Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
A Phenomenological Qualitative Study of Primary Informal Caregiver of Chinese Patients with Advanced Stage COPD: An In-Depth Exploration of Experiences and Needs
Authors Ren X, Li F, Gao T, Xu X, Sun L, Liu S, Liu Y ![]() , Wang F
, Wang F
Received 28 December 2024
Accepted for publication 19 July 2025
Published 20 March 2026 Volume 2026:21 514685
DOI https://doi.org/10.2147/COPD.S514685
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Xingshuai Ren,1,* Fang Li,2,* Tao Gao,3,* Xilin Xu,1 Liyuan Sun,1 Shuangqi Liu,1 Yanhong Liu,4 Fei Wang5
1Department of Pulmonary and Critical Care Medicine, The People’s Hospital of Zouping City, Zouping, Shandong, People’s Republic of China; 2Department of Gynecology, The People’s Hospital of Dongming City, Heze, Shandong, People’s Republic of China; 3Department of Critical Care Medicine, The People’s Hospital of Zouping City, Zouping, Shandong, People’s Republic of China; 4Department of Geratology, The People’s Hospital of Zouping City, Zouping, Shandong, People’s Republic of China; 5Department of Pulmonary and Critical Care Medicine, The People’s Hospital of Dongming City, Heze, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanhong Liu, Department of Geratology, The People’s Hospital of Zouping City, #823 2 nd Heban Road, Zouping, Shandong, 256299, People’s Republic of China, Tel +86-13792291136, Email [email protected] Fei Wang, Department of Pulmonary and Critical Care Medicine, The People’s Hospital of Dongming City, West Gongye Road, Mengdie Road, Dongming, Heze, Shandong, 274500, People’s Republic of China, Tel +86-15098371412, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a progressive respiratory disorder. It poses significant challenges in its advanced stages and requires frequent hospitalizations and complex care strategies. The burden on informal caregivers, who play a crucial role in managing the disease, is profound and multifaceted, involving physical, emotional, and social challenges.
Objective: This study aimed to explore the lived experiences and needs of primary informal caregivers for patients with advanced COPD in China, with a focus on their emotional, physical, and social challenges and coping strategies.
Methods: A phenomenological qualitative approach was employed to provide an in-depth understanding of caregiver experiences. Data were collected through face-to-face semi-structured interviews with 15 primary informal caregivers of advanced COPD patients from Central China. The interviews were analyzed using Colaizzi’s method to extract key themes.
Results: Caregivers reported significant emotional burdens, including anxiety and fear related to the patient’s health and future. Physical challenges were prevalent, with many caregivers experiencing fatigue and health deterioration due to the demands of caregiving. Social isolation was also a critical issue, as caregiving responsibilities limited personal time and social interactions. Despite these challenges, caregivers employed various coping strategies, though these were often insufficient to fully mitigate the stress of caregiving.
Conclusion: Informal caregivers of patients with advanced COPD often face intense physical and psychological burdens and need comprehensive support systems. Enhancements in caregiver education, the development of targeted psychological supports, and the integration of caregivers into formal care plans are essential to improve the health outcomes of both caregivers and patients.
Keywords: chronic obstructive pulmonary disease, informal caregiving, caregiver burden, caregiver support, emotional stress, social isolation, caregiver coping strategy
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive lung disorder characterized by airflow limitation that is not fully reversible. It ranks among the top three causes of death worldwide, accounting for over 3 million deaths annually, with a disproportionate burden in low- and middle-income countries. The global prevalence of COPD is estimated at approximately 10.3% among adults, and the burden is projected to rise due to ongoing exposure to risk factors and population aging. COPD imposes substantial economic and social burdens, including high healthcare costs and significant loss of quality-adjusted life years.1 In advanced stages, COPD presents significant challenges due to progressive disability, frequent hospitalizations, and the need for complex palliative care.2,3 Patients often experience a decline in physical function, leading to a diminished quality of life. The economic impact is substantial, affecting both healthcare systems and individual families.4,5 Medical expenses, coupled with loss of productivity, place a financial strain on patients and their caregivers.5–7 Social implications are equally profound, as patients may face isolation and decreased participation in community activities.8,9 Despite advances in pharmacotherapy and pulmonary rehabilitation, multiple barriers hinder optimal disease management, ranging from patient-level factors such as health literacy to systemic challenges in access, especially in rural areas. A recent umbrella review by Siu and Gafni-Lachter (2024)10 identified the obstacles and stressed the promise of self-management education, Health Qigong, and telehealth delivery models in augmenting COPD care outcomes. However, successful implementation of such interventions depends critically on the engagement and support of informal caregivers, whose perspectives remain under-characterized in China.
Informal caregivers play a crucial role in managing chronic illnesses such as COPD. They provide essential support that ranges from assisting with daily activities to administering medications. The significance of informal caregivers becomes more pronounced in advanced COPD, where patients require continuous care. Caregivers face specific challenges, including physical exhaustion, emotional stress, and financial burdens.7,11 They often juggle caregiving responsibilities with personal and professional commitments, leading to increased pressure. There is a clear and growing trend of caregiving duties shifting onto family members due to the dual pressures of an aging population and limited healthcare resources. This shift is associated with increased burden and challenges for family caregivers, highlighting the need for better support systems and policy interventions.12–14
Despite the critical role of informal caregivers, current literature reveals several gaps. Caregiving for COPD patients is associated with significant physical, emotional, and psychological burdens.15,16 Caregivers often experience prolonged social isolation, anxiety, and a sense of constant vigilance. Their personal lives can be disrupted, leading to feelings of abandonment.7,17 The burden is further compounded by the lack of clear expectations and support from healthcare systems.18 Caregivers have diverse support needs that are often unmet. These include emotional support, practical assistance, and access to information about the disease and its management.19,20 Existing tools, such as the Carer Support Needs Assessment Tool (CSNAT), provide a framework but lack comprehensive coverage for COPD caregivers, particularly in such areas as patient-carer relationships and carer-clinician interactions.19 Interventions designed to support informal caregivers typically include education about COPD, discharge plans, and strategies to promote adherence to therapy and healthy lifestyles.21 However, these interventions often have a narrow scope and are not specifically tailored for caregivers.
