")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Outcomes Following Initiation of Triple Therapy with Fluticasone Furoate/Umeclidinium/Vilanterol versus Multiple-Inhaler Triple Therapy Among Medicare Advantage with Part D Beneficiaries and Those Commercially Enrolled for Health Care Insurance in the United States
Authors Bogart M, Bengtson LG, Johnson MG , Bunner SH , Gronroos NN , DiRocco KK
Received 20 July 2023
Accepted for publication 15 December 2023
Published 11 January 2024 Volume 2024:19 Pages 97—110
DOI https://doi.org/10.2147/COPD.S424497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Russell
Michael Bogart,1 Lindsay GS Bengtson,2 Mary G Johnson,2 Scott H Bunner,2 Noelle N Gronroos,2 Kristi K DiRocco3
1US Value Evidence & Outcomes, R&D US, GSK, Research Triangle Park, NC, USA; 2Health Economics and Outcomes Research, Optum, Eden Prairie, MN, USA; 3USA, Medical Affairs, GSK, Collegeville, PA, USA
Correspondence: Kristi K DiRocco, US Medical Affairs, GSK, 1250 S. Collegeville Road, Collegeville, PA, 19426, USA, Tel +1 610-412-7175, Email [email protected]
Purpose: Patients with chronic obstructive pulmonary disease (COPD) have been shown to benefit from triple therapy commonly delivered by multiple-inhaler triple therapy (MITT); however, the complexity of MITT regimens may decrease patient adherence. Fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI), a once-daily single-inhaler triple therapy (SITT), became available in the United States (US) in 2017, but real-world data comparing outcomes for SITT versus MITT are currently limited. This study compared outcomes among patients with COPD initiating MITT versus SITT with FF/UMEC/VI who were either Medicare Advantage with Part D (MAPD) beneficiaries or commercial enrollees in the US.
Methods: Retrospective study using administrative claims data from the Optum Research Database for patients with COPD who initiated FF/UMEC/VI or MITT between September 1, 2017, and March 31, 2019 (index date: first pharmacy claim for FF/UMEC/VI cohort; earliest day of ≥ 30 consecutive days-long period of overlap in the day’s supply of all triple therapy components for MITT cohort). COPD exacerbations, adherence to triple therapy, and all-cause and COPD-related health care resource utilization (HCRU) and costs were compared between FF/UMEC/VI and MITT initiators.
Results: In total, 4659 FF/UMEC/VI initiators and 9845 MITT initiators for the MAPD population, and 821 FF/UMEC/VI initiators and 1893 MITT initiators for the commercial population were included in the study. MAPD beneficiaries initiating FF/UMEC/VI had a significantly lower annual rate of severe exacerbations compared to MITT initiators (0.26 vs 0.29; p=0.014). They also had a significantly higher mean adherence (proportion of days covered) (0.51 vs 0.37; p< 0.001) and significantly lower all-cause and COPD-related inpatient stays compared to MITT initiators ([32.02% vs 34.27%; p=0.017], [16.09% vs 17.72%; p=0.037]). Trends were similar among the commercial population, but the results were not statistically significant.
Conclusion: FF/UMEC/VI initiators had significantly fewer severe exacerbations, higher triple therapy adherence, and lower HCRU costs compared to MITT initiators for MAPD beneficiaries.
Plain Language Summary: Triple therapy for chronic obstructive pulmonary disease (COPD) includes the use of several inhalers daily in a respiratory therapy combination known as multiple-inhaler triple therapy (MITT), which can be challenging for patients. However, treatment can be simplified by combining these therapies into just one inhaler, in a respiratory therapy combination known as single-inhaler triple therapy (SITT). As there is currently limited information comparing treatment outcomes in patients using SITT versus those using MITT in the real world, in this study we included Medicare Advantage with Part D (MAPD) beneficiaries and commercial enrollees with COPD who started using either an SITT combination of fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) or MITT. More specifically, we looked at flare-ups in COPD symptoms (known as exacerbations), percentage of days that a patient had their medication on hand (known as treatment adherence), and health care utilization and costs. The study was conducted using administrative claims data between September 1, 2016, and March 31, 2020 from the Optum Research Database. For patients who had MAPD insurance, individuals who started FF/UMEC/VI experienced fewer severe exacerbations and increased treatment adherence, as compared to those who started MITT. They also had lower health care utilization and costs compared to those using MITT. Similar results were observed for patients who were commercially enrolled, albeit lacking statistical significance. Overall, the findings of this study indicate that triple therapy with FF/UMEC/VI can improve exacerbations and treatment adherence in patients with COPD and decrease health care utilization and associated costs.
