Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Characteristics of Patients Receiving Budesonide/Glycopyrronium/Formoterol for Chronic Obstructive Pulmonary Disease in Spain: The AURA Study
Authors Calle Rubio M ![]() , Trigueros Carrero JA
, Trigueros Carrero JA ![]() , Chaparro Briones P
, Chaparro Briones P ![]() , Escudero Herrera L, Pollack M
, Escudero Herrera L, Pollack M ![]() , Hernández Subirá I, Sánchez-Covisa J
, Hernández Subirá I, Sánchez-Covisa J ![]()
Received 5 August 2024
Accepted for publication 21 March 2025
Published 9 April 2025 Volume 2025:20 Pages 999—1008
DOI https://doi.org/10.2147/COPD.S490227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Myriam Calle Rubio,1 Juan Antonio Trigueros Carrero,2 Paula Chaparro Briones,3 Luciano Escudero Herrera,3 Michael Pollack,4 Ignacio Hernández Subirá,5 Joaquín Sánchez-Covisa3
1Pneumology Service, H. Clínico San Carlos. Institute for Health Research (IdISSC), Department of Medicine, Complutense University, CIBER de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, Madrid, Spain; 2Buenavista Primary Care Center, Toledo, Spain; 3AstraZeneca Farmacéutica Spain, Madrid, Spain; 4AstraZeneca, LP. BioPharmaceuticals Medical, Wilmington, DE, USA; 5Atrys Health SA, HEOR, Madrid, Spain
Correspondence: Joaquín Sánchez-Covisa, Email [email protected]
Background: Single-inhaler triple therapy with budesonide/glycopyrronium/formoterol fumarate (BGF; Trixeo Aerosphere®) was approved in the European Union in December 2020 for maintenance treatment in adult patients with moderate to severe chronic obstructive pulmonary disease (COPD) who are not adequately treated by dual therapy, and has been available in Spain since February 2022. This real-world, observational, retrospective cohort study, AURA Spain, describes the demographics, clinical characteristics, and healthcare resource utilization of patients initiating single-inhaler BGF triple therapy.
Methods: Electronic medical records in the Spanish Healthcare System anonymized, integrated BIG-PAC® database were analyzed to identify COPD patients aged ≥ 40 years initiating single-inhaler BGF between 1 February 2022 and 31 January 2023.
Results: Patients (N=482) had a mean (standard deviation, SD) age of 71.5 (10.0) years, mean BMI of 29.6 (6.2) kg/m2, most were aged ≥ 65 years (73.7%) and male (62.5%). Most were former (62.7%) or current (24.5%) smokers. Applying GOLD FEV1 thresholds, severity of COPD was moderate in 49.8% of patients, severe (41.9%), and very severe (6.5%). The most common comorbidities were hypertension (62.2%), dyslipidemia (56.8%), and anxiety (42.5%), and 85.9% had one or more cardiovascular-related comorbidity. Overall, 57.3% experienced at least one moderate or severe exacerbation in the 12-month baseline period, 9.5% visited the emergency department for COPD-related reasons; and 12.7% were hospitalized for COPD (median length of stay 7 [interquartile range: 6– 8] days). Patients initiating single-inhaled BGF triple therapy escalated from monotherapy (2.3%) or dual therapy (62.7%), switched from other triple therapies (31.3%), or were treatment-naïve (3.7%).
Conclusion: Single-inhaler BGF triple therapy was initiated mostly as an escalation from dual maintenance therapy, with many switching from triple therapy, in patients with a high burden of disease, as demonstrated by their frequent exacerbation profile, advanced COPD severity (moderate to very severe obstruction) and the high frequency of several comorbidities, including cardiovascular diseases.
