Back to Journals » Clinical Interventions in Aging » Volume 20
Contezolid for the Super-Elderly: Balancing Efficacy and Safety Through Pharmacokinetic Insights
Authors Liu T, Liang B, Liu B, Huang D, Zhang N, Fang X, Li H ![]() , Cai Y
, Cai Y ![]()
Received 16 July 2025
Accepted for publication 27 October 2025
Published 11 November 2025 Volume 2025:20 Pages 1963—1973
DOI https://doi.org/10.2147/CIA.S554322
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Tingting Liu,1,* Beibei Liang,2,* Bing Liu,3,* Dengfeng Huang,2 Na Zhang,2 Xiangqun Fang,1 Hongxia Li,1 Yun Cai2
1Department of Pulmonary and Critical Care Medicine, The Second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China; 2Center of Medicine Clinical Research, Department of Pharmacy, Medical Supplies Center, The First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China; 3Department of Adult Cardiac Surgery, The Sixth Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun Cai, Email [email protected] Hongxia Li, Email [email protected]
Background: Contezolid is a new oxazolidinone antibacterial agent, and its pharmacokinetic (PK) characteristics and safety in super-elderly patients remain poorly understood.
Methods: Contezolid PK parameters were analyzed in enrolled super-elderly patients (≥ 80 years), with systematic assessment of steady-state profiles and adverse events.
Results: Thirteen super-elderly patients (mean age: 94.9 ± 4.8 years) were included in the study. The plasma concentrations of contezolid peaked at 2– 3h post administration. Both Cmax and AUC0-t exhibited dose-dependent increases across regimens (400 mg q24h, 400 mg q12h, and 800 mg q12h). When receiving a dosage of 800 mg q12h, super-elderly patients demonstrated comparable Cmax (20.32 vs 26.45 mg/L), AUC0-t (97.80 vs 90.38 h·mg/L), and clearance (9.08 vs 10.20 L/h) values to those of healthy adults but prolonged Tmax (2.67 vs 0.57 h) and shorter t1/2 values (2.33 vs 4.84 h). For pathogens with a minimum inhibitory concentration (MIC) ≤ 1 mg/L, 400 mg of contezolid q12h resulted in a > 90% probability of target attainment (PTA), whereas doubling the dose to 800 mg q12h resulted in a PTA > 90% against pathogens with MICs of 2– 4 mg/L. Contezolid was well tolerated, with mild gastrointestinal adverse reactions (vomiting, n=2) and elevated AST (n=1), γ-GT (n=2), and lipase (n=1) levels. According to a self-controlled analysis of 9 patients who switched from linezolid to contezolid, the incidence of thrombocytopenia was significantly lower when taking contezolid (11.1% vs 77.8%).
Conclusion: Contezolid has comparable PKs in super-elderly and healthy adults. While a dosage of 400 mg q12h is sufficient for pathogens with MICs ≤ 1 mg/L, a higher dosage of 800 mg q12h is recommended for higher MICs (2– 4 mg/L), with both doses demonstrating favorable safety.
Clinical Trial Registration Number: ChiCTR2200056377; 4/2/2022.
Keywords: contezolid, super-elderly patients, pharmacokinetics, optimal dose regimens, safety
Introduction
Contezolid is an orally administered oxazolidinone-class antibacterial agent developed for treating multiple-drug-resistant Gram-positive bacterial infections, including methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE). Contezolid is metabolized via flavin-containing monooxygenase-5 (FMO5), whereas linezolid undergoes monoamine oxidase (MAO)-dependent metabolism. This distinct metabolic pathway utilized by contezolid contributes to the significantly reduced myelotoxicity and minimal effects of contezolid on cardiac repolarization or QT interval prolongation.1,2
In a pharmacokinetic (PK) study of healthy Chinese adults receiving multiple doses of 800 mg q12h, steady-state parameters revealed a mean peak plasma concentration (Cmax) of 26.45 mg/L, elimination half-life (t1/2) of 4.84 hours, and an area under the plasma concentration‒time curve from 0 to 24h (AUC0-24) of 90.38 mg/h/L, whereas no drug accumulation was observed over 15 days of treatment.3 Contezolid is rapidly absorbed, reaching a peak concentration approximately 0.5–1 h following oral administration.3 Contezolid should be administered within 30 minutes after meals to optimize absorption, as food significantly enhances its absorption.1,3,4 Based on the PK/pharmacodynamic (PD) target attainment (fAUC0-24/MIC ≥ 2.3), the 800 mg (two 400 mg tablets) every 12 hours (q12h) regimen is recommended for treating Gram-positive bacterial infections with minimum inhibitory concentration (MIC) values of ≤ 4 mg/L.5,6
The elderly population presents unique pathophysiological characteristics, including impaired hepatic/renal function, hypoproteinaemia, multiple comorbidities, and polypharmacy. These factors collectively lead to significant alterations in antimicrobial pharmacokinetics.7 The drug label for contezolid states that no dose adjustment is required in elderly patients aged 65–75 years. This recommendation is based on findings that weight-adjusted steady-state area under the plasma concentration‒time curve (AUC) values in this population are less than 10% different from those in younger patients (< 60 years).8 However, super-elderly patients (≥ 80 years) remain pharmacokinetically and physiologically distinct from the general elderly population, which necessitates tailored therapeutic strategies.7 Our previous study revealed significant alterations in the PK profiles of linezolid among super-elderly patients that manifested as prolonged t1/2 and reduced clearance (CL). These physiological changes are associated with drug overexposure and, consequently, increases in toxicity-related adverse events.9,10 Compared with linezolid, which has hematologic toxicity risks, conezolid has superior safety and thus has significant therapeutic potential for the super-elderly population.11 However, the lack of safety and PK data in this population leaves critical questions unanswered about dose adjustment strategies.
This single-center, prospective observational cohort study was conducted to characterize the PK/PD profiles of contezolid in super-elderly patients across diverse clinical scenarios and aimed to address critical evidence gaps in geriatric antimicrobial stewardship.
Methods and Materials
Patients and Study Design
This single-center, open-label, observational study prospectively enrolled super-elderly patients (aged ≥ 80 years) who were receiving multiple doses of contezolid at our hospital from October 2023 to December 2024. The exclusion criteria were as follows: duration of contezolid treatment < 5 days; renal replacement therapy; refusal of blood sample collection; uncontrolled acute/chronic diseases (eg, acute myocardial infarction, respiratory failure, heart failure, etc).; severe renal dysfunction (estimated glomerular filtration rate ≤ 30 mL/min/1.73m2); abnormal liver function; hypoproteinemia; immunocompromised status; or immunosuppressant use. The specific dosing regimen of contezolid was determined by the treating physician and any deviations from the clinically recommended dosage were permitted based on individualized patient assessment.