Keywords: chronic obstructive pulmonary disease, triple therapy, multiple-inhaler triple therapy, single-inhaler triple therapy, adherence, exacerbations
Introduction
The Global Initiative for Chronic Obstructive Lung Disease recommendations suggest the use of triple therapy for patients with chronic obstructive pulmonary disease (COPD) with persistent symptoms and risk of exacerbations.1 Patients with COPD on triple therapy have been shown to experience improved lung function and health-related quality of life as well as lower hospitalization rates.2–6 However, evidence suggests that the complexity of multiple-inhaler regimens may decrease patient adherence.7–11
Fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) was approved by the United States (US) Food and Drug Administration in 2017 as single-inhaler triple therapy (SITT) for the treatment of COPD.12 While several studies have shown baseline characteristics to be similar in patients using SITT and MITT,13–15 there are limited data comparing patient outcomes for SITT versus MITT.13,16,17 In 2020, an international study showed that once-daily SITT with FF/UMEC/VI provided similar overall improvements in health status, and a similar safety profile as MITT with twice-daily budesonide/formoterol and once-daily tiotropium.13 Moreover, the real-world INTREPID study showed that FF/UMEC/VI improved lung function and quality of life in patients with COPD compared to MITT.16
The current study was therefore designed to compare outcomes among patients diagnosed with COPD who initiated MITT versus SITT (comprised of FF/UMEC/VI), in two separate populations: Medicare Advantage with Part D (MAPD) beneficiaries and those commercially enrolled for health care insurance in the US.
Methods
Study Design and Data Source
This was a retrospective study of MAPD beneficiaries and commercial enrollees analyzed as separate populations, with the MAPD beneficiaries being the primary population of interest. MAPD beneficiaries were patients who received optional prescription drug coverage through their Medicare insurance. The study uses administrative claims data from the Optum Research Database (ORD) during the period from September 1, 2016, through March 31, 2020 (Figure 1). The ORD is a large US health care claims database with fully adjudicated medical and pharmacy claims and linked enrolment information since 1993 on more than 73 million lives.
 |
Figure 1 Study design diagram. Abbreviations: FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol; MITT, multiple-inhaler triple therapy. |
The study index date was the date of first prescription for FF/UMEC/VI or the earliest day of ≥30 consecutive days-long period of overlap in the day’s supply with all three triple therapy components on hand (for the MITT cohort). The patient identification period was September 1, 2017, through March 31, 2019. Patients were continuously enrolled in the 12 months before the index date (baseline period) and the 12 months after the index date (follow-up period). The index date was included in the baseline period. Propensity score methods were used to account for confounding bias.
Study Population
Eligible patients were ≥40 years of age at index and were required to have ≥1 pharmacy claim for triple therapy during the patient identification period, and ≥2 claims with a diagnosis code for COPD in any position on separate dates of service during the study period. Patients were excluded if they had ≥1 day of overlapping days’ supply with an inhaled corticosteroid (ICS), long-acting beta-agonist (LABA), and long-acting muscarinic antagonist (LAMA) (ie MITT) during the baseline period, excluding the index date; ≥1 medical claim with a diagnosis code for cystic fibrosis, lung cancer, or alpha-1 antitrypsin deficiency during the study period; pharmacy claims for both MITT and FF/UMEC/VI on the index date; and unknown age, sex, geographic region, or insurance type.
Study Objectives
The following study objectives have been considered for both the primary (MAPD beneficiaries) and the secondary (commercial enrollees) populations of interest. The primary objective was to compare COPD exacerbation rates (any, severe, moderate) between patients with COPD who initiated triple therapy with FF/UMEC/VI versus triple therapy with MITT. MITT inhalers could have comprised of FF/VI plus a LAMA, or other combinations of ICS, LABA, and LAMA. Severe exacerbations were defined as a hospitalization with a primary diagnosis code of COPD. Moderate exacerbations were defined as an emergency room, physician office, or hospital outpatient visit with a primary diagnosis code of COPD accompanied by an antibiotic or systemic corticosteroid dispensing within 5 days. Secondary objectives were to compare medication adherence between patients with COPD who initiated triple therapy with FF/UMEC/VI versus MITT, and to compare all-cause and COPD-related health care resource utilization (HCRU) between patients with COPD who initiated triple therapy with a single inhaler of FF/UMEC/VI versus multiple inhalers. Adherence was evaluated using proportion of days covered (PDC), which was defined as the number of overlapping days on which medication was available divided by 365 (the number of days between the index date through the end of 12-month follow-up period). The exploratory objective was to compare all-cause and COPD-related health care costs between patients with COPD who initiated triple therapy with FF/UMEC/VI versus MITT.
Data Analysis
Inverse probability of treatment weighting18–21 was used to control for possible confounding of the association between the outcomes and study cohort. Outcomes included: COPD exacerbations, adherence to triple therapy, all-cause and COPD-related HCRU, all-cause and COPD-related costs. The success of the weighting procedure was evaluated by comparing the standardized differences, with ≤10% considered an acceptable threshold for balance. Additionally, the distribution of weights was examined, with no extreme weights found which could have led to increased variance in comparisons of outcomes. Bivariate comparisons were performed by treatment cohort (FF/UMEC/VI vs MITT). Pearson’s chi-square tests were performed for categorical variables and two-sample t-tests were performed for continuous variables. Statistical significance of p-values was based on p<0.05 and was calculated using robust (sandwich) variance estimates to account for weights and correlation due to multiple observations per patient. Means, standard deviations (SDs), and categorical variable statistics were weighted and normalized to the original cohort sizes. Only weighted results are reported.
