Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
COPD-Related Anxiety: A Systematic Review of Patient Perspectives
Authors Christiansen CF, Løkke A ![]() , Bregnballe V, Prior TS
, Bregnballe V, Prior TS ![]() , Farver-Vestergaard I
, Farver-Vestergaard I
Received 14 January 2023
Accepted for publication 30 May 2023
Published 6 June 2023 Volume 2023:18 Pages 1031—1046
DOI https://doi.org/10.2147/COPD.S404701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Camilla F Christiansen,1,2 Anders Løkke,1,2 Vibeke Bregnballe,3 Thomas Skovhus Prior,4 Ingeborg Farver-Vestergaard1,2
1Department of Medicine, Lillebaelt Hospital, Vejle, Denmark; 2Department of Regional Health Research, University of Southern Denmark, Odense, Denmark; 3Faculty of Health, Aarhus University, Aarhus, Denmark; 4Center for Rare Lung Diseases, Department of Respiratory Diseases and Allergy, Aarhus University Hospital, Aarhus, Denmark
Correspondence: Ingeborg Farver-Vestergaard, Department of Medicine, Lillebaelt Hospital, Beriderbakken 4, Vejle, 7100, Denmark, Tel +45 79 40 98 32, Email [email protected]
Background: Anxiety in patients with chronic obstructive pulmonary disease (COPD) is prevalent but often unidentified and therefore not adequately managed. Clinicians find it difficult to detect anxiety symptoms and to differentiate subclinical anxiety from anxiety disorders, because of the considerable overlap between symptoms of COPD and anxiety.
Purpose: We synthesized existing qualitative research on patients’ experiences of COPD-related anxiety with the purpose of gaining a richer understanding and proposing a model of the construct.
Methods: Searches for qualitative studies of patients’ experiences of COPD-related anxiety were conducted independently by two authors in the databases of PubMed (MEDLINE), CINAHL (EBSCO), and PsycInfo (APA). English-language studies including patients diagnosed with COPD were reviewed, and data were analyzed using thematic analysis.
Results: A total of 41 studies were included in the review. Four themes related to COPD-related anxiety were identified: initial events; internal maintaining factors; external maintaining factors; and behavioral maintaining factors. Based on the identified four themes, a conceptual model of COPD-related anxiety from the patient perspective was developed.
Conclusion: A conceptual model of COPD-related anxiety from the patient perspective is now available, with the potential to inform future attempts at improving identification and management of COPD-related anxiety. Future research should focus on the development of a COPD-specific anxiety questionnaire containing domains that are relevant from the patient perspective.
Keywords: qualitative studies, psychological symptoms, chronic disease management, psychological distress, mental health, respiratory illness, chronic obstructive pulmonary disease
Introduction
Patients with chronic obstructive pulmonary disease (COPD) report high levels of anxiety symptoms, and anxiety disorders (eg, panic disorder, generalized anxiety disorder, social anxiety disorder) are among the most prevalent psychiatric comorbidities in patients with COPD.1–3 Clinically relevant anxiety symptoms in patients with COPD are often unidentified and therefore not managed; and potential anxiety disorders are underdiagnosed and therefore not adequately treated.4 A review of the literature from 1994 to 2009 shows that the estimated prevalence of anxiety symptoms and anxiety disorders among patients with COPD varies markedly across existing studies (6–74%),5 potentially due to difficulties in differentiating between symptoms of COPD and symptoms of anxiety.6
For patients in general, anxiety is a natural, adaptive psychophysiological response to a real or perceived threat, which is experienced as passing emotional states that the patient feels capable of coping with alone or with social support from significant others.7 However, for many patients with COPD, symptoms of anxiety are persistent over a longer period of time and can be associated with maladaptive behaviors, such as avoidance of activities that are expected to trigger dyspnea.8–10 This can lead to isolation, deconditioning, symptom progression, and reduced quality of life and eventually result in the development of an anxiety disorder, per se.1,11
Furthermore, COPD is associated with social and economic disadvantage,12 and patients with COPD often suffer from multiple comorbid diseases, such as cardiovascular diseases, lung cancer, and osteoporosis,13 with overlapping physiological (eg, dyspnea, pain, and fatigue) and psychological (anxiety and depression) symptoms and risk factors. In clinical practice, it can be difficult to differentiate psychological symptoms originating from specific life circumstances, physical symptoms or diseases, and there is a need for identification of patient experiences of anxiety that are specifically related to life with COPD.
Terms such as fear and anxiety are often used interchangeably in the literature, but there are several definitions of the concepts as well as potentially different underlying neurobehavioral mechanisms.6,14 From the patient perspective, the subjective experience of anxiety is multifaceted, and patients themselves describe states of anxiety using many different terms, including fear, worry, being afraid, anxiety, panic attacks, etc. Altogether, this adds to the confusion around the concept of COPD-related anxiety.
Taken together, the current understanding of COPD-related anxiety is generally limited, and research summarizing the concept from the patient perspective is lacking. Therefore, with the purpose of exploring the complexity of COPD-related anxiety, the present review aims to synthesize the available qualitative research on patients’ experiences with COPD-related anxiety and to propose a model of the concept.
Materials and Methods
The present study is a systematic review of qualitative studies identified in a larger systematic review of quantitative and qualitative studies of COPD-related anxiety (PROSPERO ID: CRD42021261124; https://www.crd.york.ac.uk/prospero/) and adheres to the PRISMA 2020 guidelines.15 The analysis of the quantitative studies is currently ongoing and will be presented elsewhere. The synthesis of qualitative study findings in the present study is based on Thomas and Harden’s thematic synthesis approach.16 The themes and their interrelations were discussed among the group of authors as well as other clinicians and researchers, on the basis of which a conceptual model was proposed.
Search Strategy and Study Selection
The literature search was performed in April 2023 by block search (Supplementary Material, Section 1) in the databases of PubMed (MEDLINE), CINAHL (EBSCO), and PsycInfo (APA). Danish, English, Norwegian, and Swedish-language articles describing qualitative studies of anxiety among people diagnosed with COPD were eligible for inclusion. Interview-based and focus group studies were selected as we were interested in patients’ own narratives about their experiences. References were imported to and managed using Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia (available at www.covidence.org).
The screening process was performed independently by two researchers (CFC and IFV). Conflicts were discussed and solved in agreement. If agreement was not reached, a third researcher (AL) reviewed the conflicts and made the final decision. Initially, relevance of the identified references was assessed by reviewing titles and abstracts. Full-text of the remaining references were screened based on the inclusion and exclusion criteria (Supplementary Material, Section 1). Quality appraisal was performed, and studies of low quality were excluded.
Quality Appraisal and Data Coding
Critical Appraisal Skills Programme Checklist for Qualitative Research (CASP) checklist, recommended by the GRADE working group,17 was used to assess quality and rigor by identifying strengths and weaknesses of the studies. The studies were assessed by one researcher (CFC) and afterwards discussed with another researcher (IFV).
