frailty, as measured by the FRAIL scale, and 1-year mortality in older patients undergoing hip fracture surgery. BMC Geriatr. 2025;25(1):65. doi:10.1186/s12877-025-05716-z
4. Zhang BF, Xu SL, Yang Z, Xu P. Early admission is better-the time to admission (TTA) is associated with one-year mortality in hip fracture. Int J Surg. 2024;110(12):7880–7888. doi:10.1097/JS9.0000000000001835
5. Harvey LA, Payne NL, Tan A, et al. Variation in mortality following hip fracture across the Asia Pacific region: systematic review and proportional meta-analysis. Arch Gerontol Geriatrics. 2024;126:105519. doi:10.1016/j.archger.2024.105519
6. Du G, Fan Z, Fan K, et al. Risk-stratified lifetime risk and incidence of hip fracture and falls in middle-aged and elderly Chinese population: the China health and retirement longitudinal study. J Orthopaedic Transl. 2025;50:174–184. doi:10.1016/j.jot.2024.10.013
7. Jensen TM, Pedersen JK, Waldorff FB, Søndergaard J, Overgaard S, Christensen K. Trends in incidence of hip fracture and hip replacement in Denmark, 1996 to 2018. JAMA Network Open. 2024;7(5):e249186. doi:10.1001/jamanetworkopen.2024.9186
8. Moldovan F. Correlation between peripheric blood markers and surgical invasiveness during humeral shaft fracture osteosynthesis in young and middle-aged patients. Diagnostics. 2024;14(11):1112. doi:10.3390/diagnostics14111112
9. Moldovan F, Ivanescu AD, Fodor P, Moldovan L, Bataga T. Correlation between inflammatory systemic biomarkers and surgical trauma in elderly patients with hip fractures. J Clin Med. 2023;12(15):5147. doi:10.3390/jcm12155147
10. Liu H, Wang J, Tan S, et al. Sarcopenia and myosteatosis diagnostic tool for gastrointestinal cancer: creatinine to cystatin C ratio as evaluation marker. J Transl Med. 2023;21(1):744. doi:10.1186/s12967-023-04628-z
11. Ning X, Xie C, Kong Y. Serum creatinine- and cystatin C-based indices are associated with the risk of subsequent sarcopenia: evidence from the China health and retirement longitudinal study. Front Nutrition. 2024;11:1471068. doi:10.3389/fnut.2024.1471068
12. Liu F, Liu Y, Peng Q, et al. Creatinine accelerates APAP-induced liver damage by increasing oxidative stress through ROS/JNK signaling pathway. Front Pharmacol. 2022;13:959497. doi:10.3389/fphar.2022.959497
13. Serwin N, Cecerska-Heryć E, Pius-Sadowska E, et al. Renal and inflammation markers-renalase, cystatin C, and NGAL levels in asymptomatic and symptomatic SARS-CoV-2 infection in a one-month follow-up study. Diagnostics. 2022;12(1):108. doi:10.3390/diagnostics12010108
14. Jung CY, Joo YS, Kim HW, et al. Creatinine-cystatin C ratio and mortality in patients receiving intensive care and continuous kidney Replacement therapy: a retrospective cohort study. Am J Kidney Dis. 2021;77(4):509–516.e501. doi:10.1053/j.ajkd.2020.08.014
15. Sun H, Wu Z, Wang G, Liu J. Normalized creatinine-to-cystatin C ratio and risk of cardiometabolic multimorbidity in middle-aged and older adults: insights from the china health and retirement longitudinal study. Diabet Metabol J. 2025;49(3):448–461. doi:10.4093/dmj.2024.0100
16. Ji H, Liu B, Jin P, et al. Creatinine-to-cystatin C ratio and body composition predict response to PD-1 inhibitors-based combination treatment in metastatic gastric cancer. Front Immunol. 2024;15:1364728. doi:10.3389/fimmu.2024.1364728
17. Li DY, Yin WJ, Yi YH, et al. Development and validation of a more accurate estimating equation for glomerular filtration rate in a Chinese population. Kidney Int. 2019;95(3):636–646. doi:10.1016/j.kint.2018.10.019
18. Wang P, Guo S. Correlation between Charlson comorbidity index and surgical prognosis in elderly patients with femoral neck fractures: a retrospective study. BMC Musculoskeletal Disord. 2024;25(1):678. doi:10.1186/s12891-024-07814-2
19. Hu Z, Song C, Zhang J. Elevated serum albumin-to-creatinine ratio as a protective factor on clinical outcomes among critically ill patients with sepsis: a retrospective study. Front Med. 2024;11:1436533. doi:10.3389/fmed.2024.1436533
20. Fu G, Wu R, Zhang R, et al. Preoperative vitamin D deficiency is associated with increased one-year mortality in Chinese geriatric hip Fracture patients - a propensity score matching study. Clin Interventions Aging. 2023;18:263–272. doi:10.2147/CIA.S395228
21. Fu G, Li H, Wang H, et al. Comparison of peripheral nerve block and spinal anesthesia in terms of postoperative mortality and walking ability in elderly hip fracture patients - a retrospective, propensity-score matched study. Clin Interventions Aging. 2021;16:833–841. doi:10.2147/CIA.S311188
22. Harvey L, Taylor ME, Harris IA, et al. Adherence to clinical care standards and mortality after hip fracture surgery in New South Wales, 2015-2018: a retrospective population-based study. Medl J Australia. 2024;221(9):480–485. doi:10.5694/mja2.52470