Results
Patient Attrition
After applying the inclusion and exclusion criteria, the following patient cohorts were included in the study: 4659 FF/UMEC/VI initiators and 9845 MITT initiators for the MAPD population, and 821 FF/UMEC/VI initiators and 1893 MITT initiators for the commercial population. After weighting, all standardized differences were below 10% for baseline COPD exacerbations, all-cause and COPD-related HCRU, and all-cause and COPD-related HCRU costs.
Baseline Patient Characteristics
Baseline characteristics for MAPD beneficiaries were generally similar between FF/UMEC/VI initiators and MITT initiators (Table 1). The mean age was 71.81 (SD 8.70) years for FF/UMEC/VI initiators and 71.66 (SD 8.76) years for MITT initiators, and females represented 58.03% of the FF/UMEC/VI initiators population and 58.02% of the MITT initiators population. The top three most common comorbidities were other lower respiratory diseases (85.57% FF/UMEC/VI; 84.63% MITT; p=0.171), hypertension (83.76% FF/UMEC/VI; 85.17% MITT; p=0.046), and disorders of lipid metabolism (75.96% FF/UMEC/VI; 75.55% MITT; p=0.627). While higher percentages of patients with other nutritional, endocrine, and metabolic disorders (57.59% vs 55.35%; p=0.022), as well as with a history of mental health and substance abuse (45.37% vs 43.23%; p=0.028), were recorded in the FF/UMEC/VI initiators group, compared to the MITT initiators, more patients with hypertension (85.17% vs 83.76%; p=0.046) and other connective tissue disease (53.20% vs 50.77%; p=0.013) were recorded in the MITT initiators group, compared to the FF/UMEC/VI initiators. Maintenance and rescue medication use during baseline was similar between FF/UMEC/VI initiators and MITT initiators. Other common medications taken at baseline by MAPD beneficiaries were COPD-guideline-recommended antibiotics (74.15% FF/UMEC/VI; 73.72% MITT; p=0.616) and oral corticosteroids (64.90% FF/UMEC/VI; 63.24% MITT; p=0.076).