PK Sample Collection and Determination
Blood samples were collected under steady-state conditions (≥ 5 days after initiating contezolid therapy) at the following post-dose timepoints: 2, 3, 4, 6, 8, 10, and 12 hours. Peripheral blood (1 mL) was drawn from the antecubital fossa into EDTA-coated tubes (Becton Dickinson, USA). The samples were subsequently centrifuged at 3500 × g for 5 min, after which the plasma was stored at −20 °C. Contezolid concentrations were quantified using liquid chromatography‒tandem mass spectrometry (LC-MS/MS) according to our previously established method,12 with a linear range of 0.05–15 mg/L (LLOQ: 0.05 mg/L) and inter/intrabatch precision ≤ 5.79%.
PK Analysis
WinNonlin noncompartmental analysis (version 8.4, Certara, USA) was used to estimate steady-state plasma concentration‒time profiles following multiple-dose administration of contezolid and derive the following parameters: Cmax, the time to Cmax (Tmax), the area under the plasma concentration‒time curve from time 0 to 12h (AUC0-12), the area under the plasma concentration‒time curve from time 0 infinity (AUC0-∞), t1/2, apparent oral clearance (CL/F), and the apparent volume of distribution (Vz/F).
Probability of Target Attainment (PTA)
PTA was calculated based on the actual achievement of the target in different dose groups. The area under the plasma concentration‒time curve from time 0 to 12h (AUC0-12) was calculated by Nonparametric superposition analysis using WinNonlin. The fAUC0-24 was calculated using AUC0-12 and the 90% human plasma protein binding rate of contezolid mentioned in the instructions. Based on established consensus criteria, the PK/PD target of contezolid was defined as fAUC0-24/MIC ≥ 2.3.1
Safety and Tolerability Assessments
Clinical gastrointestinal symptoms, serum enzyme markers, and hematological markers were used to evaluate the safety and tolerability of contezolid. Indicators such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), γ-glutamyl transpeptidase (γ-GT), and blood urea nitrogen (BUN) were considered elevated when they exceeded the upper limit of normal and demonstrated a 1.5-fold increase from baseline levels. Thrombocytopenia was defined as a decrease in the PLT of >30% from baseline during treatment.9 Erythropenia was defined as an erythrocyte count reduction of >30% from baseline during treatment. In patients who had previously received linezolid prior to contezolid administration, the hematological toxicity profiles of the two drugs were compared using a self-controlled study design, with a washout period of >1 week between the administrations of the two drugs.
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics 23.0 (IBM, Armonk, NY, USA). Normally distributed quantitative data are expressed as the means ± standard deviations. Nonnormally distributed quantitative data are presented as medians with interquartile ranges.
Results
Demographic and Clinical Characteristics
A total of 13 elderly patients were included, with a mean age of 94.9 ± 4.8 years; 84.6% (11/13) were male (Table 1). The most common dosage of contezolid used was 400 mg q12 h (9 patients, 69.2%), followed by 800 mg q12 h (3 patients, 23.1%), whereas only 1 patient (7.7%) received 400 mg q24 h (Table 1). All patients were fed an ordinary homogenate diet. The primary indications for contezolid were pneumonia, sepsis/septic shock, and skin/soft tissue infections (SSTIs).
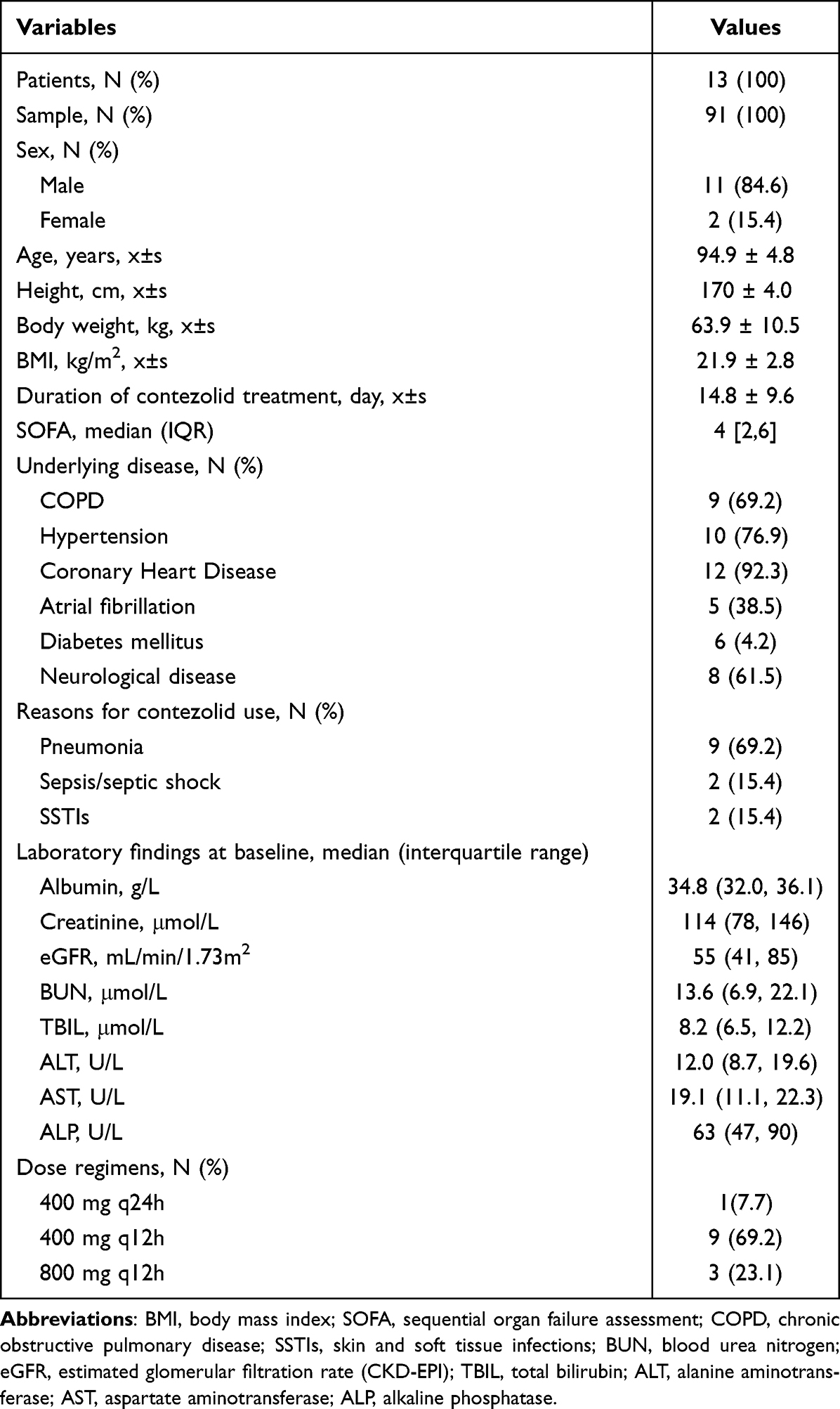 |
Table 1 Demographics and Clinical Characteristics of the Enrolled Super-Elderly Patients |
PK Parameters and PTAs in Super-Elderly Patients
Pharmacokinetic parameters of the 13 enrolled super-elderly patients were shown in Table 2. Both Cmax and AUC0-t values increased with dose, such that increasing the dose from 400 mg q12h to 800 mg q12h led to a greater-than-dose-proportional increases in the mean Cmax (7.74 vs 20.32 mg/L, 164%, Table 3) and AUC0-t (36.50 vs 97.80 h·mg/L, 168%, Table 3). t1/2 increased slightly as the dose frequency increased: 1.37 h for 400 mg q24h, 1.88 h for 400 mg q12h, and 2.33 h for 800 mg q12h. CL/F values decreased in a dose-dependent manner (26.02, 15.22 and 9.08 L/h for the respective regimens, Table 3), whereas Vz/F values were consistent between the 400 mg q12h and 800 mg q12h regimens (31.98 vs 29.48 L, Table 3). The steady-state plasma concentration‒time profiles following the administration of multiple-doses of contezolid are displayed in Figure 1A‒C. For pathogens with MIC ≤1 mg/L, the PTA (fAUC0-24/MIC ≥ 2.3) reached 100% for both the 400 mg and 800 mg dosages administered every 12 hours. However, at higher MICs (2 or 4 mg/L), only the 800 mg q12h dosage regimen maintained a PTA of 100% (Figure 1D).