While caregiving in COPD has been studied, the specific experiences and needs of caregivers for patients with advanced COPD have received comparatively limited research attention, especially in recent publications. Most studies on COPD caregiving focus broadly on the disease or on self-management, with fewer addressing the unique challenges faced by caregivers during the advanced stages of the illness.22–24 The advanced stages bring unique stressors and unmet needs that are not sufficiently explored in existing research. Furthermore, there is a lack of in-depth research within specific cultural and social contexts. In regions where family caregiving is a predominant practice, understanding the caregivers’ experiences becomes vital. In China, for example, filial responsibility often plays a significant role in caregiving dynamics.25,26 Studying caregiving experiences in such contexts is essential to develop culturally sensitive support mechanisms.
A phenomenological approach is appropriate for exploring caregivers’ lived experiences. This qualitative method allows for an in-depth understanding of individuals’ perceptions and feelings regarding their experiences.27 By focusing on their perspectives, researchers can gain valuable insights often overlooked in quantitative research.
In this study, we aim to explore the lived experiences and needs of primary informal caregivers of Chinese patients with advanced COPD. Specifically, the study aims to identify the emotional, physical, and social challenges experienced by caregivers. We seek to understand their coping strategies and unmet needs, providing actionable recommendations for healthcare professionals and policymakers.
Our study addresses a critical gap in the existing literature by focusing on the experiences and needs of caregivers of Chinese patients with advanced COPD.22–24 Practically, our findings shed light on the necessity of caregiver support services, training programs, and psychological counseling. By informing healthcare providers about the challenges faced by caregivers, the study can enhance engagement with caregivers during treatment and care planning. On a policy level, the findings advocate for caregiver-specific financial assistance and improved access to healthcare resources. Supporting the development of community-based programs tailored to caregivers of chronic illness patients becomes a priority. Academically, this research contributes to the qualitative literature on caregiving in advanced chronic diseases. It provides a culturally sensitive understanding of caregiving in COPD and add insights to global caregiving research.
Methods
Study Design
We employed a phenomenological qualitative approach to explore the lived experiences and needs of primary informal caregivers of patients with advanced COPD. Phenomenology was chosen because it facilitates an in-depth understanding of individuals’ subjective experiences related to a specific phenomenon. By focusing on caregivers’ perceptions and feelings, this approach aims to reveal the essence of their caregiving experiences without imposing preconceived notions. Reporting of the study was guided by the Standards for Reporting Qualitative Research (SRQR) guidelines.28 See Appendix 1 for a completed SRQR checklist.
Researcher Characteristics and Reflexivity
The research team consisted of eight healthcare professionals specialized in respiratory medicine, who were trained on qualitative research. The principal investigator (PI), a pulmonologist with over ten years of clinical experience, had prior interactions with COPD patients and their families, who provided contextual insights. The rest team members were healthcare professionals engaging in clinical care for COPD patients. To mitigate potential biases due to professional backgrounds and assumptions, the researchers engaged in reflexivity throughout the study. Regular team discussions were held to reflect on personal perspectives and to ensure that data collection and analysis remained grounded in participants’ narratives.
Study Context
The study was conducted at the Department of Respiratory Medicine of Zouping People’s Hospital, a tertiary comprehensive hospital in Zouping city, Shandong province, Central China. The department is a regional center for respiratory care, which allows for access to a diverse population of patients with advanced COPD and their caregivers. As one of the regions known for its historical traditions, Shandong province provides a cultural context where family caregiving is often rooted in filial piety values, which was integral to understanding the caregiving dynamics explored in our study.
We diagnosed COPD and staged disease progression according to the “Chronic Obstructive Pulmonary Disease Diagnosis and Treatment Guidelines (2021 Revised Edition)”.29 The diagnostic criteria included persistent airflow limitation with FEV1/FVC < 70% after bronchodilator inhalation, combined with symptoms such as chronic cough, sputum production, and dyspnea, as well as a history of exposure to risk factors like smoking and occupational hazards. Other diseases with similar manifestations must be excluded. Symptom severity was assessed using the mMRC or CAT scale, disease severity was graded based on the percentage of FEV1 compared to the predicted value, and the risk of acute exacerbation is evaluated according to the frequency of exacerbations and hospitalizations in the past year. Disease staging was defined by post-bronchodilator airflow limitation (FEV1/FVC < 0.70) and FEV1% predicted thresholds: mild (GOLD I, ≥ 80%), moderate (GOLD II, 50–79%), severe (GOLD III, 30–49%), and very severe (GOLD IV, < 30%). The current study focused on patients with advanced stage COPD (GOLD III & IV).
Sampling Strategy
Purposive sampling was utilized to select participants.30 Caregivers were eligible if they were the primary informal caregiver of a patient diagnosed with advanced COPD, aged 18 or older, demonstrated no physical or psychological impediments to compromise the implementation or integrity of the study, and willing to participate. Exclusion criteria included professional caregivers and individuals with impairments that would hinder the interview process, being aged under 18 years, or failure to provide informed consent. Recruitment continued until data saturation was achieved when no new significant analysis information emerged in three consecutive interviews.31
Data Collection
Data were collected through face-to-face semi-structured interviews conducted between May 11, 2024 and July 16, 2024. An interview guide was developed based on a review of existing literature and consultation with experts in respiratory care and qualitative research. It consisted of open-ended questions and was pilot tested with two participants, whose responses were not included in the final data analysis. See Appendix 2 for the final interview guide.