 |
Table 1 Weighted Baseline Characteristics for MAPD Beneficiaries |
Baseline characteristics for the commercial population are reported in Supplementary Table 1.
COPD Exacerbations
Baseline and follow-up COPD exacerbation data for MAPD beneficiaries are shown in Table 2. At follow-up, FF/UMEC/VI initiators had a significantly lower annual rate (0.26 [SD 0.65] vs 0.29 [SD 0.69]; p=0.014), duration (7.44 [SD 21.51] vs 8.80 [SD 23.74]; p=0.002), and cost ($3273.67 [SD $10,863.79] vs $4098.21 [SD $15,612.64]; p<0.001) of severe exacerbations compared to MITT initiators. They also had a significantly lower average cost of any COPD exacerbation compared to MITT initiators ($2453.56 [SD $8988.67] vs $3271.58 [SD $14,080.11]; p<0.001), and a significantly lower risk of moderate exacerbation(s) after month 1 as compared to MITT initiators (p=0.009) (Supplementary Figure 1).
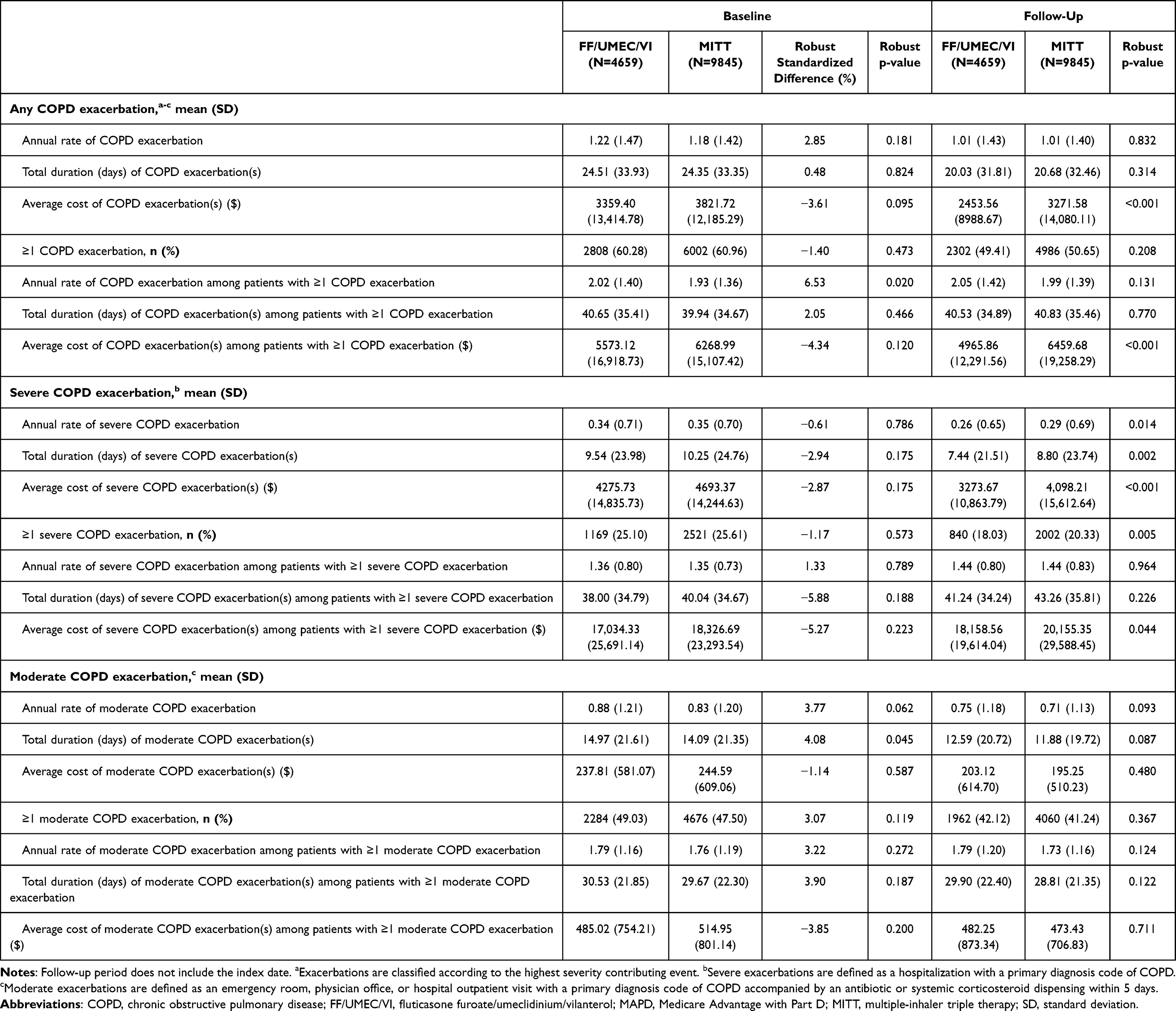 |
Table 2 Weighted COPD Exacerbations for MAPD Beneficiaries |
Results in the commercial population during follow-up were directionally consistent with those in the MAPD population, but the results were not statistically significant (Supplementary Table 2 and Supplementary Figure 2).
Adherence to Triple Therapy
MAPD FF/UMEC/VI initiators had a significantly higher mean PDC during follow-up (0.51 [SD 0.31] vs 0.37 [SD 0.29]; p<0.001), a significantly greater proportion of patients with PDC ≥0.8 (25.99% vs 13.07%; p<0.001), and a significantly lower proportion of patients discontinuing their index medication compared to MITT initiators (65.99% vs 82.16%; p<0.001) (Table 3).
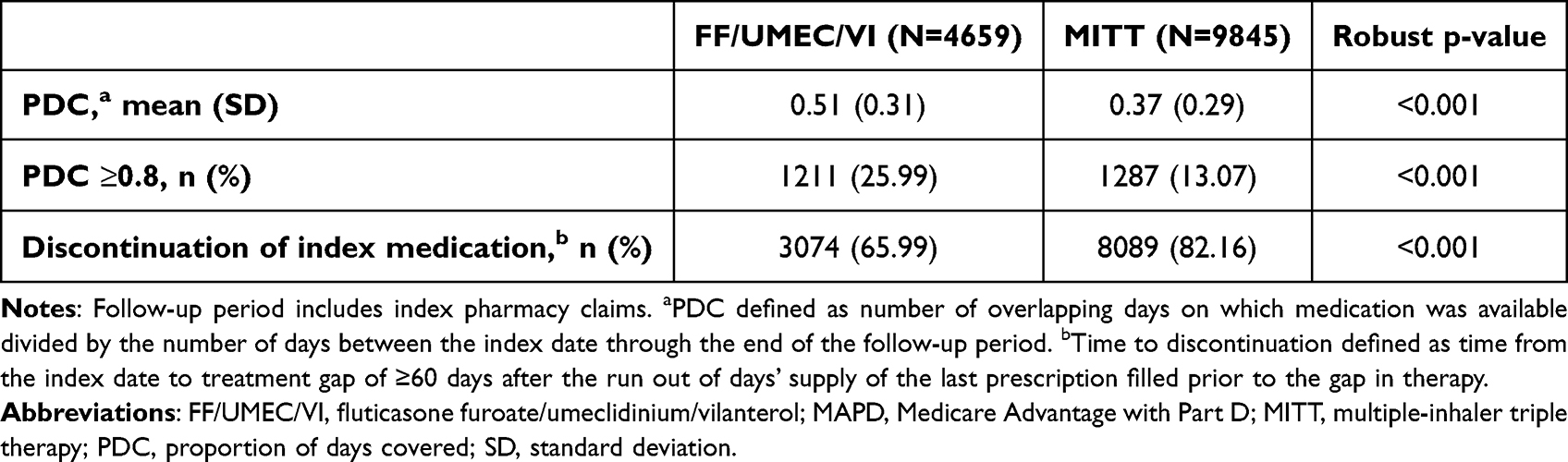 |
Table 3 Weighted Follow-Up Adherence to Triple Therapy for MAPD Beneficiaries |
Results in the commercial population during follow-up were consistent with those in the MAPD population and were statistically significant (Supplementary Table 3).
