Back to Journals » Psychology Research and Behavior Management » Volume 15
Risk Perceptions, Level of Government Trust, and Psychological Distress During COVID-19 Pandemic in Taiwan
Authors Chang PY ![]() , Shih FY, Lee MB
, Shih FY, Lee MB ![]() , Lin CF, Lyu SY
, Lin CF, Lyu SY ![]()
Received 25 July 2022
Accepted for publication 1 October 2022
Published 15 November 2022 Volume 2022:15 Pages 3313—3327
DOI https://doi.org/10.2147/PRBM.S375722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Po-Ya Chang,1 Fuh-Yuan Shih,2 Ming-Been Lee,3 Ching-Feng Lin,4– 6 Shu-Yu Lyu1
1Department of Leisure Industry and Health Promotion, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan; 2Department of Emergency Medicine, National Taiwan University Hospital, Taipei, Taiwan; 3Department of Psychiatry, National Taiwan University College of Medicine and Hospital, Taipei, Taiwan; 4Keelung Hospital, Ministry of Health and Welfare, Keelung, Taiwan; 5Department of Health Care Management, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan; 6School of Health Care Administration, Taipei Medical University, Taipei, Taiwan
Correspondence: Ching-Feng Lin, Keelung Hospital, Ministry of Health and Welfare, Keelung, Taiwan, Email [email protected]
Purpose: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is spreading worldwide, causing mental health concerns among people. People’s perceptions of the disease affect their psychological adaptation and health outcomes. In this study, we present people’s perceptions of coronavirus disease 2019 (COVID-19), level of government trust, and their psychological distress during the pandemic for examining the impact of peoples’ COVID-19 perceptions on their mental health.
Patients and Methods: This cross-sectional study was conducted through a telephone survey in Taiwan in April 2020. Participants were randomly selected for telephone screening using a computer-assisted telephone interviewer system. A total of 1098 participants aged more than 20 years participated in the survey.
Results: The mean age of participants was 47.7 ± 16.4 years. After controlling for covariates, participants who were worried about contracting COVID-19, those who believed that they had a chance of being infected with COVID-19, those who were reluctant to visit the hospital for fear of contracting the virus, those who felt that the pandemic had affected their daily life, and those with low levels of trust in the government’s capacity to manage the pandemic had anxiety, hostility, depression, interpersonal sensitivity/inferiority, and psychological symptoms.
Conclusion: People’s perception of COVID-19 and public’s trust in the government’s ability to respond to the pandemic are related to psychological distress. Although the Taiwanese government may have undertaken effective epidemic control measures to address with the COVID-19 pandemic, this crisis may have still caused mental health problems in the general population. Health professionals and policy makers should pay more attention to high-risk groups among those at risk for developing mental health problems.
Keywords: COVID-19, perceptions, psychological distress, mental health, fears, trust, economic crisis
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel pandemic that has spread worldwide, and people are gradually becoming aware of this disease.1 The symptoms of coronavirus disease 2019 (COVID-19) are fever, dry cough, fatigue, myalgia, slight dyspnea, and headache. Some patients in critical condition may experience pneumonia, respiratory failure, shock, or multiorgan failure.2–4 By September 2022, the number of global COVID-19 cases had reached 606 million, and COVID-19 had caused nearly 6.49 million deaths.5 The number of people affected by and dying from COVID-19 is rising rapidly, and this pandemic has had a negative impact on people, the global impact of the crisis is comparable to that of war.6
A public health emergency may negatively affect the health and safety of individuals and communities, and at a personal level, may lead to a sense of insecurity, confusion, and emotional isolation. At the society level, it may cause economic collapse, unemployment, lockdown, school closure, lack of medical resources, and insufficiency of daily necessities, consequently causing distress and psychiatric issues among people.7 Moreover, continuous communications by governmental or nongovernmental sources through social media; limited knowledge; or information overload regarding COVID-19 can cause mental health problems.8 The World Health Organization (WHO) has pointed out that enormous misinformation and gossips in media may cause the potential symptoms of stigma, fear, and anxiety.9
Those confirmed and suspected of having COVID-19 may suffer from loneliness, anxiety, depression, insomnia, or despair,10,11 and more likely to increase risk of suicide.12,13 The confinement due to the COVID-19 pandemic related to suicide and negative impact on mental health.14–16 However, this problem arises even after the end of lock-down. Ambrosetti et al found that there was a statistically significant increase in suicidal behavior after lockdown measures were lifted compared to during lockdown.17 During the COVID-19 pandemic, loneliness, psychosocial crises, and well-being decreased have become more common in the general population, the effects of which may be predisposing factors for suicide.18 Patients with COVID-19 may have physical symptoms, psychosocial stressors, and post-traumatic stress symptoms, therefore, the COVID-19 survivors especially individuals with severe COVID-19 may be at high risk of suicidal.19 Individuals suspected of having COVID-19 are unsure of their health and usually have symptoms of obsessive-compulsive disorder, such as repeatedly checking their body temperature and sanitizing their hands.1,20,21
Previous studies have examined the perception of COVID-19 and the mental health impact of the COVID-19.22–29 Qi et al estimated the relationship between threatened perception types and mental status among pregnant women.29 An online survey in China suggests that risk perception is a key factor related to mental health during the public health crisis.27 Han et al also demonstrated that perception risk of COVID-19 was significantly associated with emotion and subsequent mental health.30 However, these studies only focus on risk perceptions or specific populations. In this regard, our research evaluated psychological distress among Taiwanese during the COVID-19 epidemic, and examined their perceptions, fears, impact on daily life of the COVID-19, and public trust in government on their mental health.
Materials and Methods
Sampling Design and Participants
This cross-sectional study was conducted through a telephone survey in Taiwan in April 2020. People over the age of 20 living in Taiwan were the inclusion criteria for this study. Participants were randomly selected for telephone screening using a computer-assisted telephone interviewer (CATI) system. For sample selection, this study used random country- and city-stratified proportional sampling and random dialing of noninstitutionalized adults living in private households in Taiwan. According to the estimate of 19 million people more than 20 years old living in Taiwan in 2020, a representative sample size of at least 1068 was required, with a sampling error of 0.03. To ensure representativeness, after the respondent completed the survey, the ranking technology was used to weigh and adjust gender and age. A total of 1098 participants aged over 20 years participated in the survey.
Structured questionnaires were used to determine the participants’ knowledge and perceptions of COVID-19 and their psychological distress. To reduce nonsampling errors caused by human error and to ensure data quality, interviewer training will be conducted on the content of the questionnaire before the formal telephone survey. All information was collected by well-trained interviewers, and a field pretest was conducted to evaluate the internal consistency and comprehensibility of the interview. The interviewer sat in front of the computer for a telephone interview and entered the answers directly into the computer. The interview procedure was simple. To prevent sampling bias, in case of unanswered phone calls, the interviewer was required to wait for the phone to ring for 30 seconds before hanging up the call and was required to make at least three attempts at different time points. To reduce allocation bias, researchers often compared the demographic distributions of the respondents to the corresponding distribution of the population of Taiwan during the interview period.