23. Spaetgens B, Brouns SHA, Linkens A, et al. Associations between presence of diabetes, mortality and fracture type in individuals with a hip fracture. Diabetes Res Clin Pract. 2022;192:110084. doi:10.1016/j.diabres.2022.110084
24. Clement ND, Farrow L, Chen B, Duffy A, Murthy K, Duckworth AD. Delayed admission of patients with hip fracture from the emergency department is associated with an increased mortality risk and increased length of hospital stay. Emerg Med J. 2024;41(11):654–659. doi:10.1136/emermed-2023-213085
25. Kim HS, Park JW, Lee YK, et al. Prevalence of sarcopenia and mortality rate in older adults with hip fracture. J Am Geriatr Soc. 2022;70(8):2379–2385. doi:10.1111/jgs.17905
26. Mottaghi A, Alipour F, Alibeik N, et al. Serum cystatin C and inflammatory factors related to COVID-19 consequences. BMC Infect Dis. 2023;23(1):339. doi:10.1186/s12879-023-08258-0
27. Zhang Z, Zhou T, Zhang M, Cheng S. Predictive value of creatinine-cystatin C ratio for mortality and technique failure in anuric peritoneal dialysis patients. Renal Failure. 2025;47(1):2444389. doi:10.1080/0886022X.2024.2444389
28. Sun Y, Zhao J, Du J, Li Y, Ding F, Zhao W. Clinical implications and predictive value of the creatinine‑cystatin C ratio in patients with multiple myeloma and renal impairment. Oncol Lett. 2024;27(3):134. doi:10.3892/ol.2024.14267
29. Choi MC, Kim DG, Yim SH, et al. Creatinine-cystatin C ratio and death with a functioning graft in kidney transplant recipients. Sci Rep. 2024;14(1):1966. doi:10.1038/s41598-024-52649-5
30. Kawasaki Y, Nishiki K, Nojiri M, et al. Prognostic value of the serum creatinine/cystatin C ratio in patients with chronic obstructive pulmonary disease. Respiratory Investig. 2024;62(1):143–149. doi:10.1016/j.resinv.2023.11.007
31. Wang S, Yang T, Bao Y, et al. Association of serum creatinine-cystatin C ratio with all-cause, cardiovascular and cancer mortality in US adults: a nationwide cohort study. BMC Geriatr. 2024;24(1):963. doi:10.1186/s12877-024-05546-5
32. Kim HJ, Kim HB, Kim HY, Shim JK, Lee C, Kwak YL. Associations of creatinine/cystatin C ratio and postoperative pulmonary complications in elderly patients undergoing off-pump coronary artery bypass surgery: a retrospective study. Sci Rep. 2021;11(1):16881. doi:10.1038/s41598-021-96442-0
33. Karger AB, Shlipak MG. Glomerular Filtration Rate (GFR) estimation with cystatin C-past, present, and future. Clin Chem. 2025;71(7):743–751. doi:10.1093/clinchem/hvae226
34. Ng JK, Fung WW, Chan GC, et al. Modified creatinine index as a marker of skeletal muscle mass in peritoneal dialysis patients. Clin Kidney J. 2024;17(10):sfae297. doi:10.1093/ckj/sfae297
35. Cai Y, Lv H, Yuan M, et al. Genome-wide association analysis of cystatin c and creatinine kidney function in Chinese women. BMC Med. Genomics. 2024;17(1):272. doi:10.1186/s12920-024-02048-6
36. Rizk JG, Streja E, Wenziger C, et al. Serum creatinine-to-cystatin-C ratio as a potential muscle mass surrogate and racial differences in mortality. J Renal Nutrition. 2023;33(1):69–77. doi:10.1053/j.jrn.2021.11.005
37. Wang Z, Cao W, Deng B, Fan D. Lower creatinine-to-cystatin c ratio associated with increased risk of incident amyotrophic lateral sclerosis in the prospective UK biobank cohort. Sci Rep. 2024;14(1):28289. doi:10.1038/s41598-024-79910-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations Between Morphological Phenotypes of COPD and Clinical Characteristics in Surgically Resected Patients with COPD and Concomitant Lung Cancer
Suzuki Y, Kitaguchi Y, Ueno F, Droma Y, Goto N, Kinjo T, Wada Y, Yasuo M, Hanaoka M
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1443-1452
Published Date: 21 June 2022
Intertrochanteric Fracture Surgery Patients with Diabetes Mellitus are Prone to Suffer Perioperative Neurological and Endocrine/Metabolic Complications: A Propensity-Score Matched Analysis
Tang Y, Kang L, Guo M, Fan L
Therapeutics and Clinical Risk Management 2022, 18:775-783
Published Date: 6 August 2022
Characteristics of Elderly Hip Fracture Patients in Jordan: A Multicenter Epidemiological Study
Dawod MS, Alisi MS, Saber YO, Abdel-Hay QA, Al-Aktam BM, Alfaouri Y, Alfraihat LB, Albadaineh AA, Abuqudiri AZ, Odeh RM, Altamimi AAR, Alrawashdeh MA, Alebbini MM, Abu-Dhaim OA, Al-Omari AA, Alaqrabawi I, Alswerki MN, Abuawad A, Al Nawaiseh MR, Hammad Y, Al-Ajlouni J
International Journal of General Medicine 2022, 15:6591-6598
Published Date: 13 August 2022
The Widowhood Effect on Mortality in Older Patients with Hip Fracture
Zhu Z, Wang Z, Wu Y, Chen X, Liu H, Zhang J, Liu M, Liu Y
International Journal of General Medicine 2022, 15:7693-7700
Published Date: 7 October 2022
Preoperative Vitamin D Deficiency is Associated with Increased One-Year Mortality in Chinese Geriatric Hip Fracture Patients – A Propensity Score Matching Study
Fu G, Wu R, Zhang R, Chen D, Li H, Zheng Q, Ma Y
Clinical Interventions in Aging 2023, 18:263-272
Published Date: 18 February 2023