HCRU
All-Cause HCRU
Baseline and follow-up all-cause HCRU data for MAPD beneficiaries are shown in Table 4. FF/UMEC/VI initiators had a significantly lower proportion of all-cause outpatient (OP) (86.05% vs 87.83%; p=0.006), all-cause emergency room (ER) (52.77% vs 54.88%; p=0.031), and all-cause inpatient (IP) stays (32.02% vs 34.27%; p=0.017) compared to MITT initiators during follow-up. However, FF/UMEC/VI initiators had a significantly higher proportion of patients with all-cause office visits compared to MITT initiators during follow-up (98.73% vs 97.49%; p<0.001).
 |
Table 4 Weighted All-Cause HCRU for MAPD Beneficiaries |
Results in the commercial population were directionally consistent with those in the MAPD population for the proportion of patients with all-cause OP visits, all-cause ER visits, and all-cause IP stays, although the results were not statistically significant (Supplementary Table 4).
COPD-Related HCRU
MAPD FF/UMEC/VI initiators had a significantly lower average proportion of patients with COPD-related IP stays during follow-up compared to MITT initiators (16.09% vs 17.72%; p=0.037) (Table 5). There were no significant differences in the proportion of patients with COPD-related office visits, COPD-related OP visits, COPD-related ER visits, or COPD-related pharmacy use between MITT initiators and FF/UMEC/VI initiators.
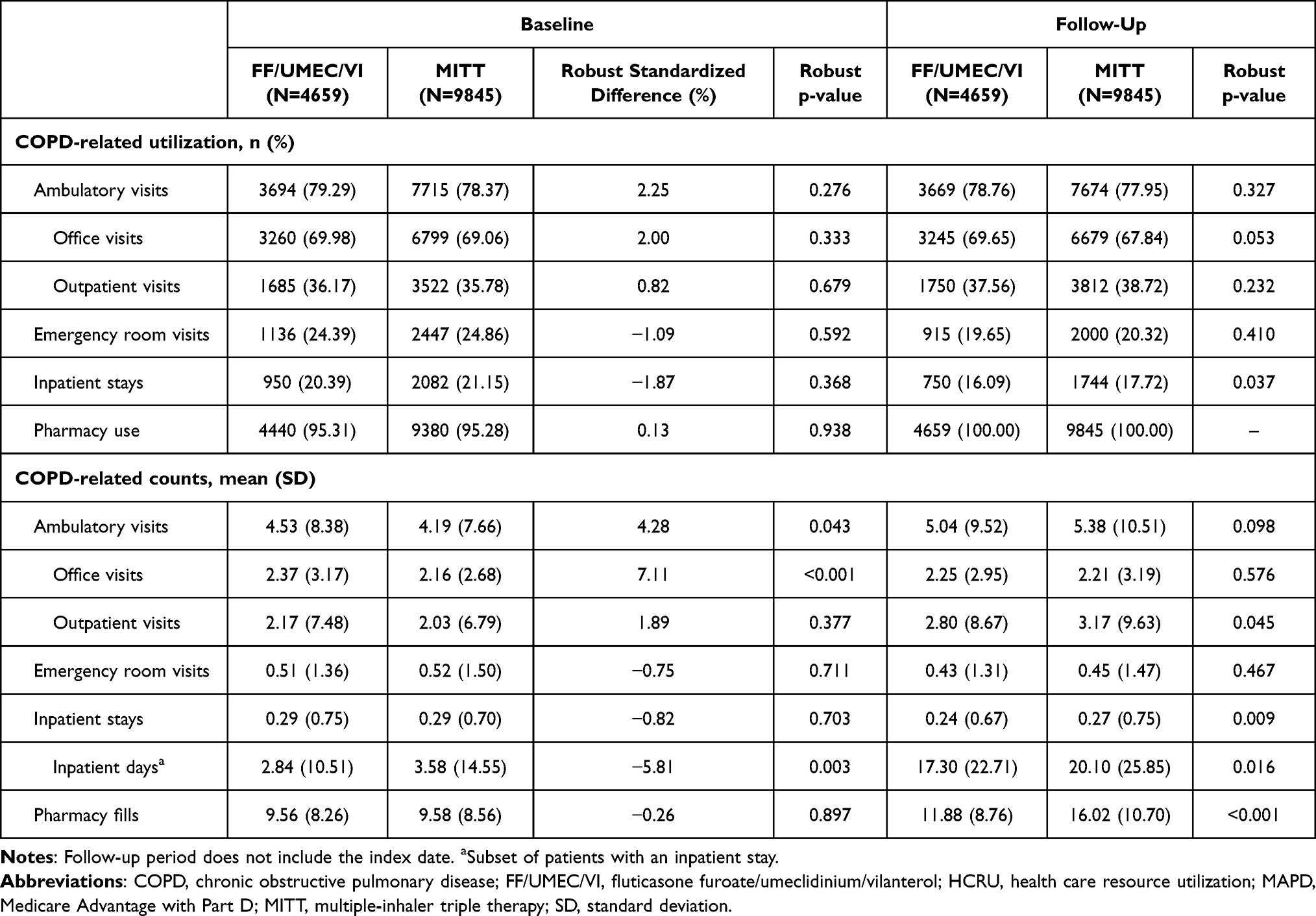 |
Table 5 Weighted COPD-Related HCRU for MAPD Beneficiaries |
Results in the commercial population were directionally consistent with those in the MAPD population for the proportion of patients with COPD-related IP stays during follow-up, although the results were not significant (Supplementary Table 5).