Ethical Considerations
The study was conducted through a telephone survey. This telephone questionnaire is anonymous, therefore, there is no information such as names, addresses, or personal information will be asked during the interview process. Each personal data of the case is strictly protected, and the survey data is for descriptive statistical analysis and research use. No personal data will be released, and all personnel who collected data will also be responsible for confidentiality. Generally, telephone interviews require only the verbal consent of the interviewee. As soon as people answered the phone, the interviewer introduced themselves and told the respondent the purpose of the call, and then asked the respondent if they would like to be interviewed. In this survey, verbal consent was obtained from all participants. This study and use verbal consent to conduct this survey was approved by the Institutional Review Board of Taipei Hospital, Ministry of Health and Welfare (No. TH-IRB-0020-0005) and adhered to the ethical principles of the Declaration of Helsinki.
Measures
The study was implemented using a structured questionnaire that included demographic information, and investigated perceptions of COVID-19 and psychological distress. Information on sociodemographic characteristics including age, sex, education level, residential area, and sources of information on COVID-19 was collected. The questionnaire had six items on perceptions, namely (1) “How would you rate the degree of severity regarding COVID-19?” (Answer: “extremely/very/slightly/not at all”); (2) “Are you worried about contracting COVID-19 in Taiwan?” (Answer: “extremely/very/slightly/not at all”); (3) “Is it possible for you to be infected with COVID-19?” (Answer: “very probable/somewhat probable/neutral/somewhat improbable/not probable”); (4) “Are you scared to visit the hospital during the COVID-19 pandemic?” (Answer: “extremely/ very/ slightly/ not at all”); (5) “Does the COVID-19 pandemic affect your daily life?” (Answer: “major affect/moderate affect/no affect”); (6) “Do you have confidence in the government’s ability to manage the COVID-19 pandemic?” (Answer: “completely confident/fairly confident/slightly confident/not confident at all”). The questionnaire was validated in terms of content validity through expert judgement.
This study used the 5-item Brief Symptom Rating Scale (BSRS-5) to measure psychological distress experienced by participants in the past week. The BSRS-5 is derived from the 50-item Brief Symptom Rating Scale, which measures anxiety, depression, hostility, interpersonal sensitivity/inferiority, and insomnia.31 Each item is scored on a 5-point Likert-style scale, with 0 indicating “not at all”, 1 indicating “a little bit”, 2 indicating “moderately”, 3 indicating “quite a bit”, and 4 indicating “extremely.” A cut-off total score of BSRS-5 of ≥6 indicates psychological morbidity; this score is determined through receiver operating characteristic curve analysis.32 The BSRS-5 is a global measurement and case-finding screening instrument with high reliability and validity.31,33 It is widely used for evaluation in psychiatric and nonpsychiatric medical settings.34,35
Study Variables and Definitions
This study divided people’s perception to COVID-19 into two categories based on the following criteria: (1) “How would you rate the degree of severity regarding COVID-19?” was divided into “mild (slightly and not at all)” and “severe (extremely and very)”; (2) “Are you worried about contracting COVID-19 in Taiwan?” was divided into “no (slightly and not at all)” and “yes (extremely and very)”; (3) “Is it possible for you to be infected with COVID-19?” was divided into “no (neutral, somewhat improbable, and not probable)” and “yes (very probable and somewhat probable)”; (4) “Are you scared to visit the hospital during the COVID-19 pandemic?” was divided into “no (slightly and not at all)” and “yes (extremely and very)”; (5) “Does the COVID-19 pandemic affect your daily life?” was divided into “no (no affect)” and “yes (major affect and moderate affect)”; (6) “Do you have confidence in the government’s ability to manage the COVID-19 pandemic?” was divided into “no (slightly confident and not confident at all)” and “yes (completely confident and fairly confident).”
The responses for the 5-item psychological distress questionnaire (anxiety, depression, hostility, interpersonal sensitivity/ inferiority, and insomnia) were dichotomized as “no” versus “yes” based on the following criteria: an item score of 0 indicated no psychological distress, and scores greater than 1 indicated having psychological distress. Total BSRS-5 score <5 indicated no psychological morbidity, and the total BSRS-5 score ≥6 indicated the presence of psychological morbidity.
Statistical Analysis
Participant characteristics were analyzed based on descriptive statistics. The chi-square test was used to determine significant differences between participants with and without psychological distress, including anxiety, depression, hostility, interpersonal sensitivity/inferiority, and insomnia. After adjusting for age, sex, education level, and residential area, we used multiple logistic regression to identify statistically significant associations between perceptions and psychological distress. Odds ratio (OR) with 95% confidence interval (CI) was calculated for each independent variable in multiple logistic regression. The results were considered statistically significant if p values were less than 0.05. All analyses and calculations were performed using SPSS Version 18 (SPSS Inc., Chicago, IL, USA).
Results
Table 1 lists the baseline demographics of the study participants. The mean age of participants was 47.7 ± 16.4 years, and most of them (48.1%) were aged 20–45 years. The majority (51.6%) of participants were female, 42.4% had studied up to junior college or above, and 69.5% lived in urban areas. With regard to the information sources of COVID-19, 74.1% of participants had received COVID-19-related information from the television. The prevalence of psychological distress among participants was as follows: 14.9% of them had insomnia, 22.4% had anxiety, 14% experienced hostility, 16.1% had depression, 6.1% experienced interpersonal sensitivity/inferiority, 5.3% had psychological morbidity, and 1% had suicidal ideation.