Interviews were held in a private meeting room in the hospital to maintain confidentiality. The interview questions were refined during the data collection process based on emerging insights. All interviews were audio-recorded with the consent of the participants attained before interview. Field notes were taken during and after interviews to capture non-verbal cues and contextual details.
Data Processing
Audio recordings were transcribed verbatim within 72 hours of interview. Transcriptions were reviewed for accuracy by comparing them with the original recordings. Participants’ identities were protected by assigning unique codes (P1, P2...) and removing any identifying information from the transcripts. All data were stored securely on password-protected flash drive accessible only to the research team to ensure confidentiality and data integrity.
Data Analysis
Data analysis followed Colaizzi’s phenomenological method,32 a rigorously structured approach designed to reveal the essential structure of caregivers’ lived experiences. First, each interview transcript was read in full at least three times by two independent researchers to achieve immersion in the data and ensure thorough comprehension of context and nuance. Next, we identified and highlighted all significant statements directly relating to caregivers’ roles, challenges, and perceptions. The statements were extracted and line-by-line coded. From each coded statement, we distilled underlying meanings. The formulated meanings were then compared and grouped where commonalities emerged, forming initial thematic clusters. We integrated the clusters into an exhaustive, narrative description that captured the breadth and depth of caregivers’ experiences and needs, carefully preserving the language of participants to maintain authenticity. Finally, we synthesized this rich description into a succinct statement of the phenomenon’s fundamental structure, detailing core themes, which were returned to participants to verify that our interpretation accurately reflected their experiences and needs.
Trustworthiness
We ensured trustworthiness of study through multiple strategies.33 First, two researchers independently reviewed and coded all transcripts, then met to compare code lists and resolve discrepancies, fostering inter-coder reliability and minimizing individual bias. An audit trail documented key analytic decisions for transparency. We conducted regular reflexivity sessions in which researchers recorded personal assumptions and examined how the assumptions might influence data interpretation.
To confirm credibility, we performed member checking by sharing preliminary themes with participants and incorporating their feedback into the final thematic structure. Transferability was supported by providing thick, contextualized descriptions of participants’ demographics and caregiving settings (Table 1), enabling readers to judge applicability to other populations. Dependability was established through peer debriefing with an external qualitative expert who reviewed our coding framework and exhaustive narrative and offered critical commentary. Finally, confirmability was achieved by triangulating data sources, comparing caregivers’ accounts with field notes and demographic data, and by retaining raw data files and analysis memos for audit.
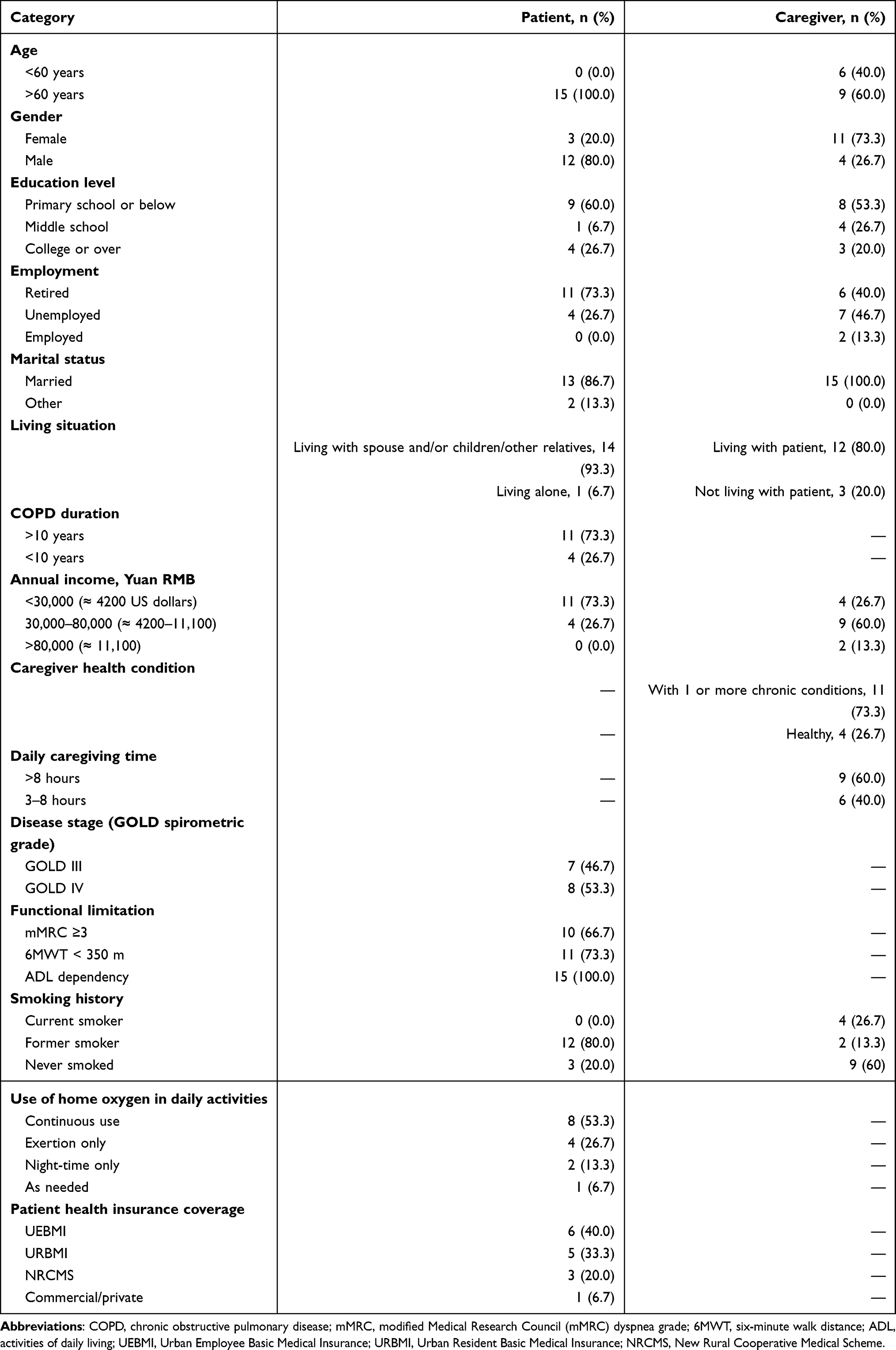 |
Table 1 Sociodemographic Characteristics of the Patients and Their Primary Informal Caregivers (N = 15) |
Ethical Approval and Informed Consenting
This study was ethically approved by the Ethical Committee of Zouping People’s Hospital (Approval number ZPLS2409). This study complied with the principles of the Declaration of Helsinki to protect the rights and well-fair of human subjects. Informed consents were signed with patients and their primary informal caregivers before participation, including consent for publication of anonymized direct quotes.
