Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
COPD Exacerbations, Costs, and Health Care Resource Utilization Before and After Initiation of Fluticasone Furoate/Umeclidinium/Vilanterol in Routine Care in the USA
Authors Hanania NA, Bunner SH, Bengtson LGS, Ismaila AS ![]() , Bogart M
, Bogart M
Received 17 June 2022
Accepted for publication 15 March 2023
Published 24 March 2023 Volume 2023:18 Pages 407—418
DOI https://doi.org/10.2147/COPD.S378867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Nicola A Hanania,1 Scott H Bunner,2 Lindsay GS Bengtson,2 Afisi S Ismaila,3,4 Michael Bogart5
1Section of Pulmonary and Critical Care Medicine, Baylor College of Medicine, Houston, TX, USA; 2Optum, Eden Prairie, MN, USA; 3Value Evidence and Outcomes, GSK, Collegeville, PA, USA; 4Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada; 5US Value Evidence & Outcomes, GSK, Research Triangle Park, NC, USA
Correspondence: Afisi S Ismaila, Value Evidence and Outcomes, GSK, 1250 S. Collegeville Road, Collegeville, PA, 19426-0989, USA, Tel +1 919-3158229, Email [email protected]
Purpose: To examine the impact of initiating fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) in a single device on chronic obstructive pulmonary disease (COPD) exacerbations, COPD exacerbation-related costs, and all-cause and COPD-related healthcare resource utilization (HCRU) and costs in patients with COPD.
Methods: Retrospective database analysis of patients with COPD aged ≥ 40 years who initiated FF/UMEC/VI between September 1, 2017, and December 31, 2018 (index date: first pharmacy claim for FF/UMEC/VI), following evidence of multiple-inhaler triple therapy (MITT) (≥ 30 consecutive days) in the year prior to index. COPD exacerbations, COPD exacerbation-related costs, and all-cause and COPD-related HCRU and costs were compared between the baseline period (12 months prior to and including index) and follow-up period (12 months following index).
Results: Data from 912 patients (mean [SD] age: 71.2 [8.1], 51.2% female) were included in the analyses. Among the overall cohort, mean count of total COPD exacerbations (moderate or severe) per patient was statistically significantly lower in the follow-up period compared to baseline (1.2 vs 1.4, p=0.001). The proportion of patients with ≥ 1 COPD exacerbation (moderate or severe) was also statistically significantly lower in the follow-up period compared to baseline (56.4% vs 62.4%, p=0.001). All-cause and COPD-related HCRU were similar during follow-up compared to baseline, although the proportion of patients with COPD-related ambulatory visits was lower during follow-up (p< 0.001). COPD-related office visit costs, emergency room visit costs, and pharmacy costs were statistically significantly lower during follow-up compared to baseline (p< 0.001; p=0.019; p< 0.001, respectively).
Conclusion: In a real-world setting, patients on MITT who subsequently initiated FF/UMEC/VI in a single device had significant reductions in the rate of COPD exacerbations (moderate or severe). Switching to FF/UMEC/VI also resulted in improvements in some HCRU and cost outcomes. These data support the use of FF/UMEC/VI among patients at high risk of exacerbation to reduce future risk and improve outcomes.
Keywords: chronic obstructive pulmonary disease, exacerbations, healthcare utilization, multiple-inhaler triple therapy, FF/UMEC/VI, single-inhaler triple therapy
Plain Language Summary
Chronic obstructive pulmonary disease (COPD) treatments can be hard for patients on triple therapy to take consistently as they involve using multiple inhalers every day. By combining inhalers, treatment can be simplified. This study investigated the effect of switching from using multiple inhalers to deliver triple therapy regimens to a single inhaler of fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI). Specifically, we looked at the rate of COPD exacerbations, how often patients accessed healthcare services, and the costs of both. To do so, we searched for health claims from patients who started taking FF/UMEC/VI between September 1, 2017 and December 31, 2018 in the Optum Research Database, which contains information from over 73 million patients. COPD exacerbation rates, healthcare service use, and costs were then compared before and after switching to FF/UMEC/VI. Among 912 patients included in the study, we found that patients experienced fewer exacerbations after switching. COPD-related ambulatory visits (ie outpatient care where the patient is not admitted to hospital) were also lower, alongside COPD-related costs associated with visiting the doctor’s office, emergency room, and pharmacy. Our results show that switching to FF/UMEC/VI is beneficial for patients who are at high risk of exacerbation, to reduce this risk and improve outcomes.
Introduction
Chronic obstructive pulmonary disease (COPD) resulted in 3.23 million deaths worldwide in 2019.1 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy document recommends inhaled triple therapy (an inhaled corticosteroid [ICS], a long-acting β2-agonist [LABA], and a long-acting muscarinic antagonist [LAMA]) for patients with advanced COPD with persistent symptoms and risk of exacerbation.2
Previous evidence suggests significant improvement in lung function and health-related quality of life, alongside reduced exacerbation frequency, among patients with COPD who utilize once-daily single-inhaler triple therapy (SITT) with fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) compared with twice-daily budesonide/formoterol combination therapy.3 Real-world data have also shown that compared to non-Ellipta multiple-inhaler triple therapy (MITT), single-inhaler FF/UMEC/VI resulted in a significantly greater proportion of patients gaining health status improvement, alongside larger improvements in lung function.4 In addition, patients with COPD initiating single-inhaler FF/UMEC/VI in the real world have demonstrated improved adherence and persistence compared to MITT.5 In September 2017, the United States (US) Food and Drug Administration (FDA) approved FF/UMEC/VI 100/62.5/25 µg for once-daily maintenance treatment of COPD and to reduce COPD exacerbations in patients with a history of exacerbation.6
There is a lack of real-world evidence of the effectiveness of FF/UMEC/VI 100/62.5/25 µg on COPD exacerbations, and whether the improved adherence translates to improved patient outcomes. In this retrospective analysis, we examine the impact of initiating FF/UMEC/VI on COPD exacerbations, COPD exacerbation-related costs, and all-cause and COPD-related healthcare resource utilization (HCRU) and costs experienced by patients with COPD in the real-world setting.