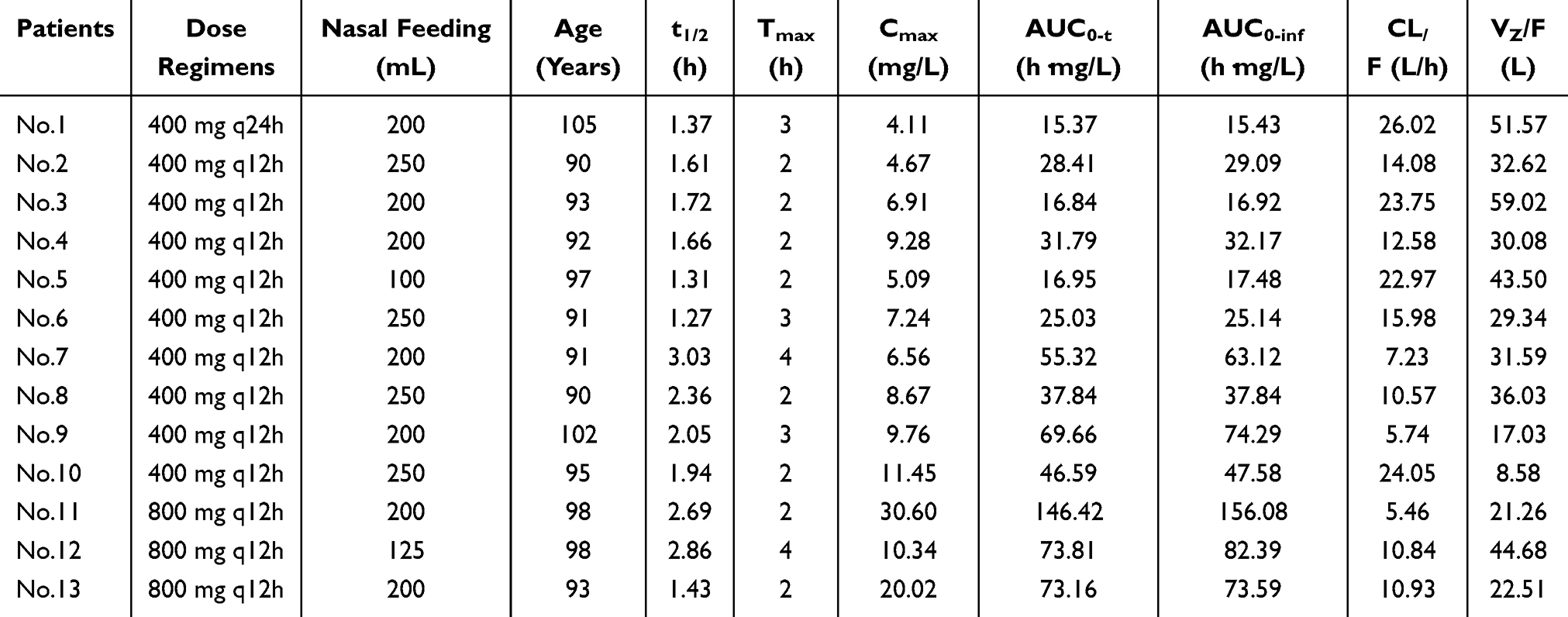 |
Table 2 Pharmacokinetic Parameters of the 13 Enrolled Super-Elderly Patients |
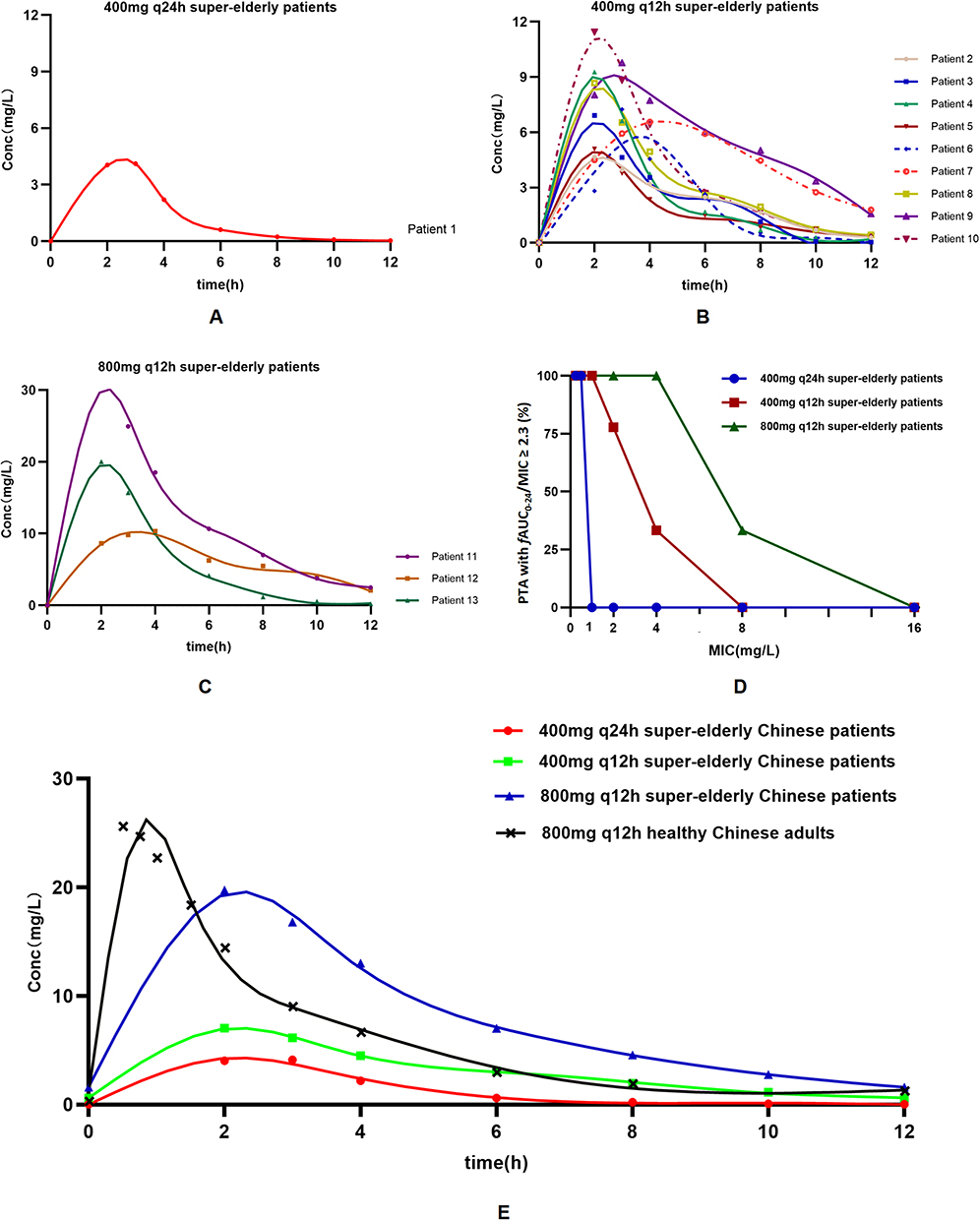 |
Figure 1 Mean plasma concentrations of contezolid in super-elderly patients and healthy adults. (A–C) Mean plasma concentration-time profiles of contezolid following multiple-dose administration (400 mg q24h, 400 mg q12h, and 800 mg q12h); (D) Probability of target attainment (PTA) of AUC0-24/minimum inhibitory concentration (MIC) following oral administration of 400 mg q24h, 400 mg q12h, and 800 mg q12h; (E) Mean plasma concentration-time profiles following multiple-dose administration (400 mg q24h, 400 mg q12h, and 800 mg q12h) across two distinct populations: super-elderly patients and healthy Chinese adults (Data from Clin Ther. 2018 Feb;40(2):322–332.e5.). |
Differences in PK Parameters Between Super-Elderly Patients, SSTIs Patients, and Healthy Adults
The PK parameters of 800 mg q12h contezolid among super-elderly patients, SSTIs patients, and healthy adults are shown in Table 3: super-elderly patients presented a prolonged Tmax compared to healthy adults (2.67 vs 0.57 h) but were comparable to those of SSTIs patients (2.67 vs 3.00 h). Super-elderly patients had a slightly lower mean Cmax than that of healthy adults (20.32 vs 26.45 mg/L) and were higher than that of SSTIs patients (20.32 vs 14.61 mg/L). Comparable AUC0-t values were observed across