Keywords: budesonide/glycopyrronium/formoterol, chronic obstructive pulmonary disease, exacerbations, real-world data, single-inhaler triple therapy
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent respiratory symptoms such as dyspnea, cough, sputum production and/or acute respiratory events (exacerbations), and persistent, often progressive, restricted airflow.1 Globally, COPD accounted for 3.23 million deaths in 2019.2
The estimated prevalence of COPD in Spain, assessed by spirometry evaluation of more than 9000 subjects in the general population aged 40 years or older is 11.8% and is higher in males (14.6%) than females (9.4%).3 This equates to approximately 3.3 million people (1.9/1.4 million males/females) living with COPD.4 National epidemiological studies suggest that COPD is significantly underdiagnosed (by approximately 78%) in Spain, especially in women and younger populations.3,5 In Spain, COPD is the third leading cause of death (behind ischemic heart disease and stroke), accounting for over 7% of all deaths nationally in 2019, ie, more than 31,000 deaths. Despite advances in therapy, COPD-related deaths have increased by 42% from 1990 (47.7 per 100,000) to 2019 (67.9 per 100,000).6
GOLD guidelines recommend triple therapy with an inhaled corticosteroid (ICS), long-acting muscarinic antagonist (LAMA) and long-acting β2-agonist (LABA) as first-line pharmacological treatment for patients with COPD with ≥2 moderate exacerbations or ≥1 exacerbation leading to hospitalization and with an eosinophil count ≥300 cells/μL. The use of inhaled triple therapy has been recommended as a treatment escalation strategy in COPD patients who, despite receiving dual therapy, still have clinically significant symptoms that adversely impact their quality of life or those who have a higher risk of exacerbation. Triple therapy improves lung function, patient-reported outcomes and reduces exacerbations when compared to LAMA alone, LAMA + LABA, and LABA + ICS.1,7 Spanish COPD guidelines (GesEPOC) also recommend ICS/LAMA/LABA triple therapy in patients with exacerbations despite treatment with LABA/LAMA.8 Single-inhaler triple therapy (SITT) improves adherence and persistence compared with multiple-inhaler triple therapy (MITT)9–11 and reduces healthcare resource utilization and improves cost-effectiveness compared with multiple inhalers.11,12
Single-inhaler budesonide/glycopyrronium/formoterol fumarate (BGF; Trixeo Aerosphere®) was efficacious when compared with the corresponding dual therapies for symptomatic patients with moderate to very severe COPD.13 Furthermore, in the 52-week ETHOS clinical trial of patients with moderate to very severe COPD who had experienced ≥1 moderate/severe exacerbation in the previous year, single inhaler BGF at two dose levels of inhaled glucocorticoid (budesonide, 320 or 160 μg) reduced the rate of moderate or severe COPD exacerbations and improved lung function compared to glycopyrronium-formoterol or budesonide-formoterol dual therapy.14,15 In the Phase 3 ETHOS clinical trial, single inhaler higher-dose glucocorticoid BGF (320 μg budesonide) reduced all-cause mortality compared with glycopyrronium/formoterol.16 In addition, recent results from the SKOPOS-MAZI retrospective study showed that BGF reduced the risk of all-cause mortality compared with MITT in a real-world setting.17 Fixed-dose triple therapy with BGF was approved in the European Union (EU) in December 2020 for maintenance treatment in adult patients with moderate to severe COPD who are not adequately treated by a combination of an ICS + LABA, or a combination of a LABA + LAMA.18 BGF is the third fixed, triple combination therapy approved in the EU for COPD and has been available in Spain since February 2022.
Since the launch of BGF, there is a lack of real-world data on characteristics of patients initiating BGF triple therapy. This retrospective, non-interventional, observational study (AURA Spain) aimed to evaluate demographics, clinical characteristics, and healthcare resource utilization among patients with COPD in Spain who initiated BGF triple therapy.
Methods
Study Design
This was a real-world, retrospective, observational cohort study comprising longitudinal analyses of electronic medical records (EMRs). This study was approved by the Ethics Committee of Consorci Sanitari of Terrassa on 24th of July 2023. The study used secondary, fully anonymized data, and consequently there was no need to obtain patient consent.
Objectives
The primary objective of the AURA Spain study was to describe the demographics, clinical characteristics, and healthcare resource utilization of patients with COPD initiating triple therapy with single-inhaler BGF.
Data Source
EMRs contained in the Spanish National Healthcare System integrated BIG-PAC® database were analyzed to identify COPD patients aged ≥40 years initiating single-inhaler BGF triple therapy between 1 February 2022 and 31 January 2023. The anonymized database includes EMRs of approximately 2 million patients and contains information on diagnoses, treatment prescriptions, procedures, and analytical data. The database is certified by Spanish Agency of Medicines and Medical Devices and has age distribution and sex profiles which are similar to the Spanish population.19
Study Population
Patients with COPD aged 40 years or older, and diagnosed by one or more ICD-9 (491.x, 492.x and 496) or ICD-10 codes (J41.x, J42, J43.x, and J44.x) (Supplementary Table 1), who initiated single-inhaler BGF triple therapy between 1 February 2022 and 31 January 2023, were included in the study. Patients were required to have a minimum patient history of 12 months before the index date.
Study Measures
Study measures were patient demographics; clinical characteristics and healthcare resource utilization during the 12-month baseline period (12 months prior to the index date); treatment history and index prescriber specialty.
Acute Exacerbation Definitions
A moderate acute exacerbation of COPD was defined as an outpatient visit to the general practitioner (GP) or pulmonologist with a diagnosis code for COPD; and a dispensation for an oral corticosteroid (OCS [glucocorticoids]; ATC codes H02AB) and/or antibiotics (ATC code J01) within 5 days following the visit, for a maximum duration of 15 days. A severe acute exacerbation of COPD was defined as an emergency department visit or hospitalization, and with a primary or secondary discharge diagnosis code for acute exacerbation of COPD (ICD-9: 491.21; ICD-10: J44.0 or J44.1).
Statistical Analysis
The database was searched using customized SQL scripts, and retrieved data were validated by frequency distribution and careful review to identify possible recording or coding errors.
Continuous variables were described by mean, standard deviation (SD), median, interquartile range (IQR), minimum and maximum, and categorical variables by number and percentage. Data were analyzed using RStudio, version 4.3.1 and Microsoft Excel.