HCRU Costs
All-Cause HCRU Costs
All-cause total (medical and pharmacy) costs were $4096.20 lower for MAPD FF/UMEC/VI initiators ($29,012.99 [SD $35,224.09] vs $33,109.19 [SD $40,942.14]; p<0.001) compared to MITT initiators (Supplementary Table 6). Medical, ambulatory, OP, IP stay, and pharmacy costs were also significantly lower for MAPD FF/UMEC/VI initiators.
Results in the commercial population were directionally consistent with those in the MAPD population, but not statistically significant (Supplementary Table 7).
COPD-Related Costs
COPD-related total (medical and pharmacy) costs were $2171.41 lower for MAPD FF/UMEC/VI initiators ($9338.83 [SD $15,486.81] vs $11,510.24 [SD $17,840.57]; p<0.001) compared to MITT initiators (Supplementary Table 8). Medical, ambulatory, OP, IP stay, and pharmacy costs were also significantly lower for MAPD FF/UMEC/VI initiators.
Commercial FF/UMEC/VI initiators had significantly lower mean COPD-related pharmacy costs compared to MITT initiators ($5400.43 [SD $2637.17] vs $6216.55 [SD $3662.06]; p<0.001). The remaining commercial results were directionally consistent with the MAPD results, but not statistically significant (Supplementary Table 9).
Discussion
This study focused on a population of MAPD beneficiaries as well as on a population of commercially insured patients diagnosed with COPD who initiated FF/UMEC/VI or MITT between September 1, 2017, and March 31, 2019.
For the MAPD beneficiaries, a lower average count of patients with severe COPD exacerbation, fewer patients discontinuing their index medication, and a higher proportion of patients with a PDC ≥0.80 for FF/UMEC/VI initiators were observed when compared to MITT initiators. Also, there were significant differences in all-cause HCRU between FF/UMEC/VI and MITT initiators, with the latter having a smaller proportion of patients with office visits but a greater proportion of patients with OP visits, ER visits, and IP stays. Higher percentages of patients with other nutritional, endocrine, and metabolic disorders, as well as with a history of mental health and substance abuse, were observed for FF/UMEC/VI initiators compared to MITT initiators. That may account for the increased percentage of patients with all-cause office visits in the FF/UMEC/VI initiators group, which did not occur for the COPD-related HCRU. This was generally consistent for COPD-related HCRU as well, although the differences for office visits, OP visits, and ER visits were not statistically significant. Moreover, FF/UMEC/VI initiators had significantly lower all-cause costs compared to MITT initiators for most measured categories. The exceptions were ER costs, office visit costs, and other medical costs, as well as two greater COPD-related HCRU costs, namely the ER visits and other medical costs.
For the commercially insured patients, the FF/UMEC/VI initiators did not have any significant differences in COPD exacerbations (any, severe, or moderate) in terms of the proportion of patients with ≥1 exacerbation, annual rate per patient, duration, cost, or time to exacerbation when compared to MITT initiators. The reason for the lack of significance in the commercially insured population compared to the MAPD population could potentially be that FF/UMEC/VI initiators in the MAPD population presented more opportunity for improvement compared to the commercial FF/UMEC/VI initiators at baseline, as they were older (71.81 years vs 61.74 years), had higher any and severe baseline annual exacerbation rates (any: 60.28% vs 55.43%; severe: 25.10% vs 15.78%), and had higher percentages of patients with hypertension (83.76% vs 65.36%), diseases of the heart (71.91% vs 58.40%) and diabetes mellitus without complications (47.80% vs 34.80%). FF/UMEC/VI initiators experienced a greater mean PDC, a higher proportion of patients with a PDC ≥0.80, and fewer patients discontinuing their index medication compared to MITT initiators. Also, the average count of all-cause OP visits was lower in FF/UMEC/VI initiators compared to MITT initiators for all-cause HCRU. For COPD-related HCRU, FF/UMEC/VI initiators had a lower proportion of patients with a COPD-related OP visit compared to MITT initiators and fewer COPD-related pharmacy fills. The latter translated into significantly lower COPD-related pharmacy costs in FF/UMEC/VI initiators compared to MITT initiators. There were no other significant differences in all-cause or COPD-related costs for commercially insured patients.