Data extraction and thematic synthesis were conducted using Thomas and Harden’s approach.16 The thematic synthesis contained three steps: 1) coding text line-by-line, 2) developing descriptive themes, and 3) generating analytical themes. An example of the synthesis is shown in Supplementary Material, Section 2.
Results
For an overview of the results of the study selection process, see Figure 1. A total of 7004 references were identified in the systematic search.
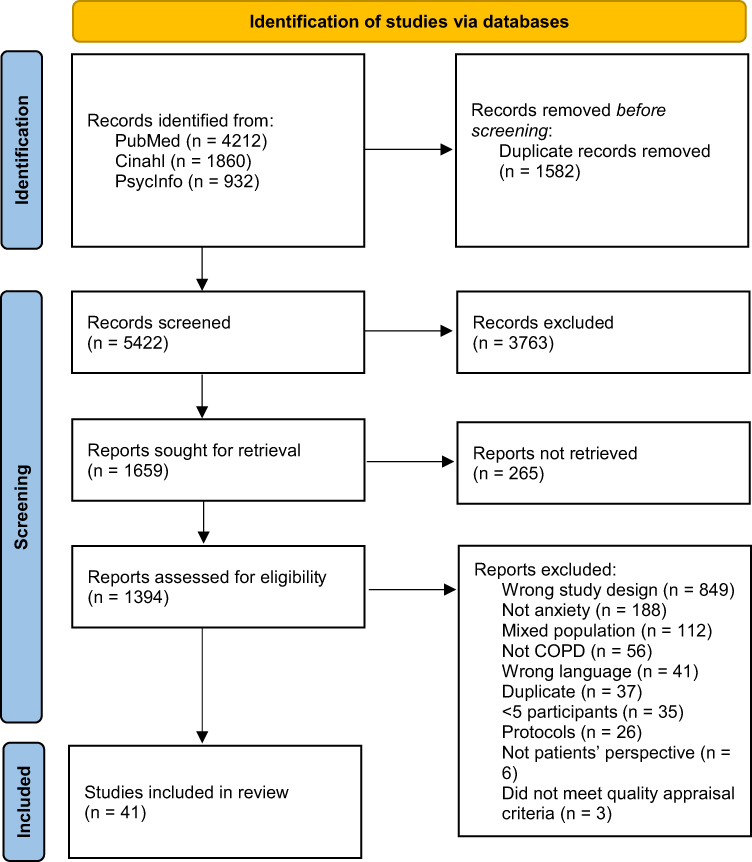 |
Figure 1 PRISMA flow diagram of the study selection process. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. Creative Commons. For more information, visit: http://www.prisma-statement.org/. |
After removal of duplicates (n=1582), the titles and abstracts of the remaining references were assessed and references irrelevant to the aim of the study were excluded (n=3763). Full-text references (n=1659) were reviewed and assessed for eligibility. A total of 44 studies met the inclusion criteria, but after quality assessment, three studies were excluded due to lack of ethical considerations, lack of ethical approval, and/or not using a qualitative design. The remaining 41 studies were considered rigorous with relevant aim, method, and study population and deemed relevant for inclusion in this review.
Study Characteristics
An overview of study characteristics is presented in Table 1. The majority of studies recruited patients from single countries, while one study18 recruited participants from five different countries. All studies used qualitative analysis methods including grounded theory, phenomenology, hermeneutics, and social constructivist approaches. In 39 studies, both men and women were included, while one study19 included women only, and one study included only men.20 Number of interviewed patients ranged from 5 to 125 across the included studies. All studies included participants with COPD of varying illness severity.
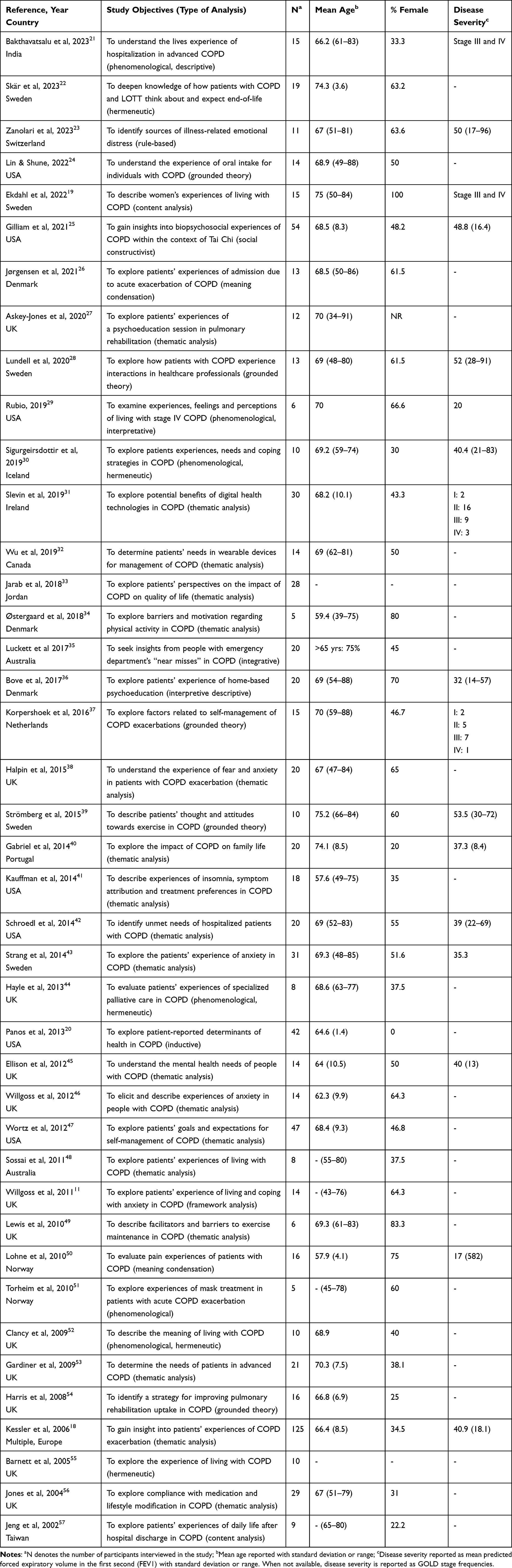 |
Table 1 Study Characteristics |
Main Results
In total, four analytical themes described COPD-related anxiety from the patients’ perspectives: initial events; internal maintaining factors; external maintaining factors; behavioral maintaining factors. The distribution of the themes by study is shown in Table 2. Based on the identified four themes, a conceptual model of COPD-related anxiety from the patient perspective was proposed (Figure 2).