Use of Large Language Model Artificial Intelligence (LLM AI)
ChatGPT was utilized in the preparation of this manuscript, including translation of participant quotes from Chinese to English, the original Chinese draft into an English version, and polishing of the English language in subsequent writing. The core contents, including conceptualization, data analysis, thematic interpretation, and synthesis of findings, was independently developed by the researchers.
Results
Sociodemographic Characteristics of Patients and Informal Caregivers
The patient cohort comprised 15 individuals, all aged over 60 years. Most patients were male (80.0%) and had low formal education, with the majority having completed only primary school or below (60.0%). All of them were jobless, with nearly three-quarters retired and four unemployed. Most were married (86.7%), reflecting stable domestic partnerships. Almost all lived with family members (93.3%), a shared household context. The vast majority had suffered from COPD for over ten years and reported severe functional limitations. As patients with advanced stage of COPD, just under half of them (46.7%) were categorized as GOLD III (FEV1 30–49% predicted) while the rest (53.3%) met criteria for GOLD IV (FEV1 < 30% predicted). Financially, over 70% subsisted on annual incomes below RMB 30,000. None of the patients were current smokers. Most were former smokers (80%). Only 20% had never smoked. Health insurance coverage varied, with urban employee and resident schemes covering most patients and a minority relying on rural cooperative or commercial plans. More than half used home oxygen continuously, while others used it only during exertion, at night, or as needed.
A total of 15 corresponding caregivers were enrolled, who displayed more diverse age and gender profiles compared with patients. Although a majority were over 60 years of age, two-fifths were younger. Women comprised nearly three-quarters of the caregiving group. Over half held only primary-level education, with the remainder split between middle school and higher education. Employment status varied. Caregivers were evenly distributed among retired and unemployed subgroups, with only two caregivers being actively employed. All caregivers were married and most cohabited with the patient (80.0%), indicating shared living arrangements that facilitated hands-on support. Most reported managing their own chronic health conditions (73.3%), while the remainder considered themselves healthy. Caregiving demands were substantial, with 60% providing care for more than eight hours daily and the rest for three to eight hours. Smoking history was mixed. The majority had never smoked or had quit, and four caregivers continued to smoke at the time of the study. Table 1 summarizes the sociodemographic characteristics of the patient and caregiver cohorts.
Main Themes
A total of four main themes with five subthemes were yielded from the interviews, as follows:
Theme 1: Emotional Burden and Coping Strategies
Subtheme 1.1: Feelings of Anxiety, Worry, and Fear
Caregivers frequently experience intense emotional burdens characterized by anxiety, worry, and fear. These emotions stem from concerns about the patient’s health deterioration, uncertainty about the future, and the distress of witnessing the patient’s suffering. The fear of not being able to help or alleviate the patient’s discomfort adds to their emotional stress.
Sample quotes:
P1:When I first learned about his illness, I was extremely worried and confused. I sought medical help everywhere. Not knowing how the disease would progress, we went to Jinan and Shenyang for treatment. Eventually, we learned that this disease cannot be cured, and it can only be managed with medication.
P2:I felt so anxious just watching. Seeing him on the verge of tears made us want to cry too. It was so upsetting. I felt powerless, unable to help, so I could only ensure his basic needs and emotional well-being were met. But I knew I could not do more.
P3:When he first got sick, I was terrified. That feeling has not changed even now.
Subtheme 1.2: Feelings of Frustration and Helplessness
Caregivers often feel frustrated and helpless when their efforts do not yield the desired outcomes or when the patient’s behavior makes caregiving more challenging. Situations such as patients refusing medication, being irritable, or experiencing sudden health declines can exacerbate these feelings, leaving caregivers feeling powerless.
P1:Sometimes I feel utterly powerless, and this feeling comes up a lot. Since he got sick, his temper has changed drastically—he gets angry easily and often refuses to take his medication. It makes me so anxious that I do not know what to do.
P2:Sometimes, even after preparing meals, he will not eat because they do not suit his taste. It’s heartbreaking to see him suffer, but there’s nothing I can do to help him. My ability is too limited.
P9:Of course, the pressure is overwhelming. Seeing him coughing and struggling to breathe makes my heart ache.
Subtheme 1.3: Coping Strategies
To manage their emotional burden, caregivers adopt various coping strategies. Some seek social support by talking to friends or family members, while others engage in personal activities like walking or exercising to relieve stress. However, time constraints and the demands of caregiving often limit their ability to engage in these activities.