The results of this study should be interpreted with the following study limitations in mind. To exclude data during the COVID-19 pandemic in the US, the data included in this study were less contemporary; thus, the patient identification period ended on March 31, 2019, to allow for 12 months of post-index continuous follow-up through March 31, 2020, and the FF/UMEC/VI population included patients who initiated treatment within approximately 18 months of the approval. Consequently, FF/UMEC/VI initiators were relatively early adopters of this therapy who may utilize health care resources differently and may not represent the broader FF/UMEC/VI population. Also, patients were required to be continuously enrolled with medical and pharmacy coverage for 12 months following the index date; this criterion may introduce survival bias by sub-setting to a healthier population of triple therapy initiators who survived for 12 months following treatment initiation. Moreover, the differences between the commercial and MAPD results are likely due to the smaller sample size in the commercial population leading to some analyses being underpowered. Furthermore, the observable increased rates of medication adherence among patients receiving FF/UMEC/VI versus MITT may be due to patients only needing to pay for one medication rather than multiple medications, thus being the more cost-effective option. Nevertheless, the adherence results of this study are consistent with previous literature.14 Lastly, one of the outcomes of interest in this study is adherence, as measured by PDC. There is a lack of consensus on the most appropriate adherence calculation when multiple medications are included in the line of therapy. In this study, a conservative estimate of PDC was calculated by requiring the patient to have all three active ingredients on hand to be considered treated. While this resulted in a lower PDC calculation, it more accurately reflects the number of days that a patient was being treated with all three active ingredients.
Conclusions
In this real-world setting, MAPD beneficiaries initiating once-daily SITT with FF/UMEC/VI had fewer severe exacerbations, higher triple therapy adherence, and lower HCRU and HCRU costs compared to those initiating MITT. The commercial results mainly mirrored the results in the MAPD population, although in general, the results were not statistically significant.
Abbreviations
COPD, chronic obstructive pulmonary disease; ER, emergency room; FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol; HCRU, health care resource utilization; ICS, inhaled corticosteroid; IP, inpatient; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist; MAPD, Medicare Advantage with Part D; MITT, multiple-inhaler triple therapy; OP, outpatient; ORD, Optum Research Database; PDC, proportion of days covered; SABA, short-acting beta-agonist; SAMA, short-acting muscarinic antagonist; SD, standard deviation; SITT, single-inhaler triple therapy; US, United States.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are contained in a database owned by Optum® and are not publicly available and therefore cannot be broadly disclosed or made publicly available at this time. The disclosure of these data to third-party clients assumes certain data security and privacy protocols are in place, and that the third-party client has executed Optum’s standard license agreement which includes restrictive covenants governing the use of the data.
Ethics Approval and Informed Consent
As this was an analysis of claims data, institutional review board (IRB) approval was not required. Per Title 45 of CFR, Part 46 (https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/index.html), the administrative claims data analysis of our study was exempt from the IRB review as it was a retrospective analysis of existing data (hence no patient intervention or interaction), and no patient-identifiable information was included in the claims dataset.
Acknowledgments
Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing, and referencing) was provided by Mirela Panea of Apollo, OPEN Health Communications, and was funded by GSK. The authors would like to thank Felix Cao, Scott Li, Yiyu Fang, Damon Van Voorhis, Lynn Wacha, and Andrea Steffens of Optum, for dataset programming support, as well as Stephanie Curran, of Optum, for project management.
These data have been previously presented in abstract/poster form at the American Thoracic Society International Conference, May 14–19, 2021: Bogart M, Bunner SH, Johnson MG, Bengtson LGS. Benefits of Initiating Single-Inhaler Triple Therapy (SITT) with Fluticasone Furoate/Umeclidinium/Vilanterol (FF/UMEC/VI) Versus Multiple-Inhaler Triple Therapy (MITT) Among Medicare Advantage with Part D Beneficiaries with Chronic Obstructive Pulmonary Disease (COPD). B39. COPD MANAGEMENT: FROM PHARMACOLOGIC TREATMENT TO NOVEL THERAPIES.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all of these areas; took part in drafting, revising, or critically reviewing the manuscript; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by GSK (study numbers 214316 and 214318) The sponsor was involved in study conception and design, and the decision to submit the article for publication. The sponsor was also given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Disclosure
MB was an employee of GSK and held stock/shares in GSK at the time of the study conduct. KKD is an employee of GSK and holds stock/shares in GSK. LGSB, MGJ, NNG, and SHB are/were employees of Optum, which received research funds from GSK to conduct this study. Current affiliation details for MB: Gilead Sciences, Foster City, CA, USA. Current affiliation details for LGSB: Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA (Boehringer Ingelheim has no connection to this study). Current affiliation details for SHB: Genesis Research, Hoboken, NJ, USA.
References
1. GOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 report); 2022. Available from: https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf.