groups (97.80 vs 90.38 vs 78.37 h·mg/L), while the t1/2 in super-elderly patients was approximately 50% shorter than that in healthy adults (2.33 vs 4.84 h) but closely aligned with that in SSTIs patients (2.33 vs 2.73 h). The steady-state plasma concentration‒time profiles following administration of multiple-doses of contezolid in super-elderly patients and healthy Chinese adults are shown in Figure 1E.
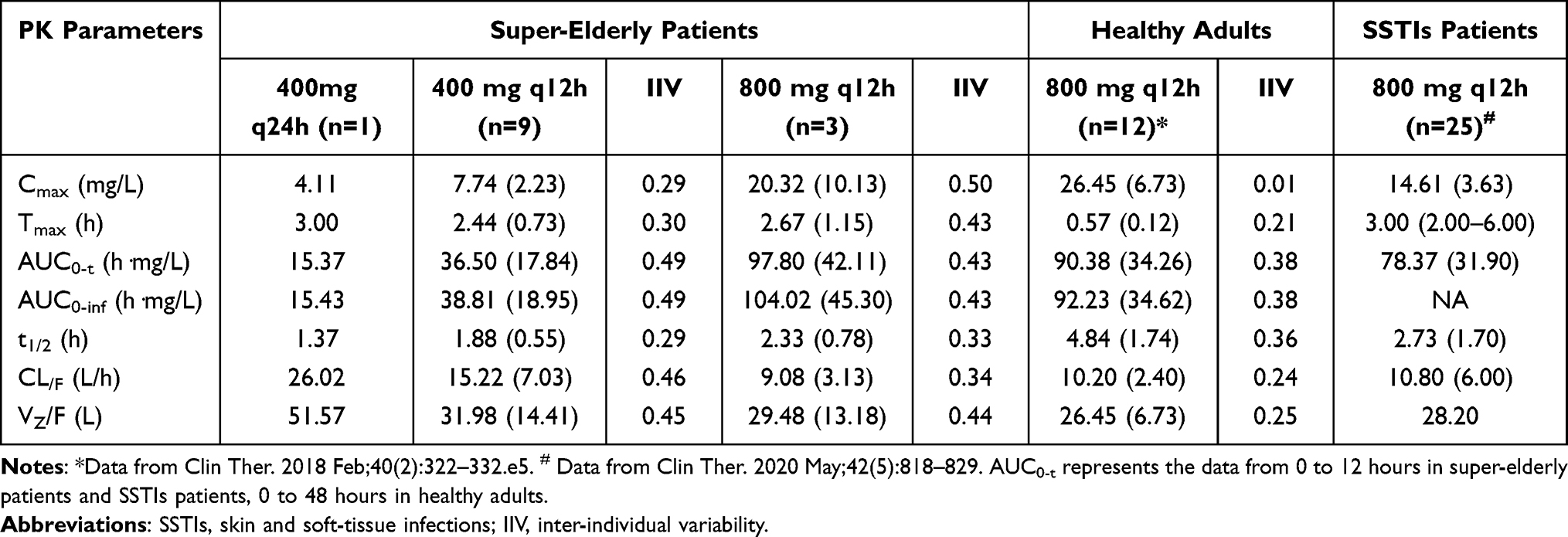 |
Table 3 Mean (SD) Pharmacokinetic Parameters of Contezolid in Super-Elderly Patients, SSTIs Patients and Healthy Adults |
Drug-Related Adverse Events
During contezolid treatment, diarrhea and elevated γ-GT levels each occurred in 2 patients (15.4%, Table 4), whereas elevated AST and lipase levels were observed in 1 patient (7.7%). Additionally, there was 1 case (7.7%) of thrombocytopenia and 1 case (7.7%) of erythropenia (Table 4). Among the three super-elderly patients receiving the recommended contezolid dose (800 mg q12h), adverse events were reported in four instances: one each of diarrhea, erythropenia, and increased AST and γ-GT. In the nine patients on lower-dose regimens (400 mg qd or 400 mg q12h), four instances were reported: one each of diarrhea, thrombocytopenia, and increased lipase and γ-GT. Overall, both the 800 mg and lower dose contezolid regimens were well tolerated, with any drug-related adverse events being mild and reversible upon discontinuation.