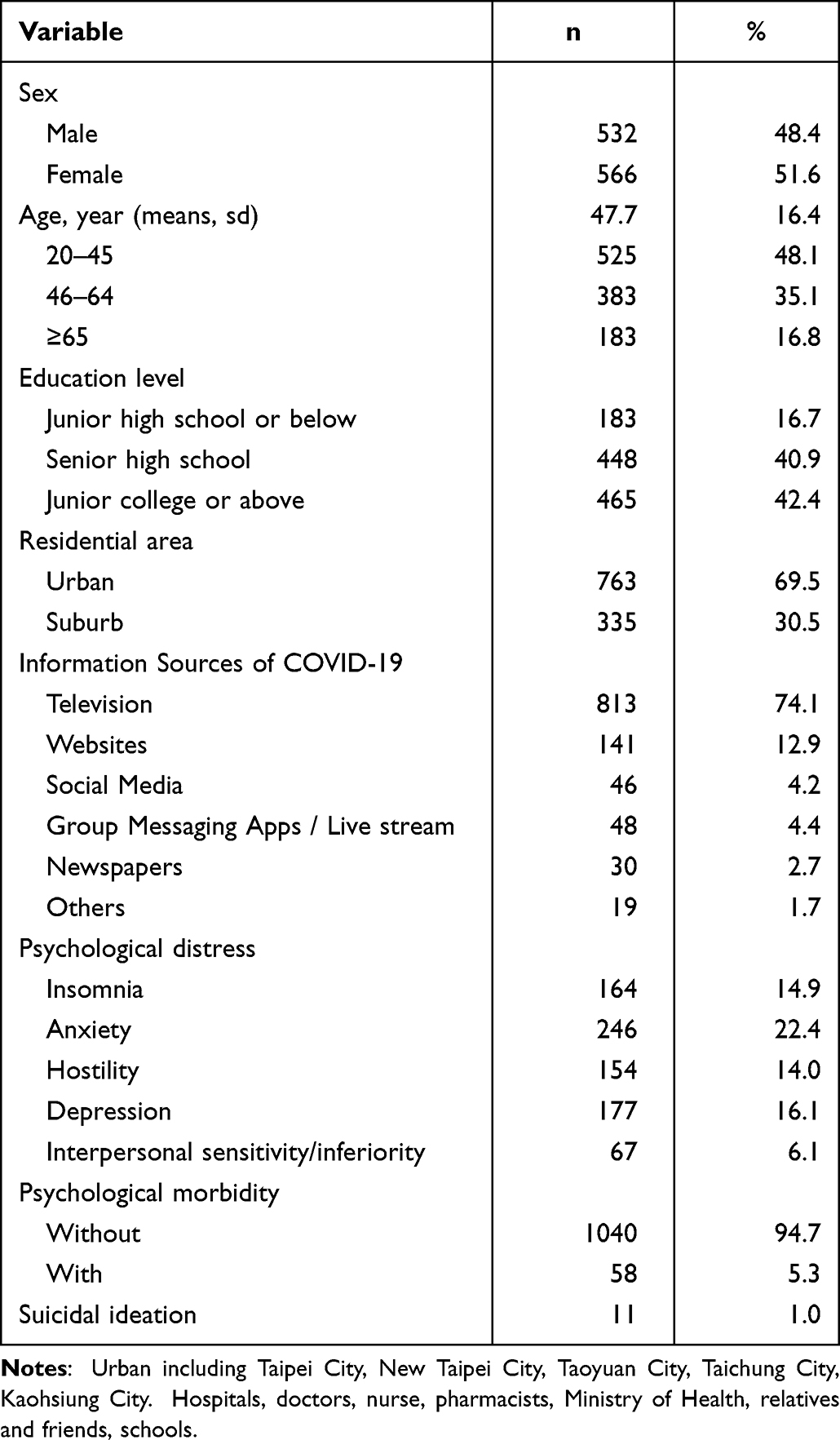 |
Table 1 The Demographic of Participants (n=1098) |
With regard to perceptions of COVID-19, the majority of participants believed that COVID-19 infection was serious. Nearly 80% of participants were worried about contracting COVID-19 (31.6% were “extremely worried”, and 47.4% were “very worried”), and about half of the participants believed that they had a chance of being infected with COVID-19. Moreover, only 24.9% of participants were reluctant to visit the hospital for fear of contracting the virus (7.8% were “extremely scared”, and 17.1% were “very scared”). Approximately 73.5% of participants reported that the pandemic has affected their daily life (19.9% thought that it had a “major effect”, and 53.6% thought that it had a “moderate effect”). Lastly, most (93.4%) participants indicated that they were confident in the government’s ability to manage the pandemic (Table 2).
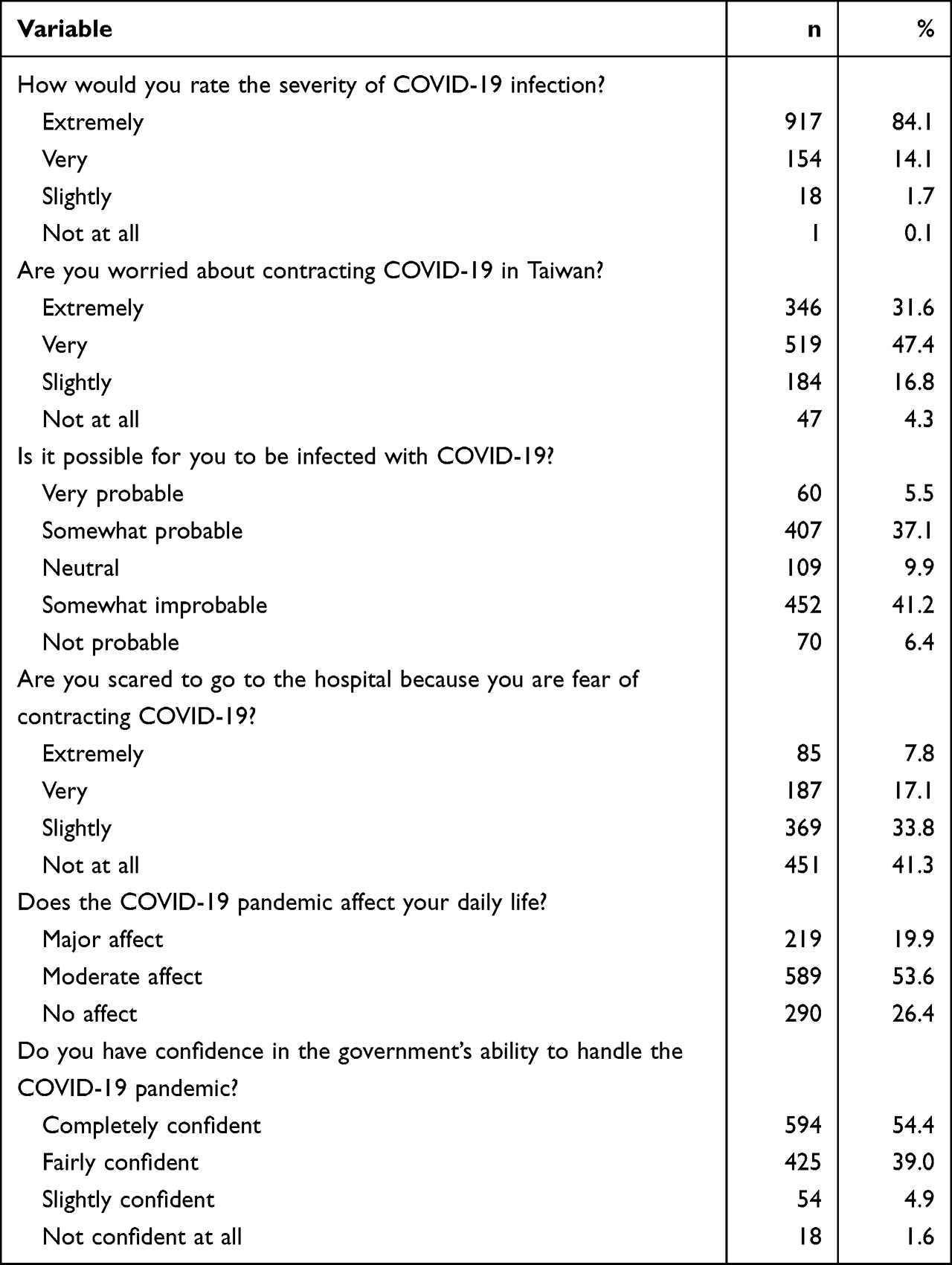 |
Table 2 Perceptions Towards COVID-19 |
Table 3 shows the distribution of psychological distress according to the demographics of participants and their perception of COVID-19. A significantly higher percentage of female patients than male patients had insomnia (60.4%), anxiety (61.8%), hostility (64.9%), and depression (63.3%). A significantly higher percentage of participants who were worried about contracting COVID-19 had anxiety (93.5%) and depression (87.6%) than participants who were not worried. A significantly higher percentage of participants who believed that they had a chance of being infected with COVID-19 had insomnia (50.0%), anxiety (53.4%), hostility (53.2%), depression (54.5%), and suicidal ideation (81.8%) than participants who believed that it was impossible for them to be infected. A significantly higher percentage of participants who were reluctant to visit the hospital for fear of contracting the virus had insomnia (40.9%), anxiety (41.6%), hostility (34.4%), depression (37.3%), and interpersonal sensitivity/inferiority (41.5%) than participants who were not afraid. A significantly higher percentage of participants who reported that the pandemic had affected their daily life exhibited insomnia (86.0%), anxiety (89.8%), hostility (93.5%), depression (92.7%), and interpersonal sensitivity/inferiority (89.6%) than participants who reported that the pandemic did not affect their daily life. A significantly higher percentage of participants who had confidence in the government’s ability to manage the pandemic had hostility (86.1%) and depression (86.4%) than participants who were not confident.