2. Aaron SD, Vandemheen KL, Fergusson D, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med. 2007;146(8):545–555. doi:10.7326/0003-4819-146-8-200704170-00152
3. Frith PA, Thompson PJ, Ratnavadivel R, et al. Glycopyrronium once-daily significantly improves lung function and health status when combined with salmeterol/fluticasone in patients with COPD: the GLISTEN study, a randomised controlled trial. Thorax. 2015;70(6):519–527. doi:10.1136/thoraxjnl-2014-206670
4. Short PM, Williamson PA, Elder DHJ, Lipworth SIW, Schembri S, Lipworth BJ. The impact of tiotropium on mortality and exacerbations when added to inhaled corticosteroids and long-acting β-agonist therapy in COPD. Chest. 2012;141(1):81–86. doi:10.1378/chest.11-0038
5. Siler TM, Kerwin E, Singletary K, Brooks J, Church A. Efficacy and safety of umeclidinium added to fluticasone propionate/salmeterol in patients with COPD: results of two randomized, double-blind studies. COPD. 2016;13(1):1–10. doi:10.3109/15412555.2015.1034256
6. Singh D, Brooks J, Hagan G, Cahn A, O’Connor BJ. Superiority of “triple” therapy with salmeterol/fluticasone propionate and tiotropium bromide versus individual components in moderate to severe COPD. Thorax. 2008;63(7):592–598. doi:10.1136/thx.2007.087213
7. Bogart M, Stanford RH, Laliberté F, Germain G, Wu JW, Duh MS. Medication adherence and persistence in chronic obstructive pulmonary disease patients receiving triple therapy in a USA commercially insured population. Int J Chron Obstruct Pulmon Dis. 2019;14:343–352. doi:10.2147/copd.S184653
8. Gaduzo S, McGovern V, Roberts J, Scullion JE, Singh D. When to use single-inhaler triple therapy in COPD: a practical approach for primary care health care professionals. Int J Chron Obstruct Pulmon Dis. 2019;14:391–401. doi:10.2147/copd.S173901
9. Humenberger M, Horner A, Labek A, et al. Adherence to inhaled therapy and its impact on chronic obstructive pulmonary disease (COPD). BMC Pulm Med. 2018;18(1):163. doi:10.1186/s12890-018-0724-3
10. Restrepo RD, Alvarez MT, Wittnebel LD, et al. Medication adherence issues in patients treated for COPD. Int J Chron Obstruct Pulmon Dis. 2008;3(3):371–384. doi:10.2147/COPD.S3036
11. Zhang S, King D, Rosen VM, Ismaila AS. Impact of single combination inhaler versus multiple inhalers to deliver the same medications for patients with asthma or COPD: a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:417–438. doi:10.2147/copd.S234823
12. US Food and Drug Administration. Highlights of prescribing information - TRELEGY ELLIPTA; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/209482s010s011lbl.pdf.
13. Ferguson GT, Brown N, Compton C, et al. Once-daily single-inhaler versus twice-daily multiple-inhaler triple therapy in patients with COPD: lung function and health status results from two replicate randomized controlled trials. Respir Res. 2020;21(1):131. doi:10.1186/s12931-020-01360-w
14. Halpin DMG, Rothnie KJ, Banks V, et al. Comparative adherence and persistence of single- and multiple-inhaler triple therapies among patients with chronic obstructive pulmonary disease in an English real-world primary care setting. Int J Chron Obstruct Pulmon Dis. 2022;17:2417–2429. doi:10.2147/copd.S370540
15. Alcázar-Navarrete B, Jamart L, Sánchez-Covisa J, Juárez M, Graefenhain R, Sicras-Mainar A. Clinical characteristics, treatment persistence, and outcomes among patients with COPD treated with single- or multiple-inhaler triple therapy: a retrospective analysis in Spain. Chest. 2022;162(5):1017–1029. doi:10.1016/j.chest.2022.06.033
16. Halpin DMG, Worsley S, Ismaila AS, et al. INTREPID: single- versus multiple-inhaler triple therapy for COPD in usual clinical practice. ERJ Open Res. 2021;7(2):00950–2020. doi:10.1183/23120541.00950-2020
17. Vestbo J, Papi A, Corradi M, et al. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group, randomised controlled trial. Lancet. 2017;389(10082):1919–1929. doi:10.1016/s0140-6736(17)30188-5
18. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
19. Desai RJ, Franklin JM. Alternative approaches for confounding adjustment in observational studies using weighting based on the propensity score: a primer for practitioners. BMJ. 2019;367:l5657. doi:10.1136/bmj.l5657
20. Xu S, Ross C, Raebel MA, Shetterly S, Blanchette C, Smith D. Use of stabilized inverse propensity scores as weights to directly estimate relative risk and its confidence intervals. Value Health. 2010;13(2):273–277. doi:10.1111/j.1524-4733.2009.00671.x
21. Rosenbaum PR, Rubin DB. Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am Stat. 1985;39(1):33–38. doi:10.1080/00031305.1985.10479383
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.