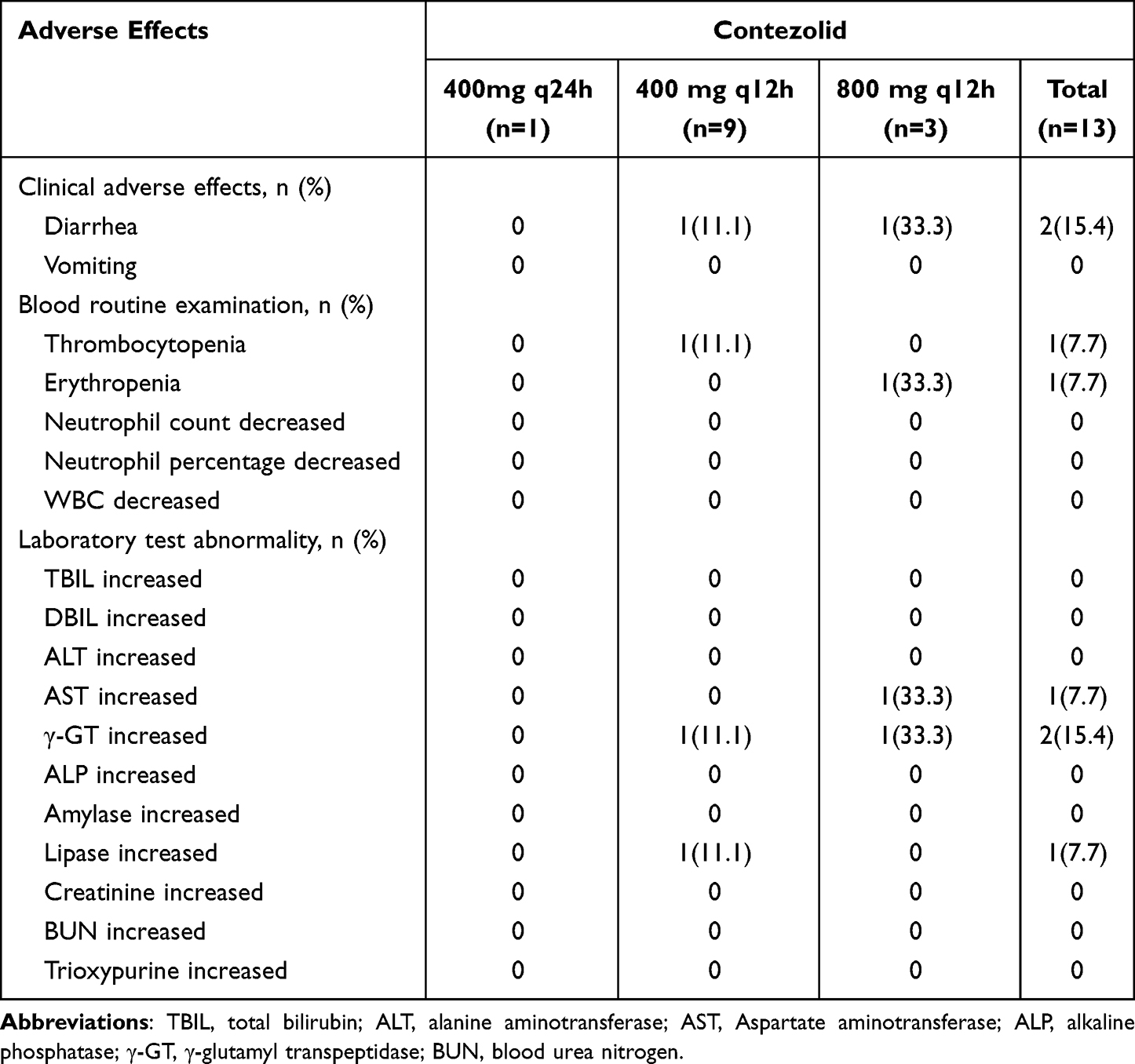 |
Table 4 Drug-Related Adverse Events After Multiple Doses of Contezolid in Super-Elderly Patients |
A Self-Controlled Analysis of Hematological Adverse Events
The decrease in the platelet count and percentage caused by linezolid was significantly greater than that caused by contizolid (Table 5, Figure 2A and B). The incidence of linezolid-induced thrombocytopenia was significantly greater than that of contezolid-induced thrombocytopenia (77.8% vs 11.1%, P=0.003; Table 5, Figure 2C and D). No significant intergroup differences were observed in erythrocyte parameters (Table 5).
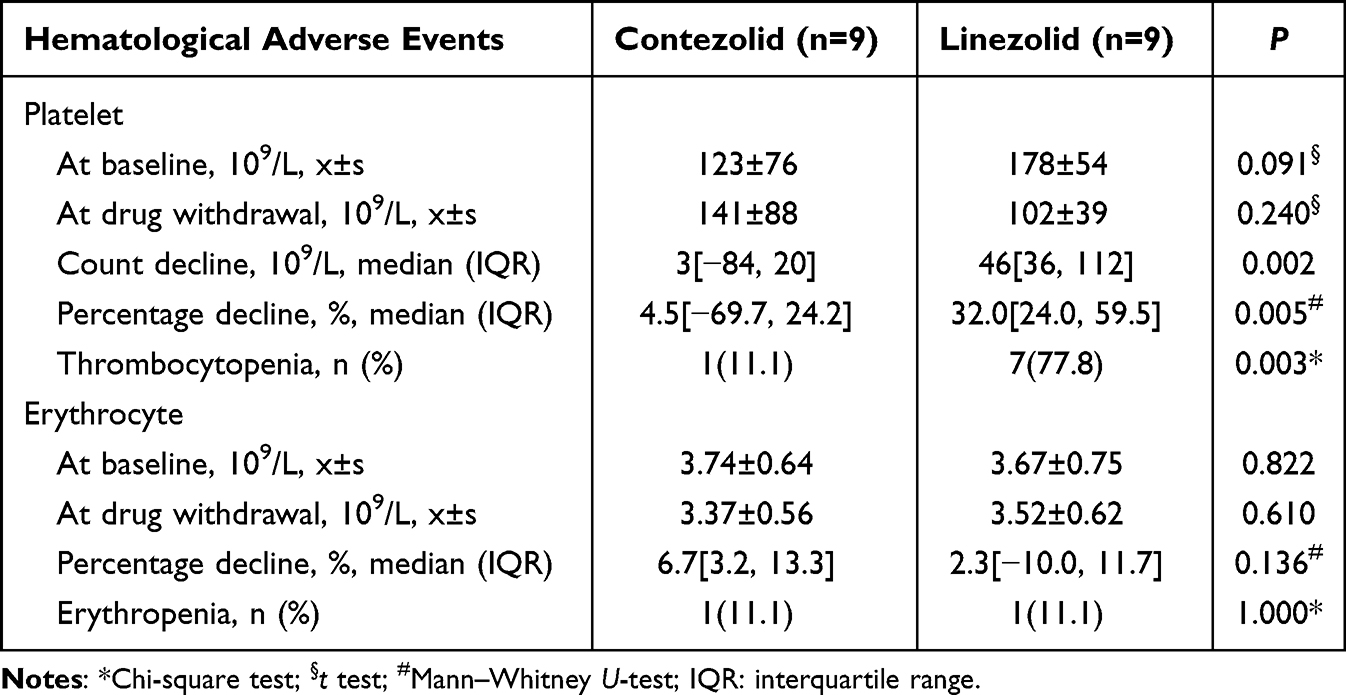 |
Table 5 Self-Controlled Analysis of Adverse Hematological Events in 9 Enrolled Patients |
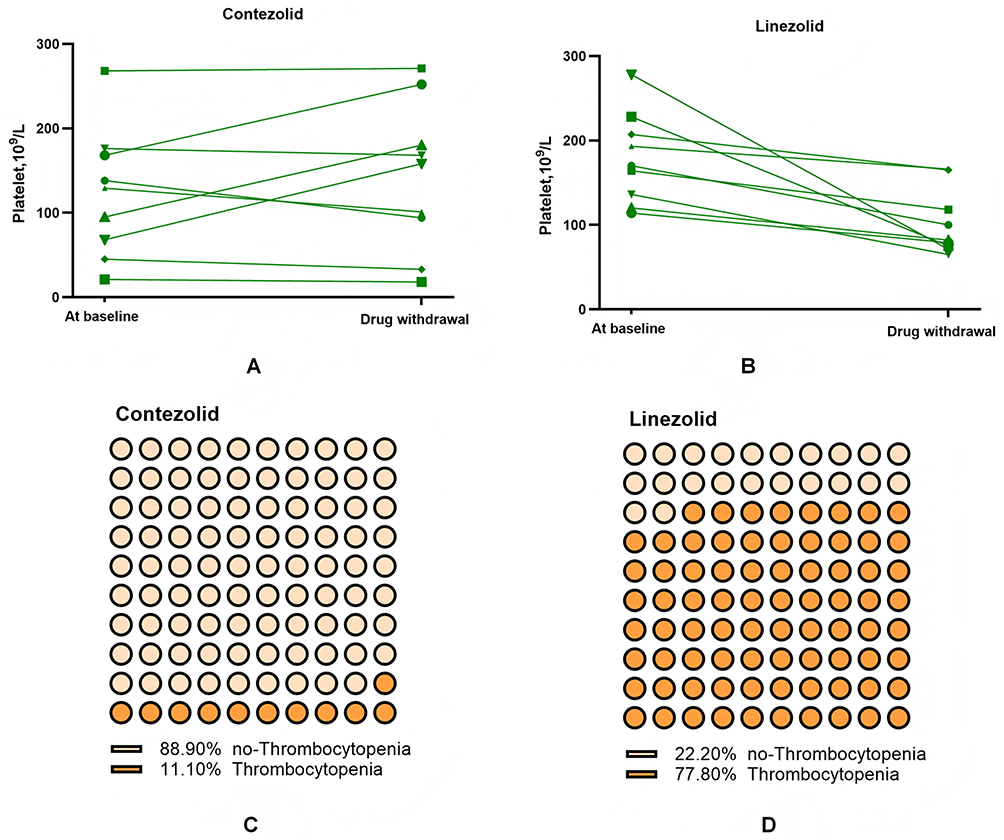 |
Figure 2 A self-controlled analysis of changes in platelet counts and thrombocytopenia using contezolid or linezolid. (A) Changes in platelet counts before and after treatment with contezolid; (B) Changes in platelet counts before and after treatment with linezolid; (C) Probability of thrombocytopenia during treatment with contezolid; (D) Probability of thrombocytopenia during treatment with linezolid. |
Discussion
This PK study revealed distinct multi-dose profiles of contezolid in Chinese super-elderly patients compared with healthy adults. These profiles are characterized by rapid absorption with dose-dependent Cmax/AUC0-t escalation. With the 800 mg q12h regimen, super-elderly patients achieved comparable drug exposure to healthy adults but exhibited a delayed Tmax and accelerated elimination. Target PK/PD attainment supports 400 mg q12h for pathogens with MICs ≤1 mg/L, whereas 800 mg q12h is warranted for strains with MICs ≤ 4 mg/L. Both regimens showed favorable tolerability in this vulnerable population.
Steady-state plasma concentrations are typically achieved on day 3 of dosing under fed conditions.3 In this cohort, all super-elderly patients received ≥5 days of 400 or 800 mg doses under fed conditions before sampling. Following oral administration, plasma concentrations peaked at 2.44–3.00 hours in super-elderly patients which indicates moderately rapid absorption. When multiple doses