Results
Patients initiating single-inhaler BGF triple therapy (N = 482) had a mean (SD) age of 71.5 (10.0) years, most were aged ≥65 years (73.7%) and were mainly male (62.5%). Most BGF initiators were former (62.7%) or current (24.5%) smokers, and patients with available data had a mean (SD) BMI of 29.6 (6.2) kg/m2 (n = 283); FEV1 predicted of 50.8 (14.5) and FEV1/FVC of 0.6 (0.1) (n = 430); and an eosinophil count of 293.6 (98.4) cells/μL (n = 422). Applying GOLD FEV1 thresholds,7 almost half of patients with available data (214/430; 49.8%) had moderate COPD (FEV1 predicted 50–79%), 41.9% had severe (FEV1 predicted 30–49%) and 6.5% very severe (FEV1 predicted <30%) COPD. The most common comorbidities were hypertension (62.2%), dyslipidemia (56.8%), anxiety (42.5%), and diabetes (27.8%). Overall, 85.9% of the cohort had one or more cardiovascular-related comorbidity. Mean Charlson Comorbidity Index (CCI) and Elixhauser Comorbidity Index (ECI) values were 1.9 and 7.6, respectively (Table 1).
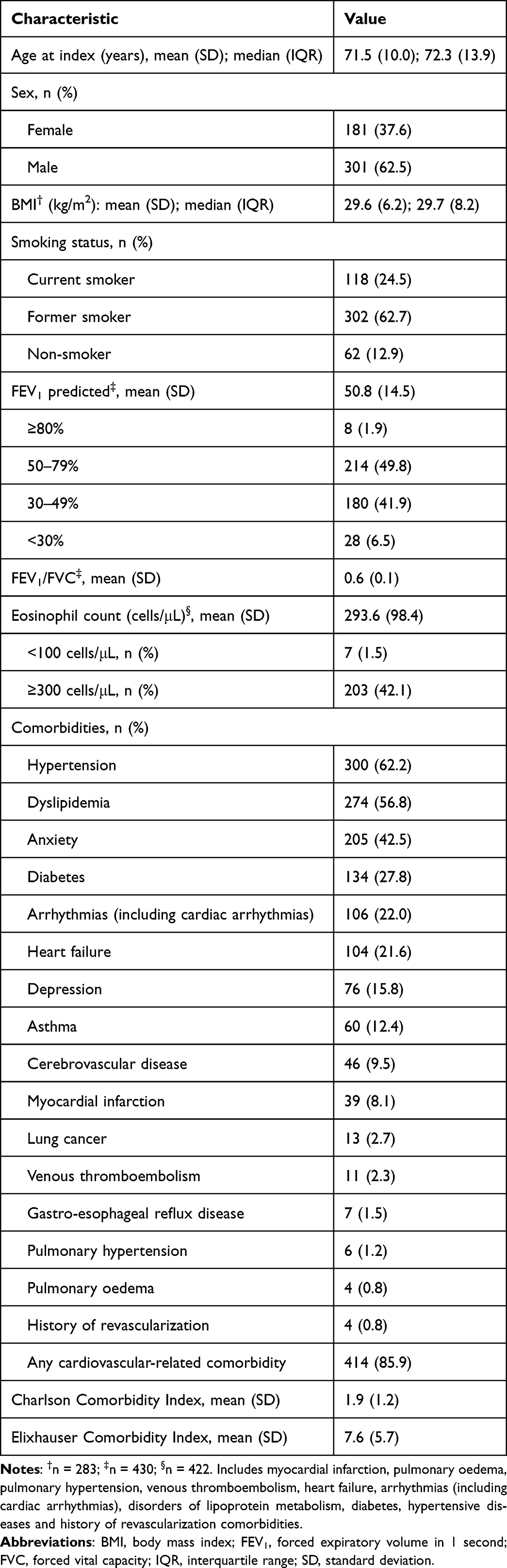 |
Table 1 Demographics and Baseline Clinical Characteristics of Cohort (N = 482) |
More than half of all patients (57.3%; n = 276) experienced at least one moderate or severe exacerbation in the previous 12 months. The mean (SD) number of moderate/severe exacerbations among all initiators was 1.6 (1.9), and 23.9% of patients experienced ≥3 moderate/severe exacerbations. A total of 232 patients (48.1%) experienced one or more moderate exacerbations and the mean (SD) number of moderate exacerbations per patient was 1.3 (1.8). At least one severe exacerbation was experienced by 86 patients (17.8%) and the mean (SD) number of severe exacerbations per patient was 0.2 (0.6) (Table 2).