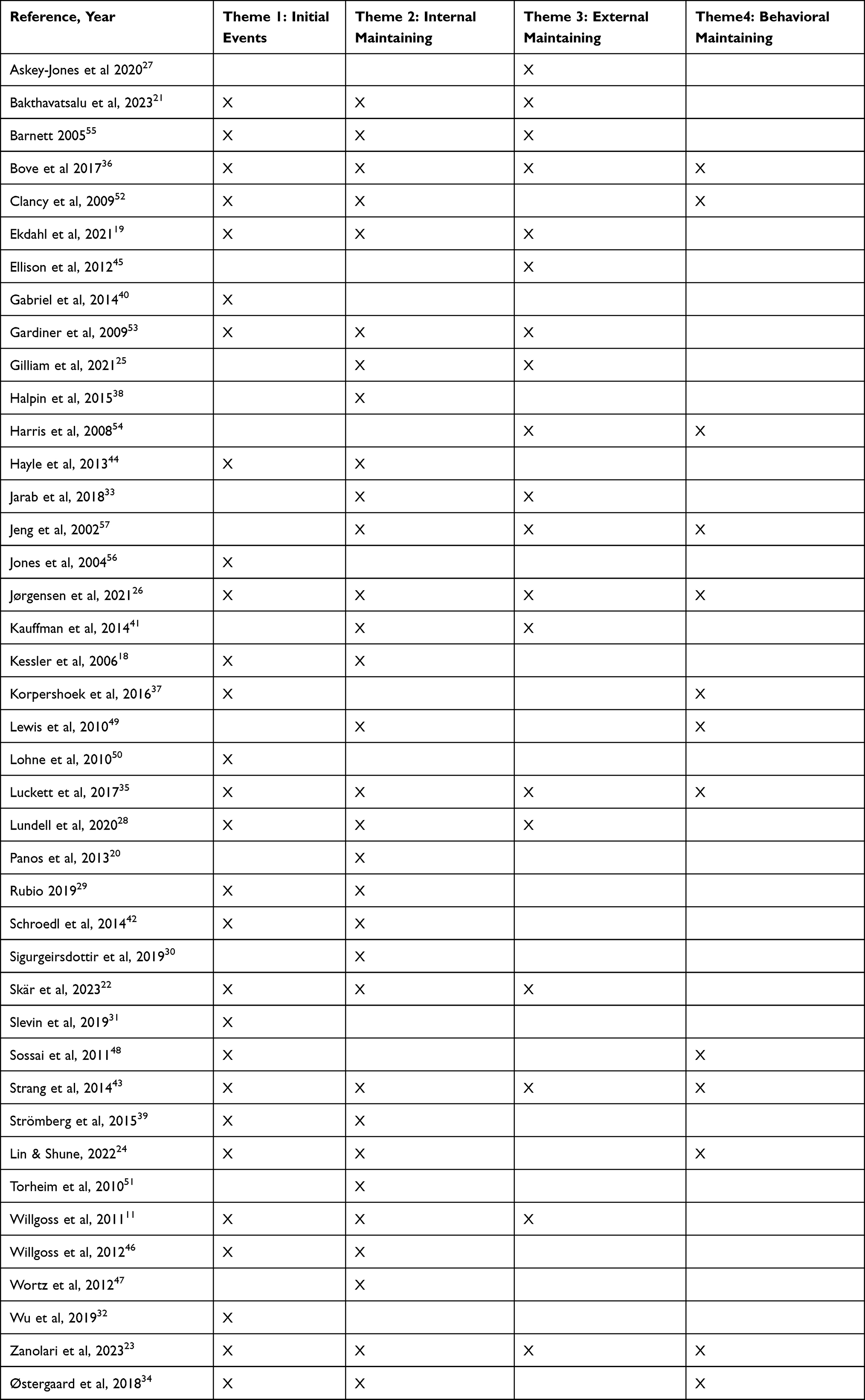 |
Table 2 Data Supporting Themes |
 |
Figure 2 Conceptual model of COPD-related anxiety from the patient perspective. |
The four themes in the conceptual model of COPD-related anxiety are interrelated, which is indicated by the arrows in the model. According to the model, COPD-related anxiety is a process that begins with the initial triggers and develops over time through maintaining factors that can be either internal (eg, inner states, thoughts, and feelings), external (eg, physical and social environment), or behavioral (eg, fear-induced avoidance).
Theme 1: Initial Events
Initial events refer to specific experiences that trigger first episodes of COPD-related anxiety: 1a) when the patient is diagnosed with COPD or realizes what the prognosis can be; 1b) the first experience of symptom progression or exacerbation; 1c) the first experience with loss of specific abilities or functions.
The Diagnosis and Realization of Prognosis
Patients described being diagnosed with COPD as a major life transition, followed by a period of psychological crisis with worry, fear, and anxiety.31,34,39 The impact of the diagnosis left patients feeling anxious about both living with and dying from COPD, and the uncertainty of the prognosis further contributed to anxiety.11,22,23,43 Being offered palliative care as a part of patients’ COPD care pathway increased anxiety, due to the realization that death was part of the prognosis.43,44,50
The First Experience of Disease Progression or Exacerbation
Patients expressed worries and fear related to the symptoms and progression of COPD.18,23,26,28,31,40,47,52 The experience of a severe exacerbation induced panic and constant fear and worry of rehospitalization.18,32 Patients described medication as “life-saving” in the event of an exacerbation. Being without it or misplacing it caused anxiety.11,46 Thoughts about potential ineffectiveness of medical treatment and having difficulty judging when inhalers (medicine) were empty led to increased anxiety during an exacerbation.18,28,37,52,56 Emergency admissions often involved quick medical decisions and immediate treatment, which at times could be overwhelming and anxiety provoking.21 When experiencing progression, patients expressed fear of dying – not of being dead but of the dying process involving suffocation.21,28,36,42,43
First Experiences with Loss of Abilities
COPD-related anxiety was described as a vicious circle, a downward spiral, and an uncontrollable force of nature,11,24,26,35,46 which had a debilitating effect on daily life and led to feelings of worry and grief due to lost abilities.19,26,48,53 Patients struggled to manage daily activities due to uncertainty related to physical activities, which increased breathlessness and panic attacks. For example, feeling breathless walking around town with their families and having to stop due to fear of collapsing, or when eating or drinking, which could trigger fear or breathlessness, coughing, or choking.24 For some patients, anxiety also resulted in profuse sweating and incontinence, which made them embarrassed and subsequently avoid social situations.11,19,21,23,29,32,52,55
Theme 2: Internal Maintaining Factors
Internal maintaining factors refer to patients’ inner processing of 2a) breathlessness; 2b) exacerbation, disease progression, and dying; 2c) uncertainty and the overlapping symptoms of COPD and anxiety.