Methods
Study Design
This was a retrospective database analysis conducted using the Optum Research Database (ORD). Commercial and Medicare Advantage with Part D (MAPD) enrollees with COPD who initiated FF/UMEC/VI during the patient identification period (September 1, 2017 to December 31, 2018) following evidence of MITT (≥30 consecutive days) in the year prior to FF/UMEC/VI initiation were included (Supplementary Figure 1).
The index date was the date of the first pharmacy claim for FF/UMEC/VI during the patient identification period. COPD exacerbations, COPD exacerbation-related costs, and all-cause and COPD-related HCRU and costs in the 12 months prior to and including the index (baseline period) were compared to those in the 12 months following index (follow-up period).
Data Collection
The ORD is a fully de-identified and Health Insurance Portability and Accountability Act (HIPAA) compliant research database that contains commercial and Medicare Advantage claims. It contains both medical and pharmacy information from 1993 to the present on more than 73 million individuals.
Study Population
Eligible patients met the following inclusion criteria: ≥1 pharmacy claim for FF/UMEC/VI during the patient identification period; ≥2 medical claims with a diagnosis code for COPD in any position on separate dates of service during the study period (baseline or follow-up period); ≥30 consecutive days of MITT during the 12 months prior to the index date; ≥40 years of age as of the year of the index date; continuous enrollment with medical and pharmacy coverage for 12 months prior to and including the index date (baseline period), and 12 months following the index date (follow-up period).
Patients were excluded from the study population if they met one or more of the following criteria: ≥1 medical claim with a diagnosis code for asthma, cystic fibrosis, or lung cancer during the study period; ≥1 pharmacy claim for FF/UMEC/VI during the baseline period; unknown or missing patient demographics (as detailed in Supplementary Table 1).
Outcomes
Primary Objectives
The primary objectives were to compare the following outcomes before and after initiation of FF/UMEC/VI: proportion of patients with ≥1 COPD exacerbation (any [moderate or severe], moderate, severe); COPD exacerbation rate (any [moderate or severe], moderate, severe); and COPD exacerbation-related costs.
COPD exacerbations were identified and categorized as moderate or severe. Severe exacerbations were defined as an inpatient hospitalization with a primary diagnosis of COPD. Moderate exacerbations were defined as an outpatient or ER visit with a primary diagnosis of COPD, and a systemic oral corticosteroid or guideline-recommended antibiotic within seven days of the medical visit. Both the rate and count of all, severe, and moderate exacerbations were reported.
Episode-level exacerbation costs were calculated for all COPD exacerbations as well as separately by severity. Costs were calculated for each exacerbation episode as the sum of COPD-related medical and pharmacy costs within the time period of the exacerbation, excluding maintenance medication costs. Mean cost of an exacerbation (any [moderate or severe], severe, moderate) was presented. Costs were adjusted to 2019 US dollars using the annual medical care component of the Consumer Price Index (CPI).
Secondary Objectives
Secondary objectives were to compare all-cause and COPD-related HCRU, and all-cause and COPD-related costs before and after initiation of FF/UMEC/VI.
HCRU was calculated for ambulatory visits (physician office and hospital outpatient), ER visits, inpatient admissions, and pharmacy fills. HCRU was defined as COPD-related if the medical claim had a diagnosis code for COPD in the primary position or was a pharmacy claim for a medication used to treat COPD.
Health care costs were CPI-adjusted and computed as the combined health plan and patient paid amounts in the baseline and follow-up period. Total costs were calculated and categorized as pharmacy costs and medical costs. Medical costs were further categorized into ambulatory costs (physician office and hospital outpatient), emergency services costs, inpatient costs, and other medical costs. Costs were defined as COPD-related if the medical claim had a diagnosis code for COPD in the primary position or was a pharmacy claim for a medication used to treat COPD.
Data Analysis
Bivariate comparisons of primary and secondary outcomes in the baseline and follow-up periods were performed. McNemar tests for categorical/binary variables (such as comparing frequency proportions), and paired t-tests for continuous variables (such as comparisons between mean values) were used based on the distribution of the measure. A statistical significance level of alpha = 0.05 was used (p<0.05).
We estimated that after applying the inclusion/exclusion criteria, approximately 900 patients would be included in the final sample. The proportion of patients with COPD exacerbations was used to estimate the minimum effect sizes that can be detected using the study design and sample identified above. Previous literature noted that 59.8% of patients with COPD in a similar cohort experienced ≥1 moderate-severe exacerbation in the 12 months prior to initiation of MITT.7 Using an estimated COPD exacerbation rate of 50% in the 12 months prior to FF/UMEC/VI initiation, correlation of 0.44 between pairs, and a sample size of 900, we had 80% power to detect a COPD exacerbation rate effect size reduction of −4.4% after initiation of FF/UMEC/VI using a one-sided test.
Results
Study Population
A total of 912 patients were eligible for inclusion in the study and were included in the analysis. Patients had a mean (standard deviation [SD]) age of 71.2 (8.1) years, with 34.5% in the 75+ age group. In addition, 51.2% of patients were female and 88.1% had Medicare coverage. Patients had a mean (SD) baseline Charlson comorbidity score of 2.2 (1.6) and mean (SD) COPD severity score was 36.2 (10.1) (severe COPD indicated by a score >51.75).8 Most common comorbidities were other lower respiratory disease (83.2%), hypertension (76.2%), and lipid metabolism disorders (71.3%). Patient demographic and baseline clinical characteristics are reported in Table 1.