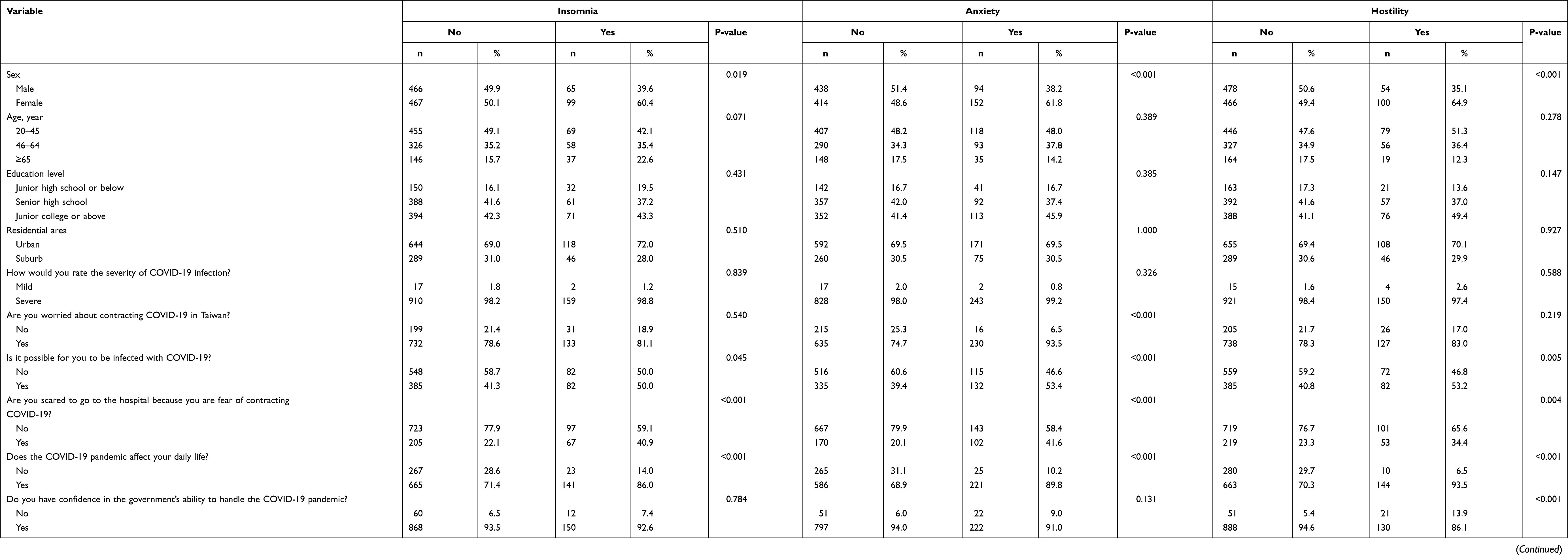 |
Table 3 The Distribution of the Psychological Distress by Demographic of Participants and Perception to COVID-19 |
Table 4 shows the distribution of psychological morbidity according to the demographics of participants and their perception of COVID-19. More participants without psychological morbidity were reluctant to visit the hospital for fear of contracting the virus (51.7%), reported that the pandemic had affected their daily life (91.4%), and had confidence in the government’s ability to manage the pandemic (93.8%).
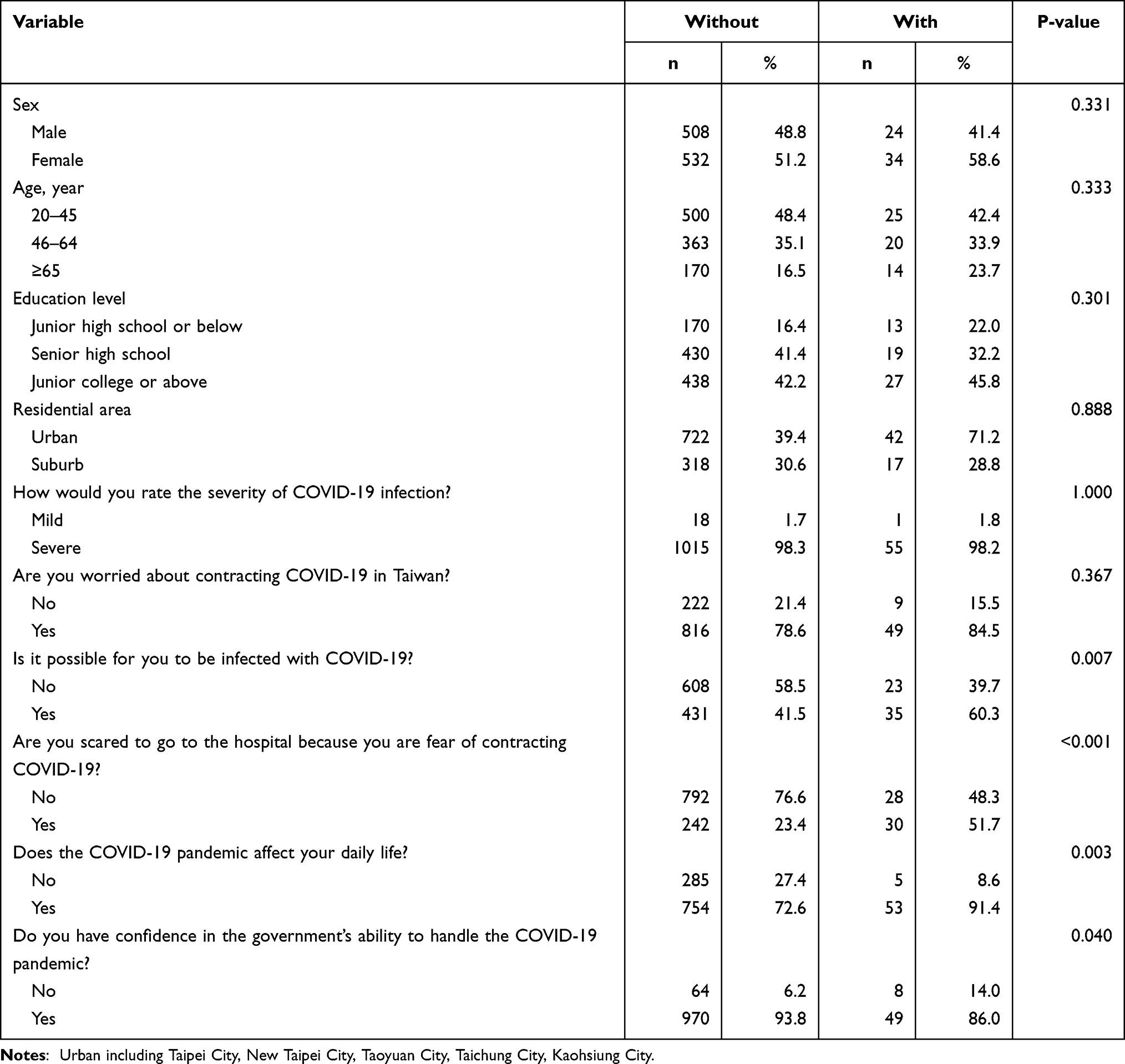 |
Table 4 The Distribution of the Psychological Morbidity by Demographic of Participants and Perception to COVID-19 |
Table 5 shows the psychological distress experienced by participants and the relevant factors. After controlling for covariates, being worried about contracting COVID-19 was positively associated with a higher odds of having anxiety (OR = 4.57, 95% CI: 2.69–7.75) and depression (OR = 1.91, 95% CI: 1.18–3.07) than not being worried. After controlling for covariates, a belief of a chance of being infected with COVID-19 was positively associated with a higher odds of having insomnia (OR = 1.44, 95% CI: 1.03–2.02), anxiety (OR = 1.74, 95% CI: 1.30–2.33), hostility (OR = 1.54, 95% CI: 1.09–2.18), depression (OR = 1.74, 95% CI: 1.25–2.42), and psychological symptoms (OR = 2.29, 95% CI: 1.32–3.97) than a belief the impossibility of infection. After controlling for covariates, reluctance to visit the hospital for fear of contracting the virus was positively associated with a high odds of having insomnia (OR = 2.33, 95% CI: 1.64–3.31), anxiety (OR = 2.87, 95% CI: 2.10–3.91), hostility (OR = 1.70, 95% CI: 1.17–2.46), depression (OR = 1.95, 95% CI: 1.38–2.77), interpersonal sensitivity/inferiority (OR = 2.45, 95% CI: 1.46–4.11), and psychological symptoms (OR = 3.35, 95% CI: 1.96–5.75) compared with not being afraid. After controlling for covariates, reporting that the pandemic had affected their daily life was positively associated with high odds of having insomnia (OR = 2.58, 95% CI: 1.60–4.16), anxiety (OR = 3.92, 95% CI: 2.50–6.13), hostility (OR = 5.79, 95% CI: 2.97–11.32), depression (OR = 5.15, 95% CI: 2.87–9.26), interpersonal