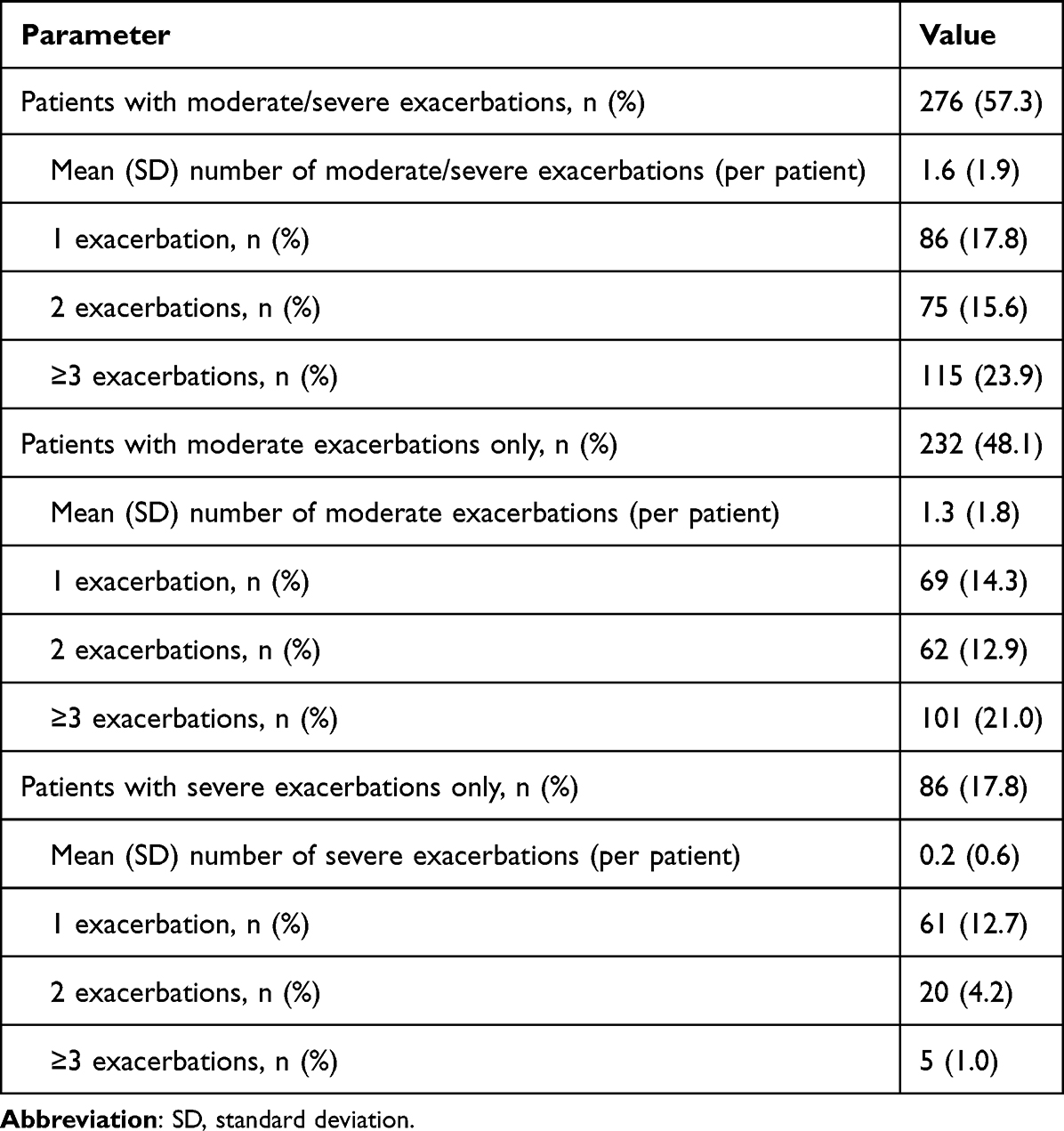 |
Table 2 Patients with Moderate/Severe Exacerbations in the Previous 12 months (N = 482) |
Healthcare resource utilization during the 12-month baseline period is shown in Table 3. Nearly all patients (99.2%) visited a GP and the mean (SD) number of visits to a GP was 15.4 (11.9). In contrast, less than half of all patients visited a pulmonologist (45.9%) and had a mean (SD) number of 0.8 (0.9) visits per patient. Approximately a tenth of all patients (9.5%) visited the emergency department for COPD-related reasons, but a higher proportion (12.7%) were hospitalized for COPD. The median length of stay in hospital was 7 (interquartile range, IQR: 6–8) days.
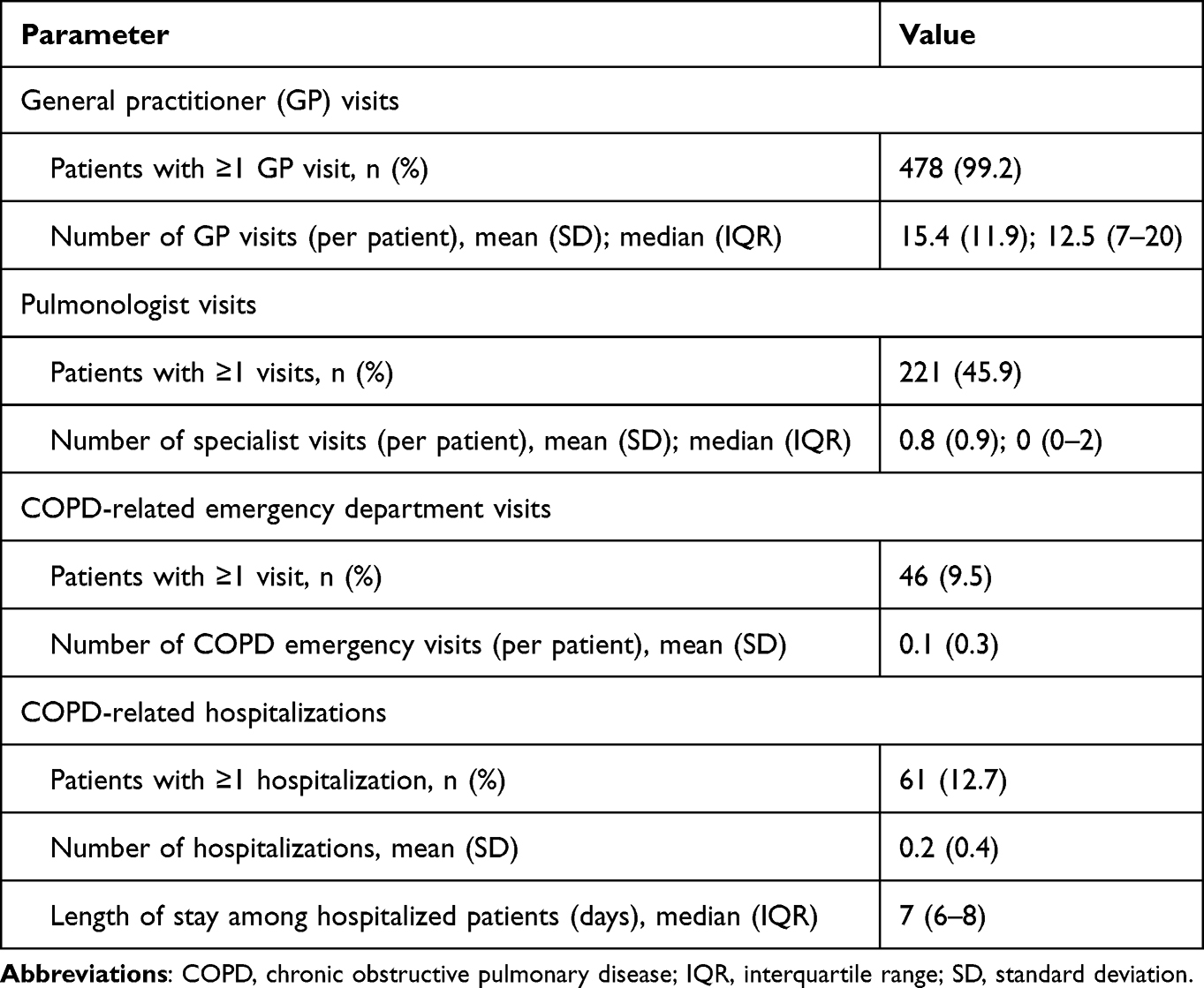 |
Table 3 Healthcare Resource Utilization During the 12-month Baseline Period (N = 482) |
Physicians prescribing SITT/MITT were mainly GPs (52.7%; n = 254) and pneumologists (44.2%; n = 213), with fewer prescribers in internal medicine (2.7%; n = 13) and emergency departments (0.4%; n = 2). Patients initiating single-inhaled BGF triple