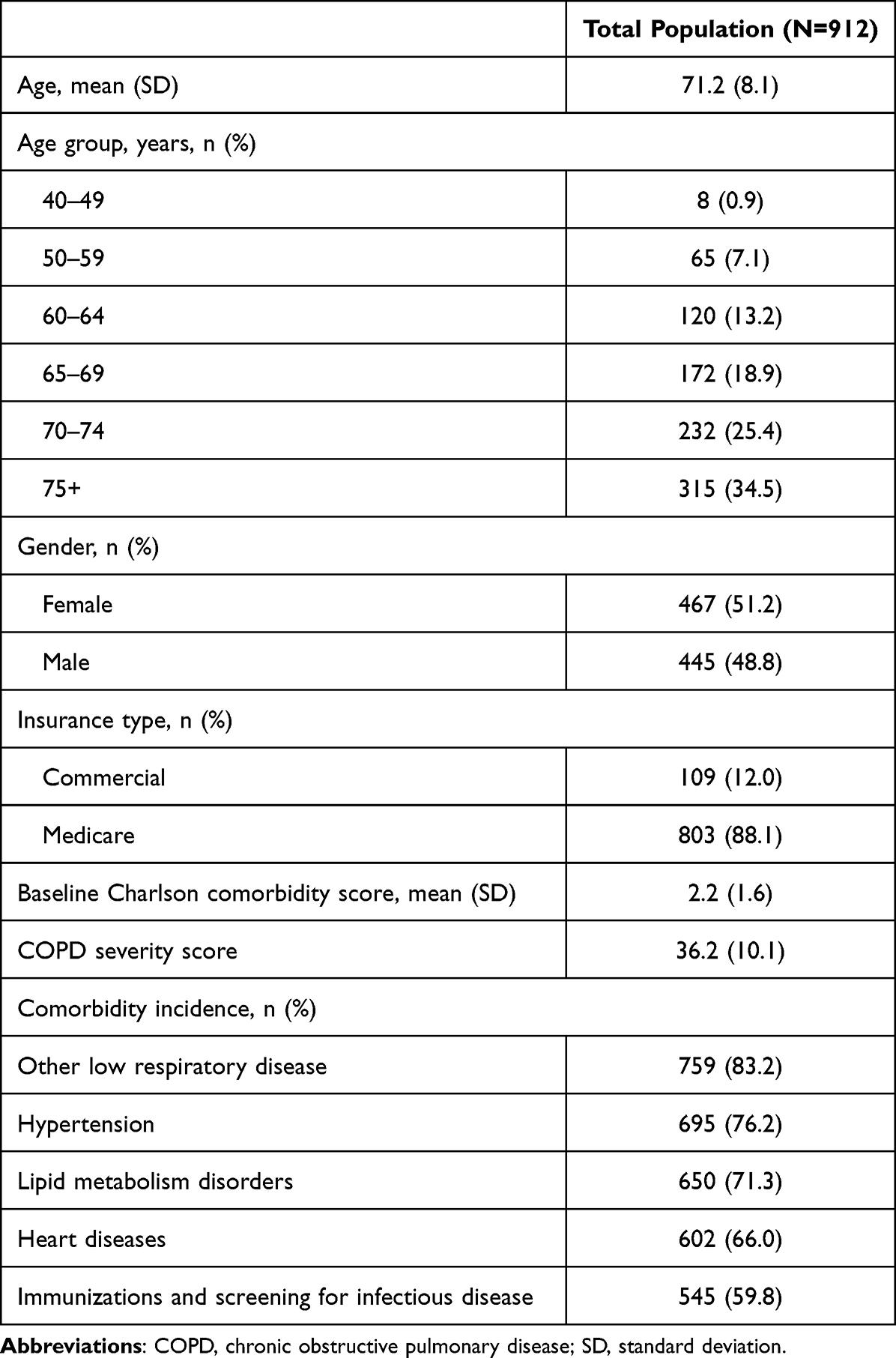 |
Table 1 Patient Demographic and Baseline Clinical Characteristics |
The most common baseline medications were ICS/LABA (90.7% with ≥1 fill), LAMA (88.8% with ≥1 fill), and short-acting beta agonists (SABA; 75.9% with ≥1 fill) (Table 2). During follow-up, patients had FF/UMEC/VI for an average of 274 days.