Inner Processing of Breathlessness
Breathlessness was a central part of all patients’ experiences and was identified as the most troublesome symptom of COPD.22,23,25,26,29,30,55 Metaphors used to describe breathlessness, eg, fear of breathlessness, were compared to fighting a war without weapons30 and as an iron ring across the chest.26 Breathlessness was experienced as an attack, feeling of suffocation, shortness of breath, lack of air, and smothering.21,24,26,34,39,47,49,51,52,55 Breathlessness led to feelings of potentially life-threatening situations, fear of dying, and uncertainty of when it was the last breath.19,20,23,24,28,35,42,43,47,51,55 Breathlessness and thoughts of suffocation were described as the worst, horrible, dramatic experience ever experienced.51
Inner Processing of Exacerbation, Disease Progression, and Dying
Patients’ descriptions of inner processing related to exacerbation, disease progression, and dying were divided into two thought directions: the memories of previous experiences (thinking back), and the fear of having another similar experience in the future (thinking ahead). Experiences of breathlessness, panic, and anxiety had a long-term impact, and former experiences were frequently revisited as flashbacks. Flashbacks to previous attacks acted as a trigger for further attacks in a vicious cycle of events.11 As an example of fear of future events, patients described being afraid of infections due to potential life-threatening consequences. Being breathless and running out of oxygen without access to help led to feelings of fear and panic.19,22,25,38,41,44 Patients, who had never experienced episodes of severe breathlessness, still felt anxiety and fearful, imagining future episodes of breathlessness.11,30,34,38,49,57 Patients were affected by the COPD diagnosis and prognosis and the realization that they had to live with COPD for the rest of their lives. These thoughts initiated worry and fear of the future.22 Patients used metaphors such as fear of ending their days as a vegetable, fading away slowly, or being pronounced dead prematurely and buried alive.43 The inner processing was described as fear of the process of dying; the long struggle of breathlessness, struggling for air, and painful suffocation.18,19,25,36,41,43,53
Inner Processing of Uncertainty and Symptom Overlap
Patients described episodes of anxiety as idiopathic and easily triggered without warning.11,33,46 The uncertainty increased feelings of losing control and resulting in panic.11,55 Their daily life was affected by meta-worry (worry about worry) about previous panic attacks, which caused escalating fear, worry, and new panic attacks.44,46 Moreover, patients were continually considering an array of possible causes for future attacks.18–20,23,33,35,46,57 Patients described how they had been living with anxiety for years without being aware of it, due to the confusing overlap of COPD and anxiety symptoms.11,46
Theme 3: External Maintaining Factors
External maintaining factors refer to patients’ surroundings that can intensify feelings of anxiety in the patient: 3a) social roles and reactions from network; 3b) the societal stigma towards having COPD; 3c) being faced with the condition of other patients; 3d) being in an unsafe environment.
Social Roles and Reactions from Network
Patients described feeling lonely when experiencing COPD-related anxiety, as they believed their symptoms were distressing for their families, and they expressed fear of becoming a burden to their network. At the same time, patients expressed anxiety of separation and leaving relations behind.11,21–23,43,53 Patients felt that relatives had difficulties understanding their situation and feelings.36,45,57 Loss of role within the family, including loss of intimacy in personal relationships due to embarrassment of breathlessness, was perceived by patients as an increase in social distancing from others.25,45,55
Societal Stigma
Patients were affected by what they perceived as societal stigma and feelings of not being taken seriously in the healthcare system,19,23,25,27,28,53 based on the assumption that causes of COPD are self-inflicted and that COPD could be compared with human immunodeficiency virus (HIV) or addiction.19,23,25,26,28,45,54
Witnessing Other Patients’ Suffering
Patients’ perception of COPD and progression worsened by speaking to and/or witnessing the condition of other patients with COPD. This self-other-awareness gave a feeling of being vulnerable, as it increased feelings of anxiety due to the imagination that their self-efficacy slowly would decrease as COPD progressed.22,36,52
Unsafe Environment
Patients feared or dreaded not being able to speak to others or call for help during an exacerbation, especially during the night.22 When feeling a small change in the quality of breathing or during the first signs of an exacerbation, patients would seek hospital intervention instead of relying on self-management or coping.33,35,41
Theme 4: Behavioral Maintaining Factors
Behavioral maintaining factors refer to behaviors that are initiated by patients with the purpose of protecting themselves, but which ends up maintaining COPD-related anxiety: 4a) avoiding physical activity, 4b) social distancing, and 4c) seeking hospital admission instead of self-management as common behavioral strategies.
Avoiding Physical Activity
Avoidance was a common coping mechanism resulting in limited ability to perform adequate self-management actions during anxiety attacks, due to the lack of exposure to anxiety-related situations or events.24,35–37,43 COPD-related anxiety was a barrier for meaningful activities due to fear of situations that were out of their control. Patients further elaborated barriers such as fear of being too far away from home, worry about collapsing due to breathlessness, and anxiety related to unfamiliar places.23,24,34,48,49,52,54,57 Physical activity revealed the illness in front of others, which further contributed to making physical activity a source of distress.23 Fear of experiencing a panic attack was described as disabling, and patients were anxious of being too breathless, which ultimately limited their activities.23,24,34,46
Social Distancing
As examples of memories of earlier experiences leading to fear of future events, patients described an exacerbation as a traumatic life-changing crisis or attack that affected their relationships with others and led to isolation during an exacerbation.18,46 Fear of dependency and becoming an additional burden to their network led to further social distancing.23,45,57 Patients expressed that relatives had difficulties comprehending their situation, which led to social distancing.36,45,57 Patients were affected by societal stigma and feelings of not being taken seriously in the healthcare system, which led to not seeking help for mental health issues.19,25,27,28,53 The stigma and blame were external barriers for patients seeking help from others.19,25,45
Seeking Hospital Intervention Instead of Self-Management
Patients misinterpreted their panic attacks as an acute exacerbation of COPD, which resulted in needless hospital admissions.11 Patients would often seek hospital intervention instead of relying on self-management or coping.33,35,41 Patients were afraid that they would be discharged from the hospital too soon, and they felt safe in the hands of health-care professionals at the hospital.26
Discussion
Our study summarized the findings from 41 existing qualitative studies of patients’ experiences of COPD-related anxiety. Four themes were identified in the analysis: initial events; internal maintaining factors; external maintaining factors; and behavioral maintaining factors. Altogether constituting a conceptual model of COPD-related anxiety from the patient perspective. According to the model, specific initial events can trigger COPD-related anxiety, ie, realizing the diagnosis and/or prognosis, experiencing exacerbation/symptom progression for the first time, and loss of function and/or abilities due to COPD. Multiple studies have explored the psychological effect of specific events in other illness trajectories,58,59 and the psychological burden of receiving a cancer diagnosis has been extensively studied.60,61 Meanwhile, it is not common to consider these events in the COPD illness trajectory as potential anxiety provoking experiences, and the psychological burden of receiving a COPD diagnosis has not been given the same degree of attention in the literature. One possible explanation for this lack of focus might be related to the consideration that smokers should expect to be ill from smoking, which is a widespread understanding of COPD, despite also being the case for certain cancers and cardiovascular disease.62 Another explanation may be the relatively slow progression of the disease, often resulting in several visits to the doctor with symptoms and declining lung function before the diagnosis is confirmed by the physician and disclosed to the patient.63 Nonetheless, cancer and COPD may have similar disease burden and survival rates,61 and patients’ reactions to this should be explored more extensively in the future – clinically and empirically.