therapy escalated from monotherapy (n = 11; 2.3%) or dual therapy (n = 302; 62.7%), switched from SITT (n = 67; 13.9%) or MITT (n = 84; 17.4%), or were treatment-naïve (n = 18; 3.7%) (Figure 1). Short-term treatment included use of short-acting beta agonists (SABA) (41.70%; n = 201) or OCS (45.2%; n = 205). Mean (SD) annual total cumulative dose of OCS among patients with ≥1 OCS prescription (n = 218) was 432.4 (629.3) mg, and while most patients (80.3%) received an OCS dose of <500 mg, 19.7% of patients received ≥500 mg OCS during the 12-month baseline period.
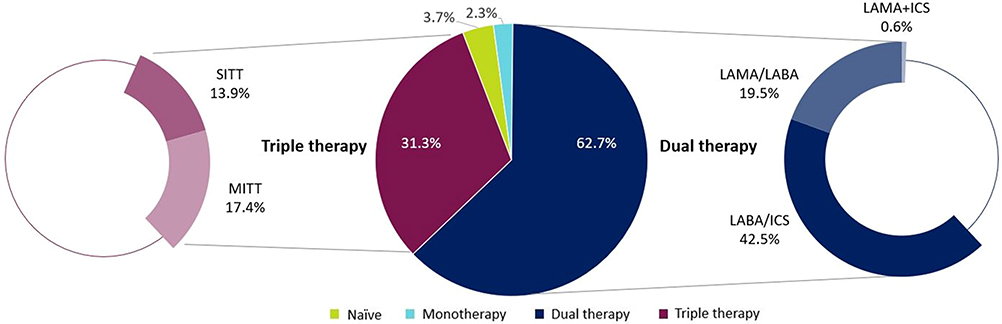 |
Figure 1 Previous treatment. Abbreviations: ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; MITT, multiple-inhaler triple therapy; SITT, single-inhaler triple therapy. |
Discussion
This real-world retrospective cohort study describes baseline characteristics, COPD treatment patterns, history of exacerbations, and healthcare resource use in patients with COPD initiating single-inhaler BGF triple therapy, during the first year since its launch in Spain in February 2022.