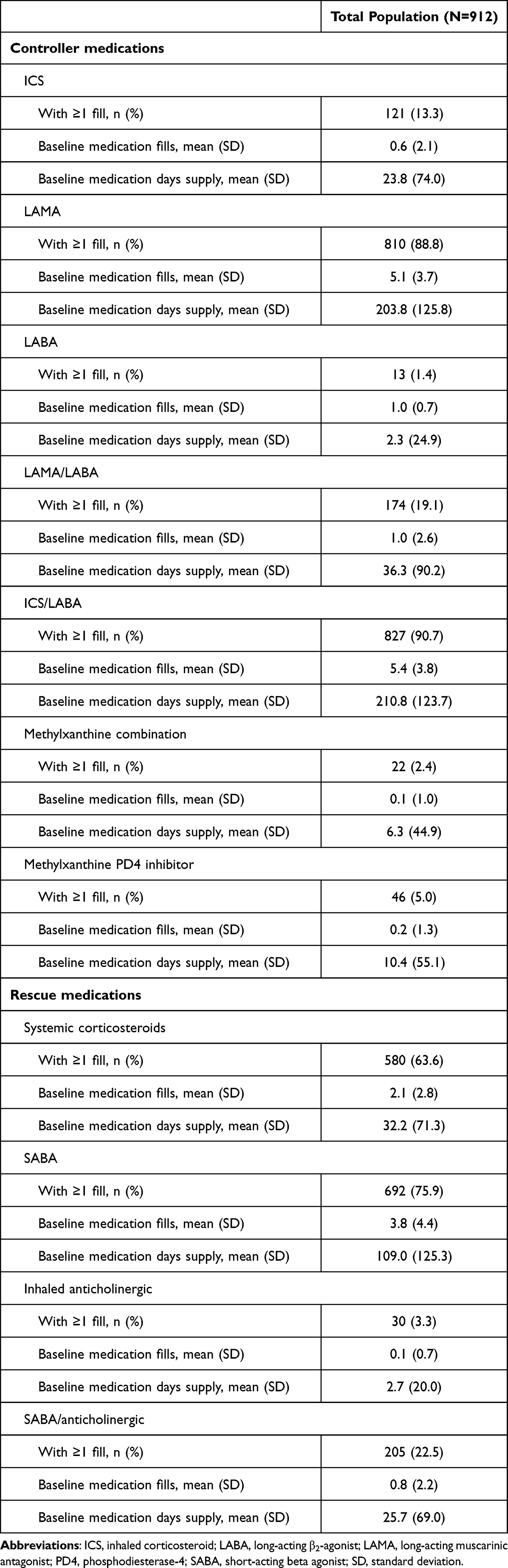 |
Table 2 Baseline Medications |
COPD Exacerbations
The mean count of total COPD exacerbations (moderate or severe) per patient was statistically significantly lower in the follow-up period compared to the baseline period (1.2 vs 1.4, p=0.001) (Table 3, Figure 1). The proportion of patients with ≥1 COPD exacerbation was also statistically significantly lower in the follow-up period compared to baseline (56.4% vs 62.4%, p=0.001).
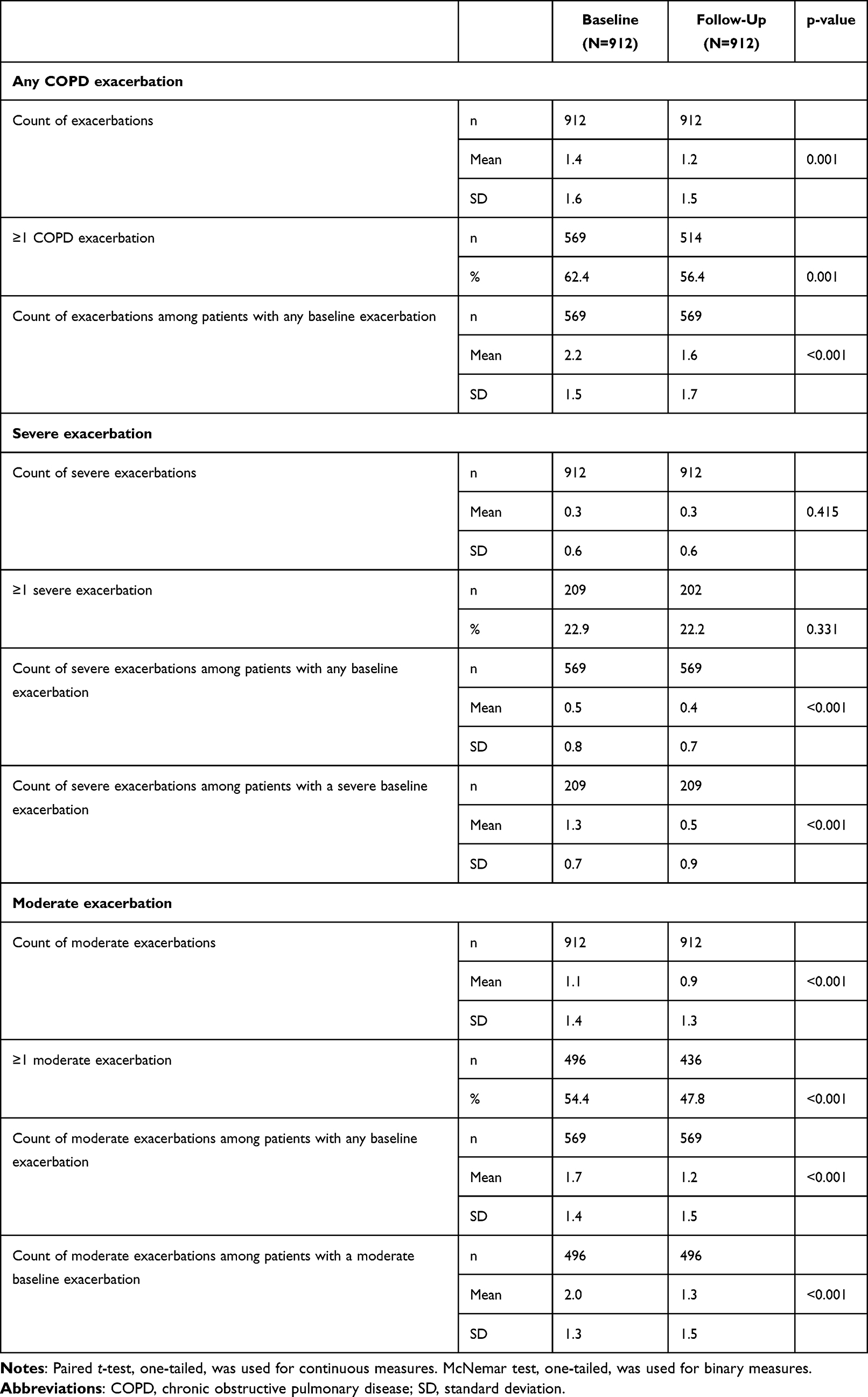 |
Table 3 COPD Exacerbations in the Follow-Up versus Baseline Period |
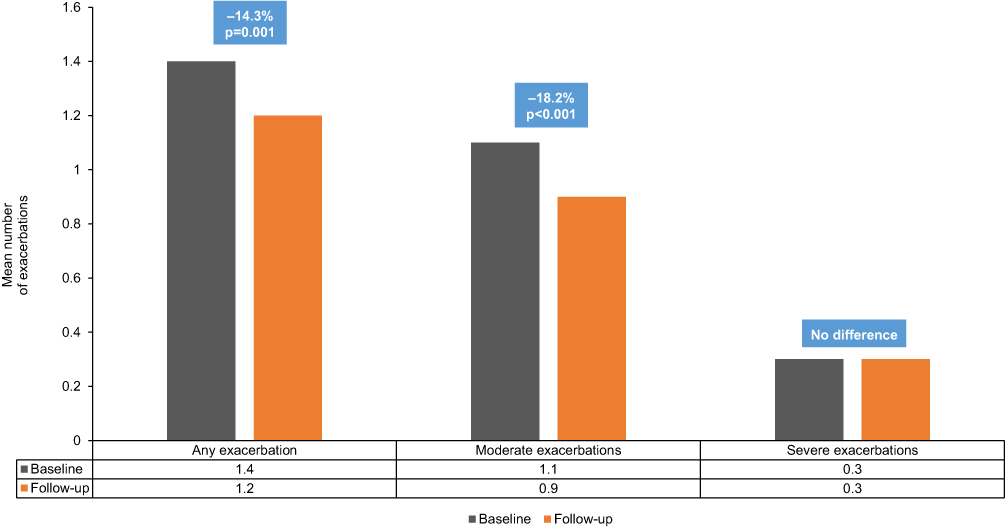 |
Figure 1 Mean Exacerbations Among Entire Cohort (n=912) in the Baseline versus Follow-Up Period. Abbreviations: FF, fluticasone furoate; MITT, multiple-inhaler triple therapy; UMEC, umeclidinium; VI, vilanterol. Note: Any exacerbation includes both moderate and severe exacerbations. |
These differences were mainly driven by moderate COPD exacerbations, with both the mean count of moderate COPD exacerbations and the proportion of patients with ≥1 moderate COPD exacerbation being statistically significantly lower in the follow-up period compared to baseline (mean count: 0.9 vs 1.1, p<0.001; proportion: 47.8% vs 54.4%, p<0.001). Among the entire study cohort, there was no statistically significant difference in either the mean count of severe COPD exacerbation or the proportion of patients with ≥1 severe COPD exacerbation (mean count: 0.3 vs 0.3, p=0.415; proportion: 22.2% vs 22.9%, p=0.331).