sensitivity/inferiority (OR = 3.19, 95% CI: 1.40–7.26), and psychological symptoms (OR = 4.01, 95% CI: 1.60–10.04) compared with a report that the pandemic did not affect daily life. After controlling for covariates, having confidence in the government’s ability to manage the pandemic was negatively associated with a low odds of hostility (OR = 0.37, 95% CI: 0.21–0.64), depression (OR = 0.38, 95% CI: 0.22–0.65), and psychological morbidity (OR = 0.42, 95% CI: 0.19–0.92) compared with not being confident.
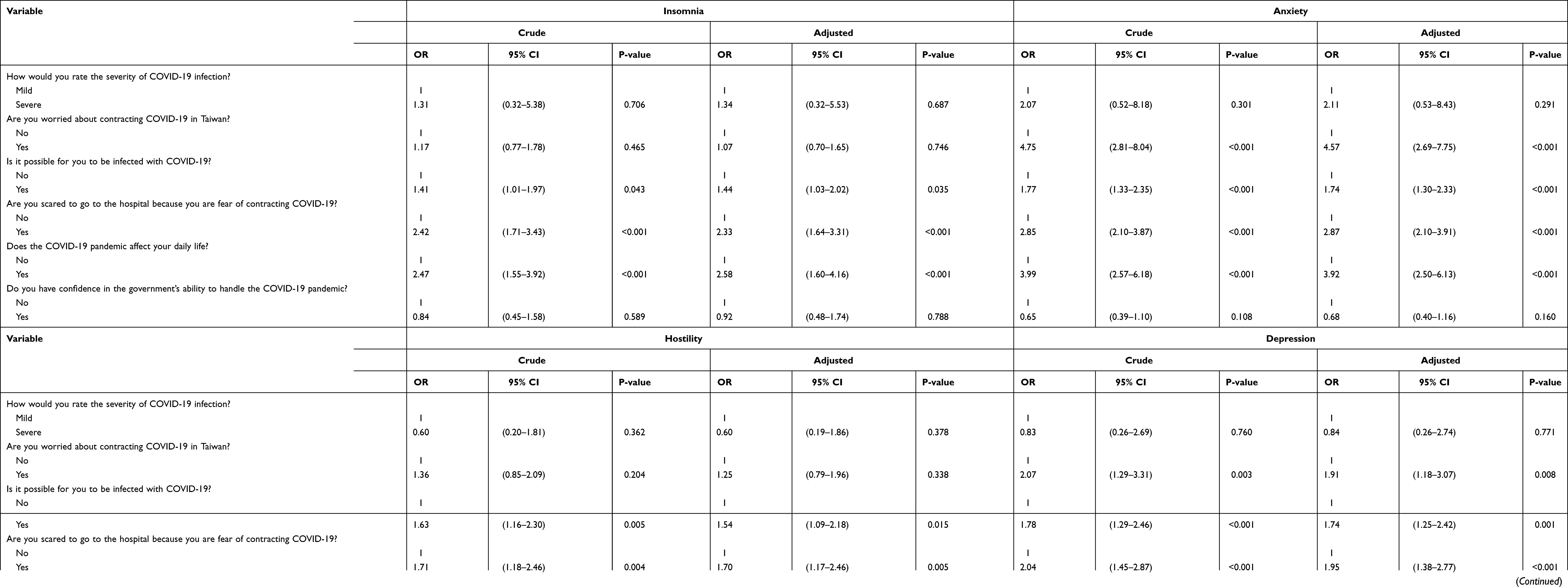 |
Table 5 Crude and Multiple Logistic Regression of Psychological Distress by Perception to COVID-19 |
Discussion
This cross-sectional study conducted through telephone surveys investigated whether people’s perceptions of COVID-19 were associated with psychological distress during the COVID-19 outbreak. As a matter of fact, during the investigation of this study in April 2020, COVID-19 had already spread and affected numerous people around the world. At that time, the pandemic condition in Taiwan was not critical. Apart from for a few sporadic clusters and infections overseas, the cumulative number of confirmed cases of COVID-19 were only about 400, and the cumulative death toll was less than 10. However, at that moment, there was a lot of news about COVID-19 on social media, there was no vaccine and specific treatments for COVID-19, and there was a shortage of personal protective equipment, which effects on people’s emotional wellbeing. Therefore, regardless of the spread and severity of the COVID-19 pandemic in each country, perceptions of COVID-19 are factors that affect people’s mental health. We found that participants who were worried about contracting COVID-19, who believed that they had a chance of being infected with COVID-19, who were reluctant to visit the hospital for fear of contracting the virus, who believed that the pandemic had affected their daily life, and who had high levels of trust in the government’s capacity to manage the pandemic experienced anxiety, hostility, depression, interpersonal sensitivity/inferiority, and psychological symptoms. To the best of our knowledge, this is the first study to investigate the impact of the perceptions of Taiwanese residents about COVID-19 on their mental health.