P1:Sometimes, when I am exhausted, I cry alone at home for a while.
P2:I chat with friends or go out for a walk or some activities. It helps release my physical and emotional tension.
P3:When I feel overwhelmed, I go for a walk alone. There’s no other way. I do not dare tell the kids because they are busy with work.
Theme 2: Physical Health Impact on Caregivers
Caregiving responsibilities often take a toll on the caregivers’ physical health. Many caregivers report fatigue, lack of sleep, and deterioration of their own health conditions. Some neglect their own medical needs due to lack of time or prioritizing the patient’s needs over their own. This physical strain can exacerbate existing health issues and make caregiving even more challenging.
P1:Ever since he got sick, I have not slept well. I used to take sleeping pills, but later I heard they are not good for long-term use, so I stopped. Now I barely sleep a few hours a night, and my legs are not in great shape either. I have been taking calcium tablets for years.
P2:In the past four years of caring for him, I developed atrophic gastritis. Last year, I underwent a colonoscopy and was found to have intestinal polyps. I was hospitalized for 11 days. I think it’s related to stress, but there’s no other option but to endure.
P4:My health is not great this year. Last year, I fractured my arm and leg. My children had to take care of me for a while. This year, my condition has not improved much.
Theme 3: Social Isolation and Impact on Social Life
Caregivers often experience social isolation due to the demands of caregiving, which limit their ability to engage in social activities, maintain relationships, or pursue personal interests. This isolation can lead to feelings of loneliness and a sense of disconnect from their social networks, further exacerbating the emotional burden.
P1:My children are very busy. My younger daughter works in corporate finance, and my older daughter, though retired, took up another job because her pension is not sufficient. Unless it’s an emergency, I try not to disturb them.
P2:I do not have time now. I cannot leave him alone. When I go out to buy food, I keep my phone with me in case he feels unwell or calls me. I do not dare to stay outside for long.
P3:The stairs at home are very high. I cannot leave him alone. I stay home all the time and only go out to buy things when necessary.
Theme 4: Knowledge and Skills in Disease Management
Subtheme 4.1: Need for Medical Knowledge
Caregivers express a desire to learn more about COPD and its management, including medication use, emergency handling, and symptom management. They seek information to better care for the patient and to reduce their own anxiety about the disease. Understanding the disease helps them feel more in control and prepared.
P1:I only have a superficial understanding. I know a bit about the medications he takes, like cough suppressants, expectorants, and inhalers. If things get worse, I take him to the hospital. I hope to learn more so he can live longer.
P6:We learn a little bit from our phones, but I do not know much about the pathology of the disease.
P13:I have heard about teaching breathing exercises, but I do not know how to do them. I searched online, but I could not teach him. Yesterday, I asked the nurse if there were any tools to assist with this.
Subtheme 4.2: Need for Training in Caregiving Skills
Some caregivers feel they lack the necessary skills for caregiving tasks and express interest in receiving training or guidance from medical professionals. They want to learn practical skills, such as administering treatments, managing equipment, and performing exercises that can help the patient.
P1:When he feels very suffocated, I give him his inhaler. I hope to learn more methods to handle these situations.
P13:I can share some videos on lung rehabilitation exercises. They are quite simple, and you can just follow along.
P14:I’d like to suggest that many commonly used chronic disease medications are not available in the hospital. For his inhaler, I have to go all the way to Jinan to get it.
Discussion
Our sample appears representative of the informal caregiving model prevalent among advanced COPD patients. Typically, the patients are older adults aged 60 years or above. They tend to live and be cared for by their immediate family members, such as spouses and children, which is a deeply rooted familial caregiving structure. The caregivers in our study, primarily women and many of whom are also elderly, frequently share the same low to middle socioeconomic background as the patients, including similar education levels and employment status. The shared living arrangements not only facilitates daily caregiving but also reflects the socio-economic and emotional interdependencies in management of advanced COPD in family settings. Nearly all caregivers report significant daily caregiving responsibilities, often exacerbated by their own chronic health issues, likely resulting in considerable physical and emotional demands on them, which are reflected in our findings.
According to Theme 1, informal caregivers of advanced COPD patients experience intense emotional burdens, such as anxiety, worry, and fear due to uncertainties about disease progression and patient suffering. Similar emotional responses are well-documented in literature, where chronic illness caregiving is consistently associated with heightened stress levels.34–36 The emotional stress in caregivers can be attributed to their close daily observations of their loved ones’ deteriorations, which may be more intense than in other illnesses due to the progressive and visible decline typical in COPD.37
Caregivers utilize coping strategies such as seeking social support and engaging in personal activities to manage their emotional burdens. Nonetheless, lack of support for informal caregivers is a common issue reported across numerous diseases and patient groups38–40 and the demanding nature of caregiving often limits the effectiveness of these strategies.16,41,42 This suggests that healthcare providers should integrate psychological support within the care frameworks, offering regular counseling and stress management workshops tailored for caregivers.43,44
According to our findings, physical health deterioration is common among caregivers, manifested as fatigue, sleep disturbances, and neglect of personal health. This deterioration often stems from the continuous physical demands of caregiving and chronic stress.45–47 The literature corroborates that long-term caregiving can lead to significant health declines, suggesting that caregivers themselves need care strategies.48–50 Clinically, it is necessary for healthcare systems to offer health screenings and preventive care specifically for caregivers, ensuring they remain healthy enough to sustain their caregiving roles.
Social isolation emerges as a significant issue for caregivers, largely due to the time-consuming nature of caregiving duties that limit social interactions (Theme 3). This isolation exacerbates the caregivers’ emotional and physical burdens by reducing their access to external support networks.19,51,52 Comparatively, studies in similar caregiving settings have shown that social isolation can lead to increased depression and anxiety.53 Policies and intervention strategies need to encourage the creation of support networks and respite care opportunities, allowing caregivers time away from their duties to rejuvenate and engage with their communities.