Among patients who had any baseline COPD exacerbation (n=569), the mean count (per patient) of any, moderate, and severe COPD exacerbations was statistically significantly lower in the follow-up period compared to baseline (any: 1.6 vs 2.2, p<0.001; moderate: 1.2 vs 1.7, p<0.001; severe: 0.4 vs 0.5, p<0.001) (Figure 2). In addition, rates of severe exacerbation were significantly reduced among patients with a severe baseline exacerbation (n=209) after initiating FF/UMEC/VI (1.3 vs 0.5, p<0.001). Rates of moderate exacerbation were also significantly reduced among those with a moderate baseline exacerbation (n=496) in the follow-up versus baseline period (2.0 vs 1.3, p<0.001).
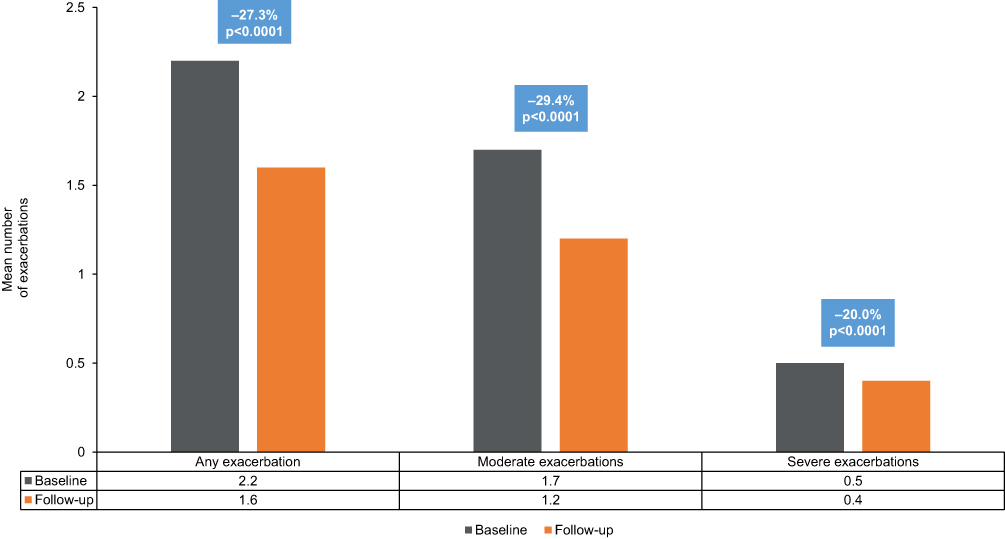 |
Figure 2 Mean Exacerbations Among Patients with Any Pre-Index Exacerbation (n=569) in the Baseline versus Follow-Up Period. Abbreviations: FF, fluticasone furoate; MITT, multiple-inhaler triple therapy; UMEC, umeclidinium; VI, vilanterol. Note: Any exacerbation includes both moderate and severe exacerbations. |
COPD Exacerbation-Related Costs
Mean average costs per moderate COPD-related exacerbation episode were statistically significantly lower during the follow-up period than the baseline period ($175.59 vs $217.69, p=0.018) (Table 4). Mean total costs of all moderate COPD-related exacerbation episodes per patient were also lower during follow-up but this difference did not reach statistical significance ($380.43 vs $445.12, p=0.066).