Our findings are similar to those of previous studies, which have reported that public health emergencies may lead to a universal psychological crisis, such as that observed during severe acute respiratory syndrome (SARS),36 the 2009–2010 swine flu (influenza H1N1),37 the 2014–2016 Ebola epidemic,38 and the 2015–2016 Zika virus.39 Our data indicated that the fear of contracting the coronavirus was positively related to psychological distress. Fear is an adaptive emotion that can mobilize the energy to cope with potential danger. However, severe fears may have adverse effects on an individual. A cross-sectional online survey indicated that health-related anxiety was related to the increased fear of the current coronavirus pandemic.40 Perceived stress related to COVID-19 was significantly associated with high suicide risk during confinement.41 A previous systematic review and meta-analysis concluded that mental health problems during COVID-19 include anxiety, depression, insomnia, post-traumatic stress disorder, and psychological distress.42 Costanza et al investigated different types of COVID-19-related fear in patients admitted to the psychiatric emergency department during the lockdown and post-lockdown periods.43 The patients were more fearful of losing their jobs or deteriorating work status during the lockdown compared to the post-lockdown.43 During the post-lockdown periods, the feeling of hopelessness became more prominent.43
In the present study, we investigated whether the belief that the COVID-19 pandemic has affected their daily life was associated with several mental health issues. To control the spread of infectious diseases, many strict public health measures have been implemented, including applying strict personal hygiene, mandatory wearing of masks, restricting social gatherings, maintaining a social distance of more than 1 m outdoors and 1.5 m indoors, strict quarantine, and restricting travel between countries.44 A previous systematic review and meta-analysis concluded that social isolation is associated with physical and mental health problems, such as increased risks of early mortality, depression, and anxiety.45 A cross-country study on Polish and Chinese populations indicated that wearing face masks could lead to public anxiety and confusion.46 A cohort study of students from the University of Pittsburgh demonstrated that lifestyle disruptions lead to an increased risk of depression during the pandemic.47 The implementation and enforcement of strict regulations and preventive strategies are critical risk factors for poor physical and mental health.48
Our data indicated that the majority of the public trusted the government’s effective response to the COVID-19 pandemic. A significant association was observed between the public’s trust in the government’s ability to respond to the pandemic and the mental health of the public. During the COVID-19 public health emergency, the Taiwanese government established the “Central Epidemic Command Center”, an epidemic information platform. From January 23, 2020, daily press conferences were held to keep the public informed of the progress of the epidemic and policy changes and to clarify misinformation.49,50 Risk communication is an important precedent for physical and mental health during a pandemic.48,51 Daily risk communication by providing the public with factual information about the current situation can relieve physical and mental tension.48 The public’s trust in risk communication by the government may affect their perceived self-efficacy in practicing preventive measures and voluntary adherence with policy programs,52,53 which is positively related to mental health.48 In times of instability or economic crisis, the “interpersonal trust” among individuals was a protective factor for mental health problems, and people with low interpersonal trust were significantly associated with suicidal ideation.54 During the Covid-19 pandemic, social networking, family support, and interpersonal trust could reduce feelings of loneliness and suicidal ideation.55 Furthermore, having trust in institutions, such as trust in the government policy measures including interventions for the unemployed, sustained welfare, and activating labor market programs, can be effective in preventing suicide.55
The present study demonstrated that women experience more insomnia, anxiety, hostility, and depression than men. A cross-sectional study in Poland showed that female gender is one of the risk factors for depression and anxiety.56 A cross-country epidemiologic survey comparing populations from China and Poland reported that men showed significantly lower scores of the Impact of Event Scale-Revised and Depression and the Anxiety and Stress Scale during the COVID-19 pandemic.46 Many studies have also shown that the prevalence of anxiety,57 panic disorder,57 depression,58 and trauma- and stress-related disorders57,59 is higher in women than in men, which might be attributable to environmental risk factors, gender-specific biological factors such as latent gender-dimorphic temperamental factors,57 and changes in ovarian hormones.60 Recent empirical research showed that women have a higher incidence of severe emotional exhaustion than men among Chilean higher education students during the COVID-19 pandemic.61 A systematic review of nine studies involving 106,814 higher education students demonstrated that health, psychological, ethnographic, and contextual factors were associated with suicidal thoughts and ideation during the COVID-19 pandemic.62
Our study has strengths and originality. This is the large population-based survey in Taiwan to investigated people’s perceptions or fear of the impact of COVID-19 on mental health. Our study specifically examined the confidence in the measures taken by the government and the psychological distress or psychiatric conditions during COVID-19 pandemic. However, the study has some limitations. First, the COVID-19 pandemic has affected Taiwan at different times and to varying degrees. This research survey represents people’s perception of COVID-19 and their psychological distress only in April 2020. Second, a bias exists in data collected through CATI, which is a noncoverage bias among citizens whose households do not have telephones. Third, our study also lacks information of potential confounding factors, such as personal mental disorder history, work condition, socioeconomic state. Fourth, we absence of methods to ensure inter-rater reliability between interviewers. However, before the interviewer conducts the formal investigation, interviewer training will be performed on the content of the questionnaire so that the interviewer can understand the purpose and content of the investigation for the interview in advance. Finally, the cross-sectional study design makes it impossible to make a causal inference.
Conclusion
This study showed that during the pandemic, the general population experienced a high rate of insomnia, anxiety, hostility, and depression. People’s perception of COVID-19 is related to psychological distress. In particular, we observed that the public’s trust in the government’s ability to respond to the pandemic was significantly associated with the mental health of the public. Although the Taiwanese government can take effective epidemic control measures to manage the COVID-19 pandemic, this crisis may still cause mental health problems in the general population. Therefore, we recommend raising awareness of the importance of mental health during the COVID-19 pandemic. Health professionals and policy makers should pay more attention to high-risk groups among those at risk for developing mental health problems. In addition, the impact of the COVID-19 on health, economy, and social environment may cause psychological problems in the next period. Therefore, government policies on mental health should be a long-term plan, and we also suggest that future research on such topics must constantly explore the mental health issues of the high-risk groups in the post-pandemic era.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li W, Yang Y, Liu ZH, et al. Progression of mental health services during the COVID-19 outbreak in China. Int J Biol Sci. 2020;16(10):1732–1738. doi:10.7150/ijbs.45120
2. Fabre JB, Grelot L, Vanbiervielt W, Mazerie J, Manca R, Martin V. Managing the combined consequences of COVID-19 infection and lock-down policies on athletes: narrative review and guidelines proposal for a safe return to sport. BMJ Open Sport Exerc Med. 2020;6(1):e000849. doi:10.1136/bmjsem-2020-000849
3. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
4. Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–943. doi:10.1001/jamainternmed.2020.0994
5. World Health Organization. WHO coronavirus dashboard; 2021. Available from: https://covid19.who.int/.
6. Walton M, Murray E, Christian MD. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur Heart J Acute Cardiovasc Care. 2020;9(3):241–247. doi:10.1177/2048872620922795
7. Pfefferbaum B, North CS. Mental health and the covid-19 pandemic. N Engl J Med. 2020;383(6):510–512. doi:10.1056/NEJMp2008017
8. Hashimoto K, Gao J, Zheng P, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS One. 2020;15:4.
9. World Health Organization. COVID 2019 PHEIC Global research and innovation forum: towards a research roadmap; 2020. Available from: https://www.who.int/blueprint/priority-diseases/key-action/Global_Research_Forum_FINAL_VERSION_for_web_14_feb_2020.pdf.