According to our findings, there is a critical need for improved knowledge and skills among caregivers, particularly in managing COPD’s complex needs. Caregivers often feel unprepared and overwhelmed, which can impair their ability to provide effective care. Our participants described limited access to formal training and resources, mirroring the “personal patient factors” and “service-model” barriers outlined by Siu and Gafni-Lachter (2024).10 Notably, caregivers expressed a strong desire for structured education, which aligns with evidence that self-management programs can reduce caregiver burden and improve patient outcomes. Similarly, the interest in remote support modalities resonates with positive telehealth results, suggesting that virtual caregiver training modules could address both informational and logistical constraints identified in this study. Furthermore, literature suggests that enhancing caregiver education on disease management not only improves patient outcomes but also reduces caregiver burden.54,55 Healthcare providers should consider implementing regular training sessions and support groups that enable caregivers to gain skills and share experiences.
Limitations
There are two main limitations to our study, which should be considered when interpreting the findings. Firstly, the sample’s sociodemographic characteristics might not be sufficiently representative. For example, the overwhelming majority of both patients and caregivers were married. Such homogeneity could limit the generalizability of the findings to other caregiving settings. Secondly, despite the aim to capture culturally specific caregiving dynamics, the findings may not fully reflect the cultural sensitivities inherent to the study’s objectives. The depth of cultural factors influencing caregiving in Chinese contexts might have been under-explored or inadequately captured due to the study’s methodological constraints. Future studies may draw upon established theoretical frameworks to delve further into this topic, especially for evidence that is more culturally sensitive, as well as exploring connections among the experiences and needs. Furthermore, our results reflect the specific experiences of caregivers in the sampled regions of China and that caution is warranted when extending the insights to caregivers in different healthcare systems or cultural environments.
Conclusions
Primary informal caregivers of Chinese patients with advanced COPD experience significant emotional burdens such as anxiety, worry, and fear, likely due to the progressive nature of COPD and the care demands. They also experience considerable physical health deterioration and social isolation. They commonly emphasize the need for comprehensive support mechanisms to address both the emotional and physical well-being. Implementation of targeted educational programs for enhancing caregivers’ skills in disease management, stronger support networks and respite care options are suggested.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. G. I. f. C. O. L. D.-. GOLD. 2025 GOLD report - global initiative for chronic obstructive lung disease - GOLD. Available from: https://goldcopd.org/2025-gold-report/.
2. Sorathia L. Palliative care in chronic obstructive pulmonary disease. Med Clin North Am. 2019;103(3):517–12. doi:10.1016/j.mcna.2018.12.010
3. Fusi-Schmidhauser T. Palliative care for patients with advanced COPD in primary care. Praxis. 2021;110(15):902–906. doi:10.1024/1661-8157/a003790
4. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of chronic obstructive pulmonary disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/copd.S234942
5. Xu J, Ji Z, Zhang P, Chen T, Xie Y, Li J. Disease burden of COPD in the Chinese population: a systematic review. Therapeutic Adv Respiratory Dis. 2023;17:17534666231218899. doi:10.1177/17534666231218899
6. Rehman AU, Hassali MAA, Muhammad SA, Harun SN, Shah S, Abbas S. The economic burden of chronic obstructive pulmonary disease (COPD) in Europe: results from a systematic review of the literature. Eur J Health Econ. 2020;21(2):181–194. doi:10.1007/s10198-019-01119-1
7. Lippiett KA, Richardson A, Myall M, Cummings A, May CR. Patients and informal caregivers’ experiences of burden of treatment in lung cancer and chronic obstructive pulmonary disease (COPD): a systematic review and synthesis of qualitative research. BMJ Open. 2019;9(2):e020515. doi:10.1136/bmjopen-2017-020515
8. Suen AO, Iyer AS, Cenzer I, et al. National prevalence of social isolation and loneliness in adults with chronic obstructive pulmonary disease. Ann Am Thoracic Soc. 2023;20(12):1709–1717. doi:10.1513/AnnalsATS.202304-288OC
9. O’Hoski S, Kuspinar A, Wald J, Richardson J, Goldstein R, Beauchamp MK. People with COPD have greater participation restrictions than age-matched older adults without respiratory conditions assessed during the COVID-19 pandemic. PLoS One. 2022;17(10):e0275264. doi:10.1371/journal.pone.0275264
10. Siu DCH, Gafni-Lachter L. Addressing barriers to chronic obstructive pulmonary disease (COPD) care: three innovative evidence-based approaches: a review. Int J Chron Obstruct Pulmon Dis. 2024;19:331–341. doi:10.2147/copd.S426050
11. Hipólito N, Ruivo A, Martins S, et al. Relationship between distress related to caregiver burden and physical activity in informal caregivers of patients with COPD. Copd. 2020;17(5):562–567. doi:10.1080/15412555.2020.1799964
12. Olagundoye O, Alugo M. Caregiving and the family. In: Mollaoglu M, editor. Caregiving and Home Care. Rijeka: IntechOpen; 2018.