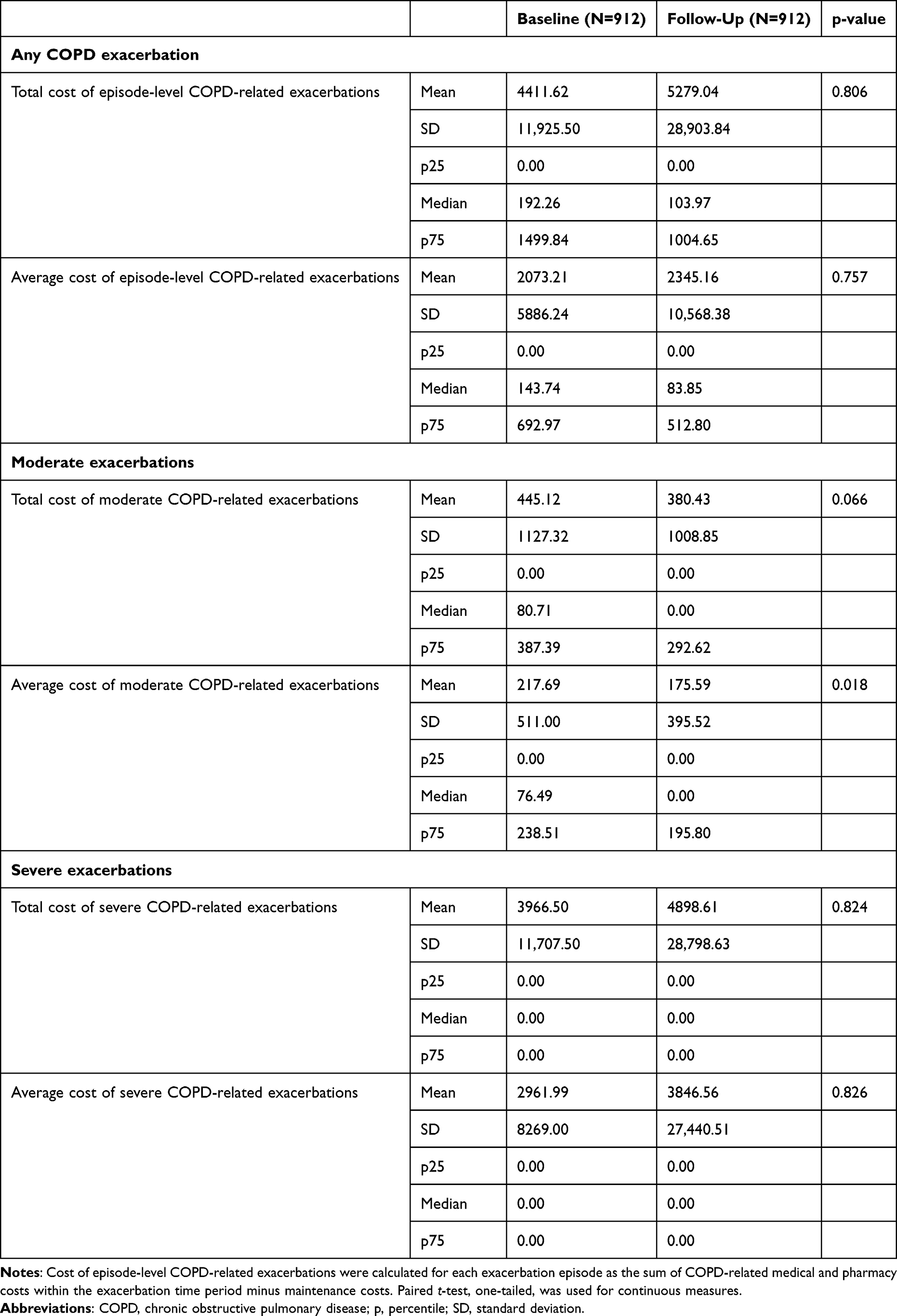 |
Table 4 COPD Exacerbation-Related Costs in the Follow-Up versus Baseline Period |
Mean total cost of all COPD exacerbation episodes per patient was higher during follow-up compared to baseline ($5279.04 vs $4411.62, p=0.806), as were mean average costs of episode-level COPD-related exacerbations ($2345.16 vs $2073.21, p=0.757).
Mean total and mean average costs of severe COPD-related exacerbations were also higher in the follow-up period compared to baseline ($4898.61 vs $3966.50, p=0.824 and $3846.56 vs $2961.99, p=0.826, respectively).
All-Cause and COPD-Related HCRU
The proportion of patients with all-cause utilization in all categories (ambulatory visit [including office visit and outpatient visit], ER visit, inpatient stay, and pharmacy use) were similar between follow-up and baseline (Supplementary Table 2). The mean count of utilization among most categories was also not statistically significantly different during follow-up compared to baseline, with the exception of pharmacy fills (60.2 vs 65.5, p<0.001).
For COPD-related HCRU, a statistically significantly lower proportion of patients had COPD-related ambulatory visits during the follow-up period compared to baseline (85.6% vs 90.7%, p<0.001), which was mainly driven by office visits (79.9% vs 85.1%, p<0.001) (Supplementary Table 3). The proportions of patients with COPD-related utilization in other categories were not statistically significantly different between baseline and follow-up.
The mean count of COPD-related utilization was also not statistically significantly different amongst categories, except for office visit and pharmacy fills. Mean count of office visits and pharmacy visits were statistically significantly lower in the follow-up period compared to baseline (office visit: 2.7 vs 3.1, p<0.001; pharmacy fills: 17.8 vs 23.0, p<0.001).