of 400 mg q12h or 800 mg q12h were administered with a regular diet, the mean Cmax and AUC increased non-proportionally with dose (~160%), whereas t1/2 increased by 24% (1.88 vs 2.33 h) and CL/F decreased by 40% (15.22 vs 9.08 L/h). Due to dysphagia, all the super-elderly patients in the study received nasal feeding for enteral nutrition. Food intake can increase the solubilization and dissolution of contezolid by stimulating bile acid secretion and delaying gastric emptying and gastric fluid volume, all of which increases the extent and rate of drug absorption.13 Overall, the super-elderly patients exhibited generally weaker digestive and absorptive function compared to healthy adults, which contributed to delayed absorption of contezolid. This was particularly evident in Patients 5 and 12, who received a feeding volume of only 100–125 mL. In these two individuals, more pronounced absorption delays and lower Cmax were observed relative to the other elderly patients. Patients 7 and 11 suffered from septic shock, and their clearance significantly decreased (7.23 L/h and 5.46 L/h respectively). Although patient 9 did not have septic shock, due to gastrointestinal bleeding, they had hypovolemic shock and their clearance also significantly decreased (5.74 L/h). Therefore, shock may affect the clearance of contezolid in this study. Contezolid is mainly metabolized by the liver,14 and shock may affect drug metabolism by causing a decrease in liver blood perfusion, thereby influencing the clearance. The 400 mg q24h group demonstrated an abnormal CL (26.02 L/h), which was likely attributable to interindividual variability. Additionally, the small sample size (n=1) for this dose precludes meaningful comparisons with other groups.
Compared with healthy Chinese adults receiving 800 mg q12h, super-elderly patients demonstrated comparable drug exposure, as evidenced by similar AUC0-t values (97.80 vs 90.38 h·mg/L). However, they also exhibited distinct PK characteristics, such as delayed absorption with an obviously longer Tmax (2.67 vs 0.57 h), a reduced peak concentration, a 20% lower Cmax (20.32 vs 26.45 μg/mL), and accelerated elimination with a 50% shorter half-life (2.33 vs 4.84 h).