13. da Rocha CG, Perrenoud B, Ramelet A-S. Perceptions of burden and preparedness for caregiving among the family caregivers of hospitalised older adults: a cross-sectional study. Geriatrics. 2022;7(1):19. doi:10.3390/geriatrics7010019
14. Shrestha S, Arora S, Hunter A, Debesay J. Changing dynamics of caregiving: a meta-ethnography study of informal caregivers’ experiences with older immigrant family members in Europe. BMC Health Serv Res. 2023;23(1):43. doi:10.1186/s12913-023-09023-4
15. Miravitlles M, Peña-Longobardo L, Oliva-Moreno J, Oliva-Moreno J. Caregivers’ burden in patients with COPD. Int J Chronic Obstr. 2015;10:347–356. doi:10.2147/COPD.S76091
16. Zhang Z, Jiang D, Jia Y, et al. Impact of caregiving burden on quality of life of caregivers of COPD patients: the chain mediating role of social support and negative coping styles. Int J Chronic Obstr. 2021;16:2245–2255. doi:10.2147/COPD.S311772
17. Bagnasco A, Rosa F, Dasso N, et al. Caring for patients at home after acute exacerbation of chronic obstructive pulmonary disease: a phenomenological study of family caregivers’ experiences. J Clin Nurs. 2021;30(15–16):2246–2257. doi:10.1111/jocn.15613
18. Strang S, Fährn J, Strang P, Ronstad A, Danielsson L. Support to informal caregivers of patients with severe chronic obstructive pulmonary disease: a qualitative study of caregivers’ and professionals’ experiences in Swedish hospitals. BMJ Open. 2019;9(8):e028720. doi:10.1136/bmjopen-2018-028720
19. Micklewright K, Farquhar M. P-81 Support needs of informal carers of patients with COPD and implications for improving carer support. BMJ Support Palliative Care. 2019;9(Suppl 4):A39–A39. doi:10.1136/bmjspcare-2019-HUKNC.104
20. Micklewright K, Farquhar M. Does the carer support needs assessment tool cover the established support needs of carers of patients with chronic obstructive pulmonary disease? A systematic literature search and narrative review. Palliative Med. 2020;34(10):1305–1315. doi:10.1177/0269216320939243
21. Marques A, Cruz J, Brooks D. Interventions to support informal caregivers of people with chronic obstructive pulmonary disease: a systematic literature review. Respiration. 2021;100(12):1230–1242. doi:10.1159/000517032
22. Bove DG, Zakrisson A-B, Midtgaard J, Lomborg K, Overgaard D. Undefined and unpredictable responsibility: a focus group study of the experiences of informal caregiver spouses of patients with severe COPD. J Clin Nurs. 2016;25(3–4):483–493. doi:10.1111/jocn.13076
23. Cooper E, Kuwornu J, Chinonyerem D, Gholami S. Understanding the unmet needs, experiences, and perspectives of COPD caregivers: a scoping review. COPD. 2025;22(1):2481260. doi:10.1080/15412555.2025.2481260
24. Matarese M, Pendoni R, Matarese M, De Marinis M. Caregivers’ experiences of contributing to patients’ self‐care in chronic obstructive pulmonary disease: a thematic synthesis of qualitative studies. J Adv Nurs. 2021;77(10):4017–4034. doi:10.1111/jan.14942
25. He L, Van heugten K. Chinese migrant workers’ care experiences: a model of the mediating roles of filial piety. Qualitative Health Res. 2020;30(11):1749–1761. doi:10.1177/1049732320925420
26. Zhu Y, Zhu Y, Yu H, Yu H. Naturally, it’s me taking care’: filial piety as anticipatory resilience in the temporal flow and stressors of Chinese only children caring for parents with cancer. J Applied Commun Res. 2025;53(1):23–45. doi:10.1080/00909882.2024.2444226
27. Coupé C, Ollagnier-Beldame M. Toward a phenomenology of taking care. Int J Qual Stud Health Well-Being. 2022;17(1):2045671. doi:10.1080/17482631.2022.2045671
28. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/acm.0000000000000388
29. 中华医学会呼吸病学分会慢性阻塞性肺疾病学组 and 中国医师协会呼吸医师分会慢性阻塞性肺疾病工作委员会 [Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society]. 慢性阻塞性肺疾病诊治指南(2021年修订版) [Chronic Obstructive Pulmonary Disease Committee of Chinese Association of Chest Physician (2021)]. 中华结核和呼吸杂志 [Chinese journal of tuberculosis and respiratory diseases]. 2021;44(3):36.
30. Campbell S, Greenwood M, Prior S, et al. Purposive sampling: complex or simple? Research case examples. J Res Nurs. 2020;25(8):652–661. doi:10.1177/1744987120927206
31. Daher W. Saturation in qualitative educational technology research. Educ Sci. 2023;13(2):98. doi:10.3390/educsci13020098
32. K.r P, S S. Application of Colaizzi’s method of data analysis in phenomenological research. Medico Legal Update. 2021;21(2):914–918. doi:10.37506/mlu.v21i2.2800
33. Amin MEK, Nørgaard LS, Cavaco AM, et al. Establishing trustworthiness and authenticity in qualitative pharmacy research. Res Social Administrative Pharm. 2020;16(10):1472–1482. doi:10.1016/j.sapharm.2020.02.005
34. Eichholz A, Dudeney J, Jaaniste T. Caregiver psychological burden in pediatric chronic pain: a systematic review and meta-analysis of associations with caregiver sociodemographic and biopsychosocial variables. J Pediatric Psychol. 2023;48(9):747–758. doi:10.1093/jpepsy/jsad041
35. Bidwell JT, Hostinar CE, Higgins MK, et al. Caregiver subjective and physiological markers of stress and patient heart failure severity in family care dyads. Psychoneuroendocrinology. 2021;133:105399. doi:10.1016/j.psyneuen.2021.105399
36. Schulz R, Beach SR, Czaja SJ, Martire LM, Monin JK. Family caregiving for older adults. Ann Rev Psychol. 2020;71(Volume 71):635–659. doi:10.1146/annurev-psych-010419-050754