All-Cause and COPD-Related Health Care Costs
All-cause mean pharmacy costs were statistically significantly lower during follow-up compared to baseline ($11,410.24 vs $12,274.11, p=0.005) (Supplementary Table 4). There were no statistically significant differences in all-cause costs in other categories. Mean medical costs, and mean costs of individual components of the medical costs (eg ambulatory, ER, or inpatient costs) were higher in the follow-up period compared to baseline. Median costs were either lower or very similar in the follow-up period compared to baseline.
For COPD-related health care costs, mean office visit costs, ER visit costs, and pharmacy costs were statistically significantly lower during follow-up compared to baseline (office visit: $289.90 vs $361.59, p<0.001; ER visit: $140.71 vs $195.05, p=0.019; pharmacy costs: $5538.59 vs $6703.94, p<0.001) (Supplementary Table 5). Mean total COPD-related costs were slightly lower in the follow-up period compared to baseline ($11,803.13 vs $11,955.26, p=0.440) whereas mean COPD-related medical costs and inpatient costs were higher in the follow-up period (medical costs: $6264.53 vs $5251.31, p=0.844; inpatient costs: $4745.15 vs $3712.50, p=0.851). Median costs were either lower or very similar in the follow-up period compared to baseline.
Discussion
In this real-world, retrospective analysis of patients who initiated FF/UMEC/VI in a single device, patients had a statistically significant reduction in total COPD exacerbations (moderate or severe) after (vs before) initiation of FF/UMEC/VI. The proportion of patients with ≥1 COPD exacerbation was also statistically significantly lower in the follow-up period compared to baseline. These data support the use of FF/UMEC/VI among patients at risk of exacerbation.
These results are consistent with clinical studies comparing FF/UMEC/VI to either dual therapy, or to MITT.4,9 For example, results from the INTREPID trial, a randomized, open-label, phase IV effectiveness study, showed that in usual clinical care, treatment with FF/UMEC/VI resulted in significantly more patients with health status improvements, and greater lung function benefit, versus MITT.4 Two additional studies comparing FF/UMEC/VI with MITT found that SITT with FF/UMEC/VI was non-inferior to MITT with no differences observed in health status outcomes, suggesting that once-daily SITT is a viable option for simplification of treatment regimens for patients with COPD.10 Future studies should seek to better understand the impact of adherence to FF/UMEC/VI on exacerbation outcomes.
In addition, patients had statistically significantly lower counts of all-cause and COPD-related pharmacy fills. All-cause pharmacy costs were also statistically significantly lower in the follow-up period compared to baseline, alongside COPD-related office visit costs, ER visit costs, and pharmacy costs. Results from this study provided evidence that, alongside decreasing incidence of COPD exacerbations, switching from MITT to FF/UMEC/VI also resulted in improvements in some HCRU and cost outcomes.
This study had several strengths. Firstly, the ORD used as the data source is generally representative of a geographically diverse sample of the US commercial and Medicare Advantage insured population. In addition, the study design filled an important gap in the literature by comparing outcomes among patients who were on MITT (although users were likely non-adherent) and switched to FF/UMEC/VI, rather than comparing patients on either treatment. By doing so, this study added to the growing evidence base of the efficacy and effectiveness of FF/UMEC/VI in patients with COPD in clinical and real-world settings.
There are several limitations which should be considered. Variable definitions were based on the presence of codes on administrative claims; however, the presence of a code does not guarantee that the patient has the diagnosis, underwent the procedure, or took the medication. Results may also not be generalizable to the overall population. The algorithm used to identify COPD exacerbations may result in non-differential misclassification of exacerbation events, although the algorithm is based on a validation study.11 As there was no comparison cohort, these findings may be due to reasons other than the initiation of FF/UMEC/VI. Patients who switched from MITT to FF/UMEC/VI may have had other reasons for this switch beyond exacerbations, such as symptoms, cost, or ease of use. Unfortunately, claims-based analyses preclude detailed examination of the rationale for medication discontinuation or initiation (eg, patient preferences). In addition, we did not adjust for multiple comparisons. Finally, this was an observational study, and causation cannot therefore be proven.
Conclusions
In a real-world setting, patients who were treated with MITT and subsequently initiated FF/UMEC/VI had significant reductions in the rate of total COPD exacerbations (moderate or severe). Patients who had an exacerbation prior to initiating FF/UMEC/VI had significant reductions in the rates of any, moderate, or severe COPD exacerbations after initiation. In addition, some HCRU and cost outcomes were improved following a switch to FF/UMEC/VI. Future studies should examine patient adherence to determine the impact of adherence on exacerbation outcomes.
Abbreviations
COPD, chronic obstructive pulmonary disease; CPI, Consumer Price Index; ER, emergency visit; FDA, United States Food and Drug Administration; FF, fluticasone furoate; FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HCRU, healthcare resource utilization; HIPAA, Health Insurance Portability and Accountability Act; ICD, International Classification of Diseases; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; MAPD, Medicare Advantage with Part D; MITT, multiple-inhaler triple therapy; ORD, Optum Research Database; p, percentile; PD4, phosphodiesterase-4; SABA, short-acting beta agonist; SD, standard deviation; SITT, single-inhaler triple therapy; UMEC, umeclidinium; US, United States; VI, vilanterol.
Data Sharing Statement
The data held in our database contains proprietary elements owned by Optum and therefore cannot be broadly disclosed or made publicly available at this time. The disclosure of these data to third-party clients assumes certain data security and privacy protocols are in place and that the third-party client has executed Optum’s standard license agreement which includes restrictive covenants governing the use of the data.
Ethics Approval and Informed Consent
This study complied with all applicable laws regarding subject privacy. No direct subject contact or primary collection of individual human subject data occurred. Study results are in tabular form and presented as aggregate analyses that omit subject identification, therefore informed consent, ethics committee, or IRB approval was not required. Any publications and reports do not include subject identifiers.