Results of our study indicated that as soon as COPD-related anxiety had been triggered, it was maintained and potentially worsened over time by internal, external, and behavioral maintaining factors. The anxiety-maintaining effect of the inner processing of breathlessness, for example in the form of breathlessness catastrophizing, has been more extensively studied,10,64,65 and a number of questionnaires have been developed to assess this specific aspect of COPD-related anxiety, eg, the Breathlessness Catastrophizing Scale,66 and the Interpretation of Breathing Problems Questionnaire.67 Other internal factors maintaining anxiety in COPD have been largely overlooked in COPD-specific anxiety questionnaires. For example, the results of the present review showed that patients were troubled by thoughts of death and the process of dying. Patients alluded that even shortly after being diagnosed with COPD and understanding the prognosis, death became a near reality, which affected their internal processes. Results elucidated that patients were not afraid of being dead, but feared the process of dying. While it is intuitive to think that death-anxiety refers to the absence of life or missing out, patients described that they were afraid of how they were going to die, ie, through suffocation. Other studies have found that patients with COPD want information on what dying might be like for them in order to prepare themselves.68,69 Patients described thoughts and fear of death as having a great impact early in the course of illness and not only towards end-of-life.70 In spite of being aware of patient needs, many health-care providers feel inadequately prepared for discussing end-of-life issues and might therefore tend to avoid bringing up the subject.71 Moreover, appropriate timing of these conversations can be challenging, due to the unpredictability of the general illness trajectory in COPD compared to cancer.70
The results of the present study indicated that patients were suppressing information about mental health, believing that their network and health-care providers could not understand or comprehend their situation, and therefore refrained from asking for help. Avoidance and social distancing were initiated by patients for protective purposes, but most likely ended up maintaining and/or worsening the symptoms, because they remain largely unidentified in a clinical setting.6,72 Studies have shown that non-pharmacological interventions, such as pulmonary rehabilitation programmes psychological interventions, improve exercise capacity, dyspnea, emotional functioning, health-related quality of life, general anxiety symptoms, and COPD-related anxiety.73–75 However, lack of attendance for such activities is common,76,77 which is in line with the findings of our study, where patients try to protect themselves by avoiding physical activity.
With the purpose of strengthening the identification of COPD-related anxiety in the future, there are a number of potential barriers among health-care providers that need to be overcome, such as not recognizing the scale of the problem, not considering anxiety as part of the remit, and lack of knowledge about or access to appropriate interventions.78 Both health-care providers and patients can benefit from implementing systematic, psychological screening processes, because it can potentially increase confidence in assessing and managing psychological symptoms.79
The questionnaires most often used to assess anxiety symptoms in COPD, eg, the Hospital Anxiety and Depression Scale (HADS)80 and the Hamilton Rating Scale for Anxiety (HAM-A),81 do not include questions about the internal (eg, fear of dying), external (eg, unsafe environments), and behavioral (eg, fear-based avoidance) factors that appeared to be characteristic of anxiety in patients with COPD. Even disease-specific anxiety questionnaires like the COPD-Anxiety-Questionnaire (CAF)82 and the Anxiety Inventory for Respiratory Disease (AIR)83 do not contain questions assessing the central aspects of COPD-related anxiety that were described in our study. If patients are not questioned on fear-inducing and difficult to cope with topics, the severity of anxiety may be underestimated or unidentified in clinical settings. This could potentially explain why the estimated prevalence of anxiety levels in COPD varies markedly across studies and should prompt a reconsideration of the sensitivity of existing questionnaires to identify aspects of anxiety in patients with COPD. Not addressing COPD-related aspects of anxiety leads to poorer identification, and leaves patients to deal with anxiety themselves.
When interpreting the results of our study, it is important to bear in mind that experiencing COPD-related anxiety does not necessarily mean fulfilling the criteria of an anxiety disorder. Theoretically, not all patients with COPD and a comorbid anxiety disorder will experience COPD-related anxiety and vice versa. Furthermore, it is also important to differentiate COPD-related anxiety from episodic, passing experiences of anxiety that can be normal reactions to events such as diagnosis or symptom exacerbation.84 According to the conceptual model of our study, COPD-related anxiety involves persistent anxiety symptoms that are related to an individual’s processing of COPD-related internal and external factors, as well as accompanying fear-induced behavior, such as avoidance of physical activity, social distancing, and seeking hospital intervention instead of self-management. Consequently, COPD-related anxiety should be described neither as a momentary feeling nor as a mental disorder, but as a biopsychosocial pattern that develops over time and reduces an individual’s functional capacity, quality of life, and ability to cope with the illness. Additionally, comorbid physical diseases and specific life circumstances that are not directly related to COPD symptoms could also impact patients’ experience of anxiety, and it may be difficult for the individual patient and the clinician to differentiate between anxiety symptoms emerging from one or the other condition. Participants in the included studies of the present review were recruited on the basis of their COPD diagnosis, but a certain proportion may also be diagnosed with other diseases, which may have influenced their narrative. It is therefore important to differentiate between COPD-related anxiety and COPD-specific anxiety, the latter being exclusively caused by or associated with COPD diagnosis. Future studies directly comparing anxiety narratives in COPD and other physical diseases are needed with the purpose of expanding our knowledge of COPD-specific anxiety.
Strengths and Limitations
The present review was protocol-based and systematically adhered to existing guidelines for review and analysis of qualitative studies. It represents one of the first attempts to systematically review the existing literature on COPD-related anxiety from the patients’ perspective and to propose a conceptual model of COPD-related anxiety.
A number of limitations should be considered when interpreting the results of the study. First, the results were based on study samples that were heterogeneous in terms of participants’ sociodemographic characteristics and symptom level as well as the geographical location where studies were conducted. Based on the present study, it is not possible to draw conclusions in terms of potential variation in the experience of COPD-related anxiety related to age, gender, symptom severity, or cultural norms. Second, caregivers’ and health-care providers’ experience of COPD-related anxiety was not included in the present review. Their observations are highly relevant in fully understanding the concept of COPD-related anxiety and should be explored in future studies. Third, exploring COPD-related anxiety was not the primary focus of all of the included studies; hence, patients were not asked specifically to describe their experience of COPD-related anxiety. With the purpose of studying the subjective specificity of the concept in the future, there is a need for studies directly prompting patients to describe their experiences with COPD-related anxiety and asking them to differentiate between COPD-related fears, fears associated with comorbid diseases, and other types of fears.
Conclusion
The present review synthesized the results of existing qualitative studies of COPD-related anxiety from the patients’ perspective. According to our proposed conceptual model, patients’ experiences of COPD-related anxiety are initially triggered by specific events in the illness trajectory and thereafter maintained by COPD-related internal, external, and behavioral factors. The present study represents one of the first steps towards understanding the complexity of COPD-related anxiety. In the future, there is a need for work that aims to 1) improve the identification of anxiety symptoms in patients with COPD, 2) differentiate between subclinical anxiety patterns and comorbid anxiety disorders, and 3) develop and deliver targeted treatment. Future research should focus on the development of a COPD-specific anxiety questionnaire for research and clinical purposes and could preferably draw on the conceptual model proposed in the present study with the purpose of assessing domains of COPD-related anxiety that are in line with patients’ experiences.