37. Walbaum C, Philipp R, Oechsle K, Ullrich A, Vehling S. Existential distress among family caregivers of patients with advanced cancer: a systematic review and meta-analysis. Psycho-Oncology. 2024;33(1):e6239. doi:10.1002/pon.6239
38. Molassiotis A, Wang M. Understanding and supporting informal cancer caregivers. Curr Treatment Options Oncol. 2022;23(4):494–513. doi:10.1007/s11864-022-00955-3
39. Price M, Surr C, Surr C, Ashley L. Experiences and support needs of informal caregivers of people with multimorbidity: a scoping literature review. Psychol Health. 2019;35(1):36–69. doi:10.1080/08870446.2019.1626125
40. Benson J, Oliver DP, Washington KT, et al. Online social support groups for informal caregivers of hospice patients with cancer. European J Oncol Nurs. 2019;44:101698. doi:10.1016/j.ejon.2019.101698
41. Kazemi A, Azimian J, Mafi M, Allen K-A, Motalebi SA. Caregiver burden and coping strategies in caregivers of older patients with stroke. BMC Psychol. 2021;9(1):51. doi:10.1186/s40359-021-00556-z
42. Zhang N, Tian Z, Liu X, Yu X, Wang L. Burden, coping and resilience among caregivers for patients with chronic obstructive pulmonary disease: an integrative review. J Clin Nurs. 2024;33(4):1346–1361. doi:10.1111/jocn.16954
43. Corry M, Neenan K, Brabyn S, Sheaf G, Smith V. Telephone interventions, delivered by healthcare professionals, for providing education and psychosocial support for informal caregivers of adults with diagnosed illnesses. Cochrane Database Syst Rev. 2019;(5). doi:10.1002/14651858.CD012533.pub2
44. Coumoundouros C, Mårtensson E, Ferraris G, et al. Implementation of e-mental health interventions for informal caregivers of adults with chronic diseases: mixed methods systematic review with a qualitative comparative analysis and thematic synthesis. JMIR Ment Health. 2022;9(11):e41891. doi:10.2196/41891
45. Secinti E, Lewson AB, Wu W, Kent EE, Mosher CE. Health-related quality of life: a comparative analysis of caregivers of people with dementia, cancer, COPD/emphysema, and diabetes and noncaregivers, 2015–2018 BRFSS. Ann Behav Med. 2021;55(11):1130–1143. doi:10.1093/abm/kaab007
46. Hipólito N, Ruivo A, Martins S, et al. Relationship between distress and physical activity in informal carers of patients with COPD. Eur Respir J. 2019;54(suppl 63):PA1245. doi:10.1183/13993003.congress-2019.PA1245
47. Chu -H-H, Kyeong-Soo L, Kwan HL, Hong CJ, Kyeong-Cheol S, Hwang T-Y. Association of physical and psychological health status between chronic obstructive pulmonary disease patients and their family caregivers. Health Care Women Int. 2019;40(10):1019–1030. doi:10.1080/07399332.2019.1617292
48. Cho J, Stevens A. The relationship between functional decline of care recipients and health of caregivers. Innovation Aging. 2020;4(Supplement_1):361. doi:10.1093/geroni/igaa057.1161
49. Roth D. Duration of family caregiving and its effects on inflammation in the caregiving transitions study. Innovation Aging. 2021;5(Supplement_1):321. doi:10.1093/geroni/igab046.1251
50. Martin MP, McEntee ML, Suri Y. Caregiver quality of life: how to measure it and why. Am J Health Promotion. 2021;35(7):1042–1045. doi:10.1177/08901171211030142f
51. Hajek A, Kretzler B, König H-H. Informal caregiving, loneliness and social isolation: a systematic review. Int J Environ Res Public Health. 2021;18(22):12101. doi:10.3390/ijerph182212101
52. Li L, Wister AV, Mitchell B. Social isolation among spousal and adult-child caregivers: findings from the Canadian longitudinal study on aging. J Gerontol B. 2021;76(7):1415–1429. doi:10.1093/geronb/gbaa197
53. Santini ZI, Jose PE, York Cornwell E, et al. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. Lancet Public Health. 2020;5(1):e62–e70. doi:10.1016/S2468-2667(19)30230-0
54. Thodi M, Bistola V, Lambrinou E, et al. A randomized trial of a nurse-led educational intervention in patients with heart failure and their caregivers: impact on caregiver outcomes. Eur J Cardiovasc Nurs. 2023;22(7):709–718. doi:10.1093/eurjcn/zvac118
55. Rouch SA, Fields BE, Alibrahim HA, Rodakowski J, Leland NE. Evidence for the effectiveness of interventions for caregivers of people with chronic conditions: a systematic review. Am J Occup Ther. 2021;75(4):7504190030. doi:10.5014/ajot.2021.042838
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Health Priorities in Chronic Obstructive Pulmonary Disease Patients with Multimorbidity: A Qualitative Study
Cai M, Cui M, Nong Y, Qin J, Mo S
Patient Preference and Adherence 2022, 16:2521-2531
Published Date: 13 September 2022
Satisfaction and Adherence of COPD Patients to a Conventional Training Associated with Functional Exercises and to a Conventional Training Isolated: A Qualiquantitative Study
Grigoletto I, de Lima FF, Eto DA, Suzuki NNV, Uzeloto JS, Ramos EMC
Patient Preference and Adherence 2022, 16:2759-2772
Published Date: 11 October 2022
Factors Affecting Patient Adherence to Inhalation Therapy: An Application of SEIPS Model 2.0
Ma J, Sun X, Wang X, Liu B, Shi K
Patient Preference and Adherence 2023, 17:531-545
Published Date: 3 March 2023
COPD-Related Anxiety: A Systematic Review of Patient Perspectives
Christiansen CF, Løkke A, Bregnballe V, Prior TS, Farver-Vestergaard I
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1031-1046
Published Date: 6 June 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025