Most patients in the study were aged ≥65 years, male, overweight, and had a history of smoking. The prevalence of individual comorbidities, together with CCI and ECI values indicated the presence of multiple long-term conditions, notably cardiovascular-related disorders, with 85.9% of the cohort having at least one cardiovascular-related comorbidity. Cardiovascular disease (CVD) is known to be a common interlinked condition to COPD and COPD patients with CVD have a worse health status, a higher risk of hospitalization, and a poorer prognosis. COPD patients frequently die of respiratory (exacerbations) and cardiovascular causes;20,21 real-world evidence from the EXACOS-CV studies in Spain22 and Italy23 has shown that patients with COPD are at high risk of severe cardiovascular events following exacerbations. Based on GOLD FEV1 thresholds,7 nearly half of the cohort in the current study (48.4%) had severe to very severe COPD and 50% had moderate COPD when initiating BGF. In addition, eosinophil cell counts were high (≥300 cells/μL) in many patients (42.1%).
A significant proportion of patients (57.3%) had at least one exacerbation during the 12-month baseline period, with 48.1% having at least one moderate exacerbation and 17.8% having one or more severe exacerbation. However, these numbers may be underestimated as exacerbations may not be fully recorded in EMRs.24 Furthermore, patients are known to underreport exacerbations and, whether unreported or reported, exacerbations have negative health implications.25 As over half of all patients had one or more exacerbation during the 12-month baseline period, this suggests that their treatment was not optimal, and they may have benefited from earlier treatment escalation. Almost all patients had at least one GP visit and less than half (45.9%) visited a pulmonologist during the 12-month baseline period. This may indicate a lack of access to specialist care and, therefore, delays in timely initiation of BGF or other therapies. Approximately 13% of patients were admitted to hospital for COPD-related reasons, with a median length of stay of 7 days. These results emphasize the high disease burden of COPD prior to the initiation of BGF triple therapy. The AURA USA real-world study of COPD patients initiating BGF also found a high disease burden among patients.26 Despite current therapy, many patients in AURA USA experienced exacerbations and respiratory symptoms, and chronic comorbidities, especially cardiopulmonary-related, were common.26 In a retrospective study of COPD patients initiating SITT (fluticasone furoate/umeclidinium/vilanterol) in the USA, most users experienced persistent symptoms or a history of exacerbations despite dual maintenance therapy, prior to initiating triple therapy.27 The EPOCONSUL 2021 audit of Spanish COPD patients found that triple therapy in high-risk COPD patients was used as escalation therapy in patients with high clinical impact.28 Furthermore, an observational retrospective analysis of Italian administrative healthcare data from the Fondazione Ricerca e Salute database showed that COPD patients receiving triple therapy were older and had more comorbidities, particularly CVD, than patients receiving other treatments, highlighting the high disease burden of these COPD patients.29
The first prescription of BGF was made by GPs in over half of cases (52.7%) and by specialized care physicians, mainly pulmonologists, in the remainder. Dual therapy was the most common previous maintenance treatment prior to escalation to BGF (62.7%), whilst just under one-third of patients (31.3%) switched from other triple therapies (MITT or SITT). This may indicate a lack of effectiveness of these treatment options or a preference for single-inhaler BGF by patients and providers. A high proportion of patients used short-term treatment in the previous year, mainly SABA (41.7%) or OCS (45.2%). With regard to OCS, approximately one-fifth of patients (19.7%) had a dose >500 mg, suggesting that treatment was suboptimal. Although the mean annual cumulative OCS dose was relatively low (432.4 mg), any exposure of OCS in COPD patients significantly increases the risk of adverse outcomes compared with no OCS exposure.30
There are several limitations of this study. Data from EMRs can be incomplete and of variable quality.31 This study validated data by frequency distribution analysis and by careful review to identify possible recording or coding errors. A second limitation is that previous symptoms (eg, dyspnea, cough, sputum production), which may also be a reason for treatment escalation, are not usually recorded by the treating physicians, especially in more severe patients (eg, previously treated with LABA + ICS) and therefore not captured by BIG-PAC®. Although, the presence of respiratory symptoms and/or exacerbations is a primary reason for escalation to triple therapy, the use of secondary data and the descriptive nature of this study precluded any attempt to determine possible reasons for initiating or switching to single-inhaler BGF triple therapy. A third limitation is that while standard algorithms were used to define exacerbations, they may be prone to miscoding24 and patients are known to underreport exacerbations.25
In conclusion, these real-world data from Spain indicate that single-inhaler BGF triple therapy was initiated, mostly as an escalation from dual maintenance therapy, in patients with a high burden of disease, as shown by their frequent exacerbation profile, advanced severity of COPD (moderate to very severe obstruction) and the high frequency of several comorbidities, including cardiovascular-related diseases. Nearly a third of patients switched to BGF from other triple therapies, possibly indicating a lack of effectiveness or preference for single-inhaler BGF by patients and providers. Based on these characteristics, there may be merit in clinicians considering escalating to SITT earlier in the patient journey. Ongoing and future studies will aim to describe real-world clinical outcomes with single-inhaler BGF triple therapy.
Data Sharing Statement
All the data generated or analyzed during this study are included in the article. Requests for further information should be sent to the corresponding author.
Ethical Approval
This study was approved by the Ethics Committee of Consorci Sanitari of Terrassa on 24th of July 2023. The study used secondary, fully anonymized data, and consequently there was no need to obtain patient consent.
Acknowledgments
Under the direction of the authors, medical writing support was provided by Robert A. Furlong PhD and David P. Figgitt PhD, CMPP™, Content Ed Net, with funding from AstraZeneca Spain.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was sponsored by AstraZeneca.