Acknowledgments
The authors wish to thank Allan Klitgaard Staal, Andreas Arnholdt Pedersen, Kristina Kock Hansen, Louise Muxoll Grønhaug, and Melina Gade Sikjær for their valuable comments and suggestions along the way.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Innovation Fund at Lillebaelt Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Willgoss TG, Yohannes AM. Anxiety disorders in patients with COPD: a systematic review. Respir Care. 2013;58(5):858–866. doi:10.4187/respcare.01862
2. Pumar MI, Gray CR, Walsh JR, Yang IA, Rolls TA, Ward DL. Anxiety and depression: important psychological comorbidities of COPD. J Thorac Dis. 2014;6(11):1615–1631. doi:10.3978/j.issn.2072-1439.2014.09.28
3. Triest FJJ, Franssen FME, Reynaert N, et al. Disease-specific comorbidity clusters in COPD and accelerated aging. J Clin Med. 2019;8(4). doi:10.3390/jcm8040511
4. Yohannes AM, Lavoie KL. Overseeing anxiety and depression in patients with physical illness. Chest. 2013;144(3):726–728. doi:10.1378/chest.13-0511
5. Yohannes AM, Willgoss TG, Baldwin RC, Connolly MJ. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: prevalence, relevance, clinical implications and management principles. Int J Geriatr Psychiatry. 2010;25(12):1209–1221. doi:10.1002/gps.2463
6. Larsen CH, Bendstrup E, Neergaard MA. Screening tools for depression and anxiety in patients with chronic obstructive pulmonary disease–a systematic review. COPD J Chronic Obstr Pulm Dis. 2021;18(6):683–689. doi:10.1080/15412555.2021.1972091
7. Gutiérrez-García AG, Contreras CM. Anxiety: an adaptive Emotion. In: Durbano F, editor. New Insights into Anxiety Disorders. InTech; 2013.
8. Dowson C, Kuijer R, Mulder R. Anxiety and self-management behaviour in chronic obstructive pulmonary disease: what has been learned? Chron Respir Dis. 2004;1(4):213–220. doi:10.1191/1479972304cd032rs
9. Hanania NA, O’Donnell DE. Activity-related dyspnea in chronic obstructive pulmonary disease: physical and psychological consequences, unmet needs, and future directions. Int J COPD. 2019;14:1127–1138. doi:10.2147/COPD.S188141
10. Stoeckel MC, Esser RW, Gamer M, Büchel C, von Leupoldt A. Dyspnea catastrophizing and neural activations during the anticipation and perception of dyspnea. Psychophysiology. 2018;55(4):e13004. doi:10.1111/psyp.13004
11. Willgoss T, Yohannes A, Goldbart J, Fatoye F. COPD and anxiety: its impact on patients’ lives. Nurs Times. 2011;107(15–16):16–19.
12. Gershon AS, Dolmage TE, Stephenson A, Jackson B. Chronic obstructive pulmonary disease and socioeconomic status: a systematic review. COPD J Chronic Obstr Pulm Dis. 2012;9(3):216–226. doi:10.3109/15412555.2011.648030
13. GOLD Global Initiative for Chronic Obstructive Pulmonary Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2023.
14. von Leupoldt A, Janssens T. Could targeting disease specific fear and anxiety improve COPD outcomes? Expert Rev Respir Med. 2016;10(8):835–837. doi:10.1080/1747634820161198697
15. Page MJ, McKenzie JE, Bossuyt PM, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. 2021;134:103–112. doi:10.1016/j.jclinepi.2021.02.003
16. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45. doi:10.1186/1471-2288-8-45
17. Munthe-Kaas H, Bohren MA, Glenton C, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings—paper 3: how to assess methodological limitations. Implement Sci. 2018;13(S1):9. doi:10.1186/s13012-017-0690-9
18. Kessler R, Ståhl E, Vogelmeier C, et al. Patient understanding, detection, and experience of COPD exacerbations: an observational, interview-based study. Chest. 2006;130:133–142.
19. Ekdahl A, Söderberg S, Rising-Holmström M. Living with an ever-present breathlessness: women’s experiences of living with chronic obstructive pulmonary disease stage III or IV. Scand J Caring Sci. 2022;36:1064–1073. doi:10.1111/scs.12998
20. Panos RJ, Krywkowski-Mohn SM, Sherman SN, Lach LA. Patient reported determinants of health: a qualitative analysis of veterans with chronic obstructive pulmonary disease. COPD J Chronic Obstr Pulm Dis. 2013;10(3):333–347. doi:10.3109/15412555.2012.752805
21. Bakthavatsalu B, Walshe C, Simpson J. The experience of hospitalization in people with advanced chronic obstructive pulmonary disease: a qualitative, phenomenological study. Chronic Illn. 2023;19(2):339–353. doi:10.1177/17423953211073580
22. Skär L, Borg C, Emtner M, Ekström M. Thoughts on the end of life in patients with oxygen-dependent chronic obstructive pulmonary disease: a qualitative interview study. Nurs Open. 2023;10:2158–2164. doi:10.1002/nop2.1463
23. Zanolari D, Händler-Schuster D, Clarenbach C, Schmid-Mohler G. A qualitative study of the sources of chronic obstructive pulmonary disease-related emotional distress. Chron Respir Dis. 2023;20:1–10. doi:10.1177/14799731231163873
24. Lin T, Shune S. The mind–body–breath link during oral intake in chronic obstructive pulmonary disease: a grounded theory analysis. Dysphagia. 2023;38:367–378. doi:10.1007/s00455-022-10473-x
25. Gilliam EA, Kilgore KL, Liu Y, et al. Managing the experience of breathlessness with Tai Chi: a qualitative analysis from a randomized controlled trial in COPD. Respir Med. 2021;184:106463.