A previous population PK study revealed that disease status, food intake, and weight significantly affect PK profiles.5,8 Disease status significantly affected the absorption rate,5,8 which may explain the longer Tmax in super-elderly patients and the similar trend of Tmax in patients with SSTIs.8 A potential reason may be that disease status could lead to less physical activity, which decreases gastric emptying and therefore decreased absorption rate.5 Disease status may also influence the medication half-life, which explains the approximately 2-fold decrease in the half-life in super-elderly patients, which is consistent with the SSTIs results.8 Although disease status and body weight affect the periphery volume distribution and central compartment volume,5 the VZ/F and CL/F in the 800 mg q12h dose group were similar in super-elderly patients, healthy adults, and patients with SSTIs (9.08 vs 10.20 vs 10.80 L/h and 29.48 vs 26.45 vs 28.20 L).3,13 Importantly, interindividual variability was amplified in super-elderly patients compared with healthy adults (CL/F: 34% vs 24%; VZ/F: 44% vs 25%, Table 3), underscoring the need for individualized dosing in this population.
The PK properties of contaminants are best described by a two-compartment model with first-order elimination,5 which reveals linear PK characteristics at doses <600 mg and nonlinear behavior at doses >600 mg.3 Its metabolism primarily involves oxidation of the dihydropyridone ring-mediated FMO5 and reductases in hepatocyte cytoplasm,14 with approximately 90% plasma protein binding. This study revealed that when the dose was increased from 400 mg q12h to 800 mg q12h, the Cmax and AUC0-t increased by approximately 160% rather than the expected 100%, indicating nonlinear increases. As the dose increases, FMO5 and reductases reach maximum catalytic capacity, which transitions their metabolism from concentration-dependent first-order kinetics to capacity-limited zero-order kinetics, and reduces CL/F. The plasma protein binding rate of contezolid is as high as 90%. Drug‒protein binding is dose dependent. At low doses, extensive plasma protein binding limits free drug availability. With increasing dose, saturation of protein binding sites increases the unbound drug fraction. In super-elderly patients, this effect is compounded by age-related hypoalbuminemia, which elevates free drug concentrations, However, the serum albumin levels in the enrolled elderly patients were only mildly reduced. As tissue binding approaches saturation, free drug may fail to effectively penetrate tissues and instead accumulates in the bloodstream, ultimately causing a decrease in Vz/F.
For pathogens with MICs ≤1 mg/L, 400 mg q12h achieved adequate PTA. However, 800 mg q12h was required to achieve the predefined PK/PD threshold against pathogens with elevated MICs (2–4 mg/L). The prescribing information indicates that the antibacterial spectrum of contezolid encompasses a broad range of aerobic Gram-positive bacteria. Notably, it is effective against methicillin-resistant staphylococci (eg, MRSA and MRSE), strains of penicillin-intermediate and -resistant Streptococcus pneumoniae, vancomycin-resistant enterococci, and other multidrug-resistant clinical pathogens. According to surveillance data, the MIC90 value of contezolid against Gram-positive strains is mostly ≤1 mg/L.15,16 Carvalhaes et al16 conducted drug susceptibility tests on 1211 clinical Gram-positive strains and reported that contezolid was effective against S. aureus (MIC50/90, 0.5/1 mg/L), coagulase-negative Staphylococcus (MIC50/90, 0.25/0.5 mg/L), Enterococcus (MIC50/90, 0.5/1 mg/L), and Streptococcus (MIC50/90, 1/1 mg/L). The latest 2024 monitoring data from the China Antimicrobial Surveillance Network (CHINET) indicates that 35% of clinical isolates of S. aureus (including both MRSA and MSSA) exhibit a MIC of 2 ug/mL against contezolid.17 Thus, the contezolid dose of 400 mg q12h may be effective against most Gram-positive strains in super-elderly patients according to the PK/PD threshold. When the MIC is 2–4 mg/L, 800 mg q12h could be more appropriate based on the severity of illness and high individual variation.
The enzymes metabolized with contezolid are FMO5, aldehyde ketone reductase (AKR), short-chain dehydrogenase/reductase (SDR), aldehyde dehydrogenase (ALDH), and aldehyde oxidase (AO).14 Since few currently known drugs share above specific metabolic pathway, the potential for clearly established drug-drug interactions is considered limited. Furthermore, as contezolid is not a substrate of CYP450 enzymes and does not undergo metabolism through CYP450 enzymes,14 the potential for interactions with CYP450 inhibitors or inducers is expected to be low. Although contezolid is a substrate of P-glycoprotein (P-gp), it is mainly cleared through metabolic pathways, so P-gp inhibitors are expected to have limited effect on contezolid. Unlike linezolid, contezolid does not significantly inhibit MAO and thus interacts less with MAO substrates (adrenergic drugs or serotonin drugs). Therefore, despite the prevalence of polypharmacy in super-elderly population, the low risk of drug-drug interactions is a key feature that makes contezolid a suitable treatment option for super-elderly patients.
Overall, contezolid demonstrated a favorable safety profile with infrequent and mild adverse reactions. In particular, the 800 mg q12h dose regimen was well tolerated in super-elderly patients, providing a rationale for maintaining the recommended dose. Additionally, compared with linezolid, contezolid demonstrated superior hematologic safety, with a 6-fold reduction in thrombocytopenia incidence (11.1% vs 77.8%) according to self-controlled analysis of nine patients. The two fluorine atoms of contezolid are introduced into the benzene ring (B), causing a significant curvature in the three-dimensional space between the benzene ring (B) and the oxazolidone (A) ring. This structure reduces the permeability of contezolid to human cells and mitochondria, thereby significantly reducing toxicity, especially in terms of bone marrow suppression.12 Actually, in the previous study on the tolerance of contezolid, the hematological toxicity of contezolid was significantly lower compared to linezolid.4 Hemoglobin, neutrophil, and platelet decline occurred in 30%, 30%, and 50% of the linezolid group, compared with 2%, 11%, and 5% of the contezolid group, respectively.4
Most of the adverse events were mild (eg, nausea, headache) and self-limiting, which is consistent with the findings of previous studies.3,4 This safety advantage is critical for super-elderly patients, who exhibit increased susceptibility to myelosuppression.
There were several limitations in this study. First, although we successfully characterized the pharmacokinetics of contezolid in super-elderly patients ≥ 80 years, the small number of participants from a single hospital limit how broadly these findings can be applied. Second, the small sample size prevented comprehensive analysis of factors that may influence interindividual variability in contezolid PK parameters. Finally, most patients had mixed infections, and few tested positives for the target bacteria (only 14% of cultures had Gram-positive bacteria), which makes these results difficult to interpret in terms of clinical and microbial efficacy.
Conclusion
Super-elderly patients present altered physiology, hypoproteinemia, and heightened susceptibility to adverse drug effects, underscoring the need for individualized antibiotic therapy. This study is the first to characterize the pharmacokinetic profile of multiple doses of contezolid in super-elderly patients (≥80 years). Compared with healthy adults receiving the same regimen, super-elderly patients demonstrated comparable drug exposure, delayed absorption, and shorter half-life. Although 400 mg q12h is likely effective against most Gram-positive bacteria, the 800 mg q12h regimen may provide increased therapeutic coverage due to the high interindividual variability and disease severity observed in super-elderly patients without compromising safety. In summary, this study establishes the pharmacokinetic basis for contezolid use in super-elderly patients and informs its optimized, clinically relevant dosing.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (Yun Cai) on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of Chinese PLA General Hospital (Ethical approval number: S2021-609-01) and complied with the Declaration of Helsinki. The written informed consent was obtained from all participants or their legal agents.