Disclosure
M.C.R. has received speaker fees from AstraZeneca, Bial, Chiesi, CSL Behring, GlaxoSmithKline, Menarini and Grifols, and consulting fees from GlaxoSmithKline and Bial. J.A.T.C. has received speaker fees from AstraZeneca, Chiesi, GlaxoSmithKline, Menarini and Orion. P.C.B., L.E.H., M.P. and J.S-C. are employees of AstraZeneca and may hold stock and/or stock options in the company. I.H.S. is an employee of Atrys Health, which was contracted by AstraZeneca to conduct this study. The authors report no conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Pulmonary Disease. Global initiative for chronic obstructive lung disease: 2023 report. 2023. Available from: https://goldcopd.org/2023-gold-report-2/.
2. World Health Organization. Chronic obstructive pulmonary disease (COPD). 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
3. Soriano JB, Alfageme I, Miravitlles M, et al. Prevalence and determinants of COPD in Spain: EPISCAN II. Arch Bronconeumol. 2021;57(1):61–69. doi:10.1016/j.arbres.2020.07.024
4. National Statistics Institute. Advance of the municipal register at 1st January 2022. Provisional results, National. 2024. Available from: https://www.ine.es/jaxi/Tabla.htm?path=/t20/e245/p04/provi/l1/&file=00000002.px&L=1.
5. García Castillo E, Alonso Pérez T, Peláez A, et al. Trends of COPD in Spain: changes between cross sectional surveys 1997, 2007 and 2017. Arch Bronconeumol. 2023;59(3):142–151. doi:10.1016/j.arbres.2022.11.014
6. Lazarus JV, Ortiz A, Tyrovolas S, et al. A GBD 2019 study of health and sustainable development goal gains and forecasts to 2030 in Spain. Sci Rep. 2022;12(1):21154. doi:10.1038/s41598-022-24719-z
7. Agustí A, Sisó-Almirall A, Roman M, Vogelmeier CF. members of the Scientific Committee of GOLD (Appendix). Gold 2023: highlights for primary care. NPJ Prim Care Respir Med. 2023;33(1):28. doi:10.1038/s41533-023-00349-4
8. Miravitlles M, Calle M, Molina J, et al. Spanish COPD Guidelines (GesEPOC) 2021: updated Pharmacological treatment of stable COPD. Arch Bronconeumol. 2022;58(1):69–81. doi:10.1016/j.arbres.2021.03.005
9. Mannino D, Bogart M, Wu B, et al. Adherence and persistence to once-daily single-inhaler versus multiple-inhaler triple therapy among patients with chronic obstructive pulmonary disease in the USA: a real-world study. Respir Med. 2022;197:106807. doi:10.1016/j.rmed.2022.106807
10. Halpin DMG, Rothnie KJ, Banks V, et al. Comparative adherence and persistence of single- and multiple-inhaler triple therapies among patients with chronic obstructive pulmonary disease in an English real-world primary care setting. Int J Chron Obstruct Pulmon Dis. 2022;17:2417–2429. doi:10.2147/COPD.S370540
11. Alcázar-Navarrete B, Jamart L, Sánchez-Covisa J, Juárez M, Graefenhain R, Sicras-Mainar A. Clinical characteristics, treatment persistence, and outcomes among patients with COPD treated with single- or multiple-inhaler triple therapy: a retrospective analysis in Spain. Chest. 2022;162(5):1017–1029. doi:10.1016/j.chest.2022.06.033
12. Zhang S, King D, Rosen VM, Ismaila AS. Impact of single combination inhaler versus multiple inhalers to deliver the same medications for patients with asthma or COPD: a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:417–438. doi:10.2147/COPD.S234823
13. Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, phase 3 randomised controlled trial. Lancet Respir Med. 2018;6(10):747–758. doi:10.1016/S2213-2600(18)30327-8
14. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
15. Rabe KF, Martinez FJ, Singh D, et al. Improvements in lung function with budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler versus dual therapies in patients with COPD: a sub-study of the ETHOS trial. Ther Adv Respir Dis. 2021;15:17534666211034329. doi:10.1177/17534666211034329
16. Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced all-cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease. a randomized, double-blind, multicenter, parallel-group study. Am J Respir Crit Care Med. 2021;203(5):553–564. doi:10.1164/rccm.202006-2618OC
17. Pollack M, Rapsomaniki E, Anzueto A, et al. Reduced risk of mortality for COPD patients associated with initiation of treatment with single inhaler triple therapy (Budesonide/Glycopyrrolate/Formoterol) versus multiple inhaler triple therapy in the United States: the MAZI Study. Am J Respir Crit Care Med. 2024;209:A3822. doi:10.1164/ajrccm-conference.2024.209.1_MeetingAbstracts.A3822
18. European Medicines Agency. Trixeo Aerosphere; formoterol / glycopyrronium bromide / budesonide. 2023. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/trixeo-aerosphere.
19. Sicras-Mainar A, Enriquez JL, Hernández I, Sicras-Navarro A, Aymerich T, Leon M. PMU146 Validation and representativeness of the Spanish BIG-PAC database: integrated computerized medical records for research into epidemiology, medicines and health resource use (real world evidence). Value Health. 2019;22(Suppl 3):S734.