26. Jørgensen L, Eikhof KD, Jensen MH, Størkersen ML, Andreasen J. Patients’ experiences following acute admission due to COPD exacerbation. A qualitative interview study. Int Emerg Nurs. 2021;58(July):10–14. doi:10.1016/j.ienj.2021.101054
27. Askey-Jones R, Hailes K. Exploring the benefits of a psychoeducation session for patients with chronic obstructive pulmonary disease (COPD) and co-morbid depression and/or anxiety. Ment Heal Pract. 2020;4:21–29. doi:10.7748/mhp.2020.e1435
28. Lundell S, Wadell K, Wiklund M, Tistad M. Enhancing confidence and coping with stigma in an ambiguous interaction with primary care: a qualitative study of people with COPD. J Chronic Obstr Pulm Dis. 2020;17(5):533–542. doi:10.1080/15412555.2020.1824217
29. Rubio M. Patient perceptions of life-limiting chronic obstructive pulmonary disease. J Nurse Pract. 2019;15(2):183–188. doi:10.1016/j.nurpra.2018.10.005
30. Sigurgeirsdottir J, Halldorsdottir S, Arnardottir RH, Gudmundsson G, Bjornsson EH. COPD patients’ experiences, self-reported needs, and needs-driven strategies to cope with self-management. Int J COPD. 2019;14:1033–1043. doi:10.2147/COPD.S201068
31. Slevin P, Kessie T, Cullen J, Butler MW, Donnelly SC, Caulfield B. Exploring the potential benefits of digital health technology for the management of COPD: a qualitative study of patient perceptions. ERJ Open Res. 2019;5(2):00239–02018. doi:10.1183/23120541.00239-2018
32. Wu RC, Ginsburg S, Son T, Gershon AS. Using wearables and self-management apps in patients with COPD: a qualitative study. ERJ Open Res. 2019;5:0036–2019. doi:10.1183/23120541.00036-2019
33. Jarab A, Alefishat E, Mukattash T, Alzoubi K, Pinto S. Patients’ perspective of the impact of COPD on quality of life: a focus group study for patients with COPD. Int J Clin Pharm. 2018;40(3):573–579. doi:10.1007/s11096-018-0614-z
34. Østergaard EB, Sritharan SS, Kristiansen AD, Thomsen PM, Løkke A. Barriers and motivational factors towards physical activity in daily life living with COPD–an interview based pilot study. Eur Clin Respir J. 2018;5(1):1484654. doi:10.1080/20018525.2018.1484654
35. Luckett T, Phillips J, Johnson M, et al. Insights from Australians with respiratory disease living in the community with experience of self-managing through an emergency department “near miss” for breathlessness: a strengths-based qualitative study. BMJ Open. 2017;7(12):1–10. doi:10.1136/bmjopen-2017-017536
36. Bove DG, Midtgaard J, Kaldan G, Overgaard D, Lomborg K. Home-based COPD psychoeducation: a qualitative study of the patients’ experiences. J Psychosom Res. 2017;98:71–77. doi:10.1016/j.jpsychores.2017.05.013
37. Korpershoek Y, Vervoort SC, Nijssen LI, Trappenburg JC, Schuurmans MJ. Factors influencing exacerbation-related self-management in patients with COPD: a qualitative study. COPD. 2016;11:2977–2990.
38. Halpin D, Hyland M, Blake S, et al. Understanding fear and anxiety in patients at the time of an exacerbation of chronic obstructive pulmonary disease: a qualitative study. JRSM Open. 2015;6(12):205427041561454. doi:10.1177/2054270415614543
39. Nordvall Strömberg P, Fjellman-Wiklund A, Wadell K. Enhanced information regarding exercise training as treatment is needed. An interview study in patients with chronic obstructive pulmonary disease. Disabil Rehabil. 2015;37(16):1424–1430. doi:10.3109/09638288.2014.972584
40. Gabriel R, Figueiredo D, Jácome C, Cruz J, Margues A. Day-to-day living with severe chronic obstructive pulmonary disease: towards a family-based approach to the illness impacts. Psychol Health. 2014;29(8):967–983.
41. Kauffman KS, Doede M, Diaz-Abad M, et al. Experience of insomnia, symptom attribution and treatment preferences in individuals with moderate to severe COPD: a qualitative study. Patient Prefer Adherence. 2014;8:1699–1704. doi:10.2147/PPA.S71666
42. Schroedl CJ, Yount SE, Szmuilowicz E, Hutchison PJ, Rosenberg SR, Kalhan R. A qualitative study of unmet healthcare needs in chronic obstructive pulmonary disease: a potential role for specialist palliative care? Ann Am Thorac Soc. 2014;11(9):1433–1438. doi:10.1513/AnnalsATS.201404-155BC
43. Strang S, Ekberg-Jansson A, Henoch I. Experience of anxiety among patients with severe COPD: a qualitative, in-depth interview study. Palliat Support Care. 2014;12(6):465–472. doi:10.1017/S1478951513000369
44. Hayle C, Coventry PA, Gomm S, Caress AL. Understanding the experience of patients with chronic obstructive pulmonary disease who access specialist palliative care: a qualitative study. Palliat Med. 2013;27(9):861–868. doi:10.1177/0269216313486719
45. Ellison L, Gask L, Bakerly ND, Roberts J. Meeting the mental health needs of people with chronic obstructive pulmonary disease: a qualitative study. Chronic Illn. 2012;8(4):308–320. doi:10.1177/1742395312449754
46. Willgoss TG, Yohannes AM, Goldbart J, Fatoye F. “Everything was spiraling out of control”: experiences of anxiety in people with chronic obstructive pulmonary disease. Hear Lung J Acute Crit Care. 2012;41(6):562–571. doi:10.1016/j.hrtlng.2012.07.003
47. Wortz K, Cade A, Menard JR, et al. A qualitative study of patients’ goals and expectations for self-management of COPD. Prim Care Respir J. 2012;21(4):384–391. doi:10.4104/pcrj.2012.00070
48. Sossai K, Gray M, Tanner B. Living with chronic obstructive pulmonary disease: experiences in northern regional Australia. Int J Ther Rehabil. 2011;18(11):631–641. doi:10.12968/ijtr.2011.18.11.631
49. Lewis R, Cramp F. Facilitators and barriers to exercise maintenance in chronic obstructive pulmonary disease: patient views. Physiother Irel. 2010;31:19–24.
50. Lohne V, Heer HCD, Andersen M, Miaskowski C, Kongerud J, Rustøen T. Qualitative study of pain of patients with chronic obstructive pulmonary disease. Hear Lung J Acute Crit Care. 2010;39(3):226–234. doi:10.1016/j.hrtlng.2009.08.002
51. Torheim H, Gjengedal E. How to cope with the mask? Experiences of mask treatment in patients with acute chronic obstructive pulmonary disease-exacerbations. Scand J Caring Sci. 2010;24(3):499–506. doi:10.1111/j.1471-6712.2009.00740.x
52. Clancy K, Hallet C, Caress A. The meaning of living with chronic obstructive pulmonary disease. J Nurs Healthc Chronic Illn. 2009;1(1):78–86. doi:10.1111/J.1365-2702.2008.01005.X
53. Gardiner C, Gott M, Small N, et al. Living with advanced chronic obstructive pulmonary disease: patients concerns regarding death and dying. Palliat Med. 2009;23(8):691–697. doi:10.1177/0269216309107003
54. Harris D, Hayter M, Allender S. Improving the uptake of pulmonary rehabilitation in patients with COPD: qualitative study of experiences and attitudes. Br J Gen Pract. 2008;58:703–710. doi:10.3399/bjgp08X342363
55. Barnett M. Chronic obstructive pulmonary disease: a phenomenological study of patients’ experiences. J Clin Nurs. 2005;14(7):805–812. doi:10.1111/j.1365-2702.2005.01125.x
56. Jones RCM, Hyland ME, Hanney K, Erwin J. A qualitative study of compliance with medication and lifestyle modification in Chronic Obstructive Pulmonary Disease (COPD). Prim Care Respir J. 2004;13:149–154. doi:10.1016/j.pcrj.2004.05.006
57. Jeng C, Tsao L, Chiung-Hua H, Chang P. Experiences of daily activities within two weeks after hospital discharge among Taiwanese elderly patients with chronic obstructive pulmonary disease. J Nurs Res. 2002;10(3):168–176.