Acknowledgments
Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing, and referencing) was provided by Kathryn Wardle of Aura, a division of Spirit Medical Communications Group Limited, and was funded by GSK. These data have been previously presented in abstract/presentation form at the American College of Chest Physicians – CHEST Conference, virtual meeting, October 17–20, 2021: Bogart M, Ismaila A, Bangalore M, Bunner S, Bengtson L. COPD exacerbations in patients switched from multiple-inhaler triple therapy to FF/UMEC/VI. Chest. 2021;160(4):A1830.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the manuscript; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by GSK (study number 213946). The sponsor was involved in study conception and design, data interpretation, and the decision to submit the article for publication. The sponsor was also given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Disclosure
The authors declare the following conflicts of interest during the last three years in relation to this manuscript: NAH reports research support from AstraZeneca, Boehringer Ingelheim, Genentech, GSK, Novartis, and Sanofi; and is a consultant for Amgen, AstraZeneca, Boehringer Ingelheim, GSK, Novartis, Regeneron Pharmaceuticals, Inc., Sanofi, and Teva. LGSB is an employee of Optum, which received research funds from GSK to conduct this study, although not for manuscript development. SHB was an employee of Optum at the time of study conduct. ASI is an employee of and holds stocks/shares in GSK. ASI is also an unpaid part-time professor at McMaster University, Hamilton, ON, Canada. MB was a permanent employee of, and held stock/shares in, GSK at the time of study conduct. He is now an employee of Gilead Sciences, Foster City, CA, USA. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Chronic obstructive pulmonary disease (COPD); 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD) [Homepage on the Internet]. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease - 2022 report; 2022. Available from: https://goldcopd.org/2022-gold-reports/.
3. Lipson DA, Barnacle H, Birk R, et al. FULFIL trial: once-daily triple therapy for patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;196(4):438–446. doi:10.1164/rccm.201703-0449OC
4. Halpin DMG, Worsley S, Ismaila AS, et al. INTREPID: single- versus multiple-inhaler triple therapy for COPD in usual clinical practice. ERJ Open Res. 2021;7(2):00950–02020. doi:10.1183/23120541.00950-2020
5. Mannino D, Bogart M, Wu B, et al. Adherence and persistence to once-daily single-inhaler versus multiple-inhaler triple therapy among patients with chronic obstructive pulmonary disease in the USA: a real-world study. Respir Med. 2022;197:106807. doi:10.1016/j.rmed.2022.106807
6. US Food and Drug Administration (FDA) [Internet]. Trelegy Ellipta (fluticasone furoate 100 mcg, umeclidinium 62.5 mcg, and vilanterol 25 mcg) inhalation powder approval letter; 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/209482Orig1s000Approv.pdf.
7. Bogart M, Stanford RH, Reinsch T, et al. Clinical characteristics and medication patterns in patients with COPD prior to initiation of triple therapy with ICS/LAMA/LABA: a retrospective study. Resp Med. 2018;142:73–80. doi:10.1016/j.rmed.2018.07.009
8. Wu EQ, Birnbaum HG, Cifaldi M, Kang Y, Mallet D, Colice G. Development of a COPD severity score. Curr Med Res Opin. 2006;22(9):1679–1687. doi:10.1185/030079906X115621
9. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
10. Ferguson GT, Brown N, Compton C, et al. Once-daily single-inhaler versus twice-daily multiple-inhaler triple therapy in patients with COPD: lung function and health status results from two replicate randomized controlled trials. Respir Res. 2020;21(1):131. doi:10.1186/s12931-020-01360-w
11. Stanford RH, Engel-Nitz NM, Bancroft T, Essoi B. The identification and cost of acute chronic obstructive pulmonary disease exacerbations in a United States population healthcare claims database. COPD. 2020;17(5):499–508. doi:10.1080/15412555.2020.1817357
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patients with Chronic Obstructive Pulmonary Disease and Evidence of Eosinophilic Inflammation Experience Exacerbations Despite Receiving Maximal Inhaled Maintenance Therapy
Chen S, Miravitlles M, Rhee CK, Pavord ID, Jones R, Carter V, Emmanuel B, Alacqua M, Price DB
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2187-2200
Published Date: 9 September 2022
Outcomes Following Initiation of Triple Therapy with Fluticasone Furoate/Umeclidinium/Vilanterol versus Multiple-Inhaler Triple Therapy Among Medicare Advantage with Part D Beneficiaries and Those Commercially Enrolled for Health Care Insurance in the United States
Bogart M, Bengtson LG, Johnson MG, Bunner SH, Gronroos NN, DiRocco KK
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:97-110
Published Date: 11 January 2024
Characteristics of Patients Receiving Budesonide/Glycopyrronium/Formoterol for Chronic Obstructive Pulmonary Disease in Spain: The AURA Study
Calle Rubio M, Trigueros Carrero JA, Chaparro Briones P, Escudero Herrera L, Pollack M, Hernández Subirá I, Sánchez-Covisa J
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:999-1008
Published Date: 9 April 2025
Cost-Effectiveness of Single-Inhaler Versus Multiple-Inhaler Triple Therapy in COPD: A German Healthcare Perspective
Beeh KM, Claussen J, Shah D, Martin A, Kendall R, Dasari P, Ismaila AS, Noorduyn SG
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2011-2022
Published Date: 19 June 2025
In Silico Lung Deposition Profiles of Three Single-Inhaler Triple Therapies in Patients with COPD Using Functional Respiratory Imaging
Singh D, Roche N, Wu L, Sadafi H, De Backer J, Monshi Tousi N, Marshall J
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2103-2116
Published Date: 27 June 2025