Consent for Publication
All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the New Medicine Clinical Research Fund (4246Z512).
Disclosure
The authors declare that they have no competing interests. This paper has been uploaded to SSRN Journal as a preprint: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5210776.
References
1. Hoy SM. Contezolid: first approval. Drugs. 2021;81(13):1587–1591. doi:10.1007/s40265-021-01576-0
2. Wu J, Wang K, Chen Y, Yuan H, Li L, Zhang J. Concentration–response modeling of ECG data from early-phase clinical studies to assess QT prolongation risk of contezolid (MRX-I), an oxazolidinone antibacterial agent. J Pharmacokinet Pharmacodyn. 2019;46(6):531–541. doi:10.1007/s10928-019-09650-7
3. Wu X, Li Y, Zhang J, et al. Short-term safety, tolerability, and pharmacokinetics of MRX-I, an oxazolidinone antibacterial agent, in healthy Chinese subjects. Clin Ther. 2018;40(2):322–332.e5. doi:10.1016/j.clinthera.2017.12.017
4. Eckburg PB, Ge Y, Hafkin B. Single- and multiple-dose study to determine the safety, tolerability, pharmacokinetics, and food effect of oral MRX-I versus linezolid in healthy adult subjects. Antimicrob Agents Chemother. 2017;61(4):e02181–16. doi:10.1128/AAC.02181-16
5. Li L, Wu H, Chen Y, et al. Population pharmacokinetics study of contezolid (MRX-I), a novel oxazolidinone antibacterial agent, in chinese patients. Clin Ther. 2020;42(5):818–829. doi:10.1016/j.clinthera.2020.03.020
6. Wu J, Wu H, Wang Y, et al. Tolerability and pharmacokinetics of contezolid at therapeutic and supratherapeutic doses in healthy chinese subjects, and assessment of contezolid dosing regimens based on pharmacokinetic/pharmacodynamic analysis. Clin Ther. 2019;41(6):1164–1174.e4. doi:10.1016/j.clinthera.2019.04.025
7. Fu G, Sun W, Tan Z, Liang B, Cai Y. An insight into pharmacokinetics and dose optimization of antimicrobials agents in elderly patients. Front Pharmacol. 2024;15:1396994. doi:10.3389/fphar.2024.1396994
8. Yuan H, Wu H, Zhang Y, et al. Clinical pharmacology and utility of contezolid in Chinese patients with complicated skin and soft-tissue infections. Antimicrob Agents Chemother. 2022;66(6):e02430–21. doi:10.1128/aac.02430-21
9. Liu T, Yuan Y, Wang C, et al. Therapeutic drug monitoring of linezolid and exploring optimal regimens and a toxicity-related nomogram in elderly patients: a multicentre, prospective, non-interventional study. J Antimicrob Chemother. 2024;79(8):1938–1950. doi:10.1093/jac/dkae188
10. Liu T, Wu J, Fang X, Xie L, Li H. Optimal dosing regimens for linezolid in older patients. Intensive Care Med. 2025;51(4):791–792. doi:10.1007/s00134-025-07843-y
11. Minamino M, Miyamoto K, Kuwahara M, et al. Characteristics of Guillain-Barré syndrome in super-elderly individuals. J Neurol. 2023;270(4):2191–2196. doi:10.1007/s00415-023-11567-8
12. Zhang G, Liu T, Ren A, Liang W, Yin H, Cai Y. Advances in contezolid: novel oxazolidinone antibacterial in Gram-positive treatment. Infection. 2024;52(3):787–800. doi:10.1007/s15010-024-02287-w
13. Abuhelwa AY, Williams DB, Upton RN, Foster DJR. Food, gastrointestinal pH, and models of oral drug absorption. Eur J Pharm Biopharm. 2017;112:234–248. doi:10.1016/j.ejpb.2016.11.034
14. Meng J, Zhong D, Li L, et al. Metabolism of MRX-I, a novel antibacterial oxazolidinone, in humans: the oxidative ring opening of 2,3-dihydropyridin-4-one catalyzed by Non-P450 enzymes. Drug Metab Dispos. 2015;43(5):646–659. doi:10.1124/dmd.114.061747
15. Guo Y, Han R, Zhang G. Setting of the tentative epidemiological cut-off values of contezolid for staphylococcus aureus, enterococcus faecalis, enterococcus faecium, streptococcus pneumoniae and streptococcus agalactiae. J Antimicrob Chemother. 2023;78(4):1055–1058. doi:10.1093/jac/dkad045
16. Carvalhaes CG, Duncan LR, Wang W, Sader HS. In vitro activity and potency of the novel oxazolidinone contezolid (MRX-I) tested against gram-positive clinical isolates from the United States and Europe. Antimicrob Agents Chemother. 2020;64(11):e01195–20. doi:10.1128/AAC.01195-20
17. 2024 annual surveillance results on bacterial antimicrobial resistance.pptx. n.d. Available from: https://www.chinets.com/Content/File/CHINET.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Pharmacokinetics and Safety with Bioequivalence of Ibuprofen Sustained-Release Capsules of Two Formulations, in Chinese Healthy Volunteers: Bioequivalence Study
Huang C, Yin Z, Yang Y, Mo N, Yang H, Wang Y
Drug Design, Development and Therapy 2023, 17:1881-1888
Published Date: 23 June 2023
Comparative Pharmacokinetics and Bioequivalence Evaluation of Two Formulations of Pramipexole Dihydrochloride Extended-Release Tablets in Healthy Chinese Subjects Under Fasted and Fed States: A Randomized, Open-Label, Single-Dose, Two-Period Crossover Clinical Trial
Yang L, Zhang L, Luo Z
Drug Design, Development and Therapy 2023, 17:2369-2381
Published Date: 15 August 2023
Clinical Utility of Contezolid-Containing Regimens in 25 Cases of Linezolid-Intolerable Tuberculosis Patients
Wang J, Nie W, Ma L, Li Q, Geng R, Shi W, Chu N
Infection and Drug Resistance 2023, 16:6237-6245
Published Date: 19 September 2023
Effect of Food on the Pharmacokinetics of Tenofovir Amibufenamide: A Phase I, Randomized, Open-Label, Two-Period Crossover Trial in Healthy Adult Subjects

Liu J, Wu M, Kai J, Lin M, Zheng Y, Jiang Y, Huang Q, Zhai Y, Qiu Y
Drug Design, Development and Therapy 2023, 17:3061-3072
Published Date: 9 October 2023
Pharmacokinetics and Bioequivalence of Two Fixed-Dose Combination Tablets of Valsartan/Amlodipine (80/5 Mg) in Healthy Chinese Subjects
Tian M, Huang J, Chen Y, Jin Q, Jiang H, Shi C, Mei J, Xu M, Yu X, Yang S
Drug Design, Development and Therapy 2025, 19:11-22
Published Date: 3 January 2025