58. Turner J, Kelly B. Emotional dimensions of chronic disease. West J Med. 2000;172:124–128.
59. Benkel I, Arnby M, Molander U. Living with a chronic disease: a quantitative study of the views of patients with a chronic disease on the change in their life situation. SAGE Open Med. 2020;8:1–7. doi:10.1177/2050312120910350
60. Wan M, Luo X, Wang J, et al. The impact on quality of life from informing diagnosis in patients with cancer: a systematic review and meta-analysis. BMC Cancer. 2020;20:618. doi:10.1186/s12885-020-07096-6
61. Lastrucci V, D’Arienzo S, Collini F, et al. Diagnosis-related differences in the quality of end-of-life care: a comparison between cancer and non-cancer patients. PLoS One. 2018;13(9):e0204458. doi:10.1371/journal.pone.0204458
62. Plaufcan MR, Wamboldt FS, Holm KE. Behavioral and characterological self-blame in chronic obstructive pulmonary disease. J Psychosom Res. 2012;72(1):78–83. doi:10.1016/j.jpsychores.2011.10.004
63. Løkke A, Hilberg O, Tønnesen P, Ibsen R, Kjellberg J, Jennum P. Direct and indirect economic and health consequences of COPD in Denmark: a national register-based study: 1998–2010. BMJ Open. 2014;4(1):e004069. doi:10.1136/bmjopen-2013-004069
64. Livermore N, Sharpe L, McKenzie D. Catastrophic interpretations and anxiety sensitivity as predictors of panic-spectrum psychopathology in chronic obstructive pulmonary disease. J Psychosom Res. 2012;72(5):388–392. doi:10.1016/j.jpsychores.2012.02.001
65. Von Leupoldt A, Mertz C, Kegat S, Burmester S, Dahme B. The impact of emotions on the sensory and affective dimension of perceived dyspnea. Psychophysiology. 2006;43(4):382–386. doi:10.1111/j.1469-8986.2006.00415.x
66. Solomon BK, Wilson KG, Henderson PR, Poulin PA, Kowal J, McKim DA. A breathlessness catastrophizing scale for chronic obstructive pulmonary disease. J Psychosom Res. 2015;79(1):62–68. doi:10.1016/j.jpsychores.2014.11.020
67. Sutton K, Cooper M, Pimm J, Wallace L. Anxiety in chronic obstructive pulmonary disease: the role of illness specific catastrophic thoughts. Cognit Ther Res. 1999;23(6):573–585.
68. Curtis JR, Wenrich MD, Carline JD, Shannon SE, Ambrozy DM, Ramsey PG. Patients’ perspectives on physician skill in end-of-life care: differences between patients With COPD, cancer, and AIDS. Chest. 2002;122:356–362.
69. Spathis A, Booth S. End of life care in chronic obstructive pulmonary disease: in search of a good death. Int J COPD. 2008;3:11–29. doi:10.2147/copd.s698
70. Murray SA, Kendall M, Boyd K, Sheikh A. Illness trajectories and palliative care. BMJ. 2005;330:1007–1011. doi:10.1136/bmj.330.7498.1007
71. Curtis JR. Palliative and end-of-life care for patients with severe COPD. Eur Respir J. 2008;32(3):796–803. doi:10.1183/09031936.00126107
72. Ouellette DR, Lavoie KL. Recognition, diagnosis, and treatment of cognitive and psychiatric disorders in patients with COPD. Int J COPD. 2017;12:639–650.
73. Coventry PA, Hind D. Comprehensive pulmonary rehabilitation for anxiety and depression in adults with chronic obstructive pulmonary disease: systematic review and meta-analysis. J Psychosom Res. 2007;63(5):551–565. doi:10.1016/j.jpsychores.2007.08.002
74. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2015(2):1–209.
75. Farver-Vestergaard I, Johannesen G, Ter BL. Occupational therapy, nutritional modulation and psychological support. In: Holland A, Dal Corso S, Spruit M, editors. Pulmonary Rehabilitation. European Respiratory Society; 2021:83–98.
76. Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011;8(2):89–99. doi:10.1177/1479972310393756
77. McCarron EP, Bailey M, Leonard B, McManus TE. Improving the uptake: barriers and facilitators to pulmonary rehabilitation. Clin Respir J. 2019;13(10):624–629. doi:10.1111/crj.13068
78. Heslop-Marshall K, Burns G. The role of cognitive behavioural therapy in living well with COPD. Breathe. 2019;15(2):95–97. doi:10.1183/20734735.0119-2019
79. Hardy S, Smart D, Scanlan M, Rogers S. Integrating psychological screening into reviews of patients with COPD. Br J Nurs. 2014;23(15):832–836. doi:10.12968/bjon.2014.23.15.832
80. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67:361–370.
81. Thompson E. Hamilton rating scale for anxiety (HAM-A). Occup Med. 2015;65(7):601. doi:10.1093/occmed/kqv054
82. Kühl K, Kuhn C, Kenn K, Rief W. Der COPD-Angst-Fragebogen (CAF): ein neues Instrument zur Erfassung krankheitsspezifi scher Ä ngste bei COPD-Patienten [The COPD-Anxiety-Questionnaire (CAF): a new instrument to assess illness specific anxiety in COPD patients]. Psychother Psychosom Med Psychol. 2011;61(1):e1–e9.
83. Willgoss TG, Goldbart J, Fatoye F, Yohannes AM. The development and validation of the anxiety inventory for respiratory disease. Chest. 2013;144(5):1587–1596. doi:10.1378/chest.13-0168
84. Volpato E, Farver-Vestergaard I, Brighton LJ, et al. Nonpharmacological management of psychological distress in people with COPD. Eur Respir Rev. 2023;32:220170. doi:10.1183/16000617.0170-2022
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Perceptions, Level of Government Trust, and Psychological Distress During COVID-19 Pandemic in Taiwan
Chang PY, Shih FY, Lee MB, Lin CF, Lyu SY
Psychology Research and Behavior Management 2022, 15:3313-3327
Published Date: 15 November 2022
Association Between Loneliness, Premenstrual Symptoms, and Other Factors During the COVID-19 Pandemic: A Cross-Sectional Study with Japanese High School Students
Takeda T, Yoshimi K, Kai S, Inoue F
International Journal of Women's Health 2023, 15:655-664
Published Date: 26 April 2023
Assessing the Smallest Detectable Change of the Kessler Psychological Distress Scale Score in an Adult Population in Japan
Uchida H, Kuroiwa C, Ohki S, Takahashi K, Tsuchiya K, Kikuchi S, Hirao K
Psychology Research and Behavior Management 2023, 16:2647-2654
Published Date: 13 July 2023
Depression, Anxiety, Stress, Associated with Lichen Planus in Jordanian Women and the Impact on Their Quality of Life
Alnazly E, Absy N, Sweileh I
International Journal of Women's Health 2023, 15:1883-1892
Published Date: 27 November 2023
A Phenomenological Qualitative Study of Primary Informal Caregiver of Chinese Patients with Advanced Stage COPD: An In-Depth Exploration of Experiences and Needs
Ren X, Li F, Gao T, Xu X, Sun L, Liu S, Liu Y, Wang F
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:514685
Published Date: 20 March 2026