20. de Miguel-Díez J, Núñez Villota J, Santos Pérez S, et al. Multidisciplinary management of patients with chronic obstructive pulmonary disease and cardiovascular disease. Arch Bronconeumol. 2024;60(4):226–237. doi:10.1016/j.arbres.2024.01.013
21. Singh D, Han MK, Hawkins NM, et al. Implications of cardiopulmonary risk for the management of COPD: a narrative review. Adv Ther. 2024;41(6):2151–2167. doi:10.1007/s12325-024-02855-4
22. Santos S, Manito N, Sánchez-Covisa J, et al. Risk of severe cardiovascular events following COPD exacerbations: results from the EXACOS-CV study in Spain. Rev Esp Cardiol. 2024;25. doi:10.1016/j.rec.2024.06.003
23. Calabria S, Ronconi G, Dondi L, et al. Cardiovascular events after exacerbations of chronic obstructive pulmonary disease: results from the EXAcerbations of COPD and their OutcomeS in CardioVascular diseases study in Italy. Eur J Intern Med. 2024;127:97–104. doi:10.1016/j.ejim.2024.04.021
24. Rothnie KJ, Müllerová H, Hurst JR, et al. Validation of the recording of acute exacerbations of COPD in UK primary care electronic healthcare records. PLoS One. 2016;11(3):e0151357. doi:10.1371/journal.pone.0151357
25. Jones P, Alzaabi A, Casas Herrera A, et al. Understanding the gaps in the reporting of COPD exacerbations by patients: a review. COPD. 2024;21(1):2316594. doi:10.1080/15412555.2024.2316594
26. Portillo EC, Pollack M, Lee I, et al. Characteristics of initiators of budesonide/glycopyrrolate/formoterol for treatment of chronic obstructive pulmonary disease (COPD) in the United States: the AURA study. Ther Adv Respir Dis. 2023;17:17534666231164534. doi:10.1177/17534666231164534
27. Wu B, Mannino D, Mu G, Stiegler M, Bogart M. Patient and clinical demographics of new users to single-inhaler triple therapy in patients with chronic obstructive pulmonary disease. Pulm Ther. 2022;8(2):195–208. doi:10.1007/s41030-022-00189-6
28. Calle Rubio M, Miravitlles M, López-Campos JL, et al. Inhaled maintenance therapy in the follow-up of COPD in outpatient respiratory clinics. factors related to inhaled corticosteroid use. EPOCONSUL 2021 audit. Arch Bronconeumol. 2023;59(11):725–735. doi:10.1016/j.arbres.2023.07.015
29. Dondi L, Ronconi G, Calabria S, et al. Clinical characteristics, use and switch of drugs for obstructive airway diseases among patients with COPD experiencing an exacerbation: a retrospective analysis of Italian administrative healthcare data. BMC Pulm Med. 2024;24(1):525. doi:10.1186/s12890-024-03339-5
30. Tse G, Emmanuel B, Ariti C, et al. A long-term study of adverse outcomes associated with oral corticosteroid use in COPD. Int J Chron Obstruct Pulmon Dis. 2023;18:2565–2580. doi:10.2147/COPD.S433326
31. Chan KS, Fowles JB, Weiner JP. Review: electronic health records and the reliability and validity of quality measures: a review of the literature. Med Care Res Rev. 2010;67(5):503–527. doi:10.1177/1077558709359007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patients with Chronic Obstructive Pulmonary Disease and Evidence of Eosinophilic Inflammation Experience Exacerbations Despite Receiving Maximal Inhaled Maintenance Therapy
Chen S, Miravitlles M, Rhee CK, Pavord ID, Jones R, Carter V, Emmanuel B, Alacqua M, Price DB
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2187-2200
Published Date: 9 September 2022
COPD Exacerbations, Costs, and Health Care Resource Utilization Before and After Initiation of Fluticasone Furoate/Umeclidinium/Vilanterol in Routine Care in the USA
Hanania NA, Bunner SH, Bengtson LGS, Ismaila AS, Bogart M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:407-418
Published Date: 24 March 2023
Outcomes Following Initiation of Triple Therapy with Fluticasone Furoate/Umeclidinium/Vilanterol versus Multiple-Inhaler Triple Therapy Among Medicare Advantage with Part D Beneficiaries and Those Commercially Enrolled for Health Care Insurance in the United States
Bogart M, Bengtson LG, Johnson MG, Bunner SH, Gronroos NN, DiRocco KK
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:97-110
Published Date: 11 January 2024
Burden of Exacerbations in Patients Newly Initiating an Inhaled Regimen for COPD: A Claims Analysis
Sethi S, Wan ES, Tejwani V, Lamprey C, Aggarwal K, Dixon A, Pan Y, Siddharthan T
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1829-1842
Published Date: 7 June 2025
In Silico Lung Deposition Profiles of Three Single-Inhaler Triple Therapies in Patients with COPD Using Functional Respiratory Imaging
Singh D, Roche N, Wu L, Sadafi H, De Backer J, Monshi Tousi N, Marshall J
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2103-2116
Published Date: 27 June 2025