10. Gu S, He Z, Sun L, et al. Effects of coronavirus-19 induced loneliness on mental health: sleep quality and intolerance for uncertainty as mediators. Front Psychiatry. 2021;12:738003. doi:10.3389/fpsyt.2021.738003
11. Hoffart A, Johnson SU, Ebrahimi OV. Loneliness during the COVID-19 pandemic: change and predictors of change from strict to discontinued social distancing protocols. Anxiety Stress Coping. 2022;35(1):44–57. doi:10.1080/10615806.2021.1958790
12. Koda M, Harada N, Eguchi A, Nomura S, Ishida Y. Reasons for suicide during the COVID-19 pandemic in Japan. JAMA netw open. 2022;5(1):e2145870. doi:10.1001/jamanetworkopen.2021.45870
13. Tandon R. COVID-19 and suicide: just the facts. Key learnings and guidance for action. Asian J Psychiatr. 2021;60:102695. doi:10.1016/j.ajp.2021.102695
14. Hermosillo-de-la-Torre AE, Arteaga-de-Luna SM, Acevedo-Rojas DL, et al. Psychosocial Correlates of Suicidal Behavior among Adolescents under Confinement Due to the COVID-19 Pandemic in Aguascalientes, Mexico: A Cross-Sectional Population Survey. Int J Environ Res Public Health. 2021;18(9).
15. de Miquel C, Domènech-Abella J, Felez-Nobrega M, et al. The mental health of employees with job loss and income loss during the COVID-19 pandemic: the mediating role of perceived financial stress. Int J Environ Res Public Health. 2022;19:6. doi:10.3390/ijerph19063158
16. Chadi N, Ryan NC, Geoffroy MC. COVID-19 and the impacts on youth mental health: emerging evidence from longitudinal studies. Can J Public Health. 2022;113(1):44–52. doi:10.17269/s41997-021-00567-8
17. Ambrosetti J, Macheret L, Folliet A, et al. Psychiatric emergency admissions during and after COVID-19 lockdown: short-term impact and long-term implications on mental health. BMC Psychiatry. 2021;21(1):465. doi:10.1186/s12888-021-03469-8
18. Pompili M. Can we expect a rise in suicide rates after the Covid-19 pandemic outbreak? Eur Neuropsychopharmacol. 2021;52:1–2. doi:10.1016/j.euroneuro.2021.05.011
19. Sher L. Are COVID-19 survivors at increased risk for suicide? Acta neuropsychiatrica. 2020;32(5):270. doi:10.1017/neu.2020.21
20. Shigemura J, Ursano RJ, Morganstein JC, Kurosawa M, Benedek DM. Public responses to the novel 2019 coronavirus (2019-nCov) in Japan: Mental health consequences and target populations. Psychiatry Clin Neurosci. 2020;74(4):281–282. doi:10.1111/pcn.12988
21. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
22. Bourmistrova NW, Solomon T, Braude P, Strawbridge R, Carter B. Long-term effects of COVID-19 on mental health: a systematic review. J Affect Disord. 2022;299:118–125. doi:10.1016/j.jad.2021.11.031
23. Mat Ruzlin AN, Chen XW, Yunus RM, Samsudin EZ, Selamat MI, Ismail Z. Promoting mental health during the COVID-19 pandemic: a hybrid, innovative approach in Malaysia. Public Health Front. 2021;9:747953. doi:10.3389/fpubh.2021.747953
24. An Y, Sun Y, Liu Z, Chen Y. Investigation of the mental health status of frontier-line and non-frontier-line medical staff during a stress period. J Affect Disord. 2021;282:836–839. doi:10.1016/j.jad.2020.12.060
25. Cui J, Lu J, Weng Y, Yi GY, He W. COVID-19 impact on mental health. BMC Med Res Methodol. 2022;22(1):15. doi:10.1186/s12874-021-01411-w
26. Teufel M, Schweda A, Dörrie N, et al. Not all world leaders use Twitter in response to the COVID-19 pandemic: impact of the way of Angela Merkel on psychological distress, behaviour and risk perception. Am J Public Health. 2020;42(3):644–646. doi:10.1093/pubmed/fdaa060
27. Ding Y, Xu J, Huang S, Li P, Lu C, Xie S. Risk perception and depression in public health crises: evidence from the COVID-19 crisis in China. Int J Environ Res Public Health. 2020;17:16. doi:10.3390/ijerph17165728
28. McGinty EE, Presskreischer R, Han H, Barry CL. Psychological Distress and Loneliness Reported by US Adults in 2018 and April 2020. JAMA. 2020;324(1):93–94. doi:10.1001/jama.2020.9740
29. Qi M, Li X, Liu S, Li Y, Huang W. Impact of the COVID-19 epidemic on patterns of pregnant women’s perception of threat and its relationship to mental state: a latent class analysis. PLoS One. 2020;15(10):e0239697. doi:10.1371/journal.pone.0239697
30. Han Q, Zheng B, Agostini M, et al. Associations of risk perception of COVID-19 with emotion and mental health during the pandemic. J Affect Disord. 2021;284:247–255. doi:10.1016/j.jad.2021.01.049
31. Lee MB, Lee YJ, Yen LL, Lin MH, Lue BH. Reliability and validity of using a brief psychiatric symptom rating scale in clinical practice. J Formos Med Assoc. 1990;89(12):1081–1087.
32. Chen HC, Wu CH, Lee YJ, Liao SC, Lee MB. Validity of the five-item brief symptom rating scale among subjects admitted for general health screening. J Formos Med Assoc. 2005;104(11):824–829.
33. Lee MB, Liao SC, Lee YJ, et al. Development and verification of validity and reliability of a short screening instrument to identify psychiatric morbidity. J Formos Med Assoc. 2003;102(10):687–694.
34. Lung FW, Lee MB. The five-item brief-symptom rating scale as a suicide ideation screening instrument for psychiatric inpatients and community residents. BMC Psychiatry. 2008;8:53. doi:10.1186/1471-244X-8-53
35. Peng EY, Lee MB, Tsai ST, et al. Population-based post-crisis psychological distress: an example from the SARS outbreak in Taiwan. J Formos Med Assoc. 2010;109(7):524–532. doi:10.1016/S0929-6646(10)60087-3
36. Cheng SK, Wong CW, Tsang J, Wong KC. Psychological distress and negative appraisals in survivors of severe acute respiratory syndrome (SARS). Psychol Med. 2004;34(7):1187–1195. doi:10.1017/S0033291704002272
37. Page LA, Seetharaman S, Suhail I, Wessely S, Pereira J, Rubin GJ. Using electronic patient records to assess the impact of swine flu (influenza H1N1) on mental health patients. Int J Ment Health. 2011;20(1):60–69. doi:10.3109/09638237.2010.542787
38. Jalloh MF, Li W, Bunnell RE, et al. Impact of Ebola experiences and risk perceptions on mental health in Sierra Leone, July 2015. BMJ Global Health. 2018;3(2):e000471. doi:10.1136/bmjgh-2017-000471
39. Dos Santos Oliveira SJG, de Melo ES, Reinheimer DM, Gurgel RQ, Santos VS, Martins-Filho PRS. Anxiety, depression, and quality of life in mothers of newborns with microcephaly and presumed congenital Zika virus infection. Arch Women’s Ment Health. 2016;19(6):1149–1151. doi:10.1007/s00737-016-0654-0
40. Mertens G, Gerritsen L, Duijndam S, Salemink E, Engelhard IM. Fear of the coronavirus (COVID-19): predictors in an online study conducted in March 2020. J Anxiety Disord. 2020;74:102258. doi:10.1016/j.janxdis.2020.102258
41. Caballero-Domínguez CC, Jiménez-Villamizar MP, Campo-Arias A. Suicide risk during the lockdown due to coronavirus disease (COVID-19) in Colombia. Death Stud. 2020;2020:1–6.
42. Cénat JM, Blais-Rochette C, Kokou-Kpolou CK, et al. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. 2021;295:113599. doi:10.1016/j.psychres.2020.113599
43. Costanza A, Macheret L, Folliet A, et al. COVID-19 related fears of patients admitted to a psychiatric emergency department during and post-lockdown in Switzerland: preliminary findings to look ahead for tailored preventive mental health strategies. Medicina. 2021;57:12.
44. Chiu W-T, Laporte RP, Wu J. Determinants of Taiwan’s Early Containment of COVID-19 Incidence. Am J Public Health. 2020;110(7):943–944. doi:10.2105/AJPH.2020.305720
45. Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci. 2015;10(2):227–237. doi:10.1177/1745691614568352
46. Wang C, Chudzicka-Czupala A, Grabowski D, et al. The association between physical and mental health and face mask use during the COVID-19 pandemic: a comparison of two countries with different views and practices. Front Psychiatry. 2020;11:569981. doi:10.3389/fpsyt.2020.569981
47. Giuntella O, Hyde K, Saccardo S, Sadoff S. Lifestyle and mental health disruptions during COVID-19. Proc Natl Acad Sci. 2021;118(9):e2016632118. doi:10.1073/pnas.2016632118
48. Olagoke AA, Olagoke OO, Hughes AM. Psychological pathways linking public trust during the coronavirus pandemic to mental and physical well-being. Front Psychol. 2020;11:570216. doi:10.3389/fpsyg.2020.570216
49. Han E, Chiou ST, McKee M, Legido-Quigley H. The resilience of Taiwan’s health system to address the COVID-19 pandemic. EClinicalMedicine. 2020;24:100437. doi:10.1016/j.eclinm.2020.100437
50. Wang CJ, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analytics, new technology, and proactive testing. JAMA. 2020;323(14):1341–1342. doi:10.1001/jama.2020.3151
51. Covello VT. Risk communication: an emerging area of health communication research. Ann Int Commun Assoc. 2016;15(1):359–373. doi:10.1080/23808985.1992.11678816
52. Olagoke AA, Olagoke OO, Hughes AM. Exposure to coronavirus news on mainstream media: the role of risk perceptions and depression. Br J Health Psychol. 2020;25(4):865–874. doi:10.1111/bjhp.12427
53. Saechang O, Yu J, Public Trust LY. Policy compliance during the COVID-19 pandemic: the role of professional trust. Healthcare. 2021;9:2.
54. Economou M, Madianos M, Peppou LE, Theleritis C, Patelakis A, Stefanis C. Suicidal ideation and reported suicide attempts in Greece during the economic crisis. World Psychiatry. 2013;12(1):53–59. doi:10.1002/wps.20016
55. Costanza A, Amerio A, Aguglia A, et al. From”the interpersonal theory of suicide” to”the interpersonal trust”: an unexpected and effective resource to mitigate economic crisis-related suicide risk in times of covid-19? Acta Bio-Medica. 2021;92(S6):e2021417. doi:10.23750/abm.v92iS6.12249
56. Drosdzol A, Skrzypulec V. Depression and anxiety among Polish infertile couples--an evaluative prevalence study. J Psychosom Obstet Gynaecol. 2009;30(1):11–20. doi:10.1080/01674820902830276
57. McLean CP, Asnaani A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res. 2011;45(8):1027–1035. doi:10.1016/j.jpsychires.2011.03.006
58. Ford DE, Erlinger TP. Depression and C-reactive protein in US adults: data from the Third National Health and Nutrition Examination Survey. Arch Intern Med. 2004;164(9):1010–1014. doi:10.1001/archinte.164.9.1010
59. Breslau N, Peterson EL, Poisson LM, Schultz LR, Lucia VC. Estimating post-traumatic stress disorder in the community: lifetime perspective and the impact of typical traumatic events. Psychol Med. 2004;34(5):889–898. doi:10.1017/S0033291703001612
60. Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci. 2015;40(4):219–221. doi:10.1503/jpn.150205
61. Yeomans MM, Martínez-Libano J, Silva AJ. Emotional exhaustion in Chilean higher education students during the pandemic: analysis by gender. Psychol Educ. 2021;2021:1.
62. Martínez-Líbano J, Cabrera MM. Suicidal ideation and suicidal thoughts in university students during the COVID-19 pandemic: a systematic review. Rev Argent Clin Psicol. 2021;30:390–405.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Has the COVID-19 Pandemic Traumatized Us Collectively? The Impact of the COVID-19 Pandemic on Mental Health and Sleep Factors via Traumatization: A Multinational Survey
Holzinger B, Nierwetberg F, Chung F, Bolstad CJ, Bjorvatn B, Chan NY, Dauvilliers Y, Espie CA, Han F, Inoue Y, Leger D, Macêdo T, Matsui K, Merikanto I, Morin CM, Mota-Rolim SA, Partinen M, Plazzi G, Penzel T, Sieminski M, Wing YK, Scarpelli S, Nadorff MR, De Gennaro L
Nature and Science of Sleep 2022, 14:1469-1483
Published Date: 26 August 2022
Pre- and Post-Pandemic (COVID-19) Mental Health of International Students: Data from a Longitudinal Study
Jamshaid S, Bahadar N, Jamshed K, Rashid M, Imran Afzal M, Tian L, Umar M, Feng X, Khan I, Zong M
Psychology Research and Behavior Management 2023, 16:431-446
Published Date: 15 February 2023
Health-Related Quality of Life for Jordanian-Recovered Individuals During Post-COVID-19 Era: A Cross-Sectional Study
Abuhammad S, Khabour OF, Alzoubi KH, Hamaideh S, Khassawneh BY, Mehrass AAO, Alsmadi BF, Ababneh AM
Patient Preference and Adherence 2023, 17:1303-1310
Published Date: 22 May 2023
COPD-Related Anxiety: A Systematic Review of Patient Perspectives
Christiansen CF, Løkke A, Bregnballe V, Prior TS, Farver-Vestergaard I
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1031-1046
Published Date: 6 June 2023
Depression, Anxiety, Stress, Associated with Lichen Planus in Jordanian Women and the Impact on Their Quality of Life
Alnazly E, Absy N, Sweileh I
International Journal of Women's Health 2023, 15:1883-1892
Published Date: 27 November 2023